Embed Size (px)
Citation preview

Universal Neonatal Hearing Screening
November 2007
MSAC reference 17
Assessment report

© Commonwealth of Australia [YEAR]
ISBN <number>
ISSN (Print) 1443-7120
ISSN (Online) 1443-7139
First printed <add month/year>
Paper-based publications
© Commonwealth of Australia [add year] This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no part may be reproduced by any process without prior written permission from the Commonwealth. Requests and inquiries concerning reproduction and rights should be addressed to the Commonwealth Copyright Administration, Attorney General’s Department, Robert Garran Offices, National Circuit, Barton ACT 2600 or posted at http://www.ag.gov.au/cca Internet sites © Commonwealth of Australia [add year of release of home page or electronic document] This work is copyright. You may download, display, print and reproduce this material in unaltered form only (retaining this notice) for your personal, non-commercial use or use within your organisation. Apart from any use as permitted under the Copyright Act 1968, all other rights are reserved. Requests and inquiries concerning reproduction and rights should be addressed to Commonwealth Copyright Administration, Attorney General’s Department, Robert Garran Offices, National Circuit, Barton ACT 2600 or posted at http://www.ag.gov.au/cca Electronic copies of the report can be obtained from the Medical Service Advisory Committee’s Internet site at http://www.msac.gov.au/
Printed copies of the report can be obtained from:
The Secretary Medical Services Advisory Committee Department of Health and Ageing Mail Drop 106 GPO Box 9848 Canberra ACT 2601
Enquiries about the content of the report should be directed to the above address.
The Medical Services Advisory Committee (MSAC) is an independent committee which has been established to provide advice to the Minister for Health and Ageing on the strength of evidence available on new and existing medical technologies and procedures in terms of their safety, effectiveness and cost-effectiveness. This advice will help to inform government decisions about which medical services should attract funding under Medicare.
MSAC recommendations do not necessarily reflect the views of all individuals who participated in the MSAC evaluation.
This report was prepared on behalf of the Medical Services Advisory Committee by Tracy Merlin, Hedyeh Hedayati, Thomas Sullivan, Liz Buckley, Skye Newton, Brent Hodgkinson, Petra Bywood, Fiona Jenner, John Moss and Janet Hiller from Adelaide Health Technology Assessment (AHTA), Discipline of Public Health, University of Adelaide, Adelaide, South Australia. The report was edited by Jo Mason from MasonEdit, South Australia. This recommendation was endorsed by the Minister for Health and Ageing on <date>.
Publication approval number: <number>

Universal neonatal hearing screening iii
Contents
Executive summary................................................................................................. ix Introduction ............................................................................................................14
Rationale for assessment............................................................................................... 14 Rationale for universal neonatal hearing screening .................................................. 14
Background............................................................................................................. 16 Neonatal hearing testing in Australia.......................................................................... 16 What is permanent childhood hearing impairment? ................................................ 17 Testing for hearing impairment in neonates.............................................................. 20 Marketing status of the screening tests....................................................................... 23 Current reimbursement arrangement ......................................................................... 23
Approach to assessment ........................................................................................ 24 Objective......................................................................................................................... 24 Research questions ........................................................................................................ 24 Assessment of screening programs............................................................................. 24 Review of literature ....................................................................................................... 28 Expert advice.................................................................................................................. 35
Results of assessment ............................................................................................ 36 How prevalent is permanent childhood hearing impairment?................................ 36 Safety of universal neonatal hearing screening.......................................................... 42 How accurate are the screening tests? ........................................................................ 51 Is it effective to screen all neonates for hearing impairment?................................. 59 What are the economic considerations?................................................................... 100
Economic model ................................................................................................... 106 Possible hearing testing programs for neonates...................................................... 107 Short-term costs........................................................................................................... 109 Cost-effectiveness of screening protocols ............................................................... 113 Incremental cost-effectiveness ratios........................................................................ 124 Long-term costs ........................................................................................................... 125 Government expenditure ........................................................................................... 134
Discussion............................................................................................................. 142 Prevalence of permanent childhood hearing impairment...................................... 142 Safety of universal neonatal hearing screening........................................................ 142 Effectiveness ................................................................................................................ 144 Diagnostic accuracy of the screening tests............................................................... 144 Effectiveness of universal neonatal hearing screening........................................... 146 Cost-effectiveness of universal neonatal hearing screening .................................. 148
Conclusions........................................................................................................... 153 Clinical need ................................................................................................................. 153

iv Universal neonatal hearing screening
Safety ............................................................................................................................. 153 Effectiveness ................................................................................................................ 153 Economic considerations ........................................................................................... 154 Research implications.................................................................................................. 154 Implementation issues ................................................................................................ 155
Recommendation.................................................................................................. 157 Appendix A MSAC terms of reference and membership.................................. 158 Appendix B Advisory Panel, Evaluator and Project Manager.......................... 160 Appendix C Search strategies ............................................................................ 162 Appendix D Internet sites searched................................................................... 165 Appendix E Critical appraisal checklists........................................................... 170 Appendix F Studies included in the review ....................................................... 176
Included studies on prevalence of permanent childhood hearing impairment.................................................................................................................... 176 Included controlled and descriptive studies on screening safety.......................... 181 Included studies on diagnostic accuracy .................................................................. 185 Included controlled studies on effectiveness of screening .................................... 188 Included descriptive studies on effectiveness of screening ................................... 192 Included economic studies......................................................................................... 214
Appendix G Excluded studies ........................................................................... 219 Appendix H Guidelines for using screening devices .......................................224
Use of the Natus Algo Portable AABR Screener ................................................... 224 Use of the ECHOCHECK hand-held ILO OAE Screener ................................. 228
Appendix I Analysis of published economic evaluations (up to 2003)..............232 Glossary .................................................................................................................254 Abbreviations ........................................................................................................256 References .............................................................................................................258

Universal neonatal hearing screening v
Tables
Table 1 Neonatal hearing screening in Australian States and Territories as at 9th October 2007 ..................................................................................................... 16
Table 2 Neonatal hearing screening equipment listed on the ARTG ........................... 23 Table 3 Evidence dimensions.............................................................................................. 32 Table 4 Grading system used to rank included diagnostic studies ................................ 33 Table 5 Designations of levels of evidence* according to type of research
question (NHMRC 2005) ...................................................................................... 33 Table 6 Quality checklists .................................................................................................... 34 Table 7 Body of evidence assessment matrix ................................................................... 35 Table 8 Prevalence of permanent childhood hearing impairment (PCHI) .................. 37 Table 9 Safety of universal neonatal hearing screening (comparative studies) ............ 46 Table 10 Safety of universal neonatal hearing screening (noncomparative
studies)...................................................................................................................... 50 Table 11 Diagnostic accuracy of hearing screening tests .................................................. 56 Table 12 Effectiveness of universal neonatal hearing screening for secondary
outcomes (controlled studies) ............................................................................... 63 Table 13 Descriptive (uncontrolled) studies of 1-stage universal neonatal
hearing screening .................................................................................................... 71 Table 14 Descriptive (uncontrolled) studies of 2-stage universal neonatal
hearing screening .................................................................................................... 73 Table 15 Descriptive (uncontrolled) studies of 3-stage (or more) universal
neonatal hearing screening .................................................................................... 88 Table 16 Relevant resource items for a neonatal hearing screening program.............. 103 Table 17 Region-dependent design of UNHS program.................................................. 109 Table 18 Identification of 2003 unit costs for neonatal hearing screening................... 110 Table 19 2003 cost of targeted screening by method of AABR delivery for a
cohort of 4,000 infants per year.......................................................................... 115 Table 20 Transitional probabilities for an Australian targeted screening
program .................................................................................................................. 116 Table 21 Transitional probabilities for an Australian UNHS program (protocol
A)............................................................................................................................. 119 Table 22 Transitional probabilities for an Australian UNHS program (protocol
B) ............................................................................................................................. 121 Table 23 Incremental cost of UNHS by choice of 2-stage screening method............. 123 Table 24 Summary cost-effectiveness of three screening options for PCHI in a
birth cohort of 4,000 infants per year ................................................................ 124 Table 25 ICER of three screening options for PCHI in a birth cohort of 4,000
infants per year ...................................................................................................... 124

vi Universal neonatal hearing screening
Table 26 Resources used (in 2003 $AUD) in therapy, rehabilitation and education of infants with PCHI to 18 years of age (or school Year 12) ...... 128
Table 27 2003 cost (discounted @ 5% p.a.) of extra rehabilitation and education per child with bilateral PCHI dependent on age of identification and whether unilateral or bilateral: best case scenario ............ 130
Table 28 Summary: Incremental yield and discounted 2003 costs ($million, discounted @ 5% p.a.) for a UNHSa program over the lifetime of an Australian annual birth cohort of 250,000 infants ........................................... 131
Table 29 One-way threshold analysis: Incremental yield and discounted 2003 costs ($million, discounted @ 5% p.a.) for a UNHSa program over the lifetime of an Australian annual birth cohort of 250,000 infants............ 132
Table 30 Estimated additional government expenditure (all jurisdictions combined) over the first 8 years of a national program of UNHS (2003 costs in $’000)............................................................................................. 136
Table 31 Savings on transfer payments per child with unilateral or bilateral hearing impairment............................................................................................... 139

Universal neonatal hearing screening vii
Figures
Figure 1 Anatomy of the ear................................................................................................. 18 Figure 2 Clinical pathway for universal neonatal hearing screening ............................... 20 Figure 3 Summary of the process used to identify and select studies for the
assessment of universal neonatal hearing screening .......................................... 30 Figure 4 Age at first hearing aid fitting for children born between 1986 and
2002........................................................................................................................... 41 Figure 5 2003 timeline of identification of PCHI in Australia in the absence of
a UNHS program.................................................................................................. 106 Figure 6 Options for neonatal hearing screening programs .......................................... 108 Figure 7 Decision model for targeted hearing screening................................................ 113 Figure 8 Decision model for universal neonatal hearing screening .............................. 118 Figure 9 Two-way threshold analysis: combinations of proportions of hearing-
impaired persons who are unemployed and PCHI infants who attain normal language skills, where a UNHS program for an Australian annual birth cohort will be less costly over the lifetime than no organised screening program .............................................................................. 133
Figure 11 Decision tree for universal and targeted neonatal hearing screening model (Keren et al 2002) ..................................................................................... 233
Figure 12 Decision tree for universal and targeted neonatal hearing screening model (Kemper & Downs 2000)........................................................................ 236
Figure 13 Decision tree for modelled universal neonatal hearing screening protocols (Kezirian et al 2001)............................................................................ 238
Figure 14 Decision tree for modelled universal neonatal hearing screening protocols (Gorga et al 2001) ............................................................................... 240
Figure 15 Decision tree for modelled universal neonatal hearing screening protocols (Boshuizen et al 2001) ........................................................................ 241
Figure 16 Screening protocols for existing 1- and 2-stage universal neonatal hearing screening programs (Vohr et al 2001).................................................. 243
Figure 17 Protocol for universal screening of well and neonatal intensive care unit babies (Gorga et al 2001) ............................................................................. 245
Figure 18 Protocol for 2-stage TEOAE or AABR universal neonatal hearing screening (Lemons et al 2002) ............................................................................ 246
Figure 19 Protocol for 2-stage TEOAE universal neonatal hearing screening (Weirather et al 1997) ........................................................................................... 247
Figure 20 Protocol for 2-stage TEOAE universal neonatal hearing screening (Maxon et al 1995) ................................................................................................ 248


Universal neonatal hearing screening ix
Executive summary
Rationale for assessment
At the July 2002 Australian Health Ministers’ Conference (AHMC) in Darwin, the health ministers considered a proposal by the Queensland Health Minister to establish a universal neonatal hearing screening (UNHS) program for Australia. It was noted that the type of screening protocol used would have a significant impact on both the direct screening and the ongoing diagnostic costs, and that current Australian data on the cost of establishing a UNHS program was not available. In order to inform decision-making regarding this proposal, the AHMC requested the MSAC to commission a full health technology assessment on the safety, effectiveness and cost-effectiveness of UNHS. This would allow an estimation of the potential costs and cost-savings of such a program, and assist with the development of (1) a national evidence-based screening protocol, (2) guidelines/standards of practice, (3) a national minimum data set, and (4) mechanisms to ensure program sustainability.
The impetus for universal screening has been the belief that targeted ‘risk factor’ screening fails to identify more than 50 to 60 per cent of all neonates who eventually display some form of permanent hearing loss. Delays in the identification of hearing impairment have been suggested to profoundly affect the quality of life of children in terms of their communication skills and subsequent education and employment prospects. With the development of transient evoked otoacoustic emissions (TEOAE) tests and automated auditory brainstem response (AABR) tests, screening for hearing impairment can take place when infants are only hours or days old. Potentially, this can have an impact on tertiary prevention by improving the times to referral, diagnosis and early management for hearing-impaired infants.
The procedure
Universal neonatal hearing screening allows for early identification and management of permanent hearing impaired children (PCHI). This means obtaining hearing screening on every infant born in the hospital as early as possible. While, to date, primary prevention of hearing loss in neonates is not apparent, universal hearing screening may reduce the disabilities that appear to be associated with PCHI, such as impairment in language acquisition, learning and speech development. Initial efforts of screening children concentrated on high-risk populations. This included children with a family or perinatal history, or physical examination findings amongst other risk factors. Although, as previously mentioned, this constitutes a large proportion of children, it fails to identify up to 60 per cent of all neonates whom eventually display some form of permanent hearing loss (Thompson et al 2001). Screening tools utilised for universal neonatal hearing screening are the otoacoustic emissions (OAE) test and the automated auditory brainstem response (AABR) test. These are objective measures that respond to different stimuli; sound stimuli evoke otoacoustic emissions from outer hair cells, while AABR, a neurological test of auditory brainstem function, responds to click or tone stimuli. Currently, conventional auditory brainstem response testing is the gold-standard for the diagnosis of hearing impairment in infants.

x Universal neonatal hearing screening
Medical Services Advisory Committee – role and approach
The Medical Services Advisory Committee (MSAC) was established by the Australian Government to strengthen the role of evidence in health financing decisions in Australia. The MSAC advises the Minister for Health and Ageing on the evidence relating to the safety, effectiveness and cost-effectiveness of new and existing medical technologies and procedures, and under what circumstances public funding should be supported.
A rigorous assessment of evidence is thus the basis of decision making when funding is sought under Medicare. In 2003 a team from Adelaide Health Technology Assessment, Discipline of Public Health at the University of Adelaide was engaged to conduct a systematic review of literature on universal neonatal hearing screening. An advisory panel with expertise in this area then evaluated the evidence and provided advice to the MSAC. In 2007 Adelaide Health Technology Assessment was commissioned to update the systematic literature review.
MSAC’s assessment of universal neonatal hearing screening
Clinical need
According to the international literature, the median prevalence of moderate to profound (>35 dB) bilateral permanent childhood hearing impairment (PCHI) is 1.3 per 1,000 infants. The median prevalence of unilateral PCHI of similar severity is 0.6 per 1,000 infants.
There are no population-based data on the prevalence of congenital PCHI in Australia. Using the median international prevalence estimate and multiplying this by the number of yearly birth registrations in Australia (259,800) suggests that 325 Australian children are born annually with moderate to profound bilateral PCHI. Unilateral PCHI of similar severity is estimated to occur in an additional 156 children each year. Overall, it is estimated that 481 Australian children are born each year with either unilateral or bilateral moderate to profound PCHI.
Safety
None of the available studies reported any physical harm resulting from universal neonatal hearing screening (UNHS).
The data available on the psychosocial harms from UNHS are of poor to average quality. The most commonly reported psychosocial outcome of UNHS was maternal anxiety regarding (1) the screen, (2) a false positive result and (3) a screen positive result. Overall anxiety levels were within the normal range, so although anxiety levels were frequently reported as higher when infants screened positive rather than negative, no clinically important differences in anxiety level were found (level III-2 interventional evidence). Likewise, no differences in anxiety were found between parents of unscreened babies, or screened babies, regardless of whether the screening outcome was positive or negative (level III-2 interventional evidence).
Maternal concern about infant’s hearing increased as the number of required tests increased. Levels of depression increased and the quality of interactions with the infant were reported to be statistically significantly lower when babies were screened as positive (level III-2 interventional evidence). It has been suggested that screen status or anxiety

Universal neonatal hearing screening xi
may have an impact on the parental relationship with the child, but in the one controlled study (level III-2 interventional evidence) that reported on parental attitudes to the child, as distinct from quality of interactions, no differences were ascertained. No studies reported on the psychosocial effects of false reassurance or of a true-positive diagnosis.
Diagnostic accuracy of the screening tests
Transient evoked otoacoustic emissions testing versus auditory brainstem response testing
Limited but good quality evidence indicates that the accuracy of transient evoked otoacoustic emissions (TEOAE) is influenced by the level of local ambient noise and the condition of infant ears at testing. Under quiet conditions, the test has been found to possess excellent sensitivity (up to 100%) and good specificity (92%). The ability of an initial TEOAE test to correctly diagnose permanent childhood hearing impairment (PCHI) is very low however, with a positive predictive value of 1.5 per cent. This is likely a consequence of both the frequency of transient hearing losses in newborns due to ear occlusion and the low prevalence of PCHI.
Automated auditory brainstem response testing versus auditory brainstem response testing
One study on an early model of the automated auditory brainstem response (AABR) test demonstrates that it possesses excellent specificity (96%) and good sensitivity (80%) in diagnosing PCHI. The positive predictive value of AABR is very low (2.2%), although marginally better than TEOAE conducted under quiet conditions. Expert opinion indicates that later models of the AABR may have better diagnostic accuracy, although this has yet to be confirmed empirically.
False positives associated with either test could be reduced with the introduction of a second-stage or third-stage screen of initial failures, prior to diagnostic testing. This may, however, result in unnecessary caregiver anxiety and added costs and delays in rehabilitation.
Effectiveness
Change in clinical management
The best evidence (III-1 screening evidence) available indicates that universal neonatal hearing screening has an impact on the clinical management of PCHI. Referral for diagnostic testing, actual PCHI diagnosis, and management of PCHI commonly occurs earlier and more frequently with universal neonatal hearing screening than without universal neonatal hearing screening. Level III-1 screening evidence indicates that the probability of referring an infant for diagnostic testing before the age of six months is nearly three times more likely [RR=2.9, 95%CI 1.4, 6.3] (19 times when controlling for the severity of hearing impairment) with universal neonatal hearing screening, than when universal screening is not available. Infants born during periods of universal neonatal hearing screening are twice as likely to receive a diagnosis of PCHI, than infants born in periods without universal hearing screening [RR=2.3, 95%CI 1.1, 4.7]. The absolute increase in benefit is small, however - an extra five children identified per 10,000 - because of the low prevalence of the condition. There is also an indication that screening may increase the likelihood of PCHI management before the age of ten months by nearly

xii Universal neonatal hearing screening
two and a half times [RR=2.4, 95%CI 1.0, 5.8] (eight times when controlling for the severity of PCHI).
Change in health outcomes
There is limited information available on the effect of universal neonatal hearing screening on primary or patient-relevant outcomes. The results, from two cohort studies (Level III-2 screening evidence) indicate that children with bilateral PCHI born in hospitals with universal neonatal hearing screening have better receptive language, but not expressive language abilities and communicative abilities than children born in hospitals without screening. Information on the impact of universal neonatal hearing screening programs on the longer term outcomes (i.e. educational and employment status) has yet to be reported.
Descriptive data indicate that the majority of universal neonatal hearing screening programs manage to screen over 90 per cent of infants in their catchment area. These programs are largely hospital-based with initial screening occurring prior to discharge. Community-based studies also obtain very good coverage when screening is “piggy-backed” onto other health or immunisation checks at the health clinic or when it occurs in the home. Losses to follow-up commonly occur when there is a long delay prior to re-screening or diagnostic testing of the infant, or when infants and mothers are discharged early from the hospital.
Economic considerations
The economic questions are whether the value to Australian society of implementing a universal neonatal hearing screening (UNHS) program is likely to be greater than that of the current situation, and how widespread the screening coverage should be. The existing situation is varied, and the design of a comprehensive screening system that will cover all Australian infants remains to be completed.
Information published up until 2003 on the cost-effectiveness of UNHS was limited and at times contradictory. Furthermore, no Australian UNHS program has yet to be reported in detail in the literature. As the majority of identified published research examining the cost-effectiveness of existing or modelled UNHS programs is from an American perspective, the results obtained can only suggest what might occur under Australian conditions.
From the available literature it can be concluded that, in the short term, the costs for the additional cases identified and diagnosed by UNHS are greater per unit than those of targeted screening. However, taking a societal perspective over the long term suggests that identifying a larger proportion of hearing-impaired infants at an early stage (ie ≤6 months of age) would result in a cost saving overall. The validity of these estimates of long-term cost savings should be regarded with caution as they are based primarily on observational data and expert opinion.
When an experiment is either not ethical or not feasible, or has simply not yet been carried out, decision analytic modelling can provide insight into the relationship between the costs and outcomes of the intervention. The base case of the model is simulated with the available data thought best to approximate the true situation.
In the short term the model presented in this report predicts that implementing a two-stage automated auditory brainstem response (AABR) universal neonatal hearing

Universal neonatal hearing screening xiii
screening (UNHS) program for a cohort of 250,000 newborns would identify an extra 607 infants with unilateral or bilateral hearing impairment by the age of 6 months compared to no formal screening program, at an incremental cost of $6–$11 million. Where a targeted screening program is already in place, expanding to a universal screening program would identify 319 more infants, at an incremental cost of $4–$8 million. These figures were reported in 2003 Australian dollars as only the literature review for UNHS has been updated until 2007.
The long-term direct cost savings from the reduced need for special education and rehabilitation and the possibility of indirect savings from enhanced productivity in adulthood outweigh by an order of magnitude the costs of the actual screening and diagnosis. Unfortunately, these potential savings are less well researched than the short-term costs and so the estimates are more uncertain. Nevertheless, the long-term savings from implementing a UNHS program derived from this model are in general agreement with previous reports.
Given the salience of the estimate of indirect cost savings in the eventual decision whether or not to implement and to continue to support a national UNHS program, it is important that more valid and accurate estimates of the indirect costs of hearing and language skill impairment be obtained for Australian conditions.
The results of the model presented in this report are influenced by the proportion of infants diagnosed and treated before 6 months of age who actually do achieve normal language skills. Systematic follow-up of these infants is therefore a high research priority.
The detection and long-term management of permanent childhood hearing impairment involves public expenditures from both Federal and State/Territory levels of government, and from both health and non-health departments. Over the long term, the States/Territories stand to save on special education and rehabilitation, and the Federal Government to save on disability support pensions.
Recommendation
MSAC recommended that on the strength of evidence pertaining to <application name> public funding <should/should not> be supported for this procedure.
- The Minister for Health and Ageing endorsed/did not endorse this recommendation on <date>… -
OR
Since there is currently insufficient evidence pertaining to <application name>, MSAC recommended that public funding should not be supported at this time for this procedure.
- The Minister for Health and Ageing endorsed/did not endorse this recommendation on <date> -

Universal neonatal hearing screening 14
Introduction
The Medical Services Advisory Committee (MSAC) has reviewed the use of universal neonatal hearing screening. The MSAC evaluates new and existing health technologies and procedures for which funding is sought under the Medicare Benefits Scheme in terms of their safety, effectiveness and cost-effectiveness, while taking into account other issues such as access and equity. The MSAC adopts an evidence-based approach to its assessments, based on reviews of the scientific literature and other information sources, including clinical expertise.
The MSAC’s terms of reference and membership are at Appendix A. The MSAC is a multidisciplinary expert body, comprising members drawn from such disciplines as diagnostic imaging, pathology, surgery, internal medicine and general practice, clinical epidemiology, health economics, consumer health and health administration.
A team from Adelaide Health Technology Assessment (AHTA), in the Discipline of Public Health, School of Population Health and Clinical Practice, University of Adelaide was engaged to conduct a systematic review of the literature on universal neonatal hearing screening. An advisory panel with expertise in this area then evaluated the evidence and provided advice to the MSAC. The advisory panel members are listed at Appendix B.
This report summarises the assessment of current evidence for universal neonatal hearing screening.
Rationale for assessment
At the July 2002 Australian Health Ministers’ Conference (AHMC) in Darwin, the health ministers considered a proposal by the Queensland Health Minister to establish a universal neonatal hearing screening (UNHS) program for Australia. It was noted that the type of screening protocol used would have a significant impact on both the direct screening and ongoing diagnostic costs, and that current Australian data on the cost of establishing a UNHS program was not available. In order to inform decision-making regarding this proposal, the AHMC requested the MSAC to commission a full health technology assessment on the safety, effectiveness and cost-effectiveness of universal neonatal hearing screening. This would allow an estimation of the potential costs and cost savings of such a program, and assist with the development of (1) a national evidence-based screening protocol, (2) guidelines/standards of practice, (3) a national minimum data set and (4) mechanisms to ensure program sustainability.
Rationale for universal neonatal hearing screening
In general, it is believed that ‘children with hearing loss have delayed development in vocabulary, grammar, conversation and reading’ (Helfand et al 2001). In an annual nationwide survey of over 38,000 students with hearing impairment in the USA, 33 to 50 per cent had at least one limitation in thinking/reasoning, maintaining attention or communication (Gallaudet Research Institute 2001). At present, little can be done in the way of primary prevention of hearing loss in neonates. However, early identification and intervention may reduce the disabilities that appear to be associated with permanent childhood hearing impairment (PCHI), such as language and communication deficit.

Universal neonatal hearing screening 15
The impetus for universal screening has been the belief that targeted ‘risk factor’ screening fails to identify more than 50 to 60 per cent of all neonates who eventually display some form of permanent hearing loss (Thompson et al 2001). Hearing-impaired infants may not be identified until months or even years later when undergoing behavioural response testing (at approximately 8 months of age) or school entry screening (at approximately 5 years of age). Between 2003 and 2006 the average reported age of initial fitting of hearing aids in Australian children was 15 months (Australian Hearing 2007).With universal neonatal hearing screening (UNHS) the fitting of hearing aids could occur as early as 3 months of age (Australian Hearing 2007).
Delays in the identification of hearing impairment have been suggested to profoundly affect the quality of life of children in terms of their communication skills and subsequent education and employment prospects (White 1997; Yoshinaga-Itano et al 2001). A population-based cohort study of Australian hearing-impaired children, aged 7–8 years with normal cognition, found substantial delays in their receptive and expressive language abilities, social-emotional development and reading age, compared to a normative population (Wake et al 2005). This is despite receiving amplification and ongoing rehabilitation once diagnosed (Wake et al 2003).
With the development of OAE and AABR methods, screening for hearing impairment can take place when infants are only hours or days old. This has the potential to impact on tertiary prevention by improving the times to referral, diagnosis and early management for hearing-impaired infants. As both of these tests are currently available for use in Australia for infants designated ‘at risk’ (ie targeted screening), it is suggested that the benefits and harms of UNHS be systematically evaluated.

Universal neonatal hearing screening 16
Background
Neonatal hearing testing in Australia
The procedure
In Australia there are two screening tools currently being used to identify infants with possible permanent childhood hearing impairment (PCHI) that may require further diagnostic assessment. These are the otoacoustic emissions (OAE) test and the automated auditory brainstem response (AABR) test.
Universal screening is currently implemented broadly throughout the Australian Capital Territory, New South Wales, Queensland and South Australia (Table 1). At present the Australian States/Territories differ in their practice of screening neonates for hearing impairment depending on the choice or availability of technology (a two- or three-stage protocol of either OAE testing or AABR testing or both).
Table 1 Neonatal hearing screening in Australian States and Territories as at 9th October 2007
Universal neonatal hearing screeninga State/Territory
State/Territory coverage Type of screening protocolb
Australian Capital Territory Territory-wide Tertiary setting 3-stage: AABR
New South Wales Statewide Tertiary setting 2-stage: AABR - AABR
Northern Territory February-March 2008 Tertiary setting 2-stage: AABR - AABR
Queensland Statewide Tertiary setting 2-stage: AABR - AABR
South Australia Statewide Tertiary setting 1-stage: OAE
Tasmania Partial Tertiary setting 2-stage: AABR - AABR
Victoria Partial Tertiary setting 1-stage: OAE
Western Australia Partial Tertiary setting 2-stage: OAE - AABR
a All babies are screened, irrespective of risk status; b All infants failing the screening stages are referred for diagnostic assessment; AABR = automated auditory brainstem response test; OAE = otoacoustic emissions test. UNHS involves the testing of all newborns, regardless of their risk factor status. This usually involves testing just prior to discharge from hospital or within a few days of delivery. Community-based initiatives have only been piloted in one state, South Australia. In this program initial screening was conducted in a tertiary setting but with comprehensive community-based follow-up (Child and Youth Health 2001).
Approximately 50–70 per cent of children with permanent congenital hearing loss have a ‘risk factor for deafness’ identified before or after ascertainment of the hearing loss (Kennedy et al 1998; Mehl & Thomson 2002). These risk factors are listed in Box 1. Based on the highest level of evidence of UNHS, 8.1 per cent of screened infants were

Universal neonatal hearing screening 17
identified as ‘at risk’ prior to testing (Kennedy et al 1998). Of the children identified with permanent childhood hearing impairment (PCHI), 41 per cent had been admitted to a neonatal intensive care unit or special care baby unit, while a further 33 per cent were well babies who had risk factors for PCHI (eg a family history or a mild craniofacial malformation) (Kennedy et al 1998). Risk factors for PCHI are listed in Box 1.
Box 1 Established risk factors for targeted neonatal hearing screening
Residence in neonatal intensive care unit / special care baby unit for ≥48 hours Prolonged usage (>7 days) of aminoglycosides Family history of permanent childhood deafness Craniofacial abnormality noticeable at birth Perinatal infection (either suspected or confirmed), eg toxoplasmosis, rubella, cytomegalovirus, herpes or acquired meningitis Birthweight <1.5 kilograms Birth asphyxia Chromosomal abnormality, including Down syndrome (Trisomy 21) Exchange transfusion or intrauterine transfusion, eg hyperbilirubinaemia Intracranial haemorrhage
What is permanent childhood hearing impairment?
Hearing impairment occurs when there is a reduction in the ability to perceive sound, resulting from an abnormality anywhere in the auditory system (Columbia University College of Physicians and Surgeons 2002; Pugh 2000).
Hearing impairment can be categorised as either congenital or acquired. Congenital hearing impairment is present at birth or arises shortly thereafter as a consequence of progressive loss, whereas acquired hearing impairment occurs later in the lifespan (Australian Hearing 2003). Acquired hearing loss can be described as perinatal or postnatal. Causes of acquired hearing loss include severe hypoxia, neonatal sepsis/meningitis, viral infections such as mumps, ototoxicity from some medications, hyperbilirubinaemia, prematurity and trauma (especially secondary to head injury).
Hearing impairment may be unilateral or bilateral. In unilateral hearing impairment one ear has normal hearing and the other is hearing impaired. Bilateral hearing impairment indicates that there is hearing loss in both ears.
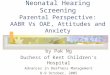
Hearing impairment can result from disorders of the auricle, external auditory canal, middle ear, inner ear, auditory nerve, central auditory pathways and auditory cortex (Figure 1) (Braunwald et al 2001).

Universal neonatal hearing screening 18
Figure 1 Anatomy of the ear
F Jenner. 2003
Hearing losses are usually categorised as conductive, sensorineural or mixed. Conductive hearing impairment occurs when there is interference with the acoustic transmission of sound to the cochlea (Department of Medical Oncology 1998). Causes of conductive hearing impairment in the outer ear include meatal atresia, wax obstruction, infections or tumours of the external ear canal, tympanic membrane perforation or severe scarring (tympanosclerosis). Causes of conductive hearing impairment in the middle ear include middle ear effusions, cholesteatoma, ossicular fixation or discontinuity, or middle ear tumours. Conductive hearing loss may be transient, and is often reversible once the cause has been identified and treated (Columbia University College of Physicians and Surgeons 2002). Speech, language and educational outcomes may be affected if the blockage is chronic, repetitive or not amenable to treatment (Nussbaum 1999).
Sensorineural hearing loss (SNHL) occurs when there is damage to the cochlear hair cells or auditory nerve. This may occur along the auditory pathway from cochlea to the brainstem (Columbia University College of Physicians and Surgeons 2002). SNHL may be genetic or non-genetic and each of these groups may have congenital, acquired or progressive SNHL. Infection, inflammatory causes, ototoxic medications, trauma, loud noise exposure and presbyacusis are potential causes of acquired SNHL (Braunwald et al 2001). SNHL can be further categorised as sensory or neural. Sensory losses are caused by insult to the cochlea by, for example, acoustic trauma or certain viruses such as mumps. Neural loss occurs with auditory nerve problems such as tumours or neurologic disorders. Generally, SNHL cannot be reversed and thus constitutes the majority of permanent childhood hearing impairment (Columbia University College of Physicians and Surgeons 2002). Early identification and intervention can be considered necessary for appropriate language development (Nussbaum 1999).
Mixed hearing loss is the result of a problem in both the conductive pathway (outer or middle ear) and the nerve pathway (inner ear) (Australian Hearing 2003).

Universal neonatal hearing screening 19
Hearing impairment may be defined as slight or mild, moderate, severe or profound. The grades of hearing impairment differ across organisations and countries. The World Health Organization has defined hearing loss (in the better ear) in adults:
• at 26–40 dB as slight or mild hearing impairment. With this hearing loss an individual should be able to hear and repeat words spoken in a normal voice at a distance of one metre.
• at 41–60 dB as moderate impairment. With this impairment an individual can hear and repeat words spoken in a raised voice at a distance of one metre.
• at 61–80 dB as severe hearing impairment. At this level an individual is able to hear some words when shouted into the better ear.
• at 81 dB or greater as profound hearing impairment, including deafness. Individuals with this type of impairment are unable to hear and understand even a shouted voice (Informal Working Group on Prevention of Deafness and Hearing Impairment Programme Planning 1997).

Universal neonatal hearing screening 20
Testing for hearing impairment in neonates
A flowchart outlining the process of clinical decision-making associated with universal neonatal hearing screening, and outcomes of interest, is presented in Figure 2.
Figure 2 Clinical pathway for universal neonatal hearing screening
OAE = otoacoustic emissions test; AABR = automated auditory brainstem response test; HVDT = health visitor distraction test; ABR = conventional auditory brainstem response test; SSEP = steady state evoked potentials test – often not readily available and may not always be necessary; PCHI = permanent childhood hearing impairment. a Some children who pass but have risk factors may be brought in for diagnostic testing at a later stage; b fail in one or both ears.
Initial screen in nursery/community (OAE and/or AABR)
Not universal screening Universal screening
OUTCOMES: Primary – screening yield, rate and quality of language acquisition, behaviour, family functioning, communication ability / social functioning, educational achievement, employment status, socioeconomic status, quality of life
Secondary – age of referral for diagnostic testing, age of PCHI diagnosis, age receiving therapeutic intervention
Passa (well) Failb
Rescreen (OAE and/or AABR) within 3 weeks
One-stage
Two-stage
Testing by indication (risk factors or behavioural). Includes targeted and opportunistic testing using OAE, AABR, HVDT or school age testing.
Failb Diagnostic assessment: diagnostic ABR, OAE, multi-frequency tympanometry, SSEP
Passa (well)
Failb
Referral/manage-ment of PCHI
Passa
Passa

Universal neonatal hearing screening 21
The two tools used for universal neonatal hearing screening are the otoacoustic emissions (OAE) test and the automated auditory brainstem response (AABR) test. These tests are used either singly, followed by diagnostic testing; or as part of a two- or even three-stage screening protocol that includes repeat testing on the same instrument or repeat testing using the other screening tool, or both.
Otoacoustic emissions testing
The cochlea produces what are now termed otoacoustic emissions (OAEs) in response to a sound stimulus. When sound enters the ear in the form of a pressure wave, the ossicles of the middle ear turn this wave into a mechanical force that causes movement of cochlear fluid, resulting in the generation of a wave within the basal membrane (Kemp 2002). This wave travels towards the apex of the cochlea, peaking and then stopping at a specific region of the cochlea unique to the input frequency of the sound. The wave stimulates hair cells located in the organ of Corti, which consists of one row of inner and three rows of outer hair cells. The inner hair cells are necessary for signal transduction to the hearing centres of the brain (Kemp 2003), and the outer hair cells are responsible for sound quality and for amplifying the energy of the wave travelling along the basement membrane. This amplification is necessary as the initial wave rapidly loses energy due to the viscosity of the cochlear fluids and the energy required to stimulate the inner hair cells. While most of the wave energy proceeds in a forward direction toward the apex of the cochlea, some is lost in a backward direction toward the tympanum (eardrum). This backward energy causes the tympanum to vibrate, producing OAEs. Outer hair cells, rather than inner hair cells, are responsible for the production of OAEs. From sound input to otoacoustic emission, the whole process takes anywhere from 3 to 15 milliseconds.
Transient evoked and distortion product otoacoustic emissions testing
Otoacoustic emissions can occur spontaneously in the absence of any external stimuli. They can also be elicited by applying either a single click or tone (via a transient evoked otoacoustic emissions test – TEOAE) or two simultaneous tones (via a distortion product otoacoustic emissions test – DPOAE) to the ear and recording the response from the cochlea (Probst et al 1991).
The term ‘transient’ refers to the presence of a latency period between the intermittent click stimuli and the returning OAEs. Wide band stimuli such as clicks can excite and elicit responses from a wide region of the cochlea. Higher frequency vibrations stimulate areas of the cochlea at its base, while lower frequency vibrations travel farther down towards the apex (Robles & Ruggero 2001). Therefore, OAEs produced by different click frequencies reach the tympanum at different times, depending upon their origin in the cochlea (ie from nearer the base or the apex) (Kemp 2002). By measuring OAE responses at different frequencies, the functionality of different regions of the cochlea can be assessed.
DPOAE responses are produced by introducing two simultaneous tones at different frequencies (F1 and F2) that, in stimulating their respective sites on the basal membrane, generate a distortion product wave of a different frequency that stimulates another set of outer hair cells (Kemp 2002). The resulting distortion product is located somewhere between F1 and F2 and is defined by the function 2F-F2.
These two methods have been described as being complementary (Kemp 2002). TEOAE testing is described as sensitive, having good frequency resolution and efficient – it can

Universal neonatal hearing screening 22
cover a wide range of frequencies in one measurement. However, most ears do not produce TEOAEs over 4 kHz, so background noise must be minimal when conducting the test. Distortion product technology is able to elicit OAEs in normal ears at frequencies over 10 kHz.
Auditory brainstem response testing (reference standard)
Conventional auditory brainstem response (ABR) audiometry consists of a neurological test of auditory brainstem function in response to click or tone stimuli (Scott & Bhattacharyya 2002). These audible stimuli result in the production of action potentials, generated by neurons along the auditory pathway, which are detected by surface electrodes placed on the scalp and earlobe of the individual. Repeated stimulus allows for the collection of multiple responses that are then averaged in an attempt to distinguish real responses from noise (real responses will provide a consistent signal and are more likely to produce a higher average response, while noise is non-synchronous). This technique allows properly trained professionals to identify the presence or absence of auditory brainstem responses from the surrounding noise and determine the hearing level threshold. The advantage of ABR testing is that it is sensitive to both cochlear and retro-cochlear pathology. Currently, conventional ABR testing is the gold-standard for the diagnosis of hearing impairment in infants.
Automated auditory brainstem response testing
With the introduction in many countries of neonatal hearing screening programs, there developed a need for more rapid testing using less technically trained staff. The automated auditory brainstem response (AABR) system consists of a small handheld device that presents fully automated ‘pass/refer’ screening results that require no interpretation by the user (see figure below). The stimulus is provided through an ear-cup fitted over the infant’s ear, and responses are measured through probes attached to the scalp, earlobe, neck and shoulder.
In the automated form of the test a detection algorithm assumes that the infant is hearing impaired and only provides a ‘pass’ when enough responses have been detected to assume with very high probability that the infant has ‘normal’ hearing (a statistical likelihood ratio model). This assumption is based on cross-matching the response with a template from an infant with confirmed normal hearing. Hearing impairment is measured by the level of loss as the ‘decibels (dB) hearing level (HL)’. The AABR test is ideally performed with a click at 35 dB HL that sweeps across a range of frequencies from 500 Hz to 5 kHz. This allows for hearing loss specifically at the intensity level and frequency range of normal speech (≥30 dB HL, 500 Hz to 4 kHz). The automated test is, however, by no means diagnostic, and it is critical to ensure that the equipment is independently calibrated to accurately capture hearing losses greater than 35 dB.

Universal neonatal hearing screening 23
Used with permission, Natus Algo.
Marketing status of the screening tests
The two major categories of tests used for screening for neonatal hearing impairment (otoacoustic emissions testing and automated auditory brainstem response testing) are included on the Australian Register of Therapeutic Goods (ARTG) (see Table 2).
Table 2 Neonatal hearing screening equipment listed on the ARTG
Product name ARTG # Product # Sponsor Oto-acoustic emission instrument 129297 213915 Medtel Pty Ltd Oto-acoustic emission instrument 145411 233456 Central Neurophysiology Supplies Pty Ltd Oto-acoustic emission instrument 94690 165324 GN Resound Pty Ltd Natus ALGO Portable 141199 228603 Scanmedics Pty Ltd Natus ALGO 3 97470 168390 Scanmedics Pty Ltd
Current reimbursement arrangement
Otoacoustic emissions (OAE) testing (MBS Item 11332) and conventional auditory brainstem response testing (ie for diagnostic assessment, MBS Item 11300) are currently listed on the Medicare Benefits Schedule (MBS). Medicare benefits are, however, not payable for OAE audiometry that is undertaken for the purpose of routine screening of infants. According to MBS requirements, the equipment used must be able to display a recorded emission rather than a pass/fail indicator. Automated auditory brainstem response testing is not listed on the Schedule.

Universal neonatal hearing screening 24
Approach to assessment
Objective
The objective of this MSAC assessment was to determine whether there is sufficient evidence to establish a program of universal neonatal hearing screening (UNHS) in Australia.
Research questions
The collated literature was assessed as to its suitability to answer specific, relevant research questions:
1. What is the prevalence of permanent hearing impairment in neonates and infants in Australia?
2. What is the diagnostic accuracy of the tests for permanent childhood hearing impairment when conducted on the neonate or infant?
3. Does universal neonatal hearing screening, and the finding of a positive and/or negative test, affect the clinical management or treatment options available to permanently hearing-impaired infants?
4. Does universal neonatal hearing screening, and therefore possible alterations in clinical management, have an impact on the adverse outcomes associated with permanent childhood hearing impairment?
Assessment of screening programs
Screening is ‘a public health service in which members of a defined population, who do not necessarily perceive they are at risk of, or are already affected by, a disease or its complications, are asked a question or offered a test to identify those individuals who are more likely to be helped than harmed by further tests or treatment to reduce the risk of disease or its complications’ (UK National Screening Committee 2000).
Screening programs can be:
• systematic/universal – mass screening of an entire segment of the population;
• selective – targeting high risk groups (see Box 1) in the population. This includes cascade screening or case finding; and
• opportunistic – screening as a result of a patient’s consultation with a clinician.
(Davies et al 2000; Muir 2001; Murray et al 1999; Schersten et al 1999)
Criteria for appraising the viability, effectiveness and appropriateness of a screening program have been developed by the UK National Screening Committee (UK National Screening Committee 2000) and are presented in Box 2.

Universal neonatal hearing screening 25
It was the aim of the evaluation team to summarise the analysis of universal neonatal hearing screening in terms of these criteria. The evaluation team recognised, however, that information or evidence addressing all of these criteria was unlikely to be available.

Universal neonatal hearing screening 26
Box 2 Criteria for appraising the viability, effectiveness and appropriateness of a screening program (UK National Screening Committee 2000)
The condition Evidence-Based Decision Yes/No/Not applicable/Comment 1.1 The condition should be an important health problem. 1.2 The epidemiology and natural history of the condition, including
development from latent to declared disease, should be adequately understood and there should be a detectable risk factor, or disease marker and a latent period or early symptomatic stage.
1.3 All the cost-effective primary prevention interventions should have been implemented as far as practicable.
The test Evidence-Based Decision Yes/No/Not applicable/Comment 1.4 There should be a simple, safe, precise and validated screening test. 1.5 The distribution of test values in the target population should be known
and a suitable cut-off level defined and agreed.
1.6 The test should be acceptable to the population. 1.7 There should be an agreed policy on the further diagnostic
investigation of individuals with a positive test result and on the choices available to those individuals.
The treatment Evidence-Based Decision Yes/No/Not applicable/Comment 1.8 There should be an effective treatment or intervention for patients
identified through early detection, with evidence of early treatment leading to better outcomes than late treatment.
1.9 There should be agreed evidence based policies covering which individuals should be offered treatment and the appropriate treatment to be offered.
1.10 Clinical management of the condition and patient outcomes should be optimised by all health care providers prior to participation in a screening program.
The screening program Evidence-Based Decision Yes/No/Not applicable/Comment 1.11 There must be evidence from high quality Randomised Controlled Trials
that the screening program is effective in reducing mortality or morbidity.
1.12 Where screening is aimed solely at providing information to allow the person being screened to make an “informed choice” (e.g. Down syndrome, cystic fibrosis carrier screening), there must be evidence from high quality trials that the test accurately measures risk. The information that is provided about the test and its outcome must be of value and readily understood by the individual being screened.
1.13 There should be evidence that the complete screening program (test, diagnostic procedures, treatment/intervention) is clinically, socially and ethically acceptable to health professionals and the public.
1.14 The benefit from the screening program should outweigh the physical and psychological harm (caused by the test, diagnostic procedures and treatment).

Universal neonatal hearing screening 27
Box 2 (cont.) Criteria for appraising the viability, effectiveness and appropriateness of a screening program (UK National Screening Committee 2000)
The screening program (cont.) Evidence-Based Decision Yes/No/Not applicable/Comment 1.15 The opportunity cost of the screening program (including testing,
diagnosis, treatment, administration, training and quality assurance) should be economically balanced in relation to expenditure on medical care as a whole (i.e. value for money).
1.15 There must be a plan for managing and monitoring the screening program and an agreed set of quality assurance standards.
1.16 Adequate staffing and facilities for testing, diagnosis, treatment and program management should be made available prior to the commencement of the screening program.
1.17 All other options for managing the condition should have been considered (e.g. improving treatment, providing other services), to ensure that no more cost effective intervention could be introduced or current interventions increased within the resources available.
1.18 Evidence-based information, explaining the consequence of testing, investigation and treatment, should be made available to potential participants to assist them in making an informed choice.
1.19 Public pressure for widening the eligibility criteria, for reducing the screening interval, and for increasing the sensitivity of the testing process, should be anticipated. Decisions about these parameters should be scientifically justifiable to the public.
This assessment of universal neonatal hearing screening is based on the framework outlined in the MSAC “Guidelines for the assessment of diagnostic technologies” handbook(MSAC 2005).
Assessing the safety and effectiveness of universal neonatal hearing screening (UNHS) was approached using two complementary techniques:
1. assessing studies of screening programs as a whole (direct evidence of the impact of screening on patient relevant outcomes)
2. assessing the diagnostic test performance (diagnostic accuracy) – sensitivity, specificity and accuracy.
Diagnostic accuracy was assessed as it was expected that only limited data would be available from the trials or studies of UNHS programs.
The cost-effectiveness of UNHS was determined on the basis of previously published reports, and was also calculated independently using Australian cost estimates and effectiveness estimates derived from this systematic review of the literature. Information on the methods and results of the economic analysis are presented elsewhere in this assessment report.

Universal neonatal hearing screening 28
Review of literature
The medical literature was searched to identify relevant studies concerning universal neonatal hearing screening (UNHS) for the period between 1966 and August 2007. Appendix C describes the electronic databases that were used for this search and the other sources of evidence – particularly grey literature – that were investigated.
The search terms, presented in Appendix C, were used to identify literature in electronic bibliographic databases on the prevalence of permanent childhood hearing impairment (PCHI); the diagnostic accuracy of the screening tests; the safety, effectiveness and cost-effectiveness of UNHS.
Inclusion/Exclusion criteria
The criteria for including articles varied depending on the type of research question being addressed. Often a study was assessed more than once because it addressed more than one research question. Two researchers separately applied the inclusion criteria to the collated literature to ensure that all potentially relevant studies were captured. In general, articles were excluded if they did not:
• address the research question
• provide information on the pre-specified target population
• include one of the pre-specified interventions
• compare results to a pre-specified comparator
• address one of the pre-specified outcomes and/or provided inadequate numerator and/or denominator data
• have the appropriate study design.
The inclusion criteria relevant to each of the research questions posed in this assessment are provided in Box 3, Box 4, Box 5, Box 6 in the results section of this report.
Grey literature1 was included in the search strategy. Unpublished literature, however, was not canvassed as it is difficult to search for this literature exhaustively and systematically, and trials that are difficult to locate are often smaller and of lower methodological quality (Egger et al 2003). It is, however, possible that these unpublished data (particularly from local screening programs) could have an impact on the results of this review.
In terms of the ‘pre-specified target population’, the definition of a neonate is a live birth who is less than 28 days old (Australian Institute of Health and Welfare 2002). As this is a review of neonatal screening, it would be expected that the target population would only fit into this age category. Neonates and infants up to 6 months of age were, however, included in this assessment of hearing screening for several reasons:
1 Literature that is difficult to find including published government reports, theses, technical reports, non- peer reviewed literature etc.

Universal neonatal hearing screening 29
• to include the critical period for language acquisition in children. Given that the first babbling stage is around 4–6 months of age , it makes sense that for a screening program to have its maximum effect, recognition of PCHI and initial management should occur prior to this stage;
• to ensure that the age period includes both the chronological and corrected (due to pre-term birth) age of the target population;
• to ensure that programs concerning infants not born in hospitals and not immediately screened due to access issues (ie in rural and remote areas) can still be assessed; and
• to exclude the effect of acquired or transient hearing loss (through infection) on the results. Older children are more exposed to situations where they can acquire infections or experience traumas.
Search results
The process of study selection for this report went through six phases:
1. All reference citations from all literature sources were collated into an Endnote 8.0 database;
2. Duplicate references were removed;
3. Studies were excluded, on the basis of the citation information, if it was obvious that they did not meet the pre-specified inclusion criteria. Citations were assessed independently by two reviewers. Studies marked as requiring further evaluation by either reviewer were retrieved for full-text assessment (after discussion);
4. Studies were included to address the research questions if they met the pre-specified criteria again independently applied by two reviewers to the full-text articles. Those articles meeting the criteria formed part of the evidence-base. The remainder provided background information;
5. The reference lists of the included articles were pearled for additional relevant studies. These were retrieved and assessed according to phase 4; and
6. The evidence-base consisted of articles from phases 4 and 5 that met the inclusion criteria.
Any doubt concerning inclusions at phase 4 was resolved by consensus between the two reviewers. A third reviewer was included to arbitrate where necessary. The results of the process of study selection are provided in Figure 3.

Universal neonatal hearing screening 30
Potentially relevant studies identified in the literature searches and screened for retrieval: prevalence (n=3810) accuracy in diagnosis (n=4501) screening (n=2703) cost effectiveness (n=2000)
Studies retrieved for more detailed evaluation: prevalence (n=148) accuracy in diagnosis (n=168) screening (n=276) cost effectiveness (n=145)
Potentially appropriate studies to be included in the systematic review: prevalence (n=38) accuracy in diagnosis (n=11) screening (n=105) cost effectiveness (n=12)
Studies included in the systematic review (n=103) and by outcome: safety (n=10) prevalence (n=19) accuracy in diagnosis (n=5) screening (n=64) cost effectiveness (n=12)
Studies excluded because did not meet inclusion criteria: prevalence (n=110) accuracy in diagnosis (n=157) screening (n=171) cost effectiveness (n=133)
Studies excluded because did not meet the inclusion criteria: prevalence (n=3662) accuracy in diagnosis (n=4333) screening (n=2427) cost effectiveness (n=1855)
Studies excluded, with reasons: Unable to extract data (n= 34) Data included in another paper (n= 15) Data not available (n=10)
Figure 3 Summary of the process used to identify and select studies for the assessment of universal neonatal hearing screening
Data extraction and analysis
A study profile was developed for each included study (see Appendix F) – outlining the level of evidence, study quality, authors, publication year, location, study design, study population characteristics, type of intervention, testing or screening protocol, comparator or reference standard, and outcomes assessed. Studies that were unable to be retrieved, or that met the inclusion criteria but contained insufficient or inadequate data, are provided in Appendix G. Definitions of all technical terms and abbreviations are provided in the appended Glossary and Abbreviations.
Descriptive statistics were extracted or calculated for all safety and effectiveness outcomes (defined in the assessment protocol) in the individual studies, including

Universal neonatal hearing screening 31
numerator and denominator information, means and standard deviations. The power of individual controlled studies to detect a clinically important effect was calculated, assuming that α = 0.05.
Relative risk/rate ratios (RR), absolute risk differences, number needed to screen or diagnose to benefit or harm, and associated 95 per cent confidence intervals, were calculated from individual comparative studies containing count data. The calculated number needed to diagnose was always rounded up to the next whole value, as the value represents the number of infants required for one extra case to be diagnosed, and this cannot be reported as a fraction. By rounding up the value, it will only overestimate the number of infants who need to undergo screening to diagnose one case, not underestimate. Mean differences and 95 per cent confidence intervals were calculated for normally distributed continuous outcomes in individual studies using the independent t-test. Where authors had reported statistical analyses, particularly adjusted analyses (eg analysis of covariance, regression), their results were reported as the primary data were not available to replicate or confirm the result.
Assessing diagnostic accuracy
In the analysis of diagnostic accuracy, calculations of sensitivity, specificity and positive predictive values of tests, with 95 per cent confidence intervals, were undertaken where possible. False positive rates (the complement of test specificity) and false alarm rates (the complement of the positive predictive value of a test) were also calculated in the analyses of diagnostic accuracy and screening effectiveness, respectively. As an analysis of screening effectiveness, as opposed to efficacy (Walter 2003), was undertaken, all data were presented according to intention-to-screen principles. That is, calculations were undertaken using as the denominator those infants that were intended for screening, as opposed to those who were actually screened. For example, if 100 infants were referred for re-screening (eg 20 were lost to follow-up, 40 failed the screen and 40 passed the screen), the failure rate would be calculated as 40/100, rather than 40/80. Data on loss to follow-up, or compliance, were assessed separately.
Meta-analysis was not undertaken as the evidence-base was heterogeneous and there were very few controlled trials of screening. A narrative synthesis of the data was therefore undertaken.
All statistical calculations and testing were undertaken using the biostatistical computer package, Stata version 7.0 (Stata Corporation 2001).
Appraisal of the evidence
The evidence presented in the selected studies was assessed and classified using the dimensions of evidence defined by the National Health and Medical Research Council (NHMRC 2000a).
These dimensions (Table 3) consider important aspects of the evidence supporting a particular intervention and include three main domains: strength of the evidence, size of the effect and relevance of the evidence. The first domain is derived directly from the literature identified as informing a particular intervention. The last two require expert clinical input as part of its determination.

Universal neonatal hearing screening 32
Table 3 Evidence dimensions
Type of evidence Definition Strength of the evidence Level Quality Statistical precision
The study design used, as an indicator of the degree to which bias has been eliminated by design.* The methods used by investigators to minimise bias within a study design. The p-value or, alternatively, the precision of the estimate of the effect. It reflects the degree of certainty about the existence of a true effect.
Size of effect The distance of the study estimate from the “null” value and the inclusion of only clinically important effects in the confidence interval.
Relevance of evidence The usefulness of the evidence in clinical practice, particularly the appropriateness of the outcome measures used.
*See Table 5
The three sub-domains (level, quality and statistical precision) are collectively a measure of the strength of the evidence. With respect, specifically, to diagnostic evidence the individual studies assessing diagnostic effectiveness were graded according to the pre-specified quality and applicability criteria (MSAC 2005) as shown in Appendix E. The designations of the levels of evidence are shown in Table 5. Study quality was assessed using the critical appraisal checklists provided in * A systematic review will only be assigned a level of evidence as high as the studies it contains, excepting where those studies are of level II evidence.
** The dimensions of evidence apply only to studies of diagnostic accuracy. To assess the effectiveness of a diagnostic test there also needs to be a consideration of the impact of the test on patient management and health outcomes. See MSAC (2004) Guidelines for the assessment of diagnostic technologies. Available at: 52Hwww.msac.gov.au . §§ The validity of the reference standard should be determined in the context of the disease under review. Criteria for determining the validity of the reference standard should be pre-specified. This can include the choice of the reference standard(s) and its timing in relation to the index test. The validity of the reference standard can be determined through quality appraisal of the study. See Whiting P, Rutjes AWS, Reitsma JB, Bossuyt PMM, Kleijnen J. The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Medical Research Methodology 2003, 3: 25. †† Well-designed population based case-control studies (eg. population based screening studies where test accuracy is assessed on all cases, with a random sample of controls) do capture a population with a representative spectrum of disease and thus fulfil the requirements for a valid assembly of patients. However, in some cases the population assembled is not representative of the use of the test in practice. In diagnostic case-control studies a selected sample of patients already known to have the disease are compared with a separate group of normal/healthy people known to be free of the disease. In this situation patients with borderline or mild expressions of the disease, and conditions mimicking the disease are excluded, which can lead to exaggeration of both sensitivity and specificity. This is called spectrum bias because the spectrum of study participants will not be representative of patients seen in practice. ‡‡ Studies of diagnostic yield provide the yield of diagnosed patients, as determined by an index test, without confirmation of the accuracy of this diagnosis by a reference standard. These may be the only alternative when there is no reliable reference standard. Note 1: Assessment of comparative harms/safety should occur according to the hierarchy presented for each of the research questions, with the proviso that this assessment occurs within the context of the topic being assessed. Some harms are rare and cannot feasibly be captured within randomised controlled trials; physical harms and psychological harms may need to be addressed by different study designs; harms from diagnostic testing include the likelihood of false positive and false negative results; harms from screening include the likelihood of false alarm and false reassurance results. Note 2: When a level of evidence is attributed in the text of a document, it should also be framed according to its corresponding research question eg. level II intervention evidence; level IV diagnostic evidence. .

Universal neonatal hearing screening 33
Table 4 Grading system used to rank included diagnostic studies
Validity criteria Description Grading System
Appropriate comparison
Did the study evaluate a direct comparison of the index test strategy versus the comparator test strategy?
C1 direct comparison CX other comparison
Applicable population Did the study evaluate the index test in a population that is representative of the subject characteristics (age and sex) and clinical setting (disease prevalence, disease severity, referral filter and sequence of tests) for the clinical indication of interest?
P1 applicable P2 limited P3 different population
Quality of study Was the study designed to avoid bias? High quality = no potential for bias based on pre-defined key quality criteria Medium quality = some potential for bias in areas other than those pre-specified as key criteria Poor quality = poor reference standard and/or potential for bias based on key pre-specified criteria
Study design: NHMRC level of evidence Study quality (QUADAS checklist): Q1 high quality (≥12/14) Q2 medium (10-11/14) Q3 poor reference standard poor quality (<10/14) or insufficient information
Table 5 Designations of levels of evidence* according to type of research question (NHMRC 2005)
Level Diagnostic accuracy ** Screening I * A systematic review of level II studies A systematic review of level II studies II A study of test accuracy with: an independent,
blinded comparison with a valid reference standard, §§ among consecutive patients with a defined clinical presentation ††
A randomised controlled trial
III-1 A study of test accuracy with: an independent, blinded comparison with a valid reference standard, §§ among non-consecutive patients with a defined clinical presentation††
A pseudorandomised controlled trial (i.e. alternate allocation or some other method)
III-2 A comparison with reference standard that does not meet the criteria required for Level II and III-1 evidence
A comparative study with concurrent controls: Non-randomised, experimental trial Cohort study Case-control study
III-3 Diagnostic case-control study †† A comparative study without concurrent controls: Historical control study Two or more single arm study
IV Study of diagnostic yield (no reference standard) ‡‡ Case series
* A systematic review will only be assigned a level of evidence as high as the studies it contains, excepting where those studies are of level II evidence. ** The dimensions of evidence apply only to studies of diagnostic accuracy. To assess the effectiveness of a diagnostic test there also needs to be a consideration of the impact of the test on patient management and health outcomes. See MSAC (2004) Guidelines for the assessment of diagnostic technologies. Available at: www.msac.gov.au . §§ The validity of the reference standard should be determined in the context of the disease under review. Criteria for determining the validity of the reference standard should be pre-specified. This can include the choice of the reference standard(s) and its timing in relation to the index test. The validity of the reference standard can be determined through quality appraisal of the study. See Whiting P, Rutjes AWS, Reitsma JB, Bossuyt PMM, Kleijnen J. The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Medical Research Methodology 2003, 3: 25.

Universal neonatal hearing screening 34
†† Well-designed population based case-control studies (eg. population based screening studies where test accuracy is assessed on all cases, with a random sample of controls) do capture a population with a representative spectrum of disease and thus fulfil the requirements for a valid assembly of patients. However, in some cases the population assembled is not representative of the use of the test in practice. In diagnostic case-control studies a selected sample of patients already known to have the disease are compared with a separate group of normal/healthy people known to be free of the disease. In this situation patients with borderline or mild expressions of the disease, and conditions mimicking the disease are excluded, which can lead to exaggeration of both sensitivity and specificity. This is called spectrum bias because the spectrum of study participants will not be representative of patients seen in practice. ‡‡ Studies of diagnostic yield provide the yield of diagnosed patients, as determined by an index test, without confirmation of the accuracy of this diagnosis by a reference standard. These may be the only alternative when there is no reliable reference standard. Note 1: Assessment of comparative harms/safety should occur according to the hierarchy presented for each of the research questions, with the proviso that this assessment occurs within the context of the topic being assessed. Some harms are rare and cannot feasibly be captured within randomised controlled trials; physical harms and psychological harms may need to be addressed by different study designs; harms from diagnostic testing include the likelihood of false positive and false negative results; harms from screening include the likelihood of false alarm and false reassurance results. Note 2: When a level of evidence is attributed in the text of a document, it should also be framed according to its corresponding research question eg. level II intervention evidence; level IV diagnostic evidence.
Table 6 Quality checklists
Study type Checklist/s Systematic reviews/HTA reports NHMRC Checklist Table 1.4 (NHMRC 2000b) Randomised controlled trials NHMRC Checklist Box 6.1 (NHMRC 2000a) Cohort study NHMRC Checklist Table 1.4 (NHMRC 2000b) Case-control NHMRC Checklist Table 1.4 (NHMRC 2000b) Diagnostic test cross sectional study
QUADAS quality assessment tool (Whiting P 2003)
Intervention case series NHS CRD Quality Assessment Scale (Box 5.9) (Khan et al 2001)
Statistical precision
Statistical precision was determined using standard statistical principles. Small confidence intervals and p-values give an indication as to the probability that the reported effect is real (NHMRC 2000b).
Size of effect in individual studies
It is important to establish whether statistically significant differences are also clinically important. The size of the effect needs to be determined, as well as whether the 95 per cent confidence interval includes only clinically important effects (NHMRC 2000b).
Relevance of evidence in individual studies
Similarly, the outcome being measured in the studies should be appropriate and clinically relevant. Inadequately validated (predictive) surrogate measures of a clinically relevant outcome should be avoided (NHMRC 2000b).
Assessment of the body of evidence
Once the results of the studies were synthesised, the overall conclusion as derived from the body of evidence (Table 7) was presented to answer each clinical question – see Discussion section.

Universal neonatal hearing screening 35
Table 7 Body of evidence assessment matrix
A B C D Component
Excellent Good Satisfactory Poor
Evidence base
several level I or II studies with low risk of bias
one or two level II studies with low risk of bias or a SR/multiple level III studies with low risk of bias
level III studies with low risk of bias, or level I or II studies with moderate risk of bias
level IV studies, or level I to III studies with high risk of bias
Consistency all studies consistent most studies
consistent and inconsistency may be explained
some inconsistency reflecting genuine uncertainty around clinical question
evidence is inconsistent
Clinical impact very large substantial moderate slight or restricted
Generalisability
population/s studied in body of evidence are the same as the target population
population/s studied in the body of evidence are similar to the target population
population/s studied in body of evidence different to target population but it is clinically sensible to apply this evidence to target population
population/s studied in body of evidence different to target population and hard to judge whether it is sensible to generalise to target population
Applicability directly applicable to Australian healthcare context
applicable to Australian healthcare context with few caveats
probably applicable to Australian healthcare context with some caveats
not applicable to Australian healthcare context
Expert advice
An advisory panel with expertise in paediatrics, otorhinolaryngology, audiology, deaf education, epidemiology, consumer issues and neonatal hearing screening was established to evaluate the evidence and provide advice to the MSAC from a clinical and client perspective. In selecting members for advisory panels, the MSAC’s practice is to approach the appropriate medical colleges, specialist societies and associations and consumer bodies for nominees. Membership of the advisory panel is provided at Appendix B.

Universal neonatal hearing screening 36
Results of assessment
How prevalent is permanent childhood hearing impairment?
Nineteen studies met the inclusion criteria delineated in the assessment protocol (Box 3) and provided estimates of the prevalence of permanent childhood hearing impairment (PCHI). Profiles of these studies, including the raw prevalence data, are provided in Appendix F. Eight studies were conducted in the UK, three in the USA, two in Australia, two in Italy, and one each in France, Cyprus, Italy and Austria.
Box 3 Study selection criteria for prevalence
Research question What is the prevalence of permanent hearing impairment in neonates and infants in Australia? Selection criteria Inclusion criteria Population Neonates and infants ≤6 months of age born in (1) Australia or, if this information was
unavailable, in (2) Western countries of similar demographic composition. If information on the prevalence in this age group was unavailable, the criterion was widened to ≤6 years of age.
Outcome Prevalence – proportion of infants with permanent childhood hearing impairment (defined as ≥35 dB).a The source of prevalence estimates was clearly defined – neonatal screening programs, school-entry screening etc.
Study design Cross-sectional surveys (with random sampling), case series of consecutive children, or cohort studies.
Search period In order to obtain relatively recent prevalence estimates, studies published before 1980 were not included.
Language Studies relevant to Australia’s demographic composition are most likely to be published in English. Therefore, studies in languages other than English were not included.
a interested in a total population prevalence or prevalence estimate, rather than the prevalence in ‘high-risk’ groups alone
There were three sources from which prevalence data were ascertained: neonatal hearing screening of well babies only, universal neonatal hearing screening of well and ‘at-risk’ babies and examination of school and/or health records or databases. Table 8 summarises the available prevalence data stratified by level of hearing impairment and source of data ascertainment.
Three studies assessed the prevalence of PCHI greater than 35 dB HL, as ascertained through universal neonatal screening of well and ‘at-risk’ babies. One study conducted in the USA found that sensorineural bilateral hearing loss occurred in 1.8 per 1,000 neonates born between December 1996 and December 1997. Unilateral hearing loss occurred in 0.9 per 1,000 neonates (Stewart et al 2000). A further study conducted in the USA reported a prevalence of sensorineural or conductive hearing loss of 4.4 per 1,000 neonates born between January 1997 and January 2002 (Connolly et al 2005). The higher prevalence estimate reported in this study is likely a result of the relatively high proportion of ‘at-risk’ neonates screened (18.1 per cent of the total sample). An Australian study found lower rates of PCHI in infants born in Western Australia between February 2000 and June 2001. Bilateral hearing loss occurred in 0.7 per 1,000 neonates and unilateral hearing loss in 0.2 per 1,000 neonates (Bailey et al 2002).

Universal neonatal hearing screening 37
Table 8 Prevalence of permanent childhood hearing impairment (PCHI)
PCHI level Country Source of data Prevalence (per 1,000)a
Bilateral >35 dB: 0.7/1,000 Australia UNHS – well and at-risk babies
Unilateral >35 dB: 0.2/1,000
USA UNHS – well and at-risk babies Sensorineural/conductive: 4.43/1,000b >35 dB HL USA UNHS – well and at-risk babies Sensorineural: 2.7/1,000
Bilateral: 1.8/1,000 Unilateral: 0.9/1,000
France UNHS – well babies only Sensorineural (bilateral): 1.4/1,000
UK Quasi-randomised trial. Children born during periods with/without UNHS - well and at-risk babies. Health records also reviewed
Group with UNHS: Bilateral >40 dB: 1.2/1,000 Group without UNHS: Bilateral >40 dB: 1.2/1,000 Overall: Bilateral >40 dB: 1.2/1,000
Germany UNHS – well and at-risk babies Congenital >40 dB: 2.1/1,000b
Italy UNHS – well and at-risk babies Congenital >40 dB: 3.2/1,000 Bilateral: 1.7/1,000
Unilateral: 1.5/1,000
Bilateral >40 dB: 1.3/1,000 41–80 dB: 1.0/1,000
>80 dB: 0.3/1,000
UK UNHS – well and at-risk babies
Unilateral >40 dB: 0.4/1,000 41–80 dB: 0.2/1,000
>80 dB: 0.1/1,000
UK UNHS – well and at-risk babies Bilateral >40 dB: 1.0/1,000
USA UNHS – well and at-risk babies Sensorineural/conductive: 1.5/1,000b
41–70 dB: 0.8/1,000 >70 dB: 0.7/1,000
Australia Other methods – health and/or education records
Bilateral: >40 dB: 1.1/1,000 >60 dB: 0.5/1,000 >90 dB: 0.2/1,000
Austria Other methods – health and/or education records
Congenital >40 dB: 1.3/1,000b
41–69 dB: 0.7/1,000 70–94 dB: 0.3/1,000
>94 dB: 0.3/1,000
UK Other methods – health and/or education records
Congenital: 0.8/1,000b
UK Other methods – health and/or education records
Bilateral >40 dB: 1.2/1,000
UK Other methods – health and/or education records
Congenital (bilateral): 1.8/1,000
>40 dB HL
UK Other methods – source of records not stated
Unilateral >40 dB: 1.2/1,000

Universal neonatal hearing screening 38
Italy UNHS – well and at-risk babies Sensorineural >56 dB: 1.9/1,000b
UK Other methods – health and/or education records
Sensorineural/mixed and congenital/ progressive: >50 dB: 1.1/1,000b
51–64 dB: 0.3/1,000 65–79 dB: 0.3/1,000 80–94 dB: 0.2/1,000
>94 dB: 0.3/1,000
>50 dB HL
Cyprus Other methods – health and/or education records
Congenital (bilateral): >50 dB: 1.2/1,000 51–69 dB: 0.3/1,000 70–94 dB: 0.4/1,000
>94 dB: 0.5/1,000 UNHS = universal neonatal hearing screening. a Rounded estimates – raw data are provided in Appendix F. b Author did not distinguish between unilateral and bilateral hearing loss.
Thirteen studies reported on the prevalence of PCHI greater than 40 dB HL. This was made up of seven studies assessing universal neonatal hearing screening (UNHS) programs, one of which was a quasi-randomised controlled trial (UNHS vs no screening) (Kennedy et al 2005). From the five studies that presented data on bilateral hearing impairment, prevalence in well and at-risk babies was found to range between 1.0 and 1.7 per 1,000. Two of these seven studies also reported the prevalence of unilateral hearing loss in the same population and found it to range between 0.4 and 1.5 per 1,000.
A further six studies reported on the prevalence of PCHI greater than 40 dB HL as estimated by retrospective examinations of health and/or education records. Three of these reported prevalence data on bilateral hearing loss and this varied between 1.1 to 1.8 per 1,000. Unilateral hearing loss was reported in one UK study using records of which the type was not specified, and it found a prevalence of 1.2 per 1,000 (Neary et al 2003).
Three studies reported prevalence data for PCHI greater than 50 dB HL. Davis and Wood (1992) studied a cohort of children in the Nottingham Health District, UK, born between 1983 and 1986. In this population the prevalence of sensorineural/mixed and congenital progressive hearing loss was 1.1 per 1,000. Similar results were obtained in Cyprus, where a cohort of children born between January 1979 and December 1990 had congenital hearing loss at the rate of 1.2 per 1,000 children (Hadjikakou & Bamford 2000). Finally, in a case series of babies born in the hospital of Sciacca, Cyprus between 2003 and 2004 and screened as part of a universal neonatal hearing screening program, the prevalence of sensorineural hearing loss greater than 56 db HL was 1.87 per 1,000 babies (Martines et al 2007).
The heterogeneity in prevalence rates, ranging from 0.7–1.8 infants per 1,000 with bilateral PCHI at all levels of hearing loss, and 0.2–1.5 infants per 1,000 with unilateral impairment at all levels of hearing loss, is unremarkable given the different methods used to measure PCHI, the different case definitions and the varying nature and locations of the sampled population.

Universal neonatal hearing screening 39
Summary
Given the range of prevalence rates, a single estimate for each level of hearing impairment was calculated from the median of the available data. The median prevalence of bilateral and unilateral permanent childhood hearing impairment (PCHI) >35 dB HL is estimated to be 1.3 and 0.6 per 1,000 infants respectively. The median prevalence of bilateral and unilateral PCHI > 40 dB HL is estimated to be 1.3 and 1.2 per 1,000 infants respectively. Lastly, the prevalence of bilateral PCHI > 50 dB is estimated to be 1.2 per 1,000 infants.

Universal neonatal hearing screening 40
Prevalence of permanent childhood hearing impairment in Australia
Two studies provided data on the prevalence of congenital permanent childhood hearing impairment (PCHI) in neonates and infants in Australia (Bailey et al 2002; Russ et al 2003). From these studies the estimated prevalence of moderate to profound bilateral PCHI ranges from 0.7–1.1 per 1,000 infants. This is lower than the median prevalence rate estimated from the international literature. Populations at risk of hearing impairment, such as indigenous, rural or immigrant Australians, are possibly under-represented in the available Australian studies. Population-level PCHI prevalence data are currently not available for Australia, although this may change once the results of the New South Wales Statewide Infant Screening – Hearing (SWISH) program are published.
Using the unrounded median prevalence rate of PCHI greater than 35 dB HL (1.25/1,000) from the international literature as a proxy for the Australian rate, and an estimated 259,800 registered births per year in Australia (ABS 2005), approximately 325 children would be born every year with moderate to profound bilateral PCHI. Unilateral PCHI of similar severity would occur in an additional 156 children born per year. Overall, this would result in 481 Australian children born each year with either unilateral or bilateral moderate to profound permanent hearing impairment.
Data available from Australian Hearing, the body that provides government subsidised hearing assessment services, hearing aid fitting and hearing rehabilitation for all Australian children, indicates that the above estimate is reasonable (Australian Hearing 2007). Rates of hearing aid fittings in children born in the years 1986 to 2001 (the years when there is likely to be reasonably complete data available, including ascertainment of mild hearing loss through school entry screening) ranged from 2.11–3.43 per 1,000 (or between 520 and 878 children per year). These data are, however, probably an over-estimation due to the inclusion of cases of aided mild hearing loss, and acquired or progressive hearing losses that would not be identified through a universal neonatal hearing screening program.
Australian Hearing also provided data on the number of children who have had hearing amplified artificially within the first 12 months of life (Australian Hearing 2007). When converted to rates per 1,000 births and graphed, the trend in improvement of early (<6 months) identification of hearing loss over a 16-year period is evident (Figure 4). This is probably due to improvements in the identification of children at risk of hearing impairment (ie targeted neonatal hearing screening).
Australian Hearing data indicates that 83–94 per cent of children who had their hearing amplified received their hearing aid after the age of 12 months.2 It is unclear, however, how many of these children had acquired hearing loss as opposed to having undetected congenital hearing loss. It is also unclear what additional benefit a program of universal neonatal hearing screening in Australia would provide in terms of identifying children with PCHI in the neonatal period.
2 Based on total hearing aid fittings for children born in the years 1986 to 2001. (Australian Hearing 2007).

Universal neonatal hearing screening 41
Summary
Credible estimates suggest that 325 Australian children are born every year with moderate to profound bilateral PCHI. Unilateral PCHI of similar severity is estimated to occur in an additional 156 newborns each year. Overall, it is estimated that 481 Australian children are born annually with either unilateral or bilateral, moderate to profound PCHI.
Figure 4 Age at first hearing aid fitting for children born between 1986 and 2005
0
0.05
0.1
0.15
0.2
0.25
0.3
1986 1988 1990 1992 1994 1996 1998 2000 2002 2004
Year
Fittin
gs pe
r 1,00
0 birth
s
< 3 months 3 to < 6 months 6 to < 12 months
Source: Adelaide Health Technology Assessment (AHTA), Discipline of Public Health, University of Adelaide. Data provided by Australian Hearing

Universal neonatal hearing screening 42
Safety of universal neonatal hearing screening
Universal neonatal hearing screening (UNHS) was assessed in terms of possible psychosocial and physical harms that may result from any aspect of the screening process.
Studies addressing these issues were assessed for inclusion according to the criteria delineated in Box 4. As the aim was to assess possible harms resulting from the screening of neonates, rather than the diagnosis of PCHI, studies with a population of only true positives were excluded (neonates with PCHI). Harms from a true positive diagnosis of PCHI are likely to be similar regardless of the diagnostic method. With UNHS, any harms are likely to occur earlier in the development of the infant which may or may not be beneficial.
Box 4 Study selection criteria for assessing safety
Research questions Is universal hearing screening safe for neonates and infants? – Are the otoacoustic emissions (OAE) and automated auditory brainstem response (AABR) tests physically safe for the
individual being tested? – What are the harmful consequences of early diagnosis and management of permanent childhood hearing impairment
(PCHI)? Selection criteria Inclusion criteria Population Neonates and infants ≤6 months of age undergoing testing for PCHI, and/or their parents/
caregivers. Intervention Universal, including targeted, neonatal hearing screening using either the OAE or AABR testing
methods. Comparator(s) No universal neonatal hearing screening. Outcomes Adverse psychological, psychosocial or physical health outcomes associated with the testing
procedure, the diagnosis and/or the treatment/management options. Study design Randomised or non-randomised controlled trials, cohort studies, registers or systematic reviews
of these study designs. In the event that the evidence-base lacked these study designs, case-control or cross-sectional studies were acceptable, although low quality, alternatives.
Search period No restriction. Language Studies in languages other than English were only translated and included if they represented a
higher level of evidence than that available in the English language evidence-base.
Physical harms
There were no reported cases of physical harm occasioned by UNHS in any of the available studies.
Psychosocial harms
One of the important aspects of assessing safety is to determine the impact of hearing screening results on the psychosocial health of the infant and the caregiver. Incorrect diagnoses (false positives) may prove to have psychological consequences (eg anxiety) for the parents or caregivers of babies who have been tested, particularly given that this added stressor would occur in the early postnatal period. The impact of false negatives also need to be assessed. The lack of accurate diagnosis and false reassurance may have serious psychosocial consequences for the infants that have been tested, and their families, particularly given the possible lengthy period before confirmation of permanent

Universal neonatal hearing screening 43
childhood hearing impairment (PCHI). These potential adverse consequences would not occur without UNHS.
Altogether, five controlled studies (level III-2) assessed the psychosocial safety of a UNHS program (Crockett et al 2005; Crockett et al 2006; Kennedy 1999; Kolski et al 2007; Watkin et al 1998) (see Table 9). These studies were of generally poor to average quality, with likely selection bias due to poor response rates or participation in the studies. One study was a nested case-control study, while the other four were cohort studies. Four studies used questionnaires to determine the anxiety of mothers whose babies screened positive for hearing impairment, using the validated (in different populations), Spielberger State Trait Anxiety Inventory (Crockett et al 2005; Crockett et al 2006; Kennedy 1999). One of the studies modified the inventory to only include 10 items (Watkin et al 1998). The remaining study used semi-structured interviews, using the Montgomery Åsberg depression rating scale and the anxiety subscale of the Edinburgh post-natal depression scale (Kolski et al 2007).
Neonatal hearing screening was compared against the health visitor distraction test (performed when the infant was over 6 months old) in an average quality cohort study (Crockett et al 2005). Anxiety levels in mothers of babies who screened positive were compared at 3 weeks and again at 6 months after screening. Overall state anxiety levels were between 29.0 and 36.9 on the Spielberger State-Trait Anxiety Inventory, which is in the normal range, and well below the ‘clinical cut-off’ of 49 out of 80, so further comparisons were not made. When satisfaction was compared between mothers of infants who were referred for further testing (from an unvalidated single item question), mothers of those who underwent neonatal hearing screening were significantly more satisfied than mothers of infants who received the distraction test (p<0.05, Cohen’s d=0.72).
Two further studies (Kolski et al 2007; Watkin et al 1998) compared anxiety levels of mothers whose babies received the screening test against mothers who gave birth in hospitals where screening was not available. Babies were age-matched. Kolski et al (2007) found no significant difference between maternal anxiety, depression levels, or any effect on the quality of early interactions when a negative screen was compared against no screening. Similarly, when a positive screen result was compared against a control group with no screening, Watkin et al (1998) found no statistically significant differences between anxiety levels.
Four poor to average quality studies compared anxiety levels in mothers of infants who were referred for further testing, against a control group of mothers whose infants screened negative (Crockett et al 2005; Crockett et al 2006; Kennedy 1999; Kolski et al 2007). Levels of anxiety were low in the three studies that reported mean values on the Spielberger State-Trait Anxiety Inventory. Kolski et al (2007) reported that a positive screening test significantly increased levels of anxiety, depression and reduced the quality of early interactions, but the clinical significance of these differences was unclear as no raw data were provided. Crockett et al (2006) found that the more screening stages that infants are required to undergo (as the potential seriousness of the results increase), the more anxious the mothers became. However, the difference between these levels of anxiety was not statistically significant. The authors proposed that the low response rate to the questionnaire and the delay in sending questionnaires (sent 3 weeks after the completion of screening) may have been responsible for the overall low levels of anxiety reported. Overall, the more knowledge the mothers had about what a referral for further

Universal neonatal hearing screening 44
tests meant, the less anxious (F(1,323)=6.8, p<0.01) or worried (F(1,332)=8.0, p<0.01) they were about the need for them.
When Kolski et al (2007) compared two different hearing screening protocols, one performed in newborns, and another strategy at 2 months of age, no significant differences were found between the anxiety (F(1,139)=0.53, p>0.05) or depression levels (F(1,139=2.97, p>0.05.) in mothers of infants receiving either negative or positive screening results. However, when an analysis of variance was performed according to time of screening, a positive screening result had more impact on anxiety (F(3,139)=3.5, p=0.01) and depression levels (F(3,139)=3.1, p=0.03) when the screening test was in the initial week of life, as compared with 2 months later. Raw data were not presented, so it is unclear whether any of the anxiety levels were outside the normal range, and thus whether there was any clinically important difference between groups on maternal anxiety levels.
One study (Kennedy 1999) did find a statistically significant difference in ‘concern for baby’ but the screen positive group actually presented with less anxiety than the screen negative group (t = -2.0, df = 148, p = 0.04). Mean anxiety scores for the control group were the same or higher than the screen positive group in this study. Anxiety scores in both groups were low overall. Only one study assessed the impact of the screen on mothers’ attitudes to their babies (Kennedy 1999). This controlled study found that mothers of screen positives and screen negatives had very low negative attitudes to their babies and that there was no difference in mean attitudinal scores between the groups.
Information from these controlled studies was supplemented by five descriptive, cross-sectional surveys (Clemens et al 2000; Hergils & Hergils 2000; Tatli et al 2007; Vohr et al 2001; Weichbold & Welzl Mueller 2001) providing information on safety outcomes for the universal screening arm alone, and predominantly assessing the anxiety of parents of screen positive babies (see Table 10). The cross-sectional surveys were generally of poor quality, with anxiety measured using non-validated tools. Two of the studies were possibly affected by recall bias as the questionnaire was administered approximately 5 months after screening (Clemens et al 2000; Hergils & Hergils 2000). One study may also have been affected by selection bias due to a poor response rate to the survey (Clemens et al 2000). These studies indicate that parental anxiety is low (3.8–7.0%) at the initial hearing screen (Hergils & Hergils 2000; Tatli et al 2007; Vohr et al 2001). Parents of babies with normal hearing who screened positive for hearing impairment at the initial test (ie false positives) experienced varying levels of anxiety, with 80 per cent ‘worried’ (Clemens et al 2000), between 17 and 33 per cent ‘worried or very worried’ (Vohr et al 2001) and 14 per cent ‘considerably or very concerned’ (Weichbold & Welzl Mueller 2001). Lasting anxiety as the result of a false positive screen was reported in 14 per cent of parents in one study, although the anxiety was characterised as mild (Clemens et al 2000). Parental anxiety in mothers of screen positive babies referred for diagnostic testing was higher (21%) (Weichbold & Welzl Mueller 2001).
There was no evidence available regarding the psychological effects of false reassurance.

Universal neonatal hearing screening 45
Summary
The data available on the safety of universal neonatal hearing screening were limited and of poor to average quality. The main outcome reported was parental anxiety concerning: (1) the screen;
(2) a false positive result – a large consideration given the high false alarm rate; and
(3) a screen positive result.
Levels of moderate to severe anxiety were predominantly low in all three groups. There were no clinically significant differences in anxiety between parents of screen positive and screen negative babies, or between parents of screen positive and unscreened babies (level III-2 interventional evidence). No clinically significant differences were found between levels of anxiety or worry about their baby’s hearing when the state of mothers of infants screened by UNHS were compared against mothers of infants ≥ 6 months screened by a behavioural test. More satisfaction was expressed after the UNHS than the distraction test.
It has been suggested that screen status or anxiety may have an impact on the parental relationship with the child, but in the one controlled study (level III-2 interventional evidence) that reported on parental attitudes to the child, no differences were ascertained. A positive screen was associated with statistically poorer quality of early interactions, but the clinical importance of this finding is unknown (level III-2 interventional evidence). The available studies did not report on the psychological effects of false reassurance nor the psychosocial impact of a true-positive diagnosis, nor mention physical harms occasioned during the screening process.

Universal neonatal hearing screening 46
Table 9 Safety of universal neonatal hearing screening (comparative studies)
Study Level of evidence
Study qualitya
Screen setting
Population Outcomes Critical appraisalb
Mean ± SD in UNHS group
Mean ± SD in control group
Mean difference [95%CI]
Statistic, df, p value
Controlled studies comparing neonatal screening vs behavioural screening or no screening Parental anxiety –
Anxiety state Scale: 20 (low) –
80 (high)
Clin I = unable to be determined R = 3/5
3 weeks 36.9 ± 11.9 6 months 30.4 ± 8.2
3 weeks 33.2 ± 10.1 6 months 35.4 ± 12.8
3 weeks 3.7 6 months -5.0
within normal range so further comparisons not performed
(Crockett et al 2005)
III-2 Cohort study
QS = 3.5/6 Response rate = 48% for HDVT, 48-49% for neonatal hearing screen Recall bias possiblee
6 maternity hospitals, health visitor clinics and general practice surgeries England
48 mothers of infants who underwent health visitor distraction test (21 were positive, 27 were negative) 42 mothers of neonates who received UNHS (16 were positive, 26 were negative) UNHS versus HVDT in screen positive infants
Worry about baby’s hearing
Scale: 0 (not at all worried) – 7
(extremely worried) (unvalidated)
Clin I = unable to be determined R = 5/5
3 weeks 2.6 ± 2.1 6 months 1.6 ± 1.2
3 weeks 3.3 ± 2.0 6 months 2.1 ± 1.6
3 weeks -0.7 6 months -0.5
p>0.05
Parental anxiety (1st strategy)
Clin I = unable to be determined R = 3/5
N/A N/A N/A t = 0.39, df = 43 p > 0.05
Parental anxiety (2nd strategy)
Clin I = unable to be determined R = 3/5
N/A N/A N/A t = 0.69, df = 25 p > 0.05
Post-partum depression (1st strategy)
Clin I = unable to be determined R = 3/5
N/A N/A N/A t = 0.25, df = 43 p > 0.05
Post-partum depression (2nd strategy)
Clin I = unable to be determined R = 3/5
N/A N/A N/A t = 0.78, df = 25 p > 0.05
Quality of early interactions (1st strategy)
Clin I = unable to be determined R = 5/5
N/A N/A N/A t = 0.03, df = 43 p > 0.05
(Kolski et al 2007)
III-2 Cohort study
QS = 1.5/6 Response rate = not stated No recall biasc
Maternity hospital, University Hospital of Picardy Amiens, France
115 mothers of well babies who were screened, 58 by 1st strategy (at birth), 57 by 2nd strategy (2 months) 28 mothers of unscreened babies Screen negative versus unscreened
Quality of early interactions (2nd strategy)
Clin I = unable to be determined R = 5/5
N/A N/A N/A t = 0.95, df = 25 p > 0.05

Universal neonatal hearing screening 47
Study Level of evidence
Study qualitya
Screen setting
Population Outcomes Critical appraisalb
Mean ± SD in UNHS group
Mean ± SD in control group
Mean difference [95%CI]
Statistic, df, p value
Parental anxiety Anxiety state
Clin I = 4/4 R = 3/5
14.8±3.9 16.3±5.2 -1.6 [-3.3, 0.1]
t = -1.8 df = 116 p = 0.07
(Watkin et al 1998)
III-2 Cohort
QS = 3.5/6 Response rate = 60% No recall biasd
Whipps Cross Hospital London, UK
57 mothers of re-screen babies versus 61 mothers of unscreened babies Anxiety trait Clin I = 4/4
R = 3/5
16.5±4.5 17.5±4.9 -1.0 [-2.7, 0.7]
t = -1.1 df = 116 p = 0.25
Controlled studies comparing screen positive with screen negative Parental anxiety after HVDT –
Anxiety state Scale: 20 (low) –
80 (high)
Clin I = unable to be determined R = 3/5
3 weeks post test 33.2 ± 10.1 6 months post test 35.4 ± 12.8
3 weeks post test 29.0 ± 11.1 6 months post test 32.8 ± 12.4
3 weeks post test 4.2 6 months post test 2.6
means within normal range, so not compared further
Parental anxiety after UNHS –
Anxiety state Scale: 20 (low) –
80 (high)
Clin I = unable to be determined R = 3/5
3 weeks post test 36.9 ± 11.9 6 months post test 30.4 ± 8.2
3 weeks post test 31.8 ± 11.1 6 months post test 32.6 ± 8.9
3 weeks post test 5.1 6 months post test -2.2
means within normal range, so not compared further
(Crockett et al 2005)
III-2 Cohort study
QS = 3.5/6 Response rate = 48% for HDVT, 48-49% for neonatal hearing screen Recall bias possiblee
6 maternity hospitals, health visitor clinics and general practice surgeries England
48 mothers of infants who underwent health visitor distraction test (21 were positive, 27 were negative) 42 mothers of neonates who received hearing screening (16 were positive, 26 were negative) Screen positive versus screen negative
Worry about baby’s hearing after HVDT
Scale: 0 (not at all worried) – 7
(extremely worried) (unvalidated)
Clin I = unable to be determined R = 5/5
3 weeks post test 3.3 ± 2.0 6 months post test 2.1 ± 1.6
3 weeks post test 1.1 ± 0.3 6 months post test 1.1 ± 0.3
3 weeks post test 2.2 6 months post test 1.0
3 weeks post test p < 0.01 6 months post test p < 0.05

Universal neonatal hearing screening 48
Study Level of evidence
Study qualitya
Screen setting
Population Outcomes Critical appraisalb
Mean ± SD in UNHS group
Mean ± SD in control group
Mean difference [95%CI]
Statistic, df, p value
Worry about baby’s hearing after UNHS
Scale: 0 (not at all worried) – 7
(extremely worried) (unvalidated)
Clin I = unable to be determined R = 5/5
3 weeks post test 2.6 ± 2.1 6 months post test 1.6 ± 1.2
3 weeks post test 1.1 ± 0.3 6 months post test 1.1 ± 0.3
3 weeks post test 1.5 6 months post test 0.5
3 weeks post test p < 0.01 6 months post test p = 0.10
Parental anxiety– Anxiety state
Scale: 20 (low) – 80 (high)
Clin I = unable to be determined R = 3/5
Group 2: 32.7 ± 12.1 Group 3: 34.0 ± 9.5 Group 4: 35.7 ± 12.8
Group 1: 32.0 ± 11.1
N/A F(3,327) = 1.5 p = 0.22
(Crockett et al 2006)
Level III-2 Cohort study
QS = 4/6 Response rate = 53% Possible recall biasf
Hospitals participating in UNHS pilot program England
344 mothers of infants were screened Group 1: clear responses in both ears from 1st or 2nd stage OAE Group 2: not clear responses in one or both ears at 1st or 2nd stage OAE but clear on AABR Group 3: not clear responses in one ear on AABR and referred for possible unilateral hearing loss Group 4: not clear responses in either ear on AABR and referred for possible bilateral hearing loss Trend analysis of between groups
Worry about baby’s hearing
Scale: 0 (not at all worried) – 7
(extremely worried) (unvalidated)
Clin I = unable to be determined R = 5/5
Group 2: 1.4 ± 1.0 Group 3: 2.7 ± 1.9 Group 4: 3.1 ± 2.2
Group 1: 1.3 ± 1.0
N/A F(3, 337)= 26.6 p < 0.01
(Kennedy 1999) (Kennedy 1999)
III-2 Nested case-
QS = 2.5/5 Response rate = 75% Possible
4 maternity hospitals Wessex,
Mothers of 150 low-risk babies 75 screen positive
Negative attitude to baby (validated) Scale: 0 (low) – 21 (high)
Clin I = 4/4 R = 1/5
4±3 4±3 0 [-1.0, 1.0]
t = 0 df = 148 p = 1.00

Universal neonatal hearing screening 49
Study Level of evidence
Study qualitya
Screen setting
Population Outcomes Critical appraisalb
Mean ± SD in UNHS group
Mean ± SD in control group
Mean difference [95%CI]
Statistic, df, p value
control recall biasg UK versus 75 screen negative
Concern for baby Scale: 0 (low) – 8 (high)
Clin I =3/4 R = 5/5
2±3 3±3 -1 [-2.0, 0.0]
t = -2.0 df = 148 p = 0.04
Parental anxiety Clin I = unable to be determined R = 3/5
N/A N/A N/A F(3,139) = 11.3 p < 0.01
Post-partum depression
Clin I = unable to be determined R = 3/5
N/A N/A N/A F(3,139) = 11.9 p < 0.01
(Kolski et al 2007)
III-2 Cohort study
QS = 1.5/6 Response rate = not stated No recall biasc
Maternity hospital, University Hospital of Picardy Amiens, France
115 mothers of well babies who were screened, 58 by 1st strategy (at birth), 57 by 2nd strategy (2 months) Screen positive versus Screen negative
Quality of early interactions
Clin I = unable to be determined R = 5/5
N/A N/A N/A F(3,139) = 6.8 p < 0.01
a This includes a quality score (QS) derived from the NHMRC (2000)) checklist (see Appendix E) with a high score indicating good quality; b determination of statistical precision (SP), rank scores for the clinical importance (Clin I) of the benefit/harm (with 1 ranked as highly clinically important and 4 ranked as clinically unimportant), and rank scores for the relevance (R) of the evidence (with 1 ranked as a highly relevant outcome and 5 as an unproven surrogate outcome); c interviews conducted after first stage screen, and prior to second stage; d Parent Stress Index administered by telephone 1 month after discharge of screen negatives and just prior to retest of screen positives; e Questionnaires sent 3 weeks and 6 months after completion of screening; f questionnaire completed 4 weeks after completion of screening; g questionnaire administered 2-12 months after screening. HVDT= Health Visitor Distraction Test; UNHS=universal neonatal hearing screening, N/A=not available.

Universal neonatal hearing screening 50
Table 10 Safety of universal neonatal hearing screening (noncomparative studies)
Study Level of evidence
Study quality Screen setting Population Outcomes Parents of screened babies (%)
Parents of screen positives (%)
Parental anxiety – ‘worried’ 80.0 (Clemens et al 2000)
Cross-sectional survey
Response rate = 64% Possible recall biasa
Women’s Hospital, Greensboro North Carolina, USA
49 parents of 76 well babies with normal hearing who screened positive Lasting anxiety 14.0c
(Hergils & Hergils 2000)
Cross-sectional survey
Response rate = 95% Possible recall biasb
University Hospital of Linköping Linköping, Sweden
Parents of 83 well babies who were screened
Parental anxiety 7.0d
Parental anxiety about screening program – ‘a little concern’
3.4
Parental anxiety prior about screening program – ‘moderate concern’
0.4
Parental anxiety about positive result– ‘a little concern’
57.1
(Tatli et al 2007)
Cross-sectional survey
Response rate = 78% Possible recall biase
Dokuz Eylul University Hospital, Izmir Turkey
Parents of 711 well and at-risk babies
Parental anxiety about positive result – ‘moderate or greater concern’
7.8
(Vohr et al 2001)
Cross-sectional survey
Response rate = 85% No recall biasf
Women & Infants Hospital Rhode Island, USA
307 mothers of initial screen babies 40 mothers of rescreen babies
Parental anxiety – ‘worried / very worried’
1997 screen: 3.8 1999 screen: 4.0 1997 rescreen: 33.0 1999 rescreen: 17.0
(Weichbold & Welzl Mueller 2001)
Cross-sectional survey
Response rate = 84% No recall bias
University Hospital Innsbruck, Austria
85 mothers of well babies with normal hearing who screened positive 43 mothers of screen positives referred for diagnostic testing
Parental anxiety – ‘considerably / very concerned’
Screen positives: 21.0 False alarms: 14.0
a survey administered at mean of 4.9 months after screening [range: 2–13 months]; b questionnaire administered 5–6 months after screening; c predominantly ‘mild’ anxiety, unclear how long after the screening this measure of anxiety was taken; d most were parents of children that needed to be retested; e Unclear when mothers were interviewed; f Iinterviews conducted after first stage screen, and prior to second stage

Universal neonatal hearing screening 51
How accurate are the screening tests?
Test accuracy is crucial to the successful implementation of any screening program. Expert opinion suggests that there are four factors that can be sources of error when conducting hearing screening tests – the infant, the screener, the equipment and the environment. Invalid test results can occur when:
(1) The infant:
• is not asleep or settled, so internal noise and muscle movement affect the test;
• is not positioned optimally such that the ear canal is blocked, or testing is impeded by the position of the head, pillow or mother’s arm; or
• is not swaddled or wrapped and moves during the test, causing the insert probe or muffins/couplers to move.
(2) The screener:
• is unfamiliar with the test equipment and inexperienced at determining whether the test result is valid;
• is inexperienced at handling infants;
• positions the insert probe or muffins/couplers inadequately or places the electrodes poorly (creating impedance problems); or
• allows insufficient time for testing.
(3) The equipment:
• malfunctions;
• is calibrated incorrectly; or
• has an occluded probe tip.
(4) The environment:
• has too much background noise; or
• causes electrical interference (eg monitors affect both automated auditory brainstem response (AABR) and otoacoustic emissions (OAE) tests).
The ‘Guidelines for using screening devices’ that were developed as part of the Western Australian universal neonatal hearing screening program (Bailey 2003) are reproduced in Appendix H.

52 Universal neonatal hearing screening
In order to evaluate the diagnostic accuracy of the tests routinely used to screen for hearing impairment in neonates and infants in an evidence-based manner, criteria for selecting studies that assessed diagnostic accuracy were delineated (Box 5).
Box 5 Study selection criteria for diagnostic accuracy
Research question What is the diagnostic accuracy of the tests for permanent childhood hearing impairment when conducted on the neonate or infant? Selection criteria Inclusion criteria Population Children ≤6 years of agea who have not experienced particular diseases or traumas associated
with hearing impairment between the neonatal testsb for permanent childhood hearing impairment (PCHI) and the later tests for hearing loss.
Intervention The otoacoustic emissions (TEOAE or DPOAE) test or the automated auditory brainstem response (AABR) test for PCHI (≥35 dB) performed at ≤6 months of age.
Reference standard(s) Medical or behavioural assessment (including pure tone audiogram), tympanometry, steady state evoked potential (SSEP) testing and/or conventional or diagnostic auditory brainstem response (ABR) testing performed at ≤6 years of age.
Outcomes Sensitivity and specificity (and therefore rates of false positives and negatives), positive and negative predictive values (and therefore false alarm and reassurance rates).
Study design Cross-sectional studies where allc neonates and infants are cross-classified on the test and reference standard (including longitudinal studies). Case-control diagnostic studies were only acceptable if cross-sectional studies were not available.
Search period The OAE and AABR tests have only been in common usage since 1980. Studies published before 1980 were not included.
Language Studies in languages other than English were only translated and included if they represented a higher level of evidence than that available in the English language evidence-base.
a This age range was selected to accommodate the reference standard which may often be performed at pre-school or school age. Studies were excluded if children were selected solely on the basis of risk factors or indications – so as to avoid spectrum bias (Brenner & Gefeller 1997); b to mitigate possible difficulties with confounding caused by the delay between neonatal and later tests ie progressive deterioration, disease or trauma that would worsen hearing for the later (reference standard) tests; c to prevent ‘work-up or verification bias.
Studies were excluded that selected children for hearing screening solely on the basis of risk factors or indications. These studies were excluded partly because of the attendant bias in estimating the efficacy of a test on a sample that does not contain the whole spectrum of ill and healthy babies. They were also excluded because children at risk of permanent childhood hearing impairment (PCHI) are often tested diagnostically in the first instance, rather than screened.
As it was a requirement that all neonates and infants should be cross-classified on the test and reference standard, and that only an appropriate spectrum of infants should be included, the only levels of evidence (as defined in Table 5) available for inclusion were levels I, II, III-1, III-2, and III-3.
There were many studies available that compared the screening tests to an acceptable reference standard in high-risk populations of infants. There were also several studies that compared the two screening tests to each other, rather than to an established reference standard. There were very few studies, however, that assessed the accuracy of the neonatal hearing screening tools in predominantly healthy infants – the target population in a universal screening situation – and compared them to an established reference standard (eg diagnostic auditory brainstem response testing).

Universal neonatal hearing screening 53
The ideal method for assessing the diagnostic accuracy of universal hearing screening tests would be to test a random or consecutive sample of neonates and infants under 6 months of age with either the otoacoustic emissions (OAE) test or automated auditory brainstem response (AABR) test, and then immediately test them on a reference standard such as conventional or diagnostic ABR. The diagnostic accuracy of the tests can then be determined using the classic 2 x 2 table, whereby the results of the screening test are cross-classified against the results of the reference standard (Armitage et al 2002; Deeks 2001) and Bayes’ Theorem is applied:
Hearing status (based on reference standard) PCHI Normal
Test + True positive False positive Total positive Screening test Test - False negative True negative Total negative
Total with PCHI Total without PCHI
The sensitivity of a hearing screening test is therefore calculated as the proportion of infants with permanent childhood hearing impairment (PCHI) who have positive screening test results:
Sensitivity = True positive / Total with PCHI
The specificity of a hearing screening test is calculated as the proportion of infants without PCHI who have normal screening test results:
Specificity = True negative / Total without PCHI
The false positive rate of a hearing screening test is calculated as the proportion of infants without PCHI who have positive screening test results:
False positive rate = False positive / Total without PCHI
Similarly the false negative rate of a hearing screening test is calculated as the proportion of infants with PCHI who have negative screening results:
False negative rate = False negative / Total with PCHI
The false alarm rate of a hearing screening test is calculated as the proportion of infants with positive screening results who do not have PCHI:
False alarm rate = False positive / Total test positive
The false reassurance rate of a hearing screening test is calculated as the proportion of infants with negative screening results who have PCHI:
False reassurance rate = False negative / Total test negative
The positive predictive value of the test(s) in an average screening population (well and ‘at-risk’ babies) estimates the likelihood that an infant has PCHI on the basis of a positive screening test result. The positive predictive value of a test is sensitive to the prevalence of the condition in the population being tested (Deeks 2001). Therefore, if the

54 Universal neonatal hearing screening
prevalence of the condition is low, the positive predictive value of the test will be poor. The formula for calculating the positive predictive value (PPV) is:
PPV = sensitivity x prevalence of PCHI (sensitivity x prevalence of PCHI) + (1 – specificity x prevalence of not having PCHI)
The prevalence of PCHI used in these calculations is the median estimated prevalence rate determined in the previous section, that is 1.25/1,000.
It is particularly important that the cross-classification on the screening and reference tests occurs with as little time-lag as possible. This is due to the nature of PCHI. Hearing impairment may be congenital (which is the target of a neonatal screening program) or an acquired or progressive condition. To accurately assess the diagnostic capabilities of a neonatal screening test, therefore, the sensitivity and specificity of the test should not be influenced by conditions that affect hearing in the postnatal period. It was fortunate that the studies assessed as suitable for inclusion in this review conducted the cross-classification of infants on the screening test and reference standard at approximately the same time.
Five studies met the inclusion criteria (Table 11). Profiles of these studies are provided in Appendix F. Three of the studies compared a transient otoacoustic emissions (TEOAE) test with a conventional auditory brainstem response (ABR) test (Jacobson & Jacobson 1994; McNellis & Klein 1997; Smyth et al 1999). One study compared the accuracy of TEOAE to tympanometry (Ho et al 2002) and one study compared the automated auditory brainstem response (AABR) screening test with a conventional ABR test (Schauseil-Zipf & Von Wedel 1988). The latter study was originally in German and has been translated into English for this assessment. There were no studies available that compared the screening distortion product otoacoustic emissions (DPOAE) test with a relevant reference standard.
The ability of TEOAE testing – in a one-stage screen – to accurately identify permanent childhood hearing impairment (PCHI) in neonates and infants varied widely in the included studies, with sensitivity ranging from 50 to 100 per cent when compared to conventional ABR testing. This variation appears to be largely a result of the conditions under which the testing was conducted. Both studies that utilised a ‘quiet’ – although not sound-proofed – environment for testing elicited sensitivity results of 100 per cent, including the better quality study produced by Smyth and colleagues (1999). Jacobson and Jacobson (1994), however, determined 50 per cent sensitivity for TEOAE to detect PCHI under ‘real world’ ambient noise conditions (ie within the nursery). In this study failures included those children who were tested but could not produce an OAE in the allocated screening time (45 minutes), mainly due to excessive noise levels. The comparator was a combination of AABR and ABR testing.
Given the likely low sensitivity of TEOAE testing under ‘real world’ noise conditions, and the concomitant large proportion of infants (50% identified by Jacobson and Jacobson, 1994) with PCHI who may not be identified (false negatives) under these conditions, TEOAE testing should only occur in environments that are quiet or possibly sound-proofed. It is critical that false negatives are avoided as this false reassurance may have considerable impact on when the children are re-tested, as well as the effectiveness of the eventual rehabilitation.

Universal neonatal hearing screening 55
The specificity of TEOAE is also variable, although the better quality study by Smyth and colleagues (1999) indicates that it can accurately determine a lack of hearing impairment in normal infants under quiet conditions in 92 per cent of cases. The number of false positive results was 3 out of 36 (8.3%) infants (Smyth et al 1999). In the study performed under normal noise conditions the false positive rate was 48 per cent (Jacobson & Jacobson 1994). The positive predictive value of an initial TEOAE screening test under the best (quiet) conditions is very low (1.5%) – meaning that a failure on an initial TEOAE test would accurately predict PCHI in only one to two infants out of 100 identified by the test with the condition. This is probably a consequence of the frequency of transient losses in newborns (ear occlusion), as well as the low prevalence of PCHI in the general population.
In terms of identifying conductive hearing loss, TEOAE testing was found to have 100 per cent sensitivity and specificity, as compared to tympanometry, in one study of infants who had no cerumen occlusion of the ear (Ho et al 2002).

56 Universal neonatal hearing screening
Table 11 Diagnostic accuracy of hearing screening tests
Study Diagnostic level of evidence
Quality scorea
Population Setting Sensitivity (%) [95%CI]
Specificity (%) [95%CI]
PPV (%)b
TEOAE vs conventional ABR (Jacobson & Jacobson 1994)
III-2c d 10/14 n = 119 babies at 33–41 weeks of age (238 ears) 56% at risk 44% well
Norfolk, Virginia, USA
50.0 [15.7,84.3]
52.3 [45.4,59.1]
0.13
(McNellis & Klein 1997)
III-2c 10/14 n = 50 healthy, low-risk full-term babies (100 ears)
Charleston, South Carolina, USA
100.0 [15.8,100.0]
62.2 [51.9,71.8]
0.32
(Smyth et al 1999)
III-1 11/14 n = 37 normal, full-term well babies (74 ears) without risk factors
Brisbane, Queensland Australia
100.0 [2.5,100.0]
91.7 [77.5,98.3]
1.49
TEOAE vs tympanometry
(Ho et al 2002)
III-2 10/14 n = 33 normal and at-risk babies <6 months of age, excluding those with cerumen occlusion of the ear (total of 29 ears)
Community screening clinics (29) in Minnesota, USA
100.0 [54.1,100.0]
100.0 [85.2,100.0]
100.00
AABR vs ABR
(Schauseil-Zipf & Von Wedel 1988)
III-2c 9/14
n = 50 babies (100 ears) 50% at risk 50% well
Women and children’s clinic, Cologne, Germany
80.0 [44.4,97.5]
95.6 [89.0,98.8]
2.22
PPV = positive predictive value; TEOAE = transient evoked otoacoustic emissions test; AABR = automated auditory brainstem response test; ABR = conventional auditory brainstem response test. a Quadas checklist appraising quality of studies of diagnostic accuracy, see Appendix E; b calculated using median prevalence estimate of PCHI as 1.25/1,000; c assumption that selection was non-consecutive as ‘consecutive’ not mentioned in text; d reference standard included combination of conventional ABR and AABR.

Universal neonatal hearing screening 57
The ability of the automated auditory brainstem response (AABR) test – in a one-stage screen – to accurately identify PCHI in neonates and infants was compared to conventional ABR testing in the one average quality study available that cross-classified infants on the two tests (Schauseil-Zipf & Von Wedel 1988). The specificity (or the likelihood of detecting normal hearing in a normal hearing individual) of AABR was particularly good, given that its primary use is as a screening tool on a population of predominantly healthy infants. However, the trade-off between sensitivity and specificity means that the test has good, although not excellent, sensitivity at detecting PCHI and thus some false negatives may result (20% in this study). As mentioned earlier, it is critical that false negatives are avoided as they may have a significant impact on when children are re-tested, as well as on eventual rehabilitation. The AABR equipment used in this study was the earliest version available on the market and it is possible that newer models have improved sensitivity. Expert opinion indicates that later models of the AABR may, in fact, have improved diagnostic accuracy. Unfortunately, empirical evidence on the accuracy of the newer AABR models at detecting hearing impairment in predominantly healthy neonates is not yet available. In this study on the earliest AABR test, the positive predictive value is still very low (2.2%), although marginally better than TEOAE testing conducted under quiet conditions.

58 Universal neonatal hearing screening
Summary
Average quality, diagnostic level III-2 evidence suggests that the accuracy of transient evoked otoacoustic emissions (TEOAE) testing appears to depend on the level of local ambient noise (and therefore ear-probe fit and the testing environment), as well as the condition of infant ears (eg whether occluded by vernix or wax) at testing (Ho et al 2002; Jacobson & Jacobson 1994; McNellis & Klein 1997). If these factors are addressed adequately, diagnostic accuracy of the test is very good (up to 100% sensitivity), although even under the best conditions the rate of false positives can still be quite high (8%). The positive predictive value of an initial TEOAE test is very low, with 1.5 per cent of children who screen positive for hearing impairment receiving diagnostic confirmation. This is probably a consequence of the frequency of transient losses in newborns (ear occlusion), as well as the low prevalence of permanent childhood hearing impairment (PCHI) in the general population.
Based on one study, the specificity of the early model automated auditory brainstem response (AABR) test is particularly good, given that its primary use is as a screening tool on a population of healthy infants. However, the trade-off between sensitivity and specificity means that the test has good, although not excellent, sensitivity at detecting PCHI and thus some false negatives may result. The positive predictive value of an AABR test is also very low (2.2%), although marginally better than a TEOAE test conducted under quiet conditions. Evidence-based assessment of more recent versions of the AABR test is required.
The number of false positives associated with either test could be reduced with the introduction of a second-stage or third-stage screen of initial failures prior to diagnostic testing. This may, however, result in unnecessary caregiver anxiety and added costs and delays in rehabilitation. False negatives are not likely to be picked up until the child is older and this false reassurance may lengthen the time until diagnostic assessment and thus the child’s rehabilitation.

Universal neonatal hearing screening 59
Is it effective to screen all neonates for hearing impairment?
An assessment of the effectiveness of a screening program is usually modelled as a systematic review of intervention studies. That is, studies are sought that directly compare the impact of screening versus not screening in the general population. The effectiveness of the screening program (as a whole) at preventing, or allowing early treatment of, potential adverse outcomes associated with a condition is then assessed.
Box 6 delineates the criteria for including studies to assess the effectiveness of a universal neonatal hearing screening (UNHS) program.
Box 6 Study selection criteria for assessing effectiveness
Research questions 1. Does universal neonatal hearing screening, and the finding of a positive and/or negative test, affect the clinical management or treatment options available to permanently hearing-impaired infants? 2. Does universal neonatal hearing screening, and therefore possible alterations in clinical management, have an impact on the adverse outcomes associated with permanent childhood hearing impairment? Selection criteria Inclusion criteria Population Neonates and infants ≤6 months of age. Intervention Universal neonatal hearing screening using either the otoacoustic emissions (OAE) or automated
auditory brainstem response (AABR) testing methodsa. Comparator(s) Not universal neonatal hearing screening. Outcomes Primary – screening yield, rate and quality of language acquisition, behaviour, family functioning,
communication ability / social functioning, educational achievement, employment status, socioeconomic status, quality of life. Secondary – age of referral for diagnostic testing, age of permanent childhood hearing impairment diagnosis, age receiving therapeutic intervention.
Study design Randomised or non-randomised controlled trials or cohort studies or systematic reviews of these study designs. Case-control studies were acceptable only for the long-term (primary) outcomes. Uncontrolled studies that provided, at minimum, screening yield data were included to provide supplementary descriptive data on screening parameters.
Search period The OAE and AABR tests have only been in common usage since 1980. Studies published before 1980 were not included.
Language Studies in languages other than English were only translated and included if they represented a higher level of evidence than that available in the English language evidence-base.
a excluding studies solely concerned with targeted screening, ie children tested on the basis of existing risk factors or indications for permanent childhood hearing impairment (PCHI), such as i) admission to a neonatal intensive care unit; (ii) prolonged usage of aminoglycosides; (iii) family history of hearing impairment; (iv) intrauterine or perinatal infection (either suspected or confirmed); (v) birthweight less than 1.5 kg; (vi) craniofacial deformity: (vii) birth asphyxia; (viii) chromosomal abnormality, including Down syndrome; or (ix) exchange transfusion or intrauterine transfusion

60 Universal neonatal hearing screening
Research question 1:
Does universal neonatal hearing screening, and the finding of a positive and/or negative test, affect the clinical management or treatment options available to permanently hearing-impaired infants?
In order to determine whether the clinical management of permanent childhood hearing impairment (PCHI) is altered by the introduction of universal neonatal hearing screening (UNHS), secondary or surrogate outcome data were extracted from the controlled studies. These included age at referral, age at PCHI diagnosis and age at treatment or management.
Given the paucity of controlled studies available, information from uncontrolled studies of screening programs – full text only – was collated to provide descriptive, supplementary data. Inclusion of these descriptive studies was limited to only those that provided data on screening yields. Additional information was also extracted on failure rates (referrals), false alarm rates (incorrectly testing positive for hearing impairment), coverage and loss to follow-up for different screening protocols and populations. These studies could not, however, assist with the determination of the effectiveness of UNHS compared to targeted (‘at-risk’ population) screening or not screening at all.
Altogether, five controlled studies (Table 12) assessed the effectiveness of a UNHS program in terms of its impact on clinical management of hearing-impaired infants (Kennedy et al 1998; Kennedy et al 2005; Kennedy et al 2006; Nekahm et al 2001a; Neumann et al 2006; Weichbold et al 2006; Yoshinaga-Itano et al 2001). The study conducted by Kennedy and colleagues was a quasi-randomised (alternate allocation) controlled trial comparing periods with and without UNHS at four different hospitals over 3 years (Kennedy et al 1998). This trial was conducted by the Wessex Universal Neonatal Hearing Screening Trial Group and was of average quality (QS = 3/6) overall, and there is a possibility that bias may have influenced the results through possible contamination from one screening period to another within each hospital. This is likely to dilute any effect of screening, however, rather than over-estimate its effect. The study was under-powered for some of the outcomes, so it is possible that clinically relevant differences have been missed or are statistically imprecise. Bias may have had an impact on the results through the lack of proper randomisation and concealment of allocation to the screening intervention. Statistical analysis also did not take into account the clustering of the data.
Two subsequent studies from the same group reported results on 8 years of follow-up of the original birth cohort of babies in the Wessex controlled trial (Kennedy et al 2005; Kennedy et al 2006). High quality was achieved for the latter study based on the critical appraisal checklists (see Appendix E). The most recent of these studies, a prospective cohort study, also included a large birth cohort from the Greater London region (Kennedy et al 2006)
Kennedy et al (2005) reported an 8 year follow-up of results in a research letter which was primarily focused on publishing an estimate of the effect of UNHS on the proportion of all true cases of PCHI ≥40dB HL that had early referral. Identifying an accurate estimate requires long-term follow-up so that false negatives and true

Universal neonatal hearing screening 61
progressive PCHI cases can be correctly ascertained, thus this was not discussed in the original published trial report.
The second follow-up study (Kennedy et al 2006) consisted of neonates from eight districts: four districts from the Wessex controlled trial and four from the Greater London group. Nonetheless, outcome measurement of identification and diagnosis was comparable across the groups. Primarily of interest in this long-term study was communication ability and language acquisition in the children. Researchers blinded to the hearing history of the children assessed the children by means of four different measures: Test for Reception Grammar, the British Picture Vocabulary Scale (receptive language), the Renfrew Bus Story Test (expressive language) and Raven’s Progressive Matrices Test (nonverbal abilities). Completeness of ascertainment was reported to be over 95 per cent in both the Wessex and London groups. It was also apparent that participants and non participants were similar with respect to age, sex and severity of hearing loss.
The remaining four studies analysed, retrospectively, cohorts of children with hearing impairment, and assessed whether UNHS affected the time of diagnosis of PCHI and the age at which management was initiated. The study of Tyrolean children born in time periods with and without UNHS was of good quality (QS = 5.5/6) (Nekahm et al 2001a). The results are likely to have been affected by bias, due to the lack of randomisation and allocation concealment, as well as by confounding as the cohorts of children were recruited over different time periods. It is possible, therefore, that differences in time of diagnosis are attributable to some factor other than screening (eg heightened parental or clinician awareness concerning certain risk factors). This group of researchers also conducted an average quality retrospective follow-up study of children born since 1990 and registered at an Austrian Ear, Nose and Throat (ENT) department or institution for the hearing impaired (Weichbold et al 2006). These included 15 institutions out of a total of 35 Austrian institutions thus expanding the population captured in their earlier study which only included Tyrolean children born between 1980 and 1999.
The study of German children, born in hospitals with and without UNHS was of good quality (QS=5/6). This study compared two groups: one receiving Universal Neonatal Hearing Screening and the other group receiving opportunistic testing outside of a screening program, who originated from different populations in Germany (Neumann et al 2006). The 17, 349 screened neonates came from the state of Hessen only, while the unscreened neonates arose from a database of the Hessian and Thuringian population. The analysis did not control for demographic and clinical differences in the two groups thus the two groups were not entirely comparable.
The fourth retrospective cohort study conducted by Yoshinaga-Itano et al (2000 & 2001) in the United States was also considered to be of good quality (QS = 5.5/6) (Yoshinaga Itano et al 2000; Yoshinaga-Itano et al 2001) and bias and confounding are likely to have had limited effect. Bias may have been introduced through unblinded assessment of some of the outcomes. Confounding was well controlled with the use of a matched-pairs design. Children were matched on age, severity of PCHI and cognitive ability – all factors that had been associated with the identification, diagnosis and management of PCHI in previous studies. This may, however, have limited the external validity of the study’s results. Other potential confounders such as gender, ethnicity, other disabilities, mode of

62 Universal neonatal hearing screening
communication and education level of the primary caregiver were not distributed differently between the screening and not-screening groups.
Table 12 provides a summary of data from the controlled studies on each of the following screening outcomes: coverage, absolute and incremental yield, age at referral, age at PCHI diagnosis and age at management or rehabilitation. This is supplemented in Table 13, Table 14, and Table 15 by 56 uncontrolled, descriptive studies. These studies provide qualitative information on screen protocol (1-stage, 2-stage, 3-stage), coverage, failure rates (referrals), loss to follow-up (LTFU), false alarms and yield for the universal screening arm alone. Several studies are mentioned repeatedly in the tables as they have undertaken different screening protocols in different settings therefore their results have been put in the appropriate sections of the table. All information presented in these tables has been calculated according to intention-to-screen principles – data on LTFU, however, are also presented so that compliance with the screening protocol can be determined.

Universal neonatal hearing screening 63
Table 12 Effectiveness of universal neonatal hearing screening for secondary outcomes (controlled studies)
Study Level of evidence
Study quality a
Setting Population Screen fail criterion
Outcomes Critical appraisalb
UNHS rate (%)
Control rate (%)
Number needed to screen (NNS)/ diagnose (NND)c
Relative risk [95% CI]
Adjusted odds ratiod
[95% CI]
2-stage: TEOAE–AABR – dx audiology
Coverage
83.1
Referrale <6 months
SP = ave. Clin I = 1/4 R = 2/5 Power = 77%
0.09 0.03 NNS 1,619 [955, 5297]
2.9 [1.4, 6.3]
19.0 [3.2, 111.0]
False alarm rate
1.5
False negative
Clin I =4/4 R =2/5
6.5 17.1f 0.4 [0.1, 1.7]
False reassurance rate
0.005
Yieldg SP = ave. Clin I = 2/4 R = 2/5 Power = 58%
0.09 0.04 NNS 1,970
[1063, 13459]
2.3 [1.1, 4.7]
(Kennedy et al 1998) (Kennedy et al 2005) (8 yr follow up)
III-1 QS = 3/6
4 hospitals in Wessex, UK
53,781 well and at-risk babies n = 25,609 born during UNHS periods n = 28,172 born during periods without UNHS Study duration: 3 years
Bilateral failure to produce emission spectrum of significant gain across 3 of 5 testing frequency bands AABR fail at ≥35 dB HL Control group received health visitor distraction test
Diagnosis <10 months
SP = NS Clin I = 4/4 R = 2/5 Power = 23%
0.06 0.04 NNS 3,706 [1546, 9337]
1.8 [0.8, 3.9]
5.0 [1.0, 23.0]

Universal neonatal hearing screening 64
Table 12 (cont.) Effectiveness of universal neonatal hearing screening for secondary outcomes (controlled studies)
Study (cont.)
Level of evidence
Study quality a
Setting Population Screen fail criterion
Outcomes Critical appraisalb
UNHS rate (%)
Control rate (%)
Number needed to screen (NNS)/ diagnose (NND)c
Relative risk [95% CI]
Adjusted odds ratiod
[95% CI]
Management <10 months
SP = NS Clin I = 2/4 R = 1/5 Power = 41%
0.06 0.02 NNS 2,965 [1458, 86207]
2.4 [1.0, 5.8]
8.0 [1.2, 51.0]
(Kennedy et al 2006)
III-2 QS=5/6 4 hospitals in Wessex, UK 4 hospitals in Greater London
68714 infants born with UNHS 88,019 infants born without UNHS 168 PCHI children identified overall 120 included (UNHS=61; Non-UNHS=59)
Wessex Subgroup: as above Greater London Subgroup Fail criteria not stated ABR fail ≥40 dB HL
Confirm-a-tion < 9 mths
Clin I = 1/4 R = 2/5
0.06 0.02 NNS 2,500 [1667, 5000]
3.3 [1.8, 5.8]

Universal neonatal hearing screening 65
Table 12 (cont) Effectiveness of universal neonatal hearing screening for secondary outcomes (controlled studies)
Study (cont.)
Level of evidence
Study quality a
Setting Population Screen fail criterion
Outcomes Critical appraisalb
UNHS rate (%)
Control rate (%)
Number needed to screen (NNS)/ diagnose (NND)c
Relative risk [95% CI]
Adjusted odds ratiod
[95% CI]
2-stage: TEOAE–TEOAE – dx audiology (Nekahm et al 2001a)
III-2 QS = 5.5/6 Tyrol, Austria
91 Tyrolean children with PCHI, born 1990–1999 UNHS = 1995–1999 Not UNHS = 1990–1994 Study duration: 10 years, retrospective
Not stated Diagnosis <6 months
SP = good Clin I = 1/4 R = 2/5 Power = 92%
50.0 9.8 NND 3 [2, 5]
5.1 [2.1, 12.4]
(Neumann et al 2006)
III-2 QS=5/6 46 maternity clinics and 3 NICU’s Hessen, Germany and Thuringia, Germany
17, 349 well and at-risk babies in 2005 UNHS group 98 Hessian and 355 German PCHI in non-UNHS group UNHS= 1995-2005 Not UNHS= 1990-2005
TEOAE ≥ 30dB AABR ≥ 35dB
Age at diagnosis
Mean 4.5 mths Median 3.1 mths
Hessen Mean 25.7 mths Median 17.8 mths Thuringia Median 52.0 mths Germany Mean 39.0 mths Median 33.0 mths
- - -

Universal neonatal hearing screening 66
Table 12 (cont) Effectiveness of universal neonatal hearing screening for secondary outcomes (controlled studies)
Study (cont.)
Level of evidence
Study quality a
Setting Population Screen fail criterion
Outcomes Critical appraisalb
UNHS rate (%)
Control rate (%)
Number needed to screen (NNS)/ diagnose (NND)c
Relative risk [95% CI]
Adjusted odds ratiod [95% CI]
Age at intervention
Mean 4.8 mths Median 3.5 mths
Mean 29.1 Median 21.0 mths
- - -
Age at confirmation 3 months (%) 6 months( %) 12 months (%)
Clin I =1/4 R = 2/5
Mean 9.7 mths 35 69 81
Mean 46 mths 2 6 12
NND 4 [3, 4] 2 [2, 2] 2 [2, 2]
17.5 [5.7, 55.7] 11.5 [6.2, 22.4] 6.8 [4.5, 10.7]
(Weichbold et al 2006)
III-2 QS=4.5/6 Innsbruck, Austria
321 children with PCHI, born 1990-2003
Not stated
Age at management 6 months (%) 12 months (%)
Clin I =1/4 R = 2/5
61 76
4 9
NND 2 [2, 3] 2 [2, 2]
15.3 [7.1, 34.7] 8.4 [5.0, 13.9]

Universal neonatal hearing screening 67
Table 12 (cont) Effectiveness of universal neonatal hearing screening for secondary outcomes (controlled studies)
Study (cont.)
Level of evidence
Study quality a
Setting Population Screen fail criterion
Outcomes Critical appraisalb
UNHS rate (%)
Control rate (%)
Number needed to screen (NNS)/ diagnose (NND)c
Relative risk [95% CI]
Adjusted odds ratiod [95% CI]
1-stage: AABR – dx audiology (Yoshinaga-Itano et al 2001)
III-2 QS = 5.5/6 Colorado, USA
25 matched pairs of children with bilateral PCHI born in hospitals with and without UNHS Study duration: 5 years, retrospective
Bilateral fail ≥35 dB
Diagnosis <6 months
SP = excellent Clin I = 1/4 R = 2/5 Power = 100%
84.0 8.0 NND 1 [1, 2]
10.5 [2.7, 40.1]
UNHS = universal neonatal hearing screening; TEOAE = transient otoacoustic emissions test; AABR = automated auditory brainstem response test; NICU=neonatal intensive care unit; dx = diagnostic; PCHI = permanent childhood hearing impairment; NS = not significant at p<0.05. a This is a quality score (QS) derived from NHMRC (2000) checklist (see Appendix E) with a high score indicating good quality; b determination of statistical precision (SP), rank scores for the clinical importance (Clin I) of the benefit/harm (with 1 ranked as highly clinically important and 4 ranked as clinically unimportant), and rank scores for the relevance (R) of the evidence (with 1 ranked as a highly relevant outcome and 5 as an unproven surrogate outcome); c NNS=number needed to screen-= number of infants who need to be screened in order to have one infant be referred/ diagnosed or managed earlier, NND= number needed to diagnose= number of infants with PCHI who would need to be screened, as opposed to not screened, in order to have one infant diagnosed with PCHI before the age of 6 months; d adjusted for severity of PCHI – logistic regression results reported by the author; e referral to an audiologist for diagnostic assessment; fpatients who were underwent distraction test not UNHS, g children confirmed with PCHI after diagnostic assessment – these data not complete until youngest children (18 months old) are approximately 5 years of age;

Universal neonatal hearing screening 68
Coverage
The largest quasi-randomised screening trial to date – the Wessex Controlled Trial – attempted to screen 25,609 infants using a two-stage screening protocol with program coverage of 83 per cent (Kennedy et al 1998). The largest uncontrolled screening program in Rhode Island, USA, screened 99 per cent of 53,121 infants using a different two-stage protocol (Vohr et al 1998). The latter program’s excellent coverage is likely to have been assisted by state legislation mandating universal neonatal hearing screening (UNHS). Bamford and colleagues (2005) also reported on the screened population of 23 areas of England, reaching 97.5 per cent coverage, however, while it is stated that there are about 120, 000 births per annum, the exact number of screened infants is unclear (Bamford et al 2005). Coverage does not appear to vary significantly according to either the size of the source population being screened or the screening protocol used. A large proportion of hearing screening programs that reported on coverage managed to screen over 90 per cent of infants in their catchment area.
The lowest coverage of 45.0 per cent was seen in a private rural hospital in Gauteng, South Africa. This study was conducted over a 4 year period, during which time the hearing screening service was subsidised for 22 months as part of the hospital birthing package. This resulted in a coverage of 75 per cent. The subsequent 26 month period, when the service was no longer subsidised, achieved coverage of only 20 per cent, giving an overall rate of 45 per cent. Nonetheless, there were several other studies (k=7) that also achieved coverage rates less than 80 per cent. Reasons for this included initial screens occurring between and one and two months after the baby was born. It is possible that there were accessibility issues and/or that resources available for these programs to ensure the ‘capture’ of infants at this age for outpatient or health clinic appointments for a stand-alone screen were limited. Additionally, the majority of these studies were located in rural areas or small clinics.
Referrals and false alarms
The highest level of evidence available (Kennedy et al 1998; Kennedy et al 2006) indicated that infants who receive universal neonatal hearing screening are nearly three times more likely [RR = 2.9, 95%CI 1.4, 6.3] to be referred for diagnostic testing within 6 months than infants who are not screened universally. When adjusted for the severity of hearing impairment, the odds of referral improve up to 19 times [OR = 19.0, 95%CI 3.2, 111.0]. In practical terms this means that 1,619 infants would need to be universally screened for hearing impairment, as compared to not screening, to ensure the referral for diagnostic testing of one infant under the age of 6 months (Table 12).
There was considerable variation (1.4–30.3%) in the referral rates from initial transient evoked otoacoustic emissions (TEOAE) screening in the uncontrolled studies Table 13, Table 14 and Table 15). No systematic differences could be ascertained according to the population screened (ie well babies or well and ‘at-risk’ babies) or to the time of screening. Bilateral fail screening criteria contributed to lower initial referral rates (1.1–12.8%), although some studies that referred according to unilateral fail criteria also managed low referral rates. Most of the variation in TEOAE referral rates can be attributed to the different definitions of a TEOAE fail (ie different emission response levels at different numbers and types of frequency bands, with different reproducibility thresholds), or were possibly a consequence of the different environmental conditions (ambient noise levels) under which the testing was conducted.

Universal neonatal hearing screening 69
There was considerably less variation (1.2-13.0%) in the referral rates from initial automated auditory brainstem response (AABR) screens. Rates did not vary substantially according to the population screened or to the screen fail criteria used Table 13, Table 14, and Table 15). AABR uses a standard referral threshold of >35 db HL, which may have contributed to the homogeneity of the results.
Diagnostic referrals in uncontrolled studies again varied widely as a consequence of TEOAE testing. After a one-stage TEOAE screen, nearly one-quarter (20.4%) of infants screened were referred for diagnostic testing (Table 13) (Hahn et al 1999). Ng (2004) used a 1-stage DPOAE and found 3.4 per cent of infants were referred for diagnostic testing. The two-stage TEOAE screening resulted in 2–46 per cent of first screen failures being referred for diagnostic testing (Table 12). The majority of these studies obtained less than a 34 per cent referral rate with one outlier to this, specifically the second strategy conducted by Kolski et al (2007) which found a referral rate of 46.2 per cent. This strategy was based on first screens taking place when the newborn was two months old and re-screens taking place at 3 months old. The authors believed that this did not have an impact on the referral rates obtained, however it is unclear why the results are disparate. Three-stage TEOAE screening resulted in 8 per cent of second screen failures receiving referrals for diagnostic testing (Table 15).
One-stage AABR screening resulted in consistently low referral rates (4.5–5.0%) for diagnostic testing (Table 13). After two-stage AABR screening, 14.6-59.2 per cent of initial screen failures were referred for diagnostic testing. The high referral rate reported in the study by Iwasaki et al. (2003) may be explained by the different population assessed, ie Japanese infants and also it was unclear how many were well babies or at-risk. After three-stage AABR screening one study reported nearly one-quarter (24.2%) of second screen failures being referred for diagnostic testing Table 15.
Studies using a combination of different screening tests reported the lowest consistent referral rates for one- and two-stage screen failures (0.6–7.7%) (Table 13, Table 14). A three-stage mixed screening protocol resulted in 16.5-45.5 per cent of screen failures being referred (Table 15).
As indicated by the diagnostic accuracy section of this report, TEOAE screening has a high false alarm rate. Incorrect (positive) initial screens were determined in 16–97 per cent of TEOAE failures. In general, false alarms were seen in approximately half of the infants receiving an initial TEOAE screen. These were infants who received unnecessary re-screening. Similarly, 0-93 per cent of those referred for diagnostic testing from a TEOAE screen were found to have normal hearing – including one study that reported no diagnostic false alarms (Owen et al 2001). Overall, the high TEOAE referral rate and the large proportion of false alarms meant that a considerable number of infants screened were incorrectly identified as having possible hearing impairment. With a TEOAE screen protocol, unnecessary re-screening (ie false alarm) occurred in 1–11.5 per cent of all infants screened, whilst unnecessary diagnostic testing occurred in 0–10 per cent.
False alarms caused through an AABR screening protocol, and requiring re-screening, occurred in 41–100 per cent of initial screen failures – although in only 0.7–7 per cent of the total infants screened. Unnecessary diagnostic testing occurred in 0–100 per cent of AABR screen failures, which equates to 0–5 per cent of the total population screened. In

Universal neonatal hearing screening 70
terms of the number of false alarms, AABR screen protocols performed better than TEOAE screen protocols.

Universal neonatal hearing screening 71
Table 13 Descriptive (uncontrolled) studies of 1-stage universal neonatal hearing screening
Stage 1 Study Setting Population Study duration
Faila criterion
Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Yieldd (/1000)
1-stage: TEOAE – dx audiology e
(Hahn et al 1999)
Hospital Münster, Germany Level IV QS=2/5
388 well babies
Not stated
Unilateral fail if TEOAE did not have ≥60% reproducib-ility and ≥80% stimulus stability
- 20.4 53.2 46.8 0.0
1-stage: DPOAE-dx audiology (3 re-screens)
(Ng et al 2004)
Tsan Yuk hospital Hong Kong Level IV QS=4/5
1064 infants born between May -October 1999
5 months Unilateral or bilateral failure >40 dB HL
98.9 3.4 - 56.8 5.6
1-stage: AABR – dx audiology
(Downs 1995)
17 hospitals in Colorado, USA Level IV QS=2/5
14,494 well and at-risk babies
Not stated
Bilateral or unilateral fail ≥35 dB HL
- 5.0 0.0 93.5 2.6
(Iley & Addis 2000)
York district hospital North Yorkshire, UK Level IV QS=3.5/5
48 babies
4 days Unilateral AABR fail ≥35 dB HL Diagnostic fail ≥40 dB
91.7 4.5 0.0 100.0f 0.0

Universal neonatal hearing screening 72
Table 13 (cont.) Descriptive (uncontrolled) studies of 1-stage universal neonatal hearing screening
Stage 1 Study Setting Population Study duration
Faila criterion
Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Yieldd (/1000)
1-stage: TEOAE+AABR – dx audiology e
(Hahn et al 1999)
Hospital Münster, Germany Level IV QS=2/5
55 well babies
Not stated
Unilateral fail if TEOAE did not have ≥60% reproducib-ility and ≥80% stimulus stability Unilateral AABR fail: >35 dB HL
-
3.6 0.0 100.0 0.0
(Chiong et al 2007)
Several communities in a rural area, Bulacan province, Philippines Level IV QS=2/5
724 babies
2 years 10 months
Fail not stated
66.6 - - - 22.1
TEOAE = transient evoked otoacoustic emissions test; AABR = automated auditory brainstem response test; dx = diagnostic. a Definition of the fail is provided in the study profiles in Appendix F; b loss to follow-up of failures after the screen; c false alarm rate – calculated as the number of infants falsely identified with hearing impairment divided by the total number of infants testing positive for hearing impairment ; d children with PCHI after diagnostic assessment – transient conductive hearing losses excluded where possible; e includes diagnostic ABR or any of the other diagnostic tests performed separately or as a test battery; f both cases were actually mild losses that fell between the screening and diagnostic hearing loss thresholds.

Universal neonatal hearing screening 73
Table 14 Descriptive (uncontrolled) studies of 2-stage universal neonatal hearing screening
Stage 1 Stage 2 Study Setting Population Study duration
Faila criterion Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
2-stage: TEOAE–TEOAE – dx audiology f
(Aidan et al 1999)
Hospital Paris, France Level IV QS = 5/5
1,727 well and at-risk babies
18 months Bilateral or unilateral fail >40 dB HL
82.3
16.7 48.3 47.9 3.8 0.0 77.8 1.4
Hospital London, UK Level IV QS = 4/5
1,492 well babies
4 years Bilateral or unilateral fail >40 dB HL
- 19.7 - 44.6 - - - 0.7 (Bantock & Croxson 1998)
Community-based health centre (~7% of population) London, UK
319 well and at-risk babies
1 year Bilateral or unilateral fail >40 dB HL
75.0 18.3
- - 2.3 - - 0.0
(Chapchap & Segre 2001)
Hospital Israelita Albert Einstein Sao Paulo, Brazil Level IV QS = 3.5/5
4,196 well and at-risk babies
3 years Failg if absent TEOAE for ≥2 of 4 frequency bands
90.6
1.7 17.8 47.9
34.2
0.0 60.0 2.4

Universal neonatal hearing screening 74
Table 14 (cont.) Descriptive (uncontrolled) studies of 2-stage universal neonatal hearing screening
Stage 1 Stage 2 Study Setting Population Study duration
Faila criterion Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
(Daemers et al 1996)
St Augustinus Hospital Antwerp, Belgium Level IV QS = 3/5
907 well babies born in 1993 and 1994
2 years Bilateral or unilateral fail if TEOAE absent for 4 frequency bands
- 18.9 25.1 56.1 18.7 59.4 34.4 1.1
(De Capua et al 2003)
University of Siena Italy Level IV QS=4.5/5
532 well and at-risk infants (448 well babies; 84 at-risk)
Not stated Fail if TEOAE reproducibility <50% with n<3 frequencies with intensity >3 dB SPL (sound pressure level)
- 11.7 - - 20.9 - - 5.6
(Govaerts et al 2001)
St Augustinus Hospital Antwerp, Belgium Level IV QS = 4/5
2,012 well and at-risk babies born in 1999
1 year Bilateral fail if TEOAE absent at 3 of 4 frequencies Dx ABR bilateral fail >40 dB
99.4
1.4 0.0 78.6 21.4 0.0 33.3 2.0
(Habib & Abdelgaffar 2005)
Dr. Soliman Fakeeh Hospital Jeddah, Saudi Arabia Level IV QS=4/5
11, 986 non-high-risk neonates
8 years Failure to produce more than 50% reproducibility and response amplitude at least 1dB SPL per octave
91.7 8.7 0.0 71.2 28.8 - 92.7 1.8

Universal neonatal hearing screening 75
Table 14 (cont.) Descriptive (uncontrolled) studies of 2-stage universal neonatal hearing screening
Stage 1 Stage 2 Study Setting Population Study duration
Faila criterion Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
(Hatzopoulos et al 2007)
Main maternity hospital of Tirana Tirana, Albania Level IV QS=3.5/5
1,561 well and at-risk babies (463 well & 1,098 NICU babies)
1 year Fail to produce ≥ 70% reproducibility, and a ≥6 dB SNR (signal-to-noise ratio) for at least 2 out of 5 frequency bands
- 13.6 50.0 42.3 7.7 12.5 75.0 1.3
(Huynh et al 1996)
Air Force community hospital Maryland, USA Level IV QS=5/5
639 well babies
6 months Bilateral fail at first screen / unilateral fail at re-screen if TEOAE <80% reproducib-ility at 2.4, 3.2, 4.0 kHz
98.1 9.6 0.0 81.7 18.3 0.0 45.5 1.6
(Isaacson 2000)
Temple University Hospital, North Philadelphia
Pennsylvania USA
Level IV QS=3.5/5
2,137 well and at-risk babies
1 year Bilateral or unilateral fail if TEOAE absent at signal-to-noise ratio ≥3 dB at 3 of 4 frequency bands
95.0
8.2 36.5 - - - - 6.9

Universal neonatal hearing screening 76
Table 14 (cont.) Descriptive (uncontrolled) studies of 2-stage universal neonatal hearing screening
Stage 1 Stage 2 Study Setting Population Study duration
Faila criterion Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
(Jakubikova et al 2003)
Two gynaecology and neonatology departments in Bratislava Department of Pathological Newborn and Intensive Care Unit of Children’s University, Bratislava Slovak Republic Level IV QS=3.5/5
3048 newborns (approx 45% at-risk)
Not stated Fail criteria not stated
100 4.9 19.3 60.7 20.0 0.0 23.3 6.9
(Kanne et al 1999)
Madigan Army Medical Centre, Tacoma Washington USA Level IV QS=4.5/5
2,537 well and at-risk babies
14 months Unilateral or bilateral failure to produce emission spectrum of significant gain across testing frequency range >30 dB HL
90.2
8.9
12.3
64.7 23.0
8.5
80.9
0.4

Universal neonatal hearing screening 77
Table 14 (cont.) Descriptive (uncontrolled) studies of 2-stage universal neonatal hearing screening
Stage 1 Stage 2 Study Setting Population Study duration
Faila criterion Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
(Khairi et al 2005)
Hospital Universiti Sains Malaysia Level IV QS=4/5
401 newborns (202 well babies, 199 at-risk)
Study duration: Feb-March 2000 & Feb-May 2001
Fail not stated - 7.7 29.0 54.8 16.1 0.0 20.0 10.0
(Khandekar et al 2006)
Hospitals in Oman, Turkey Level IV QS=4.5/5
32,080 live births (well and at-risk) in 2003
1 year Not stated 66.6 10.7 - 88.5 11.5 20.0 32.7 1.2
(Kolski et al 2007)
Maternity hospital France Level IV QS=3.5/5
Strategy 1: 3202 newborns Strategy 2: 2588 2 month old babies Study duration: not stated
Not stated Bilateral fail Strategy 1: 95.7 Strategy 2: 64.2
1.1 3.1
5.9 36.5
64.7 17.3
29.4 46.2
10.0 4.2
50.0 79.2
1.3

Universal neonatal hearing screening 78
Table 14 (cont.) Descriptive (uncontrolled) studies of 2-stage universal neonatal hearing screening
Stage 1 Stage 2 Study Setting Population Study duration
Faila criterion Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
(Lin et al 2004)
2 hospitals & 4 obstetric clinics Tainan, Taiwan Level IV QS=4/5
5,938 neonates 2 years 9 months
Failure to produce 4 pairs of alternating positive & negative peaks Diagnostic ABR: Failure to produce wave V latency within developmental norms in response to 35dB nHL clicks
59.3 9.0 26.1 56.8 17.0 - - 1.5
(Low et al 2005)h
Singapore General Hospital, Singapore Level IV QS=4/5
2,973 well and at-risk babies
2 years Fail not stated 99.7 - - - 2.4 16.7 40.0 1.2
(Martines et al 2007)
Sciacca Hospital Italy Level IV QS=3.5/5
1,068 well and at-risk babies born during 2003-2004 942 well babies 126 at-risk babies
2 years Fail criterion not stated
89.7 At-risk 11.1
At-risk 0.0
At-risk 57.1
At-risk 42.9
At-risk 0.0
At-risk -
1.9

Universal neonatal hearing screening 79
Table 14 (cont.) Descriptive (uncontrolled) studies of 2-stage universal neonatal hearing screening
Stage 1 Stage 2 Study Setting Population Study duration
Faila criterion Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
(McPherson et al 1998)
Eight community health clinics, Northern Brisbane Queensland, Australia Level IV QS=2/5
1,305 children, 1.5–2.5 months of age
30 months Unilateral or bilateral fail if TEOAE <3 dB above the noise floor and at least halfway across the test frequency bands of 2–3 kHz and 3–4 kHz
93.3 10.8 42.7 24.4 32.8 27.9 20.9 2.5
(Owen et al 2001)
Local health centres and homes in urban and rural settings West Gloucester-shire, UK Level IV QS=3.5/5
683 well babies registered at participating health centres in 1999
1 year Bilateral or unilateral fail if TEOAE response <28 dB, or response correlation <98%, or signal-to-noise ratio did not reach target level for 3 wavebands
98.8 4.3 0.0 96.6 3.4 0.0 0.0 1.5
(Rouev et al 2004)
Maternity Hospital Stara Zagora Bulgaria Level IV QS=4/5
1,750 well and at-risk babies
329 days Bilateral fail >30 dB HL
95.5 12.8 0.0 89.7 10.3 0.0 86.4 1.8

Universal neonatal hearing screening 80
Table 14 (cont.) Descriptive (uncontrolled) studies of 2-stage universal neonatal hearing screening
Stage 1 Stage 2 Study Setting Population Study duration
Faila criterion Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
(Swanepoel et al 2007)
Private hospital in urban Gauteng South Africa Level IV QS=4/5
6,241 well and at-risk babies
4 years Bilateral and unilateral sensorineural hearing loss of ≥ 35dB
45.0 11.1 - 31.5 - - - 1.0
(Tatli et al 2007)
Dokuz Eylul University Hospital, Izmir Turkey Level IV QS=4.5/5
711 well and at-risk babies (475 well babies, 236 NICU babies)
18 months Unilateral fail - 3.9 21.4 60.7 17.9 0.0 40.0 4.2
(Tsuchiya et al 2006)
Kumamoto University Hospital Kumamoto Japan Level IV QS=4/5
8979 well and at-risk babies born during 1999-2004
5 years Fail ≥ 35dB 64.8 0.4 0.0 16.2 83.8 3.2 16.1 2.9
(Vohr et al 1998)
8 maternity hospitals Rhode Island, USA Level IV QS=5/5
53,121 well and at-risk babies born 1993–1996
4 years Unilateral or bilateral fail if no TEOAE response at 2–4 kHz with 75% reproducib-ility ABR fail if wave V not present >30 dB nHL
99.1 10.2 15.2 72.2 12.5 3.0 80.6 2.1

Universal neonatal hearing screening 81
Table 14 (cont.) Descriptive (uncontrolled) studies of 2-stage universal neonatal hearing screening
Stage 1 Stage 2 Study Setting Population Study duration
Faila criterion Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
(Watkin & Baldwin 1999)
Whipps Cross hospital London, UK Level IV QS=4/5
28,890 babies
6 years Bilateral fail on initial screen and re-screen, although unilateral fail allowed if obvious parental anxiety ABR fail >40dB nHL in better hearing ear
87.2 - - - - 11.1 65.6 1.7
(Zaputovic et al 2005)
Rijeka University Hospital Croatia Level IV QS=3.5/5
6,019 neonates Study duration: 26 months
26 months Unilateral or bilateral fail on first screen
98.8 6.0 6.6 69.8 23.6 13.9 69.8 2.3
2-stage: TEOAE–AABR – dx audiology
(Bailey et al 2002)
5 maternity hospitals Perth, Australia Level IV QS=5/5
13,214 well and at-risk babies
18 months Unilaterali or bilateral fail ≥35 dB HL
96.2 2.7 8.5 73.5 3.7 0.0 47.8
0.9

Universal neonatal hearing screening 82
Table 14 (cont.) Descriptive (uncontrolled) studies of 2-stage universal neonatal hearing screening
Stage 1 Stage 2 Study Setting Population Study duration
Faila criterion Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
(Bamford et al 2005)
23 areas of England Level IV QS=4/5
About 120,000 births per annum (well and at-risk)
2 years Not stated 97.5 - - - - - - Bilateral 1/1000 Unilateral 0.64/1000
(Brennan 2004)
Instititution in Illinois USA Level IV QS=2.5/5
Not stated Not stated Not stated >98.0 - - - 3.0 - - -
(Hunter et al 1994a)
Princess Anne Hospital Southamp-ton, UK Level IV QS=5/5
217 well and at-risk babies
4 weeks Unilateral or bilateral AABR fail ≥35 dB HL
93.0
30.3 13.1 85.2 1.6 0.0 100.0 0.0
(Leveque et al 2007)
17 maternity wards, private and public, and one NICU in Champagne-Ardenne France Level IV QS=4.5/5
33, 873 well and at-risk babies born from January 2004 to March 2006
26 months Bilateral fail ≥35 dB HL -40 db HL depending on screening device used (could not be modified)
92.4 1.3 2.5 89.8 7.7 0.0 14.7 0.8

Universal neonatal hearing screening 83
Table 14 (cont.) Descriptive (uncontrolled) studies of 2-stage universal neonatal hearing screening
Stage 1 Stage 2 Study Setting Population Study duration
Faila criterion Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
(Low et al 2005)
National University Hospital, Singapore Level IV QS=4/5
4,849 well and at-risk babies
2 years Fail not stated 99.8 - - - 0.6 3.2 12.9 5.4
(Molini et al 2004)
Hospital Italy Level IV QS=4/5
2,425 full-term newborns (well and at-risk babies)
Study 1: 17 months Study 2: 9 months
Failure to produce at least 3 of the 4 frequency bands centred at 1600, 2400, 3200 and 4000 Hz.
Study 1 94.2 Study 2: 72.4
Study 1: 8.9 Study 2: 10.1
Study 1: 17.4 Study 2: 20.2
Study 1: 77.5 Study 2: 74.2
Study 1: 5.1 Study 2: 5.6
Study 1: 0.0 Study 2: 0.0
Study 1: 0.0 Study 2: 0.0
Study 1 & 2: 5.0
(Neumann et al 2006)
Germany Level IV QS=4/5
17, 349 well and at-risk babies in 2005
1 year TEOAE ≥ 30dB HL AABR ≥ 35dB HL
95.2 2-stage 7.1 1 stage AABR 1.9 1 stage TEOAE 5.2 Total: 3.0
-
-
-
-
-
2.8

Universal neonatal hearing screening 84
Table 14 (cont.) Descriptive (uncontrolled) studies of 2-stage universal neonatal hearing screening
Stage 1 Stage 2 Study Setting Population Study duration
Faila criterion Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
2-stage: DPOAE–AABR – dx audiology
(Cox & Toro 2001)
Boston Medical Centre Massa-chusetts, USA Level IV QS=5/5
1,713 well and at-risk j babies
1 year Fail not statedg - - - - - 13.3 36.7 2.9
(Mukari et al 2006)
Hospital University Kebangsaan Malaysia (HUKM) Level IV QS=4/5
4,437 newborns (315 NICU, 4122 non-NICU)
11 months Fail not stated 84.6 18.7 43.0 50.3 6.7 38.1 32.7 3.6
2-stage: AABR–AABR – dx audiology
(Clemens et al 2000)
Women’s Hospital North Carolina, USA Level IV QS=3/5
5,034 well babies k
1 year Fail >35 dB HL 99.5
2.1 17.4 68.0 14.6 6.7 33.3 1.8

Universal neonatal hearing screening 85
Table 14 (cont.) Descriptive (uncontrolled) studies of 2-stage universal neonatal hearing screening
Stage 1 Stage 2 Study Setting Population Study duration
Faila criterion Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
(Connolly et al 2005)
University of Mississippi Mississippi, USA Level IV QS=4.5/5
17,602 well and at-risk babies
5 years Fail >35 dB nHL Several re-screens at stage 1 and stage 2
100 - - - - - - 4.4
(Iwasaki et al 2003)
Seirei-Hamamatsu General Hospital & Seirei-Mikatahara General Hospital Hamamatsu, Japan Level IV QS=4.5/5
4092 infants 2 years Fail if likelihood ratio is less than 160 after 15000 sweeps
99.8 1.2 0.0 40.8 59.2 0.0 48.3 3.7
(Low et al 2005)
KK Women’s and Children’s Hospital, Singapore Level IV QS=4/5
28,273 well and at-risk babies
2 years Fail not stated 99.8 - - - - 19.6 8.5 3.0

Universal neonatal hearing screening 86
Table 14 (cont.) Descriptive (uncontrolled) studies of 2-stage universal neonatal hearing screening
Stage 1 Stage 2 Study Setting Population Study duration
Faila criterion Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
(Mason & Herrmann 1998)
Medical Center Honolulu, Hawaii Level IV QS=4/5
10,773 well and at-risk babies
5 years Bilateral AABR fail ≥35 dB HL Diagnostic fail >35 dB nHL
96.3 4.0 - - - - - 1.4
(Oudesluys-Murphy & Harlaar 1997)
Community well baby clinic, Barendrecht Netherlands Level IV QS=5/5
288 well and at-risk babies
1 year Unilateral or bilateral fail >35 dB HL
98.6 13.0 29.7 51.4 18.9 14.3 57.1 3.5
(Rao et al 2002)
5 small rural hospitals, central Minnesota USA Level IV QS=2.5/5
217 well babies born in 1999 and 2000
1 year Not stated 78.8 - - - - - - 5.8
(Yee-Arellano et al 2006)
Private hospital in San Pedro Garza Garcia Mexico Level IV QS=4/5
3,066 well and at-risk babies
2 years ABR unilateral or bilateral fail >35-40 dB HL
99.9 - - - - - - 2.0

Universal neonatal hearing screening 87
TEOAE = transient evoked otoacoustic emissions test; AABR = automated auditory brainstem response test; dx = diagnostic; DPOAE = distortion product otoacoustic emissions test; SPL=sound pressure level; NICU=neonatal intensive care unit; a Definition of the fail is provided in the study profiles in Appendix F; b loss to follow-up of failures after the screen; c false alarm rate – calculated as the number of infants falsely identified with hearing impairment divided by the total number of infants testing positive for hearing impairment ; d referral to an audiologist for diagnostic assessment; e children with PCHI after diagnostic assessment – transient conductive hearing losses excluded where possible; f includes diagnostic ABR or any of the other diagnostic tests performed separately or as a test battery; g bilateral or unilateral fail not stated; h the type of OAE is not clearly specified; i bilateral fail in 40 babies, until criteria changed; j all NICU babies received a 1-stage AABR screen followed by diagnostic referral; k approximately half of the babies that failed the initial AABR received a re-screen AABR in stage 1.

Universal neonatal hearing screening 88
Table 15 Descriptive (uncontrolled) studies of 3-stage (or more) universal neonatal hearing screening
Stage 1 Stage 2 Stage 3 Study Setting Population Study duration
Faila criterion
Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rate (%)
LTFU (%)
FA rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
3-stage: AABR–AABR–AABR – dx audiology f
(Clemens & Davis 2001)
Women’s Hospital North Carolina, USA Level IV QS=5/5
3,144 well babies
6 months Fail >35 dB HLg
99.9 4.2
4.6 70.2 25.2 0.0 75.8 24.2 0.0 12.5 2.2
3-stage: AABR–AABR–TEOAE – dx audiology
(Messner et al 2001)
Lucile Packard Children’s Hospital, Stanford California, USA Level IV QS=5/5
6,340 well babies born 1998–1999
16 months
Unilateral or bilateral fail >35 dB HL
91.0 11.2 28.2 47.1 24.7 48.8 31.3 20.0 - - 1.6
3-stage: TEOAE–ABR–TEOAE + ABR – dx audiology
(Clarkson et al 1994) (Maxon et al 1993)
Women and Infants Hospital, Providence Rhode Island, USA Level IV QS=2.5/5
1,850 well and at-risk babies born 1990–1991
6 months
Fail ≥60 dB HL referred for dx ABR; <60 dB HL referred for behavioural audiologic evaluationg
- 26.9 18.9 57.5 23.5 - - - 27.0 31.3 5.9

Universal neonatal hearing screening 89
Table 15 (cont.) Descriptive (uncontrolled) studies of 3-stage (or more) universal neonatal hearing screening
Stage 1 Stage 2 Stage 3 Study (cont)
Setting Population Study duration
Faila criterion
Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rate (%)
LTFU (%)
FA rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
3-stage: TEOAE–TEOAE–TEOAE – dx audiology
(Lin et al 2005)
Mackay Memorial Hospital Taipei, Taiwan Level IV QS=4/5
18, 260 well babies born 1998-2004
5 years 2 months
Bilateral or unilateral failure to produce TEOAE of (1) ≥5 dB in 3 of 5 frequency bands or (2) ≥3 dB in 4 of 5 frequency bands Dx ABR failure to produce a repeatable wave V at 35 dB nHL unilaterally or bilaterally
- - - - 5.8 18.6 73.4 8.0 0.0 0.0 4.5

Universal neonatal hearing screening 90
Table 15 (cont.) Descriptive (uncontrolled) studies of 3-stage (or more) universal neonatal hearing screening
Stage 1 Stage 2 Stage 3 Study (cont)
Setting Population Study duration
Faila criterion Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rate (%)
LTFU (%)
FA rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
3-stage: TEOAE–TEOAE–ABR – dx ABR
(Martines et al 2007)
Sciacca Hospital Italy Level IV QS=3.5/5
1,068 well and at-risk babies born during 2003-2004 942 well babies 126 at-risk babies
2 years Fail criterion not stated
89.7 Well-babies 4.7
Well-babies 0.0
Well-babies 75.0
Well-babies 25.0
Well-babies 0.0
Well-babies 54.5
Well-babies 45.5
Well-babies 0.0
Well-babies 20.0
1.9
(Pastorino et al 2005)
Instituti Clinici di Perfezionamento Milan, Italy Level IV QS=4/5
19777 well and at-risk babies 3-stage for well babies 1-stage for at-risk babies however only screening yield was obtainable
Not stated
Screening: Failure to produce ≥ 70% total reproducibility Failure to produce ≥50% in the 1.6-kHz band and 70% in 2,4-, 3.2- and 4-kHz bands Diagnostic ABR ≥40 dB HL
- Well babies 2.4
Well babies 12.8
Well babies 62.8
Well babies 24.4
Well babies 15.7
Well babies 67.8
Well babies 16.5
Well babies 0.0
Well babies 0.0
Well & at-risk babies 3.2

Universal neonatal hearing screening 91
Table 15 (cont.) Descriptive (uncontrolled) studies of 3-stage (or more) universal neonatal hearing screening
Stage 1 Stage 2 Stage 3 Study (cont)
Setting Population Study duration
Faila criterion
Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rate (%)
LTFU (%)
FA rate (%)
Failure rated (%)
LTFU (%)
FA rate (%)
Yielde (/1000)
3-stage: TEOAE–AABR–TEOAE– dx ABR
(Lin et al 2005)
Mackay Memorial Hospital Taipei, Taiwan Level IV QS=4/5
3,013 well babies born Feb-December 2004
10 months
Bilateral or unilateral failure to produce TEOAE of (1) ≥5 dB in 3 of 5 frequency bands or (2) ≥3 dB in 4 of 5 frequency bands Dx ABR – failure to produce a repeatable wave V at 35 dB nHL unilaterally or bilaterally
- 6.4 0.0 71.6 28.4 - - - - - 3.0
AABR = automated auditory brainstem response test; dx = diagnostic; TEOAE = transient evoked otoacoustic emissions test. a Definition of the fail is provided in the study profiles in Appendix F; b loss to follow-up of failures after the screen; c false alarm rate – calculated as the number of infants falsely identified with hearing impairment divided by the total number of infants testing positive for hearing impairment ; d referral to an audiologist for diagnostic assessment; e children with PCHI after diagnostic assessment – transient conductive hearing losses excluded where possible; f includes diagnostic ABR or any of the other diagnostic tests performed separately or as a test battery; g bilateral or unilateral fail not stated.

Universal neonatal hearing screening 92
Table 15 (cont.) Descriptive (uncontrolled) studies of 3-stage (or more) universal neonatal hearing screening
Multi-stage: TEOAE–TEOAE–TEOAE-TEOAE (4 to 7 re-screens) – dx audiology
Stage 1 Stage 2 Stage 3 Stage 4 Study Setting Population Study duration
Faila criterion
Coverage (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Failure rate (%)
LTFUb (%)
FAc rate (%)
Yielde (/1000)
(Shoup et al 2005)
Large public hospital Dallas, Texas Level IV QS=4.5/5
48, 211 well and at-risk babies
3 years Fail not stated
- 3.6 - - 34.0 - - 50.7 - - 58.2 - - 3.7
AABR = automated auditory brainstem response test; dx = diagnostic; TEOAE = transient evoked otoacoustic emissions test. a Definition of the fail is provided in the study profiles in Appendix F; b loss to follow-up of failures after the screen; c false alarm rate – calculated as the number of infants falsely identified with hearing impairment divided by the total number of infants testing positive for hearing impairment ; d referral to an audiologist for diagnostic assessment; e children with PCHI after diagnostic assessment – transient conductive hearing losses excluded where possible; f includes diagnostic ABR or any of the other diagnostic tests performed separately or as a test battery; g bilateral or unilateral fail not stated.
.

Universal neonatal hearing screening 93
Loss to follow-up
Losses to follow-up (LTFU) of initial screen failures ranged from 0–53 per cent in the uncontrolled screening programs that reported on this outcome (Table 13, Table 14, Table 15). The largest LTFU (36.5–53.2%) after the initial screen occurred in studies where there was commonly a long delay before re-screening (2 weeks to 2 months (Aidan et al 1999; Kolski et al 2007; McPherson et al 1998; Mukari et al 2006) or before diagnostic testing (4 months) in the case of a one-stage screening protocol (Hahn et al 1999). In only one of these studies (Isaacson 2000) was there an immediate re-screen. This hospital-based program was conducted in an economically depressed inner-city area and it is likely that the 37 per cent LTFU was related to very early hospital discharge rates.
The majority of hospital-based studies experienced no LTFU from diagnostic referrals. However, the largest LTFU from diagnostic referral did occur with a hospital-based screening program in Belgium (Daemers et al 1996) – 59 per cent of infants referred for diagnostic testing at 3 months of age were not assessed. The authors attribute this to a lack of parental and health professional awareness and commitment. It is probable that the longer it takes for diagnostic testing to occur, the less likely it is that there will be compliance in attendance unless, for example, reminder and educational strategies are put in place. Two of the four community-based programs experienced large LTFU – in the range of 30–43 per cent after the initial screen and 14–28 per cent after diagnostic referral (McPherson et al 1998; Oudesluys-Murphy & Harlaar 1997). However, two community-based studies managed no LTFU, in a two-stage screening program (Chiong et al 2007; Owen et al 2001).
Absolute and incremental yield
Yield is defined as the number of cases of permanent childhood hearing impairment (PCHI) ultimately identified in the screened population. This relates primarily to permanent sensorineural or conductive hearing impairment as opposed to transient conductive losses. The latter were reported in the evidence-base and generally had a much higher yield. These were not, however, included in the total presented yield figures as there is insufficient evidence to indicate that transient conductive losses have an impact on the language and learning outcomes of young children. Conductive losses were included in the yield figures when they were described as permanent losses.
The highest level of evidence available (Kennedy et al 1998) reported that infants born during periods of universal neonatal hearing screening (UNHS) are 2.3 times more likely [RR = 2.3, 95%CI 1.1, 4.7] to receive a diagnosis of PCHI than infants born in periods without universal hearing screening (Table 12) The absolute increase in benefit is small (an extra five children identified per 10,000) because of the low prevalence of the condition. This means that 1,970 infants [95%CI 1,063, 13,459] would need to be universally screened for hearing impairment, as compared to not screening, to ensure the diagnosis of one infant with PCHI. It was unclear in this study whether diagnosis before the age of 10 months occurred more frequently with or without UNHS, as there was a lack of statistical power for this outcome. Controlling for the severity of infant hearing impairment resulted in a trend towards a five-fold increase in the odds of diagnosis (before 10 months of age) during periods of hearing screening.

Universal neonatal hearing screening 94
Three average to good quality retrospective cohort studies (level III-2 screening evidence) determined that children with PCHI were more likely to be diagnosed before the age of 6 months when born during periods of, or in hospitals with, UNHS than children who were not exposed to such screening programs (Table 12) (Nekahm et al 2001a; Weichbold et al 2006; Yoshinaga-Itano et al 2001). The larger of these good quality studies indicated that diagnosis of bilateral PCHI before the age of 6 months was 5.1 times more likely to occur in children who were born in hospitals with UNHS [RR = 5.1, 95%CI 2.1, 12.4]. This means that for every three children [95%CI 2, 5] with bilateral PCHI born in an Austrian hospital with a screening program, one additional child would be diagnosed with PCHI before the age of six months than if born in a hospital without a screening program (Nekahm et al 2001a). The average quality study conducted by the same researchers, covering a larger population of Austria, also found that the early diagnosis of infants at three months of age was nearly 18 times more likely when born in a hospital with, as opposed to without, universal hearing screening [RR 17.5, 95% CI 5.7, 55.7] (Weichbold et al 2006).
In uncontrolled studies the yield of infants with PCHI from UNHS programs generally ranged from 1/1,000 to 3/1,000. This yield was fairly consistent no matter the type of screening protocol used (Table 13, Table 14, Table 15). Exceptionally high yields were seen in the studies by Chiong et al (2007) and Khairi et al (2005), reporting yields of 22.1 and 10.0/1, 000, respectively. These two studies sampled a non-Caucasian population. The study by Chiong and colleagues, reporting the highest screening yield, was conducted in underprivileged rural communities in the Philippines, with poor antenatal care. It is possible that selection of this population translated into higher rates of ‘at-risk’ babies. Variation in yields in these uncontrolled studies may have occurred due to differences in LTFU, the proportion of well and ‘at-risk’ babies, and the size of the population being sampled.
Age at management
The Wessex Controlled Trial provided the highest level of available evidence (level III-1 screening evidence) to assess the effect of universal neonatal hearing screening on the age at which children with permanent childhood hearing impairment (PCHI) receive treatment and/or rehabilitation, compared to not screening (Table 12). This study found a trend that indicated screening may increase the likelihood of PCHI management before the age of 10 months by 2.4 times [RR = 2.4, 95%CI 1.0, 5.8]. The study was under-powered for this outcome but when the authors controlled for the severity of PCHI, the odds of early management through screening increased eight-fold [OR = 8.0, 95%CI 1.2, 51.0]. The absolute increase in benefit, over not screening, is early PCHI management (<10 months of age) for an approximate additional 4 children in 10,000. In real terms this translates into screening 2,965 children [95%CI 1458, 86207] for hearing impairment, compared to not screening, to ensure the early management (<10 months of age) of one infant with PCHI. A retrospective cohort study conducted by Weichbold et al (2006) (level III-2 screening evidence) also assessed age at management but only had the population of true hearing impaired children available, thus the number needed to screen amongst the whole population could not be calculated.

Universal neonatal hearing screening 95
Summary – Does universal neonatal hearing screening, and the finding of a positive and/or negative test, affect the clinical management or treatment options available to permanently hearing impaired infants?
Referral for definitive diagnostic testing, actual permanent childhood hearing impairment (PCHI) diagnosis, and management of PCHI commonly occurs earlier and more frequently with universal neonatal hearing screening (UNHS) than without it.
Level III-1 screening evidence indicates that referring an infant for diagnostic testing before the age of 6 months is nearly three times more likely [RR = 2.9, 95%CI 1.4, 6.3] (19 times when controlling for the severity of hearing impairment) with UNHS than when universal screening is not available. Infants born during periods of UNHS are twice as likely to receive a diagnosis of PCHI, than infants born in periods without universal screening [RR = 2.3, 95%CI 1.1, 4.7]. The absolute increase in benefit is small, however – an extra five children identified per 10,000 – because of the low prevalence of the condition. There is also an indication that screening may increase the likelihood of PCHI management before the age of 10 months by nearly two-and-a-half times [RR = 2.4, 95%CI 1.0, 5.8] (eight times when controlling for the severity of PCHI). Similar, but more precise, results were reported in studies of a lower level of evidence (III-2 screening evidence).
Descriptive data indicates that the majority of UNHS programs manage to screen over 90 per cent of infants in their catchment area. These programs are largely hospital-based, with initial screening occurring prior to discharge. Community-based studies also obtain very good coverage when screening is ‘piggy-backed’ onto other health or immunisation checks at the health clinic or when it occurs in the home. Losses to follow-up commonly occur when there is a long delay prior to re-screening or diagnostic testing of the infant, or when infants and mothers are discharged early from the hospital.
Uncontrolled studies suggest that given the higher referral rate from transient evoked otoacoustic emissions screen protocols, the number of false alarms associated with these programs is higher (up to approximately 10%) than programs using automated auditory brainstem response screen protocols (up to approximately 6%). It is, however, possible to maintain low false alarm rates using either type of screening protocol.

Universal neonatal hearing screening 96
Does universal neonatal hearing screening, and therefore possible alterations in clinical management, have an impact on the adverse outcomes associated with permanent childhood hearing impairment?
Data on the longer term impact of a screening program on primary outcomes – rate and quality of language acquisition, behaviour, family functioning, communication ability / social functioning, educational achievement, employment status, socioeconomic status and quality of life – were available in limited form in two studies (Kennedy et al 2006; Yoshinaga Itano et al 2000). While Yoshinaga-Itano and colleagues conducted a retrospective matched-pair cohort study, Kennedy et al followed the birth cohort reported in their 1998 Wessex trial prospectively until schooling age (level III-2 screening evidence). Both studies compared the quality of language acquisition and communication ability in children with permanent hearing impairment born in hospitals with and without universal neonatal hearing screening (UNHS) (Kennedy et al 2006; Yoshinaga Itano et al 2000). Neither of these good quality studies, however, reported on the longer term outcomes, such as educational achievement and employment status, because the cohorts in question were not old enough.
Language acquisition
Language is a system representing concepts through the use of words (Owens 1996). Assessment of language ability incorporates the measurement of several distinct features of language. For example, receptive language deals with the extent of a child’s vocabulary, including the number of words understood, and an understanding of requests, parts of speech and semantic categories. In contrast, expressive language is more concerned with the way in which language is used, such as the expression and use of words and parts of speech (White & White 1987). Studies included in this assessment used a variety of evaluation tools to measure the various aspects of language.
Yoshinaga-Itano and colleagues (2000) assessed the expressive language, receptive language and total language ability of children with bilateral permanent childhood hearing impairment (PCHI) and determined whether there were any differences in linguistic ability according to whether the children were born in hospitals with or without UNHS. The sample size was small, consisting of 25 matched pairs, and some information on the outcome measures was incomplete. Similar outcomes were measured in a second cohort study however it was a much larger study with 120 children which included 61 who received UNHS and 59 without UNHS (Kennedy et al 2006).
Linguistic ability was measured differently across the two studies. Yoshinaga-Itano and colleagues measured it using a language quotient derived from the Minnesota Child Development Inventory. This inventory has apparently been validated using other special-needs children but has not been validated for a hearing-impaired paediatric population. Further, the language quotient is based on assessment by the parent or caregiver of the child – who, of course, was aware of the screening status of the child – rather than through an independent, blinded assessment. Only those children without significant cognitive delays (cognitive quotient >70) were included in the analysis. The children were matched on chronological age, severity of PCHI and cognitive ability, thus nullifying the effect of confounders known to have an impact on linguistic ability. Other potential confounders such as gender, ethnicity, other disabilities, mode of communication and education level of the primary caregiver were not distributed differently between the screening and not-screening groups.

Universal neonatal hearing screening 97
Children in the screened group were found to have, on average, higher language quotient scores for expressive language (UNHS = 82.9±18.5‡; not UNHS = 62.1±21.5; t[24] = 5.53, p<0.001), receptive language (UNHS = 81.5±18.5; not UNHS = 66.8±20.0; t[24] = 4.21, p<0.001) and total language (UNHS = 82.2±16.5; not UNHS = 64.4±19.5; t[24] = 5.39, p<0.001) than children in the unscreened group. Assuming that a 20 per cent difference in mean scores on the Minnesota Child Development Inventory is clinically relevant, the comparative gain in expressive and total language for the screened group was clinically significant and the gain in receptive language approached clinical significance.
In terms of expressive vocabulary, as measured by the MacArthur Communicative Development Inventory, the majority of children in the screened group had larger, more expressive vocabularies than their matched pairs in the unscreened group (nonparametric Wilcoxon signed ranks test, Z = 3.72, p<0.001). Again, these results are based on unblinded assessment.
Kennedy et al (2006) used two different tests for receptive language: the Test for Reception of Grammar and the British Picture Vocabulary Scale. An aggregate score, however, was calculated to combine the results obtained. Children in the screened group were found to have higher scores for receptive language (adjusted mean difference=0.56 [95% CI 0.03, 1.08], p=0.04), however the clinical significance of this difference is unclear due to the lack of data provided.
For determination of expressive language acquisition, an aggregate score was also calculated, this time because two components of the Renfrew Bus Story Test were used (sentence information and 5 longest sentences). This aspect of language ability, however, did not show a significant difference between those exposed and not exposed to universal hearing screening (adjusted mean difference 0.30 [95% CI -0.22, 0.81], p=0.25).
Communication ability
Speech is the neuromuscular process of producing sounds for communication. It is the verbal means of transmission of language (Owens 1996). Language and speech are distinctly different.
Yoshinaga-Itano and colleagues (2000) assessed the speech of those children with bilateral permanent childhood hearing impairment (PCHI) born in hospitals with and without universal neonatal hearing screening (UNHS). Phonological experts observed video-taped parent–child interactions and evaluated the speech intelligibility and number of intelligible words produced by the children. The phonological expert was blinded to the screening status of the child (Yoshinaga-Itano, pers comm 2003), so it is unlikely that observer bias affected the results. Median speech intelligibility for the screened group was rated as ‘speech is very hard to understand’, whilst for the matched pairs in the unscreened group it was rated as ‘always / almost always unintelligible’. The two distributions of speech intelligibility ratings were significantly different (nonparametric Wilcoxon signed ranks test, Z = 2.43, p = 0.015).
‡ Mean ± standard deviation, related t-test with degrees of freedom in brackets.

Universal neonatal hearing screening 98
On the other hand, Kennedy and colleagues (2006) measured communication ability by means of principal caregiver completion of a speech scale from the Children’s Communication Checklist. This assessment was also blinded, as the researcher conducting the interview was unaware of the child’s early hearing or audiologic history and often the caregiver was the mother. This method was distinctly different to that used by Yoshinaga-Itano and colleagues (2000). Mean z scores for children who had or did not have universal neonatal hearing screening were calculated using 63 English-speaking children with normal hearing, matched for place of birth and age at assessment. These were used to measure unadjusted and adjusted mean differences (based on severity of hearing impairment and maternal education) between the two groups. There were no statistically significant differences in measures of speech between those exposed to universal newborn hearing screening and those not exposed to screening (adjusted mean difference=0.12 [95% CI -0.46, 0.71], p=0.68). There needs to be consideration that assessment was based on parental or professional report as opposed to direct infant measurement and therefore may not be as sensitive as the results from the study by Yoshinaga-Itano and colleagues.
As UNHS programs were predominantly introduced in the mid- to late-1990s, it is unlikely that information on the longer term, but highly relevant, outcomes (ie educational and employment status) will be reported in the peer-reviewed literature for another decade or so.

Universal neonatal hearing screening 99
Summary – Does universal neonatal hearing screening, and therefore possible alterations in clinical management, have an impact on the adverse outcomes associated with permanent childhood hearing impairment?
There is very limited information available on the effect of universal neonatal hearing screening (UNHS) on primary or patient-relevant outcomes. Two good quality studies (level III-2 screening evidence) were identified, although one was a small, matched-pair retrospective cohort study that assessed the impact of screening on language acquisition and communication ability.
The results indicate that children with bilateral permanent childhood hearing impairment (PCHI) born in hospitals with UNHS have better receptive language abilities than children with PCHI born in hospitals without screening. There were contradictory results on expressive language acquisition with the larger, more recent study finding no statistically significant or clinically important differences. Differences seen in the smaller retrospective study need to be considered with caution as assessment of the language outcome measures was unblinded to the screening status of the child.
Conversely, the independent, blinded assessment conducted by Yoshinaga-Itano and colleagues of communication ability lends credence to the finding that the superior speech intelligibility of some children with bilateral PCHI is associated with birth in a screening hospital. Whilst findings were not consistent with Kennedy et al.( 2006), this may be a result of parental assessment, rather than direct assessment of children’s communication.
Information on the impact of UNHS programs on the longer term outcomes (ie educational and employment status) is unlikely to be reported in the peer-reviewed literature for another decade or so.

Universal neonatal hearing screening 100
What are the economic considerations?
The purpose of economic evaluation is to assist decision-makers in ensuring that society’s ultimately scarce resources are allocated to those activities from which it will get the most value. That is, it seeks to enhance economic efficiency.
The aim of this economic evaluation has been to systematically review the evidence for the costs and effectiveness of a nationwide universal neonatal screening program for permanent childhood hearing impairment (PCHI) compared to the alternative, no universal screening program, under Australian conditions. This information was synthesised in terms of the best current estimates, with an indication of the extent of uncertainty entailed.
The perspective for the present evaluation was that of Australian society overall. Cost data covered all resources directly used in establishing and implementing the screening program. Costs were estimated for the screening program, for subsequent diagnostic investigations and treatments, and for the longer term implications for patients and their families and were reported in 2003 Australian dollars. Only the literature review for UNHS has been updated to 2007. The original 2003 economic analysis has not been revised. Both short-term and long-term health outcomes were considered.
Quality of relevant economic evaluations
The quality of the economic evaluations of universal neonatal hearing screening (UNHS) identified in the literature search was assessed according to a checklist previously developed by the National Health and Medical Research Council (Appendix E). Quality was expressed in terms of its internal validity as a score out of 10 (which is an attribute of the original study design). The external validity, or generalisability (which depends on the setting), was expressed as a score out of 6. Description of the evaluated studies and their resulting quality scores can be found in Appendix F.
Unit costs
Possible costs of universal neonatal screening for permanent childhood hearing impairment
Notional costings of UNHS were calculated using a costing model derived from a template developed by the Medical Services Advisory Committee (MSAC 2000).
Developers of established screening programs such as the Western Australian UNHS program were consulted to assist with the identification of all non-trivial costs associated with creating a screening program. Costs of implementing a program can be evaluated for two possible treatment pathways. Present information suggests that either automated auditory brainstem response (AABR) or otoacoustic emissions (OAE) tests can be used in the initial screening in either a one- or two-stage process (Figure 2). Neonates who fail the first test are either referred directly for medical assessment (1-stage) or are tested again with either AABR or OAE (2-stage). Both of these pathways are explored in this report.

Universal neonatal hearing screening 101
ICER = increment in cost increment in effectiveness
= cost of UNHS – cost of not universal screening health outcome from UNHS – health outcome from no universal screening program
The costs of items of service reported for a given year from other countries were first expressed in Australian dollars for the same year using Purchasing Power Parity calculations developed by the Organisation for Economic Cooperation and Development (OECD) (OECD 2003). Conversion to Australian dollars for the first half of 2003 was done using the Consumer Price Index (CPI) (ABS 2004).
Reporting of the economic evaluation
The results were expressed in terms of the incremental cost-effectiveness ratio (ICER), which was calculated as shown below:
The health outcomes of interest are both short- and long-term. The primary short-term outcomes are the cases of permanent childhood hearing impairment (PCHI) identified and the cases of PCHI treated (viz when hearing aids are fitted or cochlear devices implanted). From these outcomes the following incremental cost-effectiveness ratios were reported:
• cost per case of PCHI identified
• cost per case of PCHI treated.
Where provided in the identified literature, the process measure of cost per infant screened was also reported.
The long-term outcomes of interest relate to language and social development, quality of life, education level and employability. The achievement of satisfactory long-term outcomes may require the allocation of resources to community services and educational support.

Universal neonatal hearing screening 102
Relevant cost items
When evaluating the cost-effectiveness of a program from a societal perspective, direct costs must be included from three key areas (Drummond et al 1997) and indirect costs must also be assessed:
Direct costs
1) Health care sector
Health care sector costs of implementing a universal neonatal hearing screening (UNHS) program would include: the purchase of screening equipment (AABR and OAE technology); consumables; the training and deployment of personnel for screening, diagnostics and administration; and the cost of follow-up diagnostic assessment (Bailey et al 2002).
2) Patient and family
Costs to patient and family of permanent childhood hearing impairment (PCHI) could be travel costs and time off work.
3) Other sectors
Non-medical costs that may be incurred by the identification of children with hearing impairment would be special education and rehabilitation (Mohr et al 2000).
The relevant direct costs of a neonatal hearing screening program are itemised in Table 19.
Indirect costs
The loss to society of the productivity of persons who are unable, or are limited in their capacity, to work.

Universal neonatal hearing screening 103
Table 16 Relevant resource items for a neonatal hearing screening program
Universal screening Targeted screening Resource items 2-stage OAE and
AABR 2-stage AABR 1-stage AABR
Capital equipment OAE instrument n/a n/a AABR instrument Computer
Recurrent items OAE probes n/a n/a ABR electrodes n/a OAE probe tips n/a n/a Ear couplers/muffins n/a Cables Machine calibration Other consumables (eg paper) Screener training Overheads
Personnel Nurse Audiologist Administrative support
Follow-up Patient and family
Other sectors AABR = automated auditory brainstem response test; OAE = otoacoustic emissions; = relevant; n/a = not applicable.
Reported economic evaluations
A systematic and comprehensive literature search identified all published economic analyses of the effectiveness of universal neonatal hearing screening (UNHS) up until 2003. Relevant papers were retrieved and subjected to critical appraisal, and bibliographies were searched for additional pertinent literature. For a detailed analysis of each of these studies see Appendix F.
Comparison of universal and targeted screening in the short term
Two studies determined that UNHS would, in the short term, be more expensive and less cost-effective to operate than a targeted screening program. Disparity in the incremental cost-effectiveness ratio between these two studies, for incremental cost per case identified, appears to stem from the different referral rates used to determine the costs of follow-up diagnostic assessment. In the study by Kemper and Downs (2000) the assumed difference in referral rates from universal, as opposed to targeted, hearing screening programs was much smaller than that assumed by Keren et al (2002). With similar assumed differences in referral rates, the overall cost of diagnostic follow-up for each of the programs presented by Kemper and Downs (2000) would be closer, reducing the incremental cost.

Universal neonatal hearing screening 104
Comparison of modelled universal neonatal hearing screening programs in the short term
In three modelled evaluations of UNHS protocols two- or three-stage otoacoustic emissions (OAE) screening, along with two-stage OAE and automated auditory brainstem response (AABR) screening, were recognised as the most cost-effective methods in the short term for identifying permanent childhood hearing impairment (PCHI). Differences in cost per child identified are substantial between studies, although costs per child screened are similar (Boshuizen et al 2001; Kezirian et al 2001). This could only be due to differences in referral rates and/or costs assumed for diagnostic testing, neither of which can be compared from the information published. This is based on evidence obtained prior to 2003.
Comparison of existing universal neonatal hearing screening programs in the short term
From studies of existing UNHS protocols, the cost per child screened including follow-up was quite variable (Table F, Appendix C). Two-stage protocols ranged from $25 to $80 per child screened while one-stage protocols ranged from $29 to $46 per child screened. Estimates of the cost per child identified were similarly varied, ranging from $6,700 to $23,000 for two-stage screening programs, and from $20,000 to $32,000 for one-stage protocols.
In the only study comparing one-stage transient evoked otoacoustic emissions (TEOAE) or AABR with two-stage TEOAE–AABR hearing screening, the cost per child screened and cost per child identified with PCHI were roughly equivalent (Vohr et al 2001). In a single study comparing two-stage OAE with two-stage AABR, the latter was considered more cost-effective because referral rates were lower, despite the initial higher cost outlay for AABR equipment (Lemons et al 2002).
Two included studies presented cost per child screened estimates that were substantially lower than for comparable studies examined in this evaluation. In the one-stage TEOAE study by Driscoll (Driscoll et al 2000) the screened sample were drawn from volunteer walk-in subjects to a child health clinic (CHC). Cost per child screened here was noticeably lower ($13), probably due to the higher prevalence of hearing impairment in this population, since concerned parents are more likely to attend the CHC with their child than parents of seemingly healthy infants. Similarly, the cost of using a two-stage TEOAE protocol for screening was determined to be only $11 per child screened before the costs of diagnostic assessment (Weirather et al 1997). In this study, however, the initial purchase cost of screening equipment was not included.
On the basis of this evidence, it is difficult to recommend any one protocol for UNHS.
Comparison of universal and targeted screening in the long term
Only one study attempted to model the cost-effectiveness of UNHS over the long term and from a societal perspective (Keren et al 2002). A hypothetical cohort of 80,000 newborns from one US state was used, consisting of 10,400 high-risk and 69,600 low-risk infants. Under targeted screening, only infants with identified risk factors for congenital deafness were screened. Analysis resulted in an incremental saving of $2 million per child with normal language using targeted screening compared to having no screening program, and a further saving of $1.2 million per child using UNHS. Modelling of long-

Universal neonatal hearing screening 105
Overall summary of published economic evaluation studies of neonatal hearing screening
With the exception of two studies, all identified published research examining the cost-effectiveness of existing or modelled universal neonatal hearing screening (UNHS) programs are from an American perspective. In the only study from Australia, the study design did not reflect the optimal conditions for a universal screening program, as the participation was voluntary. Therefore, due to differences in costs and the structure of the US medical system, the results obtained from the majority of the literature can be only suggestive of what might occur under Australian conditions.
Short-term costs and benefits
From the literature it can be concluded that, in the short term, costs for the additional cases identified and diagnosed by UNHS are greater per unit than those of targeted screening. However, it is inappropriate to determine incremental cost-effectiveness without considering long-term costs and cost savings. Further, modelled two-stage UNHS protocols appear to be more cost-effective than modelled one-stage protocols, but this observation is not supported by reports of existing UNHS programs using either one- or two-stage screening protocols. Therefore, based on the available evidence, no determination of the most cost-effective protocol for UNHS can be made.
Long-term costs and benefits
While it was established earlier in this report that UNHS would be more expensive to operate than a targeted screening program, taking a societal perspective over the long term suggests that identifying a larger proportion of hearing impaired infants at an early stage (ie ≤6 months of age) would result in an overall cost-effective program. However, these societal costs are based primarily on observation and expert opinion and have not been generated from properly designed studies.
term costs by Keren et al (2002) suggested that identifying a larger proportion of hearing-impaired infants at an early stage (ie ≤6 months of age) would result in savings in other sectors (such as education and social welfare) that would far outweigh the initial expense.

Universal neonatal hearing screening 106
Economic model
Decision analytic modelling can assist the policy making process by simulating the cost-effectiveness of a program of universal neonatal hearing screening (UNHS) for permanent childhood hearing impairment (PCHI) for Australia, compared to the current situation where there is no universal screening program.
In 2003, targeted neonatal hearing screening was limited in Australia, and only New South Wales approximated a statewide UNHS program. Depending on the health service, PCHI was usually identified at various stages in an infant’s development (Figure 5)§.
Figure 5 2003 timeline of identification of PCHI in Australia in the absence of a UNHS program**
in NICUtested
when "risk factors" identifiedtested
parental concerntest_0_to_5_years
community nurse follow-uptest_0_to_5_years
school entrytest_at_5_years
after discharge from birthing hospital
all newborns
test between 0 and 5 years
test between 0 and 5 years
test between 0 and 5 years
The varied situation across Australia poses a question as to the most appropriate comparator against which to estimate the incremental cost-effectiveness ratio for UNHS. Two comparators are available: no formal screening program and a targeted screening program (ie identification of potential cases on the basis of risk factors alone, and including both formal and informal identification methods).
Therefore, the use of decision analytic modelling was explored to simulate the following decisions:
1. The respective costs, cost savings (in both the short and long term) and yield of UNHS compared to no screening or targeted screening.
2. If a universal screening program was adopted, which two-stage protocol, AABR–AABR or OAE–AABR, is the most cost-effective?
§ It is noted that a few infants may acquire their hearing loss after birth but during the neonatal hospital stay, and still others will develop an acquired hearing loss after discharge.
** ‘Risk factors’ may be identified through either case finding or a formal screening program.

Universal neonatal hearing screening 107
Short-term ICER = additional costs of universal screening and diagnostic follow-up number of additional infants with PCHI identified by universal screening Long-term costs / costs of universal screening and diagnostic follow-up cost savings = minus savings on educational/rehabilitation services and productivity gain
The model was designed to calculate the incremental cost per additional case of PCHI diagnosed by the age of 6 months, the result allowing calculation of the incremental cost per additional person with normal language. The definitions of these ratios are:
Possible hearing testing programs for neonates
Three possible scenarios for a neonatal hearing screening program that a health authority might provide are described in Figure 6:
1) no formal screening program: individual infants identified by clinical case finding.
2) a targeted program where newborns identified with a risk factor for permanent childhood hearing impairment (PCHI) and thus deemed at increased risk of PCHI (Box 7) would be tested by a one-stage screening protocol, progressing directly to a diagnostic evaluation if they fail the test. In this program infants with PCHI but without recognised risk factors would only be exposed by case finding
Box 7 Established risk factors for targeted neonatal hearing screening
Residence in neonatal intensive care unit / special care baby unit for ≥48 hours Prolonged usage (>7 days) of aminoglycosides Family history of permanent childhood deafness Craniofacial abnormality noticeable at birth Perinatal infection (either suspected or confirmed), eg toxoplasmosis, rubella, cytomegalovirus, herpes or acquired meningitis Birthweight <1.5 kilograms Birth asphyxia Chromosomal abnormality, including Down syndrome (Trisomy 21) Exchange transfusion or intrauterine transfusion, eg hyperbilirubinaemia Intracranial haemorrhage

Universal neonatal hearing screening 108
3) a universal neonatal hearing screening (UNHS) program in which all babies are screened. This implies that all babies will enter a UNHS program but will follow a protocol dependent on the identification of risk factors for PCHI (including residence in the neonatal intensive care unit (NICU)). Infants with identified risk factors would be screened using the one-stage protocol as above, while infants not identified as having risk factors (‘well babies’) would still be tested, but using a two-stage screening protocol.
Figure 6 Options for neonatal hearing screening programs
no screening programcase_finding
NICUone_stage
other risk factorsone_stage
identified at risk
well babiescase_finding
targeted
NICUone_stage
other risk factorsone_stage
identified at risk
well babiestwo_stage
universal
screening program
all newborns
case finding
case finding
one stage screening
one stage screening
one stage screening
one stage screening
two stage screening
However, determining the costs involved in any formal neonatal hearing screening program is complicated by the need for screening facilities to be available in different locations, even within the same health service, in order to assure the complete coverage of all births (Table 17). Having identified that there will be different costs for hospitals in rural and remote regions, the costs for the urban setting have been calculated. It is acknowledged that screening in rural and remote settings is likely to be more costly due to diseconomies of scale and to parental costs of transporting a child to a diagnostic facility.

Universal neonatal hearing screening 109
Table 17 Region-dependent design of UNHS program
Urban region Birth location Infant designation Screening protocol used Screening location a
Tertiary hospital NICU 1-stage AABR H Identified at risk 1-stage AABR H Well babies 2-stage OAE or AABR–AABR H or H/C Lost to first screen (eg early
discharge)b 2-stage OAE or AABR–AABR C or H or H/C
Community hospital
Well babies 2-stage OAE or AABR–AABR H or H/C
Identified at risk 1-stage AABR H Lost to first screen 2-stage OAE or AABR–AABR C or H or H/C
Rural and remote region Regional hospital Well babies 2-stage OAE or AABR–AABR H or H/C Identified at risk 1-stage AABR H Lost to first screen 2-stage OAE or AABR–AABR C or H or H/C Community hospital
Well babies 2-stage OAE or AABR–AABR H or H/C
Identified at risk 1-stage AABR H Lost to first screen 2-stage OAE or AABR–AABR C or H or H/C a H = hospital, C = community, H/C = 1st stage in hospital but 2nd stage performed in community. b It is assumed that those ‘lost to first screen’ would be tracked by screening personnel and followed up with testing in the community or as outpatients at the local hospital. NICU = neonatal intensive care unit; AABR = automated auditory brainstem response test; OAE = otoacoustic emissions test.
Short-term costs
Short-term costs are those incurred in the identification of unilateral permanent childhood hearing impairment by the age of 6 months. Calculations are based on a hypothetical birth cohort of 4,000 births per annum. This number is typical of the annual number of births recorded for a tertiary birthing hospital.
Individual resource costs are summarised in Table 18. At least two commercial quotations were obtained for each item of capital equipment in 2003, and in each instance a clinically useful life of 5 years accorded with the manufacturer’s estimate. The equivalent annual cost was calculated according to the annuity method (Drummond et al 1997).

Universal neonatal hearing screening 110
Table 18 Identification of 2003 unit costs for neonatal hearing screening††
Resource item Cost ($A) Range ($A) Manufacturer Capital items
Algo 3i portable AABR 19,380 Natus Accuscreen AABR 14,943 14,943–15,781 Madsen
ABaer AABR 19,500 Biologic ECHOCHECK portable TEOAE 6,350 Medtel
Accuscreen TE/DPOAE 12,088 12,088–13,229 Madsen Accuscreen OAE/AABR 19,207 19,207–23,974 Madsen
ABaer OAE/AABR 29,900 Biologic Recurrent costs – consumables
Probe (AABR/OAE, Accuscreen) 1,545 Madsen Probe (AABR/OAE, ABaer) 1,246 Biologic Probe tips (AABR, ABaer) 3 Biologic
Probe tips (AABR, Accuscreen) 1 1–2 Madsen Couplers or muffins (AABR, Algo 3i) 17 Natus Couplers or muffins (AABR, ABaer) 16 Biologic
Electrode (AABR, ABaer)/infant 3 Biologic Electrode (AABR, Algo 3i)/infant 5 Natus
Electrode (AABR, Accuscreen)/infant 6 Madsen Probe (OAE, ECHOCHECK) 688 Medtel
Probe tips (OAE, ECHOCHECK) 1 1–2 Medtel Resource item Cost ($A)a Range ($A) Time (minutes/infant) Recurrent costs – wages including on costs ($/hr)
Coordinator 25 9 Clerk 14 4
Screener 17 35 Audiologist 24 4
Diagnostic evaluation/infant 170b a Unless otherwise stated, recurrent costs obtained from the Western Australia universal neonatal hearing screening project; b determined by addition of MBS items # 11300, 11332, 11330, 11327. AABR = automated auditory brainstem response test; OAE = otoacoustic emissions test; DPOAE = distortion product otoacoustic emissions test; TEOAE = transient evoked otoacoustic emissions test.
The costs of automated auditory brainstem response tests
Capital equipment
For the purpose of this analysis it is assumed that one machine is required for every 2,000 infants screened per annum‡‡. In Australia, in 2003, the purchase price of an
†† The capital items recorded in this table are indicative only of what is used in Australia but does not include all available products.
‡‡ It is recognised that some hospitals may already have sufficient machines in place and therefore the cost of targeted screening for some hospitals in the initial years will be nearer that calculated for the recurrent cost items. On the other hand, in rural and remote regions, distance may preclude the sharing of machines

Universal neonatal hearing screening 111
automated auditory brainstem response (AABR) machine was $17,950. With an expected clinically useful lifetime of 5 years, the equivalent annual cost was $4,150 (annuity method).
Presently, AABR technology allows for the use of either probe tips or ear couplers to deliver the stimulus. If the option of using probe tips is chosen, then the 2003 purchase price of one probe capable of both otoacoustic emissions (OAE) and AABR testing was $1,400. Assuming a 5-year lifetime, each probe had an equivalent annual cost of $325.
Consumables
One probe tip with one set of electrodes was $7 per infant screened (Table 18).
No probe is required when using ear couplers. One ear coupler with one set of electrodes was $21 per infant screened.
The costs of otoacoustic emissions tests
Capital equipment
Again it is assumed that one machine is required for every 2,000 infants screened per year. Based on two quotes of single function (ie transient evoked otoacoustic emissions (TEOAE) or distortion product otoacoustic emissions (DPOAE) only) the average purchase price of a single OAE machine in 2003 was $7,000. With an expected clinically useful lifetime of 5 years for each machine, the equivalent annual cost of one OAE machine was $1,625. Equipment is available that can perform both TEOAE and DPOAE at almost twice the purchase price (Table 18).
One probe for OAE measurements was $688 (Table 18). Assuming a 5-year clinically useful lifetime, each probe had an equivalent annual cost of $159.
Consumables
One tip per screen was $1.00.
Screener salary
From the Western Australian UNHS project it was estimated that the average time taken per screen was 0.6 hours. The hourly salary of a designated screener was reported to be $17 (nursing staff would receive much higher remuneration) and therefore the cost for the screener’s time would be $10 per screen.
Diagnostic follow-up
The cost to the MBS of one diagnostic follow-up appointment is $170 per infant. This was calculated from the combined benefits charged for four diagnostic tests (see Box 8).
between hospitals; in this situation a greater number of machines may be required unless this can be offset by a mobile screening service (which will incur travel costs).

Universal neonatal hearing screening 112
Box 8 MBS items for diagnostic assessment in paediatric audiometry
MBS # 11300 Brainstem evoked response audiometry. Fee $156.05, Benefit $117.05
MBS #11332 Otoacoustic emissions audiometry for the detection of permanent congenital hearing impairment performed by, or on behalf of a specialist or consultant physician, on an infant who is at risk due to one or more of the following factors:
admission to a neonatal intensive care unit family history of hearing impairment intrauterine or perinatal infection (either suspected or confirmed) birthweight less than 1.5 kg craniofacial deformity birth asphyxia chromosomal abnormality, including Down syndrome exchange transfusion,
where the patient is referred by another medical practitioner, and where middle ear pathology has been excluded by specialist opinion.
Fee $47.45, Benefit $35.60 MBS #11330 Impedance audiogram where the patient is not referred by a medical practitioner – one examination in any 4-week period.
Fee $6.40, Benefit $4.80 MBS #11327 Impedance audiogram involving tympanometry and measurement of static compliance and acoustic reflex performed by, or on behalf of, a specialist in the practice of his or her specialty, where the patient is referred by a medical practitioner – being a service associated with a service to which item 11309, 1132, 11315 or 11318 applies. Fee $16.00, Benefit $12.00

Universal neonatal hearing screening 113
Summary: Cost of no formal screening program
With no formal screening method, it would cost a maximum of $30,000 per 4,000 newborns per year for one child with permanent childhood hearing impairment to be identified before 6 months of age. In a total population of 250,000 newborns per annum throughout Australia, 68 children would be identified by 6 months of age, at a total 2003 cost of $1,870,000 per annum.
Cost-effectiveness of screening protocols
No screening protocol (case finding)
In an Australian study by Russ and colleagues (2002) using a screening questionnaire to identify risk factors for permanent childhood hearing impairment (PCHI), 4.4 per cent of a birth cohort of 64,116 infants in 1993 were referred for diagnostic assessment. Seventeen of 120 infants, later confirmed with PCHI were identified before the age of 6 months. Out of the total birth cohort, the yield was 0.3/1,000 infants. Therefore, if no screening protocol was implemented it was assumed that this rate would be even lower. Using the above referral rate and yield as a maximum in a hypothetical birth cohort of 4,000, 176 infants would be referred for audiologic assessment and only one child per year would be identified with PCHI before 6 months of age. (Russ et al 2002)
Targeted neonatal hearing screening
In a program of targeted neonatal hearing screening, only infants with recognised risk factors would be directed to a hearing test. Ideally this would occur prior to the discharge of the infant from hospital. Figure 7 describes the decision analytic model for determining the short-term costs and effectiveness of a targeted program of hearing screening in neonates (ie based on risk factors for PCHI being identified prior to hospital discharge).
Figure 7 Decision model for targeted hearing screening§§
PCHI (case finding)
no PCHIno identified risk factors
PCHI
no PCHIdx evaluation
lost to dx evaluation
fail
pass
tested AABR
lost to test
identified at risk or in NICU
all newborns
§§ Case finding assumes that any neonates with PCHI may be discovered through parental concern, health visitor testing or testing at school entry.

Universal neonatal hearing screening 114
This model acknowledges that some newborns at high risk of PCHI may go unidentified and therefore screening would not be performed prior to discharge. Further, this model also recognises that a percentage of infants who have no risk factors for PCHI would have congenital hearing loss.
In the absence of a full systematic review to determine the best available transition probabilities for targeted screening protocols, a search of PubMed, Embase and the MSAC’s existing literature database was performed to identify any studies that used automated acoustic brainstem response (AABR) on an identified ‘at-risk’ population.
Present technology allows for the use of AABR with either probe tips similar to those used for otoacoustic emissions (OAE) testing or the traditional ear couplers (or muffins). For the purposes of this model, this distinction is not assumed to result in different yields; however, it will affect both the cost per child screened and the cost per child identified. Using transition probabilities from Table 20 and costs of resource items from Table 18, the short-term outcomes cost per child screened and the cost per child identified by 6 months of age were calculated as follows:
Yield of targeted screening protocol (one-stage AABR)
In a cohort of 4,000 newborns it would be expected that 8.1 per cent, or 342 infants, at risk of PCHI (Kennedy et al 1998) would be identified and 314 infants (coverage 97%) (Barsky Firkser & Sun 1997) would be screened. This would result in a yield of six (5.7) infants with unilateral or bilateral PCHI identified before 6 months of age, or 1.5/1,000 infants.
In the remainder of the birth cohort it is assumed that those infants otherwise identified by case finding would be identified by the screening method as they are assumed to be the most obvious cases at risk of PCHI. Therefore, no infants in the remainder of the cohort would be identified using a case finding protocol.
However, from the cohort of 4,000 infants, 14 will be lost either to initial testing (10) or to diagnostic evaluation (4). Assuming that they would have failed testing at the same probability as those that were tested, it would be expected that less than one of those lost to initial testing would have PCHI, but that two of the four lost to diagnostic follow-up would eventually be diagnosed for PCHI. However, for the purposes of this model, it is assumed that these infants would not be identified by 6 months of age.
Program management costs for one-stage AABR and follow-up
In the absence of any available costing studies on one-stage AABR followed by diagnostic assessment, costs of administrative support per child screened were determined from individual reported data from the Western Australian UNHS project. It is assumed that one full-time program coordinator would be required for enrolment and tracking of any sized program up to 12,000 prospective neonates per year at an annual 2003 reported salary of $60,840 including on-costs. Assistance for data entry was estimated at $1.20 per infant or $4,800 per year for a cohort of 4,000 infants in 2003.
Incremental cost of targeted screening
Therefore, from a birth cohort of 4,000 infants per year, the incremental cost of screening 320 infants identified as at risk of PCHI using a targeted screening program (1-

Universal neonatal hearing screening 115
stage AABR) is shown in Table 19. Eleven infants are referred on to diagnostic assessment using this protocol.
Table 19 2003 cost of targeted screening by method of AABR delivery for a cohort of 4,000 infants per year
Cost per method of AABR delivery ($A) Item Probe tips Couplers
Capital AABR 4,150 4,150 Probe 325 n/a
Consumables AABR probe tips plus electrodes (@ $7 per screen) 2,240 n/a AABR couplers plus electrodes (@ $21 per screen) n/a 6,720
Screeners’ time (@ $10 per screen) 3,200 3,200 Administrative support
Program coordinator (1 FTE) 60,840 60,840 Data entry 4,800 4,800
Diagnostic assessment 1,870 1,870
Total cost 77,425 81,580 Cost per child screened 242 255 n/a = not applicable; AABR = automated auditory brainstem response test; FTE = full time equivalent.

Universal neonatal hearing screening 116
Summary: cost of a targeted screening program
A yield of six infants with permanent childhood hearing impairment before 6 months of age is obtained from a birth cohort of 4,000 per year, using a targeted screening program at a total 2003 cost of approximately $79,500 per year and a cost per infant screened of approximately $249.
Table 20 Transitional probabilities for an Australian targeted screening program
Transition Base case probability
Source for base case
Justification for selection
Range for sensitivity analysis
Source for range
Protocol 1-stage AABR Percentage at risk 0.081 Kennedy et al
1998 Only study including all identified at risk
n/a
Probability screened 0.970 0.970–1.000 Probability lost to screen
0.030 Barsky-Firkser & Sun 1997
Only study that described coverage 0.000–0.030
Barsky-Firkser & Sun 1997
If screened: probability initial screen positive
0.048
0.048–0.210
probability initial screen negative
0.952
Mason & Herrmann 1998
Unilateral PCHI, AABR threshold of 35 dB HL in NICU population
0.790–0.952
Mason & Herrmann
1998; McClelland et al 1992; Norton et
al 2000 If screen positive:
probability receive diagnostic follow-up
0.730
probability lost to diagnostic follow-up
0.270
McClelland et al 1992
Unilateral PCHI, ABR threshold of 30 dB HL in SCBU
If followed up diagnostically:
probability diagnosed PCHI
0.516
probability diagnosed not PCHI
0.484
McClelland et al 1992
Unilateral PCHI, ABR threshold of 30 dB HL in SCBU
AABR = automated auditory brainstem response test; PCHI = permanent childhood hearing impairment; NICU = neonatal intensive care unit; dB = decibels; HL = hearing loss; SCBU = special care baby unit.

Universal neonatal hearing screening 117
Universal neonatal hearing screening
In a program of universal neonatal hearing screening (UNHS) all newborns are directed to hearing testing through one of two pathways (Figure 8). As in targeted screening programs, all newborns identified as having one of the risk factors indicated in Box 7 undergo one-stage automated acoustic brainstem response (AABR) testing and follow up with diagnostic evaluation in the event of a failure. As distinct from targeted screening, UNHS generally directs all other newborns, designated as ‘well’, through a two-stage testing procedure of either AABR–AABR or otoacoustic emissions (OAE)–AABR testing followed by diagnostic evaluation.
Yield of universal screening protocol (two-stage AABR–AABR or OAE–AABR)
Based on transition probabilities presented in Table 21 and Table 22 UNHS on a cohort of 4,000 infants per annum would identify:
• six (5.7) infants with unilateral or bilateral permanent childhood hearing impairment (PCHI) before 6 months of age using risk factors as an indicator for one-stage AABR screening; and
• five (5.2) infants with unilateral or bilateral PCHI by 6 months of age using two-stage AABR, or seven (6.7) infants using two-stage OAE–AABR in the ‘well’ baby population.
This gives a total prevalence of unilateral and bilateral PCHI in this cohort of 2.7– 3.1/1,000.
Program management costs
The 2003 costs for administrative support were calculated by first assuming that the cohort would require a full-time program coordinator at a cost of $60,840 (source: Western Australian UNHS project). This cost was included in a total cost of $93,584 for managing a UNHS program of 12,530 births per year, leaving a total cost of other administration items of $32,744. This value was divided by the number of infants managed in the Western Australian UNHS project, giving a cost of $2.60 per infant or $10,400 per cohort of 4,000 infants (Table 23) in 2003.

Universal neonatal hearing screening 118
Figure 8 Decision model for universal neonatal hearing screening
lost to test
pass
lost to dx
no PCHI
PCHIdx test
fail (dx test)
test
identified at risk (AABR)
lost to test
pass
lost to test
pass
lost to dx
no PCHI
PCHIdx test
fail (dx test)
test
fail (AABR)
test
AABR
lost to test
pass
lost to test
pass
lost to dx
no PCHI
PCHIdx test
fail (dx test)
test
fail (AABR)
test
OAE
all others "well babies"
all newborns

Universal neonatal hearing screening 119
Table 21 Transitional probabilities for an Australian UNHS program (protocol A)
Transition Base case probability
Source for base case
Justification for selection
Range for sensitivity analysis
Source for range
UNHS protocol A: 2-stage TEOAE–AABR Probability screened 0.950 0.831–0.962 Probability lost to screen
0.050 Expert opinion based on: Bailey et al 2002; Hunter et al 1994
The mid-point of coverage rates cited by two hospital-based studies (one Australian) with TEOAE–AABR screen protocols
0.169–0.038 Bailey et al 2002;
Hunter et al 1994; Kennedy
et al 1998
If screened: probability initial screen positive
0.134
0.043–0.197
probability initial screen negative
0.866
Bantock & Croxson 1998; Daemers et al 1996; McPherson et al 1998; Owen et al 2001
Mean initial TEOAE screen failure rate of all four studies utilising TEOAE as a 1st-stage screen on well babies only and reporting unilateral and bilateral fail criteria
0.957–0.803
Bantock & Croxson 1998; Daemers et al
1996; McPherson et al 1998; Owen et al
2001
If initial screen positive:
probability rescreened
0.800
0.749–0.817
probability lost to rescreen
0.200
Expert opinion based on: Daemers et al 1996; Molini et al 2001
The mid-point of LTFU rates cited by two hospital-based studies utilising TEOAE as a 1st-stage screen on well babies only 0.251–0.183
Daemers et al 1996; Molini et al
2001
If rescreened: probability rescreen positive
0.037
0.016–0.050
probability rescreen negative
0.963
Bailey et al 2002 Australian metropolitan hospital-based study with TEOAE–AABR screen protocol. Relevant for local conditionsa
0.984–0.950
Expert opinion based on: Bailey
et al 2002; Hunter et al 1994
If rescreen positive: probability receive diagnostic follow-up
0.933
0.721–1.000
probability lost to diagnostic follow-up
0.067
Clemens et al 2000
Hospital-based study on well babies only with unilateral fail criteria and information on 2nd-stage AABR failures 0.279–0.000
LTFU for diagnostic testing from a 2nd-stage AABR referral:
Bailey et al 2002; Cox & Toro
2001; Clemens et al 2000; Hunter et al
1994; Oudesluys-Murphy &
Harlaar 1997; Yoshida et al
2002

Universal neonatal hearing screening 120
Table 21 (cont.) Transitional probabilities for an Australian UNHS program (protocol A)
Transition Base case probability
Source for base case
Justification for selection
Range for sensitivity analysis
Source for range
If followed up diagnostically:
probability diagnosed PCHIb
0.521
0.400–0.600
probability diagnosed not PCHI
0.478
Bailey et al 2002 Australian metropolitan hospital-based study with TEOAE–AABR screen protocol. Relevant for local conditionsa 0.600–0.400
Expert opinion – 10% variation each
side of point estimate
If initial screen negative:
probability diagnosed PCHI
0.000
0.000–0.500
probability diagnosed not PCHI
1.000
Smyth et al 1999; McNellis & Klein 1997
Both studies on well babies determined that false negatives on TEOAE as a first screen are negligible if the screen is implemented under quiet (ideal) conditions
0.990–0.970
Smyth et al 1999; McNellis & Klein 1997; Jacobson & Jacobson 1994 Large variation in false negatives when include study where screening occurred with normal ambient noise
If rescreen negative: probability diagnosed PCHI
0.001
0.000–0.020 probability diagnosed not PCHI
0.999
Expert opinion
Assumption that rate of false negatives is not negligible, based on: Schauseil-Zipf & Von Wedel 1988. 1.000–0.980
Expert opinion based on: Schauseil-Zipf & Von Wedel 1988
If lost to diagnostic follow-up
probability diagnosed PCHI
0.050
0.030–0.070
probability diagnosed not PCHI
0.950
Expert opinion
Child is unlikely to be tested elsewhere and receive confirmation of PCHI within 6 months.
0.970–0.930
Expert opinion
TEOAE = transient evoked otoacoustic emissions test; AABR = automated auditory brainstem response test; LTFU = lost to follow-up. a A limitation of using this source is that the study population included both well and at-risk babies – however, there are no studies available that used this screen protocol on well babies alone; b assumption that this is diagnosis <6 months of age.

Universal neonatal hearing screening 121
Table 22 Transitional probabilities for an Australian UNHS program (protocol B)
Transition Base case probability
Source for base case
Justification for selection
Range for sensitivity analysis
Source for range
UNHS protocol B: 2-stage AABR–AABR Probability screened 0.985 0.788–1.000 Probability lost to screen
0.015 Clemens et al 2000 Hospital-based study
on well babies only with unilateral fail criteria and AABR–AABR screen protocol
0.212–0.000 Expert opinion
based on: Clemens et al
2000; Bretschneider
et al 2001; Mason & Herrmann
1998; Oudesluys-Murphy &
Harlaar 1997; Rao et al 2002; Yoshida et al
2002 If screened:
probability initial screen positive
0.021
0.006–0.130
probability initial screen negative
0.979
Clemens et al 2000 Hospital-based study on well babies only with unilateral fail criteria and AABR–AABR screen protocol 0.994–0.870
Clemens et al 2000; Mason &
Herrmann 1998;
Oudesluys-Murphy &
Harlaar 1997; Yoshida et al
2002 If initial screen positive:
probability rescreened
0.830
0.703–1.000
probability lost to rescreen
0.170
Clemens et al 2000 Hospital-based study on well babies only with unilateral fail criteria and AABR–AABR screen protocol
0.297–0.000
Clemens et al 2000;
Oudesluys-Murphy &
Harlaar 1997; Yoshida et al
2002 If rescreened:
probability rescreen positive
0.146
0.000–0.189
probability rescreen negative
0.854
Clemens et al 2000 Hospital-based study on well babies only with unilateral fail criteria and AABR–AABR screen protocol 1.000–0.811
Clemens et al 2000;
Oudesluys-Murphy &
Harlaar 1997; Yoshida et al
2002 If rescreen positive:
probability receive diagnostic follow-up
0.933
0.721–1.000
probability lost to diagnostic follow-up
0.067
Clemens et al 2000 Hospital-based study on well babies only with unilateral fail criteria and AABR–AABR screen protocol
0.279–0.000
LTFU for diagnostic
testing from a 2nd-stage
AABR referral: Bailey et al
2002; Cox & Toro 2001;
Clemens et al 2000; Hunter et al 1994; Oudesluys-Murphy &
Harlaar 1997; Yoshida et al
2002

Universal neonatal hearing screening 122
Table 22 (cont.) Transitional probabilities for an Australian UNHS program (protocol B)
Transition Base case probability
Source for base case
Justification for selection
Range for sensitivity analysis
Source for range
If followed up diagnostically:
probability diagnosed PCHI
0.600
0.500–0.700
probability not diagnosed PCHI
0.400
Clemens et al 2000 Hospital-based study on well babies only with unilateral fail criteria and AABR–AABR screen protocol
0.500–0.300
Expert opinion – 10% variation each side of point estimate
If initial screen negative: probability diagnosed PCHI
0.001
0.000–0.020 probability diagnosed not PCHI
0.999
Expert opinion
Assumption that rate of false negatives is not negligible based on: Schauseil-Zipf & Von Wedel 1988. 1.000–0.980
Expert opinion based on: Schauseil-Zipf & Von Wedel 1988
If rescreen negative: probability diagnosed PCHI
0.001
0.000–0.020
probability diagnosed not PCHI
0.999
Expert opinion
Assumption that rate of false negatives is not negligible based on: Schauseil-Zipf & Von Wedel 1988. 1.000–0.980
Expert opinion based on: Schauseil-Zipf & Von Wedel 1988
If lost to diagnostic follow-up:
probability diagnosed PCHI
0.050
0.030–0.070
probability diagnosed not PCHI
0.950
Expert opinion
Child is unlikely to be tested elsewhere and receive confirmation of PCHI within 6 months.
0.970–0.930
Expert opinion
AABR = automated auditory brainstem response test; PCHI = permanent childhood hearing impairment.
Cost of universal screening
In determining the cost-effectiveness of universal screening, several assumptions have been made. For an annual birth cohort of 4,000 infants in 2003, it was assumed that two AABR machines and two OAE (if the OAE–AABR option were used) units would be required.
Further, the cost of UNHS compared to no screening involves the inclusion of the targeted screening arm for those infants identified to be ‘at risk’ of PCHI. This value was extracted from Table 23 and the administration support costs were subtracted as they were already accounted for in the ‘well baby’ arm. This provides an added cost of $11,785 using probe tips for one-stage AABR and $15,940 using couplers.

Universal neonatal hearing screening 123
Summary: cost of universal neonatal hearing screening
A yield of 11–12 infants with unilateral or bilateral permanent childhood hearing impairment identified before 6 months of age is obtained from this cohort using universal screening at a total cost of $136,000 to $203,000 per year. The cost is dependent on the two-stage screening method used – automated auditory brainstem response (AABR)–AABR or otoacoustic emissions (OAE)–AABR – and the type of AABR method used (probe tips or couplers). The 2003 cost per infant screened ranged from $36 to $52.
Table 23 Incremental cost of UNHS by choice of 2-stage screening method
Cost per method of 2-stage delivery ($A) Item AABR–AABR OAE–AABR
Well babies only Probe tips Couplers Probe tips Couplers Capital
AABR 4,150 4,150 4,150 4,150 AABR probe 325 n/a 325 n/a
OAE n/a n/a 1,625 1,625 OAE probe n/a n/a 159 159
Consumables 1st stage
AABR probe tips plus electrodes (@ $7 per screen) 25,347 n/a n/a n/a AABR couplers plus electrodes (@ $21 per screen) n/a 76,041 n/a n/a
OAE probe tips (@ $1 per screen) n/a n/a 3,492 3,492 Screeners’ time (@ $10 per screen) 36,210 36,210 34,920 34,920
2nd stage AABR probe tips plus electrodes (@ $7 per screen) 441 n/a 2,618 n/a AABR couplers plus electrodes (@ $21 per screen) n/a 1,323 n/a 7,854
Screeners’ time (@ $10 per screen) 630 630 3,740 3,740 Administrative support
Program coordinator (1 FTE) 60,840 60,840 60,840 60,840 Other administrative costs 10,400 10,400 10,400 10,400
Diagnostic assessment 1,530 1,530 2,210 2,210 Well babies only
Total cost 139,873 191,124 124,479 129,390 Cost per child screened 39 53 36 37
At-risk infants only (from Table 22) Total cost 11,785 15,940 11,875 15,940
All infants in universal screening protocol Total cost 151,658 202,909 136,264 145,330 Cost per child screened 39 52 36 38 n/a = not applicable; AABR = automated auditory brainstem response test; OAE = otoacoustic emissions test; FTE = full time equivalent.

Universal neonatal hearing screening 124
Incremental cost-effectiveness ratios
Table 24 summarises total yields and the 2003 cost for each of the three screening options, and Table 25 reports the incremental cost-effectiveness ratio (ICER).
Table 24 Summary cost-effectiveness of three screening options for PCHI in a birth cohort of 4,000 infants per year
Screening option Number screened
Number referred
Yield 2003 cost/child screened ($A)
Total program cost ($A)
No screening 0 176a 1.1 0 30,000 Targeted screening 314 11 5.7
probe tips 244 77,400 couplers 255 81,600
UNHS 2-stage OAE–AABR 3,806 24 12.4
probe tips 36 136,300 couplers 38 145,300
2-stage AABR 3,935 20 10.8 probe tips 39 151,700
couplers 52 202,900 a based on referral rate in study by Russ (Russ et al 2002). AABR = automated auditory brainstem response test; OAE = otoacoustic emissions test; UNHS = universal neonatal hearing screening.
Table 25 ICER of three screening options for PCHI in a birth cohort of 4,000 infants per year
Screening option comparison ICER (incremental cost per extra child identified in 2003 $AUD)
UNHS v no screening 2-stage OAE–AABR
2nd stage AABR using probe tips 9,300 2nd stage AABR using couplers 10,100
2-stage AABR 1st and 2nd stage AABR using probe tips 12,500
1st and 2nd stage AABR using couplers 17,600 UNHS v targeted screening 2-stage OAE–AABR
2nd stage AABR using probe tips 8,800 2nd stage AABR using couplers 9,500
2-stage AABR 1st and 2nd stage AABR using probe tips 14,600
1st and 2nd stage AABR using couplers 23,800 AABR = automated auditory brainstem response test; OAE = otoacoustic emissions test; UNHS = universal neonatal hearing screening.

Universal neonatal hearing screening 125
Summary: Cost-effectiveness of universal neonatal hearing screening for permanent childhood hearing impairment
In the absence of any screening program for a birth cohort of 4,000 infants per year, clinical case finding will identify one neonate with permanent childhood hearing impairment (PCHI) before 6 months of age, at a total 2003 cost of $30,000. Dependent upon the type of acoustic apparatus (probe tips or couplers) used in association with automated auditory brainstem response (AABR), employment of a universal screening protocol will identify an extra 10–11 infants with unilateral or bilateral PCHI before 6 months of age in this cohort, at an incremental cost of $9,000 to $17,600 per infant. Compared to targeted screening, universal neonatal hearing screening (UNHS) would identify an additional 5–7 infants with unilateral or bilateral PCHI before 6 months of age in this cohort. The incremental cost of UNHS compared to targeted screening would be $8,800 per additional infant identified using two-stage otoacoustic emissions (OAE)–AABR, and from $14,600 to $23,800 using two-stage AABR–AABR, dependent on the use of probe tips or couplers with AABR.
Long-term costs
After infants with permanent childhood hearing impairment (PCHI) have been identified, it is considered best practice to implement both hearing amplification and rehabilitation as soon as possible, followed where indicated by cochlear implantation after the age of 12 months. For the purpose of this analysis, long-term is defined as the remainder of the life-span following diagnosis of PCHI. Clinical anecdote and level III-2 evidence suggests that infants diagnosed by 6 months of age will develop normal language skills if interventions are implemented immediately, while those identified after 6 months will have some form of language skill deficit compared to their normal hearing peers. The following estimates are for the incremental long-term costs and cost savings if a universal neonatal hearing screening (UNHS) program were to be implemented in an environment where previously there was no organised screening program.
Assuming a national birth cohort of 250,000 infants per annum, adopting a UNHS program Australia-wide in an environment where there was previously no organised screening program would result in an incremental annual yield of 607 infants (2-stage automated acoustic brainstem response (AABR)) with unilateral or bilateral hearing impairment.
Studies of the long-term cost of hearing impairment
Little published literature is available that describes the long-term costs and benefits of early intervention in infants with PCHI. Three studies have attempted to determine the long-term costs of deafness (Downs 1994; Mohr et al 2000; Weinrich 1972).
Three decades ago Weinrich (1972) used census data and educational statistics to estimate that the economic costs of deafness amounted to the equivalent in 2003 Australian dollars of more than $410,000 per person with hearing impairment over the life of the person. This value was based only on the expected loss of lifetime earnings due to the reduced probability of a hearing-impaired child reaching various educational milestones. This information suggests that deaf infants lag behind their hearing peers

Universal neonatal hearing screening 126
educationally, fail more often to continue with their education, and graduate from school and enter the work force at a later age.
Downs (1994) described more recent data showing that deaf members of American society earned on average 30 per cent less than their hearing peers. Information from the Internal Revenue Service indicated that 24 per cent of deaf college graduates reported no income and that hearing-impaired secondary school graduates have twice the rate of unemployment of the national average. The report argued that this disparity is due in part to poorer language skills of deaf persons compared to their hearing peers. For example, the average reading level of 15-year-old normal hearing students corresponded to school Year 10, whereas their deaf peers had an average reading level at Year 3.
In a recent study the societal costs of severe to profound hearing loss were estimated in a US population (Mohr et al 2000). This report estimated that the lifetime financial cost to society, for each individual with prelingual onset of severe to profound hearing loss, would be the equivalent in 2003 Australian dollars of over $1.5 million. Both direct and indirect costs were included in this estimate. Direct medical costs covered diagnosis, intervention (eg hearing aids) and periodic medical evaluations. Direct non-medical costs included education and rehabilitation services (such as speech and language pathology). The costs due to loss of productivity were also considered.
The study revealed that the largest component of cost (67%) that would be borne by society due to severe to profound hearing loss would be the resulting loss in productivity due to reduced language skills. The second largest cost to society (21%) was identified as the consumption of special education resources that would be provided in an effort to improve language skills. Finally, medical costs made up 11 per cent of the total cost to society, with over half of this related to hearing aid use. However, this report does not include moderately impaired individuals who may also experience some reduction in language ability, require some form of social support such as education, and be at some risk of lower productivity.
No Australian-published literature on the long-term costs of hearing impairment was retrieved. Therefore, in order to estimate the associated long-term costs, stakeholders in the fields of therapy and rehabilitation for childhood hearing impairment were contacted. Table 28 is a summary of their cost estimates.
2003 costs of hearing treatment
It was assumed that, irrespective of whether the diagnosis of PCHI is made before or after 6 months of age, infants will receive treatment such as hearing aids or cochlear implants and will undergo some form of rehabilitation until the age of school entry. The incremental cost of treatment of screened, compared to not screened, infants was calculated on the basis of the difference between the earliest age for hearing aid fitting (3 months) and the average age at which hearing impairment is identified in the absence of a UNHS program (21 months).
Information provided by Australian Hearing estimates that a hearing aid costs approximately $125 plus $48 for four ear moulds per hearing aid in the first year (Australian Hearing 2001) (Table 26). This treatment is provided by Australian Hearing, with Commonwealth Government funding, free of charge at the point of service.

Universal neonatal hearing screening 127
Assessment, fitting and aftercare costs were based on Australian Hearing estimates of 27 hours of service by an audiologist over a 15-month period from month 3 to 18 (the point where most infants with PCHI join the Australian Hearing program). Distributed evenly over the period, this results in 16 hours in the first year and 11 hours in the second (Table 26). Cost per hour for audiologist services was estimated at $32 (Western Australian UNHS project).
Therefore, the total 2003 cost in the first year for hearing aids and moulds would be $173 per ear. Audiologist time for hearing assessment, fitting and aftercare would be approximately $512 per child in the first year and $352 in the second year (Table 26).
Direct costs and cost savings to other sectors
Where costs will differ substantially is upon entry to school. For the purposes of this evaluation, it is assumed that infants identified with PCHI by 6 months of age and receiving immediate intervention and rehabilitation will develop language skills equivalent to their hearing peers. This assumption, based on expert opinion because no definitive evidence yet exists, is revisited in a threshold analysis (see Table 28). Therefore, in the best case analysis it is assumed that when these infants enter mainstream classrooms they will require no special education interventions. Those infants identified with PCHI after 6 months of age will have some greater degree of impairment in language skills compared to their hearing peers and therefore will require some form of special education. It is acknowledged that infants with limited cognitive ability will incur other costs irrespective of the time of diagnosis of PCHI, but these costs will not be changed by UNHS.

Universal neonatal hearing screening 128
Table 26 Resources used (in 2003 $AUD) in therapy, rehabilitation and education of infants with PCHI to 18 years of age (or school Year 12)
Resource item Unit cost ($A)
# sessions per year
Cost per year ($A)
Source
Therapy Hearing aid
Prosthesis 125a Australian Hearing Assessment, fitting and aftercare 1st year 512 MSAC estimate
Assessment, fitting and aftercare 2nd year 352 MSAC estimate Ear moulds 12 Australian Hearing
Maintenance and overheads @ 30% MSAC estimate Cochlear implant
Surgical procedure, hospitalisation and prosthesis 22,984 AR-DRG D01Z
Rehabilitation To age 5 years
Individual therapy session (per session) 90 45 Cora Barclay Centre Parent–infant program group session (per session) 90 45 Cora Barclay Centre
Parent guidance individual session (per session) 45 40 Cora Barclay Centre Unilateral hearing impairment program (per session)b 90 15 Cora Barclay Centre From school entry to Year 12 Hearing specialist support for mainstream students:
Profound hearing impairment (per session) 120 80 Cora Barclay Centre Severe hearing impairment (per session) 120 40 Cora Barclay Centre
Moderate hearing impairment (per session) 120 20 Cora Barclay Centre Mild hearing impairment (per session) 120 5 Cora Barclay Centre
Unilateral hearing impairment (per session)c 120 4 Cora Barclay Centre Incremental school budget increase per student
with hearing impairmentd
Reception to Year 2 19,769 DECS Years 3 to 7 20,315 DECS
Years 8 to 10 18,747 DECS Years 11 to 12 18,070 DECS
a Based on an estimated cost of $62,500 for an extra 500 hearing aids(Australian Hearing 2001); b infants with unilateral hearing impairment require fewer sessions per year and only attend the parent–infant program (15 sessions per year are assumed); c infants with unilateral hearing impairment require fewer specialist sessions per year (approximately 4; d costs of extra teaching and capital resources. AR-DRG = Australian Refined Diagnosis Related Groups (from the Australian Department of Health and Ageing), The Cora Barclay Centre for deaf and hearing impaired, South Australia; DECS = South Australian Department of Education & Children’s Services.
Rehabilitation costs (identification to age 5)
Based on information provided by Australian Hearing, in 2003, the average age of hearing aid fitting was 18 months (Australian Hearing 2001). It is expected that universal screening will bring forward the time to hearing aid fitting to an average of 3 months of age. Therefore, it is assumed that rehabilitation will also start 15 months earlier than is presently occurring. The costs of rehabilitation of infants with unilateral or bilateral hearing impairment before or after 6 months of age (ie with or without a UNHS program) are shown in Table 27.

Universal neonatal hearing screening 129
Education cost savings (age 5 to school Year 12)
The current educational approach to children with permanent hearing impairment is direct therapist intervention, with additional assistance to the classroom teachers. Upon entering mainstream school, the child identified before the age of 6 months would incur no extra educational costs in a best case scenario. The child identified with bilateral PCHI later than 6 months of age (assumed to have some language skill deficit) would require an extra $217,000 in hearing specialist and extra teaching support costs up to Year 12 (see Table 27). Where the hearing impairment is unilateral, later identified infants require fewer rehabilitation sessions and do not require extra teaching resources, thus generating 2003 costs of an extra $4,700 up to Year 12, compared to their peers who are identified early.
In a worst case scenario children identified before the age of 6 months would still require some specialist support during their school career but to a lesser degree. Expert opinion suggests that for a moderately impaired infant, a maximum of 20 visits per year would be required from Reception to Year 2, 10 visits per year for Years 3–9, and only four visits per year for Years 10–12. In such a case the cost per child of specialist support (discounted at 5%), from Reception to Year 12, would amount to approximately $11,000, and to an overall incremental cost in hearing specialist and extra teaching support of $206,000 for infants identified with bilateral PCHI later than 6 months of age.

Universal neonatal hearing screening 130
Table 27 2003 cost (discounted @ 5% p.a.) of extra rehabilitation and education per child with bilateral PCHI dependent on age of identification and whether unilateral or bilateral: best case scenario
Resource item Cost per year ($A)
Cost to Year 12 ($A) Age of identification and unilateral/bilateral
Unilateral ≤6 months
Unilateral >6 monthsa
Bilateral ≤6 months
Bilateral >6 monthsa
Rehabilitation To age 5 years
Therapy 4,050 n/a n/a 18,400 12,400 Parent–infant program 4,050 n/a n/a 18,400 12,400
Parent guidance 1,800 n/a n/a 8,200 5,500 Unilateral parent–infant program 1,350 6,140 4,100 n/a n/a
Total 6,140 4,100 45,000 30,300 From school entry to Year 12 Hearing specialist support for mainstream students:
Moderate bilateral 2,400 n/a n/a n/a 23,700b
Unilateral 480 n/a 4,700 n/a Education support Incremental school budget increase per student with hearing impairment
Reception to Year 2 19,769 n/a n/a n/a 56,500 Years 3 to 7 20,315 n/a n/a n/a 79,800
Years 8 to 10 18,747 n/a n/a n/a 36,300 Years 11 to 12+ 18,070 n/a n/a n/a 20,600
Total 0 4,700 0 216,900
Total cost of rehab and education 6,140 8,800 45,000 247,200b
n/a = not applicable. a Assuming that the average infant did not start rehabilitation before 18 months of age (ie no costs first year and 1/2 of second year); b total cost based on yearly cost of specialist support for student with moderate hearing impairment (ie $2,400)
Indirect cost savings (beyond school Year 12 or age 18)
Conceptually, the loss of productivity due to late diagnosis could be compared to average weekly full-time adult ordinary time earnings discounted over the working lifespan. This would value the long-term benefits of UNHS by the human capital method. This estimate would depend critically upon the number unemployed as a consequence of the delay in diagnosis of hearing impairment. There is no available Australian estimate of this figure, but Downs in the US (Downs 1994) suggested this to be double the national average unemployment rate. Taking the Australian unemployment figure to be 6 per cent (ABS 2003) and ignoring hidden unemployment, for an annual cohort of 405 bilateral hearing-impaired people, the incremental annual indirect cost would amount to $931.40 x 52 x (0.06 x 405) = $1.18 million. The 2003 value of the indirect costs over the working lifespan (say age 18 to 60) and discounted at 5 per cent per annum would therefore amount to more than $20 million. Even though this is merely a rough estimate, it demonstrates that the potential long-term indirect cost savings from implementing a UNHS program will far outweigh the direct costs.
Given the salience of indirect cost savings in the eventual decision whether or not to implement and continue to support a national UNHS program, it is important that more

Universal neonatal hearing screening 131
valid and accurate estimates of the indirect costs of hearing and language skill impairment be obtained for Australian conditions.
Net long-term savings
Table 28 presents the net savings, with and without indirect savings (due to increased productivity), over the lifetime of one birth cohort of 250,000 infants, of identifying PCHI before 6 months of age using a UNHS program, compared to either a targeted screening program or no formal hearing screening program. These estimates are based on the assumption that no specialist support is required for bilateral hearing-impaired infants identified by 6 months of age and that 100 per cent of these infants would attain normal language skills. When allowance is made for some specialist support for infants with PCHI that are identified early, there is an overall reduction in the net savings by 16 per cent.
Table 28 Summary: Incremental yield and discounted 2003 costs ($million, discounted @ 5% p.a.) for a UNHSa program over the lifetime of an Australian annual birth cohort of 250,000 infants
Items UNHS compared to no organised screening program
UNHS compared to targeted screening
Indirect savings excluded
Indirect savings included
Indirect savings excluded
Indirect savings included
Incremental yield Number of infants diagnosed before
age 6 months 607 607 319 319
Direct costs Screening and diagnosis $7.6 $7.6 $4.7 $4.7
Hearing treatment $0.7 $0.7 $0.4 $0.4 Pre-school rehabilitation $6.3 $6.3 $3.3 $3.3
Total direct costs $14.6 $14.6 $8.4 $8.4 Proportion attaining normal language skills b
100% 100% 100%
100%
Direct savingsb Mainstream school services $89 ($75)c $89 ($75)c $46.7 ($39.3)c $46.7 ($39.3)c
Indirect savings b Productivity n/a $20.6 n/a $10.8
Net savings $74.4 ($60.4)c $95 ($81)c $38.3 ($30.9)c $49.1 ($41.7)c
a Based on the 2-stage AABR protocol; b under the assumption that 100% of children identified by 6 months of age will attain normal language skills (equivalent to their hearing peers); c reduced savings with worst case scenario, n/a = not applicable.
One-way threshold analyses were performed to determine the effect on overall discounted cost savings of variations in the percentage of infants with PCHI attaining normal language skills. Compared to having no formal screening program, running a UNHS program is cost saving until the proportion of infants identified with PCHI by 6 months of age and who attain language skills equivalent to their normal hearing peers, is reduced below 17 percent when direct costs and savings are considered and below 14 per cent with indirect savings included (Table 29). When the comparator is a targeted screening program, this proportion is similarly low – at 18 percent when direct costs and savings are considered and 15 per cent when indirect savings are included.

Universal neonatal hearing screening 132
Table 29 One-way threshold analysis: Incremental yield and discounted 2003 costs ($million, discounted @ 5% p.a.) for a UNHSa program over the lifetime of an Australian annual birth cohort of 250,000 infants
Items UNHS compared to no organised screening program
UNHS compared to targeted screening
Indirect savings excluded
Indirect savings included
Indirect savings excluded
Indirect savings included
Total direct costs $14.6 $8.4 Proportion attaining normal language skills b
100% 16.4% 100% 13.3% 100% 18% 100% 14.6%
Direct savings Mainstream school services $89 $14.6 $89 $11.8 $46.7 $8.4 $46.7 $6.8
Indirect savings b Productivity n/a n/a $20.6 $2.8 n/a n/a $10.8 $1.6
Net savings $74.4 $0 $95 $0 $38.3 $0 $43.1 $0 a Based on the 2-stage AABR protocol; b assuming varying percentages of children identified by 6 months of age will attain normal language skills (equivalent to their hearing peers). n/a = not applicable.
Two-way threshold analysis was performed to assess the concurrent but independent effects of variations in the proportion of infants with PCHI attaining normal language skills and in the proportion of hearing-impaired adults who are unemployed. Compared to having no formal screening program, running a UNHS program is also cost saving for the majority of possible levels of unemployment amongst the hearing impaired (Figure 9).

Universal neonatal hearing screening 133
Figure 9 Two-way threshold analysis: combinations of proportions of hearing-impaired persons who are unemployed and PCHI infants who attain normal language skills, where a UNHS program for an Australian annual birth cohort will be less costly over the lifetime than no organised screening program
Triangles (Δ) represent the threshold between favourable and unfavourable cost outcomes
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
proportion who attain normal language skills
prop
ortio
n of
hea
ring
impa
ired
pers
ons
who
are
un
empl
oyed Favourable (ie
UNHS is less costly than no screening)
Unfavourable
Summary
For universal neonatal hearing screening (UNHS) of an Australian birth cohort, the discounted direct and indirect cost savings over the lifetime far outweigh the costs of the screening program and associated diagnosis (Table 30). Thus, over the long term, a UNHS program will be cost saving for Australian society.
One-way threshold analysis indicates that these cost savings would be realised even if only about 15 per cent of children identified by 6 months of age were to attain a language level equivalent to that of their hearing peers. Two-way threshold analysis found that unemployment rates among people identified with permanent childhood hearing impairment had little negative effect on these cost savings and were robust, except at low levels of unemployment amongst hearing-impaired persons.
Under these circumstances, short-term cost-effectiveness ratios are potentially misleading. The short-term objective should be to maximise yield.
The above conclusions rely on a set of assumptions that are believed to reflect the most likely Australian situation.

Universal neonatal hearing screening 134
Government expenditure
So far, the analysis has taken a societal opportunity cost perspective on screening programs for permanent childhood hearing impairment (PCHI). It is also relevant to consider how the programs will be financed, that is their impact on government expenditure.
Assuming a national birth cohort of 250,000 infants per annum, the resulting expenditures by all levels of government combined for the identification, treatment and rehabilitation of hearing-impaired infants are summarised in Table 32.
Years 1 to 5 – the first five cohorts enter the program
Yield
According to the UNHS decision model, adopting a universal neonatal hearing screening (UNHS) program Australia-wide in an environment where there was previously no organised screening program would result in an incremental annual yield of 607 infants (2-stage automated auditory brainstem response (AABR) testing) with unilateral or bilateral hearing impairment (Table 24). Therefore, at the end of 5 years 3,035 infants with unilateral or bilateral hearing impairment will be receiving treatment and rehabilitation. This is a more conservative estimate than using two-stage otoacoustic emissions (OAE)–AABR testing, where the incremental yield would be 707 infants per annum.
Contributions to expenditure over the first 5 years
Expenditures incurred over the first 5 years of the program have been calculated in constant 2003 dollars and using the lower incremental yield of 607 infants per year with either unilateral or bilateral PCHI.
Screening and diagnosis
The incremental annual expenditure (compared to no screening) of $121,700 for a cohort of 4,000 births (Table 30) extrapolates to an annual expenditure over 250,000 births for screening and diagnosis of $7.6 million. It is anticipated that the screening program would be provided without charge at the point of delivery, and co-payments for diagnosis have been ignored.
Treatment — hearing aids (years 1 to 5)
After identification, infants are assumed to undergo immediate treatment and rehabilitation. Initial treatment involves the fitting of hearing aids. For the purpose of this evaluation, it is assumed that all identified infants (whether unilaterally or bilaterally hearing impaired) are fitted with hearing amplification. Information provided by Australian Hearing estimates that each hearing aid costs approximately $125 plus $48 for ear moulds in the first year (Australian Hearing 2001). This treatment is provided by Australian Hearing, with Commonwealth Government funding, free of charge at the point of service. From Table 8 it is estimated that one-third of the identified cohort (using the lower value of 607 infants per year) with PCHI would have unilateral impairment (202) and the remainder would have bilateral impairment (405). Therefore, total expenditure in the first year for hearing aids and moulds would be $175,000. In the

Universal neonatal hearing screening 135
second year of life the replacement cost of four ear moulds per hearing aid per infant amounts to a total expenditure of $24,000.
Assessment, fitting and aftercare expenditures were based on Australian Hearing estimates of 27 hours of service by an audiologist over a 15-month period from month 3 to 18 (the point where most infants with PCHI join the Australian Hearing program). Distributed evenly over the period, this amounts to 16 hours in the first year of life and 11 hours in the second year (Table 26). The price per hour for audiologist service was estimated at $32 (Western Australian UNHS project). Therefore, the total expenditure on audiologist time for hearing assessment, fitting and aftercare would be approximately $310,000 in the first year and $214,000 in the second year (Table 26), based on the 2003 costs.
Cochlear implants cannot normally be provided until 12 months of age (MBS 2002). It was assumed that this treatment was carried out before 2 years of age and so the time delay for implantation between those infants identified either early or late with PCHI would be small, and the expenditure difference negligible.
Thus, the overall expenditure on treatment with hearing aids would be $485,000 for each incoming cohort and $238,000 in their second year of life (Table 30).
Rehabilitation
Table 32 reports the expenditures on rehabilitation services for infants up to 5 years of age. Combined annual expenditure for therapy, the parent–infant program and parent guidance sessions amounts to $9,900 per child for infants with bilateral impairment and $1,350 for infants with unilateral hearing impairment. Again, it is assumed that an extra 405 infants per year will be identified with bilateral hearing impairment and 202 with unilateral hearing impairment in a birth cohort of 250,000 infants across Australia. Rehabilitation expenditures specific to supporting children with PCHI in mainstream schools are not included, as the initial cohort of children will not have entered school by the fifth year of the expenditure projection. Therefore, the total expenditure per year per cohort for rehabilitation is $4,280,000.
Transfer payments in the first 5 years
People with disabilities are eligible for specific allowances or pensions. For the purposes of this analysis, it is assumed that all carers of children (<16 years) identified with PCHI will be eligible for the Carer Allowance of $88 per fortnight (Table 33). Yearly transfer payments are based on an identified population of 607 infants with unilateral or bilateral hearing impairment.

Universal neonatal hearing screening 136
Table 30 Estimated additional government expenditure (all jurisdictions combined) over the first 8 years of a national program of UNHS (2003 costs in $’000)
Financial year Expenditure items 1 2 3 4 5 6 7 8
Outlays ($’000) Incoming cohort
Screening and diagnosis 7,600 7,600 7,600 7,600 7,600 7,600 7,600 7,600 Treatment (hearing aids) 485 485 485 485 485 485 485 485
Rehabilitation 4,280 4,280 4,280 4,280 4,280 4,280 4,280 4,280 Carer support payments 1,390 1,390 1,390 1,390 1,390 1,390 1,390 1,390
Second year of life Rehabilitation 4,280 4,280 4,280 4,280 4,280 4,280 4,280
Treatment (hearing aid after care) 238 238 238 238 238 238 238 Carer support payments 640 640 640 640 640 640 640
Third year of life Rehabilitation 4,280 4,280 4,280 4,280 4,280 4,280
Fourth year of life Rehabilitation 4,280 4,280 4,280 4,280 4,280
Fifth year of life Rehabilitation 4,280 4,280 4,280 4,280
Total annual outlays 13,755 18,913 23,193 27,473 31,753 31,753 31,753 31,753 Savings on special education ($’000)
Sixth year of life Specialist speech and language support
(moderate impairment) in Reception 1,069 1,069 1,069
Educational support in Reception 8,006 8,006 8,006 Seventh year of life
Specialist speech and language support (moderate impairment) in school Year 1
1,069 1,069
Educational support in school Year 1 8,006 8,006 Eighth year of life
Specialist speech and language support (moderate impairment) in school Year 2
1,069
Educational support in school Year 2 8,006
Total savings on special education 9,075 18,150 27,225 Net expenditures 13,755 18,913 23,193 27,473 31,753 22,678 13,603 4,528

Universal neonatal hearing screening 137
Summary: total expenditure over the first 5 financial years of the program
Under the assumptions mentioned in the text using two-stage automated auditory brainstem response (AABR) testing, the total expenditure of the Commonwealth, State and Territory Governments of Australia combined to identify and care for all infants with unilateral or bilateral permanent childhood hearing impairment (PCHI) over the first 5 financial years following the introduction of a universal neonatal hearing screening (UNHS) program using 2003 costs, is estimated to be $13.8 million in the first year, peaking at $32 million in the fifth year (Table 30).
Operating a UNHS program using two-stage otoacoustic emissions (OAE)–AABR testing, the total expenditure would peak in the fifth year at $35 million (not shown) due to the higher number of infants identified with PCHI.

Universal neonatal hearing screening 138
Years 6 to 18 – the first cohort enters mainstream school
Under the main assumption that all infants with unilateral or bilateral permanent childhood hearing impairment (PCHI) identified by 6 months of age would attain the same language skills as their hearing peers by mainstream school entry, the following expenditures on specialist and educational support would be avoided in the best case scenario. It should be noted that these expenditures are associated with interventions designed to support hearing-impaired students in mainstream schools.
Expert opinion suggests that a worst case scenario would envisage that all PCHI children identified early in infancy would receive some specialist support but to a lesser degree. Under such a situation the net savings for specialist support would decrease by 16 per cent.
Savings
Specialist speech and language support
From Table 30 the type and expenditure savings of this specialist speech and language support would depend on the severity of the hearing impairment. The savings per student with bilateral hearing impairment per year range from $600 for mild impairment to $9,600 for profound impairment. For the purpose of this analysis, the value of $2,400 per year for moderate impairment is used. For each student with unilateral hearing impairment, the yearly savings on specialist support is $480 (undiscounted, Table 30). This amounts to an overall expenditure saving in the first year of $1.1 million (undiscounted). Expenditure savings for severe and profound hearing loss would be higher. When the second cohort enters Reception, the total expenditure saving of eliminating the need for specialist support becomes $2.1 million (undiscounted, Table 32). As the program continues, there will eventually be a maximum of 13 cohorts in school at any one time, providing an expenditure saving for foregone specialist support of $11.4 million per year (undiscounted).
Educational support for students with hearing impairment
As with the specialist speech and language support, it is assumed that infants who are identified with unilateral or bilateral PCHI by 6 months of age would not require educational support. The expenditure savings of educational support vary depending on the grade of the child, and are given as amounts that would be provided normally if the infants did not attain the normal language skills of their hearing peers (Table 28).
From Reception to Year 2 each child with hearing impairment would normally generate an educational expenditure of $19,769 per year. This would result in a total expenditure for the Australian birth cohort of $8 million (undiscounted Table 28). When the second cohort enters Reception and with the first cohort now in Year 1, the total expenditure of educational support becomes over $16 million (undiscounted). With the implementation of a UNHS program, these expenditures would become savings.
Transfer payments over remainder of lifetime
When this cohort reaches the age of 16, the Carer Allowance no longer applies and they may instead become eligible for a disability support pension. For the purposes of this analysis, only those hearing-impaired persons who are unemployed are assumed to be eligible for the maximum pension allowance. Under the assumption that infants

Universal neonatal hearing screening 139
identified for PCHI by 6 months of age will have normal language skills, the unemployment rate of this cohort would be the same as the Australian average. In the absence of a universal screening program, it is assumed that the unemployment rate for the hearing impaired would be double that of the national average (Downs 1994), which in 2003 was about 6 per cent overall (ABS 2003). From an annual national cohort of 607, this would amount to an additional 36 hearing-impaired people being unemployed. This is probably a conservative estimate because the unemployment rate for all people aged under 25 years is much higher than the overall rate; also, the estimate does not account for the income and assets-tested partial payments that would be provided to those persons with PCHI who are in limited employment.
Table 31 Savings on transfer payments per child with unilateral or bilateral hearing impairment
Rate per persona Total annual expenditure for each cohort ($A)b
Savings on transfer payments
Per fortnight
($A)
Per year ($A)
Additional number of persons eligible Identified ≤6
months Identified >6
months
Source
Disability support pension (16–20 years)
398c 10,348 36 373,000 754,000 Centrelink
Disability support pension (>21 years)
453c 11,778 36 424,000 848,000 Centrelink
a These are probably underestimates because the unemployment rate for all people aged under 25 is much higher than the overall rate; b savings per year for cohort of 607 additional children identified with unilateral or bilateral hearing impairment by 6 months of age or after; c maximum rate of disability support pension received per fortnight – income and assets-tested.
Sensitivity analysis for government expenditure
The base case assumption was that all infants identified by 6 months of age would develop normal language skills and would therefore not incur any extra education expenditures over those generated by normal hearing children. By way of a sensitivity analysis, this assumption has been modified to evaluate the effect on government expenditure if a proportion of the children identified by 6 months of age do not achieve a language skill level equal to that of their hearing peers (Figure 10). It should be noted that any effects of reduced language skill acquisition on expenditure would occur in the increased use of special education and in transfer payments.

Universal neonatal hearing screening 140
% normal language = the percentage of a cohort identified by screening who are assumed to have attained normal for age language skills by 5 years of age
One-way sensitivity analysis illustrates that when 100 per cent, 90 per cent or 80 per cent of infants diagnosed with PCHI attain the language skills of their hearing peers, the break-even point (where net expenditures and net savings are equal) occurs between years 8 and 9 after the inception of the program. However, when only 50 per cent of infants attain the language skills of their hearing peers, this break-even point shifts down to year 12 of the program; and when 25 per cent of infants attain the language skills of their hearing peers, the break-even point will not be reached and a net expenditure of $2 million a year will be incurred.
-100
-80
-60
-40
-20
0
20
40
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Year since introduction of UNHS program
$A (i
n m
illio
ns
Net expenditure (100% normal language)90% normal language80% normal language
50% normal language25% normal language
Net
Savings
Net
Outlays
Figure 10 Predicted additional government expenditure/savings for the first 18 years following the introduction of a UNHS program

Universal neonatal hearing screening 141
Summary: Predicted expenditures/savings for the first 18 years following the introduction of a universal neonatal hearing screening program
Commonwealth and State/Territory Governments incur different elements of the overall expenditure on hearing screening and diagnosis, treatment, special education and rehabilitation, and carer and client pensions and benefits. For the first 5 years that the universal neonatal hearing screening program is in operation, government would be expected to incur a net expenditure. Thereafter, savings due to the reduced need for specialist support and education when the cohorts enter mainstream school quickly become realised. By the time the fourth cohort has entered mainstream schooling (year 8 of the program), it is estimated that government would experience a net saving that would increase progressively with each additional cohort. By the time the first cohort has finished Year 12 at school (at age 18 years), government can be expected to benefit from a net saving of $85 million in that year using a two-stage automated auditory brainstem response (AABR) program and $98 million using a two-stage otoacoustic emissions (OAE)–AABR program. These projections rely on a set of strong assumptions whose validity may change over time. The time horizon is 18 years. Once the cohort has entered adulthood, savings on disability support pensions would also be anticipated.

Universal neonatal hearing screening 142
Discussion
Prevalence of permanent childhood hearing impairment
According to the international literature, approximately 0.7–1.8 infants per 1,000 have bilateral permanent childhood hearing impairment (PCHI). The median bilateral prevalence for PCHI of greater than 35 dB HL is 1.3 per 1,000 infants. Unilateral PCHI occurs in 0.2–1.5 infants per 1,000, with a median unilateral prevalence for PCHI greater than 35 dB HL of 0.6 per 1,000 infants.
The heterogeneous nature of prevalence rates in the literature is unremarkable given the different case definitions of PCHI and the varying nature and locations of the sampled populations. Between study heterogeneity may also be related to the different methods in which prevalence was ascertained. Results obtained from universal neonatal hearing screening programs may underestimate the prevalence of PCHI given that newborns are often lost to follow-up between screening and diagnosis stages. In addition, the length of follow-up in these studies is typically not sufficient for false negative cases to be identified. Similarly, prevalence estimates obtained from retrospective examinations of health and/or education records may be subject to bias through the incorrect or incomplete reporting of PCHI cases or errors in abstracting records.
There are no population-based data on the prevalence of congenital PCHI in Australia. Credible estimates, based on the median prevalence data from the international literature, indicate that 325 Australian children are born annually with moderate to profound bilateral PCHI. Unilateral PCHI of similar severity occurs in an additional 156 children born each year. Overall, it is estimated that 481 Australian children are born annually with either unilateral or bilateral moderate to profound PCHI.
Data available from Australian Hearing (2003) indicates that the above estimate is reasonably accurate. Rates of hearing aid fittings for children born in the years 1986 to 1998 ranged from 1.66 to 4.12 per 1,000 (or between 415 and 1,002 children per year). These data are, however, probably an over-estimation due to the inclusion of cases of aided mild hearing loss, and acquired or progressive hearing losses that would not be identified through a universal neonatal hearing screening (UNHS) program. The predicted yield of unilateral and bilateral PCHI from an Australian UNHS program, using two-stage AABR screening, was estimated in this report to be 607 infants. This is higher than the median estimate from the literature but lies within the range of estimates based on Australian Hearing data. It is also clear that early (<6 months of age) identification and management of hearing loss has been steadily improving in Australia over the last 16 years – a likely consequence of improvements in the identification of children at risk of hearing impairment (ie targeted neonatal hearing screening).
Safety of universal neonatal hearing screening
Potential harms from UNHS include the harms from the screening process itself (physical and/or psychosocial), harms from false positives, harms from false reassurance, and harms that may arise from early diagnosis.

Universal neonatal hearing screening 143
No studies were available that reported on physical harm caused by UNHS. Local, transient hypersensitivity reactions to electrode gels are possible but there were no reported cases in the literature and the MSAC Advisory Panel was also not aware of any cases.
The Western Australian neonatal hearing screening program has outlined protocols to minimise cross-infection and possible electrophysical harms with the use of both the automated auditory brainstem response (AABR) and transient evoked otoacoustic emissions (TEOAE) screening equipment (see Appendix H). Other UNHS programs are likely to have developed similar protocols, including the appropriate handling of babies in neonatal intensive care.
A total of ten poor to average quality studies reported on the psychosocial effects of the screening process and of obtaining screening results. Maternal anxiety about the screening process was low across the studies. The screening process itself did not significantly raise anxiety to a higher level than in mothers whose infants were not screened, regardless of whether the infant received a positive or a negative result (level III-2 interventional evidence).
Positive screening status was often associated with an increase in parental anxiety compared to a negative screen (level III-2 interventional evidence), but the anxiety levels reported in the studies were within the normal range, so the differences seen were not deemed to be clinically important. Furthermore, higher levels of knowledge regarding the meaning of a positive test were associated with lower levels of anxiety (level III-2 interventional evidence), so it is hypothesised that if appropriate information is given to the parents of infants undergoing screening, few parents will report moderate to severe anxiety. However, the use of a cross-sectional study designs means that any causal link is unclear. An increase in knowledge regarding the meaning of the test result could decrease anxiety. However, increased anxiety levels may also decrease the ability of the parents to absorb the information about the meaning of test results (leading to lower knowledge).A positive screening result had more effect on the parent if the screen was performed soon after birth, as compared to being screened after 2 months (level III-2 interventional evidence).
When UNHS was compared against a behavioural distraction test (occurring after 6 months of age), no clinically important differences between anxiety levels in mothers of infants who screened positive (level III-2 interventional evidence) were found. However, more satisfaction was expressed in the mothers whose babies were screened by UNHS than the distraction test.
Two studies were inconsistent regarding whether screen status had an impact on the parental attitude to the child, or on the quality of early interactions (level III-2 interventional evidence). However, it is unknown whether the observed reduced quality of early mother-baby interactions was clinically important, as raw scores were not given. The importance of this finding is therefore unclear.
No studies were identified that reported on the psychosocial effects of false reassurance. While the rate of false negatives found in the literature are low (6.5%), the impact of false reassurance should be considered. If a negative screening test delays the diagnosis of hearing impairment, the infant would not received the potential benefits from early intervention.

Universal neonatal hearing screening 144
The consequences of a ‘true positive’ diagnosis of PCHI were not within the scope of this review, but also need to be evaluated. Although most cases are eventually identified, it is possible that an early correct diagnosis of PCHI may lead to increases in maternal or caregiver anxiety in the early postnatal period. This, in turn, may have an impact on the parent–child bonding process and maternal postnatal depression. Possible delays in receiving diagnostic confirmation of PCHI – as part of the screening, rescreening and audiologic battery testing process – and concomitant delays in implementation of rehabilitation or management interventions may also affect the psychological wellbeing of parents.
A B C D Component
Excellent Good Satisfactory Poor
Evidence base level III studies with
low risk of bias, or level I or II studies with moderate risk of bias
Consistency most studies
consistent and inconsistency may be explained
Clinical impact slight or restricted
Generalisability population/s
studied in the body of evidence are similar to the target population
Applicability applicable to
Australian healthcare context with few caveats
Effectiveness
Diagnostic accuracy of the screening tests
Test accuracy is crucial to the successful implementation of any screening program. However, for this assessment there were very few studies that assessed the accuracy of the screening tests at identifying permanent childhood hearing impairment (PCHI) in predominantly healthy infants – the target population in a universal screening situation – compared to an acceptable reference standard. The evidence that was available (level III-1 and III-2 diagnostic evidence) was of average quality.
The accuracy of transient evoked otoacoustic emissions (TEOAE) testing – in a one-stage screen and compared to conventional auditory brainstem response (ABR) testing – appears to depend on the level of local ambient noise, as well as the condition of infant ears at testing. Studies that use a ‘quiet’, although not sound-proofed, environment for testing elicit sensitivity results of up to 100 per cent, although even under the best conditions the rate of false positives can still be quite high (8%).

Universal neonatal hearing screening 145
In one study, testing in association with ‘real world’ ambient noise (ie within the nursery) resulted in low test sensitivity – TEOAE could only accurately detect PCHI in half the infants with the condition. Given the large proportion of infants with PCHI who may not be identified (false negatives) under these ‘real world’ noise conditions, TEOAE testing should only occur in environments that are quiet or even sound-proofed.
The ability of an initial TEOAE screen to positively predict PCHI is very low (1.5%) – meaning that a failure on an initial TEOAE test would accurately predict PCHI for only one or two infants out of 100 identified by the screen as having hearing impairment. This is probably a consequence of the frequency of transient losses in newborns (ear occlusion), as well as the low prevalence of PCHI in the general population.
In terms of identifying conductive hearing loss, TEOAE was found to have 100 per cent sensitivity and specificity, as compared to tympanometry, in a study of infants who had no cerumen occlusion of the ear.
One study of an early model automated auditory brainstem response (AABR) unit was available to assess the ability of the test, in a one-stage screen, to accurately identify PCHI in infants, compared to conventional ABR testing. On the basis of this study, it would appear that the specificity of AABR is particularly good (95.6%) given that its primary use is as a screening tool on a population of predominantly healthy infants. However, the trade-off between sensitivity and specificity means that the test has good, although not excellent, sensitivity at detecting PCHI and thus some false negatives may result. The ability of an initial AABR screen to positively predict PCHI is very low (2.2%), although marginally better than a TEOAE conducted under quiet conditions. Expert opinion indicates that later models of the AABR may have improved diagnostic accuracy although this has yet to be confirmed empirically.
False positives associated with either test could be reduced with the introduction of a second-stage or third-stage screen of initial failures prior to diagnostic testing. This may, however, result in unnecessary caregiver anxiety and added costs and delays in rehabilitation. False negatives are not likely to be identified until the child is older and this false reassurance may further lengthen the time until diagnostic assessment and thus the child’s eventual rehabilitation.

Universal neonatal hearing screening 146
A B C D Component
Excellent Good Satisfactory Poor
Evidence base level III studies with
low risk of bias, or level I or II studies with moderate risk of bias
Consistency most studies
consistent and inconsistency may be explained
Clinical impact Not Applicable
Generalisability population/s
studied in the body of evidence are similar to the target population
Applicability directly applicable to Australian healthcare context
Effectiveness of universal neonatal hearing screening
Impact on referral, diagnosis and management
Altogether, five controlled studies assessed the impact of universal neonatal hearing screening on the clinical management of infants with PCHI. This was assessed in terms of the infants’ age at referral, age at PCHI diagnosis, and age at management. This information was supplemented by 56 uncontrolled, descriptive studies that provided information on screening protocol, coverage, failure rates (referrals), losses to follow-up, false alarms and yield (diagnosis) for the universal screening arm alone.
The best evidence (III-1 screening evidence) available – a quasi-randomised controlled trial in Wessex, UK – indicates that universal neonatal hearing screening has an impact on the clinical management of PCHI. Referrals for diagnostic testing and the diagnosis and management of PCHI commonly occur earlier and more frequently with, as opposed to without, universal neonatal hearing screening.
Level III-1 screening evidence determined that infants who receive universal neonatal hearing screening are nearly three times more likely [RR=2.9, 95%CI 1.4, 6.3] to be referred for diagnostic testing within six months, than infants who are not screened universally. This means that 1,619 infants would need to be universally screened for hearing impairment, as compared to not screened, to ensure the referral of one infant (aged under six months) for diagnostic testing.
Not surprisingly, early referral for diagnosis is believed to be associated with an increase in earlier diagnosis. The evidence suggests that infants born during periods of universal neonatal hearing screening are 2.3 times more likely [RR=2.3, 95%CI 1.1, 4.7] to receive a diagnosis of PCHI, than infants born in periods without universal hearing screening. However, the low prevalence of the condition leads to a small absolute increase in benefit -

Universal neonatal hearing screening 147
with only an extra five children identified per 10,000. Level III-2 screening evidence of good quality determined that children with PCHI were more likely to be diagnosed before the age of six months when born during periods of, or in hospitals with, universal neonatal hearing screening than children who were not exposed to screening programs. The larger of the studies indicated that a diagnosis of bilateral PCHI before the age of six months was 5.1 times more likely to occur in children who were born in hospitals with universal neonatal hearing screening than without screening [[RR=5.1, 95%CI 2.1, 12.4]. This means that for every three children [95%CI 2, 5] with bilateral PCHI born in an Austrian hospital with a screening program, one additional child would be diagnosed with PCHI before the age of six months than if born in a hospital without a screening program.
Level III-1 screening evidence also reported that screening may increase the likelihood of PCHI management before the age of ten months by 2.4 times [RR=2.4, 95%CI 1.0, 5.8]. The absolute increase in benefit over not screening, is early PCHI management (<10 months) for an approximate additional four children in 10,000. In real terms this translates into screening 2,965 children [95%CI 1458, 86207] for hearing impairment, compared to not screening, to ensure the early management (< 10 months) of one infant with PCHI.
Descriptive data indicate that the majority of universal neonatal hearing screening programs manage to screen over 90 per cent of infants in their catchment area. These programs are largely hospital-based with initial screening occurring prior to discharge. Community-based studies obtain good coverage when screening is “piggy-backed” onto other health or immunisation checks at the health clinic or when it occurs in the home. The lowest coverage (45%) was seen in a study conducted in a private hospital in South Africa where patients were not subsidised for the screening service for half of the follow up period. This led to a sudden drop in the population being screened. Coverage, however, does not appear to vary significantly according to the size of the source population being screened, or according to the screening protocol utilised.
Losses to follow-up (LTFU) commonly occur when there is a long delay before re-screening or before diagnostic testing. In one study where there was an immediate re-screen, the 37 per cent LTFU was related to the very early discharge rates from the hospital that was situated in an economically depressed inner-city area. Losses to follow-up could be mitigated to some extent by instituting comprehensive reminder and educational strategies for parents.
Given the low positive predictive value of the AABR and TEOAE screening tests and protocols, the likelihood of having a hearing impairment after failing an initial screen or re-screen is very low. Uncontrolled studies of screening programs suggest that the number of false alarms associated with TEOAE screen protocols is higher (up to approximately 10%) than with AABR screen protocols (up to approximately 6%). It is, however, possible to maintain low false alarm rates using either type of screening protocol.
Impact on adverse outcomes associated with PCHI
There is limited information available on the effect of universal neonatal hearing screening on the adverse, patient-relevant outcomes associated with PCHI. Two good quality studies (level III-2 screening evidence), one of which was small, assessed the impact of screening on language acquisition and communication ability. While both studies were consistent in finding receptive language to be better in children with bilateral PCHI born in hospitals with universal neonatal hearing screening than children with PCHI born in hospitals without screening, it is unclear whether expressive language is also better. Similarly,

Universal neonatal hearing screening 148
conflicting findings were observed for the communicative abilities of children. Based on blinded assessment of the infant seen in one study, as opposed to subjective parental assessment in the other, it appears that some children with bilateral PCHI born in a screening hospital have superior speech intelligibility.
As universal neonatal hearing screening programs were predominantly introduced in the mid- to late-1990s, it is unlikely that information on the longer term, but highly relevant, outcomes (i.e. educational and employment status) will be reported in the peer-reviewed literature for another decade or so.
A B C D Component
Excellent Good Satisfactory Poor
Evidence base
one or two level II studies with low risk of bias or a SR/multiple level III studies with low risk of bias
Consistency some
inconsistency reflecting genuine uncertainty around clinical question
Clinical impact substantial
Generalisability population/s
studied in the body of evidence are similar to the target population
Applicability applicable to
Australian healthcare context with few caveats
Cost-effectiveness of universal neonatal hearing screening
The economic questions are whether the value to Australian society of implementing a universal neonatal hearing screening (UNHS) program is likely to be greater than that of the current situation, and how widespread the screening coverage should be.
The existing situation varied, and the design of a comprehensive screening system that will cover all Australian infants remains to be completed.
Evidence from published economic evaluations
As the majority of identified published research examining the cost-effectiveness of existing or modelled UNHS programs are from an American perspective, the results obtained can only suggest what might occur under Australian conditions.
The published information up until 2003 on the cost-effectiveness of UNHS is limited and at times contradictory. For instance, models of short-term cost-effectiveness are not borne out by evaluations of actual screening programs in the field. Short-term cost-

Universal neonatal hearing screening 149
effectiveness models of two-stage UNHS protocols appear to be more cost-effective than one-stage protocols, but this is not supported by published studies of existing UNHS protocols.
From the literature it can be concluded that, in the short term, costs for the additional cases identified and diagnosed by UNHS are greater per unit than those of targeted screening. However, it is inappropriate to determine incremental cost-effectiveness without considering long-term costs and cost savings.
While it was established that UNHS would be more expensive to operate than a targeted screening program, taking a societal perspective over the long term suggests that identifying a larger proportion of hearing-impaired infants at an early stage (ie ≤6 months of age) would result in cost savings overall. These estimates of long-term cost savings are based primarily on observational data and expert opinion.
Evidence from the economic model
When an experiment is either not ethical or not feasible, or has simply not yet been carried out, decision analytic modelling can provide insight into the relationship between the costs and the outcomes of the intervention. The base case of the model is simulated with the available data thought best to approximate the true situation. Once its structure has been developed, the model can then be run with the variables taking alternative values in order to observe their influence on the decision. Modelling also serves to indicate where the research needs to be targeted to obtain better information.
The model presented here is populated with an annual Australian birth cohort of 250,000 neonates. Using the highest quality and most representative literature available by 2003 and information provided by Australian stakeholders, transition probabilities were identified for estimation of the yields and 2003 costs at the stages of screening, rescreening and diagnostic assessment. These data were used to estimate the expected final yields of bilateral and unilateral hearing-impaired neonates from three scenarios: a UNHS program, a targeted program and no formal screening program (ie case finding).
In the short term this model predicted that implementing a two-stage automated auditory brainstem response (AABR) UNHS program for a cohort of 250,000 newborns would identify an extra 607 infants with unilateral or bilateral hearing impairment by the age of 6 months, compared to no formal screening program, at an incremental cost of $6–$11 million. Where a targeted screening program was already in place, expanding to a UNHS program would identify 319 more infants at an incremental cost of $4–$8 million.
In this modelled UNHS program the cost per infant screened was within the range of values presented in other studies. However, the cost per child identified derived from the model was much lower than that reported in previous studies. This analysis used transition probabilities that encompassed the testing and identification of both unilateral and bilateral hearing impairment in infants and children at all levels of risk, resulting in a higher yield of infants with permanent childhood hearing impairment (PCHI).
The long-term direct cost savings from the reduced need for special education and rehabilitation, and the possibility of indirect savings from enhanced productivity in adulthood, outweigh by an order of magnitude the costs of the actual screening and diagnosis. Unfortunately, these potential savings are less well researched than the short-term costs and so the estimates are more uncertain. Nevertheless, the long-term savings

Universal neonatal hearing screening 150
from implementing a UNHS program derived from this model are in agreement with previous reports.
Regarding screening, increasing the yield of hearing-impaired infants likely to benefit from early intervention will therefore be more efficient than choosing a screening protocol merely because it is more cost-effective per infant diagnosed in the short term – at least while the marginal cost of screening is in the neighbourhood of current figures.
Given the salience of the indirect cost savings in the eventual decision whether or not to implement and to continue to support a national UNHS screening program, it is important that more valid and accurate estimates of the indirect costs of hearing and language skill impairment be obtained for Australian conditions.
These results are influenced by whether or not all infants diagnosed and treated before 6 months of age actually do achieve normal language skills. Cost savings are realised even when only 25 per cent of children identified by 6 months of age attain a language level equivalent to that of their hearing peers. Systematic follow-up of these infants is therefore a high research priority.
The detection and long-term management of PCHI involves public expenditures from both Commonwealth and State/Territory levels of government, and from both health and non-health departments. Over the long term, the States/Territories stand to save on special education and rehabilitation, and the Commonwealth on disability support pensions. These savings would be realised even when less than 50 per cent of children identified by 6 months of age attain a language level equivalent to that of their hearing peers. But to obtain these substantial long-term savings will require expenditure now on implementing a UNHS program and a decision as to how the different levels of government will split the responsibility for the funding.
Overall assessment of universal neonatal hearing screening
Universal neonatal hearing screening has been assessed according to the criteria outlined in Box 2 of the ‘Approach to Assessment’ section of this report. The overall assessment of the viability, effectiveness and appropriateness of a universal neonatal screening program is given in Box 9 below.

Universal neonatal hearing screening 151
Box 9 Criteria for appraising the viability, effectiveness and appropriateness of a screening program (UK National Screening Committee 2000)
The condition Evidence-Based Decision Yes/No/Not applicable/Comment 1.1 The condition should be an important health problem. Yes 1.2 The epidemiology and natural history of the condition, including
development from latent to declared disease, should be adequately understood and there should be a detectable risk factor, or disease marker and a latent period or early symptomatic stage.
Yes
1.3 All the cost-effective primary prevention interventions should have been implemented as far as practicable. Not applicable
The test Evidence-Based Decision Yes/No/Not applicable/Comment 1.4 There should be a simple, safe, precise and validated screening test. Yes but low Positive Predictive
Value 1.5 The distribution of test values in the target population should be known
and a suitable cut-off level defined and agreed. Yes
1.6 The test should be acceptable to the population. Yes 1.7 There should be an agreed policy on the further diagnostic
investigation of individuals with a positive test result and on the choices available to those individuals.
Yes
The treatment Evidence-Based Decision Yes/No/Not applicable/Comment 1.8 There should be an effective treatment or intervention for patients
identified through early detection, with evidence of early treatment leading to better outcomes than late treatment.
Limited evidence
1.9 There should be agreed evidence based policies covering which individuals should be offered treatment and the appropriate treatment to be offered.
No evidence-based data
1.10 Clinical management of the condition and patient outcomes should be optimised by all health care providers prior to participation in a screening program.
Yes
The screening program Evidence-Based Decision Yes/No/Not applicable/Comment 1.11 There must be evidence from high quality Randomised Controlled Trials
that the screening program is effective in reducing mortality or morbidity.
No
1.12 Where screening is aimed solely at providing information to allow the person being screened to make an “informed choice” (e.g. Down syndrome, cystic fibrosis carrier screening), there must be evidence from high quality trials that the test accurately measures risk. The information that is provided about the test and its outcome must be of value and readily understood by the individual being screened.
Not applicable
1.13 There should be evidence that the complete screening program (test, diagnostic procedures, treatment/intervention) is clinically, socially and ethically acceptable to health professionals and the public.
Yes
1.14 The benefit from the screening program should outweigh the physical and psychological harm (caused by the test, diagnostic procedures and treatment).
Insufficient evidence of benefit but no evidence of lasting harm

Universal neonatal hearing screening 152
Box 9 Criteria for appraising the viability, effectiveness and appropriateness of a screening program (UK National Screening Committee 2000)
The screening program (cont.) Evidence-Based Decision Yes/No/Not applicable/Comment 1.15 The opportunity cost of the screening program (including testing,
diagnosis, treatment, administration, training and quality assurance) should be economically balanced in relation to expenditure on medical care as a whole (i.e. value for money).
To be determined
1.16 There must be a plan for managing and monitoring the screening program and an agreed set of quality assurance standards. To be determined
1.17 Adequate staffing and facilities for testing, diagnosis, treatment and program management should be made available prior to the commencement of the screening program.
To be determined
1.18 All other options for managing the condition should have been considered (e.g. improving treatment, providing other services), to ensure that no more cost effective intervention could be introduced or current interventions increased within the resources available.
Assuming evidence of benefit, then considerable potential cost-savings in the long term
1.19 Evidence-based information, explaining the consequence of testing, investigation and treatment, should be made available to potential participants to assist them in making an informed choice.
To be determined
1.20 Public pressure for widening the eligibility criteria, for reducing the screening interval, and for increasing the sensitivity of the testing process, should be anticipated. Decisions about these parameters should be scientifically justifiable to the public.
Not applicable – all babies screened at the earliest possible time

Universal neonatal hearing screening 153
Conclusions
Clinical need
Median estimates from the literature suggest that the prevalence of bilateral and unilateral PCHI >35 dB HL is 1.3 and 0.6 per 1,000 infants respectively. Using this estimate for Australia it is calculated that 481 children may be born with bilateral or unilateral PCHI each year. The predicted yield of unilateral and bilateral PCHI from an Australian UNHS program, using two-stage AABR screening, was estimated in this report to be 607 infants.
Safety
There was no evidence available up until 2007 that reported physical harms from UNHS. Limited poor to average quality studies suggested that there was a slight increase in anxiety and depression in mothers if their infant received a negative screening test, but these states remained within the normal range, and as such no clinically important differences were identified. UNHS was found to cause no more psychosocial distress than a behavioural test given after the infant is 6 months old, but was associated with increased satisfaction levels. Based on the literature available it is therefore concluded that UNHS does not cause psychosocial harm, although no data were found on the harms caused by false reassurance.
Effectiveness
Diagnostic accuracy
Under quiet conditions, TEOAE possesses excellent sensitivity (up to 100%) and good specificity (92%) for diagnosing PCHI. The positive predictive value of TEOAE is poor however at 1.5 per cent. In comparison, AABR has excellent specificity (96%) and good sensitivity (80%). The positive predictive value of AABR is very low (2.2%), although marginally better than TEOAE conducted under quiet conditions.
Screening
While there is a lack of level I and II screening evidence, findings from one good quality level III-1 study suggests that referral for definitive diagnostic testing, actual PCHI diagnosis, and management of PCHI commonly occurs earlier and more frequently with universal neonatal hearing screening (UNHS) than without it. This is supported by level III-2 average and good quality studies.
The effect of universal neonatal hearing screening on primary or patient-relevant outcomes is not readily apparent. Two cohort studies (Level III-2 screening evidence) were available that measured linguistic and communicative abilities quite differently. From the evidence, language acquisition improvements are seen, for receptive language but unclear findings have been reported for expressive language. Similarly, the impact of universal hearing screening on communicative abilities in children are as yet unclear as the two available retrospective cohort studies reported contradictory results.

Universal neonatal hearing screening 154
Economic considerations
From the available literature it can be concluded that, in the short term, the costs for the additional cases identified and diagnosed by UNHS are greater per unit than those of targeted screening. However, taking a societal perspective over the long term suggests that identifying a larger proportion of hearing-impaired infants at an early stage (ie ≤6 months of age) would result in a cost saving overall. The validity of these estimates of long-term cost savings should be regarded with caution as they are based primarily on observational data and expert opinion.
In the short term, the decision analytic model presented in this report predicts that implementing a two-stage automated auditory brainstem response (AABR) universal neonatal hearing screening (UNHS) program for a cohort of 250,000 newborns would identify an extra 607 infants with unilateral or bilateral hearing impairment by the age of 6 months compared to no formal screening program, at an incremental cost of $6–$11 million. Where a targeted screening program is already in place, expanding to a universal screening program would identify 319 more infants, at an incremental cost of $4–$8 million. These figures were reported in 2003 Australian dollars as only the literature review for UNHS has been updated until 2007.
The long-term direct cost savings from the reduced need for special education and rehabilitation and the possibility of indirect savings from enhanced productivity in adulthood outweigh by an order of magnitude the costs of the actual screening and diagnosis. Unfortunately, these potential savings are less well researched than the short-term costs and so the estimates are more uncertain. Nevertheless, the long-term savings from implementing a UNHS program derived from this model are in general agreement with previous reports.
Over the long term, the States/Territories stand to save on special education and rehabilitation, and the Federal Government to save on disability support pensions.
Research implications
Systematic reviews, by their nature, often identify areas in the evidence-base that are deficient or incomplete and that require further research before a definite answer can be ascertained. Areas that would benefit from further research are outlined below:
• Primary research is needed to assess the diagnostic accuracy of screening tools in a healthy ‘well baby’ population, particularly for the automated auditory brainstem response (AABR) test, compared to established reference standards. The diagnostic accuracy of newer models/versions of these screening tests should also be determined.
• Primary research on screen accuracy, especially a determination of the number of false negatives from different types of screening protocols, is required. False negatives should be framed in terms of congenital or perinatal hearing impairment rather than acquired losses.
• Evidence-based research is lacking regarding the identification of effective interventions or methods to ensure adequate follow-up of parents and babies for hearing rescreen or diagnostic appointments.

Universal neonatal hearing screening 155
• Primary research (ie trials) would be of benefit to determine the effect of screening on patient-relevant outcomes associated with moderate to severe bilateral permanent childhood hearing impairment (PCHI). These include the further information on the impact of UNHS on development of speech, language and communication, quality of life and quality of family life including social, emotional and behavioural aspects. These outcome measures should be objectively assessed using valid and reliable tools and blinded to the screening or management status of the infant.
• Primary research, as trials or cohort studies, is needed to assess the effect of screening or early intervention (<6 months of age) on longer term outcomes such as educational performance, employment status and quality of life.
• Primary research (ie trials) would be of benefit to evaluate the effectiveness of management strategies (ie amplification) compared to no management, and of early versus late management, for mild or unilateral hearing losses.
• Agreed evidence-based policies or clinical practice guidelines regarding which individuals should be offered management, as well as the appropriate management to be offered, are currently lacking.
• Primary research would be useful to assess the psychological effects on the caregiver and long-term consequences to the infant of false reassurance (regarding ‘normal’ infant hearing status) given through a UNHS program.
• Primary research to evaluate the psychological effects on the caregiver of an infant receiving a true-positive diagnosis, ascertained through UNHS, would also be of value.
Implementation issues
The available evidence-base also provides insight into how screening interventions should or should not be conducted and what issues need to be addressed. The issues discussed below may assist with the development of universal neonatal hearing screening programs:
• Given the likely low sensitivity of transient evoked otoacoustic emissions (TEOAE) testing under ‘real world’ noise conditions, and the concomitant large proportion of infants with PCHI who may not be identified (false negatives) under these conditions, TEOAE testing should only occur in environments that are quiet or even sound-proofed. [Diagnostic level of evidence: III]
• Given the low positive predictive value of both screening tests, parents of well babies that fail the screen should be counselled in terms of a ‘refer’ for a rescreen or diagnostic testing, rather than as a ‘failed’ test. It should be emphasised that it is considerably more likely (>95% after an initial screen) for the positive test to be a ‘false’ positive rather than a true positive. [Diagnostic level of evidence: III]
• As a consequence of the low positive predictive value of the screening tests, two- or three-stage well baby screening programs should be introduced to improve the predictive value of the result and lessen the burden on diagnostic services. If a one-

Universal neonatal hearing screening 156
stage screen is the only possible option, then the AABR has slightly better predictive value. [Diagnostic level of evidence: III]
• If two- or three-stage programs are introduced, delays between screening, rescreening and diagnostic testing should be minimised wherever possible to reduce parental anxiety and losses to follow-up, and to ensure early management of the condition (assuming early management is more beneficial) and the smooth coordination of services. [Intervention level of evidence: III and IV]
• Outpatient or community-based programs should ensure that neonatal hearing screening is ‘piggy-backed’ onto other health or immunisation checks, in order to ensure good screen coverage. Good coverage can also be obtained if screening is delivered in the home (eg mobile services). This may have particular relevance for rural areas where accessibility and limited resources are often a problem. [Intervention level of evidence: IV]
• Community-based screening programs should ensure comprehensive follow-up of re-screen and diagnostic referrals through reminder and parent education strategies. Hospital-based screening programs should ensure similar strategies are in place for follow-up of outpatient referrals. This is particularly important for programs conducted in economically-depressed areas or with populations that are highly mobile, indigent or non-English speaking. [Intervention level of evidence: IV]

Universal neonatal hearing screening 157
Recommendation
MSAC recommended that on the strength of evidence pertaining to <application name> public funding <should/should not> be supported for this procedure.
- The Minister for Health and Ageing endorsed/did not endorse this recommendation on <date>… -
OR
Since there is currently insufficient evidence pertaining to <application name>, MSAC recommended that public funding should not be supported at this time for this procedure.
- The Minister for Health and Ageing endorsed/did not endorse this recommendation on <date> -

Universal neonatal hearing screening 158
Appendix A MSAC terms of reference and membership
MSAC's terms of reference are to:
• advise the Minister for Health and Ageing on the strength of evidence pertaining to new and emerging medical technologies and procedures in relation to their safety, effectiveness and cost-effectiveness and under what circumstances public funding should be supported;
• advise the Minister for Health and Ageing on which new medical technologies and procedures should be funded on an interim basis to allow data to be assembled to determine their safety, effectiveness and cost-effectiveness;
• advise the Minister for Health and Ageing on references related either to new and/or existing medical technologies and procedures; and
• undertake health technology assessment work referred by the Australian Health Ministers’ Advisory Council (AHMAC) and report its findings to AHMAC.
The membership of MSAC comprises a mix of clinical expertise covering pathology, nuclear medicine, surgery, specialist medicine and general practice, plus clinical epidemiology and clinical trials, health economics, consumers, and health administration and planning:
MSAC membership who evaluated the initial reference (2003)
Member Expertise or affiliation
Dr Stephen Blamey (Chair) general surgery
Associate Professor John Atherton cardiology
Professor Bruce Barraclough general surgery
Professor Syd Bell pathology
Dr Michael Cleary emergency medicine
Dr Paul Craft clinical epidemiology and oncology
Dr Gerry FitzGerald Australian Health Ministers’ Advisory Council representative
Dr Kwun Fong thoracic surgery
Professor Jane Hall health economics
Dr Terri Jackson health economics
Professor Brendon Kearney health administration and planning Associate Professor Richard King internal medicine
Dr Ray Kirk health research
Dr Michael Kitchener nuclear medicine
Dr Ewa Piejko general practice
Ms Sheila Rimmer consumer health issues

Universal neonatal hearing screening 159
Dr Jeffrey Robinson obstetrics and gynaecology
Professor Bryant Stokes neurological surgery
Professor Ken Thomson radiology
Dr Douglas Travis urology
Current MSAC membership (2007)
Member Expertise or Affiliation
Dr Stephen Blamey (Chair) general surgery
Associate Professor John Atherton cardiology
Associate Professor Michael Cleary emergency medicine
Associate Professor Paul Craft clinical epidemiology and oncology
Professor Geoff Farrell gastroenterology
Dr Kwun Fong thoracic medicine
Professor Richard Fox medical oncology
Dr David Gillespie gastroenterology
Dr Bill Glasson ophthalmologist
Professor Jane Hall health economics
Professor John Horvath Chief Medical Officer, Department of Health and Ageing
Associate Professor Terri Jackson health economics
Professor Brendon Kearney health administration and planning
Associate Professor Frederick Khafagi nuclear medicine
Dr Ray Kirk health research
Dr Ewa Piejko general practice
Dr Ian Prosser haematology
Ms Sheila Rimmer consumer health issues
Dr Judy Soper radiology
Professor Ken Thomson radiology
Dr Mary Turner Australian Health Ministers’ Advisory Council representative
Dr David Wood orthopaedics
Mr Peter Woodley Assistant Secretary, Medical Benefits Schedule (MBS) Policy Development Branch, Department of Health and Ageing

Universal neonatal hearing screening 160
Appendix B Advisory Panel, Evaluator and Project Manager
Advisory panel for MSAC reference 17, Universal Neonatal Hearing Screening (2003)
Chair Professor Bryant Stokes AM MBBS, FRACS, FRCS Neurosurgeon Perth, Western Australia
member of MSAC
Evaluators (AHTA) Ms Tracy Merlin, Lead Researcher and Manager Mr Brent Hodgkinson, Research Officer Dr Petra Bywood, Research Officer Ms Fiona Jenner, Research Assistant Mr John Moss, Health Economist Prof Janet Hiller, Director
Panel Members A/Professor Harvey Coates MS (Otol), DABO, FRCS(C) (Otol), FRACS, FACS Senior ENT Surgeon, Princess Margaret Hospital for Children, Perth Clinical A/Professor, School of Paediatrics and Child Health, and School of Surgery and Pathology, University of Western Australia
Co-opted member
Dr Jill Duncan PhD (Applied Linguistics), MEd (Management), MEd (Hearing Impairment), BSci (Speech Pathology and Audiology), CED, Cert AVT Director, Cora Barclay Centre Gilberton, South Australia
Co-opted deaf educator – paediatrics and child health
Professor Jane Hall BA, PhD Director, Centre for Health Economics Research and Evaluation Professor of Health Economics, Faculty of Business, University of Technology, Sydney Honorary Professor, Faculty of Medicine, University of Sydney
MSAC member

Universal neonatal hearing screening 161
Mrs Marion Maurer B Nurs, PG Dip Aud, MAudSA (CCP) Audiologist (ret. 9/2003), Mater Infant Hearing Program Mater Mothers Hospital Brisbane, Queensland
Co-opted audiologist
Mr Daniel McAullay Research coordinator Kulunga Research Network Telethon Institute for Child Health Research Subiaco, Western Australia
Co-opted epidemiologist
Dr Fiona Panizza MBBS(Hons), FRACS, VMO Paediatric Otolaryngologist Mater Children’s Hospital Brisbane, Queensland
Co-opted otorhinolaryngologist
A/Professor Melissa Wake MB ChB, FRACP, MD, Grad Dip Epi Director, Research and Public Health Centre for Community Child Health Royal Children’s Hospital Parkville, Victoria
Co-opted paediatrician
Ms Diane Walsh BA, Dip Ed Member – Governing Committee, Consumer Health Forum Public Member – Medical Board of the Northern Territory
Nominee of the Consumer Health Forum
Evaluators for update of MSAC reference 17, Universal Neonatal Hearing Screening (2007)
Evaluators (AHTA) Ms Tracy Merlin, Lead Researcher and Manager Ms Hedyeh Hedayati, Research Officer Mr Thomas Sullivan, Research Officer Ms Skye Newton, Research Officer Ms Liz Buckley, Research Officer Prof Janet Hiller, Director

Universal neonatal hearing screening 162
Appendix C Search strategies
Bibliographic databases used to identify literature
Electronic database Time Period AustHealth (Informit) 1997 – 08/2007 Australian Medical Index (Informit) 1996 – 08/2007 Australian Public Affairs Information Service (APAIS) – Health (Informit) 1990 – 08/2007 Cinahl (Silverplatter) 1977 – 08/2007 Cochrane Library – including, Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects, the Cochrane Central Register of Controlled Trials (CENTRAL), the Health Technology Assessment Database, the NHS Economic Evaluation Database
1966 – 08/2007
Current Contents Connect (ISI) 1993 – 08/2007 Embase (Embase.com) 1974 – 08/2007 Pre-Medline and Medline (PubMed) 1966 – 08/2007 ProceedingsFirst 1993 – 08/2007 PsycInfo (Silverplatter) 1983 – 08/2007 Web of Science – Science Citation Index Expanded (ISI) 1995 – 08/2007 EconLit 1969 – 08/2007
Other sources of evidence (1966 – 08/2007)
Source Location Internet NHMRC – National Health and Medical Research Council (Australia) http://www.health.gov.au/nhmrc/ Australian Department of Health and Ageing http://www.health.gov.au/ US Department of Health and Human Services (reports and publications) http://www.os.dhhs.gov/ New York Academy of Medicine Grey Literature Report http://www.nyam.org/library/greylit/index.shtml Scirus – for Scientific Information Only http://www.scirus.com Trip database http://www.tripdatabase.com Current Controlled Trials metaRegister http://controlled-trials.com/ Health Technology Assessment International (HTAi) http://www.htai.org/ International Network for Agencies for Health Technology Assessment http://www.inahta.org/ National Library of Medicine Health Services/Technology Assessment Text
http://text.nlm.nih.gov/
National Library of Medicine Locator Plus database http://locatorplus.gov U.K. National Research Register http://www.update-software.com/National/ Websites of Health Technology Agencies See Appendix D Websites of Hearing Organisations See Appendix D Hand searching (journals 2006–2007) American Journal of Otolaryngology Library or electronic access Archives of Otolaryngology – head and neck surgery Library or electronic access Clinical Otolaryngology Library or electronic access Current Opinion in Otolaryngology Library or electronic access Ear and Hearing Library or electronic access Hearing Research Library or electronic access International Journal of Pediatric Otorhinolaryngology Library or electronic access

Universal neonatal hearing screening 163
Journal of Speech, Language and Hearing Research Library or electronic access Journal of the Association for Research in Otolaryngology Library or electronic access The Hearing Journal Library or electronic access The Journal of Otolaryngology Library or electronic access The Otolaryngologic Clinics of North America Library or electronic access Expert clinicians Studies other than those found in regular searches MSAC Advisory Panel Pearling All included articles had their reference lists searched for additional relevant source material
Search terms utilised
All searches MeSH: Neonatology; Infant; Child; Hearing Disorders; Hearing Impaired Persons Text words in title or abstract: neonat*; infant*; baby; child*; hear*; deaf*
Prevalence MeSH: Morbidity; Epidemiologic Studies Text words in title or abstract: frequenc*; proportion*; prevalen*; inciden*; rate Limits: Human; not “heart”; English language; 1980 - Diagnostic accuracy MeSH: Diagnostic Techniques, Otological; Sensitivity and Specificity; Diagnostic Errors; Mass Screening Text words in title or abstract: screen*; test*; universal; sensitiv*, specific*; false negative; false positive; predictive value*; accuracy; likelihood ratio*; AABR; auditory brain stem response*; TEOAE; OAE; oto?acoustic emission* Limits: Human; not “heart”; 1980 - Safety, effectiveness and cost-effectiveness of screening
MeSH: Mass-Screening; Clinical Trials; Epidemiologic Studies Text words in title or abstract: screen*; test*; universal; AABR; auditory brain stem response; TEOAE; OAE; oto?acoustic emission* Limits: Human; not “heart”; 1980 - Safety and effectiveness of early diagnosis
MeSH: Cohort-studies; Incidence; Prognosis; Communication; Language Development Disorders Text words in title or abstract: inciden*; cohort*; registry; register; prognosis; language*; communicat*; speech; referral*; diagnos*; lip?read*; signing; sign language Limits: Human; not “heart” Safety and effectiveness of early management
MeSH: Clinical Trials; Epidemiologic Studies; Hearing Aids; Otologic Surgical Procedures; Rehabilitation of Hearing Impaired;

Universal neonatal hearing screening 164
Language Development; Communication Text words in title or abstract: hearing aid*; cochlear implant*; rehabilitation; intervent*; program*; language*; communicat*; speech Limits: Human; not “heart”

Universal neonatal hearing screening 165
Appendix D Internet sites searched
Websites of health technology assessment groups
AUSTRALIA
• Australian Safety and Efficacy Register of New Interventional Procedures – Surgical (ASERNIP-S) http://www.surgeons.org/open/asernip-s.htm
• Centre for Clinical Effectiveness, Monash University http://www.med.monash.edu.au/healthservices/cce/evidence/
• Health Economics Unit, Monash University http://chpe.buseco.monash.edu.au
AUSTRIA
• Institute of Technology Assessment / HTA unit http://www.oeaw.ac.at/ita/e1-3.htm
CANADA
• Agence d’Evaluation des Technologies et des Modes d’Intervention en Santé (AETMIS) http://www.aetmis.gouv.qc.ca/en/index.htm
• Alberta Heritage Foundation for Medical Research (AHFMR) http://www.ahfmr.ab.ca/publications.html
• Canadian Coordinating Office for Health Technology Assessment (CCDTH) http://www.cadth.ca/index.php/en/media-centre/2003/03/5/38
• Canadian Health Economics Research Association (CHERA/ACRES) – Cabot database http://www.mycabot.ca
• Centre for Health Economics and Policy Analysis (CHEPA), McMaster University http://www.chepa.org
• Centre for Health Services and Policy Research (CHSPR), University of British Columbi http://www.chspr.ubc.ca
• Health Utilities Index (HUI) http://www.fhs.mcmaster.ca/hug/index.htm
• Institute for Clinical and Evaluative Studies (ICES) http://www.ices.on.ca
DENMARK
• Danish Institute for Health Technology Assessment (DIHTA) http://www.dihta.dk/publikationer/index_uk.asp
FINLAND
• FINOHTA http://www.stakes.fi/finohta/e/

Universal neonatal hearing screening 166
FRANCE
• L’Agence Nationale d’Accréditation et d’Evaluation en Santé (ANAES) http://www.anaes.fr/
GERMANY
• German Institute for Medical Documentation and Information (DIMDI) / HTA http://www.dahta.dimdi.de/
• German Scientific Working Group of Technology Assessment http://www.epi.mh-hannover.de/(eng)/hta.html
THE NETHERLANDS
• Health Council of the Netherlands Gezondheidsraad http://www.gr.nl/engels/welcome/frameset.htm
NEW ZEALAND
• New Zealand Health Technology Assessment (NZHTA) http://nzhta.chmeds.ac.nz/
NORWAY
• Norwegian Centre for Health Technology Assessment (SMM) http://www.oslo.sintef.no/smm/Publications/Engsmdrag/FramesetPublications.htm
SPAIN
• Agencia de Evaluación de Tecnologias Sanitarias, Instituto de Salud “Carlos III”I/Health Technology Assessment Agency (AETS) http://www.isciii.es/aets/cdoc.htm
• Catalan Agency for Health Technology Assessment (CAHTA) http://www.aatm.es/cgi-bin/frame.pl/ang/pu.html
SWEDEN
• Swedish Council on Technology Assessment in Health Care (SBU) http://www.sbu.se/admin/index.asp
SWITZERLAND
• Swiss Network on Health Technology Assessment (SNHTA) http://www.snhta.ch/
UNITED KINGDOM
• Health Technology Board for Scotland http://www.htbs.org.uk/
• National Health Service Health Technology Assessment (UK) / National Coordinating Centre for Health Technology Assessment (NCCHTA) http://www.hta.nhsweb.nhs.uk/
• University of York NHS Centre for Reviews and Dissemination (NHS CRD) http://www.york.ac.uk/inst/crd/

Universal neonatal hearing screening 167
• National Institute for Clinical Excellence (NICE) http://www.nice.org.uk/index.htm
UNITED STATES
• Agency for Healthcare Research and Quality (AHRQ) http://www.ahrq.gov/clinic/techix.htm
• Harvard Center for Risk Analysis – Cost-Utility Analysis Database Project http://www.hcra.harvard.edu/tablesdata.html
• U.S. Blue Cross / Blue Shield Association Technology Evaluation Center (TEC) http://www.bcbs.com/consumertec/index.html
• U.S. Dept. of Veterans Affairs Technology Assessment Program (VATAP) http://www.va.gov/resdev/prt/pubs_individual.cfm?webpage=pubs_ta_reports.htm

Universal neonatal hearing screening 168
Websites of relevant hearing organisations
Advanced Hearing Research Center http://ahrc.utdallas.edu/research_labs/pah.html
American Academy of Audiology http://www.audiology.org
American Society for Deaf Children http://www.deafchildren.org
American Society of Pediatric Otolaryngology http://www.aspo.us
American Speech-Language-Hearing Associates http://www.asha.org
Association for Research in Otolaryngology http://www.aro.org
Audiological Society of Australia http://www.audiology.asn.au
Audiology Foundation of America http://www.audfound.org
AudiologyNet http://www.audiologynet.com
Australian Hearing http://www.hearing.com.au
Canadian Hearing Society http://www.chs.ca
Centers for Disease Control and Prevention http://www.cdc.gov/ncbddd/ehdi
Child and Youth Health http://www.cyh.com
Deafness at Birth http://www.deafnessatbirth.org.uk
Defeating Deafness http://www.defeatingdeafness.org
HearingExchange http://www.hearingexchange.com
Hearing Concern http://www.hearingconcern.com
Hearing Review http://www.hearingreview.com
Hear It http://www.hear-it.org
Institute for Hearing Research http://www.ihr.mrc.ac.uk
International Federation of the Hard of Hearing http://www.ifhoh.org
Marion Downs National Center For Infant Hearing http://www.colorado.edu/slhs/mdnc
National Center for Hearing Assessment and Management http://www.infanthearing.org
National Newborn Screening and Genetics Resource Center http://www.genes-r-us.uthscsa.edu

Universal neonatal hearing screening 169
New Zealand Audiological Society http://www.audiology.org.nz
Office of Hearing Services http://www.health.gov.au/hear
Pennsylvania Academy of Audiology http://www.paaudiology.org
Searchwave http://www.searchwave.com
Sound Beginnings http://www.kdhe.state.ks.us/sb
The British Society for Audiology http://www.b-s-a.demon.co.uk

Universal neonatal hearing screening 170
Appendix E Critical appraisal checklists
Randomised controlled trial appraisal checklist
Source: (NHMRC 2000a)
1. Method of treatment assignment
a. Correct, blinded randomisation method described OR randomised, double-blind method stated AND group similarity documented
b. Blinding and randomisation stated but method not described OR suspect technique (eg allocation by drawing from an envelope)
c. Randomisation claimed but not described and investigator not blinded
d. Randomisation not mentioned
2. Control of selection bias after treatment assignment
a. Intention to treat analysis AND full follow-up
b. Intention to treat analysis AND <15% loss to follow-up
c. Analysis by treatment received only OR no mention of withdrawals
d. Analysis by treatment received AND no mention of withdrawals OR more than 15% withdrawals/loss-to-follow-up/post-randomisation exclusions
3. Blinding
a. Blinding of outcome assessor AND patient and care giver
b. Blinding of outcome assessor OR patient and care giver
c. Blinding not done
4. Outcome assessment (if blinding was not possible)
a. All patients had standardised assessment
b. No standardised assessment OR not mentioned
Cohort study appraisal checklist
Source: (NHMRC 2000b)
1. How were subjects selected for the ‘new intervention’?
2. How were subjects selected for the comparison or control group?
3. Does the study adequately control for demographic characteristics, clinical features and other potential confounding variables in the design or analysis?
4. Was the measurement of outcomes unbiased (ie blinded to treatment group and comparable across groups)?
5. Was follow-up long enough for outcomes to occur?
6. Was follow-up complete and were there exclusions from the analysis?
Total /6

Universal neonatal hearing screening 171
Case-control studies appraisal checklist
Source: (NHMRC 2000b)
1. How were subjects selected for the ‘new intervention’?
2. How were subjects selected for the comparison or control group?
3. Does the study adequately control for demographic characteristics, clinical features and other potential confounding variables in the design or analysis?
4. Was the measurement of outcomes unbiased (ie blinded to treatment group and comparable across groups)?
5. Was follow-up long enough for outcomes to occur?
6. Was follow-up complete and were there exclusions from the analysis?
Total /6
Case series appraisal checklist
Source: (NHS Centre for Reviews and Dissemination 2001) Amended for this review (amendments italicised)
1. Is the study based on a representative sample selected from a relevant population? (consecutive and not significantly different than general population of neonates)
2. Are the criteria for inclusion explicit?
3. Did all individuals enter the survey at a similar point in their disease progression? (were the neonates at a similar gestational age)
4. Was follow-up long enough for important events to occur and was follow-up adequate? (greater than 80%)
5. Were outcomes assessed using objective criteria or was blinding used?
Total /5

Universal neonatal hearing screening 172
Diagnostic accuracy study appraisal checklist
Source: (Whiting P 2003)
Item Yes No Unclear 1. Was the spectrum of patients representative of the patients
who will receive the test in practice? ( ) ( ) ( )
2. Were selection criteria clearly described? ( ) ( ) ( )
3. Is the reference standard likely to correctly classify the target condition?
( ) ( ) ( )
4. Is the time period between reference standard and index test short enough to be reasonably sure that the target condition did not change between the two tests?
( ) ( ) ( )
5. Did the whole sample or a random selection of the sample, receive verification using a reference standard of diagnosis?
( ) ( ) ( )
6. Did patients receive the same reference standard regardless of the index test result?
( ) ( ) ( )
7. Was the reference standard independent of the index test (i.e. the index test did not form part of the reference standard)?
( ) ( ) ( )
8. Was the execution of the index test described in sufficient detail to permit replication of the test?
( ) ( ) ( )
9. Was the execution of the reference standard described in sufficient detail to permit its replication?
( ) ( ) ( )
10. Were the index test results interpreted without knowledge of the results of the reference standard?
( ) ( ) ( )
11. Were the reference standard results interpreted without knowledge of the results of the index test?
( ) ( ) ( )
12. Were the same clinical data available when test results were interpreted as would be available when the test is used in practice?
( ) ( ) ( )
13. Were uninterpretable/ intermediate test results reported? ( ) ( ) ( )
14. Were withdrawals from the study explained? ( ) ( ) ( )
Total /14

Universal neonatal hearing screening 173
Checklist for appraising economic evaluation studies
Source: (NHMRC 2001)
Title of assessment:
Title of study:
Author(s):
Year:
Comparators:
Score : /16
Appraisal items for internal validity
1. Was the study question well defined?
2. Were appropriate health care options chosen and clearly described?
3. Was an appropriate study type used?
4. Was the effectiveness of the health care options established?
5. Were the cost estimates related to baseline population risk?
6. Were all the relevant costs and consequences identified for each health care option?
7. Was differential timing considered?
8. Was an incremental analysis performed?
9. Was a sensitivity analysis performed?
10. Were modelling techniques used in a clear and reasonable way?
Criteria for assessing the generalisability of economic evaluation studies
11. Patient group
12. Health system setting
13. Health care option
14. Resource costs
15. Marginal versus average cost
16. Other specific issues

Universal neonatal hearing screening 174
Rank scoring for appraising the clinical importance of benefit/harm
Source: (NHMRC 2000b)
Title of review:
Title of study:
Author(s):
Year:
Comparators:
Clinically important effect:
Rank Score : /4
Ranking
Clinical importance of benefit/harm
1 A clinically important benefit for the full range of plausible estimates. The confidence limit closest to the measure of no effect (the ‘null’) rules out a clinically unimportant effect of the intervention.
2 The point estimate of effect is clinically important BUT the confidence interval includes clinically unimportant effects.
3 The confidence interval does not include any clinically important effects.
4 The range of estimates defined by the confidence interval includes clinically important effects BUT the range of estimates defined by the confidence interval is also compatible with no effect, or a harmful effect.

Universal neonatal hearing screening 175
Rank scoring for classifying the relevance of evidence
Source: (NHMRC 2000b)
Title of review:
Title of study:
Author(s):
Year:
Comparators:
Rank Score : /5
Ranking
Relevance of the evidence
1 Evidence of an effect on patient-relevant clinical outcomes, including benefits and harms, and quality of life and survival.
2 Evidence of an effect on a surrogate outcome that has been shown to be predictive of patient-relevant outcomes for the same intervention.
3 Evidence of an effect on proven surrogate outcomes but for a different intervention.
4 Evidence of an effect on proven surrogate outcomes but for a different intervention and population.
5 Evidence confined to unproven surrogate outcomes.

Universal neonatal hearing screening 176
Appendix F Studies included in the review
Included studies on prevalence of permanent childhood hearing impairment
Study Location Study design Study population Intervention Prevalence Ascertainment via UNHS a – well babies only (Aidan et al 1999)
France Case series – hospital based
1,421/1,727 neonates from the hospital WBN b born between October 1995 and March 1997
1. Initial screen with TEOAE c 2. Rescreen of failures with TEOAE 3. Re-test of failures with audiological assessment
Sensorineural hearing loss >40 dB = 2/1,421
1.41/1,000
Ascertainment via UNHS – well and at-risk babies (Bailey et al 2002)
Perth, Australia
Multi-centre (5) case series
12,708 well and at-risk babies screened in five hospitals from a population of 13,214 born between February 2000 and June 2001
1. Initial screen with TEOAE 2. Rescreen of failures with AABRd 3. Rescreen of failures with TEOAE ± AABR 4. Re-test of failures with diagnostic ABRe
Bilateral PCHI f >35 dB = 9/12,708
0.71/1,000 Unilateral PCHI >35 dB = 3/12,708
0.24/1,000
(Connolly et al 2005)
Mississippi, USA
Case series – hospital based
17,602 well and at-risk babies who received neonatal care at the University of Mississippi between January 1997 and January 2002. 14,408 well babies (81.9%) and 3,194 at-risk babies (18.1%)
Well babies: 1. Initial screen with AABR 2. Rescreen of failures with AABR 3. Rescreen of stage 2 failures with repeated AABR. 4. Re-test of failures with diagnostic ABR At-risk babies: 1. Initial screen with AABR 2. Rescreen of failures with repeated AABR 3. Re-test of failures with diagnostic ABR. All other high risk patients referred for audiologic follow-up
Sensorineural or conductive hearing loss ≥35 dB = 78/17,602
4.43/1,000

Universal neonatal hearing screening 177
Study Location Study design Study population Intervention Prevalence (Kennedy et al 2005)
UK, Wessex trial
Multi-centre (4) quasi-randomised controlled trial.
53,781 live births between October 1993 and 1996 in 4 different hospitals 25,609 born during periods of UNHS and 21,279 screened. 28172 born during periods without UNHS
During periods of UNHS: 1. Initial screen with TEOAE 2. Rescreen of failures with AABR 3. Re-test of failures with audiological assessment During periods without UNHS: 1. Distraction test 2. Re-test of failures with audiological assessment Details of PCHI cases not initially identified by UNHS or following the distraction test were obtained from case records and outpatient lists from local audiology services
Group born during period of UNHS: Bilateral PCHI >40 dB = 31/25,609
1.21/1,000
Group born during period without UNHS: Bilateral PCHI >40 dB = 35/28,172
1.24/1,000
Entire sample: Bilateral PCHI >40 dB = 66/53,781
1.23/1,000
(Martines et al 2007)
Sicily, Italy Case series – hospital based
1,191 well and at-risk babies born in the hospital of Sciacca between 2003 and 2004. 1,068 babies underwent screening. 942 well babies (88.2%) and 126 at-risk babies (11.8%)
1. Initial screen with TEOAE 2. Rescreen of failures with TEOAE at 7 months 3. Rescreen of failures after a further 2 weeks with TEOAE 4. Re-test of failures using TEOAE and AABR
Sensorineural hearing loss > 56 dB = 2/1,068
1.87/1,000
(Neumann et al 2006)
Hessen, Germany
Multi-centre (49) case series
17,439 well and at-risk babies born in 2005 and screened at one of 46 maternity clinics or 3 NICUs g
1. Initial screen with AABR and/or TEOAE 2. Re-test of failures with diagnostic ABR
Congenital hearing loss ≥40 dB = 36/17,439
2.06/1,000 Bilateral = 30/17,439
1.72/1,000
Unilateral = 6/17,439 0.34/1,000
(Pastorino et al 2005)
Milano, Italy
Case series – hospital based
19,777 well and at-risk babies born between 1997 and 2001. 19,290 well babies (97.5%) and 487 at-risk babies (2.5%)
Well babies: 1. Initial screen with TEOAE 2. Re-screen of failures with TEOAE 3. Re-test of failures with diagnostic ABR At-risk babies: 1. Diagnostic ABR
Congenital hearing loss ≥40 dB = 63/19,777
3.19/1,000 Bilateral = 33/19,777
1.67/1,000
Unilateral = 30/19,777 1.52/1,000

Universal neonatal hearing screening 178
Study Location Study design Study population Intervention Prevalence (Stewart et al 2000)
USA Multi-centre (5) case series
11,711 neonates enrolled from 5 clinical settings born between December 1996 and December 1997. UNHS performed on neonates from WBN, NICU and intermediate care nurseries (depending on site)
1. Initial screen with AABR 2. Rescreen of failures prior to discharge with AABR (Algo 2) Outpatient re-test of missed failures also with AABR (Algo 2) 3. Failures referred for diagnostic ABR, OAE or tympanometry
Sensorineural hearing loss >35 dB = 32/11,711
2.73/1,000 Bilateral = 21/11,711
1.79/1,000
Unilateral = 11/11,711 0.94/1,000
Conductive >35 dB = 8/11,711
0.68/1,000 (Uus & Bamford 2006)
UK Multi-centre case series
169,487 well and at-risk babies born before January 1 2004 who were screened as part of the national newborn hearing screening program in England
Well babies: 1. Initial screen with TEOAE 2. Rescreen of failures with AABR 3. Failures referred for audiologic assessment At-risk babies: 1. Initial screen with TEOAE and AABR 2. Those who failed TEOAE or AABR referred for audiologic assessment
Bilateral PCHI ≥40 dB = 169/169,487
1.00/1,000 Sensorineural, mixed or conductive hearing loss ≥40 dB = 152/169,487
0.90/1,000
40-69 dB = 59/169,487 0.35/1,000
70-94dB = 40/169,487
0.24/1,000
≥95 dB = 53/169,487 0.31/1,000
(Watkin & Baldwin 1999)
UK Retrospective cohort
25,199 neonates born between January 1992 and 1997
1. Initial screen with TEOAE 2. Rescreen of failures with TEOAE or ABR 3. Re-test of failures with ABR 4. Passed ABR <40 dB: referred for behavioural localisation tests at 8 months 5. Failed ABR >40 dB: re-tested with ABR followed by behavioural observation audiometry and examined with auroscopy and tympanometry
Bilateral >40 dB = 33/25,199
1.31/1,000 41–80 dB = 26/25,199
1.03/1,000 >80 dB = 7/25,199
0.28/1,000 Unilateral >40 dB = 9/25,199
0.36/1,000 41–80 dB = 6/25,199
0.24/1,000 >80 dB = 3/25,199
0.12/1,000

Universal neonatal hearing screening 179
Study Location Study design Study population Intervention Prevalence (White et al 2005)
USA Multi-centre (7) case series
86,634 well and at-risk babies screened in seven hospitals born between May 2001 and January 2003. Only babies from families whose primary language was English or Spanish were recruited
1. Initial screen with OAE h 2.Rescreen of failures with AABR 3.Re-test of OAE failures with tympanometry, OAE or visual reinforcement audiometry
Sensorineural or conductive hearing loss > 40 dB = 133/86,634
1.54/1,000 41-70 dB = 69/86,634
0.80/1,000 > 70 dB = 64/86,634
0.74/1,000 Ascertainment via other methods
(Davis & Wood 1992)
Nottingham Health District, UK
Retrospective cohort
All 29,317 children born between January 1983 and December 1986 in the Nottingham health district to mothers living in the same district (27,581 non-NICU)
Children’s Hearing Assessment Centre records examined for all children (born January 1983 to December 1986) fitted with hearing aids NICU graduate status determined through record matching. Determined family history of congenital hearing loss; syndromes or abnormalities at birth Children with hearing aids received either: age appropriate behavioural test, or ABR or tympanometry
Sensorineural/mixed and congenital/ progressive hearing loss
>50 dB = 1.06/1,000
51–64 dB = 0.32/1,000
65–79 dB = 0.26/1,000
80–94 dB = 0.19/1,000
>94 dB = 0.29/1,000
(Fortnum & Davis 1997)
Trent region, UK
Retrospective cohort
Children born between 1985 and 1993 in the Trent Health Region at the time of data collection
Ascertained through health and/or education records. Questionnaires were also sent to some parents
PCHI ≥40 dB in better hearing ear (averaged over 0.5, 1, 2, 4 Hz) Congenital (1991–1993 n = 186,078) ≥40 dB = 147/186,078
0.79/1,000
(Hadjikakou & Bamford 2000)
Cyprus Retrospective cohort
126,369 children born between 1 January 1979 and 31 December 1990
Examination of records/ databases from the School for the Deaf to identify age of diagnosis Questionnaire also sent to parents to validate data
Congenital hearing loss >50 dB = 151/126,369 i
1.19/1,000
51–69 dB = 0.30/1,000
70–94 dB = 0.42/1,000
>94 dB = 0.47/1,000
(Kubba et al 2004)
Glasgow, UK Retrospective cohort
105,517 children born in Greater Glasgow between January 1985 and December
Ascertained through hospital and educational audiology records
Bilateral PCHI ≥40 dB = 124/105,517
1.18/1,000

Universal neonatal hearing screening 180
1994
(Mytton & Mackenzie 2005)
Oldham, UK Retrospective cohort
54,448 children born in Oldham between January 1986 to December 2002
Cases of PCHI ascertained through records from local paediatric audiology clinic and the Child Health Database of Oldham
Congenital hearing loss Bilateral ≥40 dB = 98/54,448
1.80/1,000
(Neary et al 2003)
Warrington, UK
Retrospective cohort
Children born between 1 January 1981 and 31 December 1992 and living in Warrington District in December 1998
Not stated Unilateral PCHI ≥40 dB = 37 cases
1.15/1,000
(Nekahm et al 2001b)
Tyrol, Austria Retrospective cohort
124,809 children born between 1980 and 1994 in the Tyrol
Retrospective examination of medical records and case histories from the Childhood Hearing Impairment Register of the Tyrol Survey of all ENT j practitioners in the Tyrol to verify the data
Congenital hearing loss >40 dB = 158/124,809
1.27/1,000 41–69 dB = 84/124,809
0.67/1,000 70–94 dB = 37/124,809
0.30/1,000 >94 dB = 37/124,809
0.30/1,000 (Russ et al 2003)
Victoria, Australia
Retrospective cohort
64,116 children born in 1993 in the state of Victoria and surviving the neonatal period
Retrospective examination of the Australian Hearing database for all children born in 1993 and fitted with hearing aids for hearing impairment classified as congenital (through cross-matching with VIHSP k database and parent questionnaires)
Congenital hearing loss Bilateral
>40 dB = 1.12//1,000 >60 dB = 0.48/1,000 >90 dB = 0.17/1,000
a Universal neonatal hearing screening; b well baby nursery; c transient evoked otoacoustic emissions testing; d automated auditory brainstem response testing; e conventional auditory brainstem response testing; f permanent childhood hearing impairment; g neonatal intensive care unit; h otoacoustic emissions testing; i 27 children with hearing loss were detected after 6 years of age. Age of detection for seven children was unavailable. Exclusion of these children would underestimate the prevalence; j ear, nose and throat; k Victorian Infant Hearing Screening Program.

Universal neonatal hearing screening 181
Included controlled and descriptive studies on screening safety
Study Quality Screen setting Study population Screening protocol Study design Method of data ascertainment
Outcome(s) assessed
(Clemens et al 2000)
N/A Women’s Hospital of Greensboro North Carolina, USA
49 parents of 76 well babies with normal hearing who screened positive Study duration: 1 year
2-stage Stage 1: inpatient AABR a (51% received repeat AABR 12–24 hours after fail)
Stage 2: outpatient AABR or dx ABR b
Diagnostic stage: referral for further evaluation
Cross-sectional survey
Questionnaire survey of all false-positive results after stage 2 screening
Parental anxiety
(Crockett et al 2005)
Level III-2 QS = 3.5/6
6 maternity hospitals, health visitor clinics and general practice surgeries England
48 mothers of infants who underwent health visitor distraction test (21 were referred, 27 passed) 42 mothers of neonates who received hearing screening (16 were referred, 26 passed)
2-stage health visitor distraction test (HVDT) Stage 1:
HVDT Stage 2:
HVDT Diagnostic stage:
referral for further evaluation 3-stage neonatal hearing screening Stage 1:
OAE Stage 2:
OAE Stage 3:
AABR Diagnostic stage:
referral for further evaluation
Cohort study Questionnaire survey sent to 99 mothers of babies who received HDVT, 35 mothers of babies who screened negative on first stage of neonatal hearing screening, and 30 mothers of babies who screened positive on first stage of neonatal hearing screening Spielberger State-Trait Inventory and individual item about ‘Worry about baby’s hearing’
Parental anxiety and worry
(Crockett et al 2006)
Level III-2 QS = 4/6
Hospitals participating in UNHS pilot program England
344 mothers of infants were screened Group 1: clear responses in both ears from 1st or 2nd stage Group 2: not clear
3-stage Stage 1:
OAE Stage 2:
OAE Stage 3:
Cohort study Questionnaire survey sent 3 weeks after completion of screening to random sample of mothers of infants with different screening results
Parental anxiety and worry

Universal neonatal hearing screening 182
responses in one or both ears at 1st or 2nd stage but clear on AABR Group 3: not clear responses in one ear at AABR and referred for possible unilateral hearing loss Group 4: not clear responses in either ear at AABR and referred for possible bilateral hearing loss
AABR Diagnostic stage: referral for further evaluation
Spielberger State-Trait Inventory and individual item about ‘Worry about baby’s hearing’
(Hergils & Hergils 2000)
N/A University Hospital of Linköping Linköping, Sweden
Parents of 83 well babies who were screened Study duration: 1 year
2-stage Stage 1:
TEOAE c
Stage 2: TEOAE or AABR
Diagnostic stage: dx ABR
Cross-sectional survey
Unstructured questionnaire survey of all screened in first year of universal neonatal screening program
Parental anxiety
(Kennedy 1999) (Wessex Universal Neonatal Screening Trial Group)
Level III-2 QS = 2.5/5
4 maternity hospitals Wessex, UK
Mothers of 150 low-risk babies 75 screened positive versus 75 screened negative Study duration: 3 years
2-stage Stage 1: <48 hours (WBN) d; <discharge (NICU) e
TEOAE Stage 2: same day as fail
AABR Diagnostic stage: 6–12 weeks
dx ABR
Nested case-control study (III-2)
Questionnaire survey sent to 100 mothers of infants screening positive and 100 mothers of infants screening negative Spielberger State-Trait Anxiety Inventory Attitude towards the Baby Scale
Negative attitude to baby Concern for the baby
(Kolski et al 2007) Level III-2 QS=1.5/6
Maternity hospital, University Hospital of Picardy Amiens, France
143 mothers of well babies 115 babies were screened, 58 by 1st strategy, 57 by 2nd strategy Study duration: 6 months for each
Strategy 1: 2-stage: Stage 1: (day 3)
OAE Stage 2: (3-4 weeks later)
OAE Diagnostic stage:
Cohort study 2 semi-structured interviews comprising MADRS scale for post-partum depression, anxiety scale of EPDS questionnaire, certain items of the Kennerley self-administered questionnaire and the
Parental anxiety Quality of early interactions

Universal neonatal hearing screening 183
strategy not stated Strategy 2: 2-stage: Stage 1: (2 months)
OAE Stage 2: (3-4 weeks later)
OAE Diagnostic stage:
referral for further evaluation
interaction scale, investigating visual, physical, mental and social dimensions of the mother-infant relationship 1st interview held after announcement of result of 1st stage 2nd interview held just before confirmation test
(Tatli et al 2007) Level IV QS = 4.5/5
Dokuz Eylul University Hospital, Izmir Turkey
466 well and at-risk babies Study duration: 18 months
2-stage: Stage 1: (last day of discharge)
TEOAE Stage 2:
TEOAE Diagnostic stage:
dx ABR
Cross-sectional survey
466 mothers of screened infants were interviewed prior to testing and 28 mothers interviewed again after a positive result
Parental anxiety
(Vohr et al 2001) N/A Women & Infants Hospital Rhode Island, USA
307 mothers of initial screen well babies 40 mothers of rescreen well babies
3-stage Stage 1:
TEOAE Stage 2:
TEOAE Stage 3:
AABR Diagnostic stage:
dx audiology
Cross-sectional survey
Questionnaire survey of mothers of well babies at (1) initial screen and prior to receiving result (2) rescreen, 2–8 weeks after receiving initial fail result
Parental anxiety
(Watkin et al 1998) Level III-2 QS = 3.5/6
Whipps Cross Hospital London, UK
57 mothers of rescreen babies versus 61 mothers of unscreened babies
2-stage Stage 1: < discharge
TEOAE Stage 2:
TEOAE Diagnostic stage:
dx ABR
Prospective cohort (III-2)
Speilberger State Trait Anxiety Inventory (modified to 10 items) administered to mothers of babies undergoing rescreen appointment; and posted to mothers of babies (of the same age) at another hospital who do not have access to
Parental anxiety

Universal neonatal hearing screening 184
screening
(Weichbold & Welzl Mueller 2001)
N/A University Hospital Innsbruck, Austria
85 mothers of well babies with normal hearing who screened positive 43 mothers of screen positives referred for diagnostic testing
2-stage Stage 1: <48 hours
TEOAE Stage 2: < discharge
TEOAE Diagnostic stage:
dx audiology
Cross-sectional survey
Questionnaire survey of mothers of well babies at (1) discharge for baby who failed initial test but passed re-test (2) at 1 month after baby failed re-test and prior to diagnostic test
Parental anxiety
a Automated auditory brainstem response test; b diagnostic auditory brainstem response test; c transient evoked otoacoustic emissions test; d well baby nursery; e neonatal intensive care unit; MADRS= Montgomery Åsberg Depression Rating Scale ; EPDS=Edinburgh post-natal depression score

Universal neonatal hearing screening 185
Included studies on diagnostic accuracy
All children were cross-classified on the test and reference standard.
Study
Location Diagnostic level of evidence
Quality score
Study population
Testing protocol
Diagnostic test
Reference standard
TEOAE a versus ABR b
(Jacobson & Jacobson 1994)
Norfolk, Virginia, USA
III-2
10/14
n = 119 babies (238 ears) 56% at risk M:F d = 43:24 44% well M:F = 27:25 All in stable physical condition Uncorrected age: 33 to 41 weeks
Tester: audiologist Environment: ‘real world’ – crib-side in WBN e or NICU f. Baby asleep or resting quietly Time of tests: immediately prior to discharge Test order: arbitrary but ABR probably done second as all 14 ears LTFU g didn’t receive it.
TEOAE – ILO88 Otodynamic analyser Default protocol, click rate and intensity level used Screen fail: unilateral absence of OAE h with >50% reproducibility(consistent with ≥30 dB HL in mid-frequency range)
Combined AABR i and conventional ABR Conventional ABR – Navigator, Biologic Systems Corp Test fail: absence of identifiable and replicable wave V peak at 35 dB nHL j AABR – ALGO-1, Natus Medical Inc. Test fail: unilateral refer at 35 dB HL
(McNellis & Klein 1997)
Charleston, South Carolina, USA
III-2
10/14
n = 50 babies All healthy, low risk babies Risk factors as defined by Joint Committee on Infant Hearing in 1994 Uncorrected age: full-term >37 weeks
Tester: audiologist Environment: quiet, empty room near nursery. Baby asleep or resting quietly Time of tests: 4–25 hours of age for first screen. Some rescreened in day 2. All tested prior to discharge Test order: all received ABR first
TEOAE -– Otodynamics ILO88 (vers. 4.20B) Click stimulus 80–85 dB SPL k Screen fail: unilateral absence of OAE ≥3 dB in at least 3 frequency bands (1.6, 2.4, 3.2, 4.0 kHz) or ≥4 dB at 3.2 and 4.0 kHz
Conventional ABR – Intelligent Hearing Systems SmartEP ABR system in screener mode but did not use automatic waveform identification option Test fail: absence of repeatable wave V (interpeak wave V agreement of 0.2 msec) at 40 dB HL l

Universal neonatal hearing screening 186
(Smyth et al 1999)
Brisbane, Queensland, Australia
III-1
11/14
n = 37 babies All normal, well babies without risk factors for hearing loss and normal prenatal, perinatal, postnatal and maternal history Uncorrected age: all full-term (37 to 42 weeks) Data available on special care neonates but not relevant for this assessment
Tester: audiologist Environment: quiet room. Baby asleep or resting quietly Time of tests: all tested prior to discharge at gestational age 37–42 weeks Test order: not stated
TEOAE – ILO88 Otodynamic analyser (vers. 3.94) (1) Default protocol, click rate and intensity level used, and (2) QuickScreen program option Peak stimulus 71–83 dB SPL Screen fail: unilateral absence of OAE ≥10 dB plus reproducibility of ≥65%, for the default test format
Conventional ABR – Biologic Traveller System Test fail: absence of any or all ABR waveforms I-III-V at 70 dB nHL and/or if the wave V test-retest threshold poorer than 30 dB nHL
TEOAE versus tympanometry
(Ho et al 2002)
Community screening clinics (29) in Minnesota, USA
III-2
10/14
n = 33 babies Normal and at-risk babies in the community, excluding those with cerumen occlusion of the ear Uncorrected age: 0–6 months Data available on other ages but not relevant for this assessment
Tester: trained graduate audiology students Environment: not stated Time of tests: <6 months. Both tests performed at same screening Test order: not stated
TEOAE -– Otodynamics ILO88 Default variables at 0.8, 1.6, 2.4, 3.2 and 4.0 kHz and QuickScreen program option Peak click stimulus 80 dB SPL (±2 dB) Screen fail: unilateral absence of OAE if reproducibility index ≤50% at 0.8 and 1.6 kHz or ≤75% at 2.4, 3.2 and 4.0 kHz
Tympanometry – Welch-Allyn MicroTymp II. Handheld & 226 Hz probe tone Test fail: SA <0.2 mmho / TW >300 daPa
AABR versus ABR
(Schauseil-Zipf & Von Wedel 1988)
Women and children’s clinic, Cologne, Germany
III-2
9/14
n = 50 babies 25 healthy newborns and 25 at risk for hearing loss
Tester: two investigators experienced with the tests Environment: baby asleep
AABR – ALGO-1, Fa. Nicolet Screen fail: unilateral refer at 35 dB HL
Conventional ABR – Pathfinder II Signal-Analysis – system of Fa. Nicolet

Universal neonatal hearing screening 187
Uncorrected age: 38–41 weeks for the well babies
after feeding Time of tests: <discharge. Both tests performed at same screening Test order: AABR first
Test fail: not stated
a Transient evoked otoacoustic emissions test; b auditory brainstem response test; c assumption that selection was non-consecutive as ‘consecutive’ not mentioned in text; d male:female; e well baby nursery; f neonatal intensive care unit; g lost to follow-up; h otoacoustic emissions; i automated auditory brainstem response test; j near hearing level; k sound pressure level; l hearing level.

188 Universal neonatal hearing screening
Included controlled studies on effectiveness of screening
Level of evidence
Quality Study Setting Study population Screening protocol Screen fail criterion
Comparator Outcome(s) assessed
III-1 QS=3/6 (Kennedy et al 1998) (Wessex Universal Neonatal Screening Trial Group) (Kennedy et al 2005)
Princess Anne Hospital, Southampton St Mary’s Hospital, Portsmouth Royal United Hospital, Bath Princess Margaret Hospital, Swindon Wessex, UK
53,781 well and at-risk babies born at 4 hospitals during study period 25,609 babies born during periods with hearing screening 28,172 babies born during periods without hearing screening Study duration: 3 years Follow-up: 8 years
2-stage Stage 1: <48 hours (WBN a); <discharge (NICU b)
TEOAE c
Stage 2: same day as fail
AABR d
Diagnostic stage: 6–12 weeks
dx ABR e
Tester: trained testers Environment: bedside
Bilateral fail if TEOAE not produced for either (1) ≥28 dB (2) ≥98% whole response correlation (3) 3 of 5 frequencies, with 3 dB SNR f at 0.8, 1.2 kHz and 6 dB at 2.4, 3.6, 4.0 kHz (protocol began with a unilateral fail but this changed to a bilateral fail midway through the study period) AABR fail at ≥35 dB HL
Not universal neonatal hearing screening
Coverage Failure rate/referral False alarm rate Absolute and Incremental yield Age at referral Age at diagnosis Age at management False negative
III-2 QS=5/6 (Kennedy et al 2006)
Eight districts of Southern England: Wessex subgroup: Princess Anne Hospital, Southampton St Mary’s Hospital, Portsmouth
68,714 infants born during periods hearing screening 88,019 infants born during periods without universal screening 168 PCHI children identified
Wessex Subgroup: as above Greater London Subgroup: Hillingdon Hospital: 2-stage auditory response cradle (ARC) Whipps Cross Hospital:
2-stage TEOAE Diagnostic stage:
Wessex Subgroup: as above Greater London Subgroup: Fail criteria not stated ABR fail ≥40 dB HL
Not universal neonatal hearing screening
Communication ability Language acquisition

Universal neonatal hearing screening 189
Royal United Hospital, Bath Princess Margaret Hospital, Swindon Greater London subgroup: Whipps Cross University Hospital, London One district adjacent to Whipps Cross Hillingdon Hospital Postgraduate Centre East London District of Redbridge
120 gave consent to participate in study 61 born during periods with hearing screening 59 born during periods without hearing screening
dx ABR
Two other hospitals formed the ‘Not universal neonatal hearing screening’
III-2 QS=5.5/6 (Nekahm et al 2001a)
Tyrol, Austria 91 Tyrolean children born between 1990 and 1999 and registered with PCHI g at the only audiological centre in the state UNHS h = 1995–1999 Not UNHS = 1990–1994 Study duration: 10 years, retrospective
2-stage Stage 1:
TEOAE Stage 2:
TEOAE Diagnostic stage:
dx audiology Tester: not stated Environment: not stated
Not stated Not universal neonatal hearing screening
Age at diagnosis

190 Universal neonatal hearing screening
III-2
QS=5/6 (Neumann et al 2006)
Hessen &Thuringia Germany
17, 349 well and at-risk babies in 2005 made up the UNHS group UNHS= 1995-2005 Not UNHS= 1990-2005
739 had 1 stage AABR 3,750 had 1 stage TEOAE 12,950 had 2-stage Stage 1:
TEOAE Stage 2:
AABR
TEOAE ≥ 30dB AABR ≥ 35dB
Not universal hearing screening
Age at diagnosis
III-2 QS=4.5/6 (Weichbold et al 2006)
Innsbruck, Austria 321 hearing impaired children 167 had been screened 154 had not been screened Study duration: 1990-2004 Retrospective study
Post-1995 UNHS criterion: 2-stage:
TEOAE-TEOAE Diagnostic stage:
dx audiology Tester & Environment: not stated
Not stated Not universal neonatal hearing screening
Age at confirmation Age at management
III-2
5.5/6 (Yoshinaga-Itano et al 2001)
Colorado, USA 25 matched pairs of children with bilateral PCHI born in hospital with and without UNHS Study duration: 5 years, retrospective
1-stage Stage 1:
AABR Diagnostic stage:
dx audiology Tester: not stated Environment: not stated
Bilateral fail ≥ 35 dB
Not universal neonatal hearing screening
Diagnosis <6 months
III-2
5.5/6 (Yoshinaga Itano et al 2000)
Colorado, USA 25 matched pairs of children with bilateral PCHI born in hospital with and without UNHS Study duration: 5
1-stage Stage 1:
AABR Diagnostic stage:
dx audiology
Bilateral fail ≥ 35 dB
Not universal neonatal hearing screening
Language acquisition Communication ability

Universal neonatal hearing screening 191
years, retrospective Tester: not stated Environment: not stated
a Well baby nursery; b neonatal intensive care unit; c transient evoked otoacoustic emissions test; d automated auditory brainstem response test; e diagnostic auditory brainstem response test; f signal-to-noise-ratio; g permanent childhood hearing impairment; h universal neonatal hearing screening.

192 Universal neonatal hearing screening
Included descriptive studies on effectiveness of screening Study Quality & level
of evidence Setting Study population Screening protocol Screen fail criterion Outcome(s) assessed
(Aidan et al 1999) Level IV QS=5/5
Hospital Paris, France
1,727 well and at-risk babies Study duration: 18 months
2-stage Stage 1: day 2
TEOAE a
Stage 2: <30 days TEOAE
Diagnostic stage: dx audiology b
Tester: clinical audiologist Environment: quiet room while babies slept
Bilateral or unilateral fail on at least one of these criteria: TEOAE response 1) >8 dB SPL c 2) broad spectrum (0.8–5 kHz) 3) correlation >60% between 2 traces of alternate buffers ABR fail: >40 dB HL d conventional frequencies
Coverage Failure rates LTFU e
False alarm rates Yield
(Bailey et al 2002) Level IV QS=5/5
5 maternity hospitals Perth, Australia
13,214 well and at-risk babies Study duration: 18 months
2-stage (well-baby protocol) Stage 1: day 1
TEOAE Stage 2: < discharge
AABR f + 1–2 weeks after discharge
TEOAE ± AABR Diagnostic stage:
dx ABR g
Tester: trained hearing screeners; variety of backgrounds Environment: not stated
Unilateral fail: ≥35 dB HL (bilaterally in 40 babies)
Coverage Failure rates LTFU False alarm rates Yield
(Bamford et al 2005) Level IV QS=4/5
23 areas of England
About 120,000 births per annum
2-stage Stage 1:
TEOAE
Fail not stated Coverage Failure rates Yield

Universal neonatal hearing screening 193
Stage 2: AABR
Diagnostic stage: dx ABR and middle ear
function test Tester: trained screener Environment: mother’s bedside
Hospital London, UK
1,492 well babies born in hospital 1992–1995 Study duration: 4 years
2-stage Stage 1: first few days
TEOAE Stage 2: 1 month later
TEOAE Diagnostic stage:
dx ABR Tester: not stated Environment: hospital incubator
Bilateral or unilateral fail on at least one of these criteria: TEOAE response 1) >5 dB SPL above noise level 2) broad spectrum (0.8–4 kHz) 3) reproducibility >50% ABR fail: waves I, II and V not present at >40 dB HL
Failure rate False alarm rate Yield
(Bantock & Croxson 1998)
Level IV QS=4/5
Community-based health centre (~7% of population) London, UK
319 babies born June 1995 – May 1996 Study duration: 1 year
2-stage Stage 1: 3–4 weeks
TEOAE Stage 2: 1–2 weeks later
TEOAE Diagnostic stage: 1–2 weeks later
dx ABR
Tester: research nurse Environment: quiet or sound-proofed room – in car seat or sling if asleep
Bilateral or unilateral fail on at least one of these criteria: TEOAE response 1) >5 dB SPL above noise level 2) broad spectrum (0.8–4 kHz) 3) reproducibility >50% ABR fail: waves I, II and V not present at >40 dB HL
Coverage Failure rates Yield

194 Universal neonatal hearing screening
(Brennan 2004) Level IV QS=2.5/5
Instititution in Illinois USA
Not stated 2-stage Stage 1: (pre-discharge)
OAE Stage 2: (post-discharge)
AABR Diagnostic stage:
Not stated Tester: not stated Environment: quite area of the nursery
Fail not stated Coverage Failure rate
(Chapchap & Segre 2001)
Level IV QS=3.5/5
Hospital Israelita Albert Einstein Sao Paulo, Brazil
4,196 well babies and those in the neonatal intensive care unit (NICU) born September 1996 to August 1999 Study duration: 3 years
2-stage Stage 1: day 2–3 – (well babies), < discharge (NICU babies)
TEOAE Stage 2: <30 days
TEOAE Diagnostic stage: 3 months
dx audiology (ABR, TEOAE, behavioural, tympanometry)
Tester: not stated Environment: not stated
Fail if an absent TEOAE response for 2 or more of 4 frequency bands – evaluated by: (1) ≥3 dB SPL above noise level for 1.6 kHz or reproducibility ≥50% 2) ≥6 dB SPL above noise level for 2.4, 3.2 and 4.0 kHz or reproducibility ≥70%
Coverage Failure rates LTFU False alarm rates Yield
(Chiong et al 2007) Level IV QS=2/5
Several communities in a rural area, Bulacan province, Philippines
724 neonates Study duration: 2 years 10 months
1-stage: 565 infants Stage 1: unclear
TEOAE+ABR
Fail not stated Coverage Yield
(Clarkson et al 1994) Some duplication with (Maxon et al 1993)
Level IV QS=2.5/5
Women and Infants Hospital of Rhode Island Providence, Rhode Island, USA
1,850 well and at-risk babies born 1990–1991 Study duration: 6 months
464 infants: 2-stage Stage 1: day 1–4
TEOAE + ABR Stage 2:
TEOAE + ABR 1,386 infants: 3-stage Stage 1: day 1–4
Fail: ≥60 dB HL referred for dx ABR; <60 dB HL referred for behavioural audiologic evaluation Fail: ≥25 dB HL for conductive hearing loss
LTFU False alarm rate Yield

Universal neonatal hearing screening 195
TEOAE Stage 2: day 1–4
ABR Stage 3: 4–6 weeks later
TEOAE + ABR Diagnostic stage: 12–16 weeks of age
dx ABR and behavioural audiologic evaluation
Tester: paraprofessional technician Environment: quiet room
(Clemens et al 2000) Level IV QS=3/5
Women’s Hospital of Greensboro North Carolina, USA
5,034 well babies born in hospital, July 1998 – June 1999 Study duration: 1 year
2-stage Stage 1: inpatient
AABR (51% received repeat AABR 12–24 hours after fail)
Stage 2: outpatient AABR or dx ABR
Diagnostic stage: referral for further evaluation
Tester: trained screening technician for stage 1 and audiologist for stage 2 Environment: not stated
Fail: >35 dB HL Coverage Failure rates LTFU False alarm rates Yield
(Clemens & Davis 2001)
Level IV QS=5/5
Women’s Hospital of Greensboro North Carolina, USA
3,144 well babies born in hospital, November 1999 – May 2000 Study duration: 6 months
3-stage Stage 1: inpatient
AABR Stage 2: inpatient (12–24 hours after fail)
AABR Stage 3: outpatient
AABR or dx ABR Diagnostic stage:
Fail: >35 dB HL Coverage Failure rates LTFU False alarm rates Yield

196 Universal neonatal hearing screening
referral for further evaluation
Tester: trained screening technician for stage 1 and audiologist for stage 2 Environment: not stated
(Connolly et al 2005) Level IV QS=4.5/5
University of Mississippi Mississippi, USA
17,602 well and at-risk babies Study duration: 5 years
2-stage Stage 1: (prior to discharge)
AABR Stage 2: (outpatient)
AABR Diagnostic stage:
Dx ABR and medical evaluation
Tester: trained nurse Environment: not stated
Fail >35 dBn HL Coverage Yield
(Cox & Toro 2001) Level IV QS=5/5
Boston Medical Centre Massachusetts, USA
1,713 well and at-risk babies Study duration: 1 year
2-stage (well babies) Stage 1: day 1
DPOAE h
Stage 2: immediately after fail AABR
Diagnostic stage: 2–4 weeks dx ABR
All NICU babies received a 1-stage AABR screen followed by diagnostic referral Tester: audiologist and audiometric technicians Environment: quiet room
Fail: not stated (Data from 2000) LTFU False alarm rate Yield

Universal neonatal hearing screening 197
(Daemers et al 1996) Level IV QS=3/5
St Augustinus Medical Institute Antwerp, Belgium
907 well babies born in 1993 and 1994 Study duration: 2 years
2-stage Stage 1: > day 3
TEOAE Stage 2: ~3 weeks later
TEOAE Diagnostic stage: 3 months
dx ABR Tester: clinical audiologist Environment: soundproof or quiet room
Bilateral or unilateral fail if absent TEOAE response – evaluated by: (1) >3 dB SPL above noise level for 1.6 kHz 2) >6 dB SPL above noise level for 2.4, 3.2 and 4.0 kHz (3) and reproducibility >50%
Failure rates LTFU False alarm rates Yield
(De Capua et al 2003) Level IV QS=4.5/5
Hospital Italy
532 well and at-risk infants Study duration: not stated
2 stage Stage 1: 4 days
TEOAE Stage 2:15-30 days post 1st test
TEOAE
Diagnostic stage: within 1 month of 2nd test
Click ABR
Tester: not stated Environment: not stated
Fail if TEOAE reproducibility <50% with n<3 frequencies with intensity >3 dB SPL
Failure rates Yield
(Downs 1995) Level IV QS=2/5
17 hospitals in Colorado Colorado, USA
14,494 well and at-risk babies born 1992 onwards Study duration: not stated
1-stage (unclear whether initial screen was repeated) Stage 1:
AABR Diagnostic stage: 1 month
dx ABR Tester: certified audiologist
Fail: ≥35 dB HL bilaterally/ unilaterally
Failure rate LTFU False alarm rate Yield

198 Universal neonatal hearing screening
Environment: not stated
(Govaerts et al 2001) Level IV QS=4/5
St Augustinus Hospital Antwerp, Belgium
2,012 well and at-risk babies born in 1999 Study duration: 1 year
2-stage Stage 1: day 3–5
TEOAE Stage 2: 3 weeks later in hospital or community
TEOAE Diagnostic stage: 3 months
dx ABR Tester: clinical audiologist Environment: not stated
Bilateral failure to produce TEOAE – evaluated by: 1) Signal-to-noise ratio of 6 dB for at least 3 of 4 frequencies – 1.6, 2.4, 3.2 and 4.0 kHz (2) and reproducibility >50% ABR bilateral fail >40 dB
Coverage Failure rates LTFU False alarm rates Yield
(Habib & Abdelgaffar 2005)
Level IV QS=4/5
Dr. Soliman Fakeeh Hospital Jeddah, Saudi Arabia
11, 986 non-high-risk neonates
2-stage: Stage 1: (<48 hrs of life)
OAE Stage 2: (*5th day of life)
OAE Diagnostic stage: (5 months)
ABR
Tester: audiology technician Environment: not stated
Failure to produce more than 50% reproducibility and response amplitude at least 1dB SPL per octave
Coverage Failure rates Yield
(Hahn et al 1999) Level IV QS=2/5
Hospital Münster, Germany
Study 1: 388 well babies Study duration: not stated
Study 1 1-stage: day 2–6
TEOAE Diagnostic stage: 4 months
full pedaudiological assessment
Unilateral fail if TEOAE did not have ≥60% reproducibility and ≥80% stimulus stability
Failure rate LTFU False alarm rate Yield

Universal neonatal hearing screening 199
Study 2: 55 well babies Study duration: not stated
Study 2 1-stage: day 2–6
TEOAE + AABR Diagnostic stage: 4 months
full pedaudiological assessment
Tester: trained specialists Environment: newborn ward, after baby was fed
Unilateral fail if TEOAE did not have ≥60% reproducibility and ≥80% stimulus stability Unilateral AABR fail: >35 dB HL
Failure rate LTFU False alarm rate Yield
(Hatzopoulos et al 2007)
QS=3.5/5 Main maternity hospital of Tirana Tirana, Albania
1,561 well and at-risk babies (463 well & 1,098 NICU babies) Study duration: 1 year
2–stage: Stage 1: (2-3 days)
TEOAE Stage 2: (4 wks post birth)
TEOAE Diagnostic stage
Click ABR
Tester: not stated Environment: bedside testing when possible
Fail to produce ≥ 70% reproducibility, and a ≥6 dB SNR (signal-to-noise ratio) for at least 2 out of 5 frequency bands
Coverage Failure rates LTFU False alarm rates Yield
(Hunter et al 1994b) Level IV QS=5/5
Princess Anne Hospital Southampton, UK
217 well and at-risk babies Study duration: 4 weeks
2-stage Stage 1: day 1–2
TEOAE Stage 2: < discharge
AABR Diagnostic stage: 1 month
dx ABR Tester: audiologist Environment: quiet room during sleep, or after feeding
Unilateral or bilateral fail on AABR: ≥35 dB HL
Coverage Failure rates LTFU False alarm rates Yield

200 Universal neonatal hearing screening
(Huynh et al 1996) Level IV QS=5/5
Air Force community hospital Maryland, USA
639 well babies born 1994–1995 Study duration: 6 months
2-stage Stage 1: 6–48 hours
TEOAE Stage 2: 1–3 weeks
TEOAE Diagnostic stage:
dx ABR Tester: physician, audiologist, or trained technician Environment: newborn nursery in open bassinet
Bilateral fail at first screen and unilateral fail at rescreen – evaluated by: (1) TEOAE without reproducibility ≥ 80% at 2.4, 3.2 and 4.0 kHz (2) overall reproducibility <40%
Coverage Failure rates LTFU False alarm rates Yield
(Iley & Addis 2000) Level IV QS=3.5/5
York district hospital North Yorkshire, UK
48 babies born 2000 Study duration: 4 days
1-stage Stage 1: day 1–7 days (inpatients); 1–12 weeks (outpatients)
AABR
Diagnostic stage: dx ABR
Tester: audiologist Environment: (inpatient) in crib at mother’s bedside while asleep; (outpatient) quiet room in Dept of Audiology
Unilateral AABR fail ≥35 dB HL Diagnostic fail ≥ –40 dB
Coverage Failure rate LTFU False alarm rate Yield
(Isaacson 2000) Level IV QS=3.5/5
Temple University Hospital, North Philadelphia Pennsylvania, USA
2,137 well and at-risk babies born 1998–1999 in an economically depressed, inner-city area. Study duration: 1 year
2-stage Stage 1: >16 hours
TEOAE Stage 2: immediately after fail
TEOAE Diagnostic stage: 4–6 weeks after discharge
dx ABR
Bilateral or unilateral fail if TEOAE absent at signal-to-noise ratio ≥3 dB in 3 of 4 frequency bands (1, 2, 3, 4 kHz)
Coverage Failure rate LTFU Yield

Universal neonatal hearing screening 201
Tester: trained paraprofessional screeners Environment: quiet room adjacent to nursery
(Iwasaki et al 2003) Level IV QS=4.5/5
Seirei-Hamamatsu General Hospital & Seirei-Mikatahara General Hospital Hamamatsu, Japan
4,092 infants born between January 2000 and December 2001
2-stage Stage 1: (2-3rd day of life)
AABR Stage 2: (5-6th day of life)
AABR Diagnostic stage
dx ABR Tester: trained technicians Environment: quiet room adjacent to the nursery
Fail if likelihood ratio is less than 160 after 15000 sweeps
Coverage Failure rates LTFU False alarm rates Yield
(Jakubikova et al 2003) Level IV QS=3.5/5
Two gynaecology and neonatology departments in Bratislava Department of Pathological Newborn and Intensive Care Unit of Children’s University, Bratislava Slovak Republic
3,048 high-risk or well babies Study duration: not stated
2-stage: Stage 1: (4-12th day)
TEOAE Stage 2: (1 month later)
TEOAE Diagnostic stage:
Tympanometry & ABR
Tester: two well trained specialists Environment: not stated
Fail not stated Coverage Failure rates False alarm rates Yield
(Kanne et al 1999) Level IV QS=4.5/5
Madigan Army Medical Centre, Tacoma Washington, USA
2,537 well and at-risk babies born 1995–1996 Study duration: 14 months
2-stage Stage 1: 24–72 hours < discharge (NICU) i; 2 weeks (WBN) j
TEOAE Stage 2:
TEOAE Diagnostic stage:
dx ABR
Unilateral or bilateral failure to produce emission spectrum of significant gain across testing frequency range, approx. >30 dB HL
Coverage Failure rates LTFU False alarm rates Yield

202 Universal neonatal hearing screening
Tester: audiologist Environment: secluded room
(Khairi et al 2005) Level IV QS=4/5
Hospital Universiti Sains Malaysia
401 newborns Study duration: Feb 2000-March 2000 & Feb 2001 and May 2001
2-stage: Stage 1: (24-48hrs post birth)
TEOAE Stage 2: (pre-discharge)
TEOAE Diagnostic stage
dx audiology
Tester: audiology technicican Environment: low noise ward
Fail not stated Coverage Failure rates LTFU False alarm rates Yield
(Khandekar et al 2006) Level IV QS=4.5/5
Hospitals in Oman, Turkey
32,080 live births born in 2003 Study duration: 1 year
2-stage: Stage 1: (24-48hrs post birth)
TEOAE or DPOAE Stage 2: (pre-discharge)
TEOAE or DPOAE Diagnostic stage
dx audiology
Tester: trained health staff Environment: not stated
Not stated Coverage Failure rates LTFU False alarm rates Yield
(Kolski et al 2007) Level IV QS=3.5/5
Maternity hospital France
Strategy 1: 3202 newborns Strategy 2: 2588 2 month old babies Study duration: 6 months for each strategy
2-stage: Strategy 1: Stage 1: (day 3)
OAE Stage 2: (3-4 weeks later)
OAE Strategy 2: Stage 1: (2 months)
OAE
Bilateral fail Coverage Failure rates LTFU False alarm rates Yield

Universal neonatal hearing screening 203
Stage 2: (3-4 weeks later) OAE
Diagnostic stage: not stated Tester: not stated Environment: not stated
(Leveque et al 2007) Level IV QS=4.5/5
17 maternities, private and public, and one neonatal intensive care unit (NICU) in Champagne-Ardenne France
33, 873 well and at-risk babies born from January 2004 to March 2006
2-stage Stage 1:
TEOAE Stage 2:
TEOAE/AABR Diagnostic stage:
dx audiology Tester: Stage 1: Paramedical staff Stage 2 conducted by physician Environment: not stated
Bilateral fail ≥35 dB HL -40 db HL depending on screening device used, which can not be modified
Coverage Failure rate False alarm rate Yield
(Lin et al 2004) Level IV QS=4/5
2 hospitals & 4 obstetric clinics Tainan, Taiwan
5938 neonates Study duration: 2 years 9 months
2-stage Stage 1: pre-discharge
TEOAE Stage 2: 1 month later
TEOAE Diagnostic stage:
dx audiology Tester: trained staff member or audiologist Environment: not stated
Fail to produce four pairs of alternating positive & negative peaks Diagnostic ABR: Fail to produce wave V latency within developmental norms in response to 35dB nHL clicks
Coverage Failure rate False alarm rate Yield
(Lin et al 2005) Level IV QS=4/5
Mackay Memorial Hospital Taipei, Taiwan
21,273 well babies born 1998-2004 Study duration: 6 years
Strategy 1 3-stage Stage 1: 48 hours
TEOAE Stage 2: <72 hrs
Bilateral or unilateral failure to produce TEOAE of (1) ≥5 dB in 3 of 5 frequency bands or (2) ≥3 dB in 4 of 5 frequency bands
Failure rates LTFU False alarm rates Yield

204 Universal neonatal hearing screening
TEOAE (up to 7 rescreens with TEOAE) Stage 3: 1 month later
TEOAE/Tympanogram Diagnostic stage: >1 month
dx audiology, including dx ABR
Strategy 2 3-stage Stage 1: 48 hours
TEOAE Stage 2: <72 hrs
AABR (up to 7 rescreens with TEOAE) Stage 3: 1 month later
TEOAE/Tympanogram Diagnostic stage: >1 month
dx audiology, including dx ABR
Tester: trained screeners (volunteers and student nurses) Environment: quiet room in the nursery
Dx ABR – failure to produce a repeatable wave V at 35 dB nHL unilaterally or bilaterally
(Low et al 2005) Level IV QS=4/5
National University Hospital (NUH), Singapore General Hospital (SGH), KK Women’s and Children’s Hospital (KKWCH) Singapore
36,093 well and at-risk babies born April 2002 to March 2004
2-stage Stage 1: Before discharge SGH OAE KKWCH AABR NUH OAE Stage 2: 4-6 weeks after fail SGH OAE KKWCH AABR NUH AABR Diagnostic stage <3 months
Not stated Coverage Failure rate Yield

Universal neonatal hearing screening 205
Audiological tests and medical evaluation
(Martines et al 2007) Level IV QS=3.5/5
Sciacca Hospital Italy
1068 well and at-risk babies born during 2003-2004
3-stage (well babies) Stage 1: 3 weeks post birth
TEOAE Stage 2: 2 weeks post initial test
TEOAE Stage 3: unclear
TEOAE Diagnostic stage:
TEOAE & AABR The first 2-stages for at-risk babies Tester: not stated Environment: sleeping, well-fed neonate
Fail criterion not stated Coverage Failure rate False alarm rate Yield
(Mason & Herrmann 1998)
Level IV QS=4/5
Kaiser Permanente Medical Center Honolulu, Hawaii
10,773 well and at-risk babies born 1992–1997 Study duration: 5 years
2-stage Stage 1: 3–36 hours (WBN); < discharge (NICU)
AABR Stage 2: immediately after fail
AABR Diagnostic stage: <1 month
dx ABR and audiological tests
Tester: audiologists and technicians Environment: quiet room adjacent to nursery or mother’s bedside
Bilateral AABR fail ≥35 dB HL Diagnostic fail >35 dB nHL
Coverage Failure rate Yield
(Maxon et al 1993) Level IV QS=3.5/5
Women and Infants Hospital of Rhode Island
1,850 well and at-risk babies born 1990–1991 Study duration: 6 months
464 infants: 2-stage Stage 1: day 1–4
TEOAE + ABR
Fail: ≥60 dB HL referred for dx ABR; <60 dB HL referred for behavioural audiologic evaluation
Failure rates LTFU False alarm rate

206 Universal neonatal hearing screening
Providence, Rhode Island, USA
Stage 2: TEOAE + ABR
1,386 infants: 3-stage Stage 1: day 1–4
TEOAE Stage 2: day 1–4
ABR Stage 3: 4–6 weeks later
TEOAE + ABR Diagnostic stage: 12–16 weeks of age
dx ABR and behavioural audiologic evaluation
Tester: paraprofessional technician Environment: quiet room adjacent to nursery; infant in enclosed isolette
Fail: ≥25 dB HL for conductive hearing loss
Yield
(McPherson et al 1998) Level IV QS=2/5
Eight community health clinics, Northern Brisbane Queensland, Australia
1,305 children between 1.5 and 2.5 months of age presenting for immunisation at the community health clinic [Data available on other age groups up to 5 years but most not relevant or incomplete] Study duration: 30 months
2-stage Stage 1: ~ 2 months
TEOAE Stage 2: 2 weeks later
TEOAE Diagnostic stage: 2 weeks – 1 month later
dx ABR and behavioural audiologic evaluation
Tester: audiologist or community health nurse Environment: quietest room available at each clinic
Unilateral or bilateral fail if TEOAE was not at least 3 dB above the noise floor and at least halfway across the test frequency bands of 2–3 kHz and 3–4 kHz
Coverage Failure rates LTFU False alarm rates Yield

Universal neonatal hearing screening 207
(Messner et al 2001) Level IV QS=5/5
Lucile Packard Children’s Hospital, Stanford California, USA
6,340 well babies born 1998–1999 Study duration: 16 months
3-stage Stage 1: <24 hours
AABR Stage 2:
AABR Stage 3:
TEOAE Diagnostic stage:
dx ABR Tester: trained volunteers Environment: nursery or mother’s bedside
Unilateral or bilateral failure >35 dB HL
Coverage Failure rates LTFU False alarm rates Yield
(Molini et al 2004) Level IV QS=4/5
Hospital Italy
2,425 full-term newborns Study duration: Study 1: 17 months Study 2: 9 months
2-stage Study 1: Stage 1: within 4 days
TEOAE Stage 2: within 3 months
ABR Diagnostic stage:
Dx audiology
Fail to produce at least 3 of the 4 frequency bands centred at 1600, 2400, 3200 and 4000 Hz.
Coverage Failure rates False alarm rates LTFU Yield
(Mukari et al 2006) Level IV QS=4/5
Hospital University Kebangsaan Malaysia (HUKM)
4437 newborns (315 NICU, 4122 non-NICU) Study duration:11 months
2-stage Stage 1: within 24 hrs
DPOAE Stage 2: 2 months
DPOAE Diagnostic stage:
dx ABR Tester: trained nurse staff Environment: bedside or nursery room for well babies Isolation room for NICU
Fail not stated Coverage Failure rates False alarm rates LTFU Yield

208 Universal neonatal hearing screening
babies
(Neumann et al 2006) Level IV QS=4/5
46 maternity clinics and 3 NICU’s Hessen, Germany
17,349 well and at-risk babies in 2005
739 had 1 stage AABR 3,750 had 1 stage TEOAE 12, 950 had 2-stage Stage 1:
TEOAE Stage 2:
AABR
TEOAE ≥ 30dB AABR ≥ 35dB
Coverage Failure rates False alarm rates LTFU Yield
(Ng et al 2004) Level IV QS=4/5
Tsan Yuk hospital Hong Kong
1064 infants born between May 1999 to October 1999
1-stage (3 re-screens): Stage 1a: (day 1-4)
DPOAE Stage 1b: (day 5-14)
DPOAE Stage 1c: (day 21-30)
DPOAE Diagnostic stage:
dx ABR
Tester: Trained nurse Environment: maternity ward or hospital room
Unilateral or bilateral failure >40 dB HL
Coverage Failure rates False alarm rates Yield
(Oudesluys-Murphy & Harlaar 1997)
Level IV QS=5/5
Community well baby clinic, Barendrecht Netherlands
288 well and at-risk babies born in 1995 Study duration: 1 year
2-stage Stage 1: 1–2 weeks
AABR Stage 2: 2 weeks later
AABR Diagnostic stage: 6 weeks later
dx audiology Tester: trained child care district nurses
Unilateral or bilateral failure >35 dB HL
Coverage Failure rates LTFU False alarm rates Yield

Universal neonatal hearing screening 209
Environment: in the home, with infant sleeping
(Owen et al 2001) Level IV QS=3.5/5
Local health centres and homes in urban and rural settings West Gloucestershire, UK
683 well babies registered at participating health centres in 1999 Study duration: 1 year
2-stage Stage 1: day 10–24
TEOAE Stage 2: 2 weeks later
TEOAE Diagnostic stage: 2 weeks later
dx audiology Tester: health visitors with screening training Environment: home or health clinic for screens
Bilateral or unilateral failure if TEOAE response <28 dB, or response correlation <98%, or SNR k did not reach target level for 3 wavebands (3 dB at 0.8, 1.2 kHz; 6 dB at 2.4, 3.6, 4.0 kHz).
Coverage Failure rates LTFU False alarm rates Yield
(Pastorino et al 2005) Level IV QS=4/5
Instituti Clinici di Perfezionamento Milan, Italy
19,777 well and at-risk babies Study duration: not stated
3-stage (Well babies) Stage 1: pre-discharge
TEOAE Stage 2: 15-30 days after discharge
TEOAE Stage 3:
AABR Diagnostic stage:
dx audiology 1-stage for at-risk babies Tester: not stated Environment: not stated
Screening: Fail to produce ≥ 70% total reproducibility Fail to produce ≥50% in the 1.6-kHz band and 70% in 2,4-, 3.2- and 4-kHz bands Diagnostic ABR ≥40 dB HL
Failure rates LTFU False alarm rates Yield
(Rao et al 2002) Level IV QS=2.5/5
5 small rural hospitals, central Minnesota USA
217 well babies born in 1999 and 2000 Study duration: 1 year
2-stage Stage 1: 1 month
AABR Stage 2: immediately
Not stated Coverage Yield

210 Universal neonatal hearing screening
AABR Diagnostic stage:
dx audiology Tester: registered nurse with screening training Environment: not stated
(Rouev et al 2004) Level IV QS=4/5
Maternity Hospital Stara Zagora Bulgaria
1750 well and at-risk babies Study duration: 329 days
1-stage Stage 1: (well babies 6-72 hrs after birth; NICU babies 3-60 days
AABR Stage 2: (3-4wks):
AABR Diagnostic stage:
dx ABR Tester: not stated Environment: quiet room adjoining the nursery
Bilateral fail >30 dB HL Failure rates LTFU False alarm rates Yield
(Shoup et al 2005) Level IV QS=4.5/5
Large public hospital Dallas, Texas
48,211 well and at-risk babies Study duration: 3 years
4-stage (well babies) Stage 1: newborn
AABR Stage 2: 24 hrs post birth
AABR Stage 3: pre-discharge by audiologist
AABR Stage 4: Outpatient
AABR Diagnostic stage:
dx audiology Tester: trained technicians
Fail not stated Failure rates Yield

Universal neonatal hearing screening 211
Environment: not stated
(Swanepoel et al 2007) Level IV QS=4/5
Private hospital in urban Gauteng South Africa
6,241 well and at-risk babies Study duration: 4 years
2-stage Stage 1: <discharge
TEOAE Stage 2: 6 weeks later
TEOAE Diagnostic stage:
dx OAE & ABR Tester: two qualified audiologists Environment: room with acceptably low noise levels
Bilateral and unilateral sensorineural hearing loss of ≥ 35dB A 70% reproducibility and a 6-dB signal-to-noise ratio at 2,3 and 4 kHz was set as pass criteria
Coverage Failure rates False alarm rates LTFU Yield
(Tatli et al 2007) Level IV QS=4.5/5
Dokuz Eylul University Hospital, Izmir Turkey
711 well and at-risk babies Study duration: 18 months
2-stage: Stage 1: (last day of discharge)
TEOAE Stage 2:
TEOAE Diagnostic stage:
dx ABR Tester: trained staff Environment: quite room adjacent to nursery
Unilateral fail Failure rates LTFU False alarm rates Yield
(Tsuchiya et al 2006) Level IV QS=4/5
Kumamoto University Hospital Kumamoto Japan
8,979 well and at-risk babies born during 1999-2004 Study duration: 5 years
2-stage: Stage 1: day 4 post-partum
TEOAE Stage 2: 1 month
TEOAE Diagnostic stage:
dx audiology Tester: not stated
Fail ≥ 35dB Coverage Failure rates LTFU False alarm rates Yield

212 Universal neonatal hearing screening
Environment: not stated
(Vohr et al 1998) Level IV QS=5/5
8 maternity hospitals Rhode Island, USA
53,121 well and at-risk babies born 1993–1996 Study duration: 4 years
2-stage Stage 1: 6–52 hours (WBN); < discharge (NICU) NICU babies that failed the screen went straight to diagnostic evaluation
TEOAE Stage 2: 2–6 weeks
TEOAE Diagnostic stage:
dx ABR Tester: trained technicians, nurses and nurses aides Environment: nursery, parent room or adjacent room (WBN); NICU or adjacent area (NICU)
Failure if absence of TEOAE response between 2 and 4 kHz with 75% reproducibility ABR fail if wave V not present >30 dB nHL
Coverage Failure rates LTFU False alarm rates Yield
(Watkin & Baldwin 1999)
Level IV QS=4/5
Whipps Cross hospital London, UK
28,890 babies born 1992–1997 Study duration: 6 years
2-stage Stage 1: < discharge
TEOAE Stage 2:
TEOAE Diagnostic stage:
dx ABR Tester: not stated Environment: not stated
Bilateral fail on initial screen and r-escreen, although unilateral fail allowed if obvious parental anxiety ABR fail >40 dB nHL in better hearing ear
Coverage LTFU False alarm rate Yield
(Yee-Arellano et al 2006)
Level IV QS=4/5
Private hospital in San Pedro Garza Garcia
3066 well and at-risk babies Study duration: 2 years
2-stage Stage 1: < discharge
AABR Stage 2: 3 weeks
ABR unilateral or bilateral fail >35-40 dB nHL
Coverage Failure rates LTFU False alarm rates

Universal neonatal hearing screening 213
Mexico AABR Diagnostic stage: not stated Tester: Fully trained technician Environment: not stated
Yield
(Zaputovic et al 2005) Level IV QS=3.5/5
Rijeka University Hospital Croatia
6,019 neonates Study duration: 26 months
2-stage Stage 1: < discharge CE-OAE Stage 2: 3 weeks CE-OAE Diagnostic stage:
dx AABR
Tester: not stated Environment: not stated
Fail not stated Coverage Failure rates False alarm rates Yield
a Transient evoked otoacoustic emissions test; b diagnostic audiology; c sound pressure level; d hearing level; e loss to follow-up; f automated auditory brainstem response test; g diagnostic auditory brainstem response test; h distortion product otoacoustic emissions test; I neonatal intensive care unit; j well baby nursery; k signal-to-noise-ratio.

214 Universal neonatal hearing screening
Included economic studies
Study Location Population Score Protocols – Comparisons Outcomes (Keren et al 2002)
Boston Massachusetts,USA
Hypothetical cohort of 80,000 infants
15/16 Modelled program A. No screening B. Targeted screening Only babies with identified risk factors as defined by the Joint Committee on Infant Hearing (2000) 2-stage screening 1st stage: AABRa then if fail: 2nd stage AABR all prior to discharge if fail: diagnostic evaluation by an otorhinolaryngologist and an audiologist C. Universal screening All newborns 2-stage screening 1st stage: TEOAEb then if fail: 2nd stage AABR all prior to discharge if fail: diagnostic evaluation by an otorhinolaryngologist and an audiologist Costs considered Short-term costs of screening (equipment, consumables and staff wages) Follow-up diagnostic assessment Long term societal costs; loss of productivity, requirement for special education, vocational rehabilitation and use of assistive devices and medical services
A. Incremental cost per infant diagnosed by 6 months with bilateral hearing impairment ($US)
B. Incremental cost reduction per child with bilateral hearing impairment possessing normal language ($US)
(Kemper & Downs 2000)
Chapel Hill North Carolina, USA
Hypothetical cohort of 100,000 infants
13/16 Modelled program A. Targeted screening Only babies with identified risk factors (time in neonatal intensive care unit, family history, presence of craniofacial abnormality) 2-stage screening 1st stage: TEOAE then if fail: 2nd stage AABR all prior to discharge if fail: diagnostic evaluation by an otorhinolaryngologist and an audiologist B. Universal screening All neonates: 2-stage screening 1st stage: TEOAE then if fail: 2nd stage AABR all prior to discharge if fail: diagnostic evaluation by
A. Cost per case of bilateral hearing impairment detected ($US)
B. Cost per extra case of bilateral hearing impairment detected ($US)

Universal neonatal hearing screening 215
an otorhinolaryngologist and an audiologist Costs considered Not clearly specified
(Kezirian et al 2001)
Seattle, Washington and Logan, Utah, USA
Hypothetical cohort of 2,000 births in one hospital per year
13/16 Modelled program 4 protocols examined: 1) 1-stage AABR followed
by diagnostic evaluation if infant failed screen
2) 2-stage AABR followed by diagnostic evaluation if infant failed both screening tests
3) 1-stage OAEc followed by diagnostic evaluation if infant failed screen
4) 2-stage OAE followed by diagnostic evaluation if infant failed both screening tests
Costs considered Costs directly absorbed by the hospital: equipment, personnel, overhead and clerical Follow-up diagnostic evaluation
A. Cost per infant screened
B. Cost per infant identified with unilateral or bilateral hearing loss
(Gorga et al 2001)
Omaha, Nebraska, USA
Hypothetical cohort of 4,000 babies
12/16 Modelled program Three screening protocols examined: 1) 1-stage AABR with
follow-up assessment if baby fails screen
2) 1-stage OAE with follow-up assessment if baby fails screen
3) 2-stage starting with OAE then AABR if baby fails first screen. Follow-up assessment if baby fails AABR screen
Costs considered Capital equipment (screening tools) Disposables Salaries and benefits
Cost per baby screened
(Boshuizen et al 2001)
Netherlands All newborn children not admitted to neonatal intensive care units in the Netherlands
10.5/16 Modelled program Community-based screening program 2- and 3-stage screening protocols 1) 2-stage OAE screening 1st stage: OAE then if fail: 2nd stage also OAE performed at different times at community health centre if fail: diagnostic evaluation 2) 2-stage AABR screening 1st stage: AABR then if fail: 2nd stage also AABR performed at different times at
Cost per child screened Cost per child detected with a hearing loss of ≥40 dB or more in the better ear

216 Universal neonatal hearing screening
community health centre if fail: diagnostic evaluation 3) 3-stage OAE screening 1st stage: OAE then if fail: 2nd stage also OAE, third test of OAE if fail results performed at different times at community health centre if fail: diagnostic evaluation 4) detection of bilateral
losses only 2-stage OAE as above but rescreened and evaluated only if fail in both ears 5) home visits only 2-stage OAE as above but screening performed on special visits to baby’s home Costs considered Equipment depreciation Personnel Consumables Travel costs of screeners Screener training Administration Follow-up diagnostic testing
(Vohr et al 2001)
5 US hospitals (sites undisclosed)
12,081 sequentially tested, well newborns
13.5/16 Existing program 3 UNHSd programs 1) 1-stage TEOAE initial testing with TEOAE and if fail tested again with TEOAE. Fail referred for diagnostic testing 2) 1-stage AABR initial testing with AABR and if fail tested again with AABR. Fail referred for diagnostic testing 3) 2-stage TEOAE then
AABR initial testing with TEOAE and if fail tested again with TEOAE. If fail again then screened with AABR. Finally a fail referred for diagnostic testing Note: screening was performed by nurses but an audiologist was required to interpret TEOAE results Costs considered Staff: audiologist, administration and clerical assistance, audiologist training, screener training Equipment: TEOAE, AABR Screening supplies
Cost per child born Cost per child identified with bilateral PCHIe
(Lemons et al 2002)
Cleveland, Ohio & Indianapolis Indiana, USA
1,530 newborns tested using TEOAE;
12/16 Existing program 2 UNHS programs 1) 2-stage TEOAE unilateral fail one or more
Cost per infant screened: with and without follow-up

Universal neonatal hearing screening 217
1,412 newborns tested using AABR
times using the same technology. Screen performed by 2 masters student audiologists and 5 other screeners 2) 2-stage AABR unilateral fail one or more times using the same technology. Screen performed by 26 nursing staff Costs considered Personnel: audiologist, nurse or audiology technician screeners, administration and clerical assistance Equipment: TEOAE and AABR, cart, printer and personal computer Other screening materials: probes, tips, electrodes Paper supplies
(Gorga et al 2001)
Omaha, Nebraska, USA
4,460 newborns at local birthing hospital (97.5% coverage)
13.5/16 Existing program For both well and NICUe
babies: 2-stage DPOAEf followed by second DPOAE if returned for fail in either ear diagnostic ABRg if fail All tests performed by clinical audiologists Costs considered Equipment Disposables Salary and benefits Follow-up diagnostic assessment
Cost per baby screened
(Driscoll et al 2000)
Brisbane, Qld 1,305 infants of mean age 2 months (1.5–2.5 months); voluntary enrolment
11/16 Existing program 1-stage TEOAE screening with refer for diagnostic assessment at auditory clinic if fail recorded in either ear Screening performed by audiologist Costs considered Audiologist’s salary Equipment Maintenance of equipment Replacement costs of TEOAE probe (yearly) Consumables Costs averaged out over a period of 6 years of screening (using estimated 6-year life span of equipment)
Cost per child entering program Cost of screening protocol/ child Cost of diagnostic assessment protocol/ child Cost per child identified with sensorineural/ mixed hearing impairment Cost per child identified with sensorineural/ mixed/conductive hearing impairment Total annual program cost
(Stone et al 2000)
Rapid City, South Dakota, USA
1,002 well newborns 6–72 hours old at first screen
11/16 Existing program 1-stage TEOAE performed in hospital. Fail referred for diagnostic assessment at 8 weeks of age using DPOAE and tympanometry A fail of both tympanometry and DPOAE indicated middle
Cost per screen Cost per infant diagnosed with hearing loss

218 Universal neonatal hearing screening
ear disease and treatment A fail of only DPOAE resulted in testing with AABR Costs considered DPOAE screening equipment Full-time registered nurse Administrator for 1 hour/week Audiology interpretation of results Supplies Follow-up assessment
(Maxon et al 1995)
Rhode Island, USA
4,253 infants born during 6-month period in 1993 595 special care infants 3,658 well infants
11/16 Existing program 2-stage TEOAE program 1st stage performed prior to hospital discharge. If fail recorded, then 2nd stage rescreen 4–6 weeks later. ABR performed by hospital screeners if second fail recorded. Fail of ABR referred for diagnostic audiologic evaluation Costs considered Personnel including trained screening technicians, audiologist, coordinator, clerical assistance Fringe benefits @ 28% of salaries Overhead @ 29% of salaries Supplies Cost of 3 TEOAE and 1 ABR machine, 4 computers, 2 printers (all amortised over 5 years)
Cost per child screened Cost per child identified
(Weirather et al 1997)
Logan, Utah, USA
380 well and NICU newborns (98.4% coverage)
11.5/16 Existing program 2-stage TEOAE Newborns screened prior to discharge. If fail recorded, infants brought back to hospital for stage 2 re-test with TEOAE. If fail recorded then infant referred to hospital audiology department for diagnostic assessment Costs considered Personnel: screening, rescreening, screening management, program management, patient management, scoring Fringe benefits (30% of salaries) Supplies Equipment (not screening equipment – assumed already in place) Overhead (20% of costs)
Cost per baby screened
a Automated auditory brainstem response test; b transient evoked otoacoustic emissions test; c otoacoustic emissions test; d universal neonatal hearing screening; e permanent childhood hearing impairment; f neonatal intensive care unit; g distortion product otoacoustic emissions test; h (conventional) auditory brainstem response test.

Universal neonatal hearing screening 219
Appendix G Excluded studies
Studies that met the inclusion criteria listed in the assessment protocol but on closer inspection were excluded from review are listed below. Studies are grouped by the reason for exclusion. ‘Data not useable’ indicates that the data on relevant outcomes presented in the paper may have been in graphical format or summarised in such a way that raw figures (means, standard deviations, numerators, denominators) could not be extracted. ‘Duplicated data’ means that the results were presented in some form or other in another paper included in this assessment. ‘Not available’ means that the paper was requested via inter-library loan services and could not be retrieved before the submission deadline of this report. It is possible that these studies may not have been relevant (ie met the inclusion criteria) in any event.
Prevalence
Data not useable
Cone Wesson, B., Vohr, B.R. et al (2000). ‘Identification of neonatal hearing impairment: infants with hearing loss’. Ear and Hearing, 21 (5), 488–507.
Das, V K. (1990). ‘Prevalence of otitis media with effusion in children with bilateral sensorineural hearing loss’. Archives of Disease in Childhood, 65 (7), 757–759.
Das, V.K. (1996). ‘Aetiology of bilateral sensorineural hearing impairment in children: A 10 year study’. Archives of Disease in Childhood, 74 (1), 8–12.
Davis, A., Wood, S. et al (1995). ‘Risk factors for hearing disorders: epidemiologic evidence of change over time in the UK’. Journal of the American Academy of Audiology, 6 (5), 365–370.
Finitzo, T.A.K. & O’Neal J. (1998). ‘The newborn with hearing loss: detection in the nursery’. Pediatrics, 102 (6), 1452–1460.
Fortnum, H.M., Marshall, D.H. & Summerfield, A.Q. (2002). ‘Epidemiology of the UK population of hearing-impaired children, including characteristics of those with and without cochlear implants – audiology, aetiology, comorbidity and affluence’. International Journal of Audiology, 41 (3), 170–179.
Kanne, T.J., Schaefer, L. & Perkins, J.A. (1999). ‘Potential pitfalls of initiating a newborn hearing screening program’. Archives of Otolaryngology Head and Neck Surgery, 125 (1), 28–32.
Kok, M.R., van Zanten, G.A. et al (1993). ‘Click-evoked oto-acoustic emissions in 1036 ears of healthy newborns’. Audiology, 32 (4), 213–224.
Kvaerner, K.J. & Arnesen, A.R. (1994). ‘Hearing impairment in Oslo born children 1989-91. Incidence, etiology and diagnostic delay’. Scandinavian Audiology, 23 (4), 233–239.
Maki Torkko, E.M., Lindholm, P.K. et al (1998). ‘Epidemiology of moderate to profound childhood hearing impairments in northern Finland. Any changes in ten years?’. Scandinavian Audiology, 27 (2), 95–103.

220 Universal neonatal hearing screening
Norton, S.J., Gorga, M.P. et al (2000). ‘Identification of neonatal hearing impairment: summary and recommendations’. Ear and Hearing, 21 (5), 529–535.
Stewart, D.L. & Pearlman, A. (1994). ‘Newborn hearing screening’. Journal of the Kentucky Medical Association, 92 (11), 444–449.
Uus, K. & Davis, A.C. (2000). ‘Epidemiology of permanent childhood hearing impairment in Estonia, 1985-1990’. Audiology, 39 (4), 192–197.
Duplicated data
Johnson, J. L., White, K. R. et al (2005). 'A multicenter evaluation of how many infants with permanent hearing loss pass a two-stage otoacoustic emissions/automated auditory brainstem response newborn hearing screening protocol', Pediatrics, 116 (3), 663-672.
Kennedy, C. R., Kimm, L. et al (1998). 'Controlled trial of universal neonatal screening for early identification of permanent childhood hearing impairment', Lancet, 352 (9145), 1957-1964.
Kennedy, C.R. (1999). ‘Controlled trial of universal neonatal screening for early identification of permanent childhood hearing impairment: coverage, positive predictive value, effect on mothers and incremental yield. Wessex Universal Neonatal Screening Trial Group’. Acta Paediatrica, Supplementum, 88 (432), 73–75.
MacAndie, C., Kubba, H. & McFarlane, M. (2003). 'Epidemiology of permanent childhood hearing loss in Glasgow, 1985-1994', Scott Med J, 48 (4), 117-119.
Watkin, P. (1996). ‘Neonatal otoacoustic emission screening and the identification of deafness’. Archives of Disease in Childhood, 74 (1), F16–25.
Not available
Author(s) unknown (2000). ‘Identification of neonatal hearing impairment’. Ear and Hearing, 21 (5), 345–535.
Diagnostic accuracy
Data not useable
Harrison, W.A., Dunnell, J.J. et al (2000). ‘Identification of neonatal hearing impairment: experimental protocol and database management’. Ear and Hearing, 21 (5), 357–372.
Kennedy, C.R., Kimm, L. et al (1991). ‘Otoacoustic emissions and auditory brainstem responses in the newborn’. Archives of Disease in Childhood, 66 (10 Spec No), 1124–1129.
Kennedy, C.R., Kimm, L. et al (1998). ‘Controlled trial of universal neonatal screening for early identification of permanent childhood hearing impairment’. Lancet, 352 (9145), 1957–1964.
Stevens, J.C., Webb, H.D. et al (1987). ‘A comparison of oto-acoustic emissions and brain stem electric response audiometry in the normal newborn and babies admitted to a special care baby unit’. Clinical Physics and Physiological Measurement, 8 (2), 95–104.
Tognola, G., Ravazzani, P. et al (2001). ‘ “Linear” and “derived” otoacoustic emissions in newborns: a comparative study’. Ear and Hearing, 22 (3), 182–190.

Universal neonatal hearing screening 221
Duplicated data
Kennedy, C.R. (1999). ‘Controlled trial of universal neonatal screening for early identification of permanent childhood hearing impairment: coverage, positive predictive value, effect on mothers and incremental yield. Wessex Universal Neonatal Screening Trial Group’. Acta Paediatrica, Supplementum, 88 (432), 73–75.
Screening safety and effectiveness
Data not useable
De Ceulaer, G., Daemers, K. et al (1999). ‘Neonatal hearing screening with transient evoked otoacoustic emissions: a learning curve’. Audiology, 38 (6), 296–302.
De Ceulaer, G., Daemers, K. et al (2001). ‘Neonatal hearing screening with transient evoked otoacoustic emissions – retrospective analysis on performance parameters’. Scandinavian Audiology, Supplementum, (52), 109–111.
Gabbard, S.A., Northern, J.L. & Yoshinaga-Itano, C. (1999). ‘Hearing screening in newborns under 24 hours of age’. Seminars in Hearing, 20 (4), 291–305.
Gorga, M.P., Preissler, K. et al (2001). ‘Some issues relevant to establishing a universal newborn hearing screening program’. Journal of the American Academy of Audiology, 12 (2), 101–112.
Korres, S., Balatsouras, D. G. et al, (2005). 'Overcoming difficulties in implementing a universal newborn hearing screening program', Turk J Pediatr, 47 (3), 203-212.
Korres, S. G., Balatsouras, D. G. et al, (2006). 'Making universal newborn hearing screening a success', Int J Pediatr Otorhinolaryngol, 70 (2), 241-246.
Lim, G. & Fortaleza, K. (2000). ‘Overcoming challenges in newborn hearing screening’. Journal of Perinatology, 20 (8 Pt 2), S138–142.
Mehl, A.L. & Thomson, V. (1998). ‘Newborn hearing screening: the great omission’. Pediatrics, 101 (1), E4.
Mehl, A.L. & Thomson, V. (2002). ‘The Colorado newborn hearing screening project, 1992-1999: on the threshold of effective population-based universal newborn hearing screening’. Pediatrics, 109 (1), E7.
Mathur, N. N. & Dhawan, R., (2007). 'An alternative strategy for universal infant hearing screening in tertiary hospitals with a high delivery rate, within a developing country, using transient evoked oto-acoustic emissions and brainstem evoked response audiometry', Journal Of Laryngology And Otology, 121 (7), 639-643.
Owen, M., Webb, M. & Evans, K. (2001). ‘Community based universal neonatal hearing screening by health visitors using otoacoustic emissions’. Archives of Disease in Childhood, 84 (3), F157–162.
Parving, A. & Salomon, G. (1996). ‘The effect of neonatal universal hearing screening in a health surveillance perspective – a controlled study of two health authority districts’. Audiology, 35 (3), 158–168.

222 Universal neonatal hearing screening
Stuart, A., Moretz, M. & Yang, E.Y. (2000). ‘An investigation of maternal stress after neonatal hearing screening’. American Journal of Audiology, 9 (2), 135–141.
Swedish Council on Technology Assessment in Health, C. (2004). 'Universal newborn hearing screening - early assessment briefs (Alert) (Structured abstract)'.
Tait, K. (1997). ‘A model for success: creating the model for rural success for newborn hearing screening’. Neonatal Intensive Care, 10 (5), 34–35.
Wroblewska-Seniuk, K., Chojnacka, K. et al, (2005). 'The results of newborn hearing screening by means of transient evoked otoacoustic emissions', Int J Pediatr Otorhinolaryngol, 69 (10), 1351-1357.
Duplicated data
Barry, H. (2000). ‘Is screening for newborn hearing loss cost-effective?’ Evidence Based Practice, 3 (8), 8, insert 2p NLI: 100894030.
Corabian, P., Eng, K. et al (2007). IHE Report: Screening Newborns for Hearing,
Insititute of Health Economics, Alberta, Canada.
Lin, H., Shu, M. et al (2003). 'Establishing a newborn hearing screening programme in Taiwan', Asia Pacific Journal of Speech, Language & Hearing, 8 (3), 174.
Lin, H. C., Shu, M. T. et al (2002). 'A universal newborn hearing screening program in Taiwan', International Journal of Pediatric Otorhinolaryngology, 63 (3), 209-218.
Prieve, B.A. & Stevens, F. (2000). ‘The New York State universal newborn hearing screening demonstration project: introduction and overview’. Ear and Hearing, 21 (2), 85–91.
Slawson, D. (2002). ‘Can universal newborn hearing screening improve language outcomes in children identified with profound bilateral permanent hearing loss (PHL)?’ Evidence Based Practice, 5 (1), 8, insert 2p NLI: 100894030.
Spivak, L., Dalzell, L. et al (2000). ‘New York State universal newborn hearing screening demonstration project: inpatient outcome measures’. Ear and Hearing, 21 (2), 92–103.
White, K.R., Vohr, B.R. & Behrens, T.R. (1993). ‘Universal newborn hearing screening using transient evoked otoacoustic emissions: Results of the Rhode Island hearing assessment project’. Seminars in Hearing, 14 (1), 18–29.
White, K.R., Vohr, B.R. et al (1994). ‘Screening all newborns for hearing loss using transient evoked otoacoustic emissions’. International Journal of Pediatric Otorhinolaryngology, 29 (3), 203–217.
Not available
De Capua, B., Tozzi, A. et al (1999). ‘Neonatal audiological screening with transient evocated otoacoustic emission (TEOAE): Results and comments about one years of experience’. Otorinolaringologia Pediatrica, 10 (1–2), 5–7.

Universal neonatal hearing screening 223
El-Naggar, M. & Hashlamoun, M., (2005). 'Paediatric hearing assessment and screening clinic at Fujairah: Analysis of the results of the first 6 months of clinic practice', Emirates Medical Journal, 23 (1), 15-20.
Jacobson, C.A. & Jacobson, J.T. (1990). ‘Follow-up services in newborn hearing screening programs’. Journal of the American Academy of Audiology, 1 (4), 181–186.
Joseph, R., Tan, H. K. et al, (2003). 'Mass newborn screening for hearing impairment', Southeast Asian J Trop Med Public Health, 34 Suppl 3, 229-230.
Mahulja-Stamenkovic, V., Prpic, I. et al, (2005). 'Incidence of hearing loss assessed by the universal newborn hearing screening in the region of Rijeka', Paediatria Croatica, 49 (4), 219-222.
Molteni, G., (2006). 'Early detection of newborn hearing impairment by transiently evoked otoacoustic emissions and auditory evoked potentials. Personal experience in 10,454 children', Otorinolaringologia, 56 (2), 93-96.
Paul, A. K., (2003). 'Hearing loss in children: Need for early detection and intervention', Indian Journal of Practical Pediatrics, 5 (4), 353-355.
Quintos, M. R., Isleta, P. F. et al, (2003). 'Newborn hearing screening using the evoked otoacoustic emission: The Philippine General Hospital experience', Southeast Asian J Trop Med Public Health, 34 Suppl 3, 231-233.

224 Universal neonatal hearing screening
Appendix H Guidelines for using screening devices
Extract from (Bailey 2003).
Use of the Natus Algo Portable AABR Screener
This protocol describes the use and care of the Natus Algo Portable AABR Screener in the Western Australian Newborn Hearing Screening Programme. Further information is found in the user manual. An instructional video is available.
Contents
1. Description of the Natus Algo Portable AABR Screener
2. How does it work?
3. Associated equipment
4. How to screen a baby
5. Infection control and how to clean the machine after use
6. Battery charging
7. Routine checks
1. Description of the Natus Algo Portable AABR Screener
The Natus Algo Portable AABR Screening equipment consists of:
• the screening unit
• attached printer
• attached earphone cable and sensor cable.
Each unit has a user manual; storage bag; charging unit; Acoustic Check kit; and small screwdriver.
2. How does it work?
The machine measures auditory brainstem responses. Earphones attached to the baby’s ear deliver clicking noises set at 35dB nHL. Sensors that are attached to the baby’s forehead, nape and shoulder record the brainwave response to the stimuli. The screener compares the baby’s responses to the stimuli to a template derived from other babies (AABR). It measures the probability that an adequate ABR signal is present. The machine indicates whether a Pass response has been obtained, otherwise further

Universal neonatal hearing screening 225
screening or diagnostic testing is indicated. The machine is not a diagnostic machine and cannot be used to indicate the degree of hearing loss.
A Pass response indicates normal middle ear, cochlear and retro-cochlear function.
If a Pass response is not obtained, further screening is required. Reasons that a Pass response will not be obtained include:
• the ear cups are not attached to the baby’s ear or are compressing the ear canal.
• there is too much noise (ambient light on)
• the baby is too awake or active (myogenic light on)
• the sensors are not in the correct places or are not well adhered to the skin (high impedance)
• there is other interference such as other equipment in the area or the sensor or its wires are in contact with other equipment
• there is a hearing loss.
The screen will generally run rapidly if the baby is settled, and the impedance is low. The screening device is designed for use in babies between 34 weeks gestational age and 6 months only.
3. Associated equipment
It should be used with disposable Algo Paks (set of ear cups and 3 jelly sensors) supplied by Natus only.
For skin preparation:
• mild baby liquid soap
• gauze squares
For cleaning:
• alcohol wipes/other cleaning agent
4. How to screen a baby
It should be done in a quiet room when the baby is asleep or in a quiet state. Babies can be screened while feeding although this will prolong the screen. This should only be attempted when feeding has been well established and the mother and baby are comfortable with the feeding process. At the beginning of a feed, babies may make too much noise but generally they quieten down as the feed progresses. The screen will progress very slowly if the baby is wide awake and looking around even if the baby is quiet.

226 Universal neonatal hearing screening
• Always tell parents the reasons why a result may not be obtained prior to screening.
• Use the term ‘stickers’ rather than electrodes when explaining the screening process to parents.
• Switch the machine on prior to attaching sensors to the baby and remove the sensors before switching off the machine.
• In many cases, it is easier to leave the machine in the carry bag while the screen is being conducted.
1. See the user manual for full instructions how to perform the screen and for sensor placement.
2. The better the sensor placement and contact with the skin, the faster the screen will run.
3. If the baby needs skin preparation, use only mild liquid baby soap on a gauze square moistened with warm water. Be very gentle as babies have delicate skin. Moistening the sensor and holding it in place for a few seconds may improve contact and lower impedance.
4. Place the sensors as follows
1. white - nape
2. green - shoulder (common)
3. black - high on forehead
5. Attach the earphones to the acoustic cables when still adhered to the paper card prior to attaching to the baby:
1. red - right ear
2. blue - left ear
When attached to baby, the cables should emerge towards the top of the baby’s head.
6. Commence the screen as instructed in user manual.
7. During the screen, the display shows the number of good sweeps completed (SWP) and the LR (Likelihood ratio). The screen is complete when the LR reaches at least 160. The minimum number of sweeps is 1,000 and the maximum is 15,000. The LR is updated every 500 sweeps.
8. If the LR is not increasing after about 2000 sweeps and the baby is quiet, stop the screen and check the ear cup is correctly positioned and the acoustic cable still attached.

Universal neonatal hearing screening 227
9. If the myogenic light is lit, try and settle baby. Check also if any sensor wires are in contact with each other.
10. If impedance is a problem, try re-applying the sensors. A new set of sensors may be required.
11. Sometimes other medical equipment may interfere with the screen. Consult with nursing staff to see if this can be corrected.
12. Babies can be screened while in incubators but the screen may progress very slowly.
13. When the screen is completed, use gauze moistened with warm water to help remove the sensors and ear cups from the baby.
5. Infection control and how to clean the machine after use
• Wash hands thoroughly before and after handling the baby.
• Use a new set of disposable sensors and ear couplers for each baby.
• At the completion of the test, discard the sensors and ear couplers. Wipe the sensor cables and acoustic transducers with an alcohol swab and allow them to dry.
• Carefully roll up the cables and store inside the carry case.
6. Battery charging
When fully charged the battery will last for approximately 10 hours of continuous screening. See the user manual for instructions on how to charge the battery. The machine should be charged overnight on a regular basis. To prolong the battery life, the battery should have a deep discharge prior to recharging. As this takes a lengthy period of time, it is best not to do it until there are 2 or less of the 4 battery charge level lights lit on the machine. At smaller sites, it may be sufficient to charge the battery about every 4-6 weeks.
7. Routine checks and maintenance
• Always inspect the acoustic and sensor cables prior to use: Attach the sensor clips to the Acoustic Check kits, start the machine and listen to the acoustic cables to hear if clicks are present.
• Perform the equipment checks listed in the user manual weekly and record that it has been done in the record book. If the machine passes these checks, it can be used. If not, do not use it and contact the coordinator.
• See the user manual for instructions on how to load a new printer roll. Ensure that the machine is switched off after loading the paper in order to preserve the battery.
• The Algo portable screener and charging unit should have a hospital safety check annually and before being used after being repaired.

228 Universal neonatal hearing screening
• The acoustic cables require yearly calibration by Natus. Each set of cables has a calibration certificate with the date when the calibration is due. Contact Scanmedics to arrange the loan of replacement cables at least 2 months before this is due.
Extract from (Bailey 2003).
Use of the ECHOCHECK hand-held ILO OAE Screener
This protocol describes the use and care of the Echocheck in the Western Australian Newborn Hearing Screening Programme. Further information is found in the user manual.
Contents
1. Description of the Echocheck
2. How does it work?
3. Associated equipment
4. How to screen a baby
5. Infection control and how to clean the machine after use
6. Battery charging
7. Routine checks
1. Description of the Echocheck
The Echocheck consists of a hand held, battery operated unit; and a detachable cable and probe which uses disposable ear tips for each use. The probe uses replaceable coupler tubes (changed when contaminated). Replacement probe/coupler covers are available. Each unit has a user manual; storage bag, charging unit; test cavity and test plug.
2. How does it work?
The machine measures Transient Evoked OtoAcoustic Emissions (TEOAEs or OAEs for short) and it concentrates on the main speech frequency band of 1.6-3.6Hz. The Echocheck is a screening device so no interpretation is required. The green light indicates a pass response, otherwise further screening is indicated. The machine is not a diagnostic machine and cannot be used to indicate the degree of hearing loss.
TEOAEs are low intensity sounds originating from the outer hair cells of the cochlear in response to stimuli. A probe that contains a very small microphone is placed in the baby’s ear. When switched on a continuous clicking noise is emitted from the probe (the stimulus). The microphone then detects the response. By various processes, the machine sorts out TEOAEs from other noises. If the TEOAEs are at least 6dB louder than other noises, a green pass light is obtained. If they are between 3-6dB louder, an

Universal neonatal hearing screening 229
orange light is obtained and the screen should be repeated later, preferably in quieter conditions.
A pass response indicates normal middle ear and cochlear function.
If a pass response is not obtained, further screening is required. A pass response will not be obtained if :
• the probe does not fit in the ear canal properly
• there is too much noise (either from the baby, such as noisy breathing, or the general environment)
• there is debris in the ear canal such as vernix or other birth products or wax
• there is middle ear fluid
• there is a hearing loss.
The younger the baby is, the more likely they are to have transient middle ear fluid and debris in the ear canal. We have found that babies have less than a 60% chance of passing if less than 24 hours old. By the time the baby is about 3 days old or more, they have about a 90% or more chance of passing.
3. Associated equipment
• Three sizes of disposable ear tips and spare coupler tubes should be available at all times for hospital-based newborn screening:
Tip sizes -
1. T4.5C most common used
2. T5.5B for larger/older babies
3. T3E for very small babies
4. Community based programmes may require larger size tips.
• Alcohol wipes/other cleaning agent
These should be stored in a suitable storage container such as a small, divided plastic craft box.
4. How to screen a baby
To optimise the chances of a baby passing, the screen should be done as late as possible during the hospital stay. The exact timing will depend on the length of stay in hospital at individual hospitals. Women who have had a caesarean section generally have a longer stay than those who have a vaginal delivery so the screening can be delayed.
It should be done in a quiet room when the baby is asleep or in a quiet state. Babies can be screened while feeding. This should only be attempted when feeding has been well

230 Universal neonatal hearing screening
established and the mother and baby are comfortable with the feeding process. At the beginning of a feed, babies may make too much noise but generally they quieten down as the feed progresses.
• Always tell parents the reasons why a result may not be obtained (eg noise, debris etc) prior to screening.
• See the user manual for instructions how to perform the screen.
• If the Stimulus OK light is not illuminated, check if the cable is properly attached to the machine and check if there is debris blocking the ear tip.
• Debris in the ear tip can be removed by taking the ear tip off the probe and cleaning/squeezing it with an alcohol swab. If necessary, a new ear tip can be used.
• Check that the coupler tubes are clear and change them if necessary.
• If there is debris in the ear, sometimes this can be removed by reinserting the cleaned ear tip/probe in the ear, rotating the tip/probe in the ear canal and repeating the cleaning process.
5. Infection control and how to clean the machine after use
• Wash hands thoroughly before and after handling the baby.
• Use a new ear tip for each baby.
• After completion of the test, remove used ear tip from the probe casing and discard it.
• Wipe the probe casing, cable and control panel with an alcohol swab and allow them to dry. If necessary, dry with a tissue.
• Check that the coupler tubes are free of debris before and after use. If debris is present, discard the contaminated coupler tubes and insert new ones (see user manual).
6. Battery charging
The Echocheck has an internal, rechargeable battery. When fully charged, the battery will last for about 6 hours of continuous screening. The machine should be charged overnight on a regular basis. To prolong the battery life, the battery should be allowed to ‘run down’ before being recharged. At smaller sites, it may be sufficient to charge the battery about once a fortnight. Instructions on how to charge the battery are in the user manual.
7. Routine checks and maintenance
Always inspect the Echocheck, probe and its cable before use:

Universal neonatal hearing screening 231
• check that the coupler tubes are free of debris before and after use. If debris is present, discard the contaminated coupler tubes and insert new ones (see user manual).
• if the back of the probe casing is missing, replace the whole casing.
• if the cable has white wiring visible near the probe, obtain a new probe. Careful handling of the probe and its cable will prolong its life.
• if the front panel of the machine is cracked, contact the coordinator to arrange to have this replaced.
Routine checks should be carried out weekly or after the coupler tubes or probe is changed. Record the results of the tests in the Echocheck record book. See the user manual for details of the probe checks. If the machine passes these checks it can be used. If not, do not use it and contact the coordinator.
The Echocheck and charging unit should have a hospital safety check annually and before being used after being repaired.

232 Universal neonatal hearing screening
Appendix I Analysis of published economic evaluations (up to 2003)
Comparison of universal and targeted screening in the short term
Five studies presenting economic models of universal neonatal hearing screening (UNHS) were identified and have been critically appraised.
Two of these studies compared targeted and universal screening (Kemper & Downs 2000; Keren et al 2002). A summary of the costs included in the evaluation of UNHS and targeted screening protocols in both studies is provided in Table A.
Table A Resource items considered in studies comparing modelled universal neonatal and targeted hearing screening programs
Resource items Targeted screening Universal screening 2-stage AABR
(Keren et al 2002)
2-stage TEOAE–AABR (Kemper &
Downs 2000)
2-stage TEOAE–AABR
(Keren et al 2002)
2-stage TEOAE–AABR (Kemper &
Downs 2000)
Capital equipment A A OAE instrument n/a AABR instrument Computer
Recurrent items A A OAE probes n/a ABR electrodes OAE probe tips n/a Ear couplers/muffins Cables Machine calibration Other consumables (eg paper) Screener training Overheads
Personnel A A Nurse or other trained screener Audiologist Administrative support
Follow-up Patient and family
Other sectors A = assumed, indicated as included but not described; AABR = automated auditory brainstem response test; TEOAE = transient evoked otoacoustic emissions test; OAE = otoacoustic emissions; = included; = not included; n/a = not applicable.
In the higher quality study (Keren et al 2002) cost-effectiveness was evaluated from a societal perspective for selective (targeted) and universal screening in a hypothetical cohort of 80,000 newborns from one US state. This cohort consisted of 10,400 high-risk and 69,600 low-risk infants. Under targeted screening only infants with identified risk

Universal neonatal hearing screening 233
factors for congenital deafness were screened (Box 10). The decision tree for this model is shown in Figure 11.
Box 10 Risk factors for congenital deafness (Joint Committee on Infant Hearing 2000)
Figure 11 Decision tree for universal and targeted neonatal hearing screening model (Keren et al 2002)
Residence in neonatal intensive care unit / special care baby unit for ≥48 hours Prolonged usage of aminoglycosides Family history of permanent childhood deafness Craniofacial abnormality noticeable at birth Perinatal infection (either suspected or confirmed) Birthweight <1.5 kilograms Birth asphyxia Chromosomal abnormality, including Down syndrome Exchange transfusion or intrauterine transfusion

234 Universal neonatal hearing screening
Based on literature from published universal neonatal hearing screening (UNHS) programs reporting an estimate of 1.6 cases of permanent childhood hearing impairment (PCHI) per 1,000 births, the cohort was assumed to contain 128 infants with permanent hearing impairment (Aidan et al 1999; Clemens et al 2000; Kennedy et al 1998; Mason & Herrmann 1998). The point estimates were based on an 80 per cent coverage of high-risk infants through targeted screening and 100 per cent coverage for all infants using UNHS. A referral rate for diagnostic evaluation of 0.18 per cent was assumed for targeted screening and 1.6 per cent for UNHS. For both programs it was assumed that 77 per cent of babies referred for diagnostic assessment were followed up (Prieve et al 2000). Yield from the two screening programs was estimated at 48 and 91 per cent for targeted and universal screening, respectively. Resources considered in the analysis were those of screening (equipment, consumables and staff wages); follow-up diagnostic assessment; and the societal costs of loss of productivity, requirement for special education, vocational rehabilitation and use of assistive devices and medical services (Table A) (Vohr et al 1998).
The incremental cost of diagnosing an infant with bilateral PCHI by 6 months of age was found to be higher with UNHS (Table B). Sensitivity analysis identified two variables with the greatest effects on the incremental cost. Reducing the coverage of high-risk infants in targeted screening from 100 per cent to 40 per cent reduced the incremental cost-effectiveness ratio (ICER) of universal screening compared to targeted screening from $76,000 to $45,000. Increasing the diagnostic follow-up in both programs from 50 per cent to 100 per cent increased the ICER from $52,000 to $77,000 per child identified by 6 months of age using UNHS compared to targeted screening. The authors state that the higher incremental cost of UNHS is due largely to the greater number of patients referred for diagnostic evaluation. In targeted screening the number of patients referred was estimated to be 145 of 80,000 babies (0.2%), while use of UNHS would lead to referral of nearly 10 times that number at 1,314 (1.6%). Despite the short-term costs of UNHS being substantially higher than those for the targeted or no screening options, estimates of long-term costs resulted in savings using UNHS over the lifetime of a child who developed normal language. The inclusion of long-term societal costs resulted in an incremental saving of $2 million per child with normal language using targeted screening, and a further saving of $1.2 million per child using UNHS.

Universal neonatal hearing screening 235
Table B Published economic models of universal vs targeted neonatal hearing screening
Study Population Quality Ratio Protocol / Results ($AUS) No screening Targeted
screening
2-stage AABR
Universal screening 2-stage OAE and AABR
Incremental cost per infant diagnosed by 6 months with bilateral hearing impairment
0 22,820
61,600b
Varying coverage of high-risk infants from 100% to 40%
45,800–76,400
Varying follow-up diagnostic evaluation from 50% to 100%
52,800–77,800
(Keren et al 2002)
Hypothetical cohort of 80,000 infants from one US State 10,400 high-risk, 69,600 low-risk infants
15/16
Incremental cost reduction per child with bilateral hearing impairment possessing normal language [see also Table J]
0 2,030,000a 1,212,000b
Targeted screening 2-stage TEOAE and AABR
Universal screening 2-stage TEOAE and AABR
Cost per case of bilateral hearing impairment detected
4,640 17,350
(Kemper & Downs 2000)
Hypothetical cohort of 100,000 infants
13/16
Cost per extra case of bilateral hearing impairment detected
35,650
a ICER targeted vs no screening; b ICER UNHS vs targeted (assuming 80% of high-risk patients screened in targeted screening scenario and 77% of infants followed up with diagnostic assessment after positive screen in both scenarios). AABR = automated auditory brainstem response test; OAE = otoacoustic emissions test; TEOAE = transient evoked otoacoustic emissions test.
The other study of the cost-effectiveness of targeted versus universal screening was modelled from a health care perspective in a population of 100,000 hypothetical newborns (Kemper & Downs 2000). The decision tree for this model is presented in Figure 12.
Based on the results of other evaluations of neonatal hearing screening (Davis et al 1997; Maxon et al 1995) and a population-based surveillance program (Van Naarden et al 2000), the prevalence of bilateral hearing loss was estimated to be 0.11 per cent or 1.1 per 1,000 newborns (range 0.10–0.59%). From the model, targeted screening resulted in 67 referrals for diagnostic assessment from the total cohort of 100,000 (0.07%). UNHS resulted in 406 referrals or 0.4 per cent of the total cohort. Cost analysis was performed from a health care perspective. If the cost of risk screening was assumed to be $1 per child screened (range $0.5–$15), the authors determined that for UNHS the use of automated transient evoked otoacoustic emissions (TEOAE) testing would cost $7.42 (range $5–$15) and automated auditory brainstem response (AABR) testing $25 (range $15–$40) per child screened. Diagnostic auditory brainstem response (ABR) testing would cost $150 (range $100–$200) per child sent for assessment. Only the process measures of cost per case identified and cost per extra case identified were reported. Short- or long-term outcomes were not considered. In agreement with the previous study (Keren et al 2002), the authors determined that the incremental cost per case of

236 Universal neonatal hearing screening
Summary of cost-effectiveness of modelled universal and targeted neonatal hearing screening programs, contrasting the short term and the long term
While both studies determined that universal neonatal hearing screening would, in the short term, be more expensive and less cost-effective to operate than a targeted screening program, modelling of long-term costs by Keren and colleagues (2002) suggested that identifying a larger proportion of hearing-impaired infants at an early stage (ie ≤6 months of age) would result in savings in other sectors (such as education and social welfare) that would far outweigh the initial expense. Disparity in the incremental cost-effectiveness ratio between these two studies, for incremental cost per case identified, would probably stem from the different referral rates used to determine the costs of follow-up diagnostic assessment. In the study by Kemper & Downs (2000), the assumed difference in referral rates from universal, as opposed to targeted, hearing screening programs was much smaller than that assumed by Keren and colleagues (2002). With similar assumed differences in referral rates, the overall cost of diagnostic follow-up for each of the programs presented by Kemper & Downs (2000) would be closer, reducing the incremental cost.
identifying bilateral PCHI was more expensive with UNHS than for targeted screening (Table B). However, it was predicted that UNHS would detect 40 per cent more PCHI cases compared to targeted screening. The resulting cost of $35,650 per extra case detected would be due largely to the increase in the number of false positives (from 16 to 320) that would be referred for follow-up diagnostic evaluation.
Figure 12 Decision tree for universal and targeted neonatal hearing screening model (Kemper & Downs 2000)

Universal neonatal hearing screening 237
Comparison of modelled universal neonatal hearing screening programs in the short term
Three identified studies compared the costs and outcomes of models of different protocols for universal neonatal hearing screening (UNHS) (ie automated auditory brainstem response (AABR) vs otoacoustic emissions (OAE)) (Boshuizen et al 2001; Gorga et al 2001; Kezirian et al 2001). All studies took a health care sector perspective. A summary of the costs considered in all screening protocols is presented in Table C.
The highest quality study examined the cost effectiveness of four different screening methods: one-stage AABR and OAE–AABR, and two-stage AABR and OAE on a hypothetical cohort of 2,000 babies born in one hospital in 1 year (Kezirian et al 2001). The one-stage OAE–AABR technique involved performing an AABR directly after a positive (fail) result on the initial OAE test. The decision tree for this model is presented in Figure 13.
Table C Resource items considered in studies comparing different modelled universal neonatal hearing screening programs
Resource item (Kezirian et al 2001) 1-stage AABR, 1 stage
OAE–AABRa, 2-stage OAE, 2-stage AABR
(Gorga et al 2001) 1-stage AABR, 1-stage OAE,
2-stage OAE–AABR
(Boshuizen et al 2001) 2-stage OAE, 2-stage AABR,
3-stage OAE
Capital equipment Ab A OAE instrument AABR instrument Computer
Recurrent items A A A OAE probes ABR electrodes OAE probe tips Ear couplers/muffins Cables Machine calibration Other consumables (eg paper)
Screener training Overheads
Personnel A A A Nurse or other trained screener
Audiologist Administrative support
Follow-up Patient and family
Other sectors a Protocol considered 1-stage but AABR performed immediately after OAE fail result; b A = assumed (indicated as included but not described). AABR = automated auditory brainstem response test; ABR = auditory brainstem response test; OAE = otoacoustic emissions; = included; = not included.

238 Universal neonatal hearing screening
Figure 13 Decision tree for modelled universal neonatal hearing screening protocols (Kezirian et al 2001)
Based on previous studies (Watkin et al 1990; White 1997), the prevalence of combined bilateral or unilateral hearing loss was estimated to be 3.5 per 1,000 infants. Referral rates of each program were not provided but were used in cost calculations. Costs included were those directly absorbed by the hospital such as equipment, personnel, overheads and clerical, and the cost of follow-up diagnostic evaluation (Table C). Costing information was obtained from a report compiled by the National Centre for Hearing Assessment and Management (NCHAM) at Utah State University (NCHAM 2003). The method with the least cost per infant screened was found to be two-stage OAE (Table D), which was also the most cost-effective in terms of the cost per infant identified with unilateral or bilateral permanent childhood hearing impairment (PCHI). The least cost-effective method was a one-stage AABR. These results were consistent when best case – worst case scenarios were examined. Although the one-stage AABR was determined as identifying the greatest number of infants with hearing loss, analysis revealed that more than $126,000 of extra funding would be required under this protocol in order to identify one more case than with two-stage OAE (sic). However, exclusion of infants lost to follow-up from effectiveness calculations, and the use of sensitivity and specificity values from studies examining targeted (ie ‘at-risk’) infants means that these results are likely to be conservative and should be regarded with caution.
In a hypothetical cohort of 4,000 babies, the cost-effectiveness of one-stage AABR, one-stage OAE or two-stage OAE followed by AABR was modelled (Gorga et al 2001). The decision tree for this model is presented in Figure 14.

Universal neonatal hearing screening 239
Table D Published economic models of various universal neonatal hearing screening protocols
Study Population Quality Ratio Protocol / Results ($AUS) 1-stage
AABR 2-stage AABR
1-stage OAE–AABRa
2-stage OAE
Cost per infant screened
35 28 28 18
Best case – worse caseb
26–70 25–46 20–45 14–28
Cost per infant identified with hearing loss
13,350 11,430 11,270 7,200
Kezirian et al 2001
Hypothetical cohort of 2,000 births in one hospital in 1 year
13/16
Best case – worse caseb
9,680–28,020 9,370–20,290 7,610– 20,230 5,240–12,560
1-stage AABR 1-stage OAE 2-stage OAE–AABR
Cost per baby screenedc
32 33 24
Gorga et al 2001
Hypothetical cohort of 4,000 babies born in 1 year
12/16
Sensitivity analysisd
27–218 31–104 16–280
2-stage OAE (CHCf)
2-stage AABR (CHC)
3-stage OAE (CHC)
2-stage OAE (CHC)g
2-stage OAE (home)
2-stage OAE (CHC + home)
Cost per child screened
29 41 25 23 33 28
Boshuizen et al 2001
All newborn children not admitted to NICUe
10.5/16
Sensitivity analysish
± 3 ± 4 ± 2 ± 2 ± 4 ± 2
Cost per child detected with hearing loss ≥40 dB in the better ear
40,880 57,380 35,240 33,130 45,250 38,630
Sensitivity analysish
± 9020 ± 13250 ± 7610 ± 8310 ± 11560 ± 8450
a Considered 1-stage in hospital: AABR test performed if baby fails initial OAE; b worst case scenario when costs maximised and sensitivity/ specificity of the protocol is minimised; in the best case scenario the values are the reverse; c includes costs of follow-up for 1-stage AABR and 2-stage OAE–AABR of 2% and for 1-stage OAE of 8%; d based on number of births per year ranging from 8,000 to 25; e NICU = neonatal intensive care unit; f CHC = child health clinic; g detection of bilateral losses only; h sensitivity expressed as the standard error determined from 500 simulations using Monte-Carlo simulation model. AABR = automated auditory brainstem response test; OAE = otoacoustic emissions test.

240 Universal neonatal hearing screening
Figure 14 Decision tree for modelled universal neonatal hearing screening protocols (Gorga et al 2001)
Coverage was assumed to be 100 per cent and the referral rate for diagnostic assessment was assumed to be 2 per cent for AABR and 8 per cent for OAE testing (no source given). Two-stage OAE with AABR was assumed to have a final referral rate that was the same as one-stage AABR, namely 2 per cent. Costs included in this study were for capital equipment (screening tools), disposables, salaries and employee benefits (Table C). Follow-up costs of babies returning a positive screening test for bilateral PCHI were estimated at $280 per baby. Based only on the cost per baby screened, the two-stage OAE followed by AABR was found to be the most cost-effective (Table D). Although the follow-up rate was assumed to be the same for both one-stage AABR and two-stage OAE–AABR (2%), the six-fold greater expense of disposables used in screening 4,000 newborns initially with AABR ($40,000 vs $7,200 for the 2-stage) makes this method less cost-effective than an initial screen with OAE. Sensitivity analysis varied the number of babies born in the hospital in a 5-year period (the assumed useful life of the screening equipment) from between 25 and 8,000 babies per year. As expected, using any of the programs became more expensive if fewer babies were born to the hospital. This is also illustrated when comparing similar programs, as modelled by Kezirian et al (2001) using a birth rate of 2,000 babies per year.
In the only non-US study, Boshuizen and colleagues (2001) modelled the cost-effectiveness of six different existing programs aimed at identifying both unilateral and bilateral hearing impairment in an unspecified cohort of newborn infants not admitted to a neonatal intensive care unit. Variation in the programs consisted of two- or three-stage screening, testing at a child health clinic (CHC) or at home, identification of unilateral and/or bilateral hearing impairment, and use of automated OAE or AABR tests (Figure 15).

Universal neonatal hearing screening 241
Summary of modelled universal neonatal hearing screening protocols in the short term
In three modelled evaluations of universal neonatal hearing screening protocols, two- or three-stage otoacoustic emissions (OAE) screening, along with two-stage OAE and automated auditory brainstem response screening, were recognised as the most cost-effective methods in the short term for identifying permanent childhood hearing impairment. While costs per child screened are similar, costs per child identified are substantially different in the two studies (Kezirian et al 2001; Boshuizen et al 2001). This could only be due to differences in referral rates and/or costs assumed for diagnostic testing, neither of which can be compared from the information published.
Figure 15 Decision tree for modelled universal neonatal hearing screening protocols (Boshuizen et al 2001)
There was no mention of the coverage obtained by any of the programs. The percentage of infants referred for diagnostic testing for the six programs was determined to range from 1.8 ± 0.6 per cent for three-stage OAE to 3.6 ± 1.0 per cent for two-stage OAE. The perspective was that of the medical system in the Netherlands. Costs included equipment depreciation, personnel, consumables, travel costs (of screeners), training, administration and follow-up diagnostic testing (Table C). The study reported the costs per child screened and per child detected with PCHI. The most cost-effective program was found to be a two-stage screen with OAE performed at a CHC, with babies who tested positive for bilateral hearing impairment being referred for diagnostic assessment (Table D). However, if the criteria for a diagnostic referral included infants testing positive for either unilateral or bilateral hearing impairment, then a three-stage screen using OAE at the CHC was found to be the most cost-effective program. These conclusions were mirrored in analysis of the cost per child detected with a hearing loss of ≥40 dB in the better ear.

242 Universal neonatal hearing screening
Comparison of existing universal neonatal hearing screening programs in the short term
Seven studies were included that performed an economic analysis on programs that already existed within their health system (Driscoll et al 2000; Gorga et al 2001; Lemons et al 2002; Maxon et al 1995; Stone et al 2000; Vohr et al 2001; Weirather et al 1997). Again, all included studies took a health care sector perspective.
Table E Resource items considered in studies comparing actual UNHS programs
(Vohr et al 2001)
1-stage
AABR or TEOAE, 2-stage TEOAE– AABR
(Gorga et al 2001)
2-stage DPOAE
(Lemons et al 2002)
2-stage
TEOAE or AABR
(Weirather et al 1997)
2-stage TEOAE
(Driscoll et al 2000) 1-stage TEOAE
(Maxon et al 1995)
2-stage TEOAE
(Stone et al 2000)
1-stage DPOAE
Capital equipment OAE instrument AABR instrument n/a n/a Computer
Recurrent items A A A A A A OAE probes ABR electrodes OAE probe tips Ear couplers/muffins
Cables Machine calibration Other consumables (eg paper)
Screener training Overheads
Personnel Nurse or other trained screener
n/a n/a
Audiologist Administrative support
n/a
Follow-up Patient and family
Other sectors A = assumed (indicated as included but not described); AABR = automated auditory brainstem response test; OAE = otoacoustic emissions test; TEOAE = transient evoked otoacoustic emissions test; DPOAE = distortion product otoacoustic emissions test; = included; = not included; n/a = not applicable.
In a high quality retrospective study, the cost-effectiveness of three universal neonatal hearing screening (UNHS) programs was compared on a total of 12,081 sequentially-tested well newborns at five different American hospitals (Vohr et al 2001). Each hospital followed one of three protocols: one-stage transient evoked otoacoustic emissions (TEOAE); one-stage automated auditory brainstem response (AABR); or two-stage TEOAE followed by AABR (Figure 16). In reality, the first stage of each of the

Universal neonatal hearing screening 243
protocols consisted of testing with the designated screening method prior to hospital discharge, and if the infant failed the test in both ears then the same test was administered again. For the one-stage protocols, infants failing the (second) test were referred for diagnostic testing. In the two-stage protocol, infants failing TEOAE (twice) were then tested with AABR post-discharge. Infants failing the AABR were then referred on for diagnostic assessment. In all cases nurses performed the screenings, although an audiologist interpreted the TEOAE results.
Figure 16 Screening protocols for existing 1- and 2-stage universal neonatal hearing screening programs (Vohr et al 2001)
Costs considered in this cost-effectiveness analysis were the wages of the audiologist, any administration and clerical support, and the time for training of the audiologist and the nurse screeners. The costs of purchasing the TEOAE and AABR equipment along with all screening supplies and overheads were also considered. Failure and referral rates were determined using the retrospective cohort data, while the costing was performed on a hypothetical population of 1,500 newborns. The authors assumed that for every 1,500 infants, two new pieces of equipment were required for first-stage testing and one new piece of equipment was needed for second-stage testing. The cost of follow-up diagnostic assessment was also included in each protocol. Outcomes of interest were the cost per child tested and cost per child identified with bilateral permanent childhood hearing impairment (PCHI).
Results of all three protocols are similar (Table F). While the TEOAE technology was the cheapest to purchase, it had the highest referral rate to diagnostic assessment (6.5%), resulting in the highest post-discharge costs. Conversely, one-stage AABR was the most expensive technology to purchase but resulted in the lowest referral rate (3.2%). It must be remembered that these one-stage protocols actually consist of multiple tests using the same technology in the event of an initial failed screening test. This would result in lower referral rates than might be expected if only one test was performed prior to discharge. The two-stage program yielded an intermediate referral rate (4.7%), but the overall higher cost per child tested and per child identified with bilateral PCHI is probably due to (1) the need to purchase two different technologies, thereby increasing costs, and (2) the acknowledgement that a significant proportion of newborns at one two-stage screening hospital (9.9%) were bypassed for TEOAE and tested directly with AABR, resulting in increased overall referral rates for this protocol.

244 Universal neonatal hearing screening
Table F Short-term costs and cost-effectiveness of existing UNHS programs
Study Population Quality Ratio Protocol / Results ($AUS) 2-stage TEOAE
and AABR 1-stage TEOAE
1-stage AABR
Cost per child born
46 40 46
Scenario 1a 52 57 41 Scenario 2b 43 40 41
Vohr, Oh et al 2001
12,081 sequentially tested well newborns
13.5/16
Cost per child identified with bilateral PCHI
23,300 20,220 23,120
2-stage DPOAE Cost per baby screened
Year 1 Year 5 c
Without follow-up costs
32 19
Gorga et al 2001
4,460 newborns at local hospital (97.5% coverage)
13.5/16
With follow-up costs
37 25
2-stage TEOAE 2-stage AABR
Cost/baby screened
Without follow-up costs
44 46
Lemons et al 2002
1,530 newborns screened with TEOAE; 1,412 newborns screened with AABR
12/16
With follow-up costs
80 63
1-stage TEOAE
Cost per child entering program 12.99
Cost of screening protocol per child 6.91
Cost of diagnostic assessment protocol per child
6.08
Cost per child identified with sensorineural / mixed hearing impairment
2,333
Cost per child identified with sensorineural / mixed / conductive hearing impairment
318
Driscoll et al 2000
1,305 infants of mean age 2 months (1.5–2.5 months); voluntary enrolment
11/16
Total annual program cost 84,019
2-stage TEOAE
Cost per child screened 40
Maxon et al 1995
4,253 infants born during 6-month period in 1993 595 special care; 3,658 well
11/16
Cost per child identified 6780
1-stage DPOAE
Cost per child screened 29
Stone et al 2000
1,002 well newborns 6 to 72 hours old at screen
11/16
Cost per child diagnosed with PCHI 32,950
2-stage TEOAE Weirather et al 1997
380 well and NICU newborns
11.5/16 Cost per baby screened 11
a Use of non-dedicated screeners (ie no cost); b performed by dedicated screeners ($17.00/hr); c average over 5-year life-span of the DPOAE equipment. AABR = automated auditory brainstem response test. TEOAE = transient evoked otoacoustic emissions test. DPOAE = distortion product otoacoustic emissions test. NICU = neonatal intensive care unit.

Universal neonatal hearing screening 245
Sensitivity analysis was used to demonstrate the effect of changing the type of personnel used in screening. This was based on the author’s observation that non-dedicated screeners have higher referral rates than dedicated screeners. Costs of using non-dedicated screeners were assumed unrealistically to be $0, pushing overall costs down, but because the referral rates of non-dedicated screeners were higher, two-stage and one-stage TEOAE screening became more expensive per baby screened (Table F). The referral rate for one-stage AABR did not change (as non-dedicated screeners were already in use in this program), and was found to be the most cost-effective option. Using dedicated screeners ($17 per hour) lowered the referral rate for the two-stage and one-stage AABR protocols. The TEOAE referral rate did not change as dedicated screeners were already being used at the hospital site using this program. In this analysis one-stage TEOAE became the most cost-effective option.
This study highlights a number of issues. The choice of program is dependent upon those goals that are more important to the health care system contemplating a screening program. Ultimately, each program identifies the same number of infants with PCHI within the newborn population. If cost minimisation was a priority, TEOAE may be selected as the method of choice. However, if the goal was to alleviate the burden on follow-up screening and reduce unnecessary parental anxiety due to false positive results, then a two-stage or one-stage AABR program may be preferable.
A study of the cost-effectiveness of a single program (2-stage distortion product otoacoustic emissions (DPOAE)) on 4,460 newborns from both well and neonatal intensive care unit (NICU) populations was evaluated by Gorga and colleagues (2001) (Figure 17). Pre-discharge babies were screened with DPOAE and rescreened with the same technology if they failed the test in either ear. Following a second fail result, diagnostic auditory brainstem response (ABR) was performed. A clinical audiologist performed all tests.
Figure 17 Protocol for universal screening of well and neonatal intensive care unit babies (Gorga et al 2001)
Costs considered in the evaluation were those of equipment, disposables, salary and benefits of the audiologists as well as the cost of follow-up diagnostic assessment. Costs were estimated over the period of 5 years (the estimated lifetime of the screening equipment), assuming a birth cohort of 2,200 babies per year and a referral rate of 2 per cent (as determined from results of the local program). Analysis attempted to determine the cost per baby screened, but did not amortise the purchase cost of the equipment over its useful clinical life. First-year costs per baby, with and without follow-up costs included, were $32 and $37 respectively (Table F). However, since the cost of the purchase of screening equipment was only included in this first year, over the lifetime (5 years) of the equipment the average cost per baby screened, with and without follow-up costs, fell to $19 and $25 respectively.

246 Universal neonatal hearing screening
Cost-effectiveness of start-up of either a two-stage TEOAE or a two-stage AABR screening program at two separate hospitals was compared in another recent study (Lemons et al 2002). All newborn infants were targeted for screening at both hospitals, resulting in 99 per cent coverage using TEOAE (1,530 newborns) and 96 per cent coverage using AABR (1,412 newborns). A fail in either ear resulted in a second test using the same technology. If another fail resulted, then the infant was referred for audiologic assessment (Figure 18).
Figure 18 Protocol for 2-stage TEOAE or AABR universal neonatal hearing screening (Lemons et al 2002)
Audiologists always performed TEOAE screening, while nursing staff performed AABR screening. Resources included in the costing were personnel (audiologist and nurse time, and administration and clerical assistance), screening materials (probes, tips, electrodes), screening equipment (TEOAE, AABR, cart, printer, computer) and paper supplies. Eighty-one per cent of infants passed the initial TEOAE screen, while 77 per cent passed the initial AABR test. However, rates for follow-up assessment were reported to be 15 per cent for TEOAE and averaged 7 per cent for AABR during the study period. The cost per infant screened, with and without follow-up, is presented in Table F. Due to higher numbers of infants requiring follow-up assessment in the TEOAE program, the costs per child screened were higher than for AABR despite the initial higher cost of AABR equipment (total equipment start-up costs estimated to be $25,000 for AABR and $13,000 for TEOAE). Supplies such as electrodes and probes were also determined to be more costly for AABR than for TEOAE ($20,600 for AABR and $5,100 for TEOAE) over the duration of the study. Conversely, the cost of personnel was more expensive for the TEOAE program due to the requirement of using audiologists to interpret the results, as opposed to using nurses for the AABR program where no such interpretation was required ($19,600 for AABR and $50,000 for TEOAE).
In a study of 386 well and NICU infants born over a 2-month period, the cost-effectiveness of a hospital universal neonatal screening program using two-stage TEOAE was evaluated (Weirather et al 1997). First-stage screening was performed prior to hospital discharge. A fail on the screening test meant the infant was scheduled to return to hospital for a second TEOAE at 1–3 weeks of age. The infant was referred to the hospital audiology department for diagnostic assessment if they failed the second TEOAE test (Figure 19).

Universal neonatal hearing screening 247
Figure 19 Protocol for 2-stage TEOAE universal neonatal hearing screening (Weirather et al 1997)
With this program the authors reported 98 per cent coverage (380/386) prior to discharge, and 100 per cent coverage by 1 week of age. Eighty-nine per cent passed the first-stage screen and 11 per cent returned for a second screening test. No information was provided on the number of infants referred for diagnostic assessment. Costs considered in the analysis included: personnel for screening, rescreening, screening management, program management, patient management and scoring; fringe benefits (30% of salaries); supplies; equipment (not screening equipment, which was assumed already in place); and overhead costs (20% of costs). This paper argued that the resulting cost per baby screened of only $11 dispelled any claim that the cost of a UNHS program could be prohibitive (Table F). However, the study did not include in its analysis the costs of purchasing screening equipment such as TEOAE devices. Further, large costs incurred for diagnostic assessment of infants who had been referred were not taken into account for costing of the program, nor were the referral rates reported in the study.
In an Australian study the cost-effectiveness of a one-stage TEOAE screening program operated within community child health clinics (CHC) was evaluated on a voluntary enrolment of 1,305 infants (Driscoll et al 2000). The mean age at time of testing was 2 months (range 1.5–2.5 months). The test was performed by an audiologist, and if the infant failed the test in either ear they were referred to an auditory clinic for diagnostic assessment. The referral rate for diagnostic evaluation was determined to be 11 per cent. Costs considered in the evaluation were the audiologist’s salary, screening equipment and maintenance, replacement cost of TEOAE probes on a yearly basis, consumables and follow-up costs. Costs were averaged over an assumed lifetime of the TEOAE apparatus of 6 years. The cost per child screened (entering program) was determined to be $13 and the cost per child identified with sensorineural or mixed hearing loss was $2,333 (Table F). However, due to the voluntary nature of the enrolment, it is possible that parents who were concerned about the hearing of their infant were more likely to attend a CHC. This may have increased the level of risk in the sample and reduced the cost per child identified. Further, identifying infants with either sensorineural or mixed hearing impairment may also have increased the prevalence of affected infants in this sample, lowering the cost per infant identified.
A two-stage TEOAE program in Rhode Island (USA) was evaluated for the cost-effectiveness of screening 4,253 infants (595 special care and 3,658 well infants) born during a 6-month period in 1993 (Maxon et al 1995). First-stage screening was performed prior to hospital discharge. If a failure was recorded the infant was scheduled for a rescreen 4–6 weeks later. If a second failure was recorded, ABR was performed by the hospital screening staff, and infants who failed the ABR test were referred for diagnostic audiologic evaluation (Figure 20).

248 Universal neonatal hearing screening
Figure 20 Protocol for 2-stage TEOAE universal neonatal hearing screening (Maxon et al 1995)
Analysis of effectiveness was based on a 93 per cent pass rate at the first-stage screen and a referral rate of 1 per cent. The final yield of unilateral and bilateral permanent childhood hearing impairment (PCHI) for this population of infants was determined to be 6.0/1,000. Annual costs considered for the program were: personnel (including trained screening technicians, audiologists, a coordinator, clerical assistance), fringe benefits (28% of salaries), overhead costs (29% of salaries), supplies, cost of diagnostic ABR evaluation, and equipment (three TEOAE screening tools, one ABR machine, four computers and two printers – all amortised over 5 years). In this study two-stage TEOAE was determined to cost $40 per child screened and $6,780 per child identified with unilateral or bilateral PCHI (Table F).
Cost-effectiveness of a one-stage TEOAE UNHS program was performed on 1,002 well newborns 6–72 hours old (Stone et al 2000). An infant who failed the first-stage TEOAE test was referred for diagnostic assessment at 8 weeks of age using DPOAE and tympanometry. A fail on both tympanometry and DPOAE indicated middle ear disease and treatment. A fail on the DPOAE test alone resulted in further testing with AABR. Costs included in the analysis were for a full-time registered nurse, administrator time for 1 hour/week, interpretation of results by an audiologist, DPOAE screening equipment, supplies and follow-up assessment. Effectiveness of the program was based on a failure rate of 11 per cent of infants tested with DPOAE in the first-stage screen (hence referral rate to diagnostic assessment and a yield of 0.2 %). Outcomes of interest were the cost per child screened and the cost per child diagnosed with PCHI. It is unclear whether the protocol was interested in identifying unilateral and bilateral PCHI or only bilateral PCHI. The cost per child screened was slightly lower than that reported by Vohr, Oh and colleagues (2001) in a one-stage TEOAE ($29 vs $40 respectively) but the resulting cost per child identified was found to be roughly 60 per cent higher than that of Vohr, Oh and colleagues (2001) (Table F). Again, this is probably due to higher referral rates in this study compared to the previous one (11% versus 6%).

Universal neonatal hearing screening 249
Summary of existing universal neonatal hearing screening protocols in the short term
From studies of existing universal neonatal hearing screening protocols, the cost per child screened, including follow-up, was quite variable. Two-stage protocols ranged from $25 to $80 per child screened while one-stage protocols ranged from $29 to $46 per child screened. Estimates of the cost per child identified were similarly varied, ranging from $6,700 to $23,000 for two-stage screening programs, and from $20,000 to $32,000 for one-stage protocols.
In the only study comparing two-stage transient evoked otoacoustic emissions (TEOAE) – automated auditory brainstem response (AABR) and one-stage TEOAE or one-stage AABR hearing screening, the cost per child screened and cost per child identified with permanent childhood hearing impairment (PCHI) were roughly equivalent (Vohr et al 2001). In a single study comparing two-stage otoacoustic emissions testing with two-stage AABR, the latter was considered more cost-effective because referral rates were lower, this despite the initial higher cost outlay for AABR equipment (Lemons et al 2002).
Two included studies presented cost per child screened estimates that were substantially lower than for comparable studies examined in this evaluation. In the one-stage TEOAE study by Driscoll (Driscoll et al 2000) the screened sample was drawn from volunteer walk-in subjects to a child health clinic (CHC). Cost per child screened here was noticeably lower ($13), which was probably due to the higher prevalence of hearing impairment in this population, since concerned parents are more likely to attend the CHC with their child than parents of seemingly healthy infants. Similarly, the cost of using a two-stage TEOAE protocol for screening was determined to be only $11 per child screened before the costs of diagnostic assessment (Weirather et al 1997). In this study, however, the initial purchase cost of screening equipment was not included.
On the basis of this evidence, it is difficult to recommend any one protocol for UNHS in the short term.

250 Universal neonatal hearing screening
Overall summary of published economic evaluation studies of neonatal hearing screening
With the exception of two studies, all identified published research examining the cost-effectiveness of existing or modelled universal neonatal hearing screening (UNHS) programs are from an American perspective. In the only study from Australia, the study design did not reflect the optimal conditions for a universal screening program, as the participation was voluntary. Therefore, due to differences in costs and the structure of the US medical system, the results obtained from the majority of the literature can be only suggestive of what might occur under Australian conditions.
Short-term costs and benefits
Based on existing evidence from Keren et al (2002) and Kemper and Downs (2000), it is suggested that UNHS is less cost-effective in the short term (incremental cost per child identified with permanent childhood hearing impairment (PCHI)) than targeted screening (Table B). The difference in the incremental cost-effectiveness ratio between the two studies (Table G) may be due in part to costs incurred by the larger number of infants referred from UNHS compared to targeted screening in the Keren et al study (UNHS/targeted = 1.6%/0.18%, or 8-fold higher), compared to the Kemper and Downs study (UNHS/targeted = 0.4%/0.07%, or 6-fold higher).
Table G Short-term incremental cost-effectiveness ratio, cost per case identified, in modelled studies comparing UNHS and targeted screening
Protocol ICER (universal/targeted) $AUS
Study
UNHS Targeted TEOAE/AABR AABR/AABR 61,600a (Keren et al 2002) TEOAE/AABR TEOAE/AABR 35,650b (Kemper & Downs 2000)
ICER = incremental cost-effectiveness ratio. a all relevant costs included with the exception of a computer, consumables, screener training and overheads; b assumed capital, consumable and personnel costs included but not described
Amongst studies of both modelled and existing UNHS protocols, the cost per child screened including follow-up was quite variable (Table H). Two-stage protocols ranged from $18 to $80 per child screened, while one-stage protocols ranged from $29 to $46 per child screened. Modelled programs were consistently less expensive per child screened than similar protocols for existing programs (eg 2-stage transient evoked otoacoustic emissions (TEOAE) – automated auditory brainstem response (AABR) model vs existing program, $24 vs $46 per child screened). This suggests that some costs incurred by the existing programs have not been accounted for in the modelled programs. Variations in cost per child screened appear to depend on rates of referral to diagnostic assessment. An exception to this would be the study by Driscoll and colleagues (2000), in which the referral rate is high.
Within studies comparing different protocols (Table H – studies designated by G, V, K, B, and L), modelled programs have shown that two-stage protocols are less costly per child screened than one-stage protocols, probably due to the lower referral rate of two-stage protocols (Table H – studies G and K). Two-stage protocols incorporating otoacoustic emissions (OAE) testing are less costly than two-stage AABR protocols due to the increased cost of consumables in AABR testing for the first stage of screening (Table H – studies K and B). However, existing UNHS programs tell a somewhat different story, with one study finding no difference in cost per child screened between

Universal neonatal hearing screening 251
two-stage TEOAE with AABR and one-stage TEOAE or one-stage AABR (Table H – study V). Another existing program found the opposite result of that of a modelled study (Table H – study K), with a two-stage AABR being less costly than a two-stage TEOAE (Table H – study L).
Table H Short-term cost per child screened for reported universal neonatal hearing screening programs (Lemons et al 2002)
Type of assessment
Referral rate (%)
2003 cost/child screened ($AUS) Study Technique
Without follow-up costs
With follow-up costs
2-stage TEOAE–AABR Modelc 2 24 G (Gorga et al 2001) Existingc 4.7 46 V (Vohr et al 2001)
AABR Modelc ? 28 K (Kezirian et al 2001) Modelc 2–4 41 B (Boshuizen et al 2001) Existingb 6.5 46 63 L (Lemons et al 2002)
DPOAE Existingc 2 19 25 (Gorga et al 2001) TEOAE Existingb 15 44 80 L (Lemons et al 2002)
Existingc 1 40 (Maxon et al 1995) Existingd ? 11a (Weirather et al 1997)
OAE Modelc ? 18 K (Kezirian et al 2001) Modelc 2–4 29 B (Boshuizen et al 2001)
1-stage TEOAE Existingc 6.5 40 V (Vohr et al 2001)
Existingc 10.8 13 (Driscoll et al 2000) DPOAE Existingc 0.2 29 (Stone et al 2000) AABR Modelc ? 35 K (Kezirian et al 2001)
Modelc 2 32 A (Gorga et al 2001) Existingc 3.2 46 V (Vohr et al 2001)
OAE Modelc 2 33 A (Gorga et al 2001) AABR = automated auditory brainstem response test; TEOAE = transient evoked otoacoustic emissions test; DPOAE = distortion product otoacoustic emissions test; OAE = otoacoustic emissions test; a Costs do not include purchase of screening equipment; b most resources included in costing; c assumed some or most resources included in costing but not described; d important resources absent from costing.
The outcome of ‘cost per child identified’ showed similar variation amongst studies, ranging from $6,700 to $23,000 for two-stage screening programs and from $20,000 to $32,000 for one-stage protocols (Table I). Modelled UNHS programs once more identified a lower cost (per child identified) than existing programs using similar screening protocols. This discrepancy is again probably due to the omission of cost items in the modelled program that were included in the existing programs. Within studies comparing different protocols (studies designated by V, K and B in Table I), modelled programs have shown that two-stage OAE protocols are less costly per child identified than one- or two-stage AABR protocols (Table I – studies K and B). However, the one existing program comparing cost per child identified for different UNHS protocols found no difference in cost per child screened between two-stage TEOAE with AABR and one-stage TEOAE or one-stage AABR (Table I – study V).

252 Universal neonatal hearing screening
Summary
From the literature it can be concluded that, in the short term, the costs for the additional cases identified and diagnosed by universal neonatal hearing screening (UNHS) are greater per unit than those of targeted screening. However, it is inappropriate to determine incremental cost-effectiveness without considering long-term costs and cost savings. Further, modelled two-stage UNHS protocols appear to be more cost-effective than modelled one-stage protocols, but this observation is not supported by reports of existing UNHS programs using either one- or two-stage screening protocols. Therefore, based on the available evidence, no determination of the most cost-effective protocol for UNHS in the short term can be made.
Table I Short-term cost per child identified in reported universal neonatal hearing screening programs
Technique Type of assessment Cost/child identified ($AUS) Study
2-stage TEOAE–AABR Modela 17,350 (Kemper & Downs 2000)
Existinga 23,300 V (Vohr et al 2001) TEOAE Existinga 6,780 (Maxon et al 1995)
OAE Modela 7200 K (Kezirian et al 2001) Modela 40,880 B (Boshuizen et al 2001)
AABR Modela 11,430 K (Kezirian et al 2001) Modela 57,380 B (Boshuizen et al 2001)
1-stage TEOAE Existinga 20,220 V (Vohr et al 2001)
Existinga 2,333 (Driscoll et al 2000) DPOAE Existinga 32,950 (Stone et al 2000) AABR Modela 13,350 K (Kezirian et al 2001)
Existinga 23,120 V (Vohr et al 2001) AABR = automated auditory brainstem response test; TEOAE = transient evoked otoacoustic emissions test; DPOAE = distortion product otoacoustic emissions test; OAE = otoacoustic emissions test; a assumed some or most resources included in costing but not described.

Universal neonatal hearing screening 253
Summary
While it was established earlier in this report that universal neonatal hearing screening would be more expensive to operate than a targeted screening program, taking a societal perspective over the long term suggests that identifying a larger proportion of hearing-impaired infants at an early stage (ie ≤6 months of age) would result in an overall cost-effective program. However, these societal costs are based primarily on observation and expert opinion and have not been generated from properly designed studies.
Long-term costs and benefits
Only one study attempted to model the cost-effectiveness of universal neonatal hearing screening (UNHS) over the long term and from a societal perspective (Keren et al 2002). A hypothetical cohort of 80,000 newborns from one US state was used and consisted of 10,400 high-risk and 69,600 low-risk infants. Under targeted screening, only infants with identified risk factors for congenital deafness were screened (Box 10). The decision tree for this model is shown in Figure 11. Based on literature estimates of 1.6 cases of permanent childhood hearing impairment (PCHI) per 1,000 births, the cohort was assumed to contain 128 infants with PCHI. The point estimates presented were based on 80 per cent coverage of high-risk infants through targeted screening and 100 per cent coverage for all infants using UNHS. Yield from the two screening programs was estimated at 48 per cent (61 infants) for targeted screening and 91 per cent (116 infants) for UNHS.
Lifetime societal costs of deafness that were considered for this model were lost productivity, special education, vocational rehabilitation, additional medical costs and assistive devices. Analysis resulted in an incremental saving of $2 million per child with normal language using targeted screening compared to having no screening program, and a further saving of $1.2 million per child using UNHS.
Table J Societal benefit of hearing screening protocols
Study Population Quality Ratio Protocol /Results ($AUS) No
screening Targeted screening
2-stage AABR
Universal screening
2-stage OAE and AABR
Keren et al 2002
Hypothetical cohort of 80,000 infants from one US state 10,400 high-risk, 69,600 low-risk infants
15/16
Incremental cost reduction per child with bilateral hearing impairment possessing normal language
0 2,030,000a 1,212,000b
a ICER for targeted vs no screening; b ICER for UNHS vs targeted (assuming 80% of high-risk patients screened in targeted screening scenario and 77% of infants followed up with diagnostic assessment after positive screen in both scenarios). AABR = automated auditory brainstem response test; OAE = otoacoustic emissions test; TEOAE = transient evoked otoacoustic emissions test.

254 Universal neonatal hearing screening
Glossary
Absolute SpPin A diagnostic finding where the Specificity is so high that a Positive result rules-in the diagnosis.
Absolute SnNout A diagnostic finding where the Sensitivity is so high that a Negative result rules-out the diagnosis.
Absolute yield or yield The number of cases of permanent childhood hearing impairment ultimately identified in the screened population.
Aminoglycosides A group of antibiotics used to treat certain bacterial infections.
Confounding A variable that is related to or causative of the outcome of interest and is differentially distributed between the groups with and without the intervention/condition.
Cytomegalovirus Any of a group of herpes viruses that induces birth defects and affects humans with impaired immunological systems.
External validity The degree to which the results of a study can be applied to the wider population.
Failure rate The number of infants who failed a screen or rescreen divided by the number of individuals who were intended to be screened.
False alarm rate Complement of the positive predictive value of a test. In other words, the number of infants falsely identified with hearing impairment divided by the total number of infants testing positive for hearing impairment.
False negative rate Complement of the sensitivity of a test. In other words, the number of infants incorrectly identified with normal hearing (false negative) divided by the total number of infants with hearing impairment.
False positive rate Complement of the specificity of a test. In other words, the number of infants falsely identified with hearing impairment (false positive) divided by the total number of infants without hearing impairment.
False reassurance rate Complement of the negative predictive value of a test. In other words, the number of infants incorrectly identified as having normal hearing divided by the total number of infants testing negative for hearing impairment.
Hyperbilirubinaemia In the newborn, a disorder usually caused by immaturity of the liver that usually subsides spontaneously.
Incremental yield The number of additional cases of permanent childhood hearing impairment ultimately identified in the screened population, compared to usual targeted screening or case-finding methods.

Universal neonatal hearing screening 255
Positive predictive value The number of infants correctly identified with hearing impairment divided by the total number of infants testing positive for hearing impairment.
Power The ability of a study to demonstrate an association, given that the association exists.
Sensitivity The number of infants correctly identified by a test as having hearing impairment divided by the total number of infants with hearing impairment.
Specificity The number of infants correctly identified by a test as having no hearing impairment divided by the total number of infants without hearing impairment.
Toxoplasmosis A disease caused by infection with the parasite Toxoplasma gondii. In newborns, congenital toxoplasmosis is an infection that results from the transplacental passage of parasites from the infected mother to the fetus (Braunwald et al 2001)
True positive The number of cases correctly identified by a test as having the condition.

256 Universal neonatal hearing screening
Abbreviations
AABR automated auditory brainstem response (test)
ABR auditory brainstem response (test)
AHMAC Australian Health Ministers’ Advisory Council
AHMC Australian Health Ministers’ Conference
ANCOVA analysis of covariance
ARTG Australian Register of Therapeutic Goods
AR-DRG Australian Refined Diagnosis Related Groups
CDI Communicative Development Inventory
CDR clinical decision rule
CEA cost-effectiveness analysis
CHC child health clinic
CHIP Colorado Home Intervention Program
CI confidence interval
Clin I clinical importance
CPI consumer price index
CPG clinical prediction guide
CQ cognitive quotient
dB decibel
DECS South Australian Department of Education & Children’s Services
DPOAE distortion product otoacoustic emissions (test)
DQ development quotient
dx diagnostic
ECA economic cost analysis
ENT ear, nose and throat
FA false alarm
FN false negative
FP false positive
HL hearing level
HVDT health visitor distraction test
ICER incremental cost-effectiveness ratio
kHz kilohertz
LQ language quotient
LR likelihood ratio

Universal neonatal hearing screening 257
LTFU loss/lost to follow up
MBS Medicare Benefits Schedule
MCDI Minnesota Child Development Inventory
MeSH medical subject heading
MSAC Medical Services Advisory Committee
n number
n/a not applicable
nHL near hearing level
NHMRC National Health and Medical Research Council
NICU neonatal intensive care unit
NNTB number needed to treat to benefit
NS not significant
OAE otoacoustic emissions (test)
OECD Organisation for Economic Cooperation and Development
OR odds ratio
PAQ play assessment questionnaire
PCHI permanent childhood hearing impairment
PPV positive predictive value
QS quality score
R relevance
RCT randomised controlled trial
RR relative risk / rate ratios
SCBU special care baby unit
SD standard deviation
SNHL sensorineural hearing loss
SP statistical precision
SPL sound pressure level
SR systematic review
SSEP steady state evoked potentials (test)
SWP sweeps
TEOAE transient evoked otoacoustic emissions (test)
TN true negative
TP true positive
UMDNS Universal Medical Device Nomenclature System
UNHS universal neonatal hearing screening
WBN well baby nursery

258 Universal neonatal hearing screening
References
ABS (2003). Labour force Australia [Internet]. Australian Bureau of Statistics. Available from: www.abs.gov.au/Ausstats/aba106 [Accessed 12th November]. ABS (2004). 6401.0 Consumer Price Index [Internet]. Australian Bureau of Statistics. Available from: http://www.abs.gov.au/Ausstats/abs%40.nsf/e8ae5488b598839cca [Accessed 28/09]. ABS (2005). 3301.0 Births, Australian Bureau of Statistics, Australia. Aidan, D., Avan, P. & Bonfils, P. (1999). 'Auditory screening in neonates by means of transient evoked otoacoustic emissions: a report of 2,842 recordings', Ann Otol Rhinol Laryngol, 108 (6), 525-531. Armitage, P., Berry, G. & Matthews, J. N. S. (2002). Statistical methods in medical research. Fourth Edition Blackwell Science, Oxford. Australian Hearing (2001). Universal neonatal hearing screening (UNHS)- Implications for Australian Hearing, Australian Hearing. Australian Hearing (2003). Causes of hearing loss [Internet]. Australian Hearing. Available from: www.hearing.com.au [Accessed July 24 2003]. Australian Hearing (2007). 'Demographic details of persons under the age of 21 years with a hearing impairment who have been fitted with a hearing aid - 2007'. Audiology Circular, 2007/6. Australian Institute of Health and Welfare (2002). The Knowledgebase - national health data dictionary [Internet]. version 11. Available from: http://www.aihw.gov.au/knowledgebase/indexkbhealth.html [Accessed Accessed April 2 2003]. Bailey, H. D., Bower, C. et al (2002). 'Newborn hearing screening in Western Australia', Medical Journal of Australia, 177 (4), 180-185. Bamford, J., Uus, K. & Davis, A. (2005). 'Screening for hearing loss in childhood: Issues, evidence and current approaches in the UK', Journal of Medical Screening, 12 (3), 119-124. Bantock, H. M. & Croxson, S. (1998). 'Universal hearing screening using transient otoacoustic emissions in a community health clinic', Archives of Disease in Childhood, 78 (3), 249-252. Barsky Firkser, L. & Sun, S. (1997). 'Universal newborn hearing screenings: a three-year experience', Pediatrics, 99 (6), E4. Boshuizen, H. C., van der Lem, G. J. et al (2001). 'Costs of different strategies for neonatal hearing screening: a modelling approach', Archives of disease in childhood. Fetal and neonatal edition, 85 (3), F177-181.

Universal neonatal hearing screening 259
Braunwald, E., Fauci, A. S. et al (2001). Harrison's (15th Edition) principles of internal medicine, Vol. 1. 15 McGraw-Hill Medical Publishing Division, New York. Brennan, R. A. (2004). 'A nurse-managed universal newborn hearing screen program', MCN: The American Journal of Maternal Child Nursing, 29 (5), 320. Chapchap, M. J. & Segre, C. M. (2001). 'Universal newborn hearing screening and transient evoked otoacoustic emission: new concepts in Brazil. Proceedings from the 3rd International Congress of Paediatric Audiology, Copenhagen, Denmark, May 9-12, 2000', Scandinavian Audiology Supplementum, 30, 33-36. Child and Youth Health (2001). Universal neonatal hearing screening in Australia: a national forum for consensus and implementation [Internet]. Child and Youth Health. Available from: http://www.cyh.com/cyh/contents/cms_content.html [Accessed 13 November 2002]. Chiong, C., Ostrea Jr, E. et al (2007). 'Correlation of hearing screening with developmental outcomes in infants over a 2-year period', Acta Oto-Laryngologica, 127 (4), 384-388. Clarkson, R. L., Vohr, B. R. et al (1994). 'Universal infant hearing screening and intervention: the Rhode Island program', Infants and Young Children, 6 (3), 65-74. Clemens, C. J. & Davis, S. A. (2001). 'Minimizing false-positives in universal newborn hearing screening: a simple solution', Pediatrics, 107 (3), 1 - 3. Clemens, C. J., Davis, S. A. & Bailey, A. R. (2000). 'The false-positive in universal newborn hearing screening', Pediatrics, 106 (1), E7. Columbia University College of Physicians and Surgeons (2002). Hearing loss [Internet]. Columbia Presbyterian Medical Center. Available from: http://www.entcolombia.org/hearloss.htm [Accessed 14/05/2003]. Connolly, J. L., Carron, J. D. & Roark, S. D. (2005). 'Universal newborn hearing screening: are we achieving the Joint Committee on Infant Hearing (JCIH) objectives?' Laryngoscope, 115 (2), 232-236. Cox, L. C. & Toro, M. R. (2001). 'Evolution of a universal infant hearing screening program in an inner city hospital', International Journal of Pediatric Otorhinolaryngology, 59 (2), 99-104. Crockett, R., Baker, H. et al (2005). 'Maternal anxiety and satisfaction following infant hearing screening: A comparison of the health visitor distraction test and newborn hearing screening', Journal of Medical Screening, 12 (2), 78-82. Crockett, R., Wright, A. J. et al (2006). 'Maternal anxiety following newborn hearing screening: The moderating role of knowledge', Journal of Medical Screening, 13 (1), 20-25. Daemers, K., Drickx, J. D. et al (1996). 'Neonatal hearing screening with otoacoustic emissions: an evaluation', Acta Oto-Rhino-Laryngologica Belgica, 50 (3), 203-209.

260 Universal neonatal hearing screening
Davies, S. C., Cronin, E. et al (2000). 'Screening for sickle cell disease and thalassaemia: a systematic review with supplementary research.' Health Technology Assessment, 4 (3), i-v, 1 - 99. Davis, A., Bamford, J. et al (1997). 'A critical review of the role of neonatal hearing screening in the detection of congenital hearing impairment', Health Technology Assessment, 1 (10), i-iv, 1-176. Davis, A. & Wood, S. (1992). 'The epidemiology of childhood hearing impairment: factor relevant to planning of services', British Journal of Audiology, 26 (2), 77-90. De Capua, B., De Felice, C. et al (2003). 'Newborn hearing screening by transient evoked otoacoustic emissions: analysis of response as a function of risk factors', Acta Otorhinolaryngol Ital, 23 (1), 16-20. Deeks, J. J. (2001). 'Systematic reviews of evaluations of diagnostic and screening tests', British Medical Journal, 323 (21 July), 157-162. Department of Medical Oncology (1998). On-Line Medical Dictionary [Internet]. University of Newcastle upon Tyne. Available from: http://cancerweb.ncl.ac.uk/cgi-bin/omd?query=hearing+loss [Accessed 17/07/2003]. Downs, M. P. (1994). 'The case for detection and intervention at birth', Seminars in Hearing, 15 (2), 76-84. Downs, M. P. (1995). 'Universal newborn hearing screening--the Colorado story', International Journal of Pediatric Otorhinolaryngology, 32 (3), 257-259. Driscoll, C., Kei, J. & McPherson, B. (2000). 'Cost comparison of hearing screening programs: Transient evoked otoacoustic emissions in infant screening and screening at school entry', Australian and New Zealand Journal of Audiology, 22 (2), 77-84. Drummond, M. F., O'Brien, B. J. et al (1997). Methods for the economic evaluation of health care programmes. 2nd Edition, Oxford University Press, Oxford. Egger, M., Juni, P. et al (2003). 'How important are comprehensive literature searches and the assessment of trial quality in systematic reviews? Empirical study.' Health Technology Assessment, 7 (1), 76. Fortnum, H. & Davis, A. (1997). 'Epidemiology of permanent childhood hearing impairment in Trent Region, 1985-1993', British Journal of Audiology, 31 (6), 409-446. Gallaudet Research Institute (2001). Regional and national summary report of data from the 1999-2000 annual survey of deaf and hard of hearing children and youth, Gallaudet University, Washington, D.C. Gorga, M. P., Preissler, K. et al (2001). 'Some issues relevant to establishing a universal newborn hearing screening program', Journal of the American Academy of Audiology, 12 (2), 101-112. Govaerts, P. J., Yperman, M. et al (2001). 'A two-stage bipodal screening model for universal neonatal hearing screening', Otology & Neurotology, 22 (6), 850-854.

Universal neonatal hearing screening 261
Habib, H. S. & Abdelgaffar, H. (2005). 'Neonatal hearing screening with transient evoked otoacoustic emissions in Western Saudi Arabia', International Journal of Pediatric Otorhinolaryngology, 69 (6), 839-842. Hadjikakou, K. & Bamford, J. (2000). 'Prevalence and age of identification of permanent childhood hearing impairment in Cyprus', Audiology, 39 (4), 198-201. Hahn, M., Lamprecht-Dinnesen, A. et al (1999). 'Hearing screening in healthy newborns: feasibility of different methods with regard to test time', International Journal of Pediatric Otorhinolaryngology, 51 (2), 83-89. Hatzopoulos, S., Qirjazi, B. & Martini, A. (2007). 'Neonatal hearing screening in Albania: Results from an ongoing universal screening program', International Journal of Audiology, 46 (4), 176-182. Helfand, M., Thompson, D. C. et al (2001). Newborn hearing screening, Agency for Healthcare Research and Quality, Rockville. Hergils, L. & Hergils, A. (2000). 'Universal neonatal hearing screening - Parental attitudes and concern', British Journal of Audiology, 34 (6), 321-327. Ho, V., Daly, K. A. et al (2002). 'Otoacoustic emissions and tympanometry screening among 0-5 year olds', Laryngoscope, 112 (3), 513-519. Hunter, M. F., Kimm, L. et al (1994a). 'Feasibility of otoacoustic emission detection followed by ABR as a universal neonatal screening test for hearing impairment', British Journal of Audiology, 28 (1), 47-51. Hunter, M. F., Kimm, L. et al (1994b). 'Feasibility of otoacoustic emission detection followed by ABR as a universal neonatal screening test for hearing impairment', British Journal of Audiology, 28 (1), 47-51. Huynh, M. T., Pollack, R. A. & Cunningham, R. A. J. (1996). 'Universal newborn hearing screening: Feasibility in a community hospital', Journal of Family Practice, 42 (5), 487-490. Iley, K. L. & Addis, R. J. (2000). 'Impact of technology choice on service provision for universal newborn hearing screening within a busy district hospital', Journal of Perinatology, 20 (8 Part 2), S122-127. Isaacson, G. (2000). 'Universal newborn hearing screening in an inner-city, managed care environment', Laryngoscope, 110 (6), 881-894. Iwasaki, S., Hayashi, Y. et al (2003). 'A model of two-stage newborn hearing screening with automated auditory brainstem response', International Journal of Pediatric Otorhinolaryngology, 67 (10), 1099-1104. Jacobson, J. T. & Jacobson, C. A. (1994). 'The effects of noise in transient EOAE newborn hearing screening', International Journal of Pediatric Otorhinolaryngology, 29 (3), 235-248.

262 Universal neonatal hearing screening
Jakubikova, J., Kabatova, Z. & Zavodna, M. (2003). 'Identification of hearing loss in newborns by transient otoacoustic emissions', International Journal of Pediatric Otorhinolaryngology, 67 (1), 15-18. Kanne, T. J., Schaefer, L. & Perkins, J. A. (1999). 'Potential pitfalls of initiating a newborn hearing screening program', Archives of Otolaryngology -- Head and Neck Surgery, 125 (1), 28-32. Kemp, D. T. (2002). 'Otoacoustic emissions, their origin in cochlear function, and use', British Medical Bulletin, 63, 223-241. Kemp, D. T. (2003). OAE's and the cochlea [Internet]. Otodynamics. Available from: http://www.oae-ilo.co.uk/page_view.asp?id=59 [Accessed 02/05/03]. Kemper, A. R. & Downs, S. M. (2000). 'A cost-effectiveness analysis of newborn hearing screening strategies', Archives of Pediatrics and Adolescent Medicine, 154 (5), 484-488. Kennedy, C., McCann, D. et al (2005). 'Universal newborn screening for permanent childhood hearing impairment: an 8-year follow-up of a controlled trial', Lancet, 366 (9486), 660-662. Kennedy, C. R. (1999). 'Controlled trial of universal neonatal screening for early identification of permanent childhood hearing impairment: coverage, positive predictive value, effect on mothers and incremental yield. Wessex Universal Neonatal Screening Trial Group', Acta Paediatrica, 88 (432 (Supplement)), 73-75. Kennedy, C. R., Kimm, L. et al (1998). 'Controlled trial of universal neonatal screening for early identification of permanent childhood hearing impairment', Lancet, 352 (9145), 1957-1964. Kennedy, C. R., McCann, D. C. et al (2006). 'Language ability after early detection of permanent childhood hearing impairment', N Engl J Med, 354 (20), 2131-2141. Keren, R., Helfand, M. et al (2002). 'Projected cost-effectiveness of statewide universal newborn hearing screening', Pediatrics, 110 (5), 855-864. Kezirian, E. J., White, K. R. et al (2001). 'Cost and cost-effectiveness of universal screening for hearing loss in newborns', Otolaryngology - Head and Neck Surgery, 124 (4), 359-367. Khairi, M. D., Din, S. et al (2005). 'Hearing screening of infants in Neonatal Unit, Hospital Universiti Sains Malaysia using transient evoked otoacoustic emissions', J Laryngol Otol, 119 (9), 678-683. Khan, K. S., Ter Riet, G. et al (2001). Undertaking systematic reviews of research on effectiveness. CRD's guidance for those carrying out or commissioning reviews, NHS Centre for Reviews and Dissemination, University of York, York. Khandekar, R., Khabori, M. et al (2006). 'Neonatal screening for hearing impairment--The Oman experience', International Journal of Pediatric Otorhinolaryngology, 70 (4), 663-670.

Universal neonatal hearing screening 263
Kolski, C., Le Driant, B. et al (2007). 'Early hearing screening: What is the best strategy?' International Journal of Pediatric Otorhinolaryngology, 71 (7), 1055-1060. Kubba, H., MacAndie, C. et al (2004). 'Is deafness a disease of poverty? The association between socio-economic deprivation and congenital hearing impairment', International Journal of Audiology, 43 (3), 123-125. Lemons, J., Fanaroff, A. et al (2002). 'Newborn hearing screening: costs of establishing a program', Journal of Perinatology, 22 (2), 120-124. Leveque, M., Schmidt, P. et al (2007). 'Universal newborn hearing screening: a 27-month experience in the French region of Champagne-Ardenne', Acta Paediatrica. Lin, C. Y., Huang, C. Y. et al (2004). 'Community-based newborn hearing screening program in Taiwan', International Journal of Pediatric Otorhinolaryngology, 68 (2), 185-189. Lin, H. C., Shu, M. T. et al (2005). 'Comparison of hearing screening programs between one step with transient evoked otoacoustic emissions (TEOAE) and two steps with TEOAE and automated auditory brainstem response', Laryngoscope, 115 (11), 1957-1962. Low, W. K., Pang, K. Y. et al (2005). 'Universal newborn hearing screening in Singapore: the need, implementation and challenges', Ann Acad Med Singapore, 34 (4), 301-306. Martines, F., Porrello, M. et al (2007). 'Newborn hearing screening project using transient evoked otoacoustic emissions: Western Sicily experience', International Journal of Pediatric Otorhinolaryngology, 71 (1), 107-112. Mason, J. A. & Herrmann, K. R. (1998). 'Universal infant hearing screening by automated auditory brainstem response measurement', Pediatrics, 101 (2), 221-228. Maxon, A. B., White, K. R. et al (1995). 'Referral rates and cost efficiency in a universal newborn hearing screening program using transient evoked otoacoustic emissions', Journal of the American Academy of Audiology, 6 (4), 271-277. Maxon, A. B., White, K. R. et al (1993). 'Using transient evoked otoacoustic emissions for neonatal hearing screening', British Journal of Audiology, 27 (2), 149-153. McNellis, E. L. & Klein, A. J. (1997). 'Pass/fail rates for repeated click-evoked otoacoustic emission and auditory brain stem response screenings in newborns', Otolaryngology - Head and Neck Surgery, 116 (4), 431-437. McPherson, B., Kei, J. et al (1998). 'Feasibility of community-based hearing screening using transient evoked otoacoustic emissions', Public Health, 112 (3), 147-152. Mehl, A. L. & Thomson, V. (2002). 'The Colorado newborn hearing screening project, 1992-1999: on the threshold of effective population-based universal newborn hearing screening', Pediatrics, 109 (1). Messner, A. H., Price, M. et al (2001). 'Volunteer-based universal newborn hearing screening program', International Journal of Pediatric Otorhinolaryngology, 60 (2), 123-130.

264 Universal neonatal hearing screening
Mohr, P. E., Feldman, J. J. et al (2000). 'The societal costs of severe to profound hearing loss in the United States', International Journal of Technology Assessment in Health Care, 16 (4), 1120-1135. Molini, E., Ricci, G. et al (2004). 'Identifying congenital hearing impairment. Personal experience based on selective hearing screening', Acta Otorhinolaryngol Ital, 24 (3), 109-116. MSAC (2000). Funding for new medical technologies and procedures: application and assessment guidelines, Commonwealth of Australia, Canberra, ACT. MSAC (2005). Guidelines for the assessment of diagnostic technologies [Internet]. Medical Services Advisory Committee, Commonwealth of Australia. Available from: www.msac.gov.au [Accessed Muir, J. A. (2001). Evidence-based healthcare. second edition Churchill Livingstone, Edinburgh. Mukari, S. Z., Tan, K. Y. & Abdullah, A. (2006). 'A pilot project on hospital-based universal newborn hearing screening: Lessons learned', International Journal of Pediatric Otorhinolaryngology, 70 (5), 843-851. Murray, J., Cuckle, H. et al (1999). 'Screening for cystic fibrosis.' Health Technology Assessment, 3 (8), i-iv, 1 - 104. Mytton, J. & Mackenzie, I. (2005). 'Observed and expected prevalence of permanent childhood hearing impairment in Oldham', Journal of public health (Oxford, England), 27 (3), 298-302. NCHAM (2003). What does a newborn hearing screening program cost? [Internet]. National Center for Hearing Assessment and Management (NCHAM). Available from: www.infanthearing.org/resources/cost/index.html [Accessed 1/07/03]. Neary, W., Kent, S. et al (2003). 'The Role of Audiological Testing and Computed Tomography in the Aetiological Investigation of Children with Permanent Unilateral Hearing Loss', Audiological Medicine, 1 (4), 215-223. Nekahm, D., Weichbold, V. et al (2001a). 'Improvement in early detection of congenital hearing impairment due to universal newborn hearing screening', International Journal of Pediatric Otorhinolaryngology, 59 (1), 23-28. Nekahm, D., Weichbold, V. & Welzl Muller, K. (2001b). 'Epidemiology of permanent childhood hearing impairment in the Tyrol, 1980-94', Scandinavian audiology, 30 (3), 197-202. Neumann, K., Gross, M. et al (2006). 'Effectiveness and efficiency of a universal newborn hearing screening in Germany', Folia Phoniatr Logop, 58 (6), 440-455. Ng, P. K., Hui, Y. et al (2004). 'Feasibility of implementing a universal neonatal hearing screening programme using distortion product otoacoustic emission detection at a university hospital in Hong Kong', Hong Kong Medical Journal, 10 (1), 6-13.

Universal neonatal hearing screening 265
NHMRC (2000a). How to review the evidence: systematic identification and review of the scientific literature, National Health and Medical Research Council, Canberra. NHMRC (2000b). How to use the evidence: assessment and application of scientific evidence, National Health and Medical Research Council, Canberra. NHS Centre for Reviews and Dissemination (2001). Undertaking systematic reviews of research on effectiveness: CRD's guidance for those carrying out or commissioning reviews, CRD Report 4. 2nd edition. Nussbaum, D. (1999). About hearing loss [Internet]. series number 5001. Laurent Clerc National Deaf Education Center, Galludet University. Available from: http://clerccenter.galludet.edu/SupportServices/series/5001.html [Accessed 24 July 2003]. OECD (2003). Prices and Purchasing Power Parities [Internet]. Organisation for Economic Co-operation and Development. Available from: http://www.oecd.org/topicstatsportal/0,2647,en_2825_495691_2759297_1_1_1_1,00.html#500300 [Accessed 20/08/03]. Oudesluys-Murphy, A. M. & Harlaar, J. (1997). 'Neonatal hearing screening with an automated auditory brainstem response screener in the infant's home', Acta Paediatrica, 86, 651 - 655. Owen, M., Webb, M. & Evans, K. (2001). 'Community based universal neonatal hearing screening by health visitors using otoacoustic emissions', Archives of disease in childhood. Fetal and neonatal edition, 84 (3), F157-162. Owens, R. (1996). Language development. Fourth edition Allyn and Bacon, New York. Pastorino, G., Sergi, P. et al (2005). 'The Milan Project: A newborn hearing screening programme', Acta Paediatrica, International Journal of Paediatrics, 94 (4), 458-463. Prieve, B., Dalzell, L. et al (2000). 'The New York State universal newborn hearing screening demonstration project: outpatient outcome measures', Ear and Hearing, 21 (2), 104-117. Pugh, M. (2000). Stedman's medical dictionary. 27th edition, Lippincott Williams & Wilkins, Philadelphia. Rao, A., Anderson, G. & Zack, J. (2002). 'A collaborative early hearing detection and intervention program for five rural hospitals', International Pediatrics, 17 (2), 102-106. Robles, L. & Ruggero, M. A. (2001). 'Mechanics of the mammalian cochlea', Physiological Reviews, 81 (3), 1305-1352. Rouev, P., Mumdzhiev, H. et al (2004). 'Universal newborn hearing screening program in Bulgaria', International Journal of Pediatric Otorhinolaryngology, 68 (6), 805-810. Russ, S. A., Poulakis, Z. et al (2003). 'Epidemiology of congenital hearing loss in Victoria, Australia', International Journal of Audiology, In Press.

266 Universal neonatal hearing screening
Russ, S. A., Rickards, F. et al (2002). 'Six year effectiveness of a population based two tier infant hearing screening programme', Archives of Disease in Childhood, 86 (4), 245-250. Schauseil-Zipf, U. & Von Wedel, H. (1988). 'Hearing screening by means of acoustic evoked brain stem potentials in newborns and infants', Klinische Padiatrie, 200 (4), 324-329. Schersten, T., Baile, M. A. et al (1999). Prostate cancer screening., The Swedish Council on Technology Assessment in Health Care (SBU); Basque Office for Health Technology Assessment (OSTEBA); Department of Health Basque Government., Vitoria-Gasteiz. Scott, M. E. & Bhattacharyya, N. (2002). Auditory brainstem response audiometry [Internet]. e-medicine. Available from: www.emedicine.com/ENT/topic473.htm [Accessed 28/04/03]. Shoup, A. G., Owen, K. E. et al (2005). 'The Parkland Memorial Hospital experience in ensuring compliance with universal newborn hearing screening follow-up', Journal Of Pediatrics, 146 (1), 66-72. Smyth, V., McPherson, B. et al (1999). 'Otoacoustic emission criteria for neonatal hearing screening', International Journal of Pediatric Otorhinolaryngology, 48 (1), 9-15. Stata Corporation. (2001). Intercooled stata 7.0 for windows 98/95/NT [computer program], Stata Corporation, College City, Texas. Stewart, D. L., Mehl, A. et al (2000). 'Universal newborn hearing screening with automated auditory brainstem response: a multisite investigation', Journal of Perinatology, 20 (8 Pt 2), S128-131. Stone, K. A., Smith, B. D. et al (2000). 'Universal newborn hearing screening', Journal of Family Practice, 49 (11), 1012-1016. Swanepoel, D., Ebrahim, S. et al (2007). 'Newborn hearing screening in a South African private health care hospital', International Journal of Pediatric Otorhinolaryngology, 71 (6), 881-887. Tatli, M. M., Bulent Serbetcioglu, M. et al (2007). 'Feasibility of neonatal hearing screening program with two-stage transient otoacoustic emissions in Turkey', Pediatr Int, 49 (2), 161-166. Thompson, D. C., McPhillips, H. et al (2001). 'Universal newborn hearing screening: summary of evidence', Jama, 286 (16), 2000-2010. Tsuchiya, H., Goto, K. et al (2006). 'Newborn hearing screening in a single private Japanese obstetric hospital', Pediatr Int, 48 (6), 604-607. UK National Screening Committee (2000). Second report of the UK national screening committee., Health Departments of the United Kingdom, London. Uus, K. & Bamford, J. (2006). 'Effectiveness of population-based newborn hearing screening in England: Ages of interventions and profile of cases', Pediatrics, 117 (5), e887-e893.

Universal neonatal hearing screening 267
Van Naarden, K., P., D. & Caldwell, K. (2000). 'Prevalence and characteristics of children with serious hearing impairment in metropolitan Atlanta, 1991-1993', Pediatrics, 103 (3), 570-575. Vohr, B. R., Carty, L. M. et al (1998). 'The Rhode Island Hearing Assessment Program: experience with statewide hearing screening (1993-1996)', J Pediatr, 133 (3), 353-357. Vohr, B. R., Oh, W. et al (2001). 'Comparison of costs and referral rates of 3 universal newborn hearing screening protocols', J Pediatr, 139 (2), 238-244. Wake, M., Hughes, E. K. et al (2003). 'Outcomes of children with mild-profound congenital hearing loss at 7-8 years: a population study', Ear and Hearing, (In Press). Wake, M., Poulakis, Z. et al (2005). 'Hearing impairment: a population study of age at diagnosis, severity, and language outcomes at 7-8 years', Archives of Disease in Childhood, 90 (3), 238-244. Walter, S. D. (2003). 'Mammographic screening: case-control studies', Ann Oncol, 14 (8), 1190-1192. Watkin, P. M. & Baldwin, M. (1999). 'Confirmation of deafness in infancy', Archives of Disease in Childhood, 81 (5), 380-389. Watkin, P. M., Baldwin, M. et al (1998). 'Maternal anxiety and attitudes to universal neonatal hearing screening', British Journal of Audiology, 32 (1), 27-37. Watkin, P. M., Baldwin, M. & Laoide, S. (1990). 'Parental suspicion and identification of hearing impairment', Archives of Disease in Childhood, 65 (8), 846-850. Weichbold, V., Nekahm-Heis, D. & Welzl-Mueller, K. (2006). 'Ten-year outcome of newborn hearing screening in Austria', International Journal of Pediatric Otorhinolaryngology, 70 (2), 235-240. Weichbold, V. & Welzl Mueller, K. (2001). 'Maternal concern about positive test results in universal newborn hearing screening', Pediatrics, 108 (5), 1111-1116. Weinrich, J. E. (1972). 'Direct economic costs of deafness in the United States', American Annals of the Deaf, 117 (4), 446-454. Weirather, Y. P., Korth, N. et al (1997). 'Cost analysis of TEOAE-based universal newborn hearing screening', Journal of Communication Disorders, 30 (6), 477-493. White, K. R. (1997). 'Universal newborn hearing screening issues and evidence', Conference Proceeding: Early Hearing Detection and Intervention, Atlanta, Georgia, In: Universal newborn hearing screening issues and evidence, White, K. R., Vohr, B. R. et al (2005). 'A multisite study to examine the efficacy of the otoacoustic emission/automated auditory brainstem response newborn hearing screening protocol: research design and results of the study', Am J Audiol, 14 (2), S186-199.

268 Universal neonatal hearing screening
White, S. J. & White, R. E. (1987). 'The effects of hearing status of the family and age of intervention on receptive and expressive oral language skills in hearing-impaired infants', AHSA Monographs, (26), 9-24. Whiting P, R. A., Reitsma JB, Bossuyt PM, Kleijnen J. (2003). 'The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews.' BMC Med Res Methodol., 3 (1), 25. Yee-Arellano, H. M., Leal-Garza, F. & Pauli-Muller, K. (2006). 'Universal newborn hearing screening in Mexico: Results of the first 2 years', International Journal of Pediatric Otorhinolaryngology, 70 (11), 1863-1870. Yoshinaga-Itano, C., Coulter, D. & Thomson, V. (2001). 'Developmental outcomes of children with hearing loss born in Colorado hospitals with and without universal newborn hearing screening programs', Semin Neonatol, 6 (6), 521-529. Yoshinaga Itano, C., Coulter, D. & Thomson, V. (2000). 'The Colorado Newborn Hearing Screening Project: effects on speech and language development for children with hearing loss', Journal of Perinatology, 20 (8 part 2), S132-137. Zaputovic, S., Stimac, T. et al (2005). 'Molecular analysis in diagnostic procedure of hearing impairment in newborns', Croatian Medical Journal, 46 (5), 797-800.