-
8/11/2019 Unit 25 Adminstration
1/31
-
8/11/2019 Unit 25 Adminstration
2/31
individual treatment plans; to give skilled nursing care and
therapy; and to direct, monitor, and evaluate
the nursing care furnished.
(2)The staffing pattern must insure the availability of a
registered professional nurse 24 hours each
day. There must be adequate numbers of registered nurses,
licensed practical nurses, and mental health
workers to provide the nursing care necessary under each
patient's active treatment program.
(e)Standard: Psychological services.The hospital must provide or
have available psychological
services to meet the needs of the patients.
(f)Standard: Social servi ces.There must be a director of social
services who monitors and evaluates
the quality and appropriateness of social services furnished.
The services must be furnished in
accordance with accepted standards of practice and established
policies and procedures.
(1)The director of the social work department or service must
have a master's degree from an
accredited school of social work or must be qualified by
education and experience in the social services
needs of the mentally ill. If the director does not hold a
masters degree in social work, at least one staffmember must have
this qualification.
(2)Social service staff responsibilities must include, but are
not limited to, participating in discharge
planning, arranging for follow-up care, and developing
mechanisms for exchange of appropriate,
information with sources outside the hospital.
(g)Standard: Therapeutic activit ies.The hospital must provide a
therapeutic activities program.
(1) The program must be appropriate to the needs and interests
of patients and be directed toward
restoring and maintaining optimal levels of physical and
psychosocial functioning.
(2)The number of qualified therapists, support personnel, and
consultants must be adequate to provide
comprehensive therapeutic activities consistent with each
patient's active treatment program.
Model for Minimum Staffing Patterns for Hospitals Providing
Acute Inpatient Treatment for
Children and Adolescents with Psychiatric Illnesses.
Acute psychiatric treatment for children and adolescents
requires the use of intensive and complex
resources. We have the responsibility to our patients to ensure
the quality and effectiveness of thistreatment. The standards are
designed to be a minimum in terms of both staffing structure and
numbers
of staff.
Various factors of patient selection and program objectives
require increased staffing. Training ad
research programs are examples. It should be noted that the
requirements for psychiatrists are fordiagnostic and psychiatric
management only. Individual and family psychiatrists are for
diagnostic and
psychiatric management only. Individual and family
psychotherapy, done by the attending
psychiatrists, are considered to require additional time
commitment.
The availability of a sufficient number of high quality staff is
an absolute necessity to qualify a
program to provide acute psychiatric hospital treatment. While
there are many appropriate variations in
programs and staffing, it is important that a model be
established for minimum patterns of staffing.
-
8/11/2019 Unit 25 Adminstration
3/31
Team and Authority
Staffing for an inpatient program depends on the mission of the
program, severity of the illness, the
degree of impairment, and the complexity of the situation.
Program focus and physical design interactwith program staffing.
The responsibility for balancing these interactive factors rests
with the program
administrative team.
At a minimum, the program administrative team with the
responsibility for the entire treatmentprogram must include a
qualified child and adolescent psychiatrist, and a qualified
psychiatric nurse.
The program must be consistent with a hospital administration as
conveyed by an appropriate
representative of the administration.
The program is developed by the administrative team and approved
by the medical staff and hospitaladministration.
Staffing and program organization and other ancillary services
such as psychology, education, social
work, pediatric medicine and occupational therapy, need to be
professionals in those disciplines.
It is the responsibility of the child and adolescent
psychiatrists to maintain the integrity of professionaljudgements
and behaviors independent of influence of the source of
compensation (Principles of
Practice of the American Academy of Child and Adolescent
Psychiatry).
The staff of various disciplines must meet the facility's
specific written criteria for credentials andclinical
privileges.
The administrative team has the responsibility for a program of
continuous quality improvement.
Attending Psychiatrist
Credentials:
A licensed physician who has completed an approved program in
child and adolescent psychiatry. Forpatients 14 years of age and
older, a general psychiatrist with documented specialized
training,
supervised experience and demonstrated competence in work with
adolescents and their families, may
be considered a qualified attending psychiatrist. Continuing
medical education is essential.
Ratio:
There will be a sufficient number of qualified attending
psychiatrists to prove the basic functions of
evaluations, admissions, diagnoses, prescribing of treatment,
and discharging patients, and to supervisethe clinical treatment
team.
Basic Functions:
At a minimum, functions must be performed as outlined at the
frequency prescribed in theDocumentation of Medical Necessity of
Child and Adolescent Psychiatric Treatment: Guidelines for
Use in Managed Care, Third-Party Coverage and Peer Review
(AACAP, October 1990).
At a minimum, the attending psychiatrists must document
psychiatric management with progress notesevery three days.
At a minimum and not including individual, group or family
psychotherapy, the attending psychiatristmust spend sufficient
hours per week in the patient's psychiatric management and
treatment to properly
provide for admission, discharge, treatment team, family and
staff conferences, ordering and
supervising treatment, communication with parents, ongoing
psychiatric assessment, and
-
8/11/2019 Unit 25 Adminstration
4/31
documentation. Week-by-week the time will increase or decrease
according to the number of
admissions, initial evaluations, basic evaluations or
comprehensive examinations. Ordinarily it would
be expected that these responsibilities would require no less
than 2.5 hours per week.
This minimum number of hours will need to be increased to
account for additional medical factors,
training and research.
Social Worker or Other Professional Responsible for Family
Contacts
Credentials:
Mental health professional who has a master's degree in social
work or related field. A mental health
professional with a bachelor's degree supervised by a
master's-level social worker is also considered
qualified. Continuing education and in-service training is
essential.
The staff must include at least one social worker who has
experience in child and adolescent inpatienttreatment.
Ratio:
The number of social workers, or another discipline charged with
family assessment and family
contacts per week, should be at least one-full time equivalent
to 10 patients. The number of staff may
need to increase if extensive supplementary functions are
included.
Basic Functions:
A basic family assessment within three days of admission.
A comprehensive social assessment within 14 days.
A weekly family and/or agency contact and progress note
documenting the staff's active involvement in
the implementation of treatment plan goals.
Coordination of discharge planning. Participation in at least
one treatment team meeting a week.
Supplemental Functions:
Family therapy and group therapy.
Family, parent and patient education.
Psychiatric Nurses
Credentials:
Registered nurse with appropriate state license supervised by a
qualified psychiatric nurse, i.e., abachelor's - or - master's -
level nurse with experience in child and adolescent psychiatric
inpatientnursing. Continuing education and in-service training is
essential.
Ratio:
A program requires one psychiatric nurse per shift for each 12
patients. An additional group of 10
patients. This number also needs to be adjusted according to the
acuity, medical treatment, medication
and extensive functions.
-
8/11/2019 Unit 25 Adminstration
5/31
Basic Functions:
Initial assessment of patient's nursing needs and documentation
of nursing needs and documentation ofnursing components of an
initial treatment plan.
A daily assessment and documentation of the patient, the
patient's treatment and response to treatment.
Supervision of assessments done by psychiatric technicians and
countersigning of their documentation. Provision and documentation
of medical treatment and medication as needed.
Development of the appropriate psychiatric nursing components of
the treatment plan.
Implementation of the interventions in the treatment plan that
are designated for psychiatric nurses.
Implement milieu management.
Health teaching.
Supplemental Functions:
Primary nursing.
Individual milieu interventions (individualized behavioral
management).
Group therapy. Specialized treatment for high-acuity patients,
e.g., suicidal, assaultive, severely disorganized,
elopement risk, acute medical distress (unstable diabetes or
asthma).
Child and Adolescent Psychiatric Technician
Also known as a child care worker, mental health specialist,
child care specialist, mental health
associate.
Credentials:
Educational credentials vary. Extensive pre-service and ongoing
in service training is essential. The
assignment of clinical responsibilities must consider careful
evaluation of the combination of training,experience and personal
characteristics such as maturity, empathy and objectivity.
Ratio:
This is determined by considering general/generic supervision in
the treatment milieu. (See finalsection on generic staffing).
Basic Functions:
Establish and maintain behavioral supervision of children.
Maintain implementation of safe, therapeutic milieu.
Implement specific assigned aspects of the treatment plan.
Observe, assess, and document the patient's status.
Assist in planning and supervision of leisure activities.
Participate in the observation and documentation of the
patient's treatment.
Functions Shared By Nur se and Psychiatri c Technician:
Certain functions are done by the nurse and/or psychiatric
technician.
-
8/11/2019 Unit 25 Adminstration
6/31
Observation, assessment and documentation of the patient's
condition on each shift. Where the
observation and documentation is done by the psychiatric
technician, the note is countersigned by the
nurse responsible for the patient on that shift.
Supervision of the patients and maintaining the safety and
therapeutic quality of the milieu. (Both have
responsibility for this).
Assisting, as necessary, the children in their daily activities,
including leisure activities, transportation,activities related to
personal hygiene.
Shared Supplemental F unctions:
Individual patient discussions.
Assisting in group therapy.
Leading various therapeutic activities.
Mental health education with parents and patients.
Behavioral management classes.
Ratio for General Staffing/Generic Supervision
In these parameters, units are considered to be from 9 to 24
child or adolescent patients.
When the children are occupied primarily in the program unit
during the day and evening, the
minimum number is three staff to nine patients, proceedings in a
three-to-one ratio.
With this staffing pattern staff can accomplish their basic
responsibilities. Supplemental complex or
intensive interventions will require additional staffing.
When 18 or fewer patients located on one program unit are
asleep, the minimum number of staff is
two. With over 18 patients asleep, the minimum level is three
staff. In either case, there must be anadditional person available
to help with sudden change in acuity. This should not reduce the
basic
staffing on another unit.At night, when the patients are asleep
there should be one nurse to 50 patients per shift with an
on-callnurse who can come on site.
Ratios are dependent on such variables as the number of children
in the living unit, the physical
configuration of the facilities, the acuity including
developmental levels, the frequency of turnover andlength of stay,
and the availability of off-unit activities, e.g., specialized
recreational activities.
Other Staffing Requirements:
Children and adolescents treated in acute psychiatric hospital
programs require additional special staff.
Due to the variability in program structure and patient
characteristics, the number of staff is not
specified. Staff must be available to meet the following program
and supervisory functions:
Psychological Services:
Sufficient licensed psychologist to provide relevant and
appropriate psychological testing. Cognitive
evaluation is particularly important. In some programs,
psychologists may be involved in treatment
plan development, individual, group and family psychotherapy and
other types of therapeuticintervention.
-
8/11/2019 Unit 25 Adminstration
7/31
Educational Services:
Educators to assess academic achievement and needs, maintain
educational progress and accomplish
transfer into an appropriate post-hospital educational program.
Patients need an educational program 5days per week under the
direction of a special educator.
Therapeutic Recreation Services:
A therapeutic recreation program provided 7 days per week under
the direction of a certified recreationtherapist.
Relevant and Appropriate Consultation in the Following
Areas:
Medical specialties
Speech and hearing evaluation
Occupational therapy
The Council of the American Academy of Child and Adolescent
Psychiatry accepted these Guidelinesfor Minimum Staffing in 1990.
The Academy has led in the development of policies, position
statements and review standards. These labor-intensive efforts
are fueled by the Academy's pledge toassure our patients and their
families an adequate quality of medically necessary psychiatric
treatment.
PLANNING EQUIPMENTS AND SUPPLIES
Functional, accurate and safe clinical equipments is an
essential requirements in the provision of healthservices. Well
maintained equipments will give nurses greater confidence in the
reliability of its
performance and contribute to a high standard of client care .
Equipment management is an important
issue for cost and safety in hospitals operations. Planning of
equipment and supplies recommends that
at the outset of each project,; identify project goals,
including clinical priorities, budget, schedule andphasing
Medical equipment and supplies:
Equipments are defined as those items necessary for the
functioning of all services of the facility suchas accounting and
records, maintenance of buildings and grounds, laundry, public
waiting rooms,public health and related services.
The term equipment is used for more permanent type of article
and may be classified as fixed and
movables. Fixed equipment is not a structure of the building,
but it is attached to the walls or floors
(egg; steriliser,) Movable equipment includes furniture,
instruments etc.
Supplies are those items that are used up or consumed; hence the
term consumable is used for supplies.
The supplies in hospital include drugs, surgical goods
(disposables, glass wares), chemicals,
antiseptics, food materials, stationeries, the linen supply
etc.
Definition of planning equipments and supplies:
Planning of equipments and supplies is defined as process of
selection and organization of the articlesor items used in the
diagnosis, treatment, and monitoring of patients in order to ensure
that they are
safe, available, accurate, and affordable.
-
8/11/2019 Unit 25 Adminstration
8/31
Need of planning equipments and suppplies:
Medical equipment and supplies planning includes all the related
policies and procedure governactivities from selection and
acquisition through to the incoming inspection, acceptance,
maintenance
and eventual retirement and disposal of medical
equipment.Planning and management of all
equipments and supplies used in hospital is need to be done to
;
ensure that equipment and supplies used in patients care are
operational, safe, and properly configured
to meet the mission of the medical treatment facility.
manage safety and cost of articles.
overcome the problems in nursing care or other patient related
activities due to inadequacy in
equipments and supplies.
stabilize fluctuations in consumptions.
provide reasonable level of client services.
satisfy the demands during the period of replenishment.
cross bureaucratic hurdles in case of imported equipments. know
about possible legal or licensure issues.
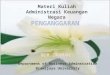
Phases of equipment management:
A typical life cycle of medical equipment has the following
phases:
1. Planning phase:
The following conditions that should be met to help the decision
process in planning phase:
Demonstrated clinical needs.
Availability qualified users.
Aproved and reassured source of recurrent operating budget.
confirmed maintenance services and support.
Adequate environment support.
A clear cut policy should be there on acquisition, utilization
and maintenance of equipment need to be
established.This will help to reduce any future problems arising
out of contracts, spare parts and
maintenance of equipment acquired locally, internationally.
PLANNING
COMMISIONING &
ACCEPTANCEPROCUREMENT
MAINTENANCEMONITORING
OF USE &
PERFORMANCE
DE- COMMISIONING
-
8/11/2019 Unit 25 Adminstration
9/31
2. Procurement phase:
Standardize on models or manufacturers of equipment.
Specify the conditions and special requirements in the purtchase
order to specify the supplier withholdpayment if specified
conditions are not met.
3.
Incoming inspections: Incoming inspections should be carefully
checked for possible damages; compliance with
specifications in the purchase ordere; and delivery of
accessories, spare parts and operating and servicemanuals.
4. Equipment inventory and documentation system:
It provides information to support different aspects of medical
equipment management;
Inventory entries should includes accessories, spare parts and
operating and service manuals.
Make copies of the manuals for distribution to the users, while
the originals of the manuals should bekept at the technical
document library for safekeeping.
5.
Commissioning and acceptance: Commissioning can be carried out
by hospital technical staff.if they are familiar with that item
of
equipment. If commissioning by the suppliers is needed , the
process should be monitored by hospital
technical staff so that any technical matters can be noted and
recorded.
6. Monitoring of use and performance:
A link should be maintained between user and supplier and
observe any suppliers technical services.
7. Maintenance:
Proper maintenance of equipment is essential to obtain sustained
benefits and to preserve capital
investment . Equipment must be maintained in working order and
periodically calibrated foreffectiveness and accuracy. Proper
maintenance has a direct impact on the quality of care.
8. De-commissioning:
Repair existing old equipments.
Dismantle old units if required.
De-Commisioned equipment must be deleted to keep the inventory
current.
INVENTORY ANDDOCUMENTATION
INCOMINGINSPECTION
-
8/11/2019 Unit 25 Adminstration
10/31
Factors affecting selection and planning of equipment
1. Type of service provided by the hospital: A maternity
hospital requires more equipment related to
gynaecologic procedures than a cardiac hospital.
2. Age of patients:children need different type and amount of
equipments than adults.
3.
Sex-Men and women sometime require different type of
equipment.4. Degree and type of illness-neurologic patients
sometimes require more bedsides, rubber mattress and
linen than patients with other type of illness.
5. Cost of items-cost of items will limit the purchase of number
of equipment.
General utility services in the hospital
1. Electric supply and installations : A hospital must have a
steady electrical supply at a stable voltage.
Voltage fluctuations play havoc with sophisticated electronic
equipment, endoscope, sterilisers, X-ray
equipments etc. While planning hospital departments, provision
should be made for voltage
stabilisation in areas with heavy concentration of electrical
and electronic equipment. This is preferredover using voltage
stabilisers with individual equipment. There should be an emergency
generator
capable of supplying power to all emergency areas of the
hospital. This generator should be of right
capacity and kept in working order by periodic test runs.
2. Water supply : Since safe water supply is not always assured,
hospitals must have their own
purification system. Also there should be plumbing system.
3. Disposal of wasteliquids and solids: Disposal of waste both
solid and liquid is a totally neglected
area. A hospital incinarator good for the waste management.
4.
Refrigeration, air conditioning, ventilation and environment
control: Air conditioning is requiredfor protection of
sophisticated electronic equipment, X ray, machines etc.
5. Transport : Lifts are needed for vertical transport. There
should be separate lifts for patients, visitors,staff and supply.
Patients lift should accommodate a standard hospital bed. Sides of
the lift must be
protected to prevent damage by trolleys. Lift surfaces and
flooring should be capable of easy cleaning
and disinfection. Ventilation, communication and emergency
escape system should be provided on alllifts. As for horizontal
transport also trolleys and ramps with gentle gradient are
useful.
6. Supply of medical gases , compressed air, hot water, vacuum
suction and gas plants: Piped supply
of medical gases , compressed air, vacuum suction , hot water,
steam, necessitates thoughtful planning
at all stages to consider problems of
Easy uninterrupted safe supply
Fire and explosion hazards
Easy of servicing and maintenance without disrupting hospital
services.
7. Laundry: A hospital laundry has 2 separate areas, with
provision for decontamination and sterilising
of soiled linen.
-
8/11/2019 Unit 25 Adminstration
11/31
-
8/11/2019 Unit 25 Adminstration
12/31
o blood counter
o analytical balance
o calorimeter( spectrophotometer)
o Centrifugea small centrifuge that can accommodate six 15ml
tubes should be available.
o Water bathused for stabilising temperature at 25, 37, 42, or
56degree Celsius.
o
Incubator/oven- a small hot air oven to carry out standard
cultivations and sensitisations. Refrigeratoran ordinary household
refrigerator with a freezer unit, for storing preparations,
vaccines,
blood etc.
Distillation and purification apparatus - it should be made of
metal that resists acid, and alkali and
should be free standing.
3) Electrical medical equipment.
Portable electrocardiograph
Defibrillator( external)
Portable anaesthetic unit2 small aesthetic units should be
obtained, complete with a range of masks.
Respiratorit should be applicable for prolonged administration
during post operative care. Dental chair unit- a complete unit
should be available to carry out standard dental operations.
Suction pumpone portable and one other suction pump are
required.
Operating theatre lamp- one main lamp with at least 8 shadows
lamp and an auxiliary of 4 lamp units.
Delivery table- it should be standard and manually operated.
Diathermy unit a standard coagulating unit which is operated by
hand or foot switch, with variable
poor control.
4) Other equipment
autoclavefor general stabilisation
Small sterilisers- for specific services- eg. Stabiliser cold
chain and other preventive medical equipment
ambulance
5) Small , inexpensive equipment and instruments
Equipment and instrument, such as BP apparatus, oxygen
manifolds, stethoscope, diagnostic sets andspotlights.
Equipment and supplies required during emergency
The World Health Organization (WHO), in consultation with other
international organizations, has adopted astandard classification
that places humanitarian supplies in 10 different categories. This
form of identification is
particularly useful for the sorting and recording of supplies
during emergency or disaster:The categories arethe following:
Medicines,
Water and environmental health,
-
8/11/2019 Unit 25 Adminstration
13/31
Health supplies/Kits,
Food,
Shelter/Electrical/Construction,
Logistics/Administration,
Personal needs/Education,
Human resources,
Agriculture/Cattle
Unsorted.
Role of nursing managers in maintaining equipment and
supply:
The nurse manager should apply system approach for maintaining
equipment and supply in nursing unit.
INPUT:
The main objective of input component is to ensure adequate
supply of equipment ad supplies of nursing unit.
The nurse managers need to:
Take active part in estimating the demand of equipment and
supply.
Be aware of hospital policy for requirement , indenting, stock
etc.
Nursing norms for equipment and supply as per nursing
council.
Develop ward policy as per requirement.
Communicate higher authority about the gap between demand and
supply.
Conduct meetings with superiors and subordinates for requirement
.
Prepare guidelines for handling and taking over for the
staff.
PROCESS:
Objective:
To maximize the proper utilization of available equipment and
supply by the staff and proper
maintenance of equipment and supplies.
Mainten current inventory of functional/in working order
equipment and supplies.
Send requisition monthly, weekly, daily as per the policy
developed.
Have inventory control, maintain buffer stock for emergency.
Do proper distribution for evening , night shift.
Conduct supervisory round.
-
8/11/2019 Unit 25 Adminstration
14/31
Check daily and periodically the functioning of emergency and
general equipment andlife saving
equipment.
Assign and delegate the work to junior staff.
Make them accountable for any loss and misuse of equipment and
supplies.
Ask them to use the articles for rendering patient care.
Communicate all the team members about the out of stock and non
functioning of equipment.
Develop orientation plan for the patient and their relatives
about the availability and non availability of
particular article, equipment and supplies and ward policy.
Maintain record and report of equipment and supplies.
Regularly maintain the equipment and supply.
Condemn the non functioning and outdated equipment as per
policy.
Check all the work has been done.
OUTPUT:
Objective:
To render quality patient care;
All the staff should be aware of policy: hospital, ward related
to equipment and supply.
There should be adequate supply of equipment and supplies
without any interruption.
Equipment s should be in working order.
HOSPITAL POLICIES AND PROCEDURES.
(1) The governing body must ensure that a written policies and
procedures manual is maintained. In
addition to meeting the requirements of rule. Policies and
Procedures for all facilities, themanual mustinclude the following
elements:
(a) A quality assurance procedure for the assessment of the
quality of care. This procedure must
ensure appropriate treatment has been delivered according to
acceptable clinical practice;
(b) A written program description which must be available to
staff, patients and members of the
public. The description must include, but need not be limited
to, the following:
1. Characteristics of the persons to be served,2. Referral
process,
3. Program rules for patients, and4. Referral mechanisms for
services outside the facility (both medical and non-medical);
And
(c) Procedures to ensure how the patients parents, guardian,
members of the immediate family or
other responsible adult are to be notified in the case of any
unusual occurrence including
-
8/11/2019 Unit 25 Adminstration
15/31
serious illness, accidents or death.
QUALITY ASSURANCE
DEFINITION:-Qual ity assurance:-
Quality assurance is a management system designed to give
maximum guarantee and ensure
confidence that the service provided is up to the given accepted
level of quality, the standards
prescribed for that service which is being achieved with a
minimum of total expenditure.
(British Standards Institute)
Quality assurance "Quality assurance is the monitoring of the
activities of client care to determine the
degree of excellence attained to the implementation of the
activities". (Bull, 1985)
Quality assurance is a judgment concerning the process of care,
based on the extent to which that cares
contributes to valued outcomes. (Donabedian 1982)
Quality Assurance is the definition of nursing practice through
well written Nursing standards and the
use of those standards as a basis for evaluation on improvement
of client care. (Marker 1998)
Quality assurance system motivates nurses to strive for
excellence in delivering quality care and to be
more open and flexible in experimenting with innovative ways to
change outmoded systems.
OBJECTIVES OF QUALITY ASSURANCE:-
According to Jonas (2002), the two main objectives are:-
To ensure the delivery of quality client care
To demonstrate the efforts of the health care providers to
provide the best possible results.
NURSING SERVICE:-
Formulate plan of care Attend to the patients physical and non
physical needs
Evaluate achievement of nursing care
Support delivery of nursing care with administrative and
managerial services
NURSING EDUCATION: - (Decker, 1985 and Schroeder, 1984)
-
8/11/2019 Unit 25 Adminstration
16/31
To provide technical assistance in designing and implementing
effective strategies for monitoring
quality and correcting systemic deficiencies.
To refine existing methods for ensuring optimal quality health
care through an applied research
programme
PRINCIPLES:-
The main 8 Principles of Quality Assurance. Quality Assurance
principles are based on the ISO 9001
standard and are intended to be used by senior Quality Managers
to run a business based on continual
improvement and quality assurance
1. Customer focus: - The customer is always the most important
factor for any business, which is why
organisations need to understand current and future customer
needs and aim to surpass expectations.
Quality assurance relies on researching and understanding the
customers needs and ensuring that the
organisations objectives are in line with those expectations. A
quality management system needs to be
in place to manage customer relationships and communicate those
needs across the organisation.
2. Leadership:-Quality assurance principles also suggest that an
organisation needs leadership in order
to have purpose and direction. Quality assurance relies on a
business having a clear vision of the future
a vision which should consider the needs of all relevant parties
including customers, directions,
employees, local community etc. Good leadership within an
organisation should establish trust and
remove fear, whilst encouraging and recognising employees
contributions
3. Involvement of people: - An organisation needs to be able to
put quality management training into
practice. People at all levels of the business need to be
motivated, committed and fully involved in the
organisation. This principle of quality assurance involves
people evaluating their own performance and
identifying their constraints, as well as actively seeking
opportunities
4. Process approach: - ISO 9001 training encourages that in
order to achieve a desired result, resources
and activities should be managed as a process. The process
should focus on resources, methods and
materials which affect the key activities within a business. In
order to maintain quality assurance within
a service or product, risks, consequences, the impaction
customers and suppliers and other relevant
parties should be continuously evaluated
5. System approach to management:- Quality assurance training
demonstrates how to create a structure
system which is designed to achieve the organisations aims and
objectives using the most effective and
efficient methods. Quality management system training should
provide a better understanding of the
-
8/11/2019 Unit 25 Adminstration
17/31
-
8/11/2019 Unit 25 Adminstration
18/31
-
8/11/2019 Unit 25 Adminstration
19/31
other group techniques. Once a health facility team has
identified several problems, it should set quality
improvement priorities by choosing one or two problem areas on
which to focus. Selection criteria will
vary from program to program.
6. Defining the Problem Having selected a problem:-
The team must define it operationally-as a gap between actual
performance and performance as
prescribed by guidelines and standards. The problem statement
should identify the problem and how it
manifests itself. It should clearly state where the problem
begins and ends, and how to recognize when
the problem is solved.
7. Choosing a Team:-
Once a health facility staff has employed a participatory
approach to selecting and defining a problem,
it should assign a small team to address the specific problem.
The team will analyze the problem,
develop a quality improvement plan, and implement and evaluate
the quality improvement effort. The
team should comprise those who are involved with, contribute
inputs or resources to, and/or benefit
from the activity or activities in which the problem occurs.
8. Analyzing and Studying the Problem to Identify the Root
Cause:-
Achieving a meaningful and sustainable quality improvement
effort depends on understanding the
problem and its root causes. Given the complexity of health
service delivery, clearly identifying root
causes requires systematic, in-depth analysis. Analytical tools
such as system modeling, flow charting,
and cause-and-effect diagrams can be used to analyze a process
or problem. Such studies can be based
on clinical record reviews, health center register data, staff
or patient interviews, service delivery
observations.
9. Developing Solutions and Actions for Quality Improvement
The problem-solving team should now be ready to develop and
evaluate potential solutions. Unless the
procedure in question is the sole responsibility of an
individual, developing solutions should be a team
effort. It may be necessary to involve personnel responsible for
processes related to the root cause.
10. Implementing and Evaluating Quality Improvement
Efforts:-
-
8/11/2019 Unit 25 Adminstration
20/31
-
8/11/2019 Unit 25 Adminstration
21/31
d) Certification:- Certification is usually a voluntary process
with in the profession. A person's
educational achievements, experience and performance on
examination are used to determine the
person's qualifications for functioning in an identified
specialty area.
e) Charter- It is a mechanism by which a state government agency
under state law grants corporate
state to institutions with or without right to award
degrees.
f) Recognition- It is defined as a process whereby one agency
accepts the credentialing states of and
the credential confined by another.
g) Academic degree
II) SPECIFIC APPROACH: - These are methods used to evaluate
identified instances of provider
and client interactions.
a) Audit- It is an independent review conducted to compare some
aspect of quality performance, with a
standard for that performance. Nursing audit may be defined as a
detailed review and evaluation of
selected clinical records in order to evaluate the quality of
nursing care and performance by comparing
it with accepted standards
b) Direct observation- Structured or unstructured based on
presence of set criteria.
c) Appropriateness evaluation-The extent to which the managed
care organization provides timely,
necessary care at right levels of service.
d) Peer review- Comparison of individual providers practice
either with practice by the providers
peer or with an acceptable standard of care. To maintain high
standards, peer review has been initiated
to carefully review the quality of practice demonstrated by
members of a professional group. Peer
review is divided in to two types. One centers on the recipients
of health services by means of auditing
the quality of services rendered. The other centers on the
health professional by evaluating the quality
of individual performance.
e) Bench marking- A process used in performance improvement to
compare oneself with best
practice.
f) Supervisory evaluation
-
8/11/2019 Unit 25 Adminstration
22/31
g) Self-evaluation
h) Client satisfaction
i) Control committees
j) Services- Evaluates care delivered by an institution rather
than by an individual provider.
k) Trajectory- It begins with the cohort of a person who shares
distinguishing characteristics and then
follows the group going through the healthcare system noting
what outcomes are achieved by the end
of a particular period
l) Staging- It is the measurement of adverse outcomes and the
investigation of its antecedence.
m) Sentinel- It involves maintaining of factors that may result
in disease, disability or complications
such as;
Review of accident reports
Risk management
Utilization review
FACTORS AFFECTING QUALITY ASSURANCE IN NURSING CARE:-
1) Lack of Resources: Insufficient resources, infrastructures,
equipment, consumables, money forrecurring expenses and staff make
it possible for output of a certain quality to be turned out under
the
prevailing circumstances.
2) Personnel problems: Lack of trained, skilled and motivated
employees, staff indiscipline affects
the quality of care.
3) Improper maintenance: Buildings and equipments require proper
maintenance for efficient use. If
not maintained properly the equipments cannot be used in giving
nursing care. To minimize equipment
down time it is necessary to ensure adequate after sale service
and service manuals.
4) Unreasonable Patients and Attendants Illness, anxiety,
absence of immediate response to treatment,unreasonable and un
co-operative attitude that in turn affects the quality of care in
nursing.
5) Absence of well informed population: To improve quality of
nursing care, it is necessary that the
people become knowledgeable and assert their rights to quality
care. This can be achieved through
continuous educational program.
-
8/11/2019 Unit 25 Adminstration
23/31
6) Absence of accreditation laws:There is no organization
empowered by legislation to lay down
standards in nursing and medical care so as to regulate the
quality of care. It requires a legislation that
provides for setting of a stationary accreditation / vigilance
authority to:
8) Lack of good and hospital information system: A good
management information system is
essential for the appraisal of quality of care.
9) Absence of patient satisfaction surveys: Ascertainment of
patient satisfaction at fixed points on an
ongoing basis. Such surveys carried out through questionnaires,
interviews to by social worker,
consultant groups, and help to document patient satisfaction
10) Lack of nursing care records: Nursing care records are
perhaps the most useful source of
information on quality of care render.
ASSESSMENT OF QUALITY ASSURANCE:-
Quality assurance follows client care rather than organizational
structure, focus on process rather thanindividuals and uses a
systematic approach with the intention of improving the quality of
care The
main methods of assessing quality assurance are as follows:
1. Train ing the nur sing staff:- Training includes the
explanation of the purpose of each critical
indicator meaning of each criterion ,proper approach of data
collection.
2. Perf orming the audit:-An audit may be focused on the
particular medical diagnosis and related to
the patient care while he is in the hospital. Audit are of two
type
a) Concurrent audit-In this patient care is observed as it is
given
b)
Retrospective audit-In this patient care is evaluated only aeter
the discharge of patient.
3. Analysis of medical record data:- After screening of sampled
medical records ,the surveyor should
refer records showing variations from established criterion to
the desired task,so that they can
determine whether the variation is justified or corrective
action is taken.
4. Peer view:-Peer view is also one method for increasing
nursing accountability for effective decision
making and interventions.In this view mainly evaluate the
performance against accepted standards
-
8/11/2019 Unit 25 Adminstration
24/31
PRACTICE STANDARDS FOR PSYCHIATRIC NURSING:
The nursing process consist of six steps and uses a problem
solving approach that has come to be
accepted as nursings scientific methodology. It is goal directed
, with the objective being delivery
of quality client care.
STANDARDS OF CARE:
Standards of care pertain to professional nursing activities
that are demonstrated by the nurse
through the nursing process. These involve assessment,
diagnosis, outcome identification,
planning, implementation, and evaluation. The nursing process is
the foundation of clinical
decision making and encompasses all significant action taken by
nurses in providing psychiatric
mental health care to all clients.
STANDARD I. ASSESSMENT
The psychiatric/ mental health nurses collects patient health
data
The assessment interview which require linguistically and
culturally effective communication
skills, interviewing, behavioural observation, record review and
comprehensive assessment of the
patient and relevant system enable the mental health nurse to
make sound clinical judgement and
plan appropriate interventions.
STANDARD II. DIAGNOSIS:
The mental health nurse analyzes the assessment data in
determining diagnosis
Data gathered during the assessment are analysed. Diagnoses and
potential problem statement are
formulated and prioritized.
STANDARD III. OUTCOME IDENTIFICATION:
The mental health nurse identifies expected outcomes
individualized to the patient
Expected outcomes are derived from the diagnosis. They must be
measurable and estimate a time
for attainment. They must be realistic for the clients
capabilities, and are more effective when
formulated by the interdisciplinary members, the client, and
significant other together.
STANDARD IV. PLANNING:
The mental health nurses develops a plan of care that is
negotiated among the patient, nurse,
family, and health care team and prescribes evidence based
interventions to attain expected
outcomes.
A plan of care is used to guide therapeutic intervention
systematically, document progress, and
achieve the expected patient outcome. The care plan is
individualized to the clients mental health
problems, condition, or need and is developed in collaboration
with the client, significant others,
and interdisciplinary team member. For each diagnosis
identified, the most appropriateinterventions are selected.
-
8/11/2019 Unit 25 Adminstration
25/31
-
8/11/2019 Unit 25 Adminstration
26/31
-
8/11/2019 Unit 25 Adminstration
27/31
-
8/11/2019 Unit 25 Adminstration
28/31
PRESERVATION AND STORAGE
Written policies and procedures shall govern the compilation,
storage, dissemination and
accessibility of patient records. The policies and procedures
shall be designed to assure that the
facility fulfills its responsibility to safeguard and protect
the patient record against loss,
unauthorized alteration, or disclosure of information; to assure
that each patient record contains all
required information; to uniformity in the format and forms in
use in patient records; to require
entries in patient records to be dated and signed.
The facility shall provide facilities for the storage,
processing and handling of patient records,
including suitably locked and secured rooms and files. When a
facility stores patient data on
magnetic tape, computer files, or other types of automated
information systems, adequate security
measures shall prevent inadvertent or unauthorized access to
such data. A written policy shall
govern the disposal of patient records. Methods of disposal
shall be designed to assure the
confidentiality of information in the records.
PERSONNEL
The patient records department shall maintain, control and
supervise the patient records, and shall
be responsible for maintaining the quality.
A qualified medical record individual who is employed on at
least a part-time basis, consistent
with the needs of the facility and the professional staff, shall
be responsible for the patient records
department. This individual shall be a registered record
administrator or an accredited record
technician.
When it can be demonstrated that the size, location or needs of
the facility do not justify
employment of a qualified individual, the facility must secure
the consultative assistance of a
registered record administrator at least twice a year to assure
that the patient record department is
adequate to meet the needs of the facility.
CENTRALIZATION OF REPORTS
1 All clinical information pertaining to a patient's stay shall
be centralized in the patient's record.
2. The original or all reports originating in the facility shall
be filed in the medical record.
3. Appropriate patient records shall be kept on the unit where
the patient is being
treated and shall be directly accessible to the clinician caring
for the patient.
CONTENT OF RECORDS
The medical record shall contain sufficient information to
justify the diagnosis and warrant the
treatment and end results. The patient record shall describe the
patient's health status at the time of
admission, the services provided and the patient's progress in
the facility, and the patient's health
status at the time of discharge. The patient record shall
provide information for the review and
evaluation of the treatment provided to the patient. When
appropriate, data in the patient record
-
8/11/2019 Unit 25 Adminstration
29/31
shall be used in training, research, evaluation and quality
assurance programs. When indicated, the
patient record shall contain documentation that the rights of
the patient and of the patient's family
are protected. The patient record shall contain documentation of
the patient's and, as appropriate,
family members' involvement in the patient's treatment program.
When appropriate, a separate
record may need to be maintained on each family member involved
in the patient's treatmentprogram. The patient record shall contain
identifying data that is recorded on standardized forms.
This identifying data shall include the following:
1. Full name;
2. Home address;
3. Home telephone number;
4. Date of birth;
5. Sex
6. Race or ethnic origin;
7. Next of kin;
8. Education;
9. Marital status;
10. Type and place of employment;
11. Date of initial contact or admission to the facility;
12. Legal status, including relevant legal documents;
13. Other identifying data as indicated;
14. Date the information was gathered; and
15. Signature of the staff member gathering the information.
The patient record shall contain information on any unusual
occurrences such as the following:
1. Treatment complications;
2. Accidents or injuries to the patient;
3. Morbidity;
4. Death of a patient; and
5. Procedures that place the patient at risk or that cause
unusual pain.
-
8/11/2019 Unit 25 Adminstration
30/31
As necessary, the patient record shall contain documentation of
the consent of the patient,
appropriate family members or guardians for admission,
treatment, evaluation, aftercare or
research.
The patient record shall contain both physical and psychiatric
diagnoses that have been made
using a recognized diagnostic system.
The patient record shall contain reports of laboratory,
roentgenographic, or other diagnostic
procedures and reports of medical/surgical services when
performed.
The patient record shall contain correspondence concerning the
patient's treatment, and signed and
dated notations of telephone calls concerning the patient's
treatment.
A discharge summary shall be entered in the patient's record
within a reasonable period of time
(not to exceed 14 days) following discharge as determined by the
professional staff bylaws, rules
and regulations.
The patient record shall contain a plan for aftercare.
All entries in the patient record shall be signed and dated.
Symbols and abbreviations shall be used
only if they have been approved by the professional staff, and
only when there is an explanatory
legend. Symbols and abbreviations shall not be used in the
recording of diagnoses.
When a patient dies, a summation statement shall be entered in
the record in the form of a
discharge summary. The summation statement shall include the
circumstances leading to death
and shall be signed by a physician. An autopsy shall be
performed whenever possible. When an
autopsy is performed, a provisional anatomic diagnosis shall be
recorded in the patient's record
within 72 hours. The complete protocol shall be made part of the
record within three (3) months.
PROMPTNESS OF RECORD COMPLETION
Current records shall be completed promptly upon admission.
Records of patients discharged shall
be completed within 14 days following discharge. The staff
regulations of the facility shall provide
for the suspension or termination of staff privileges of
physicians who are persistently delinquent
in completing records.
IDENTIFICATION, FILING AND INDEXING
A system of identification and filing to ensure the prompt
location of a patient's medical record
shall be maintained.
The patient index cards shall bear at least the full name of the
patient, the address, the birth date
and the medical record number.
Records shall be indexed according to disease and physician, and
shall be kept up to date. For
indexing, any recognized system may be used.
Indexing shall be current within six (6) months following
discharge of the patient.
-
8/11/2019 Unit 25 Adminstration
31/31