Embed Size (px)
Citation preview

A guide for patients and their families
Understanding the Genetics of FTD

1
The authors wish to acknowledge
the following centers and
associations which contributed to
the creation of this booklet:
v The University ofPennsylvania Center for Neurodegenerative DiseaseResearch
v The University ofPennsylvaniaFrontotemporal Degeneration Center
v The Association forFrontotemporalDegeneration
This booklet was created by the University of PennsylvaniaCenter for NeurodegenerativeDisease Research.
© 2012 by the Trustees of the University of Pennsylvania. All rights reserved. No part of this publication may be reproduced without permission from theTrustees of the University of Pennsylvania.
Acknowledgements

2
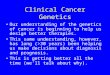
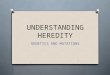
Frontotemporal degeneration (FTD) isone of the most common forms ofdementia in individuals under the ageof 65 years. Symptoms of FTD arecaused by the progressive loss of nervecells (neurons) in mainly the frontaland temporal regions of the brain,although other regions can beaffected in some cases. The frontallobes of the brain are involved in a number of functions, includingpersonality, behavior, planning,reasoning, judgment, impulse control,and motor functions. The temporallobes of the brain are involved inlanguage, memory, and speech.
Despite many years of research, it is still not known what triggers the process of neurodegeneration(neuron cell death) in the brains ofpeople who develop FTD. However,clues are gleaned from the presence ofparticular protein accumulationsinside the diseased neurons. In asubset of patients, the root cause ofthose protein accumulations can befound in the individual’s genetic code.
v Behavior: changes in personality, loss of empathy, apathy, inappropriate socialbehavior, and poor judgment
v Language: problems with expression of language or problems with word meaning
Symptoms
FTD is characterized by progressive decline in behavior and/or language with an averageage of onset in the mid-50s to 60s. The clinical presentations of FTD can include:
Frontotemporal

For any form of neurodegenerativedisease, the final and definite
diagnosis is made at the end of life bydoing a brain autopsy. The autopsy willexamine the location and severity ofbrain tissue loss (atrophy) as well asperform detailed microscopic exam -inations to detect the types of abnormalprotein accumulations in the brain. InFTD, an autopsy can usually distinguishbetween two main types of pathology.One group is characterized by clusters of tau protein. Tau plays an important rolein the structure and function of a healthyneuron, but in some forms of FTD, the tau protein begins to stick to itself and accumulates, eventually forminglarge clumps. These clumps are called
“inclusions.” The second group ischaracterized by inclusions of a proteinknown as TDP-43. TDP-43 is also a majordisease-associated protein found atautopsy in the brains of patients withamyotrophic lateral sclerosis (ALS). Asmall percentage of FTD is found to havea third protein, the FUS (fused in sarcoma)protein, as the characteristic finding atautopsy. In most patients with FTD, theautopsy findings will pinpoint one ofthese proteins as the primary finding, butsometimes, especially in older patients,there may be an accumulation of morethan one type of protein, includingproteins that are associated with other
neurodegenerative diseases,such as Alzheimer disease.Research is currently focused onunder standing why and howthese proteins accumulate, inhopes that the answer will leadto the development of FTD-specific therapies.
Frontal Lobe
Temporal Lobe
Parietal Lobe
Occipital Lobe
CerebellumEmotionsJudgment
Personality MemoryLanguage
Pathology
v Movement: decreased movement, muscle rigidity,parkinsonism (tremor, problems with gait andbalance), or motor neuron disease/ amyotrophiclateral sclerosis (Lou Gehrig’s disease)
v Executive: difficulty with planning, judgment andworking memory
TreatmentsSince the causes of FTD areunknown, there is no way toprevent it, slow down diseaseprogression, or cure it. However,physi cians may use medicationsand treatments used in similardisorders such as Alzheimer diseaseor psychiatric illnesses to helpmanage some of the symptoms.
3

4
Type of FTD
Behavioralvariant FTD(bvFTD)
Nonfluent oragrammaticprimaryprogressiveaphasia (PPA)
Semanticvariant PPA
Logopenicvariant PPA
Corticobasalsyndrome(CBS)
Progressivesupranuclearpalsy (PSP)
FTD withamyotrophiclateralsclerosis(FTD/ALS)
Pick’s disease
ClinicalDescription
Changes inpersonality,emotions, and/orbehaviors
Deterioration inthe ability toproduce speech
Deterioration inthe ability tounderstand wordsand recognizeobjects.
Deterioration inthe ability toretrieve words inspeech
Involuntarymovementsand/or cognitivedysfunction
Deterioration ofgait and balance;eye movementabnormality
Same changesseen in othersubtypes of FTDaccompanied bydeterioration ofthe motorneurons (alsosometimes calledFTD/MND)
A historic term forFTD, named forDr. Arnold Pick
Description of Possible Symptoms
3 Hyperoral (ex. eating only sweetsor a certain type of food)
3 Disinhibited actions (ex. makinginappropriate comments)
3 Apathy, lack of motivation to dothings
3 Lack of Insight (unaware of theimpact of symptoms on others)
3 Impaired decision-making
3 Hesitant, effortful speech3 Comprehension of the speech of
others may be preserved in earlystages
3 Typically lack features of bvFTD
3 Difficulty naming objects orrecognizing the meaning of theword that names an object
3 May have difficulty recognizingfamiliar objects and faces
3 Fluent speech usually preserved
3 Speech can be slow due todifficulty finding the right words
3 Able to understand word meaning
3 Apraxia or difficulty with use oftools
3 Executive or social deficits3 Cognitive problems such as
difficulty with simple mathcalculations and difficulty orientingobjects in space
3 Hallmark feature is inability tomove eyes up and down
3 May also have other features ofFTD subtypes
3 Any symptoms associated withbvFTD or PPA
Features of ALS can include:3 Muscle weakness & atrophy3 Muscle cramps3 Difficulty swallowing3 Slurred speech
3 Any symptoms associated withbvFTD or PPA (see above)
Type of PathologySeen in Brain
Associated with tauor AD pathology
Most frequently tauprotein pathologyfound
Most frequently TDP-43 protein pathologyfound
Most oftenassociated withAlzheimer disease(AD) pathology
Associated with tauor AD pathology
Tau protein
TDP-43 protein
“Pick bodies”consisting of tauprotein
TYPES OF FTD

Genetics plays an important role in
helping to better understand FTD.
Even before genetic causes of FTD
were first identified, doctors
recognized that in some families,
there was a history of multiple
family members all being affected
by a similar set of symptoms. These
families and their participation in
genetic research provided the first
insights into understanding the
hereditary forms of FTD. For the
majority of patients with FTD, there
is no family history of the disease
and genetics is of little concern.
However, for those individuals that
do have concerns about the role
that genetics plays in FTD, it is
important to understand not only
the specific genetic causes of FTD,
but also the basic science behind
why and how genes impact the risk
and causes of human disease.
FTD &Genetics
5

6
Our genetic material, DNA, is storedin every cell of our body. A DNA
chain is made up of individual units callednucleotides (an alphabet of 4 letters).DNA chains are then packaged into largerunits called chromosomes. Individualshave a total of 46 chromosomes.Chromosomes come in pairs, and in eachpair, one chromosome comes from thefather and the other from the mother. Thefirst 22 pairs of chromosomes are thesame in males and females (known asautosomes), whereas the 23rd pairdetermines our sex (males, XY andfemales, XX).
Genes are specific segments of DNA thatcarry the instructions for makingproteins. The instructions are made up ofa unique string of nucleotides that thecell knows how to read and translate into
proteins. Proteins are molecules made upof a chain of amino acid building blocks.Proteins are used by the body formaintaining its structure and function.Because our cells have two copies ofevery autosomal chromosome, thismeans we have two copies of each gene.There are many different genes presenton each chromosome. Both the sequenceof the DNA and the number of copies ofeach specific gene are important inmaintaining normal function of thehuman body.
A mutation is a change in the DNAsequence; in other words there is aspelling mistake or typo in theinstructions to make a protein. When amutation occurs in a gene, that copy ofthe gene has the wrong instructions tomake the protein and therefore it may
Genetics 101
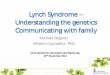
Cell
Nucleus
Chromosome
DNA Molecule
Gene
Protein
Our entire genetic code is stored in each cell of our bodies. The DNA is packaged in units called chromosomes. A gene is a speci�c section of DNA that containsinstructions for building a protein.

7
make a protein that does not functioncorrectly in the body or is not produced insufficient quantity. There are manydifferent types of gene mutations. Forexample, a mutation can occur becauseone or more nucleotides that encode(spell) the gene is either changed,inserted, or deleted. In some cases theinsertions and deletions can be large, eveninvolving the whole gene. In another type of mutation, a region of DNA that normally has a small number of a repeated sequence is abnormallyexpanded to have too many repeats,therefore affecting the function of nearbygenes.
The sequence of DNA in any individual isdetermined using a variety of methodscollectively called “molecular biology.” Notevery change identified in the DNA isautomatically considered to be a disease-causing mutation. Some identified DNA
changes are not harmful, they are justnormal variations in the genetic code.These normal variations are calledpolymorphisms and they are what makeeach of us look and behave differently.Sometimes a variation in the DNAsequence is identified that has never beenseen before so it can’t be classified asbeing harmful (mutation) or normal(polymorphism). There are tools and rules that researchers and doctors can useto evaluate these variations, but even so,sometimes a clear answer is not possible.In these cases the changes are “inde -terminate” and are often referred to asvariants of unknown significance (VOUS).When a test result is indeterminate, more work is needed to help determinewhether or not that change will have anegative effect. Studying additional familymembers can sometimes be helpful.
Mutations are Genetic Spelling MistakesWhen a gene is spelled correctly, the body is able to read the DNA letters in groups of three, similar to how we group letters to form words and sentences. If the gene is written correctly, the body can read the instructions.
Correct Gene CodeGene: ATC CAG AAT TACSentence: BUY THE RED CAR
A mutation changes the type or order of DNA letters. In the example below, one of the DNA letters changed from a C to an A. This changes the word, and thus the instructions change as well.
Incorrect Gene Code
Gene: ATC CAG AAT TAASentence: BUY THE RED CAT

Most cases of FTD are sporadic,meaning that there is no known
family history of FTD. In some cases thereis not enough information known aboutthe neurological health of the familymembers to rule out a possible geneticcomponent; this situation may bereferred to as a family history of unknownsignificance. While a very small per -centage of families that appear to be ofsporadic origin or those that have familyhistories of unknown significance may infact have a detectable genetic cause, thevast majority of gene mutations arefound in cases with a family history ofneurodegenerative disease.
Approximately 40% of individuals withFTD have a family history that includes atleast one other relative who also has orhad a neurodegenerative disease. Inapproximately 15-40% of all FTD cases, agenetic cause (e.g. a gene mutation) canbe identified as the likely cause of thedisease and in most cases it is aninherited mutation. The gene mutationrate can vary due to factors such as
ancestry, family history, and the type ofFTD (see table “Types of FTD.”) Clinically,both inherited and sporadic FTD exhibitthe same symptoms, which makesevaluation of the family history the mostsensitive tool for determining thelikelihood of a genetic cause.
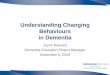
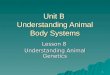
As seen in the pie chart image, familiesthat include a history of multiple relativeswith FTD and/or ALS are the most likelyto have an underlying genetic cause,while cases with sporadic or unknownfamily histories are the least likely. Thereare also families that fall in the middle,meaning that there is at least one relativewho has or had a related neuro -degenerative disease like Alzheimer orParkinson disease, but not a clear-cutfamily history of FTD or ALS in closerelatives. In short, the greater the familyhistory of FTD or an associated diseaselike ALS, the more likely genetics plays arole. It is important to note that not allindividuals with a family history ofneurodegenerative disease will have an identifiable gene mutation. This could
Genes & Family History
8
Sporadic or unknown
family historyNo mutation identified
Sporadic or unknown family history
Gene mutation
Strong family history of FTD and/or ALSGene mutation
Strong family historyof FTD and/or ALS
No mutation identified
Some family history of neurodegenerative
diseaseGene mutation
Some family history of neurodegenerative
disease No mutation
identified
Strong family history of FTD and/or ALS: Accounts for about 10-15% of FTD. The majority, but not all, have a mutation in a currently known FTD gene.
Some family history of neurodegenerative disease: Accounts for about 20-25% of FTD. Less than half have a mutation in a currently known FTD gene.
Sporadic or unknown family history: Accounts for about 60-70% of FTD. Only a small percent (less than 10%) have a mutation in a currently known FTD gene.
Legend

9
be because the respon -sible gene has not yetbeen identified, orbecause the disease isnot actually due to agene mutation. Thespecific genes that havebeen associated withFTD are discussed indetail in the nextsection.
There are many descrip tive words used inthe medical setting when discussingfamily history. These words are often usedinterchangeably, making it potentiallyconfusing to understand each term’smeaning and significance. For example,the term “hereditary” indicates that a traitor disease can be directly transmittedbetween parent and offspring. “Familial”is a very broad term used to indicate thatmore than one person in a family has atrait or disease. “Familial” denotes thatthere is a possibility of a genetic causedue to apparent clustering of affectedindividuals in a family. This may occur by chance or due to a genetic mutation(hereditary cause). When a geneticcounselor looks at a person’s familyhistory and draws a pedigree, they lookfor patterns of disease in the family anddepending on the number and type ofaffected individuals, a “pattern ofinheritance” is assigned.
A classic pattern of genetic inheritance iscalled autosomal dominant. “Autosomal”refers to the first 22 pairs of chromo -somes, which are identical in both malesand females. Therefore, both gendershave an equal chance of being affected ifa mutation is present on a gene in anautosomal chromosome. “Dominant”
inheritance means that only one copy ofa gene has to have a mutation to causedisease. Typically, the copy of the genewith the mutation is inherited from aparent, and most individuals with anautosomal dominant condition will havea family history of the disease. A child ofa person with a dominant mutation has a50% chance of inheriting the copy of thegene with the mutation and a 50%chance of inheriting the copy of the genewithout the mutation.
At this time, the only proven geneticcauses of FTD fall under the pattern ofautosomal dominant inheritance. It isbelieved that there are likely otherfactors, both genetic and environmental,that influence an individual’s risk ofdeveloping FTD. There may be genes orspecific mutations that do not directlycause FTD, but rather increase suscep -tibility to disease. This type of geneticfinding is referred to as a risk factor. It isalso likely that a combination of bothgenetic and environmental factorsinfluence the risk of disease; this is oftenreferred to as multifactorial inheritance.Research is underway to determine otherrisk factors that play a role in thedevelopment of FTD.
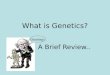
Autosomal Dominant Inheritance
ParentGeneration
OffspringGeneration
Did not inherit mutation
Did inherit mutation
Did inherit mutation
Did not inherit mutation
Gene Mutation No Mutation
Legend
This diagram shows all the possible inheritance combinations for a couple in which one parent has a gene mutation and the other parent does not. Each time the parent with the gene mutation has a child, there is a 50% chance of passing on the copy of the gene with the mutation, and a 50% chance of passing on the copy without a mutation. The chances are equal for males and females.

10
C9orf72 – Found onChromosome 9 • The genetic mutation on chromosome9 was discovered in 2011, after manyyears of research. The function of theprotein that C9orf72 codes for is not yetunderstood. Individuals with theC9orf72 mutation have abnormalaccumulations of the TDP-43 protein inaffected neurons.
• The C9orf72 mutation can cause FTD,ALS, or a combination of both FTD andALS. Research is ongoing to betterunderstand how this mutation can leadto two different types of clinicalsymptoms.
• The C9orf72mutation is believed to bethe most common genetic cause ofhereditary FTD, accounting for 5-20% ofall FTD cases. Most cases will have afamily history of either dementia orALS, but a small percentage of C9orf72cases may occur in apparently sporadiccases.
• The clinical features of patients withFTD due to C9orf72 mutations are stillbeing compiled, but initial reportsshow:o Average age of onset is in the 50’s
(range 30’s to 70’s)o Wide range of symptoms and
disease progression. Patients withbehavioral, language, and ofcourse, ALS symptoms have beenreported in cases of C9orf72mutations.
• The penetrance of C9orf72 is not yetfully understood, but it may have havereduced penetrance.
• The mutation is an expansion, orincrease in size of a small section ofDNA by increasing the number of
repeats. The section of DNA is referredto as a hexanucleotide repeat, whichmeans that 6 (hexa) units of DNA(nucleotides) are repeated to such anextent as to negatively impact thegene’s ability to create a functionalprotein.
Microtubule-Associated ProteinTau (MAPT) – Found onChromosome 17• MAPT, discovered in 1998, was the firstgene found to be associated withhereditary FTD. MAPT codes for theprotein tau and individuals with MAPTmutations have abnormal accumu -lations of the tau protein in affectedneurons.
• Mutations in MAPT account for 5-10%of all FTD cases. People who have FTDdue to MAPTwill typically have a familyhistory of other relatives affected by thedisease; however, family history may beunknown because of lost familymembers, early death, or adoption.
Genes Associated with Hereditary FTD
All of the genes described in this section can cause hereditary FTD and follow theautosomal dominant pattern of inheritance (see page 9).

11
• Mutations in MAPT are associated witha wide range of FTD subtypes includingbvFTD, semantic variant PPA, PSP, andCBS. The most common subtypeassociated with MAPT mutations isbvFTD.
• Average age of onset is 52 years (range:40-60).
• Wide range of symptoms, diseaseprogression, and age of onset bothbetween families and within the samefamily.
• Most cases reported have completepenetrance.
• Mutations in the MAPT gene areassociated with the clinical diagnosis ofFTDP-17, which stands for FTD withparkinsonism on chromosome 17. Thename arose because some, but not all,patients with MAPT mutations alsodeveloped movement symptoms, suchas tremors or balance problems.
Progranulin (GRN) – Found onChromosome 17• GRNwas discovered in 2006 and codesfor the protein progranulin. Individualswith GRN mutations have abnormalaccumulations of the TDP-43 protein inaffected neurons.
• Mutations in GRN account for 5-10% ofall FTD cases. People who have FTD dueto GRN will typically have a familyhistory of other relatives affected by thedisease; however, family history may beunknown because of lost familymembers, early death, or adoption.
• GRN mutations are associated with awide range of FTD subtypes includingbvFTD, nonfluent variant PPA, and CBS.Similar to MAPTmutations, bvFTD is themost common subtype associated withGRNmutations.
• Average age of onset is 59 years (range:35-87 years).
• There can be a wide range ofsymptoms, disease progression, andage of onset both between families andwithin the same family.
• Reduced or age-dependent pene -trance has been reported.
Valosin-Containing Protein (VCP)• VCP mutations are associated with aspecific condition called inclusion bodymyopathy with Paget disease of thebone and FTD (IBMPFD). Inclusion bodymyopathy (IBM) is characterized byslowly progressive muscle weaknessbeginning in the teens to earlyadulthood. Paget disease of the bone ischaracterized by enlarged and mis -shapen bones.
• VCPmutations account for a very smallpercentage of FTD cases, but only infamilies with the specific constellationof symptoms as described above.
• There is a wide range of symptoms,disease progression, and age of onsetboth between families and amongfamilies with a VCP mutation. Affectedindividuals may develop FTD, IBM,Paget disease of the bone or anycombination of the three conditions.
Other genes associated with rare FTD cases:
Charged multivesicular body protein 2B(CHMP2B)
• Extremely rare cause of FTD, onlyfound in a few families world-wide
TAR DNA-binding protein (TARDBP)• Mutations in TARDBP are very rare.These mutations are more commonlyassociated with hereditary ALS thanFTD.
Fused in sarcoma (FUS)• Mutations in FUS are very rare. Thesemutations are more commonlyassociated with hereditary ALS thanFTD.

12
Genetic testing for FTD is performedby analyzing a DNA sample for
changes in the genes known to causeFTD. This process is similar to the conceptof spell-checking a document to makesure everything is correct. The DNAsample is typically obtained from blood,but sometimes other sample types, suchas saliva or tissue from an autopsy can beused as the source. These sample typesmay be used if blood cannot be obtained,and autopsy tissue can be useful fortesting a deceased affected familymember.
Clinical genetic testing isavailable for all of the genesassociated with hereditary FTD,as well as many of the genesassociated with rare FTD cases.To obtain a clinical genetic test,a doctor orders the test from aclinical laboratory that islicensed and certified to pro -vide clinical genetic testingservices. Testing of the sampleby a clinical lab is usually donein 1-2 weeks, although in somecases it may take up to 1-2
months to complete. Someinsurance companies cover the costs, but policies varyregarding coverage and reim -burse ment for genetic testingservices. Costs of clinical genetictesting can vary from a fewhundred dollars to over athousand dollars. The results ofthe clinical test would bereported back to the individual,as well as the doctor whoordered the test, so that theresults can be recorded in thepatient’s medical record.
Many FTD research centers conductgenetic research studies in which indi -viduals can participate; however, policiesvary regarding whether or not resultsfrom research tests would be returned tothe individual. When participating in agenetic research study, it can be helpfulto ask whether or not results are evershared with participants. If results areshared with participants, ask when andhow results might be communicated;often research testing takes much longerto conduct than clinical testing.
The difference between clinical & research testingTesting
Testing
Scientific knowledgeand discovery of
treatments
Results givento researcher
Cost to the researcher
Kept in researcher’s records
CLINICAL
RESEARCHDiagnosis or risk
information
Results givento patient
Cost to the patient
Kept in patient’s medical record
Genetic Testing

(cont’d. on page 14)
If an individual definitely want the resultsof the genetic testing, it would beadvisable to first look into clinical genetictesting, as this provides a guarantee ofreceiving results.
Family history provides the biggest clueas to whether genetic testing mightdetect a disease-causing mutation.Typically, the stronger the history ofdementia and/or movement disorders inother family members, the greater the
possibility that there is a gene mutationresponsible. Not every individual with afamily history of disease will have adetectable mutation, but it does providesome insight regarding the possibility.There is a much lower likelihood offinding an FTD gene mutation in asporadic family pedigree; however,sometimes mutations are found inpatients that do not have a family historysuggestive of hereditary disease. There
Penetrance is an important concept toreview in order to better understand thegenetics of FTD. It is a term used to referto the likelihood that a mutation in aparticular gene will result in a disease.Complete penetrance occurs when everyindividual with a particular gene muta -tion develops symptoms of the disease.
Reduced penetrance occurs when someindividuals with a particular gene muta -tion do not develop symptoms of thedisease. Sometimes the term “age-dependent penetrance” is used in FTD.This means that, for an individual with a gene mutation, the likelihood ofsymptom onset increases with age.
The Concept of Penetrance
Penetrance refers to the proportion of individuals with a mutation in a particular gene who will actually develop symptoms of the disease.
Complete penetrance occurswhen every individual with a
gene mutation develops symptoms of the disease
Reduced penetrance occurs when some individuals with a
gene mutation develop symptoms of the disease
while others do not
Gene mutation but no symptomsGene mutation & symptoms
13

14
are a few reasons why this may occur.Other relatives that had the mutationmay have died of an unrelated causeprior to ever developing symptoms ofFTD. Sometimes patients are not aware ofmedical information on more distantrelatives that might have been affectedand an assumption is made that no oneelse was affected. In many families, it canbe difficult to get accurate medicalinformation on aunts, uncles, and grand -parents. Sometimes, it is not possible toget any family medical informationbecause the affected indi vidual wasadopted or unsure of the identity of hisor her biological father. This is why somepedigrees are classified as “unknownsignificance” for genetic risk assessment.Importantly, this does not mean a FTDgene mutation won’t be found, just thatwe don’t have enough information toassess and quantify the risk.
Any patient with FTD has the option topursue genetic testing for the known FTDgenes, although a genetic cause is morelikely in those individuals who also havea family history of FTD or other neuro -degenerative diseases. For specificquestions about genetic testing for FTD,it would be best to speak with a clinicianfamiliar with genetic testing, such as amedical geneticist or genetic counselor.
Genetic Testing for Individuals with FTDIf a mutation is found in a geneassociated with FTD, the patient’sdiagnosis would be confirmed. In somecases, it may provide insight into theprogression of the disease, or even the
risk of developing other symptoms, suchas symptoms of ALS in C9orf72mutations. The detection of a mutationwould also determine the risk to otherfamily members for inheriting the samegene mutation. At the time of thispublication, there is not a specificmedication or treatment that would begiven to a patient based on the results ofa genetic test; however, the results mayprevent the patient from gettingadditional, unnecessary testing orprevent treating the patient for thewrong diagnosis. As the field of FTDresearch advances, patients with genemutations might be candidates for newtreatment options or clinical trials for thespecific FTD subtype identified.
Genetic Testing for FamilyMembers of Individuals withFTDOnce a disease-causing gene mutationhas been found in an individual affectedby FTD, this information can be used toprovide genetic testing services to otherindividuals in the family. Affected familymembers can be tested specifically forthe known mutation to confirm itspresence.
Unaffected family members who are at-risk of inheriting the mutation canchoose to have presymptomatic genetictesting. Presymptomatic genetic testingrefers to the idea of testing a currentlyunaffected person to determine whetheror not they have inherited a known genemutation that has been found in theirfamily. This is also sometimes calledpredictive genetic testing. At this time,
Genetic Testing (continued)

15
there are no preventative optionsavailable for FTD and therefore thedecision to pursue presymptomaticgenetic testing is entirely personal innature and can be a difficult decision tomake.
The purpose of the presymptomaticgenetic testing process is to provide astructured, thorough, and supportiveapproach to the personal decision tolearn one’s genetic status. In order toaccomplish this goal, presymptomaticgenetic testing typically involves severalvisits. A genetic counseling session isconducted to discuss the testing decisionin detail. Prior to learning one’spresymptomatic testing result, it isimportant to consider the decision from
every possible angle, such as exploringthe potential impact of the results andthe risks and benefits of testing for theperson being tested, their relatives, andtheir significant others. It is alsoimportant to explore the motivations orreasons for learning the test result, as wellas the limitations of knowing this type ofgenetic information. Some clinics mayadvise that the individual have aneurology exam and/or a mental healthevaluation as part of the genetic testingprocess.
The blood for the genetic test is drawn ata subsequent visit, allowing for a windowof time during which the individual canreflect and feel absolutely sure of his orher decision to learn their genetic result.
Any patient with FTD
has the option to pursue
genetic testing for the
known FTD genes,
although a genetic
cause is more likely
in those individuals
who also have a family
history of FTD or other
neurodegenerative
diseases.
(cont’d. on page 16)

The results are then disclosed during anin-person visit; not by mail or over thetelephone. Most centers require thepresence of a support person at this post-test visit. If the individual has notinherited the mutation, he or she is not atrisk for the hereditary FTD that hasaffected other family members. Theindividual would have the same risk forneurodegenerative diseases (includingFTD) as the general population. If theindividual has inherited the mutation, heor she is at definite risk for developingFTD at some point in her life. It is nearlyimpossible to predict the exact age ofonset or the type of symptoms to expect,but in some cases, the specific gene orgene mutation may provide someadditional insight into the risk.
Genetic Testing for FamilyPlanning ReasonsThe topic of family planning is immenselypersonal. For individuals with either a riskof inheriting an FTD gene mutation orindividuals known to have a mutation,there may be difficult feelings andquestions to face regarding starting afamily of their own. Often individuals are concerned about the risk of passingthe mutation on to their own children,the next generation of the family. Thereare reproductive technologies, such aspreimplantation genetic diagnosis (PGD),that have been developed to address thisconcern. In PGD, the process of in vitrofertilization (IVF) is used to developembryos. These embryos are then testedfor the known family mutation, and only
embryos that did not inheritthe mutation are used forimplantation. PGD is only oneexample of available repro -ductive options. Other familyplanning options includegamete (egg or sperm)donation, adoption, naturalconception, or the decisionnot to have children. There areclinicians, including physiciansand genetic counselors, whospecialize in providing pre -conception and prenatalgenetic services. For indi -viduals that desire moreinformation and supportregarding family planning, it isadvisable to schedule aconsultation with such aprofessional.
16
Genetic Testing (continued)

17
(cont’d. on page 18)
FAQs for FTD Genetic Testing
Q: Is there a genetic test for FTD?
A: Yes, clinical genetic testing is available to look formutations in MAPT, GRN, VCP, TARDBP, C9orf72 andFUS. A doctor or genetic counselor would be able toprovide more details about the specific genetic testingoptions that are most appropriate based on anindividual’s symptoms and family history.
Q: How is the genetic test done?
A: Blood or saliva is collected and used to isolate asample of DNA. This DNA sample can then beanalyzed for mutations in the specific genes of interest.For individuals with an unknown genetic cause, a com -plete analysis for any known disease-causing geneticchanges would need to be performed. However, for indi -vi duals that already know the specific gene muta tionthat is present in their family, the genetic test can betargeted to just check for that known family mutation.
Q: Who can get genetic testing?
A: Any individual with FTD who is interested ingenetic testing may get tested, although a genetic causeis more likely in those individuals who also have afamily history of FTD. Anyone considering genetictesting or who has a family history of FTD should seekgenetic counseling prior to genetic testing. The test ismost beneficial when a family member with FTD is thefirst person tested. Once a mutation has been identified,other members of the family may choose to be tested forthe same mutation even if they don’t have symptomsof the disease (presymptomatic genetic testing).
The following
is a guide to
some of the
most
frequently
asked
questions
about genetic
testing for
FTD.
If you have
questions that
are not
addressed,
please contact
a genetic
counselor or
other clinician
familiar with
genetic
testing.
Q&A• • •

Q&A
18
Q: What is genetic counseling?
A: The goal of genetic counseling is to helppeople understand more about the geneticcauses of a disease and how it may affectthem so they may make informeddecisions. Genetic counselors can explainhow genetic conditions are inherited,determine if an individual is at risk,provide options and guidance for genetictesting, and find referrals for otherresources.
Q: If I already have FTD, whatwould a genetic test tell me?
A: Genetic testing may help define the riskof FTD for other family members. Thereare three possible types of genetic testresults: positive, negative, and inde -terminate.
Positive: A positive test result wouldmean that the individual has a disease-causing mutation. A positive test resultindicates that the cause of FTD observed inthe family has been found. This wouldfurther define the risk for other familymembers to develop FTD and allow themto pursue presymptomatic genetic testing ifinterested.
Negative: A negative test result wouldmean that the individual did not have amutation in the tested gene or genes.However, a negative result would not ruleout the possibility of a genetic causeentirely for the following reasons:
• Not all genes may have been tested. Forexample, some tests may look at only onespecific gene, whereas others may testmultiple genes.
• Genetic testing methods may vary. Forexample, some tests only look for specificmutations, whereas others look for anyand all mutations in the gene.
• Not all genetic causes are known.Scientists are still working to find othergenes that contribute to FTD.
Indeterminate: An indeterminate resultmeans that a change was found in thegenetic sequence of the gene, but thelaboratory cannot yet make a cleardetermination as to whether it is a disease-causing mutation, a risk factor, or anormal polymorphism. Normal poly -morphisms are common variations in DNA that do not cause disease. Anindeterminate result is sometimes called avariant of unknown significance.
The interpretation of genetic test results canbe confusing. It is recommended thatanyone who has genetic testing for FTDdiscuss the results with a genetic counseloror another medical genetics professional.
Q: If I have a family history of FTD,should I be tested even if I do nothave symptoms?
A: Testing a person who is currently notshowing symptoms but who is at risk forinheriting a known family mutation iscalled presymptomatic (or predictive)testing. For presymptomatic testing, amutation must have been first identified inthe family so that the clinician knows theappropriate test to order and can properlyinterpret the results. Individuals in thesame family may have differing opinionson whether or not to pursue pre symp -

tomatic testing. The pursuit of pre -symptomatic testing is a very personaldecision that may be confusing andemotionally difficult. Therefore, geneticcounseling and psychological evaluationare usually required to help the individualthroughout the testing process.
Q: What is the difference betweenclinical and research genetic testing?
A: The purpose of clinical genetic testingis primarily for diagnosis or prediction ofdisease. The testing is performed in anaccredited laboratory. A report of theresults is generated and will be part of thepatient’s official medical record. There is acharge for clinical testing, which may ormay not be covered by insurance. Clinicalgenetic testing does not help scientistsdiscover a cure or new treatments for FTDand the results do not affect medicalmanagement at this time (because thereare no approved treatments) .
The purpose of research genetic testing isto discover and to better understand thegenetic factors of FTD and how theseimpact the clinical presentation andpathology. In research, patient identifiersand information remain confidential andresults do not become part of the patient’sofficial medical record. There is no feewhen participating in a research study,and generally results are not returned toparticipants. Many individuals choose toparticipate in research genetic testing tohelp advance the FTD field for the benefitof future generations. Research genetictesting may lead to a better understandingof the causes of FTD and the developmentof better treatments or a cure in the future.
Research testing may also identify or testfor new disease-associated genes beforethey are available as a clinical test.
Q: What are the risks that my childwill also get FTD?
A: If an individual has a mutation in oneof the known FTD associated genes, thereis a 50% chance of passing on themutation and a 50% chance of NOTpassing on the mutation to his/her child.This same 50/50 risk applies to every childof that individual. If the child does inheritthe mutation, he or she will most likelydevelop symptoms of the disease at somepoint in adulthood, but the age of onset,severity, and type of symptoms cannot bepredicted at this time.
19
(cont’d. on page 20)

Q&A
20
If an individual with FTD does not have amutation in a known FTD gene and doesnot have a family history suggestive of ahereditary cause, the risk to children ismuch lower and is likely close to thegeneral population risk, which is low. If anindividual with FTD does not have amutation, but does have a family historysuggestive of a hereditary cause, it wouldbe important for that family to getinvolved with an FTD genetic researchstudy to try to determine whether a geneticcause or risk factor can be identified. Thisinformation would be crucial for providingaccurate information to individualspossibly at-risk. As with any humandisease, there may be environmental orgenetic risk factors that could increasesusceptibility to a disease. At this time,there are no known risk factors that couldindicate a susceptibility to FTD, butongoing research is working to betterunderstand risk factors for FTD.
Q: Is there protection from geneticdiscrimination?
A: The Genetic Information Nondis -crimination Act (GINA) was signed intofederal law in 2008. GINA provides legalprotections against genetic dis criminationin health insurance coverage and mattersrelated to employment. GINA does notprovide protections for life insurance, long-term care insurance, or disabilityinsurance. Individuals who are consideringgenetic testing to determine if they are atrisk for FTD are encouraged to learn moreabout the protections GINA does and doesnot provide, as well as any relevant statelaws. (A guide to GINA is provided in“Helpful Links and Resources”.)
Q: If I have a genetic mutation,what can be done about it?
A: At this time, we cannot change or alteran individual’s genetic make-up. There areresearch studies looking into newtechnologies for treating genetic diseases,but this is currently not available as amedical treatment for FTD. Identifying agene that causes FTD in an affectedindividual will not provide an answer forcuring the disease, but may help preventthe patient from being treated for thewrong diagnosis. Additionally, if anunaffected person finds out that theyinherited a FTD gene mutation, there is notreatment available at this time to preventthe onset of disease.
Q: What causes a gene mutation?
A: In FTD, most identified mutations arebelieved to have been inherited, passedfrom parent to child throughout manygenerations. There is likely an ancientancestor who was the first person to havethe mutation. In the genetics profession,this ancient ancestor is referred to as the“founder.” It can be very difficult todetermine why the mutation ever occurredin the first place. Sometimes, there is aregion of DNA that is less stable and proneto mistakes (i.e. mutations) being made.Our bodies have a way to detect and correctthese mistakes, but sometimes not everymistake is corrected. Gene mutations due toenvironmental exposures can occur, but aretypically restricted to the exposed personand it is unlikely that the mutation couldbe passed to the next generation. Genemutations due to environmental factorshave not been reported to cause FTD.

Q: If I did not inherit the FTD genemutation that has been found in myfamily, could it still appear in myown children?
A: If an individual has been tested for amutation that is known to affect theirfamily, and they do not have it, they arenot at risk themselves for the geneticdisease and cannot pass it to their ownchildren. Sometimes people refer to theidea of a disease “skipping a generation;”this is a common genetic myth. A trulygenetic disease cannot skip through afamily, as the only way to get the diseaseis the direct inheritance of a disease-causing mutation from parent to child.There are several reasons a genetic diseasemay appear to skip a generation, eventhough the mutation itself does not skip ageneration. For example, sometimes anindividual may pass away from anunrelated cause before ever developingsymptoms of the disease. Also, somemutations do not always result in diseasebecause of reduced penetrance (see page13). In both of these scenarios, the personcarrying the mutation can still pass it onto the next generation.
Q: Everyone has always said that Ilook and act just like my mom, whohas been diagnosed with FTD. Doesthis mean I’m more likely to also getFTD?
A: Having a resemblance to a parent withFTD does not increase the risk of alsodeveloping FTD. It can be very easy toassume that if we strongly resemble one ofour parents, we are destined to share manyof their same fates. From a purelybiological standpoint, humans are a 50/50combination of both parents’ genes, evenif a person cannot see that combination bylooking in a mirror. When it comes toFTD, the only known genetic causes areinherited in an autosomal dominantmanner. In this type of inheritance, thereis a 50% chance of inheriting the copy ofthe gene with the mutation, and a 50%chance of inheriting the copy of the genewithout a mutation. There is also no sexeffect, in that sons are not more likely toinherit the disease from their father, norare daughters more likely to inherit thedisease from their mother.
21

22
Glossary of FTD and Genetic Terminology
Allele – Another word for gene. Sometimes used when referring to different versions ofa gene.
Amino acids - Small chemical units that link together to form a protein.
Autosomal dominant – A type of inheritance in which only one copy of a gene pairneeds to have a mutation in order for the trait or disease to present.
Behavioral variant FTD (bvFTD) – The clinical term for an individual with behavioral andpersonality changes as the primary symptoms.
C9orf72 – A gene of unknown function with a specific type of mutation, called ahexanucleotide repeat (a large repeat of a section of genetic material) that was recentlydiscovered on chromosome 9. This mutation can cause hereditary FTD and/or ALS.
CHMP2B – A very rare cause of genetic FTD, this gene makes the charged multivesicularbody protein 2b.
Chromosome – A unit of tightly wound and packaged DNA. Each chromosome hasthousands of genes.
Corticobasal syndrome (CBS) – An FTD-related diagnosis that typically first presentswith motor symptoms, similar to Parkinson disease. The term corticobasal degeneration(CBD) is also used, but usually is reserved for the final autopsy diagnosis of this condition.
DNA – Deoxyribonucleic acid. DNA is a long, double-stranded structure of geneticmaterial.
Frontotemporal degeneration (FTD) or Frontotemporal lobar degeneration (FTLD)– These 2 terms are used interchangeably to refer to a spectrum of disorders that causeprogressive changes in personality, behavior, and/or language.
FUS – The FUS gene makes the fused in sarcoma protein, which is believed to helpsupport normal DNA functions. Mutations in this gene are a rare cause of genetic FTD.
Gene – A unit of DNA that carries the instructions to make a specific protein.
Genetic testing – The process of using laboratory techniques to analyze genetic material(DNA).
GRN – see Progranulin
Microtubule-Associated Protein Tau (MAPT) -The official name of the gene that makesthe tau protein.
Motor neuron disease – Also known as amyotrophic lateral sclerosis (ALS) or Lou Gehrig’sdisease. A progressive loss of the neurons that control muscle movement. 10-15% ofpatients with FTD may also develop symptoms of ALS, and the two disorders have beenclosely linked based on results of recent research advances.
Mutation – A change in DNA that affects a gene’s ability to make a protein. May result indisease.

23
Nucleotide – An individual chemical unit; nucleotides are the letters that make up thespelling of DNA. In DNA, the nucleotides are A, T, G, and C.
Parkinsonism – A term used to describe motor symptoms that are similar to those seenin Parkinson’s disease, such as tremors, stiffness, and walking/balance difficulties.
Penetrance – The likelihood that a genetic mutation will result in disease.
Pick’s disease – An old diagnostic term for FTD, named for the physician that firstdescribed the condition. It is also used as a pathological diagnosis for some types of FTD.
Polymorphism – A normal variation in the DNA code. In contrast to disease genemutations, polymorphisms do not directly cause disease.
Primary progressive aphasia (PPA) – The clinical term for an individual with languagedifficulties as the primary symptom. There are several different types of PPA, includingsemantic, non-fluent/agrammatic, and logopenic.
Progranulin – The progranulin gene (GRN) makes the progranulin protein, whichfunctions in cell growth and repair. Mutations in GRN cause hereditary FTD.
Progressive supranuclear palsy (PSP) – A rare diagnosis related to both FTD andParkinson disease that causes both cognitive and movement difficulties, including acharacteristic difficulty with eye movements.
Protein – A molecule that serves a specific function in the body. Proteins are made up ofindividual units called amino acids.
Sequencing – A genetic testing method in which the letters of the genetic code are readnucleotide by nucleotide and then compared to the normal sequence in humans to lookfor differences or misspellings.
TARDBP – The tar DNA-binding protein, also known as TDP-43, is made by the TARDBPgene. Mutations in this gene can cause genetic FTD.
Tau –This protein is found in about half of FTD cases at autopsy. While not all FTD caseswith tau protein are genetic, there are some cases of FTD that are caused by mutationsin the gene that makes the tau protein (MAPT).
TDP-43 – This protein is found in about half of FTD cases and almost all cases of ALS. Thefunction of TDP-43 in the brain and it’s relation to neurodegeneration is not fullyunderstood.
Variant of unknown significance (VOUS) - a change in DNA that has an unknownclinical impact.
VCP – The valosin-containing protein is made by the VCP gene. Mutations in this genecause a specific condition called inclusion body myopathy with Paget disease of the boneand FTD (IBMPFD).

24
Websites
The Association for FrontotemporalDegenerationwww.theaftd.org
University of Pennsylvania Center forNeurodegenerative Disease Researchwww.med.upenn.edu/cndr
National Society of Genetic Counselorswww.nsgc.org
The Coalition for Genetic Fairness: A Guide to the Genetic InformationNondiscrimination Actwww.geneticfairness.org/ginaresource.html
Genetics Home Reference http://ghr.nlm.nih.gov/
National Institute on Aging: FrontotemporalDisorders, Information for Patients, Familiesand Caregiverswww.nia.nih.gov/alzheimers/publication/frontotemporal-disorders-information-patients-families-and-caregivers
Books
What if it’s not Alzheimer’s? A Caregiver’s Guide to Dementia (2008),edited by Lisa Radin & Gary Radin
Helpful Links& Resources