Embed Size (px)
Citation preview
BLOCK 1 REVIEWBLOCK 1 REVIEWPART 1PART 1

UPPER LIMBUPPER LIMB
22
33
The websites for practice The websites for practice questions.questions.
http://www.med.umich.edu/lrc/http://www.med.umich.edu/lrc/coursepages/M1/anatomy/html/coursepages/M1/anatomy/html/courseinfo/mich_quiz_index.htmlcourseinfo/mich_quiz_index.html
****
44
anterior rami of C5-T1 spinal nerves
Prefixedor Postfixed)
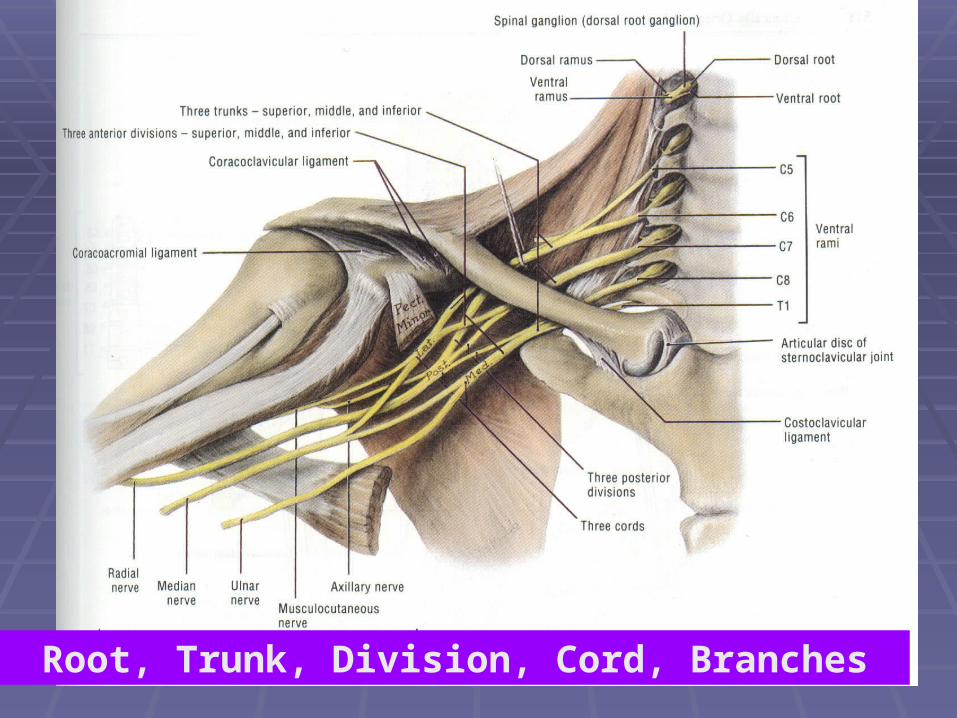
55Root, Trunk, Division, Cord, Branches
66
Branches from Root & TrunkBranches from Root & Trunk
Dorsal Scapular Dorsal Scapular [C5][C5]
Long Thoracic Long Thoracic [C5, C6, C7][C5, C6, C7]
Nerve to scalanae musclesNerve to scalanae muscles Accessory Phrenic [C5]Accessory Phrenic [C5]
Nerve to subclaviousNerve to subclavious Supra scapular Supra scapular [C5, C6][C5, C6]
For final exam
77
Branches from lateral cordBranches from lateral cord
Lateral PectoralLateral Pectoral Lateral root of median Lateral root of median [C6,C7][C6,C7]
Musculo Cutaneous Musculo Cutaneous [C5,C6,C7][C5,C6,C7]
88
Branches from medial cordBranches from medial cord
Medial PectoralMedial Pectoral Medial root of median Medial root of median [C8,T1][C8,T1]
Medial Cutaneous nerves of arm and Medial Cutaneous nerves of arm and forearmforearm
Ulnar Ulnar [C8,T1][C8,T1]
99
Branches from Posterior cordBranches from Posterior cord
Axillary Axillary [C5,C6][C5,C6]
Upper and Lower SubscapularUpper and Lower Subscapular Thoraco DorsalThoraco Dorsal Radial Radial [C5-T1][C5-T1]
1010
Multisegmental nerves Vs. Multisegmental nerves Vs. DermatomesDermatomes
It is interesting to look at the sensory It is interesting to look at the sensory supply to skin in a different way- on basis supply to skin in a different way- on basis of DERMATOMES.of DERMATOMES.
Dermatomes are area of skin supplied by Dermatomes are area of skin supplied by single spinal nerves.single spinal nerves.
Study of dermatomes is useful clinically for Study of dermatomes is useful clinically for dertermination of site of lesion of spinal dertermination of site of lesion of spinal cords.cords.
1111
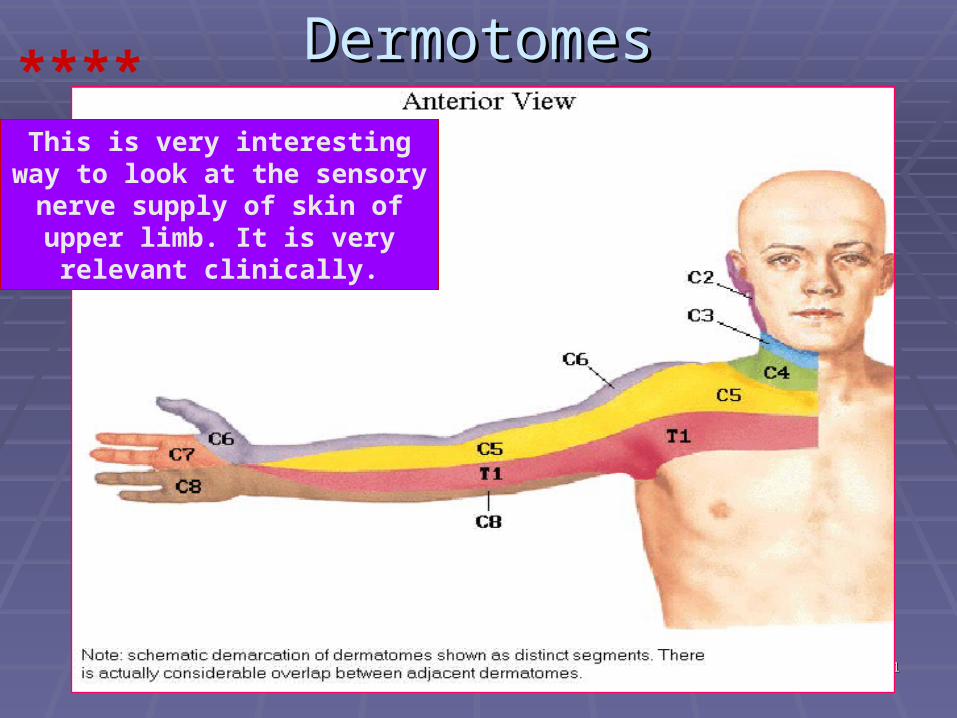
DermotomesDermotomes****This is very interesting way to
look at the sensory nerve supply of skin of upper limb. It is very
relevant clinically.
1212
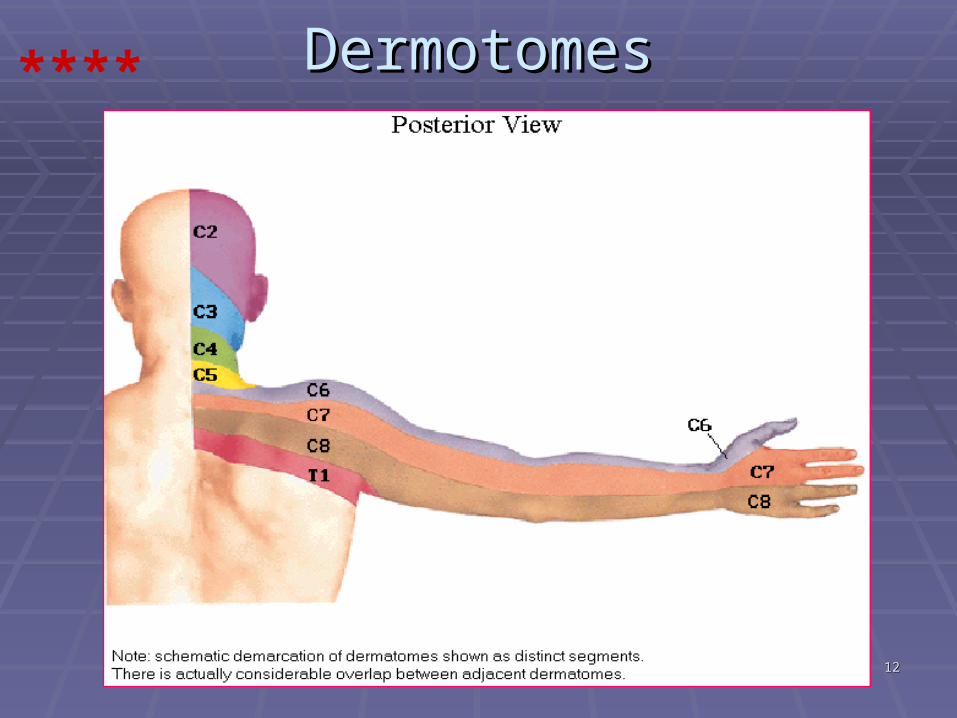
DermotomesDermotomes****
1313
Cutaneous InnervationCutaneous Innervation
1515
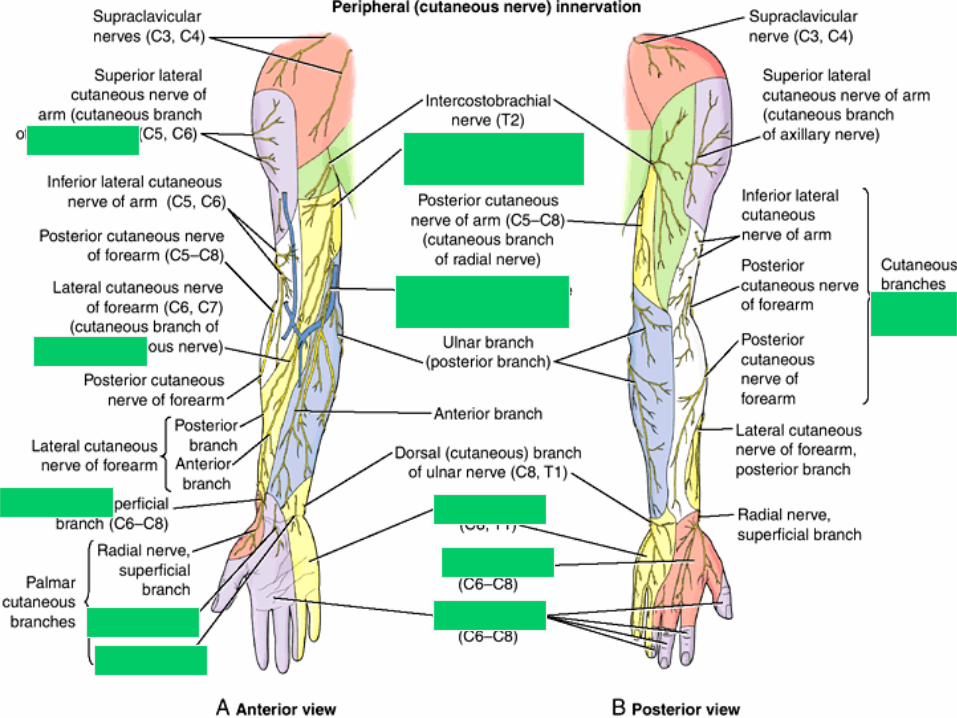
You should focus on approximate skin You should focus on approximate skin territories supplied by following nervesterritories supplied by following nerves
Axillary Axillary [upper lateral shoulder][upper lateral shoulder] Radial Radial [posterior and lower lateral arm; posterior [posterior and lower lateral arm; posterior
forearm and lateral 2/3 of posterior hand + forearm and lateral 2/3 of posterior hand + lateral 3&1/2 fingers posterior surface except lateral 3&1/2 fingers posterior surface except near tip]near tip]
Medial CutaneousMedial Cutaneous of arm and forearm of arm and forearm MusculocutaneousMusculocutaneous [lateral patch forearm] [lateral patch forearm] MedianMedian [lateral 2/3 of anterior surface of palm [lateral 2/3 of anterior surface of palm
and lateral 3&1/2 fingers-Ant surface + tips on and lateral 3&1/2 fingers-Ant surface + tips on dorsal aspect]dorsal aspect]
UlnarUlnar [Medial 1/3 of anterior surface of palm + [Medial 1/3 of anterior surface of palm + posterior hand; and medial 1&1/2 fingers posterior hand; and medial 1&1/2 fingers anterior+posterior surfacesanterior+posterior surfaces
1616
Important Muscles for ActionsImportant Muscles for Actions Serratus AntereriorSerratus Antererior Pec MajorPec Major Lat DorsiLat Dorsi Supraspinatus , Infraspinatus & SubscapularisSupraspinatus , Infraspinatus & Subscapularis Trap., Rhomboids & Levator scapulaeTrap., Rhomboids & Levator scapulae DeltoidDeltoid Biceps & TricepsBiceps & Triceps Brachioradialis, Brachialis, CoracobrachialisBrachioradialis, Brachialis, Coracobrachialis FCR, FCU, ECRL, ECRB, ECU, FDS, FDPFCR, FCU, ECRL, ECRB, ECU, FDS, FDP Supinator, Pronator teres & quadratusSupinator, Pronator teres & quadratus Lumbricals & InterosseiLumbricals & Interossei 1717
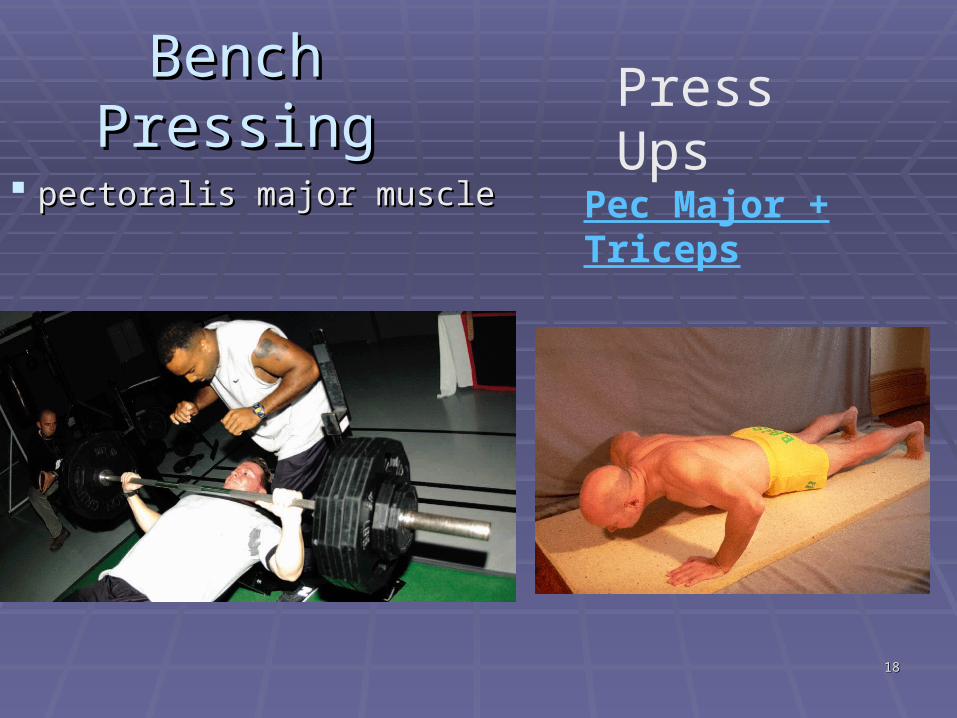
Bench Bench PressingPressing
pectoralis major musclepectoralis major muscle
1818
Press Ups
Pec Major + Triceps
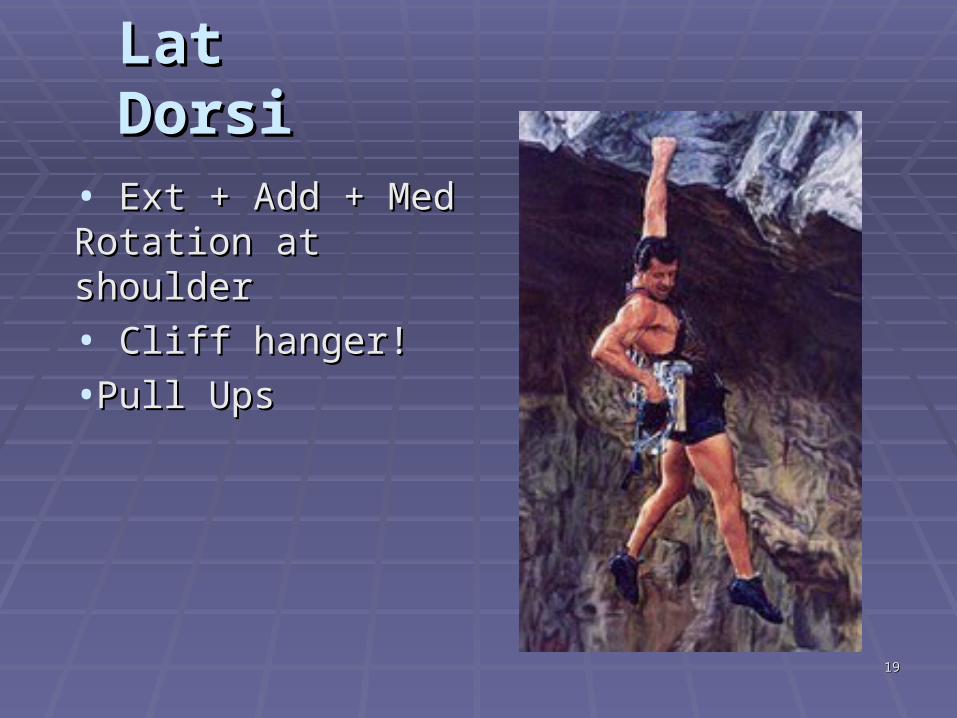
Lat DorsiLat Dorsi• Ext + Add + Med Ext + Add + Med Rotation at shoulderRotation at shoulder• Cliff hanger!Cliff hanger!•Pull UpsPull Ups
1919
2020
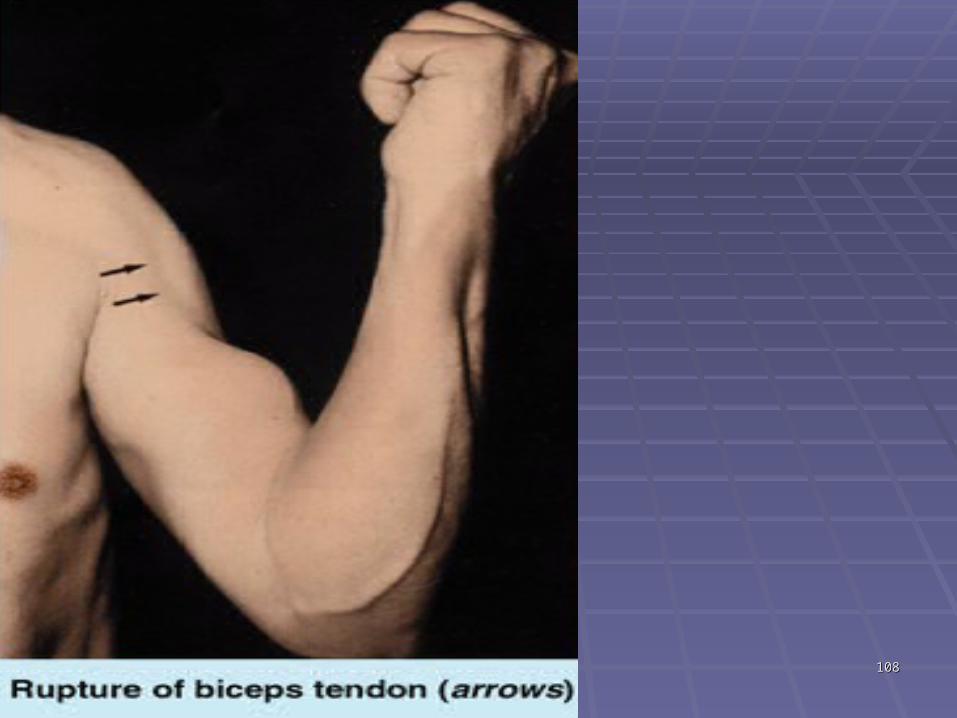
Tendon reflexes:
1-Biceps brachii tendon reflex: C5,6(flexion of the elbow joint by tapping the biceps tendon)
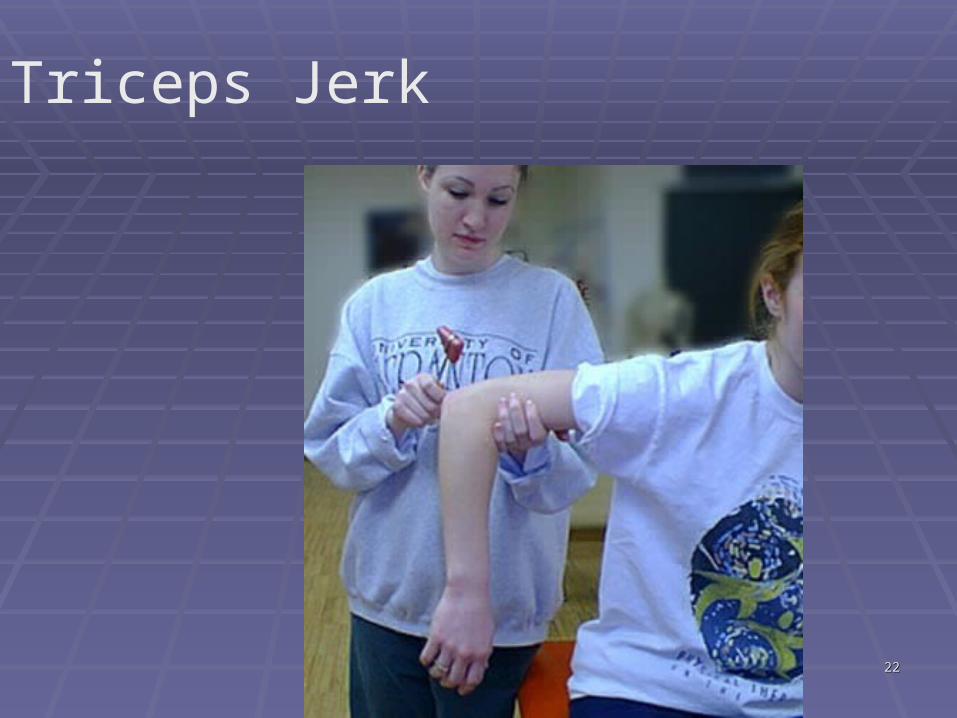
2-Triceps tendon reflex: C6 ,7,8(extension of elbow joint by tapping the triceps tendon)
2121
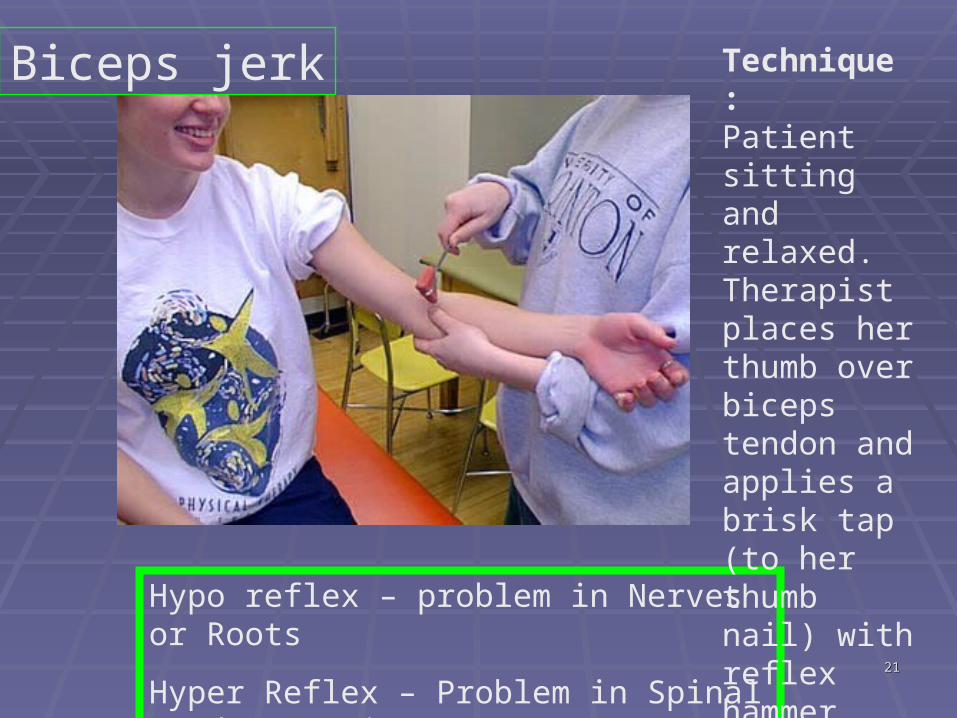
Hypo reflex – problem in Nerves or Roots
Hyper Reflex – Problem in Spinal cord or Brain
Technique :Patient sitting and relaxed. Therapist places her thumb over biceps tendon and applies a brisk tap (to her thumb nail) with reflex hammer
Biceps jerk
2222
Triceps Jerk
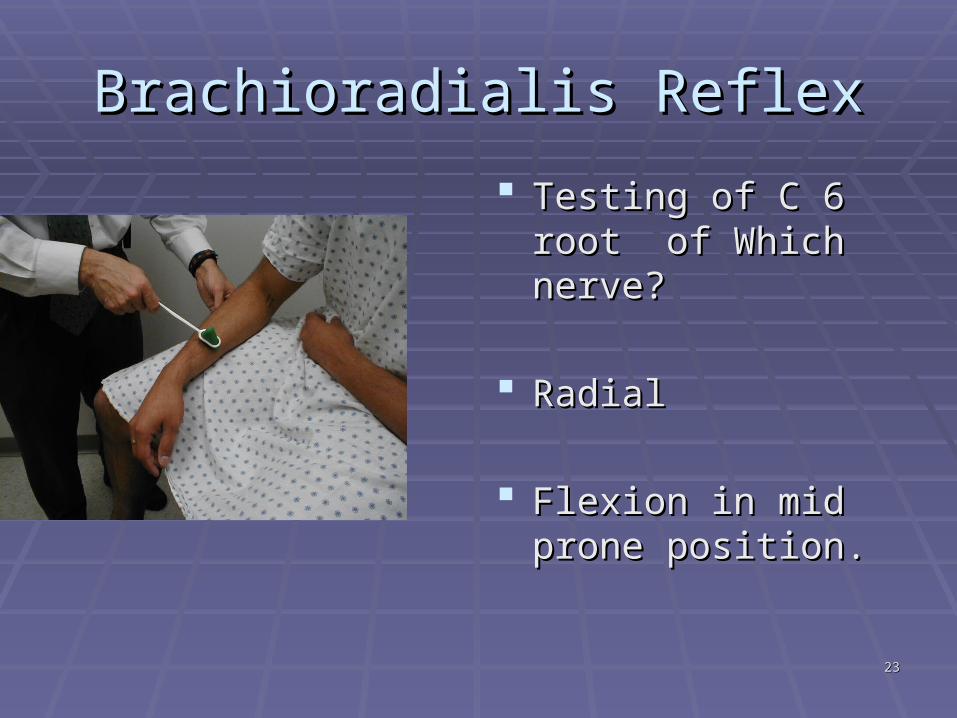
Brachioradialis ReflexBrachioradialis Reflex Testing of C 6 root of Testing of C 6 root of
Which nerve?Which nerve?
RadialRadial
Flexion in mid prone Flexion in mid prone position.position.
2323
Nerves and InjuriesNerves and Injuries
2424
2525
Injury to Brachial plexusInjury to Brachial plexus
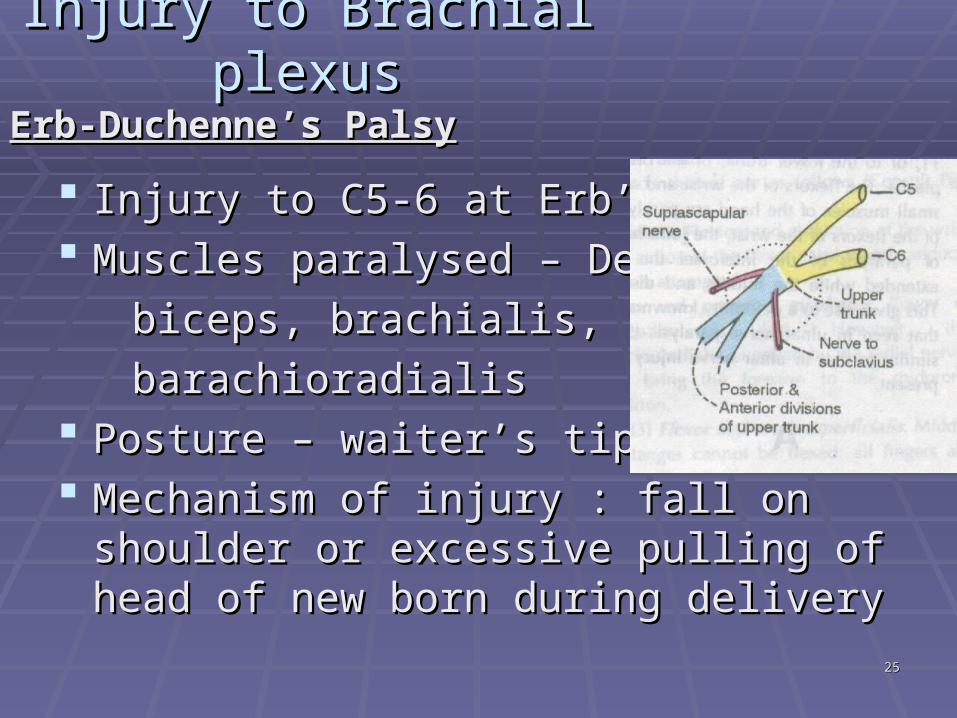
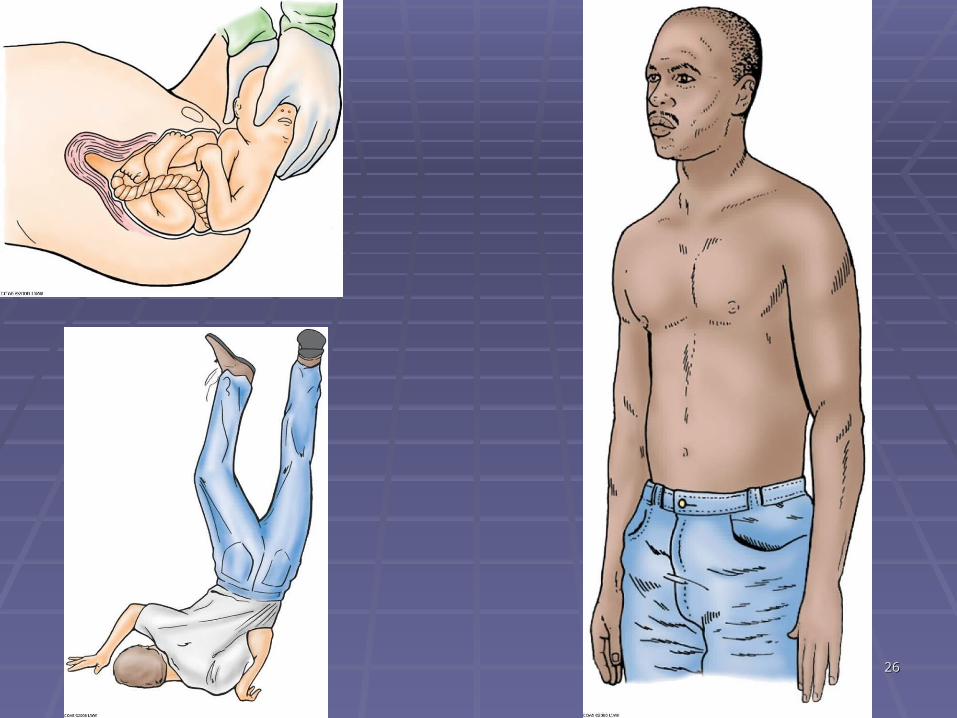
Injury to C5-6 at Erb’s pointInjury to C5-6 at Erb’s point Muscles paralysed – Deltoid,Muscles paralysed – Deltoid, biceps, brachialis,biceps, brachialis, barachioradialisbarachioradialis Posture – waiter’s tip deformityPosture – waiter’s tip deformity Mechanism of injury : fall on shoulder or Mechanism of injury : fall on shoulder or
excessive pulling of head of new born excessive pulling of head of new born during deliveryduring delivery
Erb-Duchenne’s PalsyErb-Duchenne’s Palsy
2626
2727
_Symptom: ( Waiter’s Tip position) The arm just droops there, hangs by the side shoulder medially rotated, shoulder adducted, elbow extended , forearm pronated.
• Loss of abduction @ shoulder-paralysis of deltoid• Loss of external rotation of shoulder-paralysis of supra and infraspinatus• Loss of flexion at elbow-paralysis of biceps, brachialis and brachioradialis • Loss of supination – paralysis of Biceps and supinator
2828
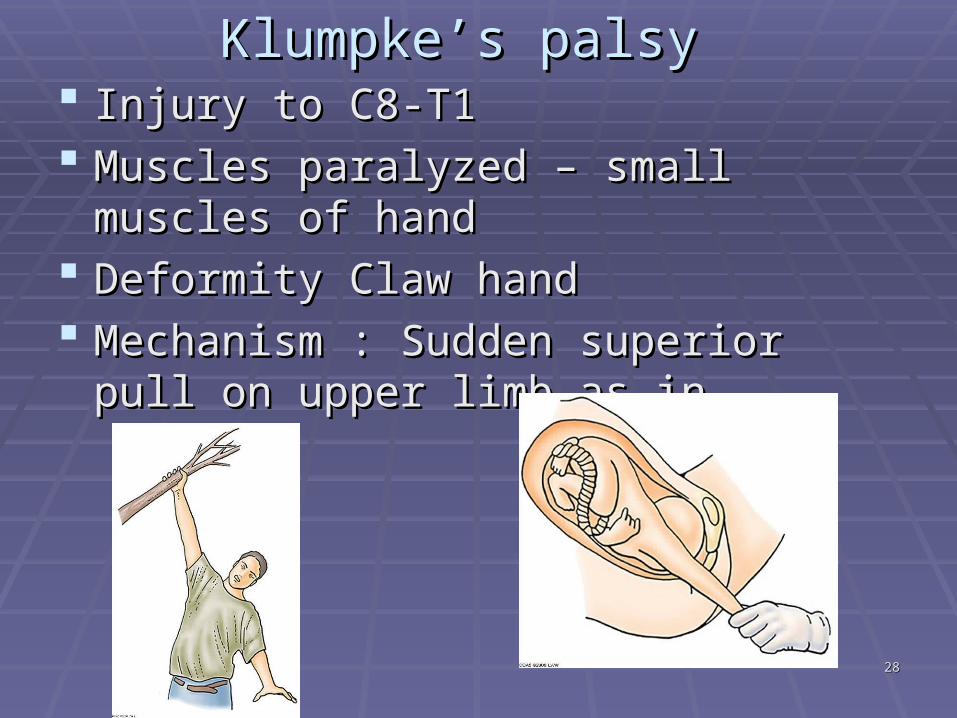
Klumpke’s palsyKlumpke’s palsy Injury to C8-T1Injury to C8-T1 Muscles paralyzed – small muscles of Muscles paralyzed – small muscles of
handhand Deformity Claw hand Deformity Claw hand Mechanism : Sudden superior pull on Mechanism : Sudden superior pull on
upper limb as in upper limb as in
2929
KLUMPKE’S PARALYSIS:
Mechanism of injury:1_Traction injuries caused by excessive abduction of the arm2_Presence of a cervical rib or malignant metastasis from the lung in the lower deep cervical Lymph Nodes
Basically, Loss of part of Median and most of Ulnar nerves
3030
Symptoms: * In acute stage – Loss of finger adduction & abduction *In Chronic stage - Clawed hand due to loss of innervation of Intrinsic muscle of the hand *Loss of sensation on medial aspect of arm , forearm and hand (due to loss of ulnar nerve & medial cutaneous nerves of arm and forearm.)*Horner’s Syndrome: [may be sometimes associated with klumpke’s paralysis]If there is damage to sympathetic chain along with injury to lower trunk of brachial plexusresulting in :-Ptosis-Constriction of the pupils-Enophthalmos apparent recession of the eyeball -Anhydrosis
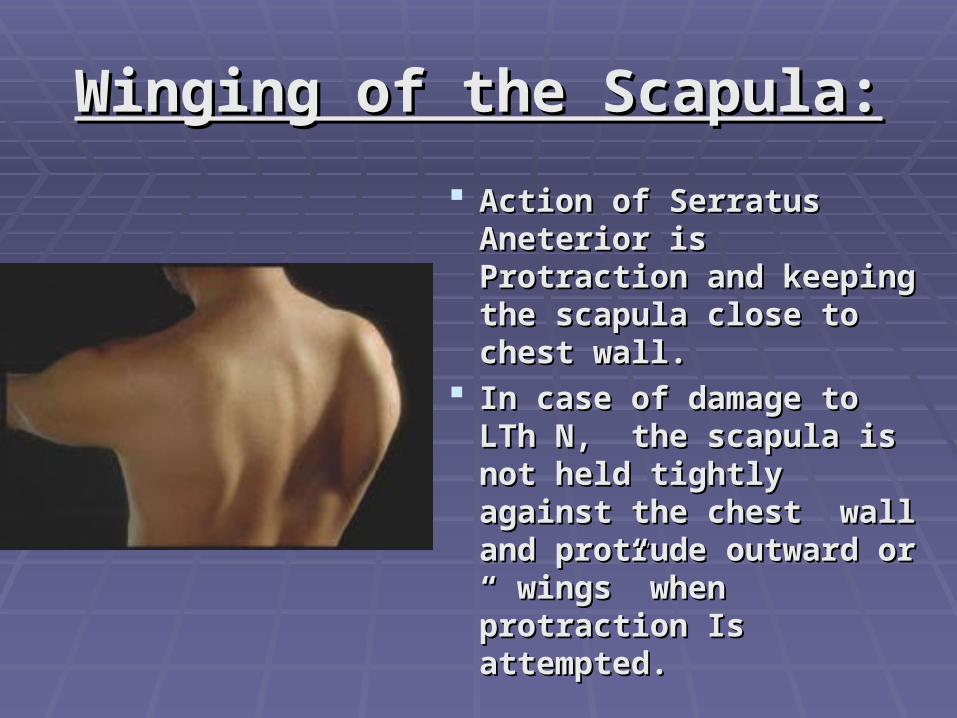
Winging of the Scapula:Winging of the Scapula: Action of Serratus Action of Serratus
Aneterior is Protraction Aneterior is Protraction and keeping the scapula and keeping the scapula close to chest wall.close to chest wall.
In case of damage to In case of damage to LTh N, the scapula is LTh N, the scapula is not held tightly against not held tightly against the chest wall and the chest wall and protrude outward or “ protrude outward or “ wings” when protraction wings” when protraction Is attempted.Is attempted.
3232
3333
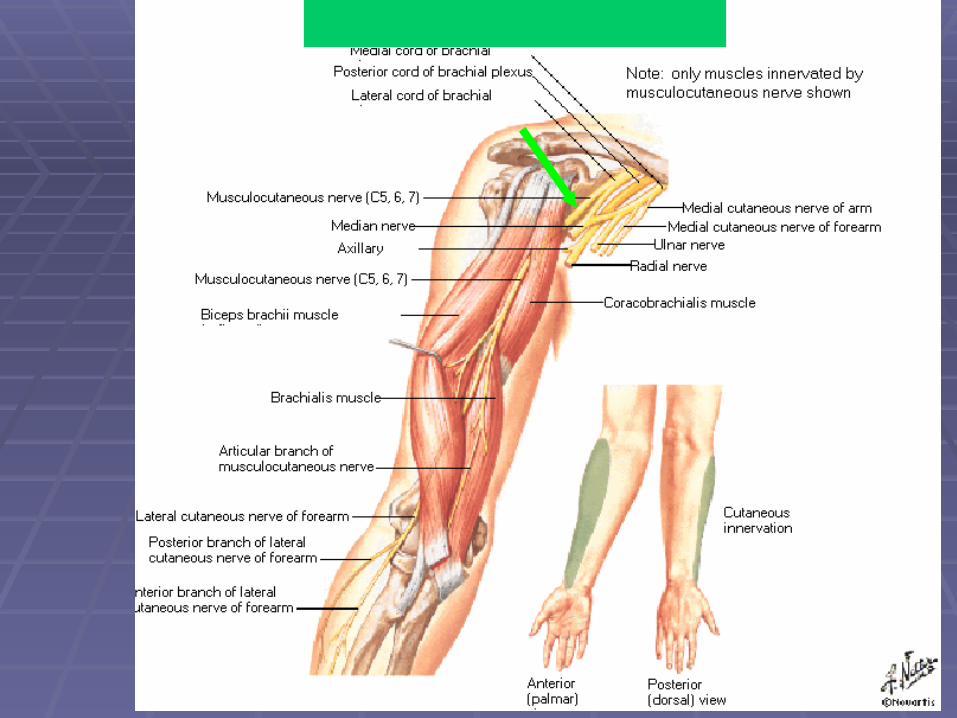
Branches: *Muscular -BBC ! [biceps, brachialis and corocobrachialis]*cutaneous -Lat.cut.n.of FA (Till the root of the thumb)
#Injury to MCN is uncommon 1-weakness of flexion & supination of FA 2-Loss of sensation on lat. side of FA
3434
Median nerve SummaryEnter Forearm by passing thru’ two heads of P T muscle & gives a deep branch : anterior interosseous nerve
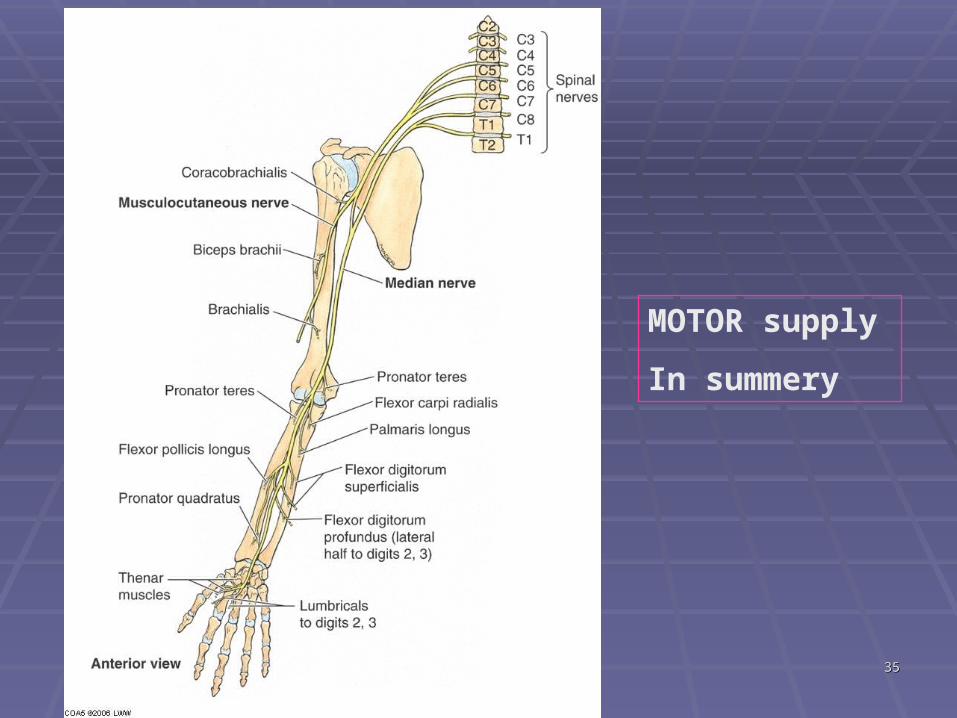
Supply in Forearm [only motor]: PT, FCR,PL, FDS, FPL, half of FDP, and PQ
Pass with in the carpal tunnel to go in Palm
Supply in Hand [motor and sensory]:
Motor- Abd P B, FPB, OP, 1st and 2nd Lumbricals
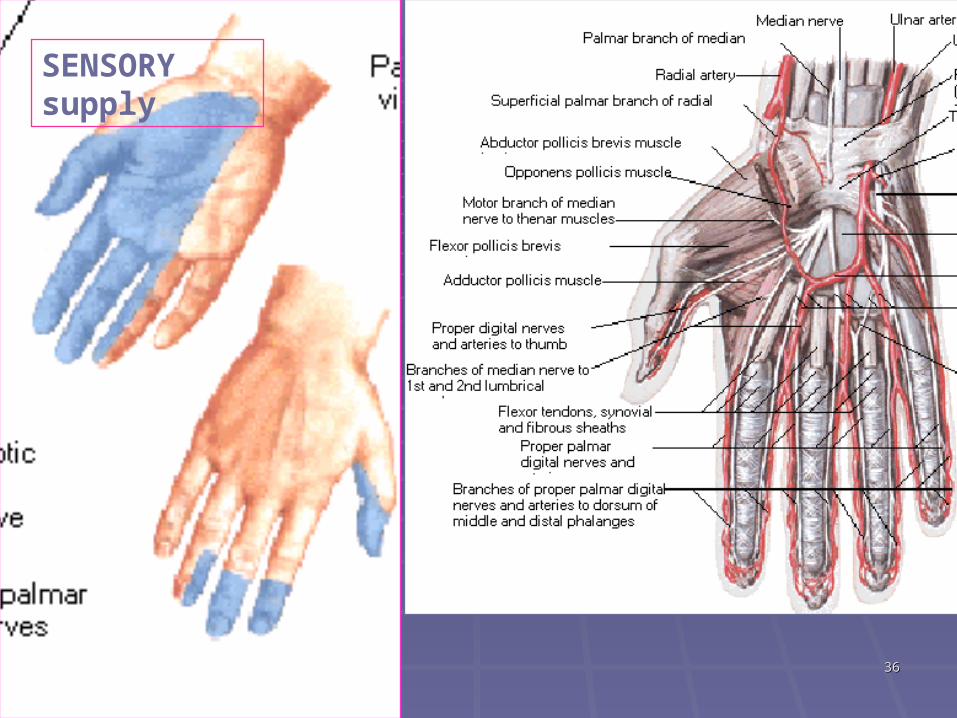
Sensory- lateral half of palm, lateral 3 and half fingers on palmar side and their tips on dorsal side.
3535
MOTOR supply
In summery
3636
SENSORY supply
3737
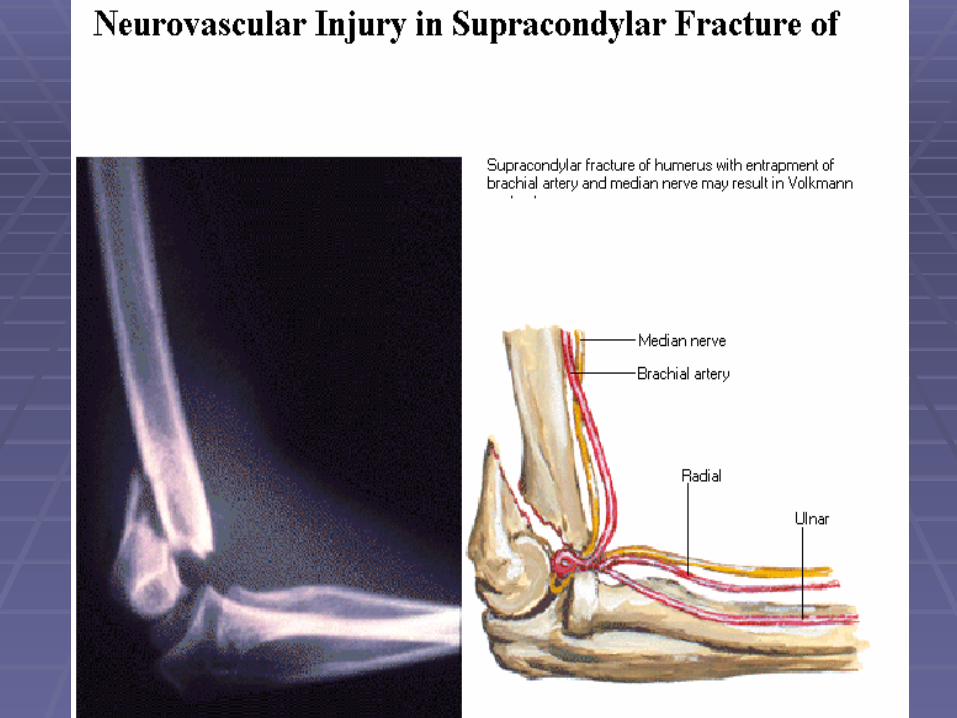
Median Nerve InjuriesMedian Nerve Injuries
Common SitesCommon Sites Near Elbow [supracondylar fractures or Near Elbow [supracondylar fractures or
penetrating wounds or pronator trap penetrating wounds or pronator trap syndromesyndrome
Near wrist before entering carpal tunnel, Near wrist before entering carpal tunnel, deep laceration proximal to the wrist.deep laceration proximal to the wrist.
At the wrist, compression in the carpal At the wrist, compression in the carpal tunnel.tunnel.
3838
3939
•Weakness in flexion of wrist [ulnar deviation on attempted flexion]
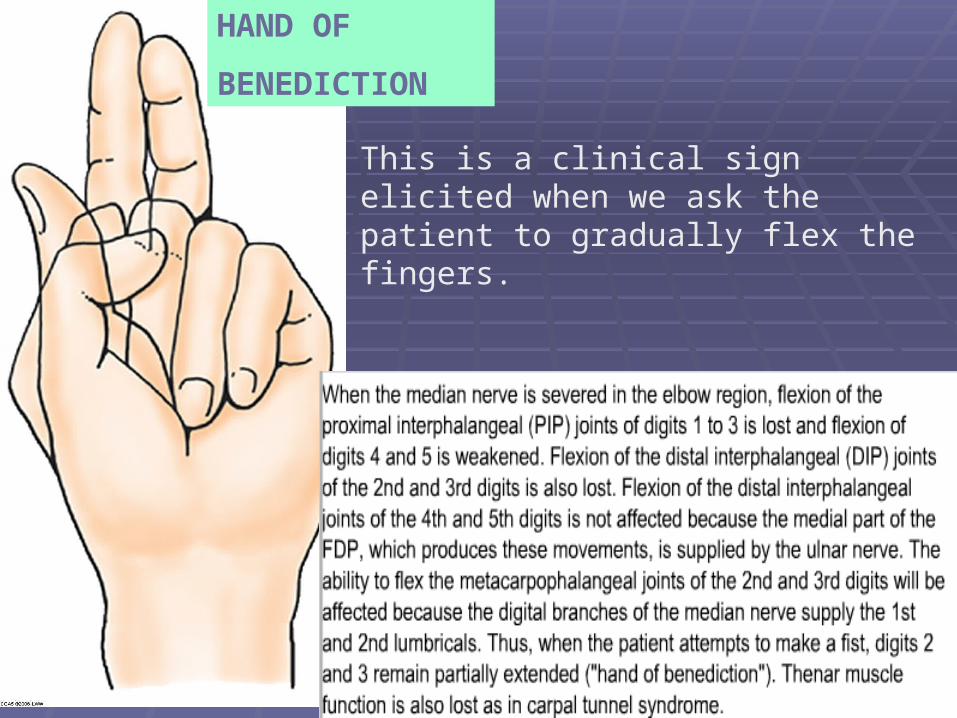
•Weakness of flex. of 1st,2nd,3rd IP joints + 2nd , 3rd MP joints [ hand of benediction]
•Thenar Weakness [atrophy of muscles]
•Weakness of thumb abd. And opp. [Ape Hand]
•Sensory loss/abnormality in 3 and half fingers + lateral aspect of skin of palm
•Carpal Tunnel syn. [ Sensory symptoms along the supply]
Summary of Median Nerve Injury
4040
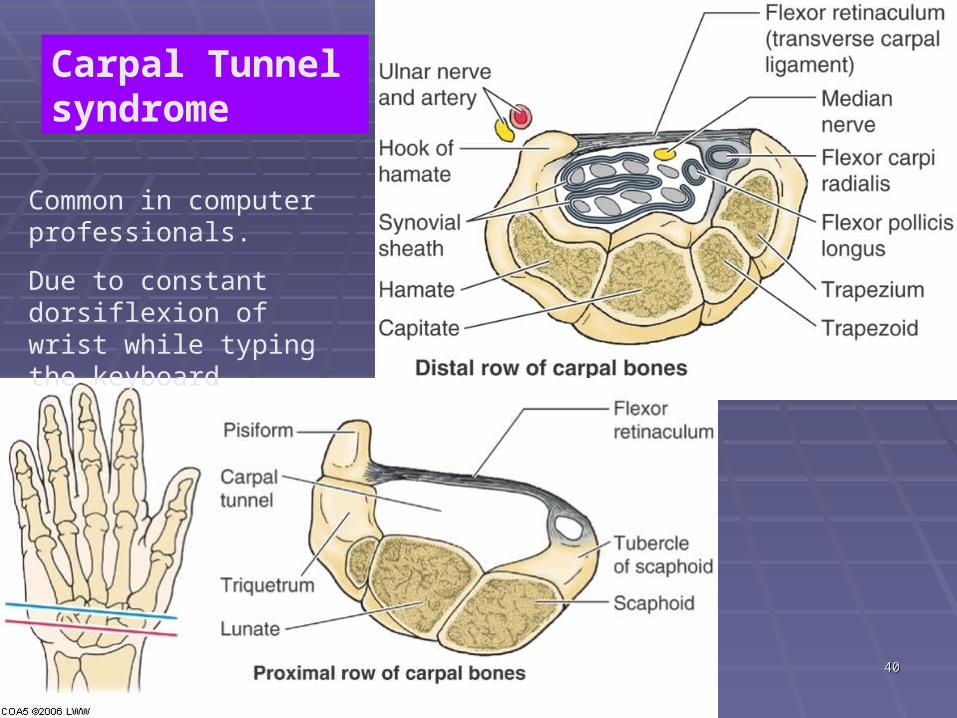
Carpal Tunnel syndrome
Common in computer professionals.
Due to constant dorsiflexion of wrist while typing the keyboard
4141
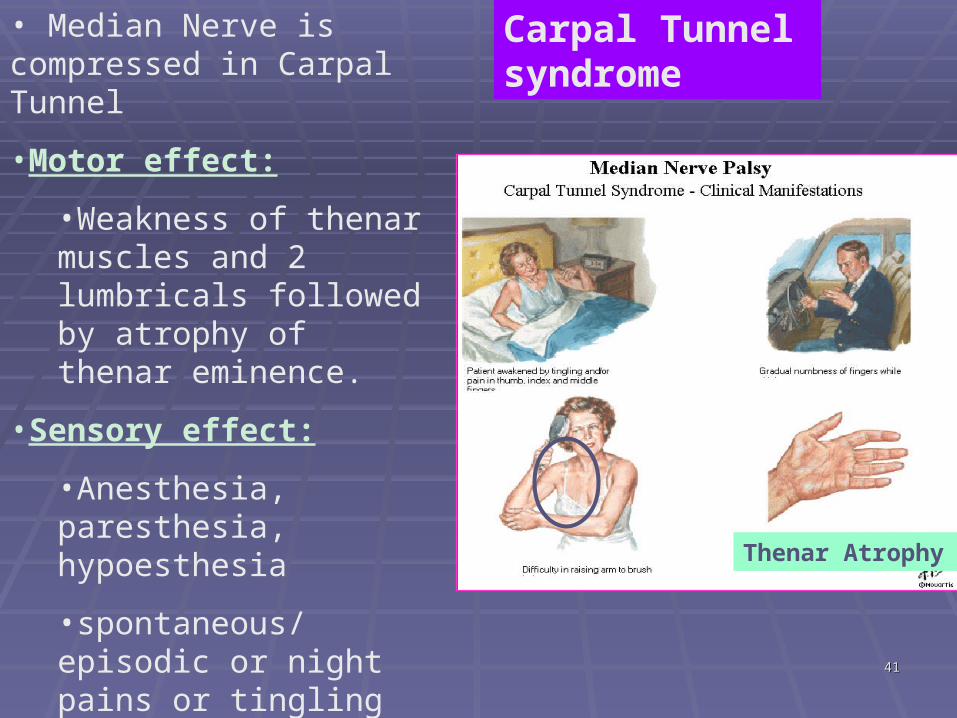
Thenar Atrophy
• Median Nerve is compressed in Carpal Tunnel
•Motor effect:
•Weakness of thenar muscles and 2 lumbricals followed by atrophy of thenar eminence.
•Sensory effect:
•Anesthesia, paresthesia, hypoesthesia
•spontaneous/episodic or night pains or tingling numbness in lateral 3 fingers; skin of the palm is mostly not involved.
Carpal Tunnel syndrome
4242
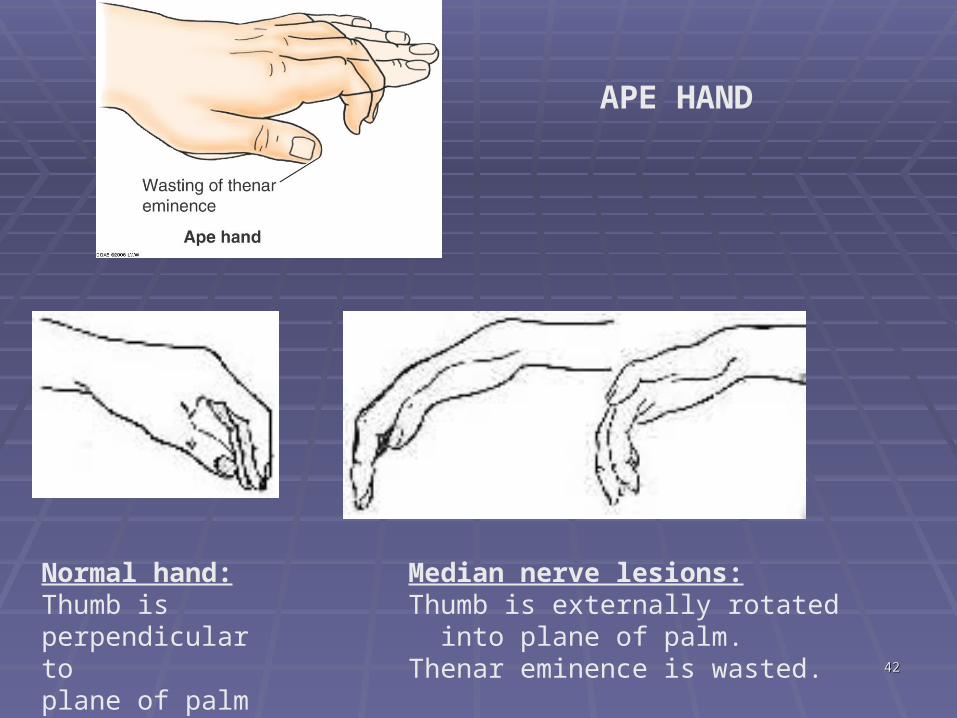
Normal hand:Thumb is perpendicular toplane of palm
Median nerve lesions:Thumb is externally rotated into plane of palm.Thenar eminence is wasted.
APE HAND
4343
HAND OF
BENEDICTION
This is a clinical sign elicited when we ask the patient to gradually flex the fingers.
4444
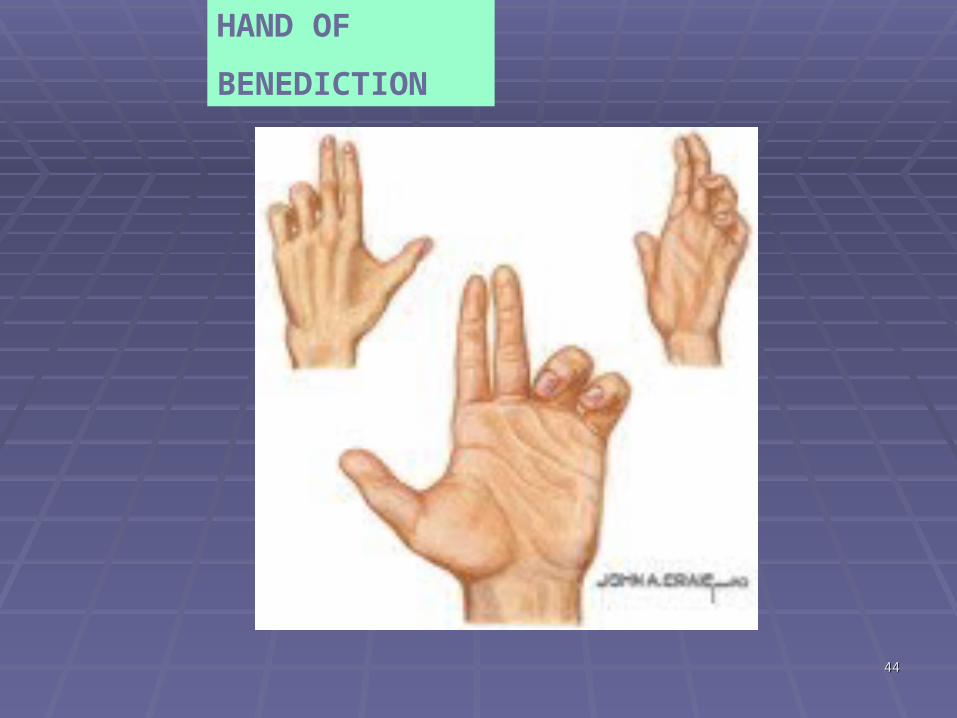
HAND OF
BENEDICTION
4545
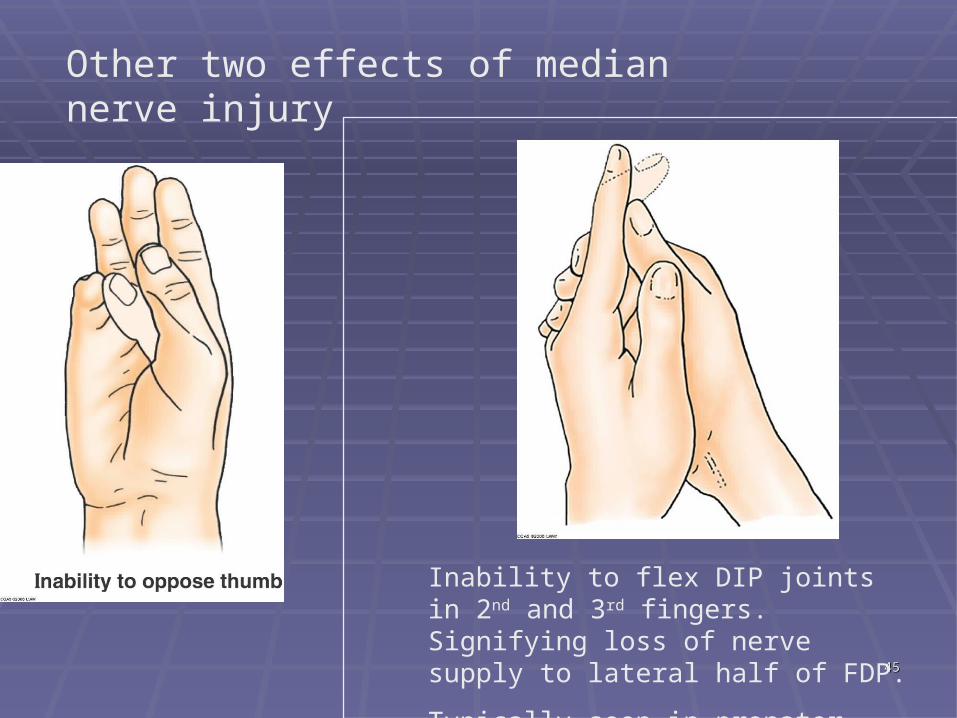
Other two effects of median nerve injury
Inability to flex DIP joints in 2nd and 3rd fingers. Signifying loss of nerve supply to lateral half of FDP.
Typically seen in pronator trap syndrome.
4646
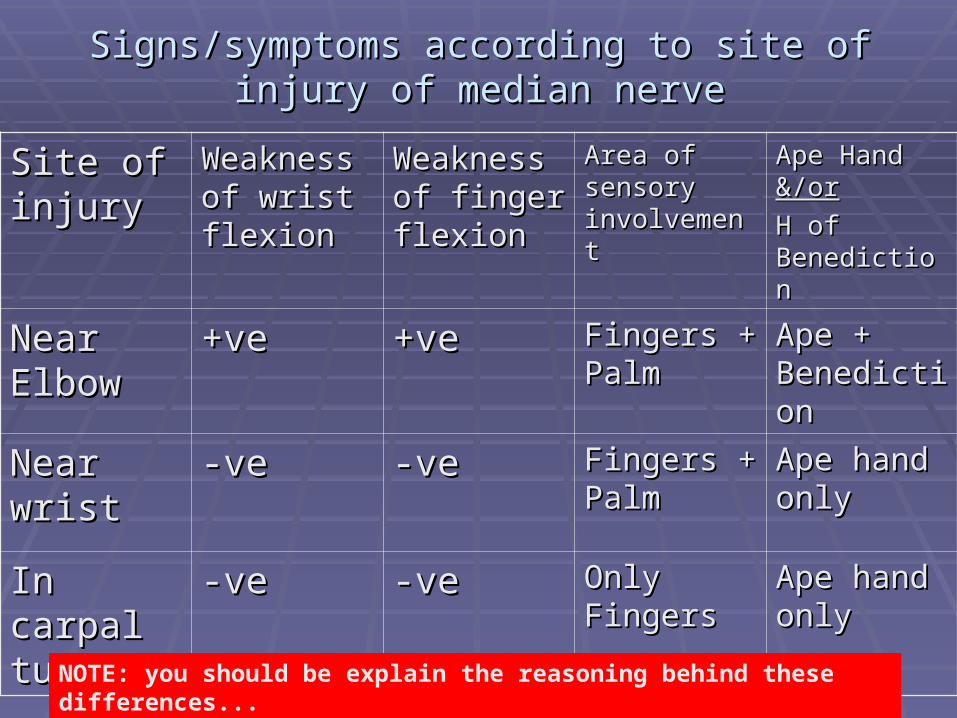
Signs/symptoms according to site of injury of Signs/symptoms according to site of injury of median nervemedian nerve
Site of Site of injuryinjury
Weakness Weakness of wrist of wrist flexionflexion
Weakness Weakness of finger of finger flexionflexion
Area of Area of sensory sensory involvementinvolvement
Ape Hand Ape Hand &/or&/orH of H of BenedictionBenediction
Near Near ElbowElbow
+ve+ve +ve+ve Fingers + Fingers + PalmPalm
Ape + Ape + BenedictionBenediction
Near wristNear wrist -ve-ve -ve-ve Fingers + Fingers + PalmPalm
Ape hand Ape hand onlyonly
In carpal In carpal tunneltunnel
-ve-ve -ve-ve Only Only FingersFingers
Ape hand Ape hand onlyonly
NOTE: you should be explain the reasoning behind these differences...
4747
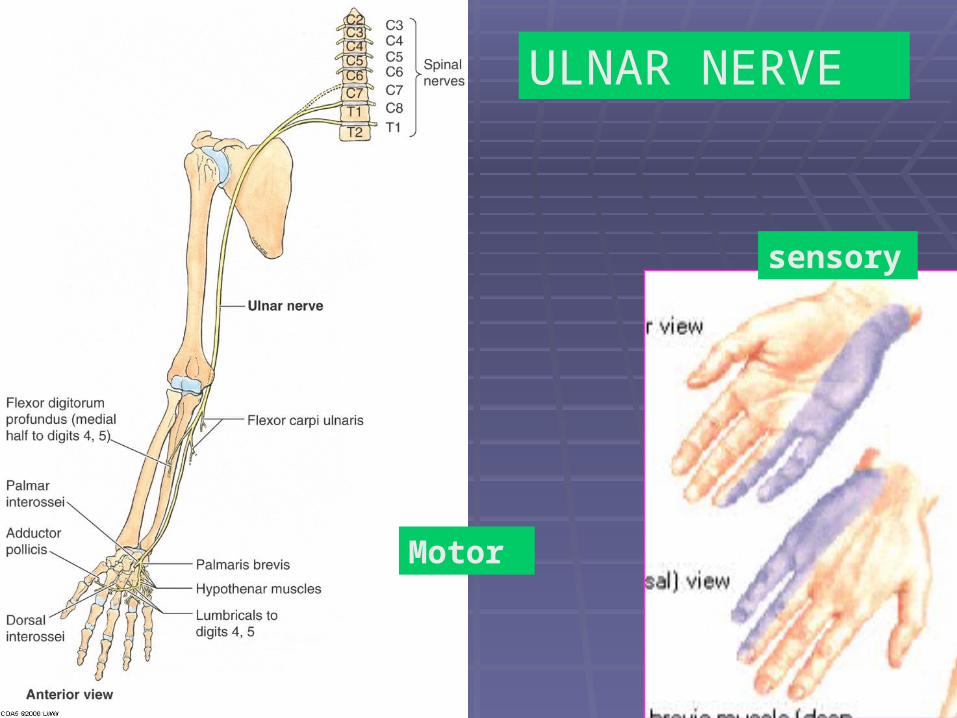
Motor
sensory
ULNAR NERVE
4848
Summary of Ulnar nervePass behind the medial epicondyle : palpable there, likely to get damage in Fracture there.
Pass superficial to flexor retinaculum
Supply :
Forearm : Only motor : FCU and half of FDP
Palm :
Motor : Abd Di Mi, F Di Mi, O Di Mi, Add P, 3rd and 4th Lumbricals, All interossei
Sensory : medial 1/3rd of skin of palm and on dorsum of hand, medial 1 and half fingers on palmer and dorsal aspect
4949
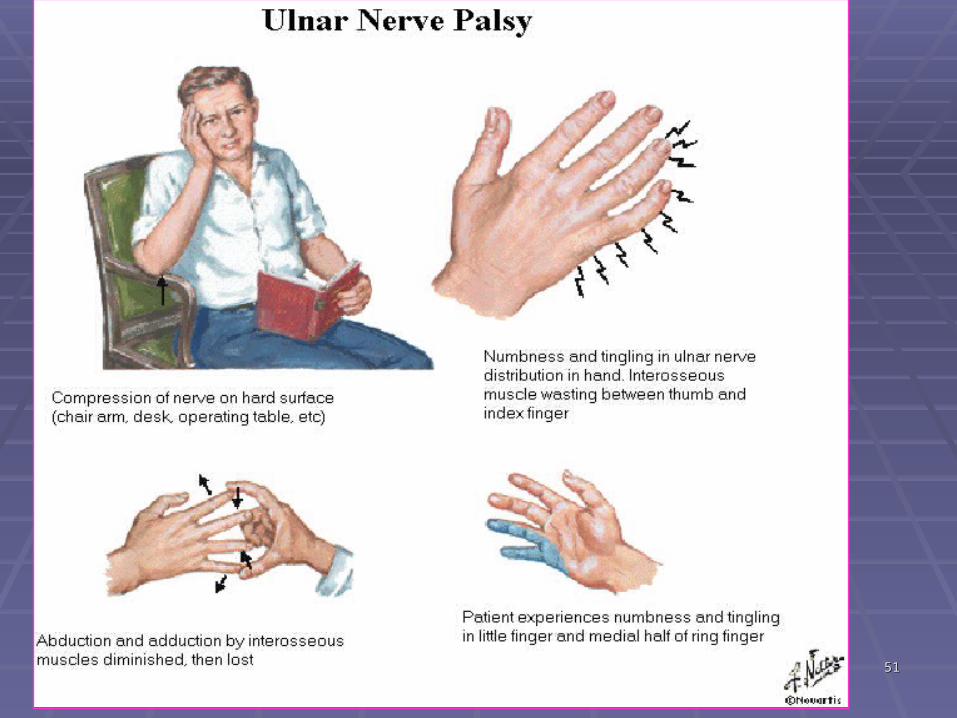
Injury of ULNAR nerve has primary effect on the hand muscle
A.Motor loss: [HAND]•Acute stage-
•inability to abduct and adduct the digits (paralysis of dorsal and palmar interossei muscle)• loss of adduction of the thumb (paralysis of adductor pollicis)• weakneness of flexion of the 4th and 5th digits at the MP joint (paralysis of the medial two lumbricals)•Difficulty making a fist because they can not flex their 4th and 5th digits at the distal IP joint
• Chronic Stage-• (partial) Claw hand[weak flexion at MP and weak extension at IP due to loss of Intrinsic muscles but long extensors will extend MP and long flexors will flex IP joints… therefore CLAW For claw hand consider loss of action of lumb. and
interossei muscles on MP and IP joints.
5050
MOTOR LOSS: [Forearm]
•impaired flexion and adduction of the wrist (paralysis of the flexor FCU)
• When an attempt is made to flex the wrist joint, the hand is drawn to the lateral side by the flexor carpi radialis (supplied by median nerve)
B. Sensory loss:
Medial one and 1/2 finger and medial part of palm
5151
5252
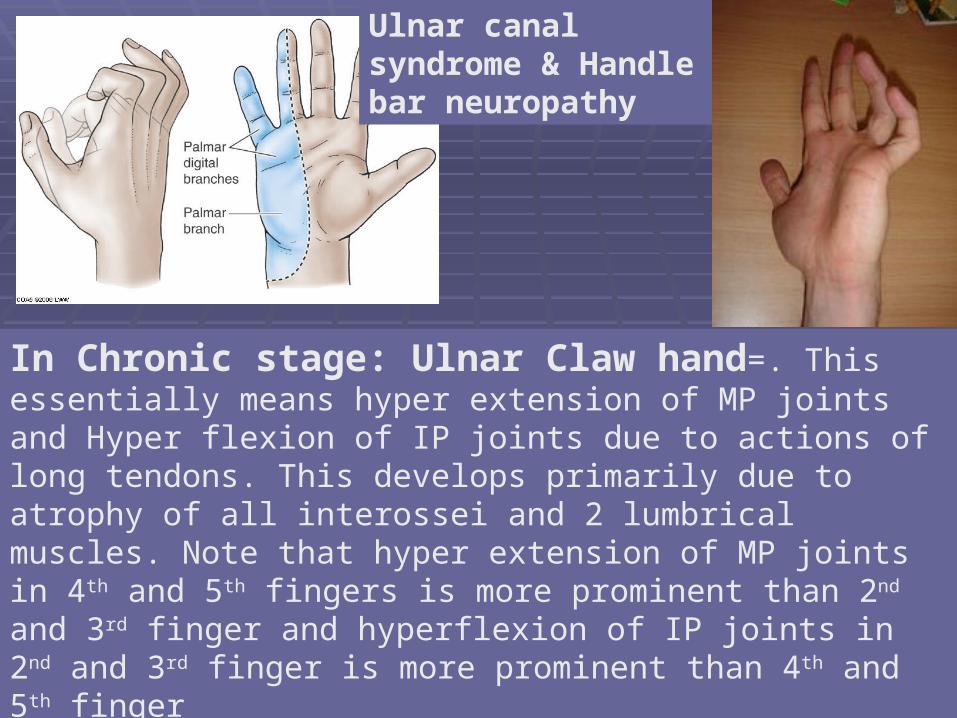
In Chronic stage: Ulnar Claw hand=. This essentially means hyper extension of MP joints and Hyper flexion of IP joints due to actions of long tendons. This develops primarily due to atrophy of all interossei and 2 lumbrical muscles. Note that hyper extension of MP joints in 4th and 5th fingers is more prominent than 2nd and 3rd finger and hyperflexion of IP joints in 2nd and 3rd finger is more prominent than 4th and 5th finger
Ulnar canal syndrome & Handle bar neuropathy
5353
5454
Clinical summary for ulnar nerve injury :
Radial deviation on attempting wrist flexion
Ulnar Claw hand Paper holding test Finger spreading test Sensory symptoms in ulnar nerve
territory.
5555
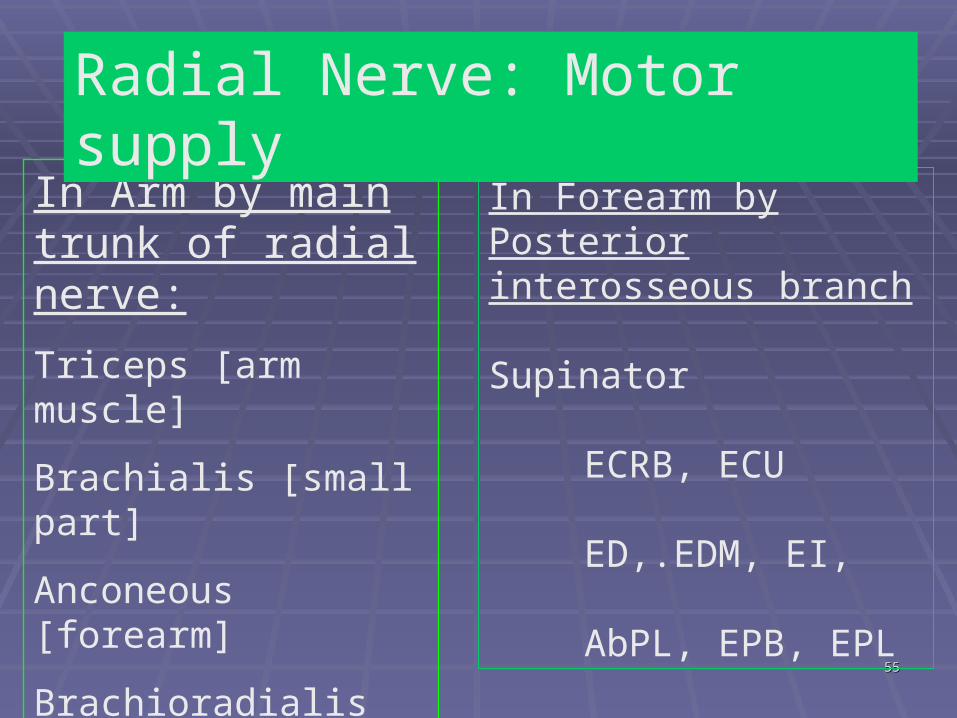
In Arm by main trunk of radial nerve:
Triceps [arm muscle]
Brachialis [small part]
Anconeous [forearm]
Brachioradialis [forearm]
Extensor Carpi radialis Longus [forearm]
In Forearm by Posterior interosseous branch
Supinator
ECRB, ECU
ED,.EDM, EI,
AbPL, EPB, EPL
Radial Nerve: Motor supply
5656
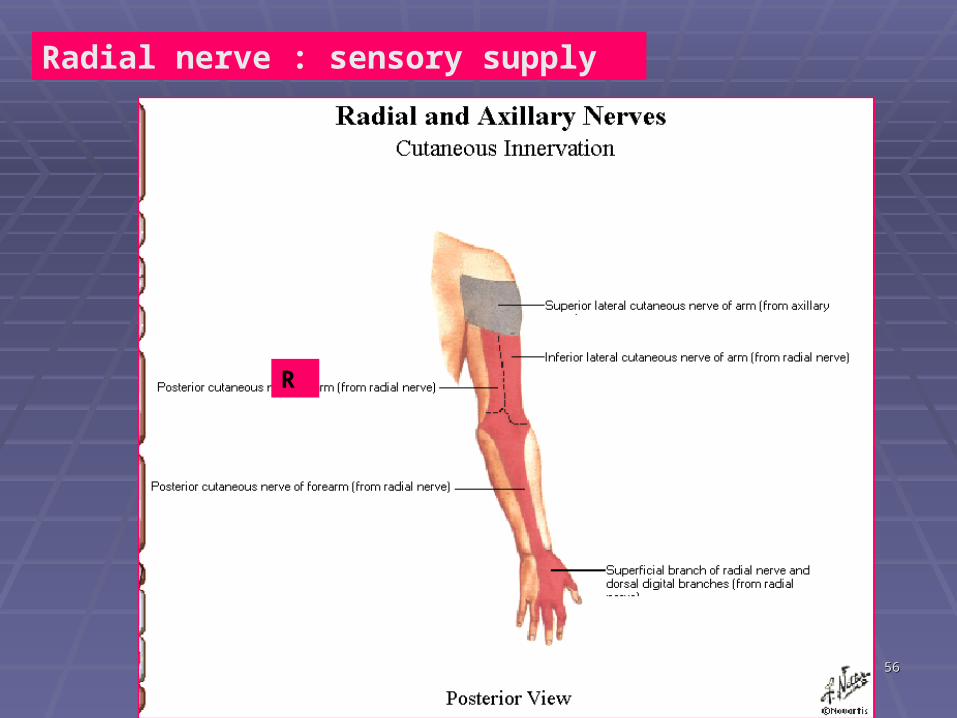
Radial nerve : sensory supply
R
5757
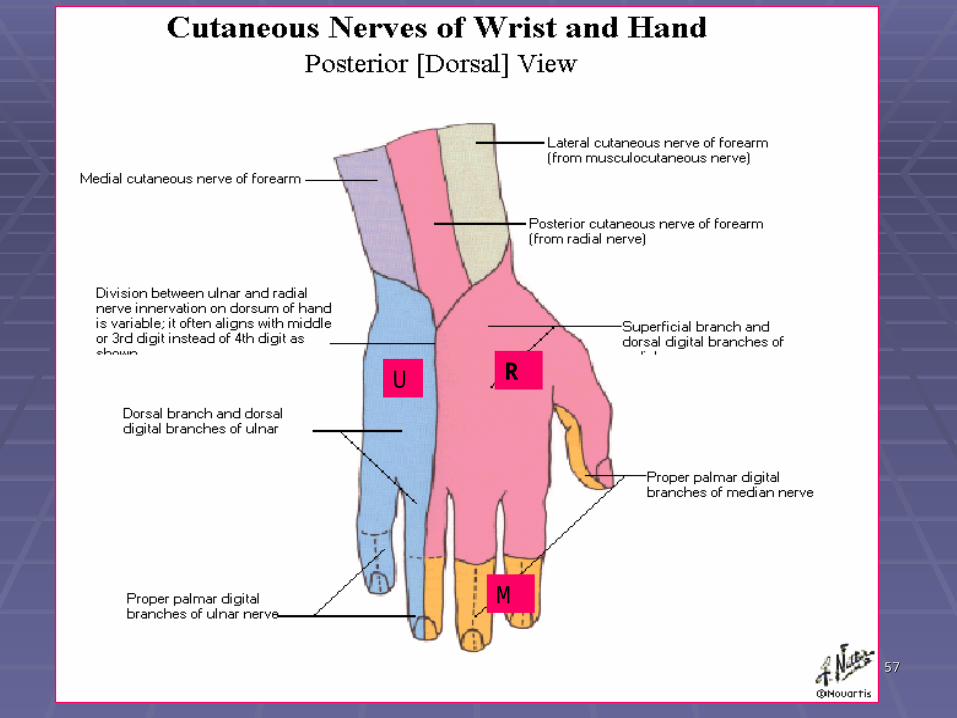
RU
M
5858
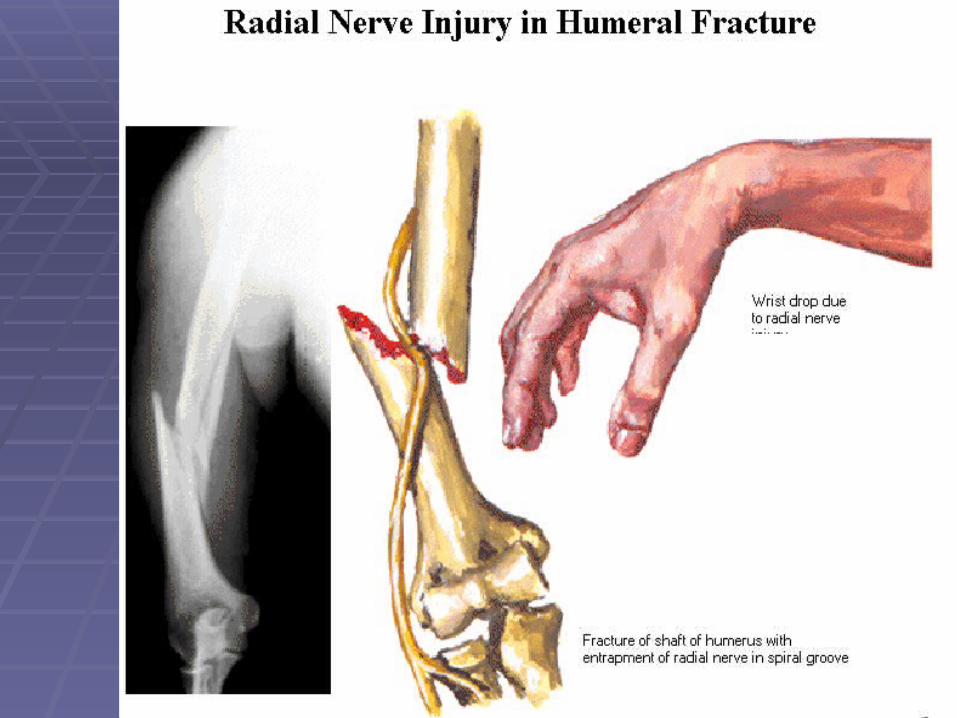
Clinical: Injuries of radial nerve in the spiral groove
-fracture of the shaft of the humerus -prolonged application of tourniquet to the arm -site of injury: the injuries of radial n. occurs most commonly in the distal Part of the spiral groove, beyond the origin of the nerves to the triceps and Anconeus muscle and the origin of cut. N
Symptoms : motorthe pt. Is unable to extend the wrist(wrist drop) sensorysmall area dorsal surface of the hand
5959

6060
Radian nerve palsy/ SATURDAY NIGHT PALSY / Lover’s palsy/ Honeymooner’s palsy
Main Effect: WRIST DROP
1. Crutches pressing axilla
2. Backrest of chair pressing lower axilla or upper shaft of humerus
3. Placement of one’s arm over back of neighboring chair (movie theater)
4. Letting another person’s head rest over one’s arm while sleeping
6161
JOINTS, BONES and JOINTS, BONES and InjuriesInjuries
6262
JOINTS :JOINTS :
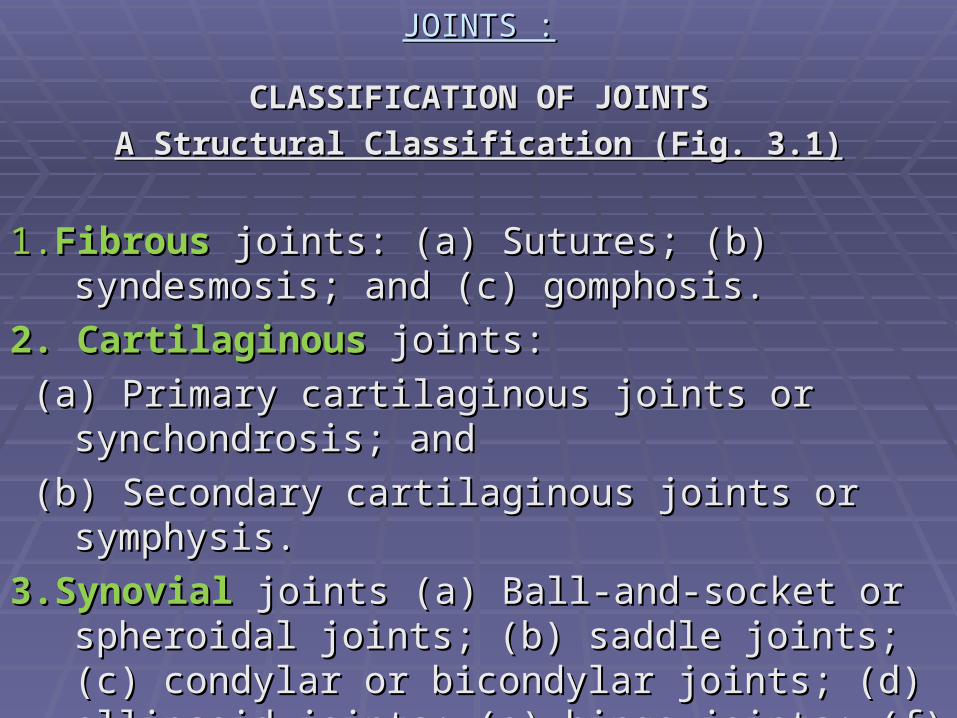
CLASSIFICATION OF JOINTSCLASSIFICATION OF JOINTSA A Structural Classification (Fig. 3.1)Structural Classification (Fig. 3.1)
1.1.Fibrous Fibrous joints: (a) Sutures; (b) syndesmosis; and (c) joints: (a) Sutures; (b) syndesmosis; and (c)
gomphosis.gomphosis.2. Cartilaginous 2. Cartilaginous joints: joints: (a) Primary cartilaginous joints or synchondrosis; and(a) Primary cartilaginous joints or synchondrosis; and (b) Secondary cartilaginous joints or symphysis.(b) Secondary cartilaginous joints or symphysis.3.Synovial3.Synovial joints (a) Ball-and-socket or spheroidal joints (a) Ball-and-socket or spheroidal
joints; (b) saddle joints; (c) condylar or bicondylar joints; (b) saddle joints; (c) condylar or bicondylar joints; (d) ellipsoid joints; (e) hinge joints; (f) pivot joints; (d) ellipsoid joints; (e) hinge joints; (f) pivot joints and (g) plane joints.joints and (g) plane joints.
6565
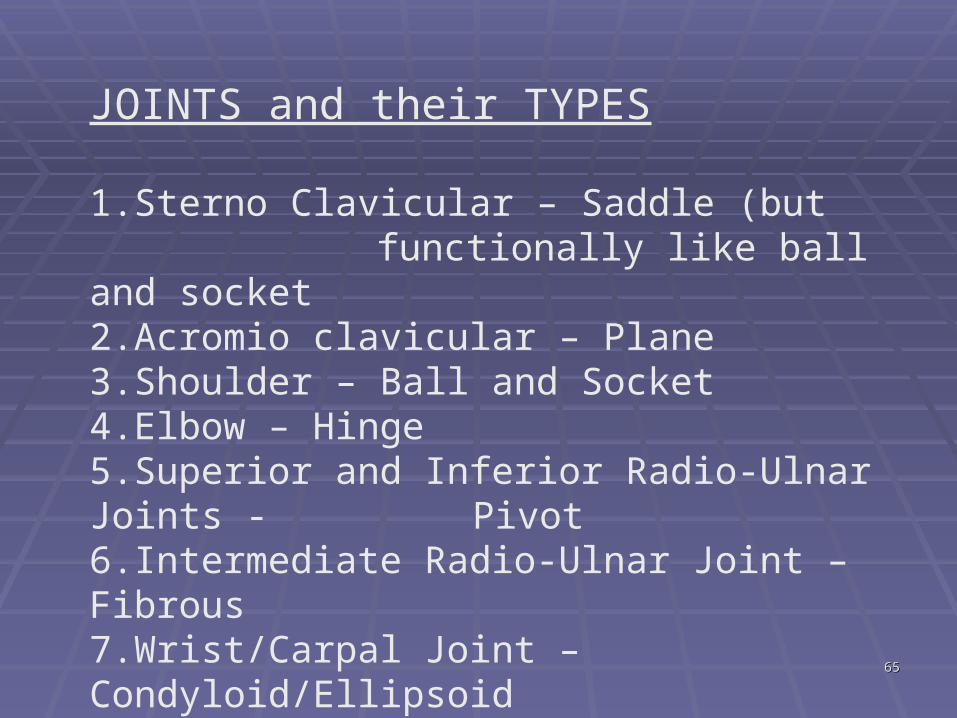
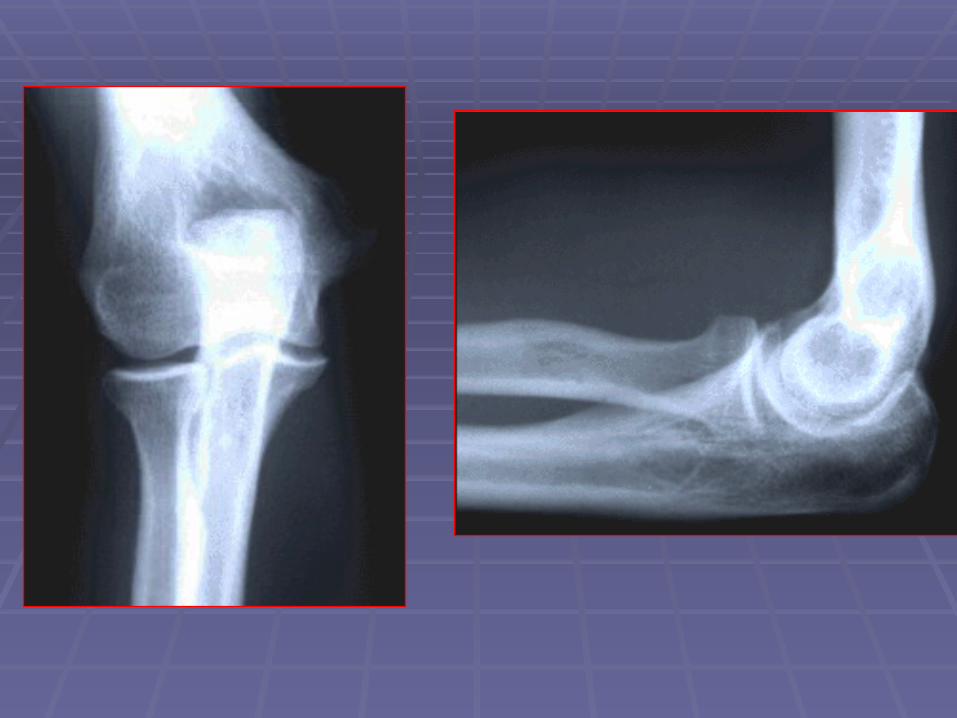
JOINTS and their TYPES
1.Sterno Clavicular – Saddle (but functionally like ball and socket
2.Acromio clavicular – Plane3.Shoulder – Ball and Socket4.Elbow – Hinge5.Superior and Inferior Radio-Ulnar Joints -
Pivot6.Intermediate Radio-Ulnar Joint – Fibrous7.Wrist/Carpal Joint – Condyloid/Ellipsoid8.First Carpo-metacarpal Joint - Saddle
6868
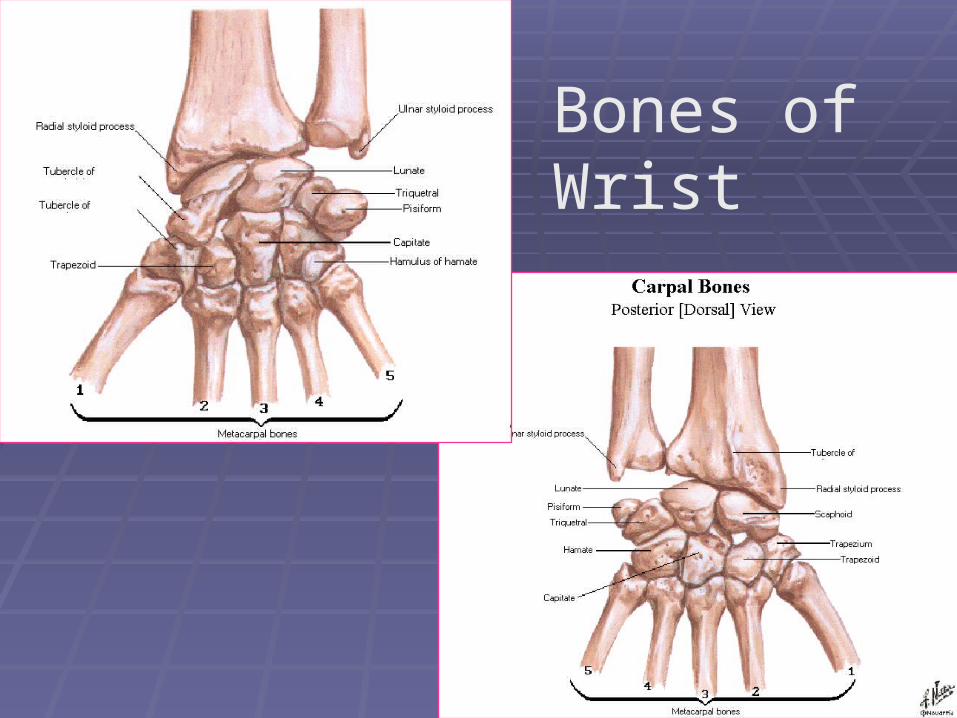
Bones of Wrist
6969
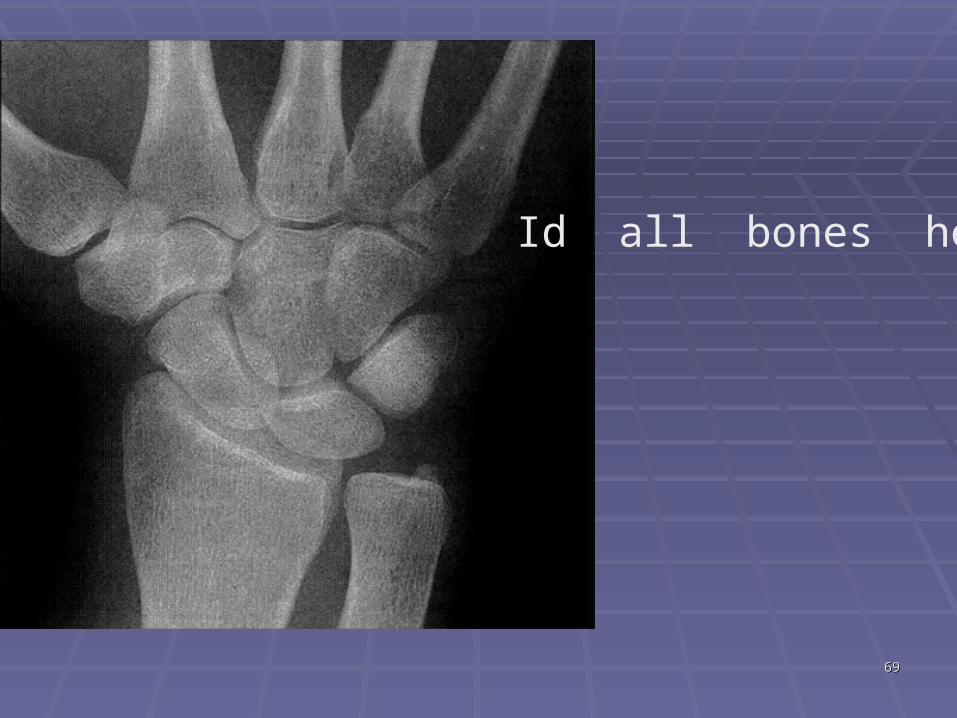
Id all bones here
7070
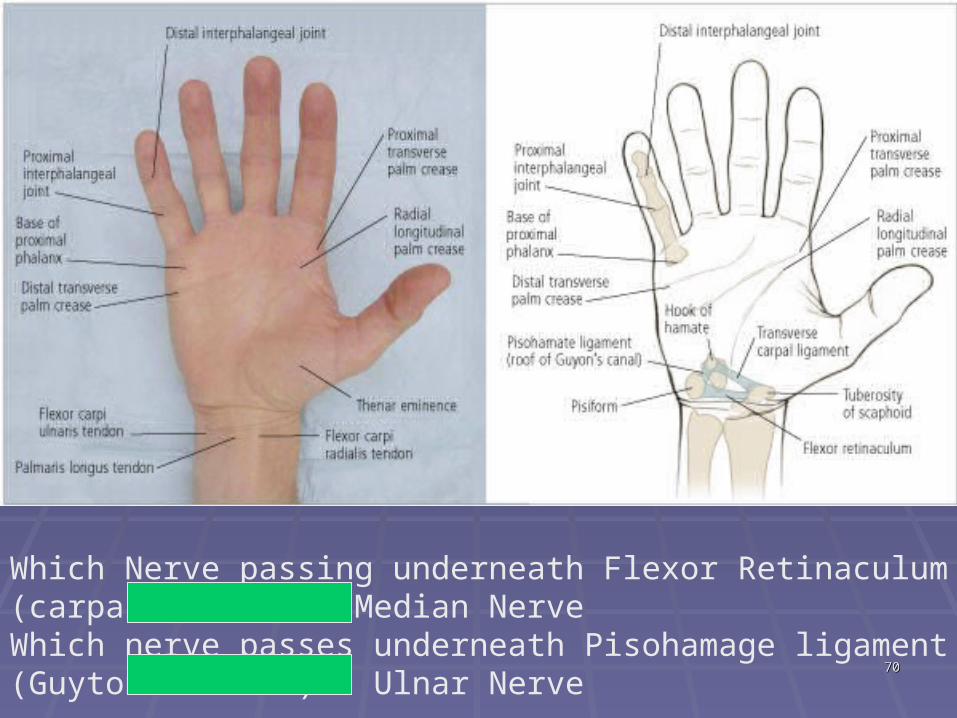
Which Nerve passing underneath Flexor Retinaculum (carpal tunnel) = Median NerveWhich nerve passes underneath Pisohamage ligament (Guyton’s canal) = Ulnar Nerve
7171
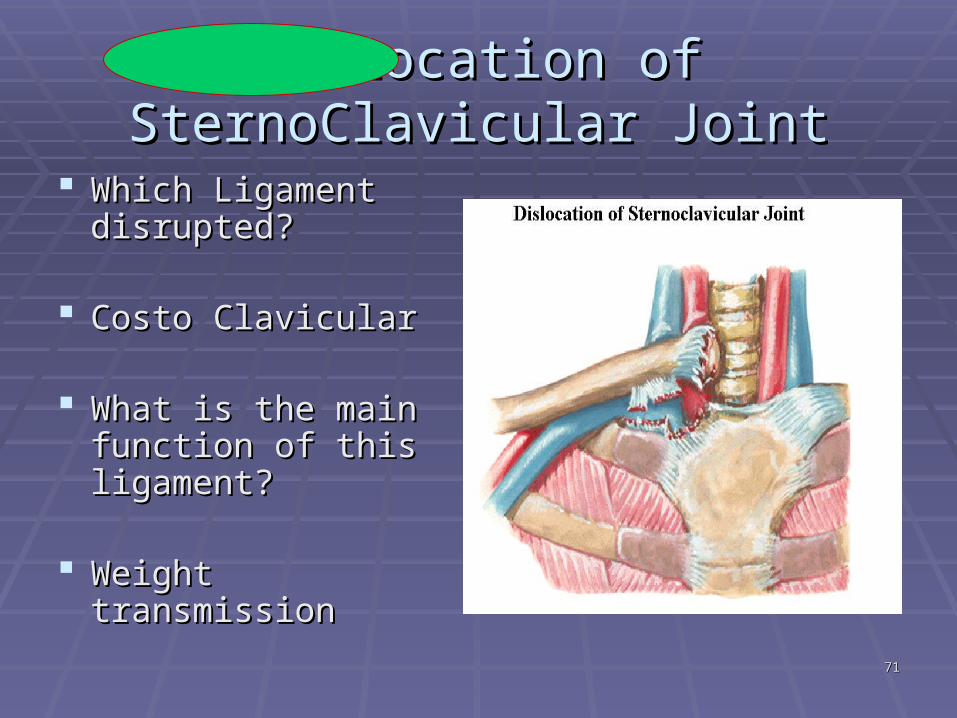
Dislocation of SternoClavicular Dislocation of SternoClavicular JointJoint
Which Ligament Which Ligament disrupted?disrupted?
Costo ClavicularCosto Clavicular
What is the main What is the main function of this function of this ligament?ligament?
Weight transmissionWeight transmission
7272
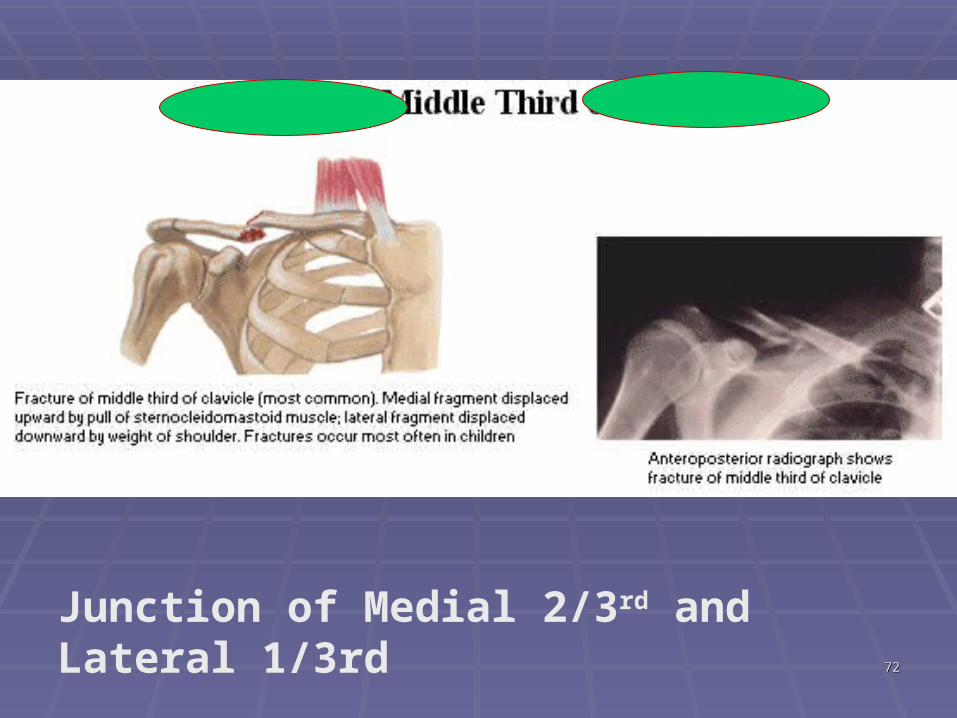
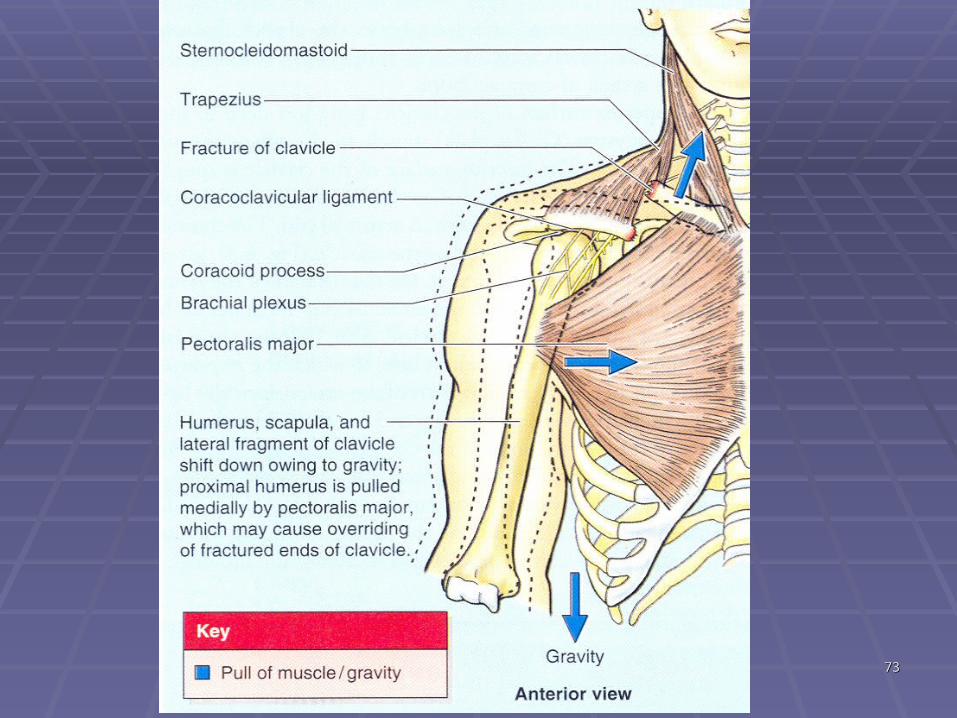
Junction of Medial 2/3rd and Lateral 1/3rd
7373
7474
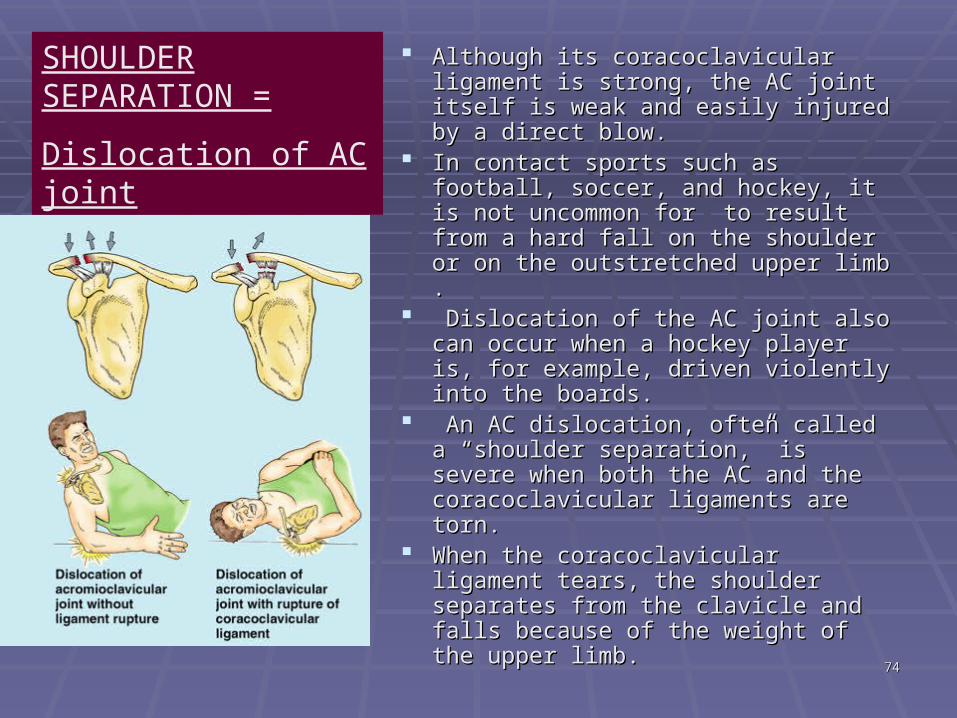
Although its coracoclavicular ligament Although its coracoclavicular ligament is strong, the AC joint itself is weak and is strong, the AC joint itself is weak and easily injured by a direct blow. easily injured by a direct blow.
In contact sports such as football, In contact sports such as football, soccer, and hockey, it is not soccer, and hockey, it is not uncommon for to result from a hard uncommon for to result from a hard fall on the shoulder or on the fall on the shoulder or on the outstretched upper limb .outstretched upper limb .
Dislocation of the AC joint also can Dislocation of the AC joint also can occur when a hockey player is, for occur when a hockey player is, for example, driven violently into the example, driven violently into the boards.boards.
An AC dislocation, often called a An AC dislocation, often called a “shoulder separation,” is severe when “shoulder separation,” is severe when both the AC and the coracoclavicular both the AC and the coracoclavicular ligaments are torn. ligaments are torn.
When the coracoclavicular ligament When the coracoclavicular ligament tears, the shoulder separates from the tears, the shoulder separates from the clavicle and falls because of the weight clavicle and falls because of the weight of the upper limb. of the upper limb.
SHOULDER SEPARATION =Dislocation of AC joint
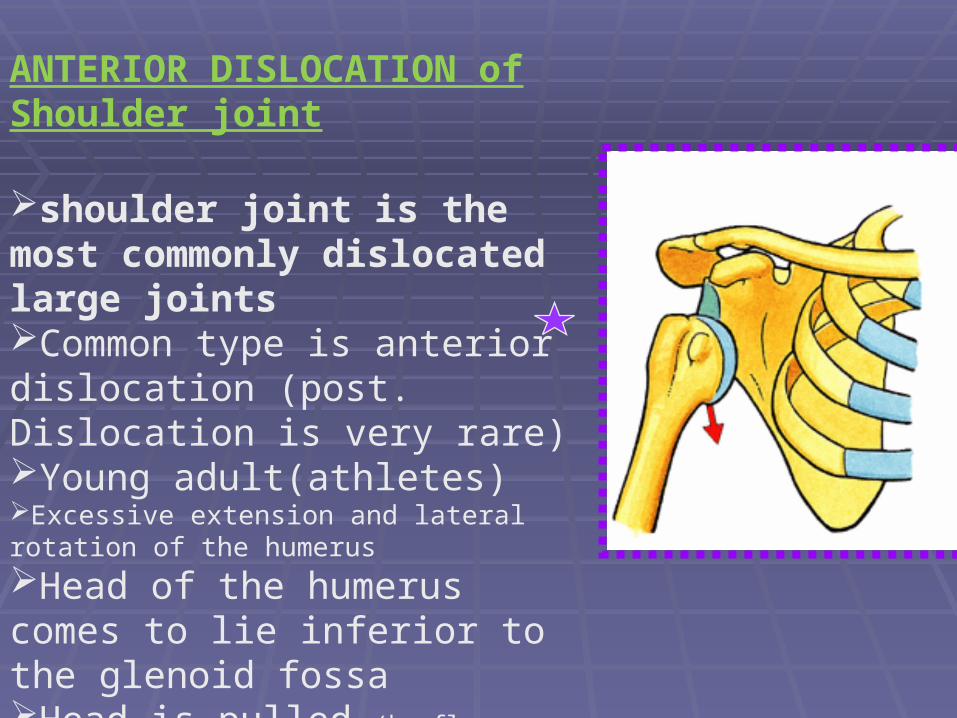
ANTERIOR DISLOCATION of Shoulder joint
shoulder joint is the most commonly dislocated large jointsCommon type is anterior dislocation (post. Dislocation is very rare)Young adult(athletes)Excessive extension and lateral rotation of the humerusHead of the humerus comes to lie inferior to the glenoid fossaHead is pulled (by flexors and adductors of the
shoulder joint) forward And upward into the subcoracoid position
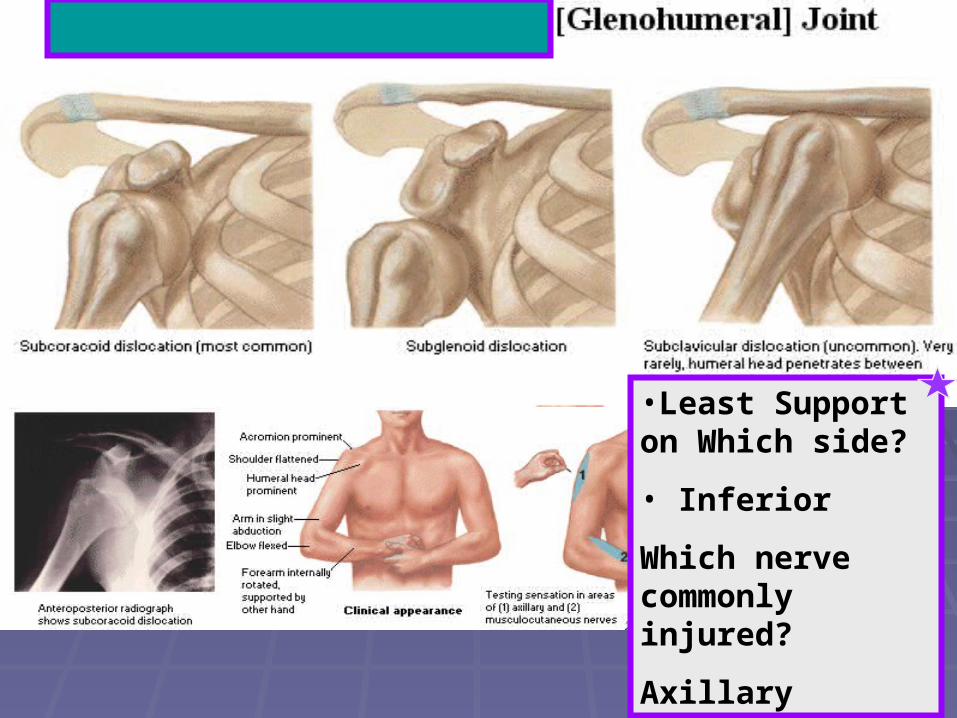
•Least Support on Which side?
• Inferior
Which nerve commonly injured?
Axillary
7878
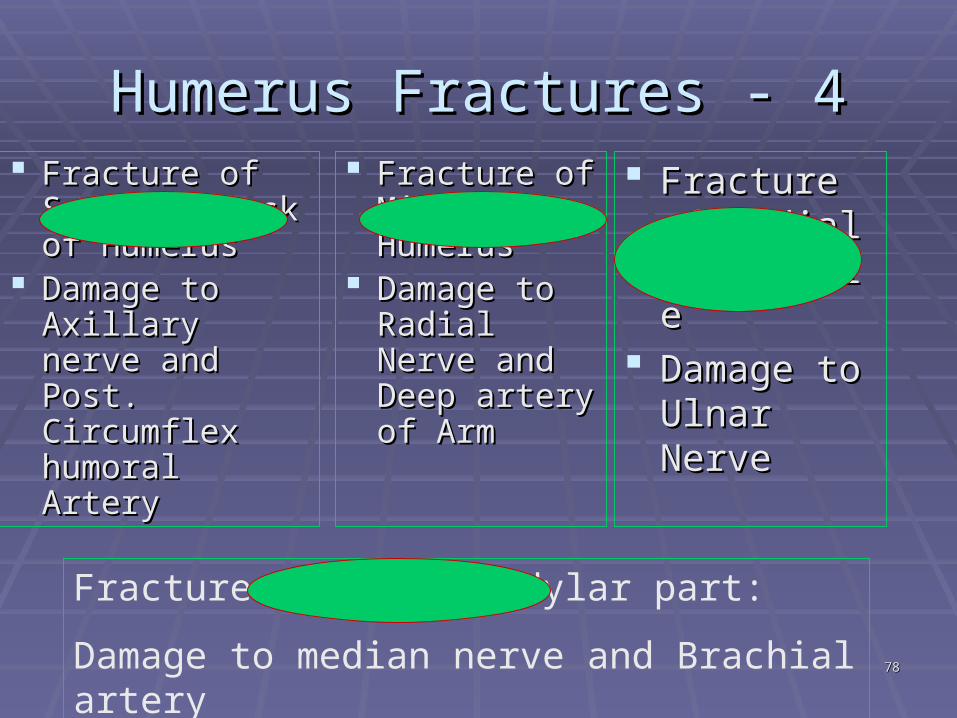
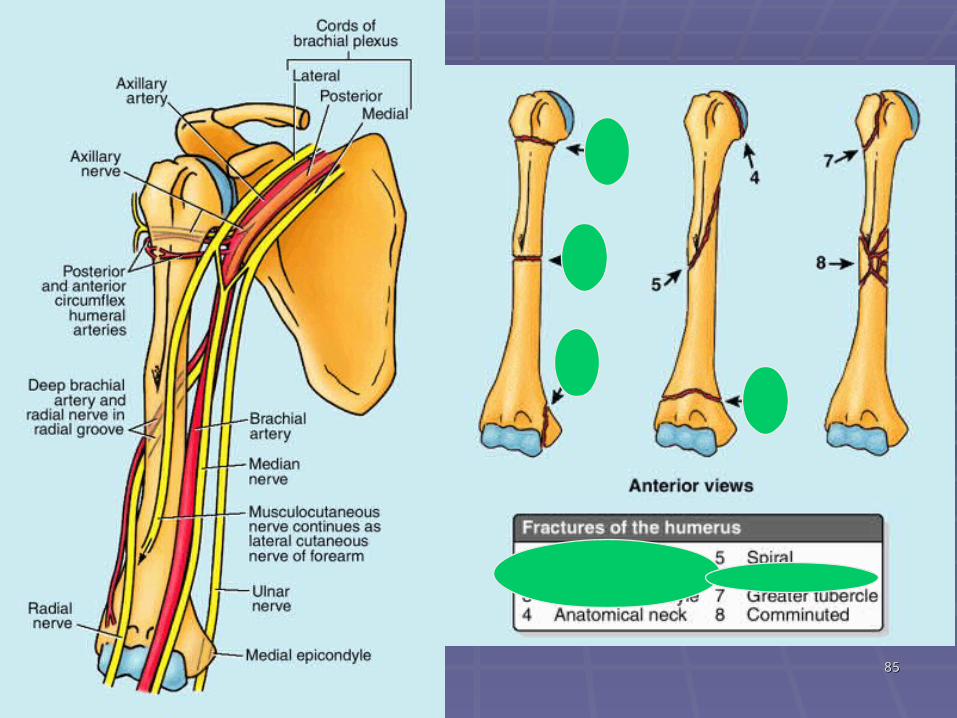
Humerus Fractures - 4Humerus Fractures - 4 Fracture of Fracture of
Surgical Neck Surgical Neck of Humerusof Humerus
Damage to Damage to Axillary nerve Axillary nerve and Post. and Post. Circumflex Circumflex humoral Arteryhumoral Artery
Fracture of Fracture of Mid Shaft Mid Shaft HumerusHumerus
Damage to Damage to Radial Nerve Radial Nerve and Deep and Deep artery of Armartery of Arm
Fracture of Fracture of Medial Medial EpicondyleEpicondyle
Damage to Damage to Ulnar NerveUlnar Nerve
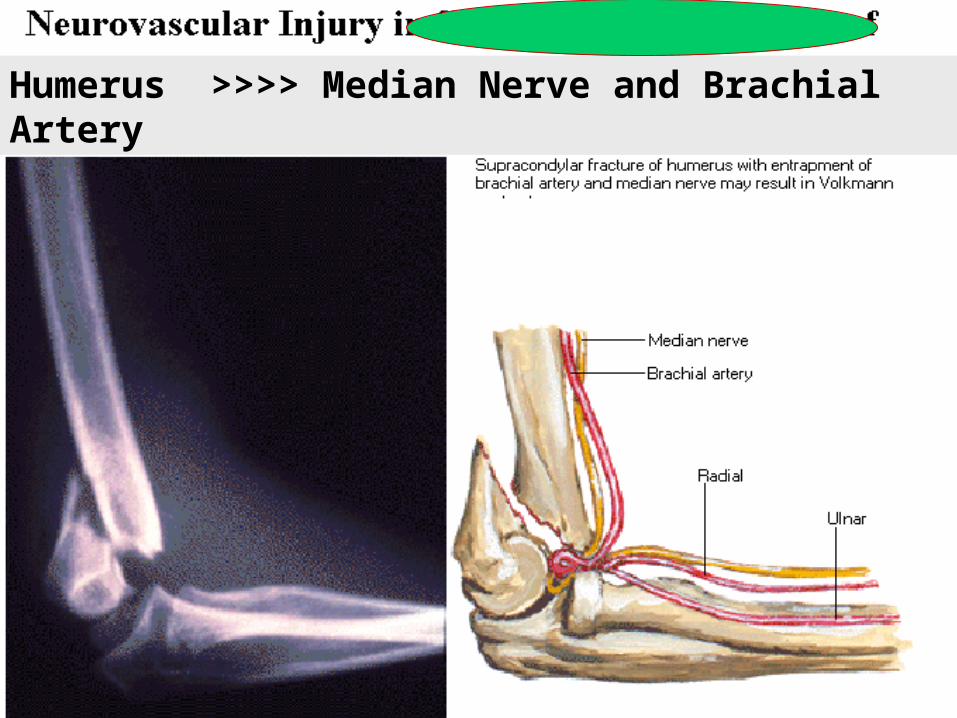
Fracture of Supracondylar part:
Damage to median nerve and Brachial artery
7979
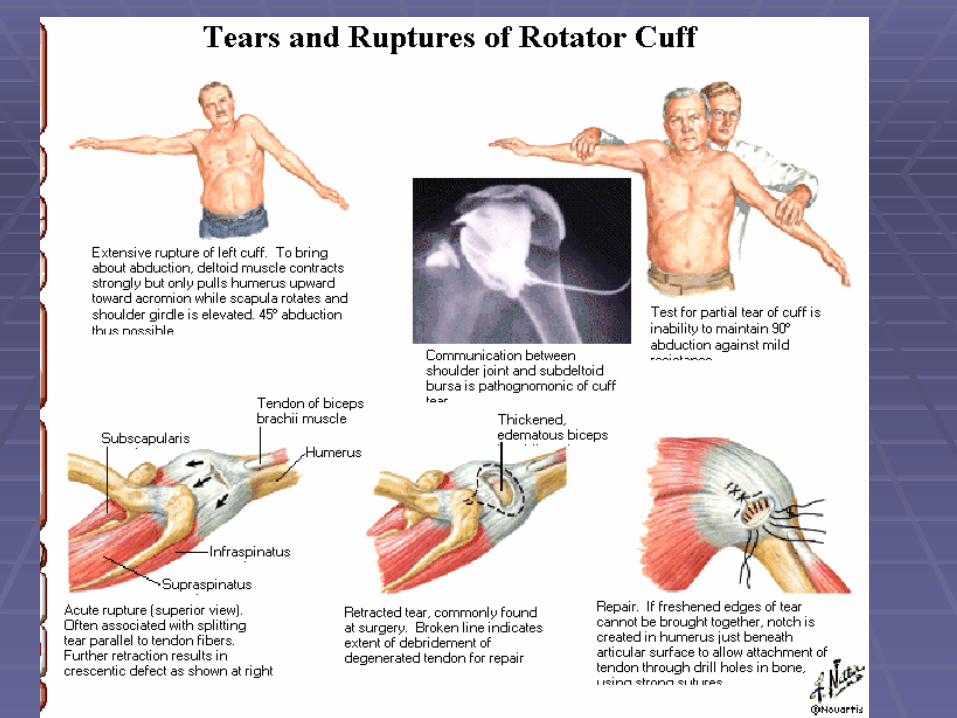
Rotator Cuff InjuriesRotator Cuff Injuries Introduction:Introduction: commonly injured during repetitive use of the upper commonly injured during repetitive use of the upper
limb above the horizontal (e.g., during throwing and limb above the horizontal (e.g., during throwing and racquet sports, swimming, and weight lifting, baseball racquet sports, swimming, and weight lifting, baseball pitchers).pitchers).
Leads to Shoulder pain. Leads to Shoulder pain. Repetitive use of the rotator cuff muscles may allow Repetitive use of the rotator cuff muscles may allow
the humeral head and rotator cuff to impinge on the the humeral head and rotator cuff to impinge on the coracoacromial arch, producing irritation of the arch coracoacromial arch, producing irritation of the arch and inflammation of the rotator cuff. and inflammation of the rotator cuff.
Recurrent inflammation may lead to degenerative Recurrent inflammation may lead to degenerative tendinitis of rotator cuff. Especially the relatively tendinitis of rotator cuff. Especially the relatively avascular area of the supraspinatus tendon is avascular area of the supraspinatus tendon is affected. affected.
8080
Continue…Continue…Rotator Cuff InjuriesRotator Cuff Injuries
Tear of the supraspinatusTear of the supraspinatus difficulty in initiation of abduction of difficulty in initiation of abduction of
the upper limb. the upper limb. If the arm is passively abducted 15° or If the arm is passively abducted 15° or
more, the person can usually maintain more, the person can usually maintain or continue the abduction using the or continue the abduction using the deltoid.deltoid.
But there is also Difficulty in But there is also Difficulty in maintaining abduction against maintaining abduction against resistanceresistance
Continue… Continue… Rotator cuff injuryRotator cuff injury
If there is rupture of If there is rupture of SubscapularisSubscapularis Weakness of medial rotation (its action)Weakness of medial rotation (its action) More pain on lateral rotation (stretching of More pain on lateral rotation (stretching of
ruptured subscapularis)ruptured subscapularis) If there is rupture of If there is rupture of infraspinatus or teres infraspinatus or teres
minorminor Weakness of lateral rotation (their action)Weakness of lateral rotation (their action) More pain on medial rotation (stretching of More pain on medial rotation (stretching of
ruptured tendons)ruptured tendons)8282
8383
Calcific Supraspinatus TendinitisCalcific Supraspinatus Tendinitis[leads to subacromial bursitis][leads to subacromial bursitis]
Subacromial Bursitis = Deposition of calcium in the Subacromial Bursitis = Deposition of calcium in the supraspinatus tendon may irritate the overlying subacromial supraspinatus tendon may irritate the overlying subacromial bursa, producing an inflammatory reaction.bursa, producing an inflammatory reaction.
result in pain, tenderness, and limitation of movement of the result in pain, tenderness, and limitation of movement of the glenohumeral joint. glenohumeral joint.
As long as the glenohumeral joint is adducted, no pain usually As long as the glenohumeral joint is adducted, no pain usually results because in this position the painful lesion is away from results because in this position the painful lesion is away from the inferior surface of the acromion. the inferior surface of the acromion.
In most people, the pain occurs during 50–130° of abduction In most people, the pain occurs during 50–130° of abduction ((Painful Arc SyndromePainful Arc Syndrome) because during this arc the ) because during this arc the supraspinatus tendon is in intimate contact with the inferior supraspinatus tendon is in intimate contact with the inferior surface of the acromion. surface of the acromion.
The pain usually develops in males 50 years of age and older The pain usually develops in males 50 years of age and older after unusual or excessive use of the glenohumeral joint.after unusual or excessive use of the glenohumeral joint.
8484
Adhesive Capsulitis of the Adhesive Capsulitis of the Glenohumeral JointGlenohumeral Joint
Adhesive fibrosis and scarring between the Adhesive fibrosis and scarring between the inflamed capsule of the glenohumeral joint, inflamed capsule of the glenohumeral joint, rotator cuff, subacromial bursa, and deltoid rotator cuff, subacromial bursa, and deltoid usually cause (“frozen shoulder”). usually cause (“frozen shoulder”).
A person with this condition has difficulty A person with this condition has difficulty abducting the arm but can obtain an apparent abducting the arm but can obtain an apparent abduction of up to 45° by elevating and rotating abduction of up to 45° by elevating and rotating the scapula. the scapula.
Injuries that may initiate this condition include Injuries that may initiate this condition include glenohumeral dislocations, calcific glenohumeral dislocations, calcific supraspinatus tendonitis, partial tearing of the supraspinatus tendonitis, partial tearing of the rotator cuff, and bicipital tendonitisrotator cuff, and bicipital tendonitis
8585
8686
Humerus >>>> Median Nerve and Brachial Artery
8787
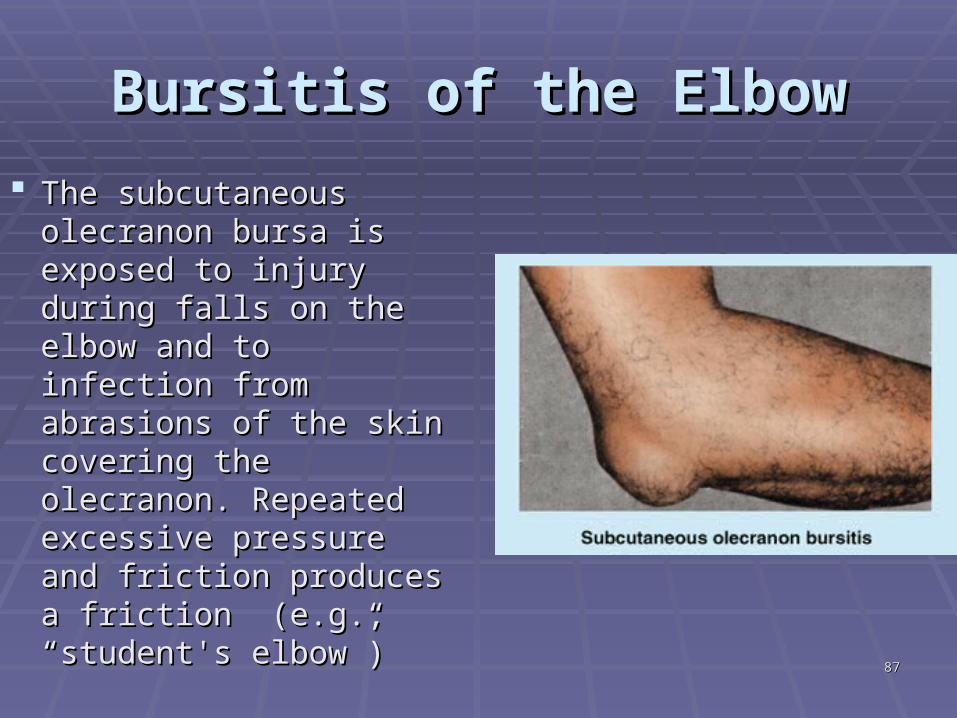
Bursitis of the ElbowBursitis of the Elbow The subcutaneous The subcutaneous
olecranon bursa is olecranon bursa is exposed to injury during exposed to injury during falls on the elbow and to falls on the elbow and to infection from abrasions infection from abrasions of the skin covering the of the skin covering the olecranon. Repeated olecranon. Repeated excessive pressure and excessive pressure and friction produces a friction produces a friction (e.g., “student's friction (e.g., “student's elbow”)elbow”)
8888
Avulsion of Medial EpicondyleAvulsion of Medial Epicondyle
Avulsion of the medial epicondyle in children can Avulsion of the medial epicondyle in children can result from a fall that causes severe abduction of the result from a fall that causes severe abduction of the extended elbow. extended elbow.
The resulting traction on the ulnar collateral ligament The resulting traction on the ulnar collateral ligament pulls the medial epicondyle distally. pulls the medial epicondyle distally.
The anatomical basis of avulsion of the medial The anatomical basis of avulsion of the medial epicondyle is that the epiphysis for the medial epicondyle is that the epiphysis for the medial epicondyle may not fuse with the distal end of the epicondyle may not fuse with the distal end of the humerus until up to age 20. humerus until up to age 20.
Injury to the ULNAR nerve, is a complication of the Injury to the ULNAR nerve, is a complication of the abduction type of avulsion of the medial epicondyle.abduction type of avulsion of the medial epicondyle.
8989
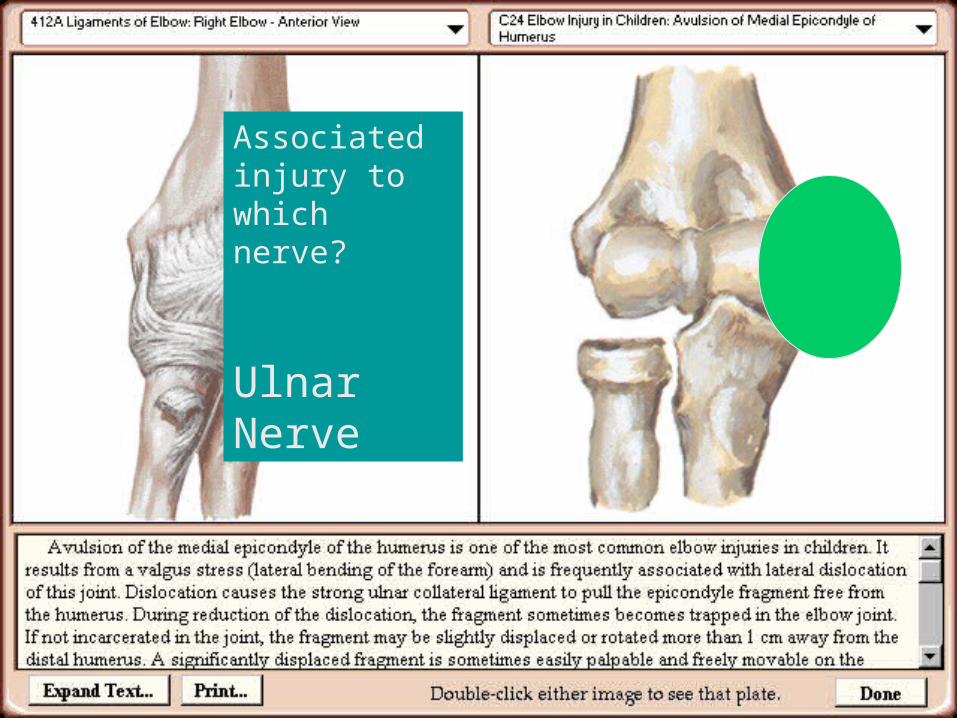
Associated injury to which nerve?
Ulnar Nerve
9090
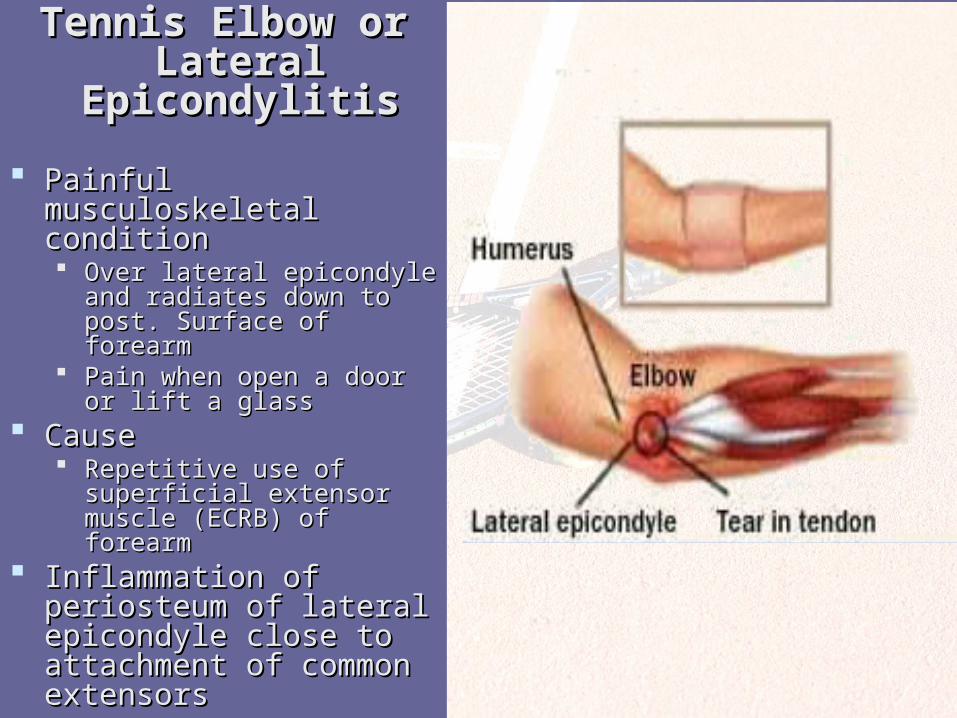
Tennis Elbow or Tennis Elbow or Lateral Lateral
EpicondylitisEpicondylitis Painful musculoskeletal Painful musculoskeletal
conditioncondition Over lateral epicondyle and Over lateral epicondyle and
radiates down to post. radiates down to post. Surface of forearmSurface of forearm
Pain when open a door or lift Pain when open a door or lift a glassa glass
CauseCause Repetitive use of superficial Repetitive use of superficial
extensor muscle (ECRB) of extensor muscle (ECRB) of forearm forearm
Inflammation of periosteum Inflammation of periosteum of lateral epicondyle close of lateral epicondyle close to attachment of common to attachment of common extensorsextensors
9191
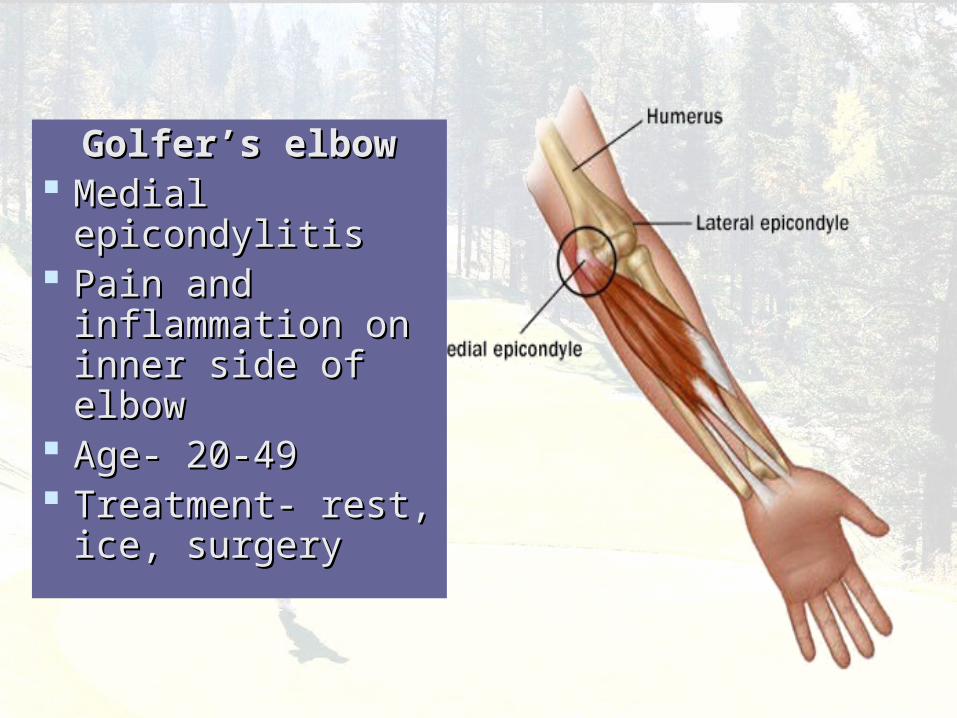
Golfer’s elbowGolfer’s elbow Medial Medial
epicondylitis epicondylitis Pain and Pain and
inflammation on inflammation on inner side of elbowinner side of elbow
Age- 20-49Age- 20-49 Treatment- rest, Treatment- rest,
ice, surgeryice, surgery
9292
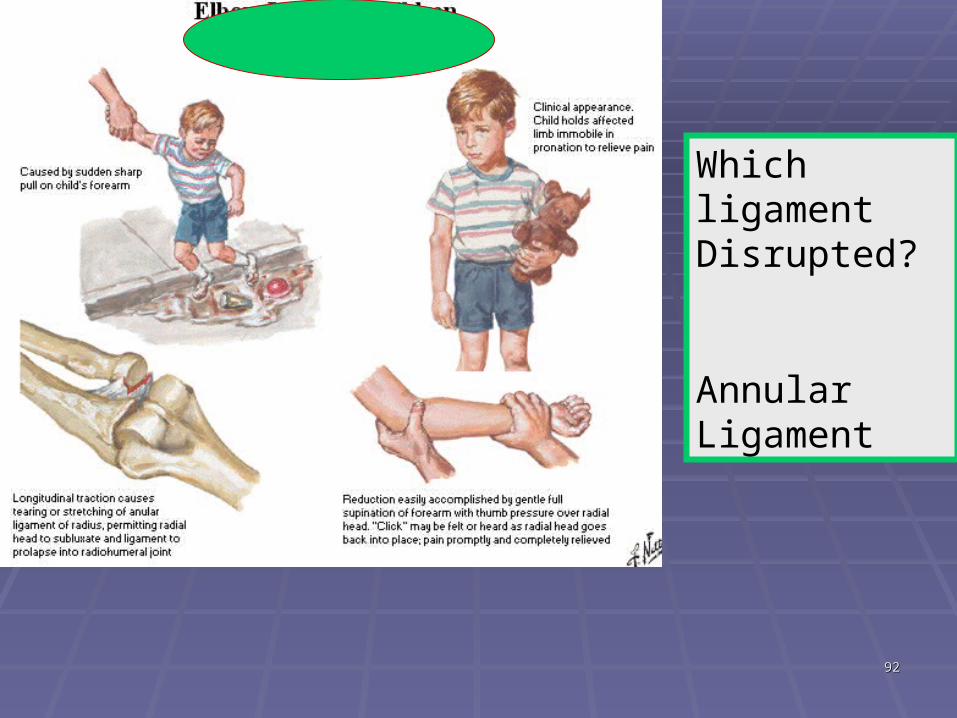
Which ligament Disrupted?
Annular Ligament
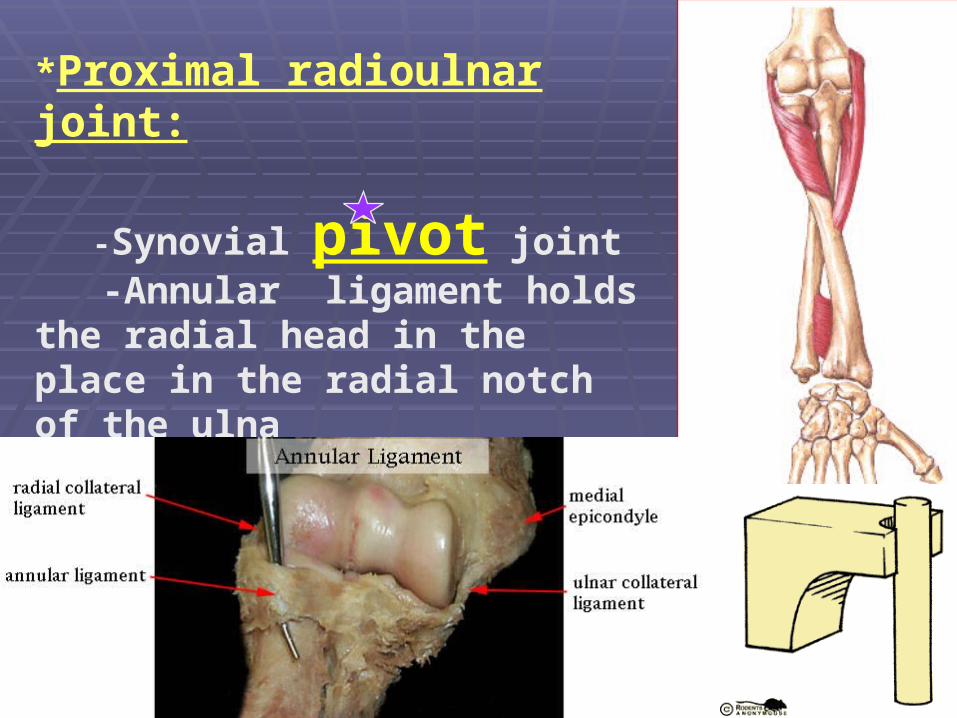
*Proximal radioulnar joint:
-Synovial pivot joint -Annular ligament holds the radial head in the place in the radial notch of the ulna
9494
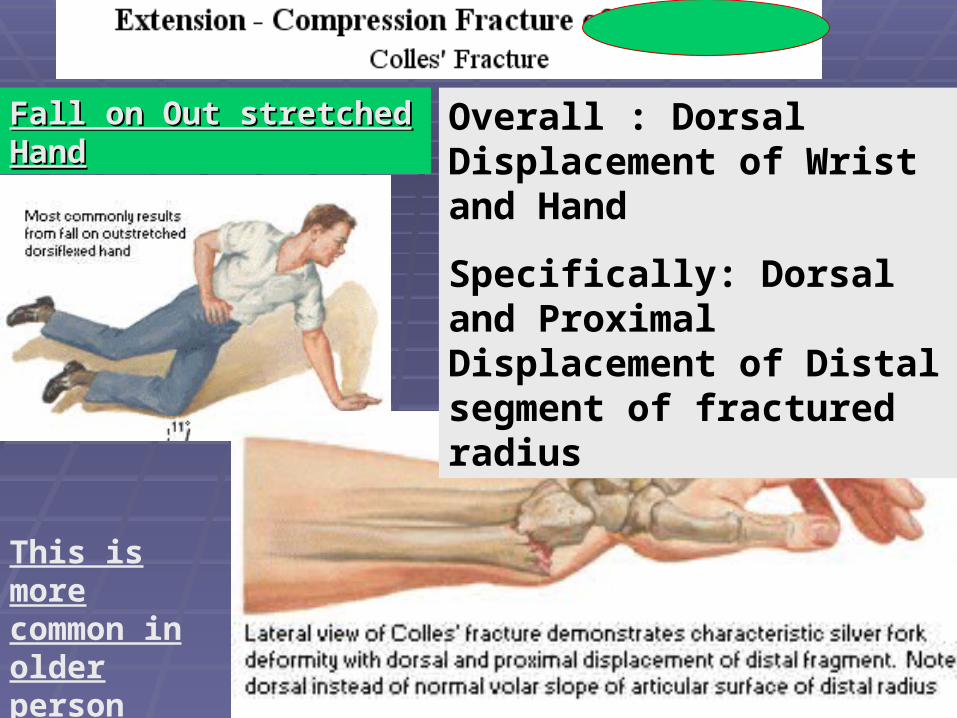
Overall : Dorsal Displacement of Wrist and Hand
Specifically: Dorsal and Proximal Displacement of Distal segment of fractured radius
Fall on Out stretched HandFall on Out stretched Hand
This is more common in older person
9595
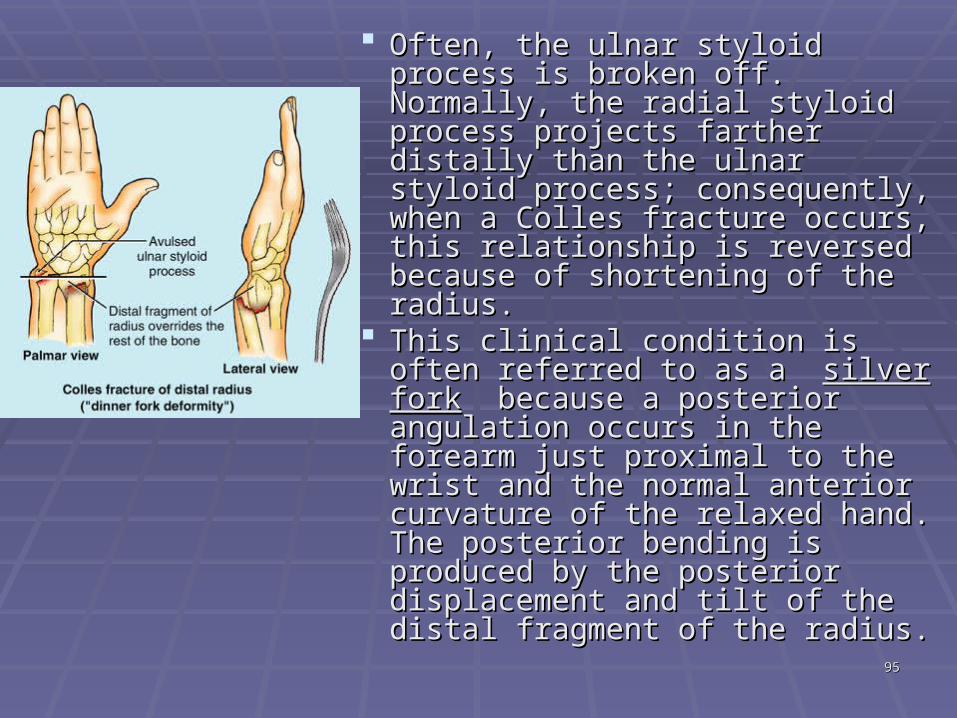
Often, the ulnar styloid process is Often, the ulnar styloid process is broken off. Normally, the radial broken off. Normally, the radial styloid process projects farther styloid process projects farther distally than the ulnar styloid distally than the ulnar styloid process; consequently, when a process; consequently, when a Colles fracture occurs, this Colles fracture occurs, this relationship is reversed because relationship is reversed because of shortening of the radius. of shortening of the radius.
This clinical condition is often This clinical condition is often referred to as a referred to as a silver forksilver fork because a posterior angulation because a posterior angulation occurs in the forearm just occurs in the forearm just proximal to the wrist and the proximal to the wrist and the normal anterior curvature of the normal anterior curvature of the relaxed hand. The posterior relaxed hand. The posterior bending is produced by the bending is produced by the posterior displacement and tilt of posterior displacement and tilt of the distal fragment of the radius. the distal fragment of the radius.
9696
Smith’s Fracture•Occurs from a fall on the back of the hand•Fracture of the distal end of the radius•Distal fragment is displaced anteriorly
9797
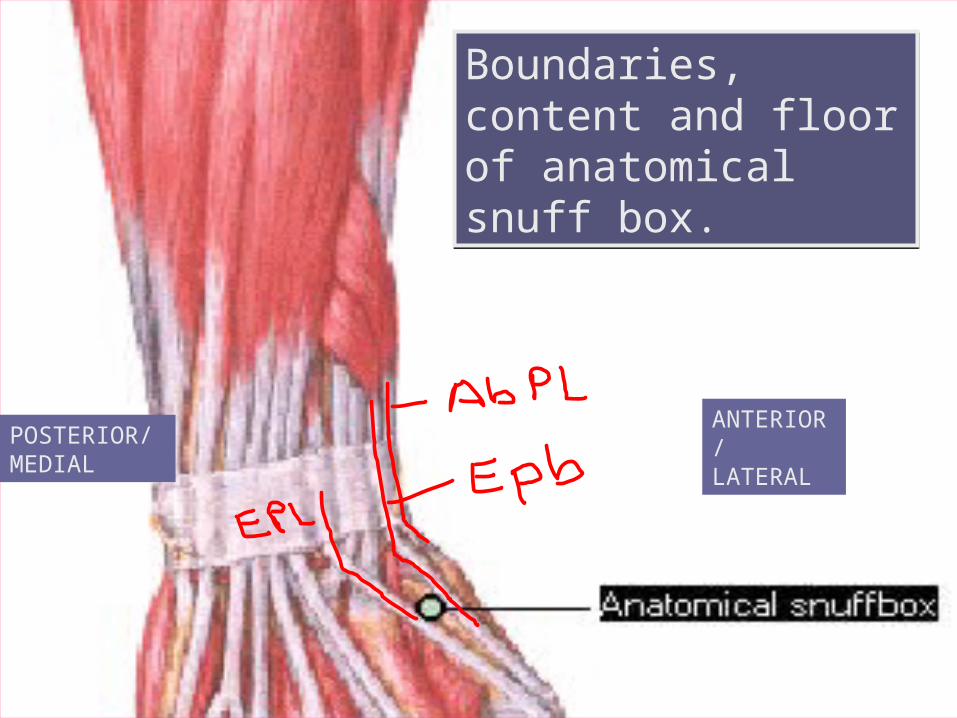
POSTERIOR/ MEDIAL
ANTERIOR/ LATERAL
Boundaries, content and floor of anatomical snuff box.
9898
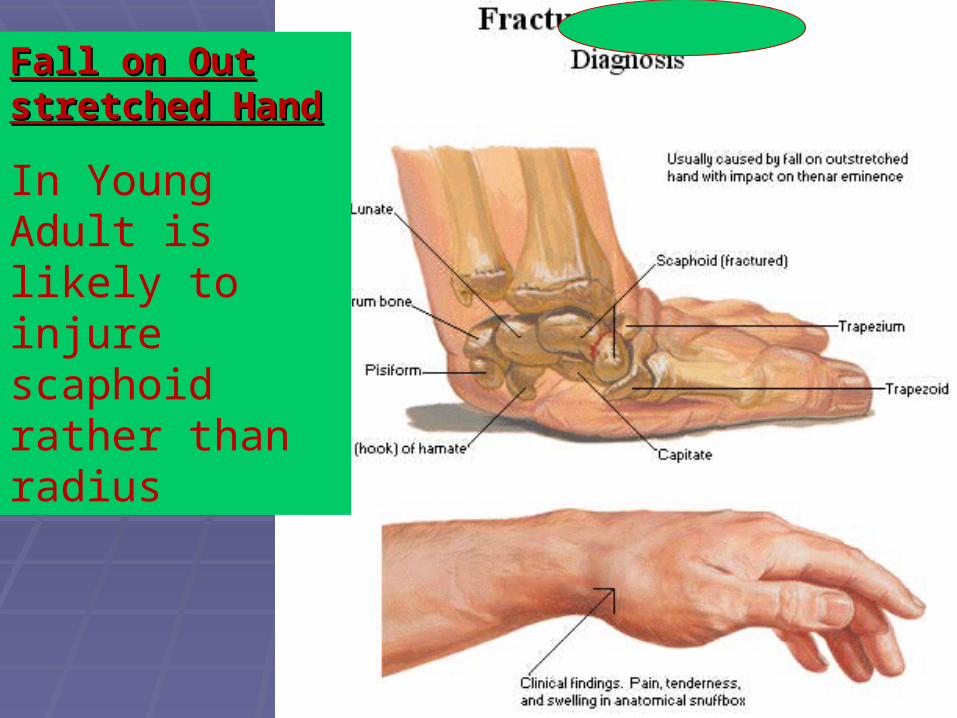
Fall on Out Fall on Out stretched Handstretched Hand
In Young Adult is likely to injure scaphoid rather than radius
9999
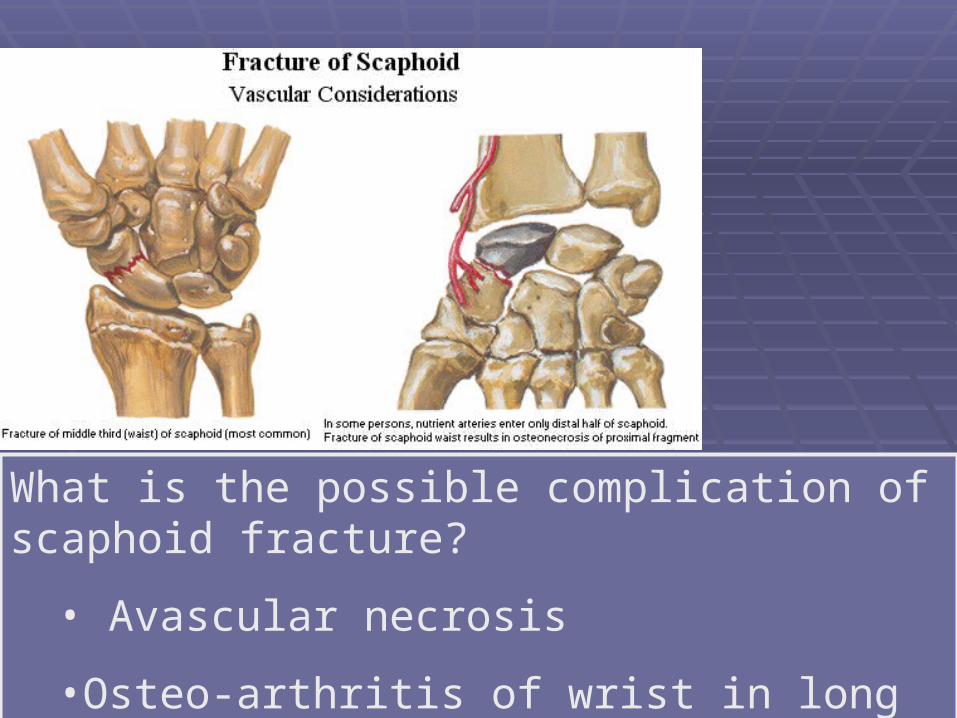
What is the possible complication of scaphoid fracture?
• Avascular necrosis
•Osteo-arthritis of wrist in long term
100100
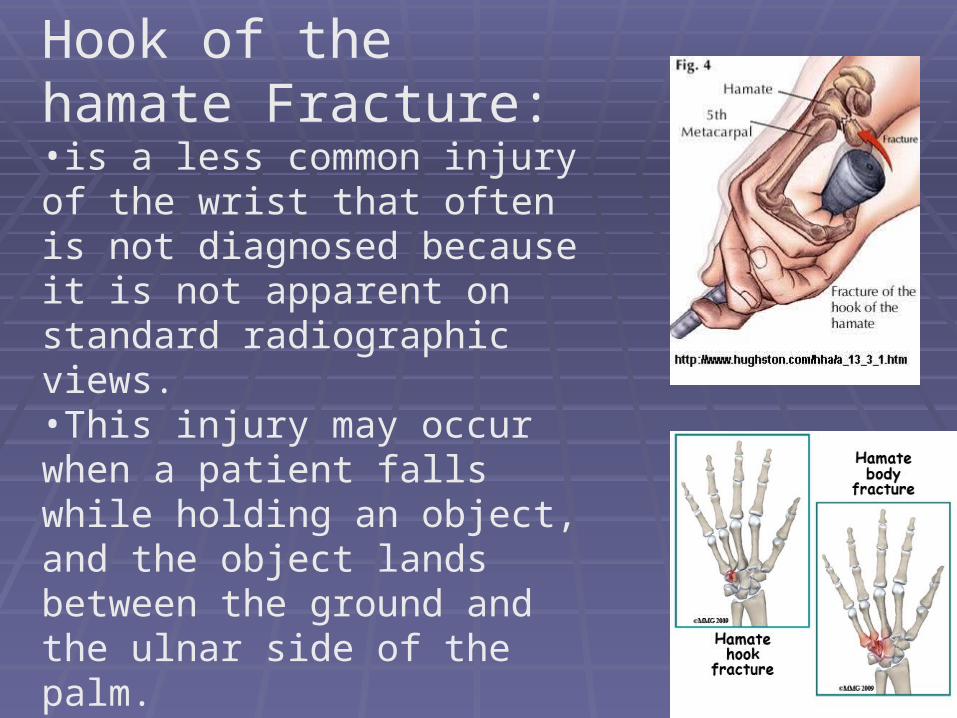
Hook of the hamate Fracture:•is a less common injury of the wrist that often is not diagnosed because it is not apparent on standard radiographic views. •This injury may occur when a patient falls while holding an object, and the object lands between the ground and the ulnar side of the palm. •It also may be caused when a bat hits a ball or a golf club catches the ground, and the hypothenar eminence is struck.
101101
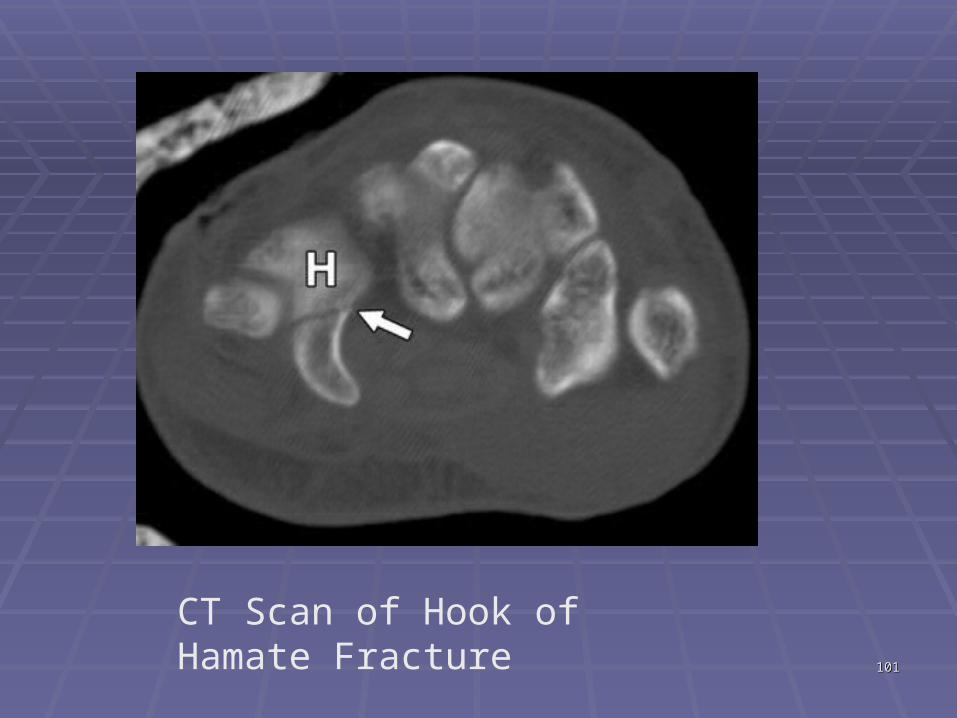
CT Scan of Hook of Hamate Fracture
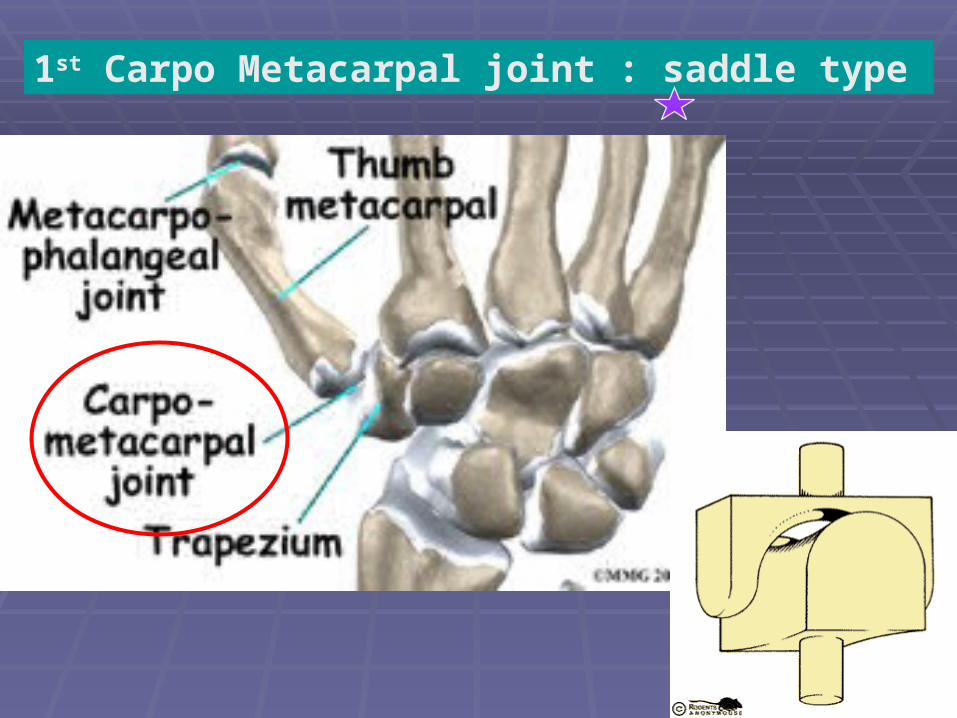
1st Carpo Metacarpal joint : saddle type
103103
Skier's ThumbSkier's Thumb
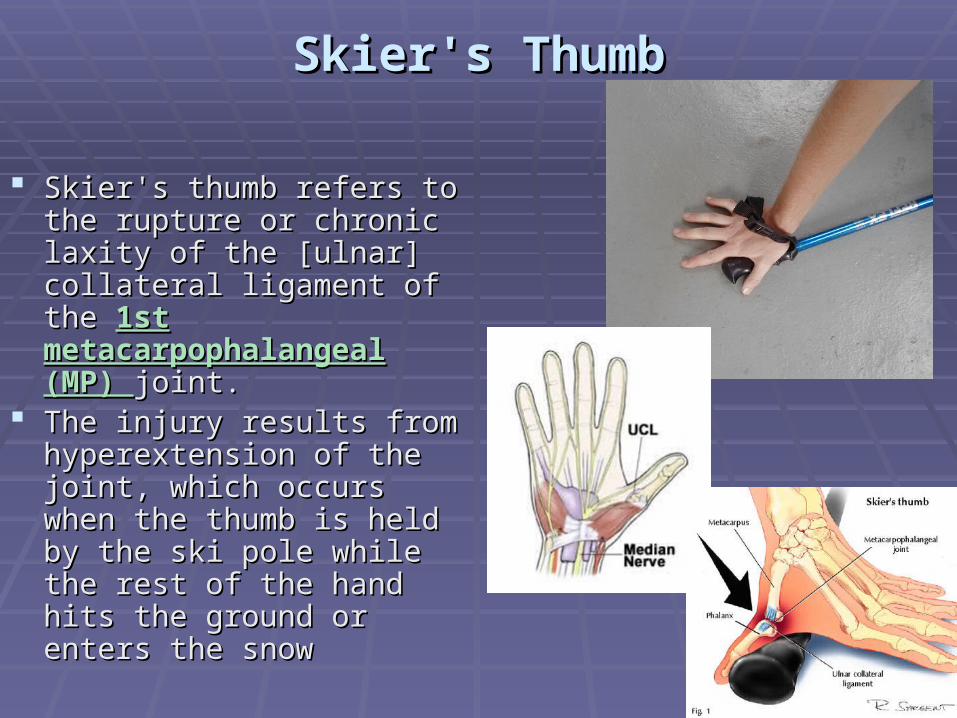
Skier's thumb refers to the Skier's thumb refers to the rupture or chronic laxity of rupture or chronic laxity of the [ulnar] collateral ligament the [ulnar] collateral ligament of the of the 1st 1st metacarpophalangeal (MP) metacarpophalangeal (MP) joint. joint.
The injury results from The injury results from hyperextension of the joint, hyperextension of the joint, which occurs when the which occurs when the thumb is held by the ski pole thumb is held by the ski pole while the rest of the hand hits while the rest of the hand hits the ground or enters the the ground or enters the snowsnow
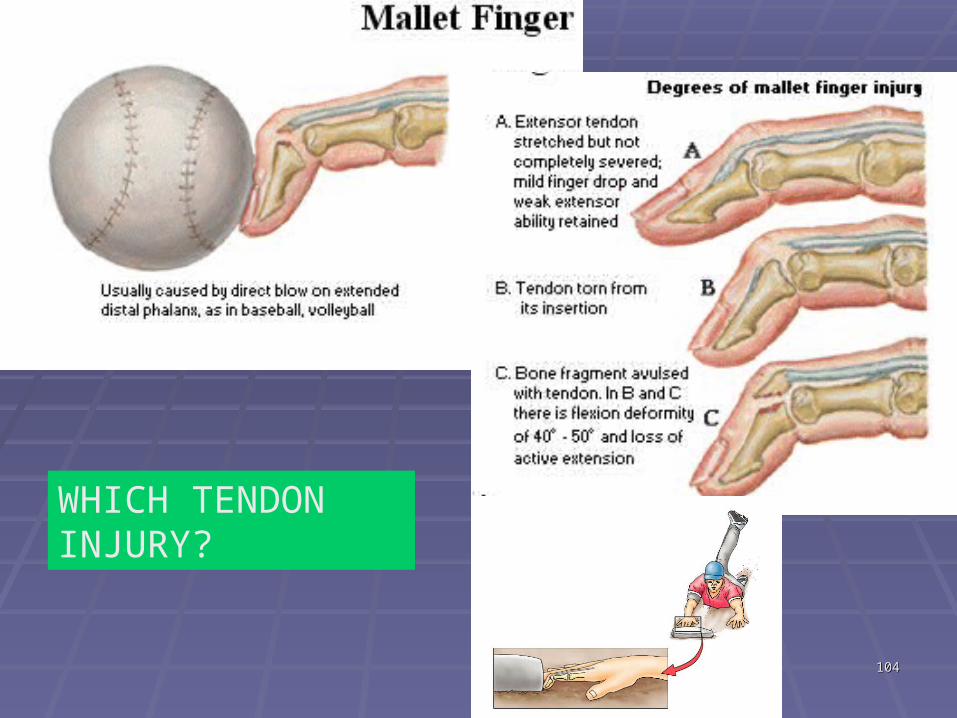
104104
WHICH TENDON INJURY?
105105
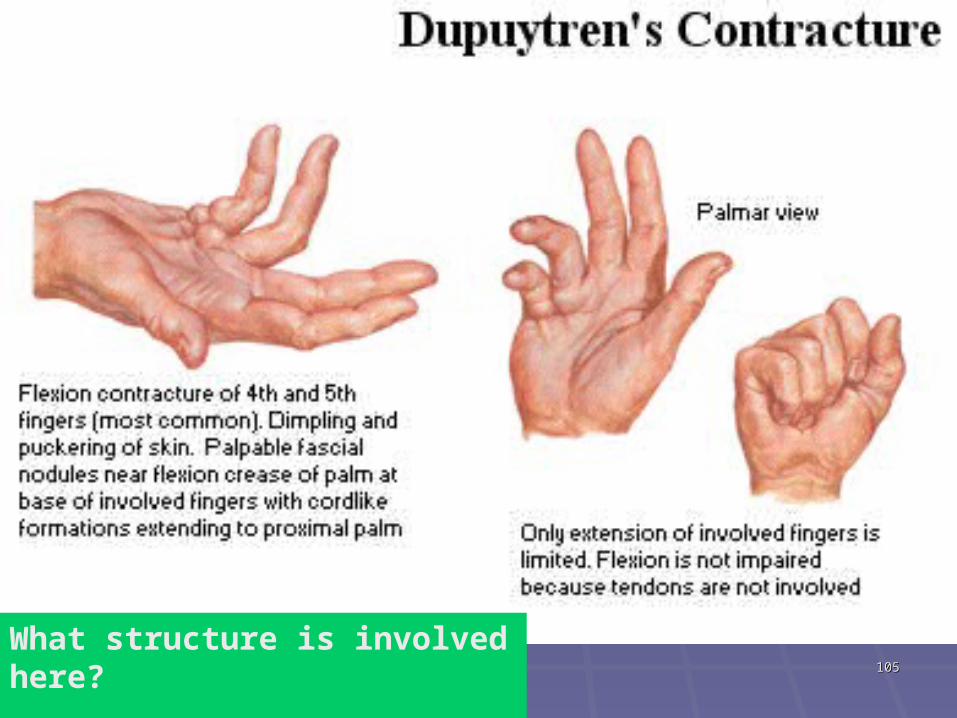
What structure is involved here?
Palmar Apponeurosis
106106
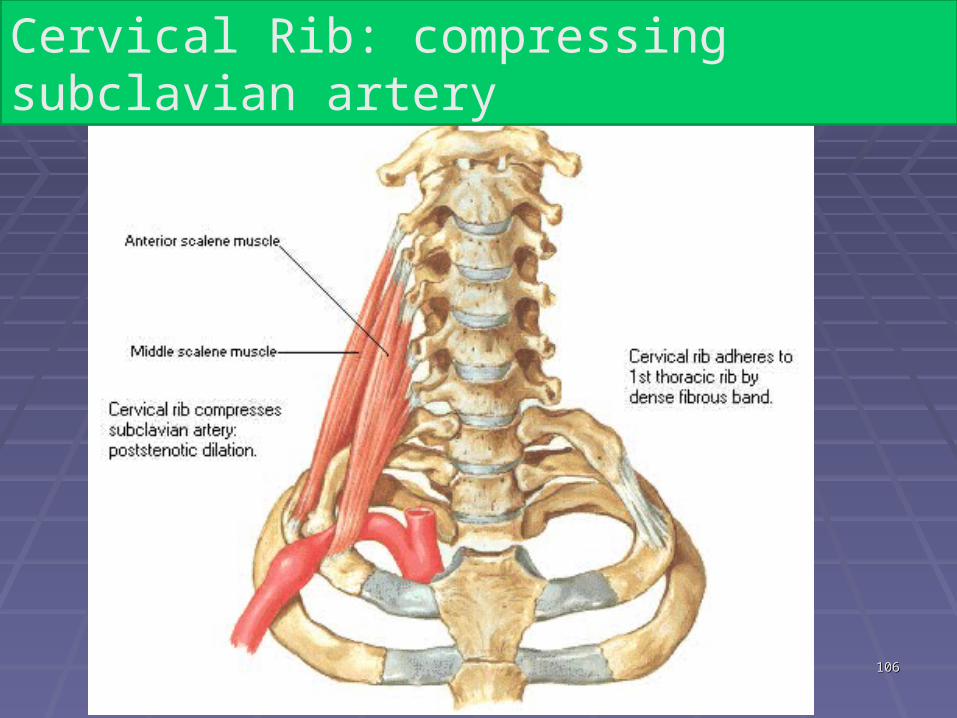
Cervical Rib: compressing subclavian artery
107107
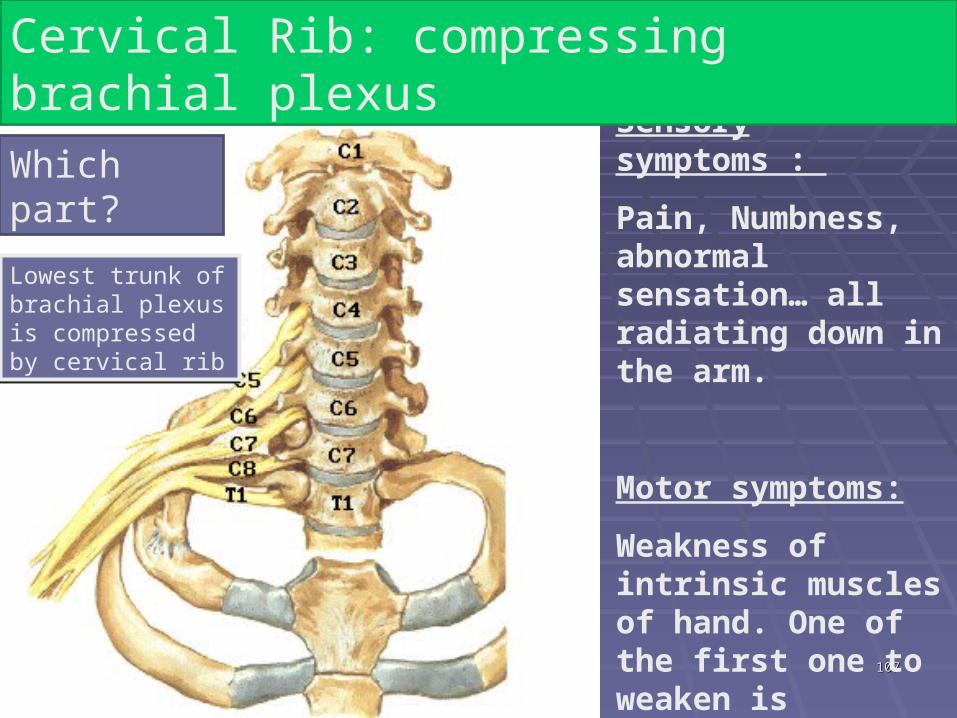
Sensory symptoms :
Pain, Numbness, abnormal sensation… all radiating down in the arm.
Motor symptoms:
Weakness of intrinsic muscles of hand. One of the first one to weaken is Abductor Digiti minimi
Cervical Rib: compressing brachial plexus
Which part?
Lowest trunk of brachial plexus is compressed by cervical rib
108108
109109
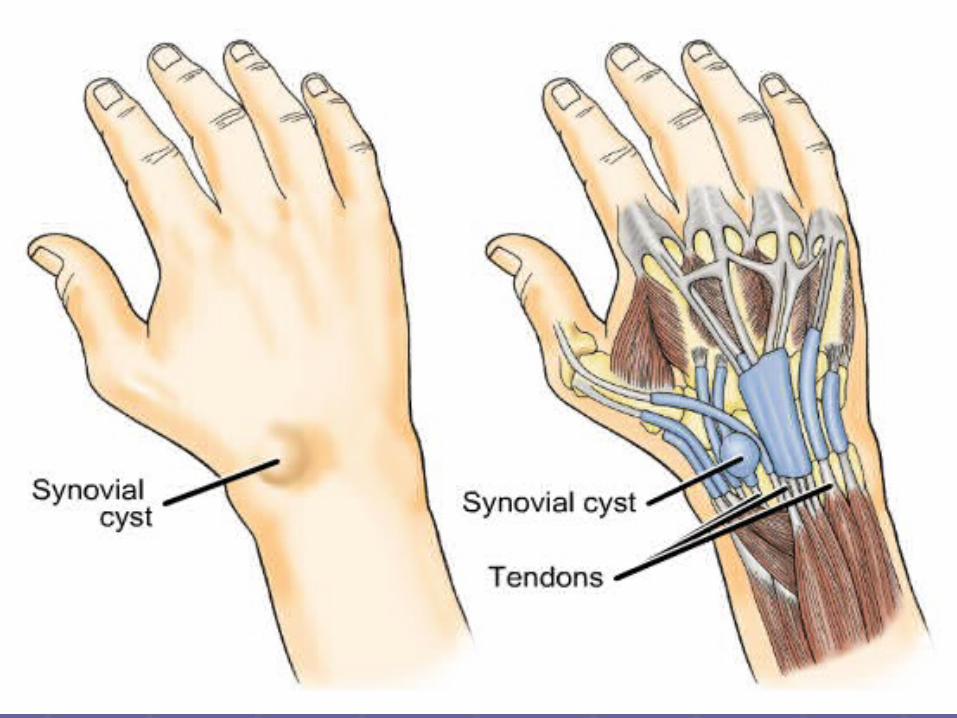
Synovial Cyst of WristSynovial Cyst of Wrist Ganglion Ganglion (misnomer)(misnomer)
Non-tender, cystic swelling Non-tender, cystic swelling Common site- Distal attachment of ECRB Common site- Distal attachment of ECRB
tendon (at dorsum of wrist) tendon (at dorsum of wrist) Thin-walled, and contains clear mucinous Thin-walled, and contains clear mucinous
fluidfluid Often communicate with synovial sheathsOften communicate with synovial sheaths Can compress median nerve by Can compress median nerve by
narrowing the carpal tunnel if it is devlops narrowing the carpal tunnel if it is devlops in flexor tendonin flexor tendon
110110
111111
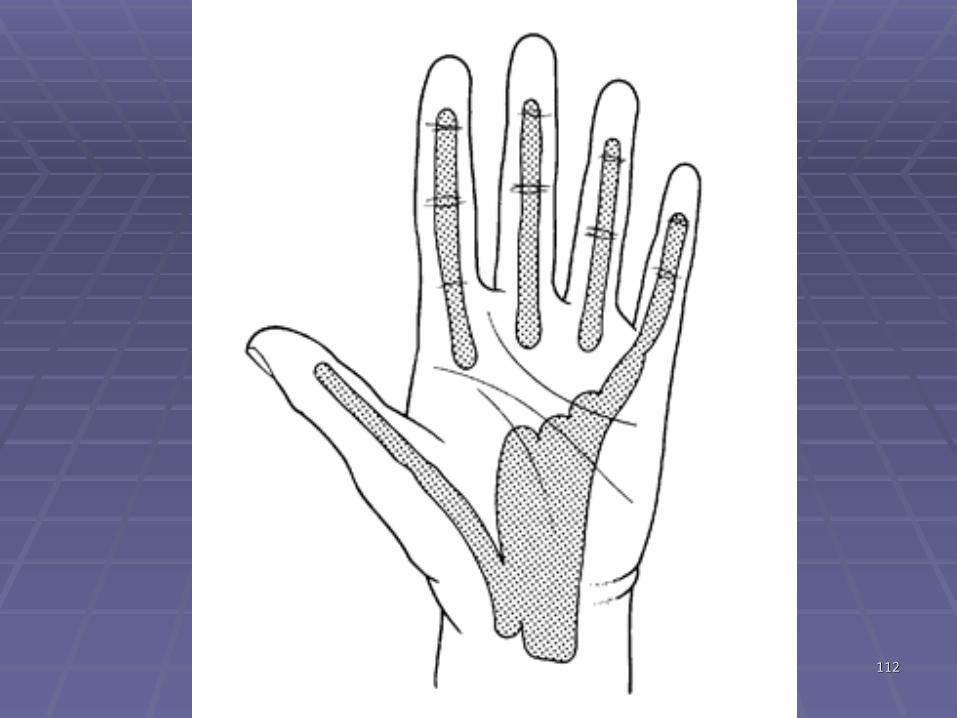
Hand InfectionsHand Infections Swellings appear on dorsum of hand where Swellings appear on dorsum of hand where
fascia is thinner fascia is thinner Potential fascial spaces of palm may become Potential fascial spaces of palm may become
infectedinfected Spread- Depending on site of infection, pus will Spread- Depending on site of infection, pus will
accumulate in thenar, hypothenar, or adductor accumulate in thenar, hypothenar, or adductor compartmentscompartments
Infection of the tendon sheaths of thumb or little Infection of the tendon sheaths of thumb or little finger may spread to radial or ulnar bursa, finger may spread to radial or ulnar bursa, respectively respectively
Treatment- Antibiotic, I & DTreatment- Antibiotic, I & D
112112
113113
TenosynovitisTenosynovitis Inflammation of tendon and synovial sheathInflammation of tendon and synovial sheath S/S- pain, swelling, and difficulty moving particular jointS/S- pain, swelling, and difficulty moving particular joint Cause- Cause-
Puncture of a finger by a rusty nail Puncture of a finger by a rusty nail Tendons of 2nd–4th digits have separate synovial Tendons of 2nd–4th digits have separate synovial
sheaths, infection usually is confined to infected digitsheaths, infection usually is confined to infected digit If infection is untreated, proximal ends of sheaths may ruptureIf infection is untreated, proximal ends of sheaths may rupture
Infection spread to midpalmar space Infection spread to midpalmar space Tenosynovitis of 5Tenosynovitis of 5thth finger spread to common sheath and finger spread to common sheath and
thus through palm and carpal tunnel to anterior forearmthus through palm and carpal tunnel to anterior forearm Tenosynovitis of thumb may spread through continuous Tenosynovitis of thumb may spread through continuous
synovial sheath of FPL (radial bursa)synovial sheath of FPL (radial bursa)
114114
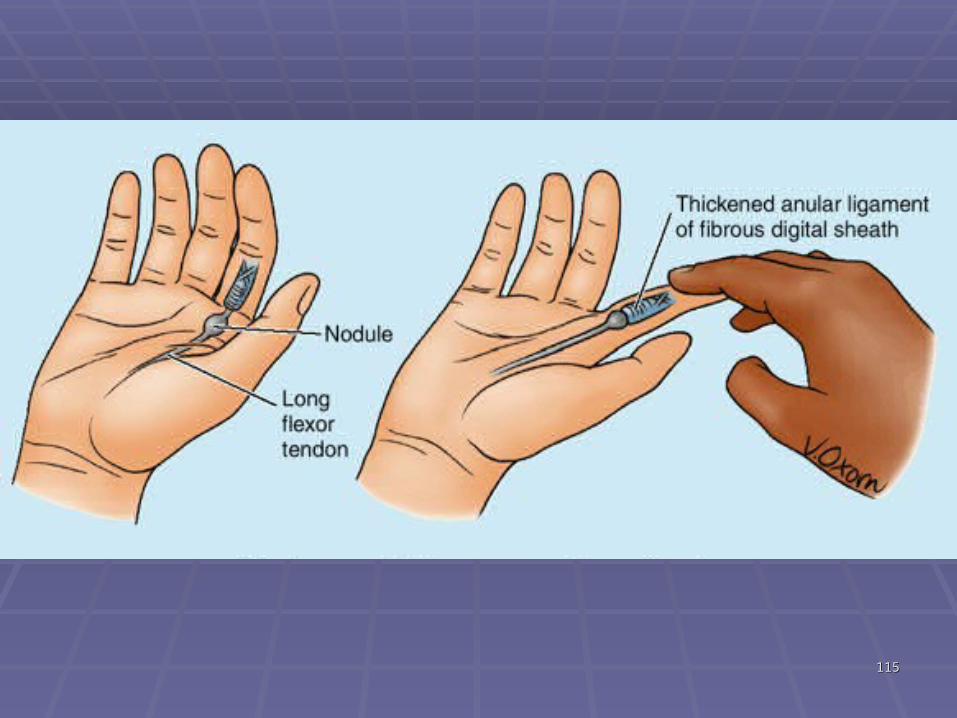
Trigger finger or Snapping fingerTrigger finger or Snapping finger
Excessive friction of tendon results in Excessive friction of tendon results in fibrous thickening of sheath and stenosis fibrous thickening of sheath and stenosis of osseofibrous tunnelof osseofibrous tunnel
S/S- pain in wrist that radiates proximally S/S- pain in wrist that radiates proximally to forearm and distally to thumb/fingersto forearm and distally to thumb/fingers
Snap is audible when finger is extended or Snap is audible when finger is extended or flexedflexed Called trigger finger or snapping fingerCalled trigger finger or snapping finger
115115
1
2
3
4
5 6
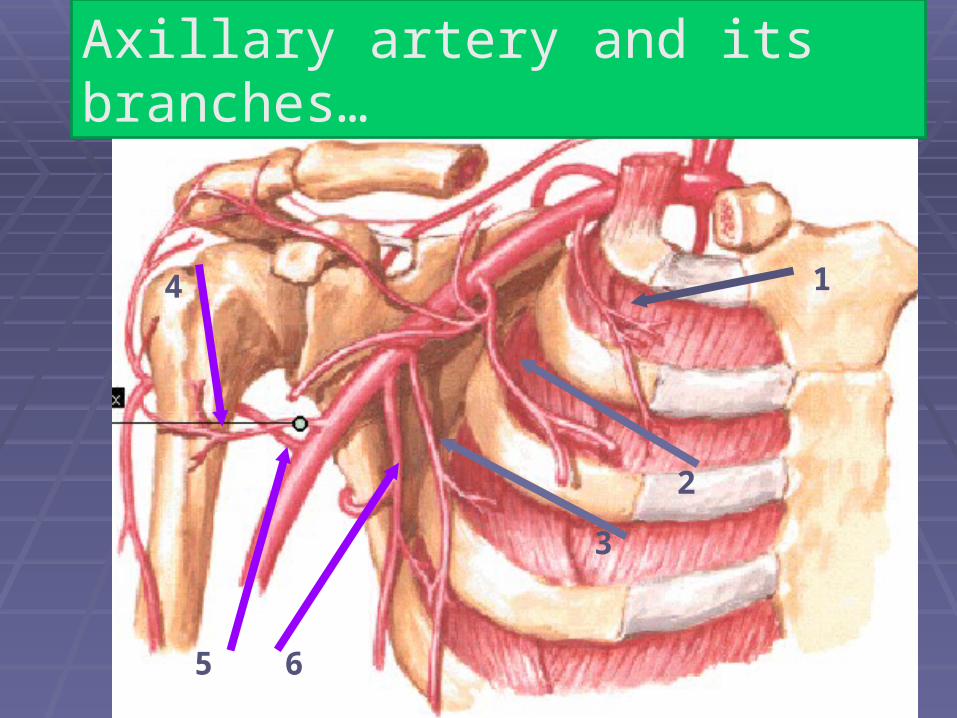
Axillary artery and its branches…
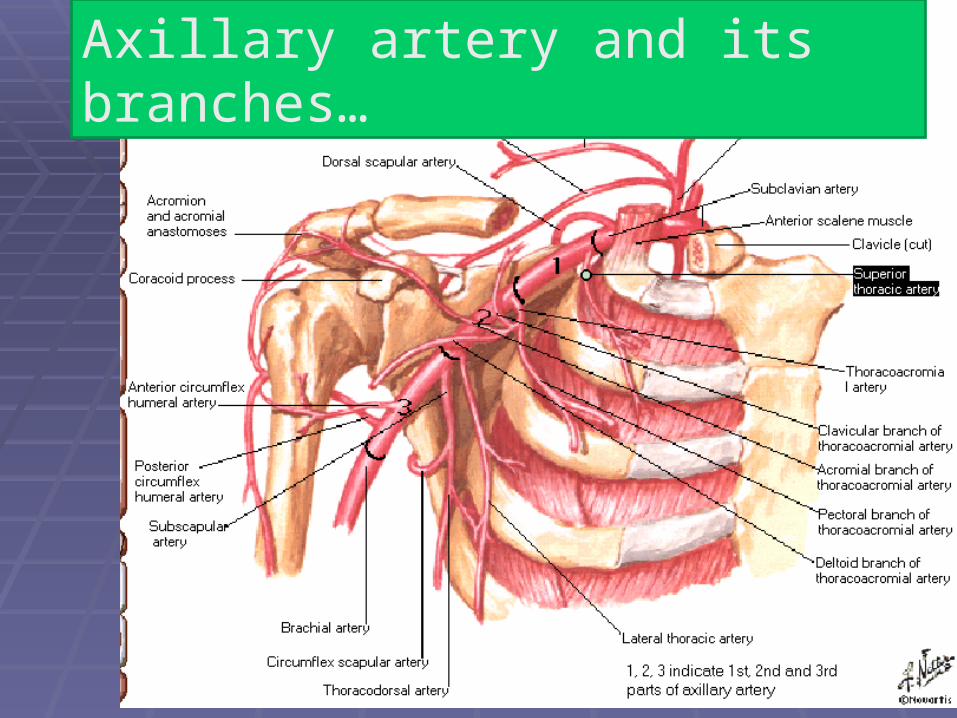
Axillary artery and its branches…
# Scapular Anastomoses:This anastomosis is between branches of subclavianArtery and branches of 3rd part of Axillary artery.
Branches of subclavian – suprascapular and Dorsal scapular
Branches of Axillary – Subscapular : its circumflex scapular branch.
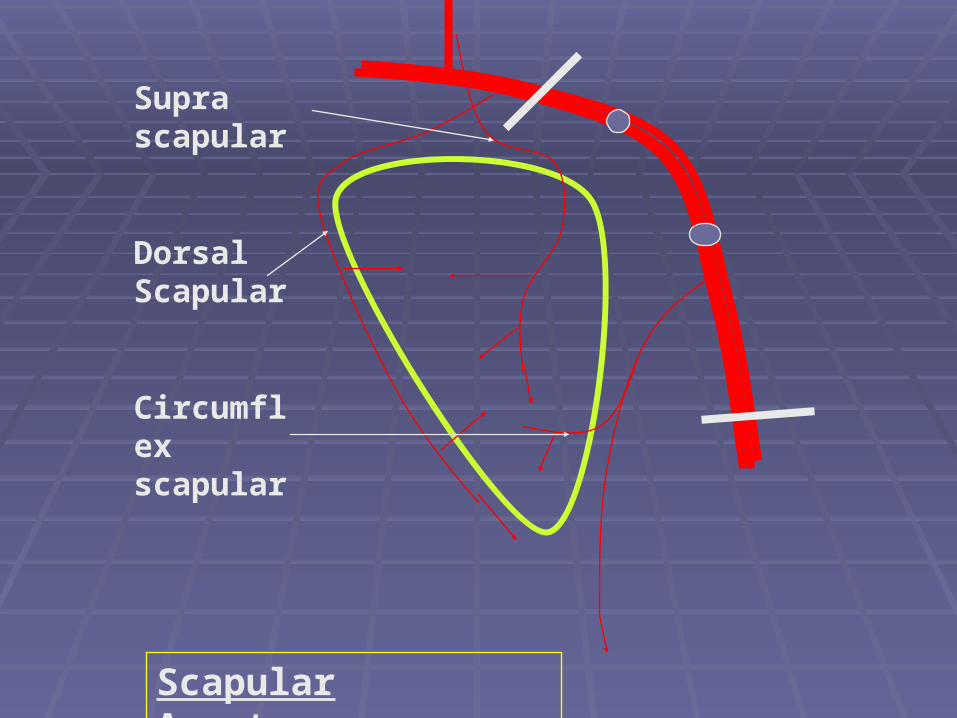
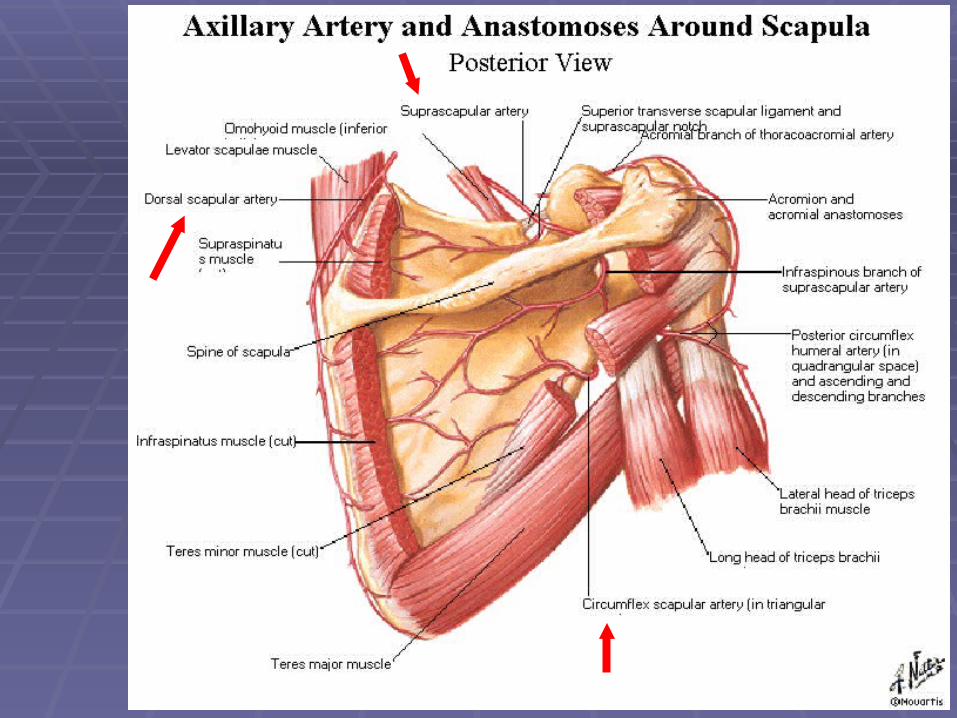
Supra scapular
Dorsal Scapular
Circumflex scapular
Scapular Anastomoses
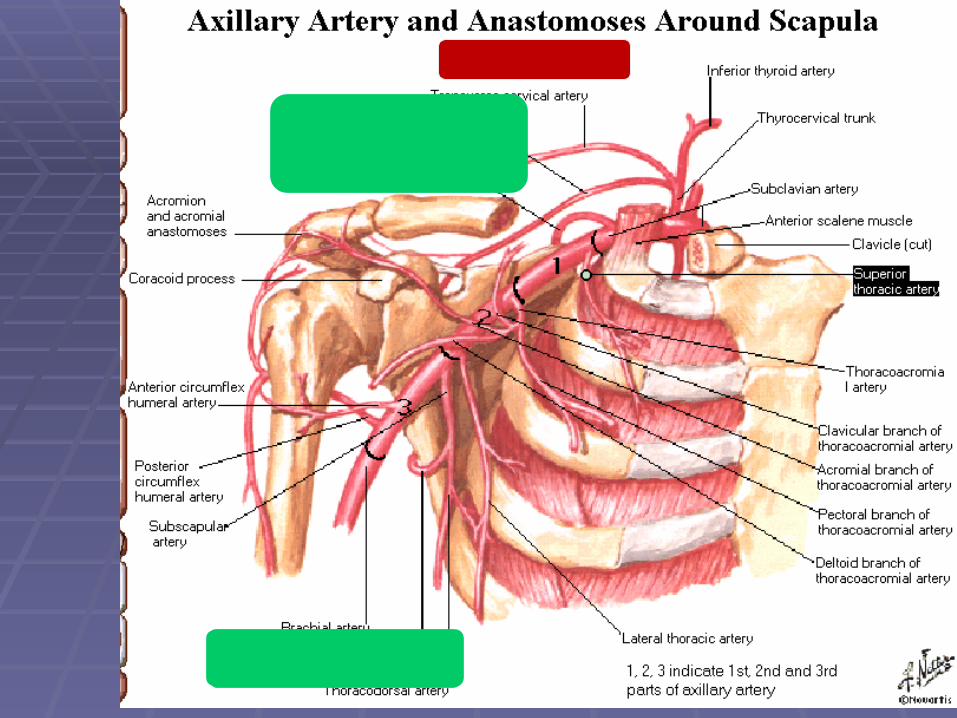
Clinical:1-The anastomoses around the scapula play a major surgical role during ligation of the an injured axillary or subclavian artery . The axillary artery can be ligated between the thyrocervical and the subscapular artery which result in directing the blood flow from the Anastomoses site to the axillary artery distal to the ligation (i.e the Subscapular a. will receive blood from suprascapular, & dorsal scapular),
Clinical:
2-Axillary artery aneurysm = ballooning of the axillary artery Because the axillary artery and the major branches of the brachial plexus are contained within the axillary sheath , a progressive dilatation of the axillary a will compress the nerves of the brachial plexus and produce neurological deficits.This a good example of how symptoms involving one system [arterial] of the body may point to Pathology Elsewhere [neurological]
124124
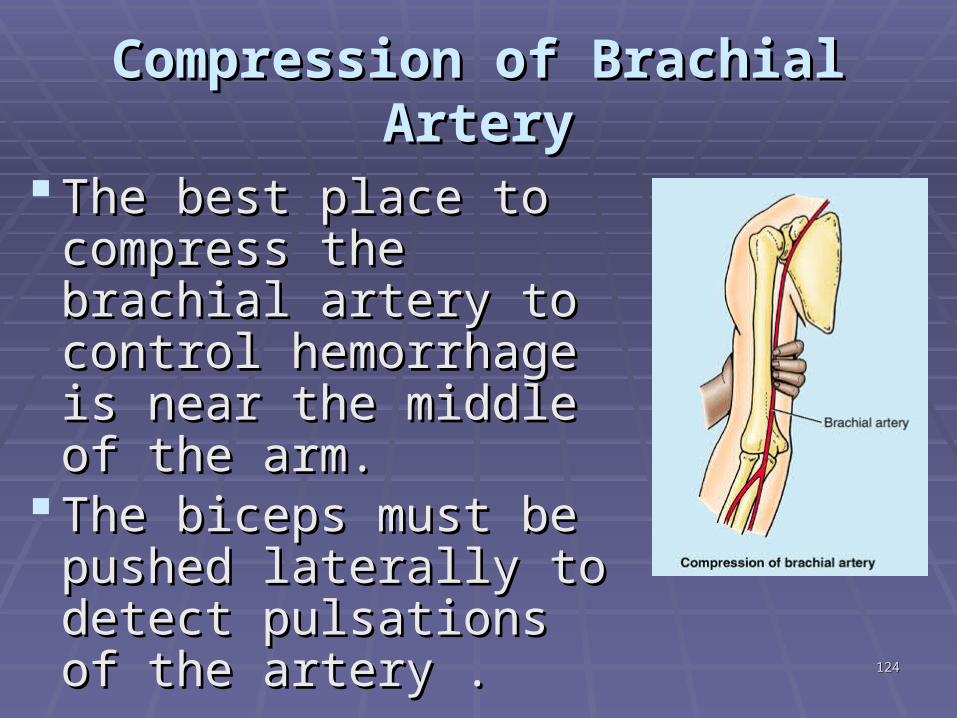
Compression of Brachial ArteryCompression of Brachial Artery
The best place to The best place to compress the brachial compress the brachial artery to control artery to control hemorrhage is near hemorrhage is near the middle of the arm. the middle of the arm.
The biceps must be The biceps must be pushed laterally to pushed laterally to detect pulsations of the detect pulsations of the artery .artery .
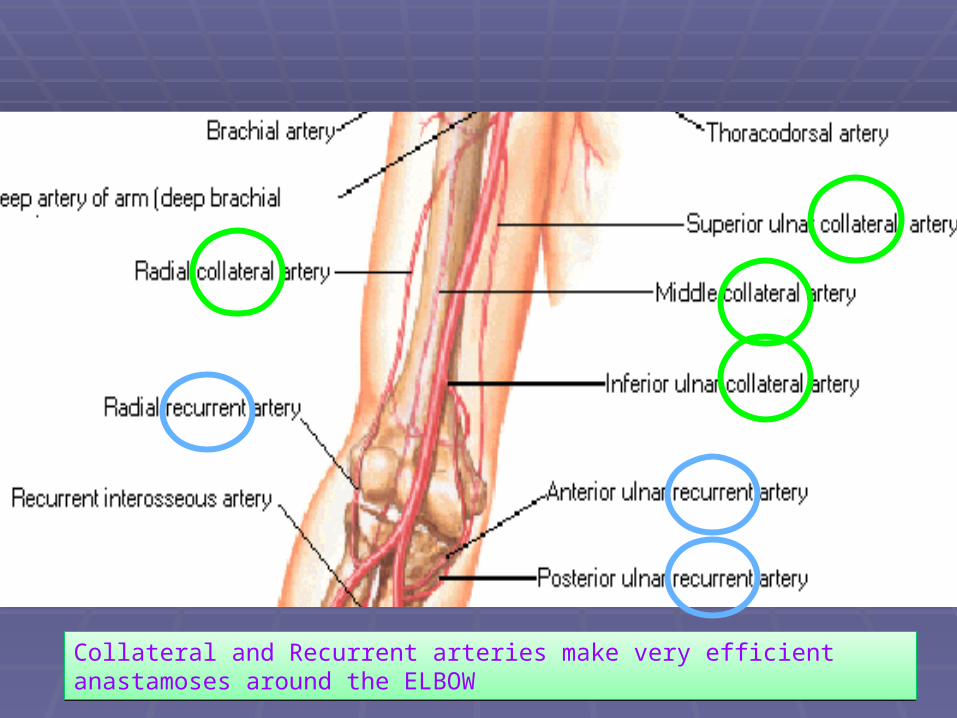
Collateral and Recurrent arteries make very efficient anastamoses around the ELBOW
126126
Anastomosis around elbow:
Gradual or partial occlusion of Brachial artery:• Anastomosis between Collateral and Recurrent branches provide enough circulation to prevent ischemia in forearm• If occlusion is distal to origin of inferior ulnar collateral, this anastomosis will be quite effective.• BUT if the occlusion is proximal to origin of deep brachial artery then ischemia can not be prevented by anastomosis.
127127
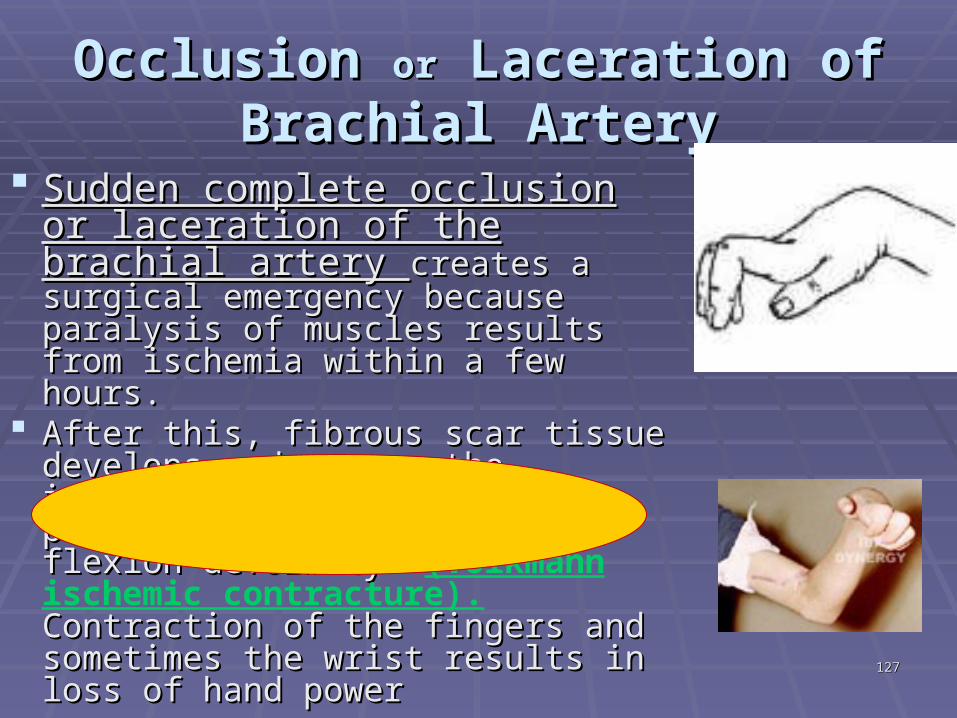
Occlusion Occlusion oror Laceration of Laceration of Brachial ArteryBrachial Artery
Sudden complete occlusion or Sudden complete occlusion or laceration of the brachial artery laceration of the brachial artery creates a surgical emergency because creates a surgical emergency because paralysis of muscles results from paralysis of muscles results from ischemia within a few hours. ischemia within a few hours.
After this, fibrous scar tissue develops After this, fibrous scar tissue develops and causes the involved muscles to and causes the involved muscles to shorten permanently, producing a shorten permanently, producing a flexion deformity— flexion deformity— (Volkmann ischemic contracture). Contraction Contraction of the fingers and sometimes the wrist of the fingers and sometimes the wrist results in loss of hand powerresults in loss of hand power
128128
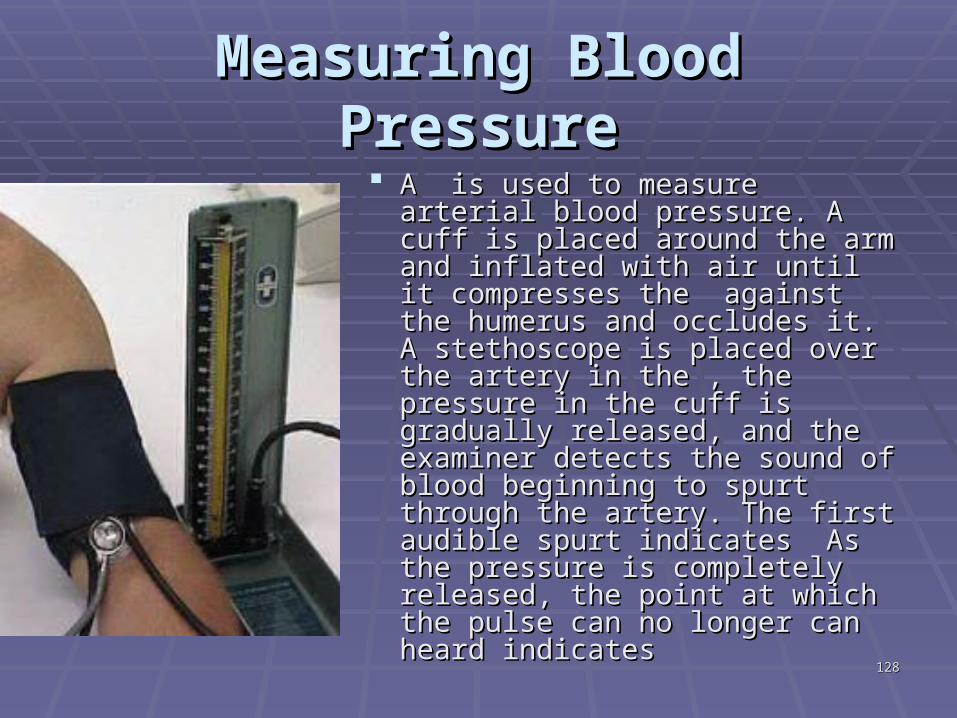
Measuring Blood PressureMeasuring Blood Pressure A is used to measure arterial A is used to measure arterial
blood pressure. A cuff is placed blood pressure. A cuff is placed around the arm and inflated with around the arm and inflated with air until it compresses the air until it compresses the against the humerus and against the humerus and occludes it. A stethoscope is occludes it. A stethoscope is placed over the artery in the , the placed over the artery in the , the pressure in the cuff is gradually pressure in the cuff is gradually released, and the examiner released, and the examiner detects the sound of blood detects the sound of blood beginning to spurt through the beginning to spurt through the artery. The first audible spurt artery. The first audible spurt indicates As the pressure is indicates As the pressure is completely released, the point at completely released, the point at which the pulse can no longer which the pulse can no longer can heard indicates can heard indicates
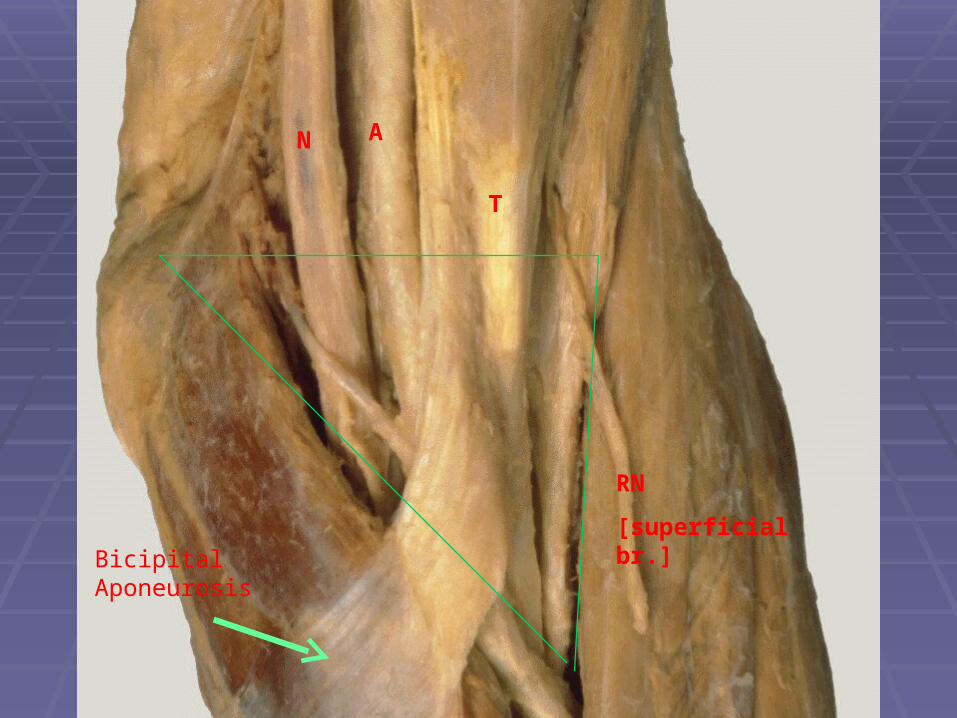
*CUBITAL FOSSA:Depression in front of the the elbow and triangular-shaped
# BOUNDRIES:-Laterally: Brachioradialis muscle-Medially: Pronator teres muscle-Base: triangle is formed by an imaginary line drawn b/w the 2 epicondyle-Floor: Supinator m laterally Brachialis m medially-Roof: skin, fascia,& reinforced by the bicipital aponeurosis
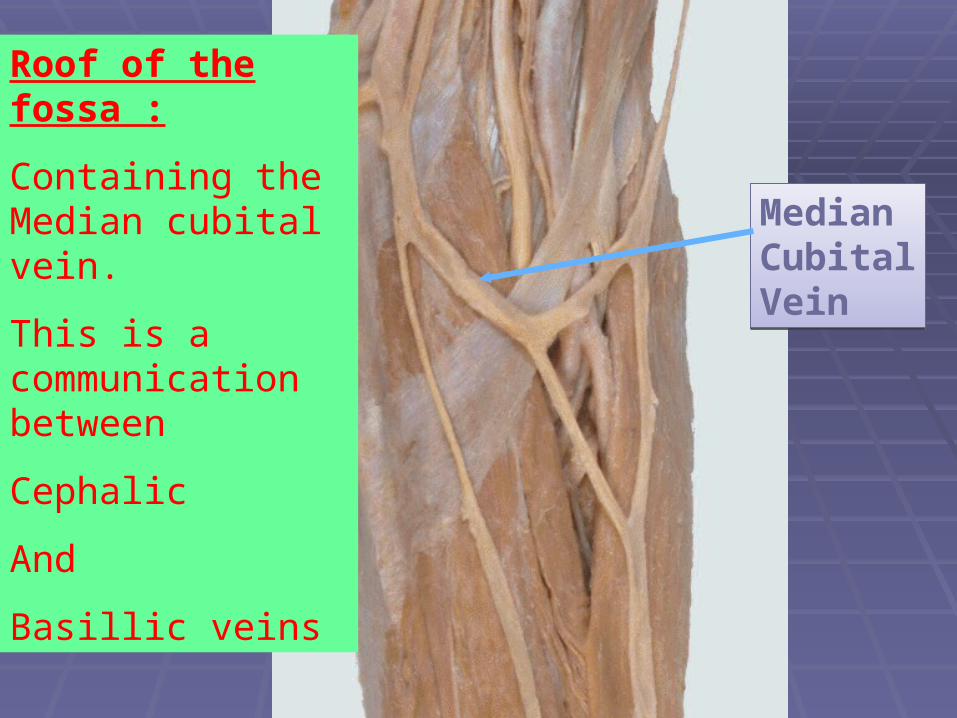
Median Cubital Vein
Roof of the fossa :
Containing the Median cubital vein.
This is a communication between
Cephalic
And
Basillic veins
132132
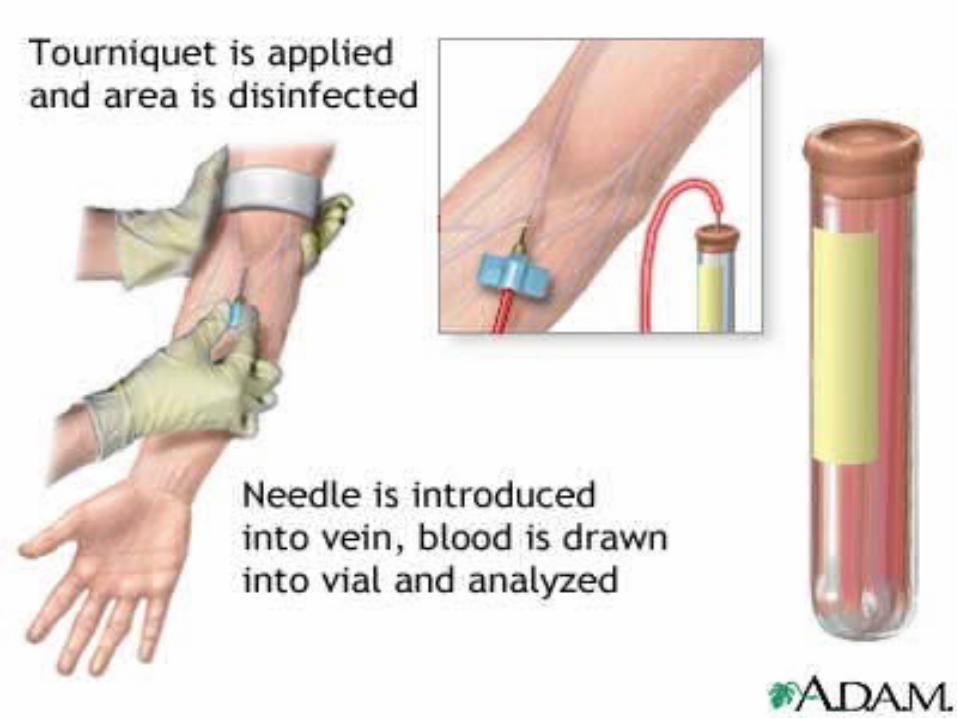
Why this vein?
• it is superficial• It is stabilized by cephalic and basillic on both side• it is has protective layer of bicipital aponeurosis underneath it to prevent accidental injury
CONTENTS: [of cubital fossa]From medial to lateral side
1-Median Nerve 2-Bifurcation of brachial artery into radial and ulnar artery 3-Tendon of biceps muscle 4-Radial nerve and its deep branch
N A
T
RN
[superficial br.]Bicipital Aponeurosis
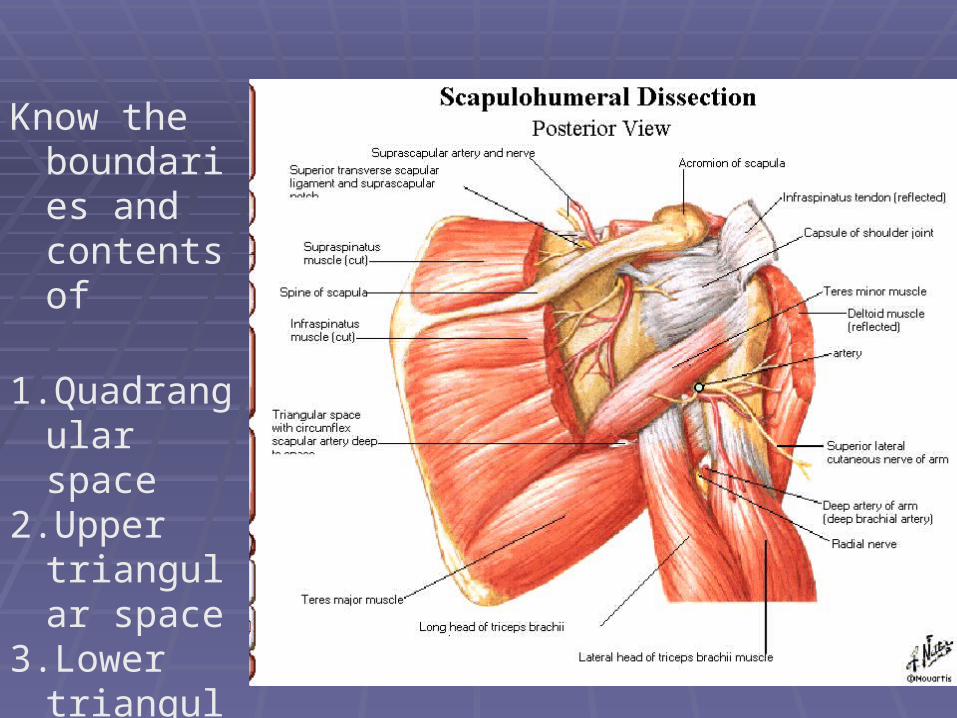
Know the boundaries and contents of
1.Quadrangular space
2.Upper triangular space
3.Lower triangular space
![1. PPT-Sugimoto-revised (final).ppt - Disaster risk reduction · 2013-05-23 · Microsoft PowerPoint - 1. PPT-Sugimoto-revised (final).ppt [Compatibility Mode] Author: ISDR_Visitor](https://img.pdfslide.us/doc/110x75/5f37e6f8ff8dba6f7114cd91/1-ppt-sugimoto-revised-finalppt-disaster-risk-reduction-2013-05-23-microsoft.jpg)



![Global population[revised].ppt](https://img.pdfslide.us/doc/110x75/55cf91cb550346f57b90bcea/global-populationrevisedppt.jpg)























