Embed Size (px)
Citation preview

Early mobility in the intensivecare unit (ICU) is critical to apatient’s short- and long-term
recovery. Studies show early mo-bility programs result in more venti-lator-free days, fewer skin injuries,shorter ICU and hospital stays, re-duced delirium duration, and im-proved physical functioning. But accomplishing early mobili-
ty requires significant coordina-tion, commitment, and physical ef-fort by the multidisciplinary team.How do we balance the benefitsof early mobilization against thepotential risk of staff or patient in-jury during the mobilization activi-ty? Part of the solution to ensuringsafe mobilization of critically illpatients is to view mobilizationalong a continuum based on pa-tient readiness, progression basedon goals, strategies to preventcomplications, and assessment ofactivity tolerance. This view keepssafety at the forefront.Within the ICU, barriers to ear-
ly mobility may include clinicians’knowledge deficits and fears, in-sufficient human and equipment
resources, patients’ physiologic in-stability, lack of emphasis on thevalue and priority of mobilizingpatients, and the ICU culture relat-ed to mobility. A 2014 internation-al survey of early mobilizationpractices in 833 ICUs found only27% had formal early mobilityprotocols, 21% had adopted mo-
www.AmericanNurseToday.com September 2014 Current Topics in Safe Patient Handling and Mobility 7
Transforming theculture: The key tohardwiring earlymobility and safepatient handlingCulture change requires deliberate focus, staffeducation, and full engagement. By Kathleen M. Vollman, MSN, RN, CCNS, FCCM, FAAN, and Rick Bassett, MSN, RN, APRN, ACNS-BC, CCRN
bility practices without a protocol,and 52% hadn’t incorporated ear-ly mobility into routine care prac-tices. Barriers to implementation ofmobility initiatives included com-peting staffing priorities, insuffi-cient physical therapy staff, andconcern about patient and care-giver injury. The study found that astandardized protocol may pro-mote successful implementation ofan early mobility program.

Importance of a culturechange Sustaining any clinical improve-ment initiative requires an organi-zational culture change. Baselineassessment of the current culture aswell as early engagement of teammembers is the starting point. In2012, the authors led a VHA, Inc.critical care improvement team col-laborative of 13 ICUs from eightorganizations to implement safeand effective early patient mobilityin the ICU. Efforts focused on elements central to sustainablechange. First, team members acquired key knowledge to under-stand why ICU mobility is impor-tant. Next, strategies for organiza-tional, leadership, and clinical staffengagement were discussed. Topromote the transition in practiceand the required culture change,ICU clinicians needed guidance.An organizational developmenttool was designed to help teamscreate an effective culture change.Although it was adapted specifical-ly to integrate with early patientmobility efforts in the ICU, this toolcan be applied to other settings.(See Learning progression for pa-tient mobility.) Three elements are crucial to
successfully implementing and sus-taining an improvement initiative: • Team members must understandand be able articulate what’sbeing proposed. To help themunderstand, they must receiveevidence-based literature andother relevant information.
• Team members must grasp whythe initiative is important to thepatient, themselves, and the or-ganization. Clinicians typicallyrespond favorably to changewhen they can connect it to real impacts.
• The leader of the initiative must
8 Current Topics in Safe Patient Handling and Mobility September 2014 www.AmericanNurseToday.com
Learning progression for patient mobility This diagram shows the four stages of staff learning regarding early patient mobility andsafe patient handling.
1
2 3
4
Right type of support, right time
To progress to the next level: Educate regardingevidence and progressive mobility continuum, use scenarios to build problem-solving skillsaround contingencies and high-risk patients.Leverage physical therapy in teaching nursesspecific skills.
STAGE 2: Conscious,unskilled
“I care now, but I feel clueless.”
• Staff are receptive toprogressive mobility concepts.
• Staff may be fearful of process and risks.
STAGE 3: Conscious,skilled
“I know but need support andextra time to execute.”
• Staff are ready to put progressivemobility into daily practice.
• Staff are motivated by sense ofefficacy and success/failureexperiences.
STAGE 1: Subconscious,unskilled
“I don’t know why I should careabout patient mobility.”
• Staff are unclear on purposebehind progressive mobility.
• Old paradigms andassumptions around immobilityare present.
STAGE 4: Subconscious,skilled
“I am skilled and can help others.”
• Staff skillfully put progressivemobility into daily practice.
• Further staff learning isenhanced by teaching andmentoring others.
To support process:educate staff regardinghow to effectivelymentor, coach. Exapnd role:storyteller, champion,and mentor.
SkilledUnskilled
Cons
cious
Subc
onsc
ious
Cons
cious
ness
© 2010 Brandwene Associates
To progress to the next level:Overcome staff's emotional andintellectual barriers by usingstorytelling and evidence,engage in discussions andaddress positive/negative aspectsof immobility. Include sources(evidence and experience)outside the organization as well.
To progress to the next level:Coach and mentor staff duringexecution. Encourage throughfailure experiences (such aspatient not tolerating mobility),and build sense of competenceby recognizing successes.
define the role of each teammember and discipline. Under-standing team roles creates asolid platform on which the cul-ture change builds.
Four stages of learning To learn a skill or concept, a per-son progresses through fourstages, according to a learningmodel attributed to AbrahamMaslow. This model can be ap-plied to clinicians learning aboutsafe patient handling and mobility(SPHM).
Stage 1: Subconscious, unskilled In this stage, team members areunaware of how little they knowand don’t realize a change is nec-essary. Also, they may have fearsand misconceptions about thechange. For example, some criti-cal care clinicians believe reposi-tioning or mobilizing critically illpatients threatens the security ofvital tubes and lines. But with theproper knowledge, training, andresources, staff can mobilize andreposition ICU patients safely with-out jeopardizing tubes and lines.In one study, 1,449 activity events(such as sitting up in bed, sittingin a chair, and ambulating) wereperformed with mechanically venti-lated patients; fewer than 1% ex-perienced adverse events. As partof the culture change, misconcep-tions about SPHM need to be ad-dressed through education andcoaching. Once the purpose ofSPHM is defined clearly and mis-conceptions have been addressed,team members are ready to moveon to stage 2.
Stage 2: Conscious,unskilled In the conscious, unskilled stage,
team members understand whySPHM is important but don’tknow how to accomplish it. Al-though open to new learning,
they may have fears about specif-ic processes or actions involvedin patient mobilization. For in-stance, they may fear certain
www.AmericanNurseToday.com September 2014 Current Topics in Safe Patient Handling and Mobility 9
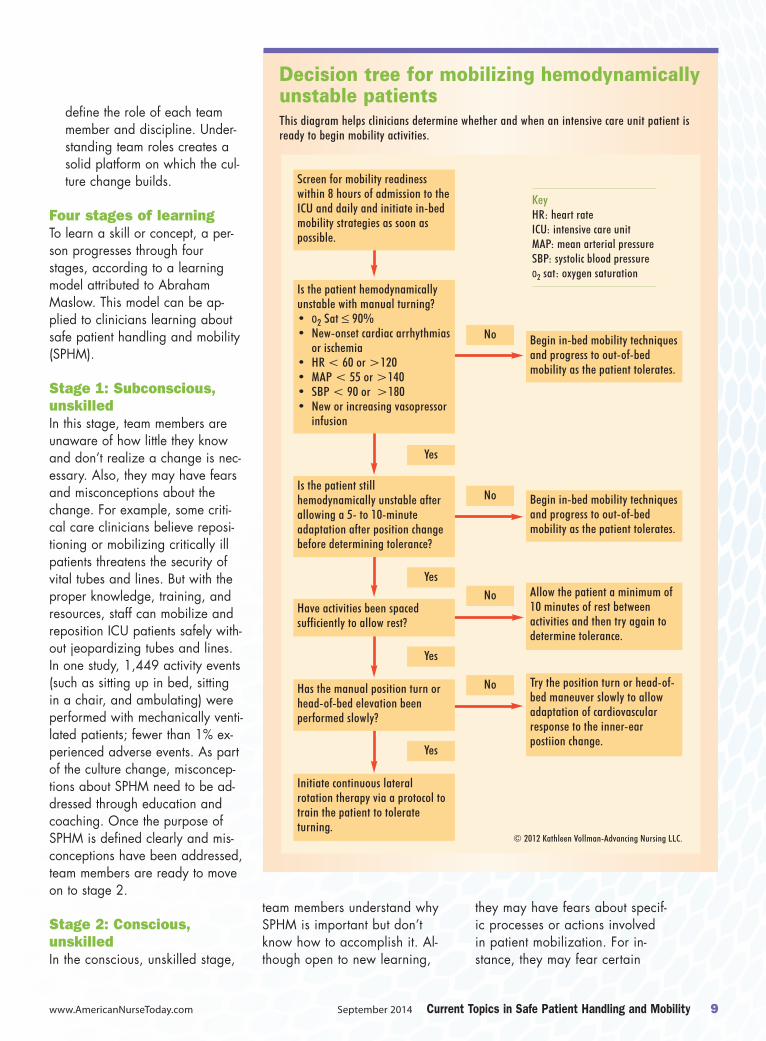
Decision tree for mobilizing hemodynamicallyunstable patients This diagram helps clinicians determine whether and when an intensive care unit patient isready to begin mobility activities.
Begin in-bed mobility techniquesand progress to out-of-bedmobility as the patient tolerates.
No
No
No
No
Screen for mobility readinesswithin 8 hours of admission to theICU and daily and initiate in-bedmobility strategies as soon aspossible.
Is the patient hemodynamicallyunstable with manual turning?• O2 Sat ≤ 90% • New-onset cardiac arrhythmias
or ischemia• HR < 60 or >120• MAP < 55 or >140• SBP < 90 or >180• New or increasing vasopressor
infusion
Yes
Begin in-bed mobility techniquesand progress to out-of-bedmobility as the patient tolerates.
Yes
Yes
Yes
Allow the patient a minimum of10 minutes of rest betweenactivities and then try again todetermine tolerance.
Is the patient stillhemodynamically unstable afterallowing a 5- to 10-minuteadaptation after position changebefore determining tolerance?
Have activities been spacedsufficiently to allow rest?
Has the manual position turn orhead-of-bed elevation beenperformed slowly?
Initiate continuous lateralrotation therapy via a protocol totrain the patient to tolerateturning.
Try the position turn or head-of-bed maneuver slowly to allowadaptation of cardiovascularresponse to the inner-earpostiion change.
KeyHR: heart rateICU: intensive care unitMAP: mean arterial pressureSBP: systolic blood pressureO2 sat: oxygen saturation
© 2012 Kathleen Vollman-Advancing Nursing LLC.

types of mobilization activitiescan cause hemodynamic instabili-ty. Education and practical appli-cation experiences can help themovercome this fear. Another wayeducators can break through suchbarriers is to use a decision treethat incorporates the latest scien-tific knowledge to help cliniciansminimize the hemodynamic im-pact or retrain patients to toleratemovement. (See Decision tree formobilizing hemodynamically un-stable patients.) A critical resource used with
the VHA team was a nurse-driven,evidence-based multidisciplinaryprogressive mobility continuumtool that addresses mobility phas-es and corresponding interven-tions. The team received educationon the tool and how to apply it in
practice. The tool provided a visu-al foundation to guide safe mobili-ty practices, create consistency,promote team communication, andenhance processes.Numerous studies show that ed-
ucation, skill building, and proto-cols may not be enough to createsustainable change. Using strate-gies to evaluate available nursingresources and systems that canproduce change makes it easierfor clinicians to provide the rightcare for the right patient at theright time while balancing theseneeds against caregivers’ needsfor safety.
In bed and out-of-bedactivitiesStrategies to promote patient andcaregiver safety during mobiliza-tion can be divided into two basiccategories—those used when thepatient is in bed and those usedwhen the patient is out of bed. In-bed mobility encompasses reposi-tioning activities, lateral-rotationtherapy, tilt-table exercises, andbed-chair sitting. Modern critical-care beds should be capable of ro-tating the patient continuously, cre-ating a tilt table through the use ofa reverse Trendelenburg positionand an adjustable footboard, pro-gressing the body through thehead elevation–foot down positionto a chair, and ultimately assistingthe patient with standing. Thesefeatures reduce the risk of patientand caregiver injury and make iteasier to perform mobility actions. For in-bed repositioning from
side to side and moving up, usinga breathable glide sheet and spe-cially designed foam wedgeshelps reduce shear and friction forthe patient and help prevents in-juries to caregivers because theyrequire a pulling rather than liftingmotion. In one study, implementa-tion of this turn-and-position systemreduced hospital-acquired pres-sure ulcers by 28% and reducedstaff injuries by 58%. Lifts can beused for some in-bed mobility ac-tivities and are effective duringambulation and the transition fromin-bed to out-of-bed activities.
Stage 3: Conscious, skilled Stage 3 learning focuses on imple-menting the change, with attentionto fine-tuning the process. Coach-ing, mentoring, and maintainingengagement are critical. In previ-ous stages, much effort was ex-pended in educating and training
staff. During the transition fromstage 3 to stage 4, the skills andknowledge required for the SPHMinitiative must become “hard-wired” or ingrained into care-givers’ subconscious. This requiresdeliberate, focused energy on con-tinued engagement. However,staff energy, resource availability,and competing priorities may posebarriers to sustaining the change. Throughout stage 3, positive
feedback, motivation, and sharingof successes and challenges areimportant for driving continual im-provement and culture change.These goals can be accomplishedin various ways. Here are someexamples: • Networking with other organi-zations in various stages of thepractice change can be ex-tremely useful. It allows collabo-rative identification and sharingof challenges, struggles, effec-tive strategies, and success sto-ries. This process creates syner-gistic energy among the teammembers, helping to motivatethem and accelerate thechange.
• Within the VHA mobility collab-orative network, teams sharedreward strategies. One teamgave out M&Ms® when “caughtin the act” of Moving and Mo-bilizing patients. Such momentspresent crucial coaching oppor-tunities. For example, after amobility event, staff can huddlebriefly to discuss the event andwhat, if any, improvementscould be made to make theprocess more effective.
Stage 4: Subconscious,skilled During this stage, the practice andculture changes are well on their
10 Current Topics in Safe Patient Handling and Mobility September 2014 www.AmericanNurseToday.com
(continued on page 25)
In-bed mobility encompasses
repositioningactivities lateral-rotation
therapy, tilt-table exercises, and
bed-chair sitting.
units. On the other hand, using aPAR system means slings will bereadily available on all shifts,which leads to better compliancewith the SPHM program.
Centralized distributionWith this system, access to slingsmay not be available when need-ed, especially on evenings,nights, weekends, and holidays.A staff member must be put incharge of maintaining central stor-age for efficient distribution, anda process for obtaining slingsmust be established. For instance,is a runner needed? If so, whosupplies the runner? Nonetheless, a well-organized
centralized distribution processcan be highly effective if commu-nication is clear and consistent.Also, lack of unit storage forslings isn’t a concern.
Sling tracking Sling tracking promotes return ofslings to the proper unit. Trackingcan be handled in several ways:• Slings can be labeled with anindelible marker, barcoded, orembroidered. A simple mark-ing system can yield valuablebenefits.
• Vendors may have sling track-ing systems your facility canuse.
Support for the SPHMprogram A well-developed sling manage-ment system supports a facility’sSPHM program. The SPHM mustelicit input from units that will usethe system and from the laundrydepartment or outsourced laun-dry company to ensure all par-ties’ needs are met. It mustchoose sling styles and fabric
and put in place procedures forsling purchase, inventory mainte-nance, care, laundering, track-ing, and replacement. Once theseissues have been addressed, thefacility is ready to embark on anSPHM program that can improvepatient care and help preventstaff injuries. 8
Selected referencesThe Facility Guidelines Institute. 2010 HealthGuidelines Revision Committee Specialty Sub-committee on Patient Movement. Patient han-dling and movement assessments: A white pa-per. April 2010. https://www.dli.mn.gov/wsc/PDF/FGI_PHAMAwhitepaper_042710.pdf. Ac-cessed June 24, 2014.
Occupational Safety and Health Administration.Lift program policy and guide: Introduction to the lift program. https://www.osha.gov/CWSA-attachment/beverlyliftprogramguide.pdf.Accessed July 3, 2014.
Jan DuBose is director of Safe Patient HandlingPrograms and Services at Hill-Rom.
www.AmericanNurseToday.com September 2014 Current Topics in Safe Patient Handling and Mobility 25
way to becoming firmly rootedand incorporated into caregivers’daily practice. Although the prac-tice change is becoming the newnorm, coaching and mentoringare needed to help maintain mo-mentum. Stories learned along thejourney should be used to inspireboth novice and expert clinicians. Objective evaluation of the im-
provement process should contin-ue, focusing on outcome measuresand identifying improvement op-portunities to promote refinement.Team members are now doingthings they never thought werepossible—and previously believedto be unsafe. Recently, I learned ofa ventilator patient at St. Luke’sMedical Center, Boise/Meridian(Idaho) who was receiving contin-uous renal replacement therapy(CRRT). Staff safely mobilized the
patient to the chair using the hos-pital’s mobility protocol. In manyICUs, such a patient would bebedbound. But at St. Luke’s, earlymobility is now routine practiceeven for these patients. Conversa-tion about mobility occurs in dailyrounds and often is a major focusof daily patient goals. In fact, staff members are likely
to comment that they no longer askthe question “Can we mobilize thispatient?” Instead, they ask, “Isthere a reason why we can’t mobi-lize the patient?” Key lessonslearned to promote and maintainthis cultural transformation includethe importance of testing new prac-tices on a small scale, getting regu-lar feedback of performance andoutcome data, providing sufficienteducation, and increasing care-givers’ will to mobilize patients byseeing the work in action.
Deliberate focus, fullengagement Incorporating new evidence intodaily practice isn’t enough to sus-tain a culture change to empha-size early mobility and SPHM.Such a change comes only with adeliberate focus on three key ques-tions: What are we are doing?Why are we doing it? What’s myrole? Full engagement and culturaltransformation can occur onlywhen all team members can re-spond to these questions with fullunderstanding. 8
Visit www.AmericanNurseToday.com/Archives/aspx for a multidisciplinary progressive mobilitycontinuum tool and a list of selected references.
Kathleen M. Vollman is a clinical nurse specialist,educator, and consultant with Advancing Nurs-ing, LLC in Northville, Michigan. Rick Bassett is acardiovascular clinical nurse specialist in adultcritical care at St. Luke’s Medical Center,Boise/Meridian, Idaho.
(continued from page 10)