Embed Size (px)
Citation preview

Top 10 (or so) Stroke Studies
McGill Neurology Academic Half-DayWednesday, November 10th 2010
Alexandre Poppe MD CM, FRCPCCentre des maladies vasculaires cérébrales
Hôpital Notre-Dame, CHUMUniversité de Montréal

Disclosures
I have received speaker’s honoraria from Sanofi-BMS and Boehringer Ingelheim
I am co-investigator in a study sponsored by Shire

Choice of studies
1. Inform our everyday management of stroke
2. Cited in major stroke care guidelines (e.g. AHA)
3. Felt by colleagues to be important
4. Probably good to know for the Royal College…

Just ten studies...

Caveats
I will focus only on ischaemic stroke
I will focus only on therapeutic RCTs– Meta-analyses will be highlighted over single
studies in some cases
Some important studies may have been omitted…

Outline
Acute stroke managementAntiplateletsThrombolysisDecompressive hemicraniectomyAcute TIA/minor stroke
Secondary stroke preventionAntihypertensivesAntiplateletsAnticoagulantsHypolipemic agentsCarotid revascularisation


Acute Stroke: Antiplatelets
CAST: randomised placebo-controlled trial
of early aspirin use in 20,000 patients with
acute ischaemic stroke. CAST (Chinese
Acute Stroke Trial) Collaborative Group.
Lancet 1997 Jun 7;349(9066):1641-1649

CAST
Randomized, placebo-controlled trial of 21106 patients at 413 Chinese hospitals.
Effect of aspirin treatment (160 mg/day) vs placebo started within 48 h of the onset of suspected acute ischaemic stroke and continued in hospital for up to 4 weeks.
10,554 patients were randomized to receive aspirin (160 mg/day) and 10,552 received placebo.

CAST
Primary OutcomeDeath from any cause during 4-week treatment period and death or dependence at the time of discharge from hospital.
Secondary Outcome:Fatal or non-fatal recurrent stroke and death or non-fatal stroke.

CAST: Results
Death at 4 wks:
3.3% vs 3.9% (p=0.04)
Recurrent ischaemic stroke at 4 wks:
1.6% vs 2.1% (p=0.01)
Hemorrhargic stroke at 4 wks:
1.1% vs 0.9% (p>0.1)

Acute stroke: antiplatelets
The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke. International Stroke Trial Collaborative Group.Lancet 1997 May 31;349(9065):1569-1581

IST
Randomised, open trial of up to 14 days of antithrombotic therapy started as soon as possible after stroke onset.
467 hospitals in 36 countries
Inclusion CriteriaSuspected acute ischemic stroke presenting within 48 hours of symptom onset.

IST
Half of the 19,435 participating patients received unfractionated heparin (5000 or 12,500 IU twice daily) and half were told to avoid heparin. In a factorial design, half received aspirin 300 mg daily and half were told to avoid aspirin. Treatment was continued for 14 days or until hospital discharge.
ASA No ASA
Heparin(5000 bid12 500 bid)
n/4 n/4
No Heparin
n/4 n/4

IST
Primary outcomes
Death within 14 days and death or dependency at 6 months

IST: Results
Heparin group Fewer recurrent ischaemic strokes within 14 days (2.9% vs 3.8%) Offset by a similar-sized increase in haemorrhagic strokes (1.2% vs 0.4%) No difference in death or non-fatal recurrent stroke (11.7% vs 12.0%)More severe extracranial bleeds, ICH, death and non-fatal stroke at 14 days with 12 500 units (12.6% vs 10.8%)
IST: Results
ASA group
Fewer recurrent ischaemic strokes within 14 days (2.8% vs 3.9%)
No significant excess of ICH (0.9% vs 0.8%)
Reduction in death or non-fatal recurrent stroke (11.3% vs 12.4%)
Non-significant excess of 2 severe extracranial bleeds per 1000 patient with ASA alone (no heparin)

IST and CAST
ASA (160-300 mg) within 48 hours of AIS:– prevents 11 nonfatal strokes or deaths per
1000 patients in the first few weeks (NNT ≈ 100)
– causes two hemorrhagic strokes per 1000 patients
– prevents death or dependency in 13 of 1000 patients at 6 months

Acute Stroke: Antiplatelets AHA Guidelines 2007

Thrombolysis

Acute stroke: Thrombolysis 0-3 hrs
N Engl J Med.1995;333:1581-1587.

NINDS-tPA
Double-blinded RCT of 624 patients with acute ischaemic stroke
Placebo or rtPA (0.9 mg/kg IV, maximum 90 mg) within 3 hours of symptom onset
Trial done in 2 parts– Part 1: 291 patients (144 tPA, 147 placebo)– Part 2: 333 patients (168 tPA, 165 placebo)

NINDS-tPA
Primary outcomes
Part 1: improvement of 4 NIHSS points over base-line or resolution of neurologic deficit within 24 hours stroke onset
Part 2: Global functional outcome (Barthel index, modified Rankin scale, Glasgow outcome scale, and NIHSS) at 90 days

NINDS-tPA: 24 hours
Part 1: no significant difference in outcome at 24 hours (47% vs 39%, p=0.21)
Part 1 and 2 combined: trend towards benefit at 24 hours (47% vs 39%, p=0.06)

NINDS-tPA: 90 days
12% absolute increase (32% relative) in favourable functional outcome
NNT ≈ 8
OR = 1.7 (95%CI 1.2-2.6)

NINDS-tPA: Bleeding and death
Major systemic bleeding: no difference (<1%)Minor systemic bleeding: 23% vs 3%
Any ICH10.6% vs 3.2%
Symptomatic ICH within 36 hours6.4% vs 0.6% (p<0.001)
61% of patients with sICH dead at 90 days
Death17% vs 21% (p=0.30)

IV-tPA 0-3hrs
NINDS results comparable to most large registries (Phase IV studies) such as CASES, SITS-MOST, STARS
AHA guidelines 2007

Acute stroke: Thrombolysis 3 - 4.5 hrs
Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke.N Engl J Med 2008 Sep 25;359(13):1317-29

ECASS-3
Multicenter, randomized, double blind, placebo controlled trial in 110 hospitals in 15 European countries
821 patients randomized to placebo or IV-tPA within 3-4.5 hours of stroke onset– 418 tPA, 403 placebo

ECASS-3
Primary OutcomeModified Rankin Scale 0-1 at 90 days
Secondary OutcomeGlobal Outcome (Modified Rankin Scale 0-1, Barthel Index 95-100, NIHSS 0-1, Glasgow Outcome Score 0-1) at 90 days

ECASS-3: Exclusions
>80 years old
NIHSS >25
Combination of previous stroke and diabetes
On anticoagulants regardless of INR
>1/3 MCA rule

ECASS-3: Results
Median OTTT: 3h59min
7.2% absolute increase in favourable outcome (52.4% vs. 45.2%)
NNT ≈ 14
OR 1.34 (95%CI 1.02 to 1.76)

ECASS-3: Bleeding and death
Systemic bleeding: no differences (1-2%)
Any ICH27% vs 17.6% (p=0.001)
sICHECASS-3 definition: 2.4 vs 0.2% (p=0.008)NINDS definition: 7.9 vs 3.5% (p=0.006)
Death7.7% vs 8.4% (p=0.68)
IV-tPA 3-4.5hrs
AHA Science Advisory 2009
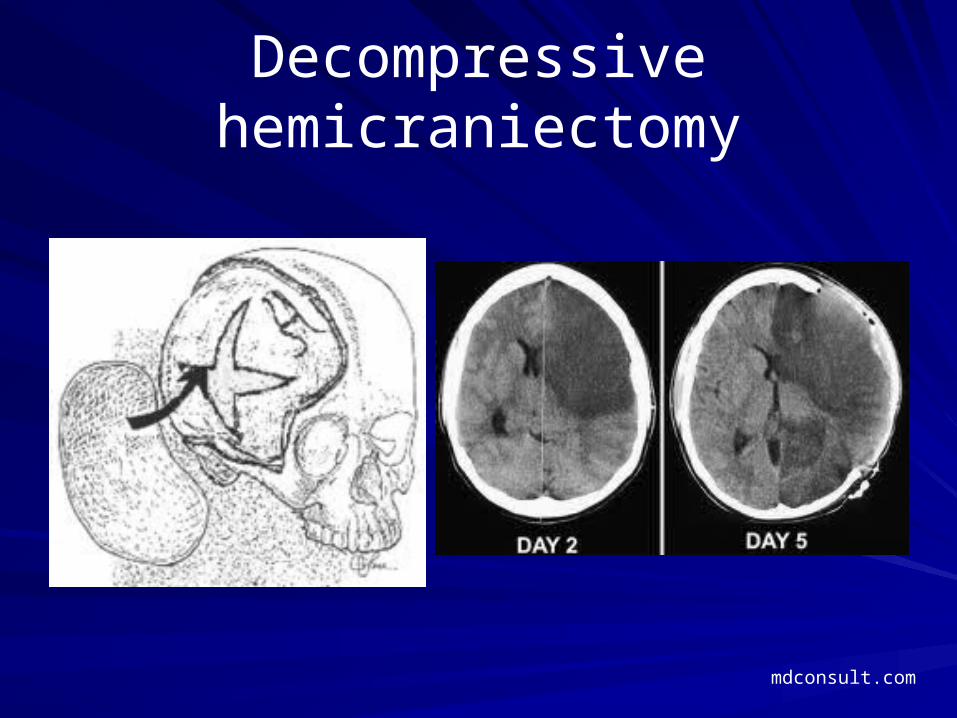
Decompressive hemicraniectomy
mdconsult.com

Acute Stroke: Decompressive hemicraniectomy
Lancet Neurol. 2007 Mar;6(3):215-22.

Decompressive hemicraniectomy
Preplanned pooled analysis of three European RCTs (DECIMAL, DESTINY, and HAMLET)
Early decompressive hemicraniectomy (<48hrs) vs medical management

Decompressive hemicraniectomy
93 patients enrolled

Decompressive hemicraniectomy
Primary outcome mRS at 1 year dichotomised between favourable (0–4) and unfavourable (5-6)
Secondary outcomecase fatality rate at 1 year dichotomisation of the mRS between 0–3
and 4-6

Decompressive hemicraniectomy
mRS 0-4: 75% vs 24%, ARR 51% (34-69%), NNT = 2mRS 0-3: 43% vs 21%, ARR 22% (5-41%), NNT = 4Survival: 78% vs 29%, ARR 50% (33-67%), NNT = 2

Acute TIA/minor stroke management

EXPRESS
Prospective before (phase 1: April 1, 2002, to Sept 30, 2004) versus after (phase 2: Oct 1, 2004, to March 31, 2007) study Effect on process of care and outcome of more urgent assessment and immediate treatment in clinic, rather than subsequent initiation in primary care, in all patients with TIA or minor stroke not admitted direct to hospital

EXPRESS
Nested within a rigorous population-based incidence study of all TIA and stroke (Oxford Vascular Study; OXVASC)
Primary outcome
Risk of stroke within 90 days of first seeking medical attention

EXPRESS: Results
Phase 1: 310 pts, Phase: 281 pts
Median delay to assessment in the study clinic:
Phase 1: 3 (IQR 2–5)
Phase 2: <1 (0–3) (p<0·0001)
Median delay to first prescription of treatment
Phase 1: 20 (8–53),
Phase 2: 1 (0–3) (p<0·0001)

EXPRESS - Results
90-day risk of recurrent stroke
Phase 1: 10·3% (32/310 patients)
Phase 2: 2·1% (6/281 patients)(p=0·0001)
ARR: 8.2%, NNT = 12-13

Stroke: Secondary Prevention
presstoexit.org.mk

Antihypertensives
Randomised trial of a perindopril-based
blood-pressure-lowering regimen among
6,105 individuals with previous stroke or
transient ischaemic attack.
PROGRESS Collaborative Group.
Lancet. 2001 Sep 29;358(9287):1033-41.

PROGRESS
RCT of perindopril vs placebo in patients with stroke or TIA
6105 individuals from 172 centres in Asia, Australasia, and Europe – Active treatment (n=3051), Placebo (n=3054)
Indapamide could be added by the treating physician

PROGRESS
Primary outcome
Any recurrent stroke

PROGRESS: Results
4 year follow-up
Recurrent stroke
10% vs 14% (95%CI 17-38, p<0.0001)
ARR 4%, NNT = 25
Combination therapy reduced blood pressure by 12/5 mm Hg and stroke by 43% (30-54) (RRR)
Single-drug therapy reduced blood pressure by 5/3 mm Hg and produced no discernable reduction in stroke risk

Antihypertensives
Dutch TIA trial (atenolol)
Stroke. 1993;24:543–548.
Poststroke Antihypertensive Treatment
Study (PATS; indapamide)
Chin Med J (Engl). 1995;108:710 –717.
Heart Outcomes Prevention Evaluation (HOPE; ramipril)
Lancet. 2000;355:253–259.

AHA 2010

Antiplatelets: ASA
Johnson ES, Lanes SF, Wentworth CE,
Satterfield MH, Abebe BL, Dicker LW.
A meta-regression analysis of the dose-
response effect of aspirin on stroke.
Arch Intern Med. 1999;159:1248 –1253.

ASA
Eleven randomized, placebo-controlled trials of ASA vs placebo in stroke/TIA patients – 5228 ASA – 4401 placebo
RRR for any type of stroke (hemorrhagic or ischemic): 15% (95%CI 6% to 23%)
Uniform effect from 50 to 1500 mg qd

Clopidogrel
A randomized, blinded, trial of clopidogrel
versus aspirin in patients at risk of ischaemic
events (CAPRIE).
Lancet. 1996;348:1329 –1339.

CAPRIE
Double-blind RCT of ASA 325 mg vs Clopidogrel 75 mg in patients with– recent ischaemic stroke, or– recent myocardial infarction, or – symptomatic peripheral arterial disease
19 185 pts, mean follow-up 1.9 yrs
Primary outcome
Composite of ischaemic stroke, myocardial infarction, or vascular death

CAPRIE
Primary Outcome
5.32% (Clopidogrel) vs 5.83% (ASA) p=0.043
ARR 0.51%, NNT = 200
No difference in subgroup of pts enrolled with stroke (7.15% vs 7.71% p=0.26)

ASA-DipyridamoleESPS-1
Lancet. 1987:2:1351–1354.
ESPS-2
J Neurol Sci. 1996;143:1–13
ESPRIT
Lancet. 2006;367:1665–1673.
ProFESS
N Engl J Med. 2008;359:1238 –1251
Sample size 2500 6602 2739 20 332
Comparison ASA 325+dipyridamole 75tid vs placebo
Aggrenox vs ASA 25bid vs Dipyridamole vsplacebo
ASA (30-325) vs ASA+dipyridamole
Aggrenox vs Clopidogrel 75
Results Stroke/death16% vs 25%
StrokeRRR 37% Aggrenox vs ASA
Vasc death, MI, stroke or bleed13% vs 16%
Stroke9% vs 8.8%

AHA 2010


Anticoagulation after stroke due to atrial fibrillation
Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic
therapy to prevent stroke in patients who have nonvalvular atrial
fibrillation. Ann Intern Med 2007; 146: 857–67.
Meta-analysis of 6 trials (n=2900)
64% RRR in stroke (95%CI 49-74%)
Annual stroke rate– Control: 4.5%, Coumadin: 1.4%– ARR 3.1%, NNT = 33

AHA 2010

Statins

SPARCL
Double-blind RCT of placebo vs Atorvastatin 80 mg
Patients with stroke or TIA within last 1-6 months, LDL 2.6-4.9 and no known CAD
N= 4731
Median follow-up 4.9 yrs
Primary outcome
Fatal or non-fatal stroke

SPARCL: ResultsMean LDL
1.9 vs 3.3 mmol/L
Any stroke
11.2% vs 13.1% (p=0.02)
ARR 2%, NNT 50 over 5 years
Major cardiovascular events
14.1% vs 17.2%
ARR 3.1% (P=0.002), NNT 33 over 5 years

AHA 2010

Carotid endarterectomy for symptomatic stenosis
Rothwell PM, Eliasziw M, Gutnikov SA, Fox
AJ, Taylor DW, Mayberg, MR, Warlow CP,
Barnett HJ.
Analysis of pooled data from the randomised
controlled trials of endarterectomy for
symptomatic carotid stenosis.
Lancet. 2003;361:107–116.

CEA
Pooled analysis of 3 RCTs of CEA vs medical management 6092 patients)
Veterans Affairs Cooperative study
JAMA.1991;266:3289–3294.
NASCET
N Engl J Med. 1991;325: 445–453.
ECST
Lancet. 1991;337:1235–1243.

CEA
Primary outcome
Ipsilateral stroke at 5 years
By degree of stenosis:• <30% : CEA harmful• 30-49% : no benefit of CEA • 50-69% : ARR 4.6%, NNT ≈ 22• >70% : ARR 16% (p<0.001), NNT≈6

Factors influencing benefit of CEA (>50%):• Sex
• NNT for men vs women: 9 vs 36
• Age• NNT for ≥ 75 vs <65: 5 vs 18
• Time from event to CEA• NNT within 2 wks vs >12 wks: 5 vs 125

CEA

AHA 2010


Questions?

Quebec’s busiest acute stroke service
6 dedicated stroke neurologists 4 interventional neuroradiologists
Opportunities for clinical research
All in beautiful Montreal!
Centre d’AVC aigu le plus occupé au Québec
6 neurologues neurovasculaire4 neuroradiologistes d’intervention
Possibilité de recherche clinique
Le tout au coeur de Montréal!





























