Embed Size (px)
Citation preview

Up-date in Budd-Chiari syndrome
Dr Aurélie Plessier
Centre de Référence des Maladies Vasculaires du Foie
Service d’Hépatologie
Hôpital Beaujon - Clichy

I have not financial relationships to disclose within the past 12
months relevant to my presentation
AND
My presentation does not include discussion off-label or
investigational use

Epidemiology of BCS
Sweden°
1990-
2003
France
2010
Korea
2009-2013
NPL
1990-1992
Incidence(/ 106/ yr) 0.8 0,68 0,87 2.50
Prevalence(/ 106)
1.4 4 5,3 NA
Rare disease = < 1/2000
Shresta J Gastro Hepato 1996. Rajani Liver Int 2008, Ollivier EASL 2014, Ki Liv Intern 2016

Gender specific incidence rate in
Northwestern Italy
Overall gender-specific incidence rates
• for PVT
– 3.78 per 100,000 inhabitants in males
– 1.73 per 100,000 inhabitants in females
• for BCS
– 2.0 in males
– 2.2 per million inhabitants in females
Ageno Thromb Haemost 2017
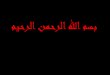
HEPATIC VEIN OBSTRUCTION LEADS TO ASCITES FORMATION
BCS defined as Obstruction of venous
outflow
Sinusoidal perfusion
Sinusoidal pressure
Portal and splanchnic pressure

A multifactorial systemic disorder
• At least one condition 87%
• Multiple conditions 48%
• Local factor 5%
EN-Vie BCS Cohort. Darwish Murad Ann Intern Med 2009
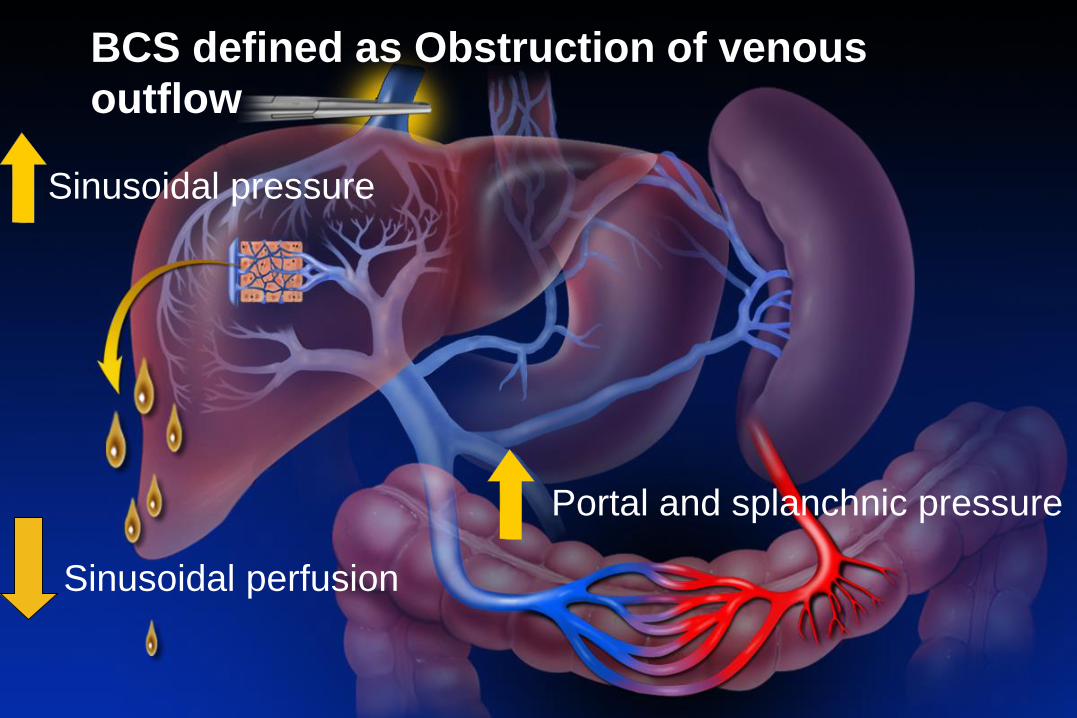
Cause varies according to
geographic origins
% Europe
N=157
Algeria
N=115
China
N=92/127
MPN/Jak2 + 49/29 34 4
APLS 37 22 NA
V Leiden 19 11 0
PNH 15 4 1,6
Coeliac /Behcet 1/4 12/3-9 NA
Oral contraceptive 33 34 4
Pregnancy 6 4 NA
Darwish Murad Ann Int Med 2009, Afredj World J Hep 2015,
Seijo Hepatology,2014 Qi. J Gastroenterol Hepatol 2012, D’amico int J vasc med 2014;
De Stefano 2011

Primary Budd-Chiari SyndromeSite Specificity in Prothrombotic Disorders
• Behcet’s D. • V Leiden • Poverty
• MPD• OC
• PNHValla J Hepatol 2009,
Riggio JTT 2013

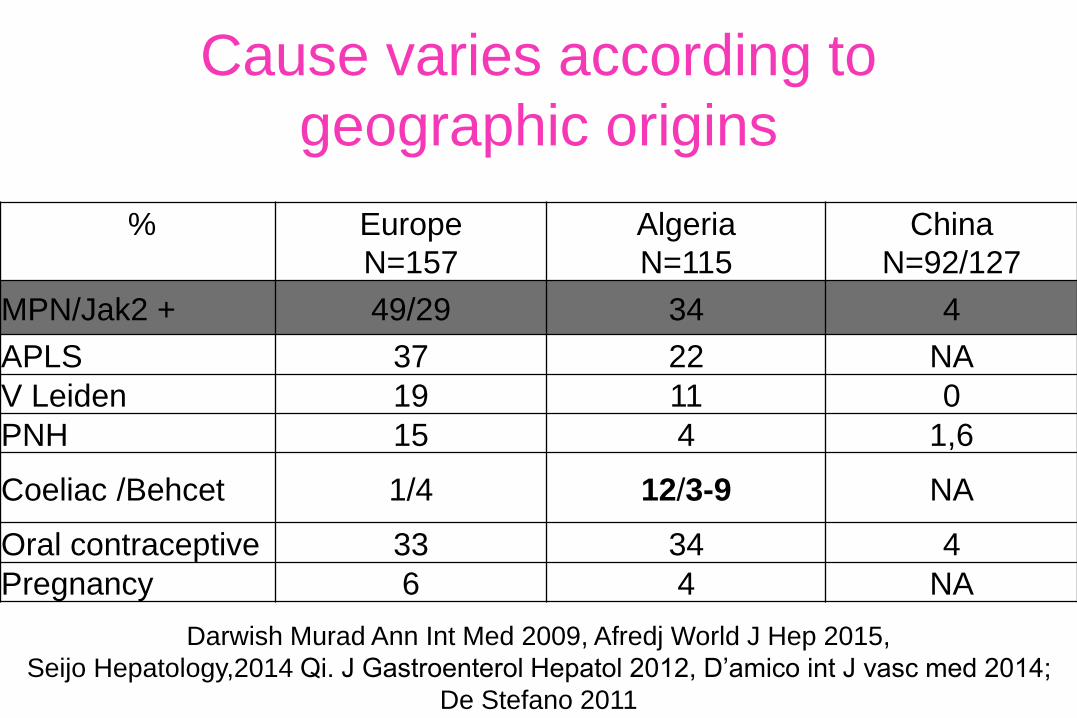
MPD specificity in Splanchnic vein
thrombosis
Plt > 200 000 et SPM > 16cm
Highly predictive of MPD
312 splanchnic vein thrombosis
(99 Budd-Chiari, 212 PVT)
MPD JAK2V617F+
N=58 (20%)JAK2V617F-
(N=254)
Spleen ≥ 16 cm and
platelets > 200/µL
(N=9)
Spleen< 16 cm and
platelets< 200/µL
(N=234)
MPD N=7 85%
(CALR mutation N=5
BM N=2)
MPD N=8
3%
No MPD
(N=226)
Rautou EASL 2015
Spleen? N=11
CALR mutations testing can be restricted to patients with
splanchnic vein thrombosis having a spleen height ≥ 16
cm and a platelet count > 200 G/L and no JAK2V617F
Causes specificity in Splanchnic vein
thrombosis
Plt > 200 000 et SPM > 16cm
Highly predictive of MPD
Treating cause well tolerated and may improve
BCS outcome
Thrombosis can recure in anticoagulated patients
Chait 2005 Br J Hem, Killadjian Blood 2008, Jasper Blood 2012, Pieri Am J Hematol 2017,Desbois Orphanet J Rare Dis. 2014,De Stefano,Blood Cancer Journal 2016

Recurrent thrombosis in patients
with splanchnic vein thrombosis and
MPD• incidence rate of 4.2 per 100 pt-years
• Significantly higher risk of recurrence
– BCS (hazard ratio (HR): 3.03),
– history of previous thrombosis (HR: 3.62),
– splenomegaly (HR: 2.66)
– leukocytosis (HR: 2.8)
• Vitamin K-antagonists (VKA) 85% of patients
– recurrence rate 3.9 per 100 pt-years,
– no VKA 7.2 per 100 pt-yearsDe Stefano,Blood Cancer Journal 2016

Treating the cause
• MPD PEG: IFN-a, anti-JAK2, Hematopoietic SCT
• PNH: Eculizumab, Hematopoietic SCT
• Behcet: Corticoids, Endoxan,..
• Coeliac disease: Gluten free diet
Available treatments
Chait 2005 Br J Hem, Killadjian Blood 2008, Jasper Blood 2012, pieri Am J Hematol 2017,Desbois Orphanet J Rare Dis. 2014, De stefano 2016

EASL guidelines -causes
1. Investigate underlying local and systemic
prothrombotic factors. Identification of one risk
factor should not deter from looking for additional
risk factors. (A1)
2. Work-up consists of diagnosis for inherited and
acquired thrombophilia factors, myeloproliferative
neoplasms, paroxysmal nocturnal haemoglobinuria
and auto-immune disorders. (A1)
3. Investigate patients with both BCS and PVT for
local risk factors, including intra-abdominal
inflammatory conditions and abdominal
malignancies. (A1)
Journal of Hepatology 2016

EASL guidelines 2015-causes 1. Thrombophilia screening includes protein S, protein C and
antithrombin levels, FVL mutation, prothrombin G20210A
gene variant and anti-phospholipid antibodies (APA). In
case of APA positivity, this should be repeated after 12
weeks. (A1)
2. Test for MPN in SVT patients, also when normal peripheral
blood cell counts by testing for JAK2V617F mutation (A1).
In JAK2V617F mutation negative patients, Cal R mutation
screening and if both negative bone marrow histology
should be considered. Patients have to be referred to a
haematologist. (B2 )
3. Treat the underlying condition as appropiate. In case of
MPN, anticoagulation indefinetely(B1).
Journal of Hepatology 2016

Primary BCS – Natural History
100
50
0
1 53
Su
rviv
al %
1960-1970
Ascites with emaciation
GI bleeding due to PHT
Liver failure
Adapted from Tavill.
Gastroenterology 1975
years

9,5%
42%
29%
12%
6%2,5%
1-7 days Fortuitus8 d - 1 month >1-6 months 6 months – 1 year > 1 year
Time of diagnosis in 158 patients
48,7%
Allaire, Ollivier EASL 2014

Ascites 83 %
Pain 61%
Oesophageal varices
Upper GI bleeding
58%
5%
Hepatomegaly 67 %
Splenomegaly 52 %
Murad Ann int med 2009
BCS at diagnosis

When should we suspect BCS?
1. Acute liver failure and hepatomegaly
2. Acute liver failure and ascites
3. Ascites and hepatomegaly
3. Refractory ascites but PT >60%
4. Known prothombotic state and liver disease
5. Any liver disease (because it can be cured)
Murad, ann int med 2009, Plessier, Hepatology,
2006

Valla, D-C Gut 2008;57:1469-1478
Diagnostic Strategy
Any patient with acute or chronic,
symptomatic or asymptomatic
liver disease

C
B
D
A


•Consider diagnosis of BCS in any symptomatic
or asymptomatic patient with acute or chronic
liver disease
•US-Doppler is the first line investigation for BCS.
MRI and CT have to be used for diagnostic
confirmation
•Reevaluate with expert radiologist negative
imaging studies patients with high BCS suspicion.
•Refer patients with BCS to expert centers on
this disease
EASL guidelines 2015-diagnosis
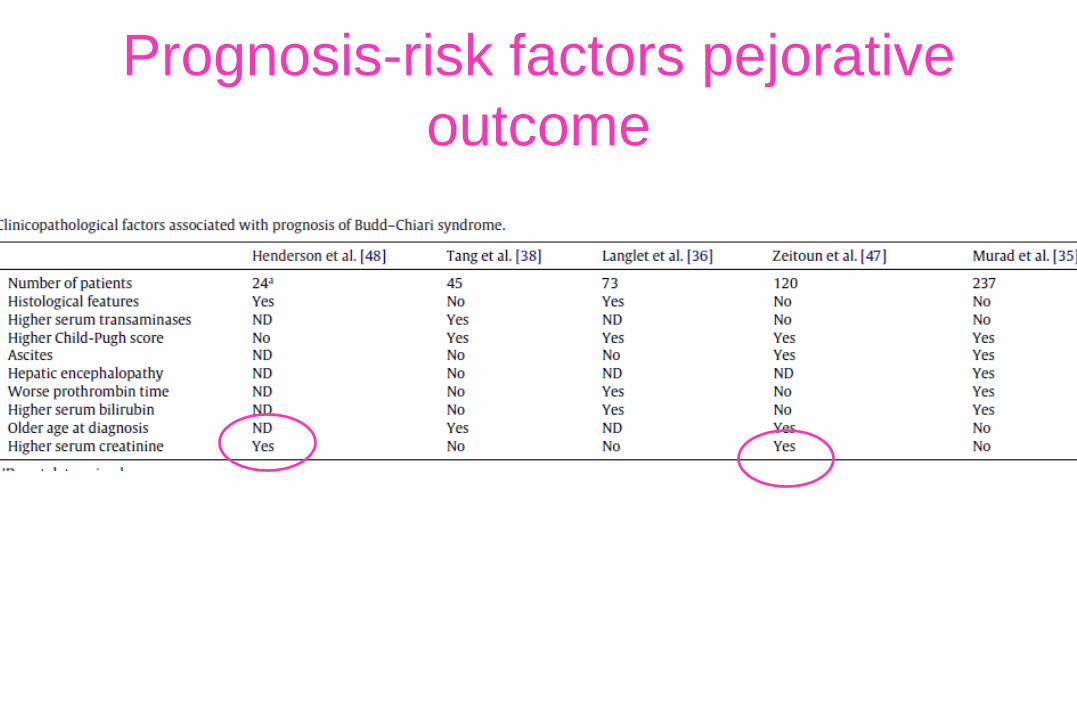
Prognosis-risk factors pejorative
outcome

Prognosis-risk factors pejorative
outcome
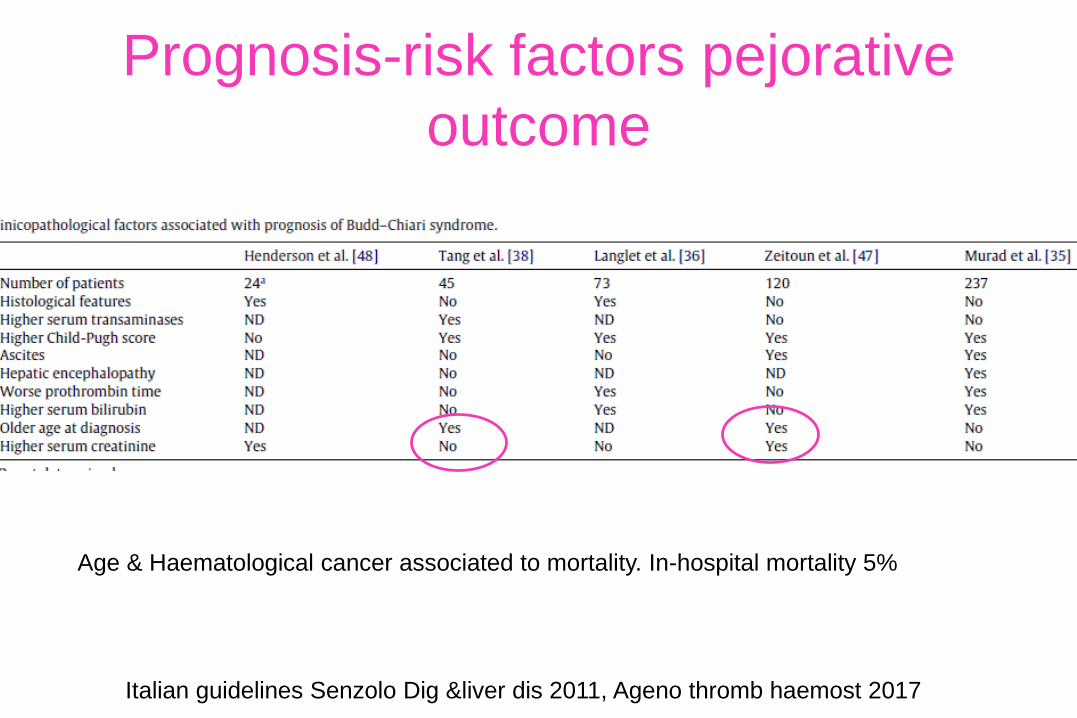
Italian guidelines Senzolo Dig &liver dis 2011, Ageno thromb haemost 2017
Age & Haematological cancer associated to mortality. In-hospital mortality 5%
Prognosis-risk factors pejorative
outcome

Symptoms NoAnticoagulation
Anticoagulation
Treat cause and
PHT
TIPS
Transplantation
Angioplasty/
Stent
yes
Treatment failure
Treatment failure
Baveno 2009 and 2015, AASLD guidelines 2009, EASL guidelines 2015

At least one 1 criteria Day 15
• Significant ascites
• Factor V < 40%
• C Bilirubin > 15µmol/L or not decreasing
• Upper GI bleeding from PHT
• Infection
• BMI remaining < 20 kg/m2
• No natriuresis with diuretics
Treatment failure criteria
Plessier Hepatology 2006
Patient outcome
• Yes 6l/week
• Factor V 36%
• Conjugate Bilirubin > 18 µmol/L
• No
• No
• Denutrition
• Na u< 20 /24h despitespironolactone and furosemide

BCS - Improved survival over 50 years
Copyright ©2008 BMJ Publishing Group Ltd. Valla, D-C Gut 2008;57:1469-1478
1960-1970

BCS - Improved survival over 50 years
Copyright ©2008 BMJ Publishing Group Ltd. Valla, D-C Gut 2008;57:1469-1478
1960-1970
ANTICOAGULATION Rx

EN-Vie cohort. Seijo. Hepatology 2013
Hepatic Vein Thrombosis - Survival
26% †
13% LTx
39% TIPS
27% Tt méd.

Recanalisation
• Partial or segmental stenoses present in:
– 60% with IVC obstruction,
– 25–30% with hepatic vein obstruction
• In the West, performed 25% of patients
• In the East, performed 80-90%
– Low morbidity
– Low recurrence rate BCS 15%
Plessier hepatology 2006, eapen gut 2006, Han WJG 2014, Munkund WJR 2011, Li Eur Rad 2017

Valla, Gut 2008
Plessier, Hepatology 2006
Eapen, Gut 2006
Darwish Murad, Ann Intern 2009
TIPS? To whom? when? how ?

Indication for TIPS placement % Garcia Pagan Ronot
Ascites 59 93
Liver failure 22 31
Upper Gi bleed from PHT 10 7
Other 10 17
Median/Mean Meld 17 (16-19) 14+4 (6-25)
Garcia-Pagan Gastroenterology 2008, Ronot, Radiology 2016
Indication for TIPS

Stratégie thérapeutique
Valla, Gut 2008
Plessier, Hepatology 2006
Eapen, Gut 2006
Darwish Murad, Ann Intern 2009
15 days
TIPS : How ?

A challenging procedure Barcelona Clichy
Transcaval % 57 92
Hyperarterialisation % 80-100 80-100
Number of stents 1/2/3/4 37/50/10/3 36/49/13/2
Portal vein thrombosis % 10 6
Anticoagulants ~100 100
Thrombophilia MPD/APLS
%
56/12 52/13
Success ITT/per prot 84/93 93/98
Garcia-Pagan Gastroenterology 2008, Ronot Radiology 2016


TIPS– learning curve
Plessier Hepatology 2006

Alternative attitude?
TIPS is the mostly used treatment for BCS… However,timing for TIPS was not stated.
Due to the rarity of BCS, management guidelines comefrom experts opinion, are empirical and notevidence-based
Given that benefit of treatments for BCS is not underdebate, I wonder if anticipating invasive treatments,before no response to medical therapy appears, coulddecrease hepatic fibrosis development, diseaseprogression and finally improve outcome
Mancuso, Hepatology 2013

Budd-Chiari Syndrome
Current Challenges
• Complications of therapy
• Pregnancy
• Regenerative nodules and HCC

Per procedure and acute TIPS
complications 20 to 30% % Garcia
pagan
N=124
Ronot
N=54
Death 2 4
Bleeding (hematoma, hemobilia) 12 14
Cardiac 4 NA
Other (thrombosis) 3 12
Garcia-Pagan Gastroenterology 2008, Ronot, Radiology 2016

Late complications : encephalopathy
1-year HE 21-25%
Transient 18-20
Recurring 2-4*
*Rifaximin efficient
Garcia-Pagan Gastroenterology 2008, Ronot, in press Radiology 2016

Late complications: TIPS dysfunction
Garcia-Pagan, Gastroenterology 2008

Factors associated with dysfunction 42% (27
months)
Number of stents initially placed > 2
HR = 3,90, p = 0,027
Early complications (< 7 days)
HR = 11,34, p = 0,009
Myeloproliferative neoplasm
HR = 8,18, p = 0,017
Technical factors
Longer tracks
Complex procedures
Ronot radiology 2016

N N Death
Prolonged Anticoagulation 139 89%
Bleeding 24 17% 3 2%
Portal hypertension 14 2
Intracranial 3 1
Other 7 0
Seijo. Hepatology 2013
BCS - Bleeding on Anticoagulation Therapy

N N Death
Prolonged Anticoagulation 139 89%
Bleeding 24 17% 3 2%
Portal hypertension 14 2
Intracranial 3 1
Other 7 0
Seijo. Hepatology 2013, Rautou J Hepatol 2010
Severe bleeding Incidence 24%p.yr vs 7%

Budd-Chiari Syndrome
Current Challenges
• Complications of therapy
• Pregnancy
• Regenerative nodules and HCC

VTE in pregnancy• Pregnant women are at an increased risk for venous thromboembolic
disease (VTE)
– 2-4 fold increase compared to non-pregnant state
– 1 in 1000 pregnancies
– Cesarian delivery > vaginal delivery
– 2/3 of DVT occur antepartum (equally distributed among all three trimesters)
– 43-60% of PE occur 4-6 weeks after delivery
– Daily risk of PE and DVT highest following delivery than antepartum
• PE is a major non-obstetric cause of maternal mortality
– 2/100 000 pregnancies
Courtesy of A Berzigotti

Effects of PH/VLD on the mother and child
Pregnancy in patients with known VLD
Effects of pregnancy on PH/VLD
Courtesy of A Berzigotti

Circulatory changes occurring during pregnancy
Increased plasma and RBC volumeIncreased venous capacity (estrogen) Decreased systemic vascular resistance (peripheral vasodilation due to prostacyclin and NO)
Net effect: worsening of hyperdynamic
circulation
P= R * Q

Mechanical effect of pregnancy
Increase in intrabdominal pressure increases portal pressure
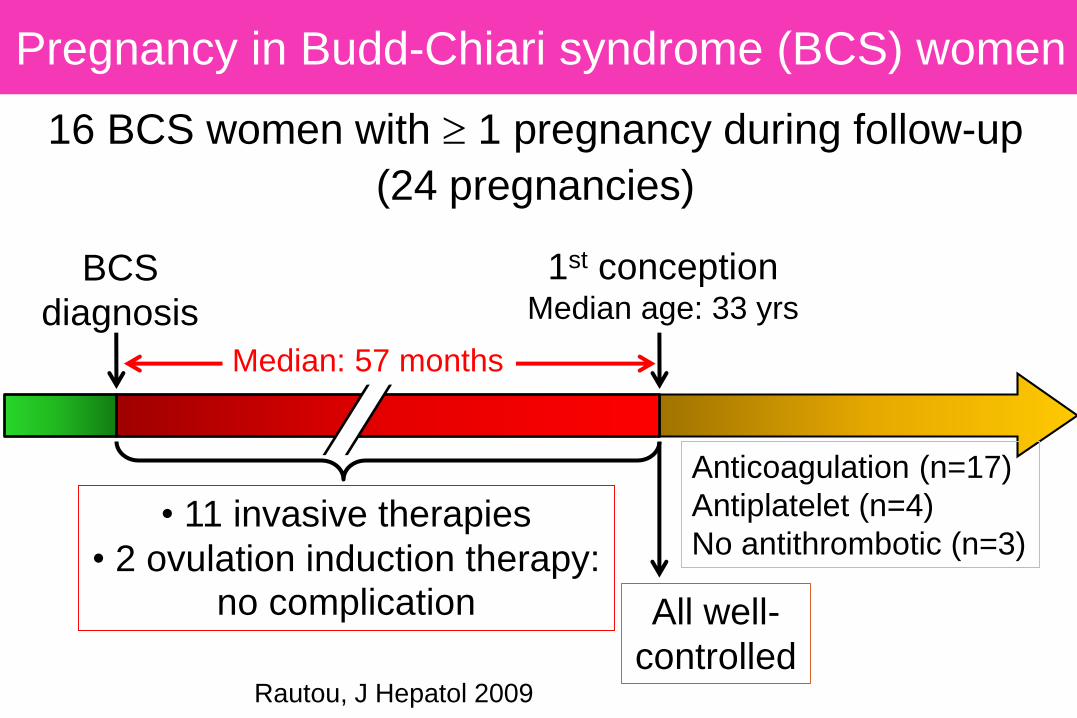
Pregnancy in Budd-Chiari syndrome (BCS) women
Rautou, J Hepatol 2009
16 BCS women with 1 pregnancy during follow-up
(24 pregnancies)
BCS
diagnosis
1st conceptionMedian age: 33 yrs
All well-
controlled
Anticoagulation (n=17)
Antiplatelet (n=4)
No antithrombotic (n=3)• 11 invasive therapies
• 2 ovulation induction therapy:no complication
Median: 57 months

Rautou, J Hepatol 2009
Pregnancy in BCS women: Fetal outcomeN
um
ber
of pre
gnancie
s
weeks of gestation
Miscarriage/
ectopic
pregnancy
Early
preterm
Preterm
Term
24 pregnancies 16 alive
No sequelae
1 stillbirth

Rautou, J Hepatol 2009
Pregnancy in BCS women: Maternal outcome
Ascites in 2 patients:
- 1 portal vein thrombosis
- 1 TIPS obstruction
- Intrahepatic cholestasis (n=3)
- Intrauterine hematoma (n=3)
- Preeclampsia (n=1)
- Placenta praevia (n=1)
- Postpartum bleeding (n=4)
Gestational
course and
perinatal complications
Liver-related complications

Favorable:
- But screen for bleeding and pre eclampsia
- healthy infant born after gestation week 32
Pregnancy in BCS women: Outcome
• No maternal death (follow-up: 34 months after last delivery)
Rautou, J Hepatol 2009

What to do in patients with BCS in childbearing age
• Ask regularly if a pregnancy is desired
• If it is, anticipate actions to avoid problems:
• Re-evaluate the status of the underlying liver disease: discourage pregnancy if LD not stable/recompensated; optimise primary/secondary prophylaxis of variceal bleeding if needed
• Explain that there is a high risk of early fetal loss (> BCS) decreasing after 20 weeks, that prematurity is likely and explain risk for the mother (> BCS)
• LMWH is safe in pregnancy: if on OAC shift to this class as soon as conception might have occurred (test ASAP). Close anti Xa surveillance with haematologist
• Collaboration haematologist, obstetrician and haepatologist
• Vaginal delivery whenever possible

Budd-Chiari Syndrome
Current Challenges
• Complications of therapy
• Pregnancy
• Regenerative nodules and HCC

T1
T2
Cazals-Hatem. Hepatology 2003
Regenerative changes
Macronodules
Budd-Chiari Syndrome
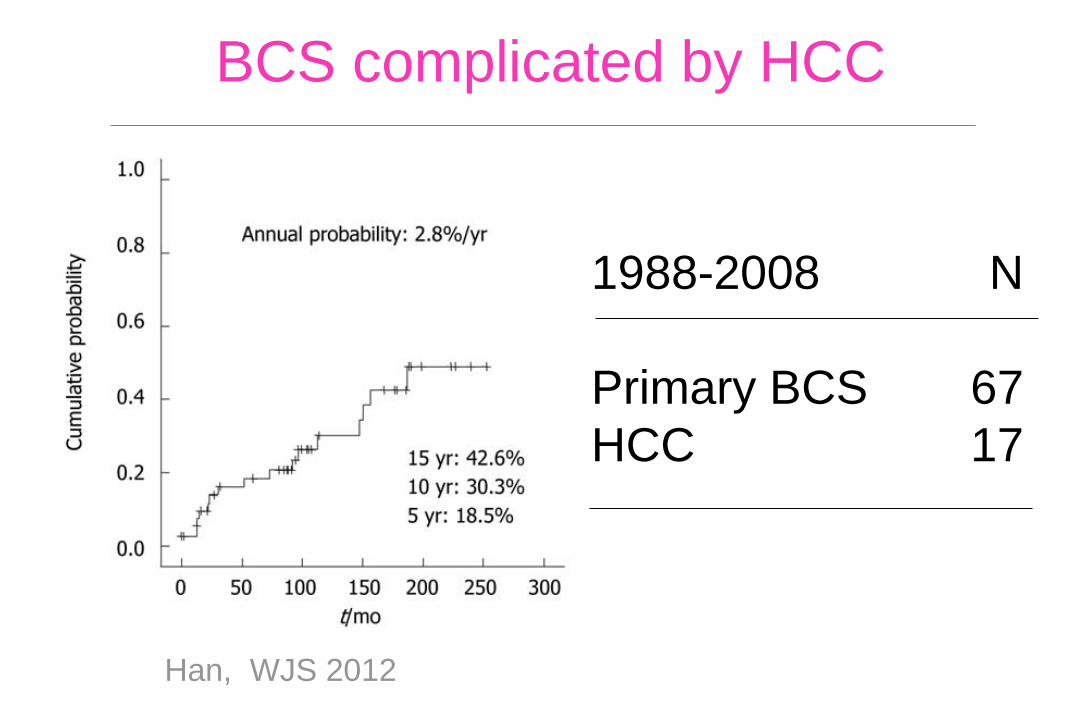
BCS complicated by HCC
Han, WJS 2012
1988-2008 N
Primary BCS 67
HCC 17

BCS and Hepatocellular Carcinoma
WithoutNoduleN = 68
BenignNoduleN = 25
HCC
N = 9
Follow-up yrs 5 7 9
Age yrs 37 36 34
Male% 29 24 67
Blocked IVC % 7 0 78OR 78 [95% CI 11-560]
Moucari. Gut 2008. 102 consecutive patients without nodules at inception, 1995-2005

T2 2004 T2 2006
T2 2008 T2 2010

BCS and Hepatocellular Carcinoma
BenignN = 25
HCCN = 9
P
Largest diameter - cm 2 8 .0001
Number of nodules 5 1 .001
% Heterogeneous 0 100 .0001
AFP > 10 ng/ml - % 0 78 .0001
Moucari. Gut 2008. 102 consecutve patients without nodules at inception, 1995-2005

allowing to
• differentiate
FNH from FNH-like
FNH from adenoma
• classify adenoma in different subtypes
characteristicbiomarkers**
*Zucman-Rossi et al Hepatology 2006; Rebouissou et al J Hepatol 2008
** Bioulac-Sage et al Hepatology 2007; Liver Int 2008; Seminars Liver diseases 2011; WHO book 2011
Can hepatocellular adenoma bio markers help for the
characterization of nodules in BCS ?
Courtesy from Paulette Bioulac Sage

Retrospective multicenter survey
45 cases of liver vascular disease (mainly
explanted livers)2015
11 adenomas:
• 9 previously diagnosed were
subtyped using the
immunohistochemical panel
• 2 additional adenomas come
from reclassification of
LRN/FNH-like
Hepatocellular adenomas-patho-molecular
classification in vascular liver disease
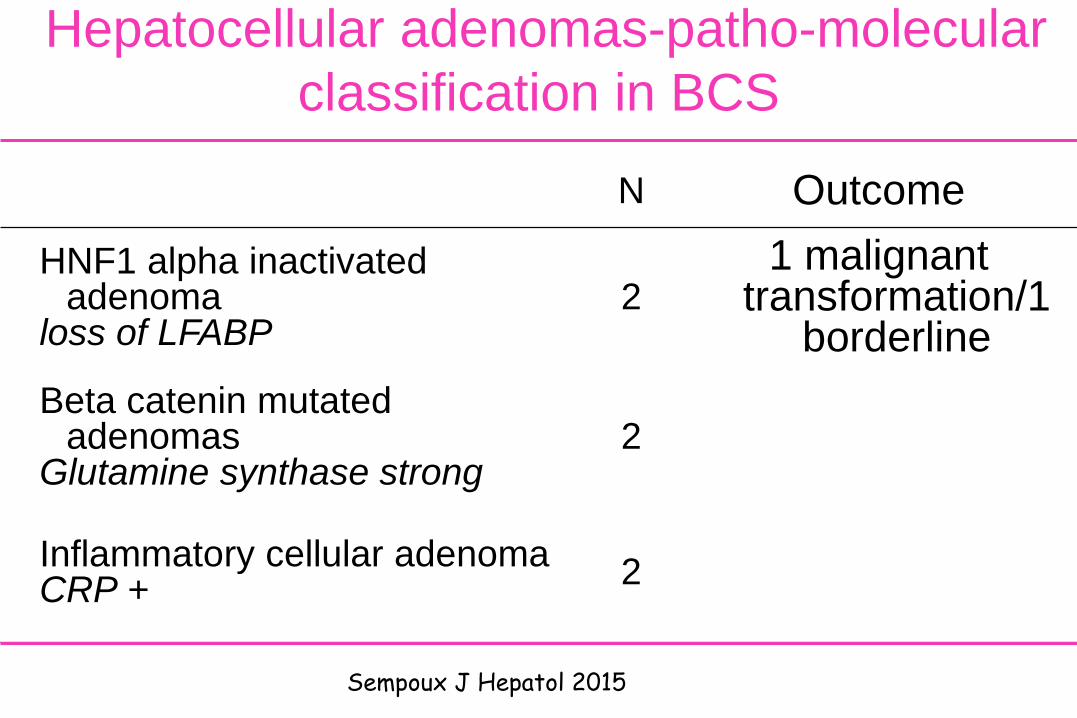
Hepatocellular adenomas-patho-molecular
classification in BCS
N Outcome
HNF1 alpha inactivatedadenoma
loss of LFABP2
1 malignanttransformation/1
borderline
Beta catenin mutatedadenomas
Glutamine synthase strong2
Inflammatory cellular adenomaCRP +
2
Sempoux J Hepatol 2015
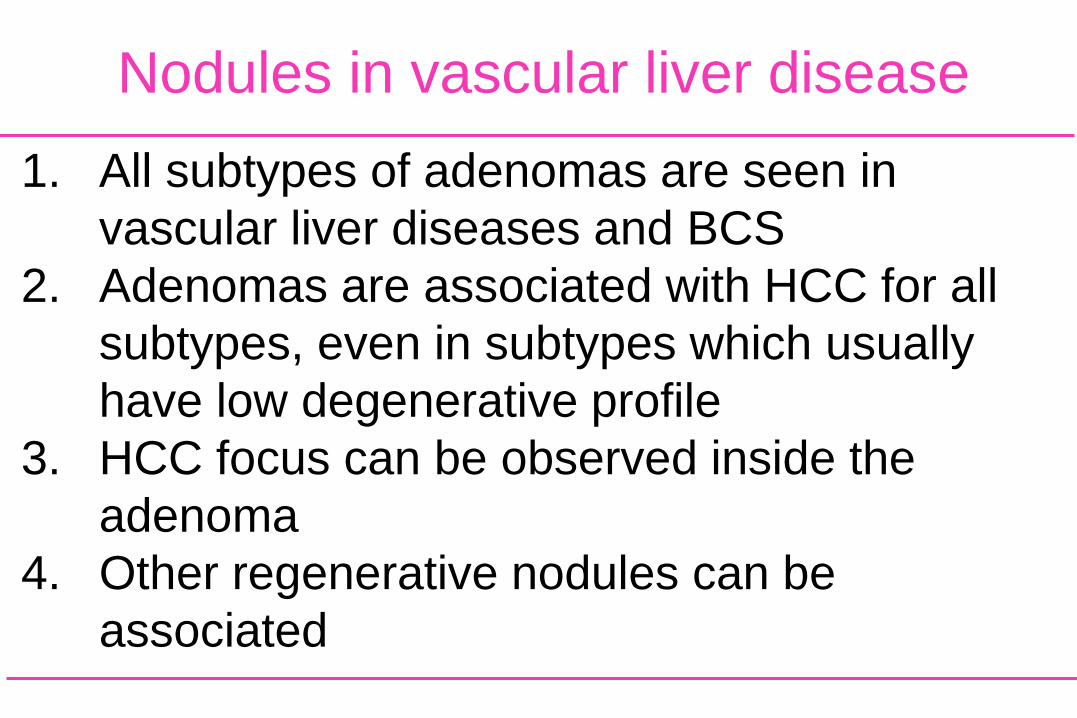
1. All subtypes of adenomas are seen in
vascular liver diseases and BCS
2. Adenomas are associated with HCC for all
subtypes, even in subtypes which usually
have low degenerative profile
3. HCC focus can be observed inside the
adenoma
4. Other regenerative nodules can be
associated
Nodules in vascular liver disease

1. Initiate therapy for complications of portal
hypertension as in cirrhosis (C2).
2. Treat all patients with BCS with
anticoagulation, in the absence of major
contraindications (A1).
3. Adequately treated portal hypertension
complications are not a contraindication for
anticoagulation (B1)
EASL guidelines 2015-Treatment

EASL guidelines 2015-Treatment and outcome
4. Consider brief interruption of anticoagulation for invasive procedure,
including paracentesis (B1)
5. Consider angioplasty/stenting first in patients with short hepatic vein
stenosis or IVC stenosis (A1).
6. Closely monitor these patients for early detection of liver deterioration.
Treat patients who do not respond to initial therapy or that are not
candidates, or do not respond to angioplasty/stenting with portal
derivative techniques (A1). TIPS, using PTFE-covered stents, is the
derivative treatment of choice (A1). Discuss surgical shunting when
TIPS is not feasible or fails (B1).
7. Propose liver transplantation as salvage treatment when derivative
techniques failed (A1). Anticoagulation needs to be continued after most
liver transplantation. (B1).
8. Screen patients for HCC. Distinct benign /malignant liver nodules is
very difficult (A1).

• Underlying blood disorder is the rule in the west, with myeloproliferative neoplasm in the first place.
• BCS to be considered – and assessed withDoppler-US – in any patient with liver disease.
Summary

Summary
• Good results of a therapeutic strategy based on minimal invasiveness and stepwise approach.
• Prognostication at baseline is not satisfactory.
• Long-term outcome jeopardized by malignancy(underlying blood disease and HCC).