-
8/10/2019 Tissue Layers and Incisions
1/19
Sterile means free of microorganisms including the pores while
asepsis means absence ofmicroorganisms that cause disease . Sterile
techniques are methods employed inside theoperating room to prevent
contamination of organisms throughout the surgical procedure.It is
very important for nurses to know and understand the principles
governing sterility topromote safety of the patient during
operation.
When are sterile techniques used or applied?
1. Preparation for an invasive procedure2. In preparation of the
sterile team to handle sterile supplies and contact to the
surgical site (gowning, gloving and scrubbing)
3. Skin preparation and draping of the patient
4.
Sterility maintenance throughout the operation
Principles of Sterility
Principle Number 1 : Only sterile items are used within the
sterile field.
Drapes, basins, sponges are obtained from a stock room with
sterile packages. Theinstruments used are sterilized and are placed
in a sterile table. Any person who holds thesterile equipments
should be very cautious to maintain sterility. One
importantconsideration in implementing sterility is this: IF YOU
ARE IN DOUBT ABOUT THE
STERILITY OF A CERTAIN OBJECT, CONSIDER IT UNSTERILE. Any
suspected or knownunsterile items should not be placed the sterile
field.
Any sterile package found in an unsterile or contaminated area
is consideredunsterile.
If the actual timing or sterilization procedure is undetermined
and the nurse isunsure about the sterilization process, the
equipments sterilized with the suspectedprocedure are considered
contaminated.
A sterile table which has been touch or rubbed accidentally by
an unsterile personor vice versa is no longer considered
sterile.
If the packaging material is broken or has missing pieces it is
no longer sterile.
Microorganisms can enter a packed sterile package when it is
damp or wet. Thus,damp packages are unsterile.
A sterile package dropped on a floor is considered
contaminated.
Principle Number 2: Sterile persons are gown and gloved.
When wearing a gown, the considered sterile area is the part
where you can see in frontdown to the level of the sterile field.
Thus, gowns are only considered sterile in front of the
-
8/10/2019 Tissue Layers and Incisions
2/19
chest, sleeves above the elbow to the cuffs down to the level of
the sterile field. Certainmethods should be employed in the OR:
Gowning is not done on the sterile table to avoid dripping water
onto the sterileequipments. Gloving and self-gowning should be done
in a distinct sterile surface.
Stockinette cuffs of the gowns are absorbent and may retain
moisture, thus makingit a suitable area for bacteria or
microorganisms to thrive in. because of the saidprinciple,
stockinette cuffs should be inserted beneath the sterile
gloves.
Principle Number 3 : Tables are only sterile at Table Level
Edges and sides of the table drape are considered contaminated.
Below the tablelevel is also considered unsterile.
Any sterile person who touches a part of the drape hanging below
the table level isconsidered unsterile. Any object or equipment
that drops below the table surface isconsidered contaminated.
In unfolding and placing a sterile drape any portion of that
falls below the tablesurface is unsterile and should not be moved
or touched or brought back up to thelevel of the table.
To prevent cords and tubing from sliding to the edge of the
table, it should befastened with a non-sharp device or object.
Principle Number 4: Sterile Persons Touch ONLY Sterile Items
while Unsterile ORPersonnel Touch Only Unsterile Items
Sterile OR personnel comes in direct contact with persons who
wears gowns andgloves only. The items that they will touch are the
sterile equipments. Any supply
brought by an unsterile staff should transfer the item in a
sterile manner. Unsterile OR personnel (circulator), should not
directly come in contact with a
gowned and gloved person.
Principle Number 5 : Unsterile persons avoid reaching over
sterile field and sterilepersons avoid touching or leaning over an
unsterile area.
In cases where a solution has to be poured into a sterile basin,
the unsterile ORpersonnel should only hold the lip of the bottle
over the basin to prevent any contactwith the sterile area.
To prevent the circulator from reaching over a sterile area when
pouring solutions,the scrub person places the basin and glasses or
any container for solutions near theedge of the table. This
prevents the circulator from reaching over the sterile area byjust
standing near the edge of the table to fill the container with the
liquid solution.
When surgeons perspire on their brows, he or she should to turn
away from thesterile field and have the sweat removed by the
circulator.
In draping or covering an unsterile table the scrub person drops
the sterile drape atthe center of the table while holding the
fan-folded drape high and standing backfrom the table to protect
the sterile gown.
-
8/10/2019 Tissue Layers and Incisions
3/19
Sterile gloves are protected by cuffing a drape. The sterile OR
personnel shouldplace the gloved hands inside the sterile part of
the drape.
The scrub person unfolds the drape towards him or herself first
to allow him or herto move closer to the table when working on the
opposite side of the table since thefirst part of the unfolded
drape now protects the sterile gown.
Principle Number 6: Edges of anything that encloses sterile
contents are consideredunsterile
Sterile supplies are packed. In opening sterile packages, the
area within 1 inch fromthe edges is considered unsterile. Supplies
are handled by the circulator. The upperportion of the package is
flapped away from the self and turns the side under. Indoing so,
the end of the flaps is secured by the band of the circulator to
prevent itfrom dangling loosely. The other flap is pulled towards
the circulator; hence, thecontents are exposed yet away from the
unsterile hands.
To open a sterile package, the flaps on peel-open packages
should be pulled not
torn. The sterile contents should be flipped and lifted upward.
The circulator shouldprevent the sterile contents to slide over the
unsterile edges.
When lifting contents from packages, sterile personnel should
lift the object straightup while holding their elbows high.
In cases where a sterile wrapper is used as a table cover
instead of a drape, it shouldcover the entire table surface. Only
the interior surface of the wrapper is consideredsterile.
Sterile bottles when opened cannot be recap without
contaminating the pouringedges. Thus, all contents must be used or
in cases where there is still a solution left,it should be
discarded.
Principle Number 7: Sterile field is set-up just before a
surgical procedure
The longer a sterile item is exposed to air and environment, the
higher thepossibility of contamination.
The practice of covering a sterile set-up does is not in the
best interest of the patient.Sterility cannot be guaranteed by just
covering a sterile set-up, unless it is under aconstant
surveillance.
Covering and uncovering a table may contaminate the sterile
items.
Principle Number 8: Sterile areas are continuously kept in
view.
Sterility cannot be guaranteed by just covering a sterile
set-up, unless it is under aconstant surveillance.
Sterile persons should face the sterile area. While waiting for
the patient to come inside the OR, someone must stay in the
sterile
area to maintain vigilance on the sterile set-up. Direct
observation ensures sterility.
Principle Number 9: Sterile persons keep well within sterile
area.
-
8/10/2019 Tissue Layers and Incisions
4/19
-
8/10/2019 Tissue Layers and Incisions
5/19
If any part of the package becomes damp or wet it is considered
unsterile andshould be discarded or re-sterilized.
Tables used for operation should be dried before draped. If the
sterile drape is soaked with a solution the wet area should be
covered with an
impermeable sterile towels or drape.
Sterile items should be placed not only in clean but also in dry
areas. In handling sterile packages, the hands should be dried
first. Air can also cause contamination. Thus, undue pressure on
sterile packs should be
avoided. This prevents the ejection of sterile air and the entry
of unsterile air intothe pack.
Principle Number 13: Microorganisms must be kept to irreducible
minimum
Sterilization is the process of removing ALL microorganisms
including the bacterial spores.However, not all things or area can
be sterilized. The following principles are employed toemploy
sterile technique in:
Skin
Skin cannot be sterilized thus, it can be very good source of
contamination in anyoperation. To prevent entrance of microorganism
to the patients wou nd the following aredone:
1. Surgical hand washing2. Chemical antisepsis of the skin
around the surgical site3. Gowning and gloving4. Application of
sterile draping.
Air
Air contains dust, droplets and shedding that may cause
contamination. Environmentalcontrol measures include:
1. Movement around the sterile field is kept to a minimum.2.
Drapes are not flipped and fanned to avoid the spread of dusts.3.
Talking inside the operating room is kept to a minimum because
moisture droplets
are expelled with force into the mask when a person is
talking.
-
8/10/2019 Tissue Layers and Incisions
6/19
Deciding the right type of surgical incision is extremely
important.
The ideal incision allows:
ease of access to the desired structures can be extended if
needed ideally muscles should be split rather than cut heals
quickly with minimal scarring
aesthetically pleasing
It is also important that incisions are placed in the direction
of lines of cleavage of the skin(Langer's lines) so that a hairline
scar is the outcome. These lines correspond to thedirection of
collagen fibres in the dermis and epidermis.
Incisions should also be placed as far as possible from stoma
sites in order to avoidinterfering with the stoma site and causing
complications such as retraction and prolapseof the stoma.
Surgical incisions on the abdomen can be divided into
transverse, vertical and
oblique incisions.
Vertical incision 1: Midline incision
Use : Virtually all abdominal procedures may be performed
through this incision.
-
8/10/2019 Tissue Layers and Incisions
7/19
Location: in the midline of the abdomen, and can extend from the
xiphoid process to justabove the umbilicus. It can be continued to
below the umbilicus by curving the incisionaround the
umbilicus.
Layers of the abdominal wall: skin, fascia (camper's and
scarpa's), linea alba,transversalis fascia, extraperitoneal fat and
peritoneum.
Advantages
1. Adequate exposure of most if not all of the abdominal
viscera2. Minimal blood loss as the incision is through the linea
alba
3. Minimal nerve injury4. Minimal muscle injury5. Can be quickly
made, such as in an emergency and quickly closed with a mass
closure
technique
Disadvantages
1. Care needs to be taken just above the umbilicus where the
falciform ligament is2. Midline scar
Vertical incision 2: Paramedian incision
Use: provides laterality to the midline incision, allowing
lateral structures such as thekidney, adrenals and spleen to be
accessed.
http://www.fastbleep.com/assets/notes/image/2228_1.jpg
-
8/10/2019 Tissue Layers and Incisions
8/19
Location: about 2- 5cm to the left or right of the midline
incision. Incision is over themedial aspect of the transverse
convexity of the rectus.
Layers of the abdominal wall: skin, fascia (camper's and
scarpa's) and the anterior rectussheath are incised. The anterior
rectus muscle is freed from the anterior sheath andretracted
laterally. The posterior rectus sheath (if above the arcuate line)
or transversalisfascia (if below the arcuate line), extraperitoneal
fat and peritoneum are then excisedallowing entry to the abdominal
cavity.
Advantages
1. Provides access to lateral structures2. Rectus muscle is not
divided3. Incisions in anterior and posterior sheath is seperated
by muscle which acts as a
buttress, therefore closure is more secure4. Can be extended by
a curvilinear incision towards the xiphoid process if required
Disadvantages
1. Takes longer to make and close2. Incision needs to be closed
in layers3. Difficult extension superiorly as limited by the costal
margin
http://www.fastbleep.com/assets/notes/image/2223_1.jpg
-
8/10/2019 Tissue Layers and Incisions
9/19
4. Tends to strip the muscles of their lateral blood and nerve
supply resulting in atrophy ofthe muscle medial to the incision
Vertical incision 3: Mayo-Robson incision
This is really a paramedian incision that has been curved
towards the xiphoid process. Itallows a bigger and wider opening.
Dissection continues in the same fasical planes as theparamedian
incision.
Transverse incision 1: Transverse incision
Use: right or left colon, duodenum, pancreas, subhepatic
space.
Location: This incision is made just above the umbilicus,
dividing one or both of the rectus
muscles.Layers of the abdomen: skin, fascia, anterior rectus
sheath, rectus muscle (+/- internaloblique, depending on the length
of the incision), transversus abdominus, transversalisfascia,
extraperitoneal fat and peritoneum. The medial aspect of this
incision will bethrough the layers just like as in the midline
incision.
http://www.fastbleep.com/assets/notes/image/2219_1.jpg
-
8/10/2019 Tissue Layers and Incisions
10/19
Advantages
1. Less pain than a midline incision2. Good access to midline
upper GI structures3. Transverse incisions cause the least amount
of damage4. As the recti have a segmental nerve supply, it can be
cut transversely without weakening
a denervated segment5. Muscular segments can be rejoined6.
Commonly used in children and the obese as greater abdominal
exposure is gained in
comparison with the vertical midline. This is due to the longer
transverse length of theabdomen in children and the obese.
Disadvantages
1. Limited lateral access in comparison with midline incisions
that can then be extended2. More wound infections compared to
midline thought to be due to greater difficulty in
controlling bleeding and haematoma formation.
Transverse incision 2: Subcostal incision
Use: gallbladder and biliary tract, spleen. It is also known as
the Kocher subcostal incision,after the person who discovered it.
With the roof top or Chevron modification, access to
http://www.fastbleep.com/assets/notes/image/2220_1.jpg
-
8/10/2019 Tissue Layers and Incisions
11/19
-
8/10/2019 Tissue Layers and Incisions
12/19
Use: This is the incision of most appendicetomies and can be
used in the left lowerquadrant in left sided colonic pathology.
Location: McBurney's point, as described by Charles McBurney in
1884, is two thirds fromthe umbilicus and a third from the right
anterior superior iliac spine. The incision isoblique beginning
laterally from above and ending medially.
If palpation reveals a mass, perhaps an appendiceal abcess, then
the incision is madedirectly over the mass.
Nowadays, the incision is made transverse and placed in a skin
crease, the so calledtransverse Lanz incision as this is more
aesthetically pleasing and the scar is hidden in thebikini
line.
If it is anticipated that the incision will need to be extended,
the oblique incision is usedwith lateral extension and as a muscle
splitting (gridiron) surgical technique. Musclesplitting involves
spitting the muscles fibres in a direction that is parallel to the
direction ofthe muscle fibres.
Layers of the abdominal wall: skin, fascia, internal oblique
medially and external obliquelaterally, transversus abdominus,
transversalis fascia, extraperitoneal fat and peritoneum.
Advantages
1. Aesthetically pleasing incisions as they both follow Langer's
skin lines
http://www.fastbleep.com/assets/notes/image/2225_1.jpg
-
8/10/2019 Tissue Layers and Incisions
13/19
2. A wide range of pathologies in the right and left lower
quadrants can be dealt with, withroom for extension if required
3. Minimal damage to muscles as muscle splitting techniques can
be utilised4. Avoids damage to local nerves
Disadvantages
1. The ilioinguinal and iliohypogastric nerves cross the
appendicectomy incision and thereis a risk of injury. This can then
predipose to inguinal hernia formation post-operatively.This is
more evident with the Lanz incision.
Transverse incision 4: Pfannenstiel incision
Use: Allows exploration of the lower GI and UT, as well as the
pelvic reproductive organs.
Location: A convex 12cm incision, located a the suprapubic skin
crease about 5cm abovethe pubic symphysis. Once the peritoneum is
reached, it is incised vertically, taking care toavoid the
bladder.
Layers of the abdominal wall: skin, fascia, anterior rectus
sheath, rectus muscle,transversalis fascia, extraperitoneal fat,
perineum.
NOTE: this incision is below the arcuate line and this there is
no posterior rectus sheath.
EXTRA: MAYLARD INCISION
This incision is placed a couple of cm's above the pfannenstiel
and also provides goodexposure of the pelvic organs. It cuts
through the rectus fascia and muscle as well asexternal and
internal obliques. Once transverse abdominus and transversalis
fascia arereached, a muscle splitting technique is employed.
-
8/10/2019 Tissue Layers and Incisions
14/19
Advantages
1. A convex incision is made instead of a transverse as this
parallels the course of thesegmental nerves that are cut and so
minimising muscle parasthesia and paralysis post-operatively. It
also follows the cleavage lines in the skin resulting in less
scarring
2. Location of incision means it is hidden in the pubic hair
line
Disadvantages
1. Limited exposure of the abdominal organs. Use of incision is
therefore restricted to thepelvic organs
2. High risk of injury to the bladder especially because the
fascia thins towards the lowerabdomen, leaving the bladder
relatively exposed, and if the bladder is not catheterisedduring
surgery
3. Extension of the incision is difficult laterally
4. Exploration of the deep pelvic organs is difficult making
dissection in the obese difficult
Oblique incision: Thoraco-abdominal incisions
http://www.fastbleep.com/assets/notes/image/2229_1.jpg
-
8/10/2019 Tissue Layers and Incisions
15/19
Thoracoabdominal incisions may be located in the RUQ or LUQ.
They convert the pleuraland peritoneal cavities into one. They
allow good access to the lungs, liver and spleen. Theleft incision
can also provide good exposure to the oesophagus and the
stomach.
Laporoscopic incisions
These incisions are small cuts in the skin made in the abdominal
wall to allow theinstruments of laparoscopy access to the contents
of the abdominal cavity.
Their location will depend on the organ being operated on.
Generally there will be 3-4.One is always at the umbilicus to allow
a port for the camera. The other incisions will belocated in one of
the 4 quadrants for tools such as the griper, cutting and
dissecting scissorsand so on.
http://www.fastbleep.com/assets/notes/image/2231_1.jpg
-
8/10/2019 Tissue Layers and Incisions
16/19
Care of the surgical incision
Surgical incisions may be closed with sutures, staples,
steri-strips or local tissue glue.
It is important to keep the wound site clean and incisions are
often covered with a
protective dressing. Patients are encouraged to keep the wound
as dry as possible to limitwound infection. Showering and bathing
can resume after a couple of days. Wounds thatare closed with
nonabsorbable sutures and staples require removal of these
materials first.
While gentle exercise is encouraged, it is important to avoid
pressure, pulling andstretching on wounds.
As wounds heal, it is common for patients to see their wounds
becoming itchy, red, swollenand wounds may even ooze
sero-sangiunous fluid. These all represent the healing process.It
is important to know what is normal so that abnormalities in wound
healing that mayrepresent infection, wound dehiscence, hypertrophic
and keloid scars may be detected.
http://www.fastbleep.com/assets/notes/image/2232_1.jpg
-
8/10/2019 Tissue Layers and Incisions
17/19
Tissue Layers
Tissue Layers: Skin, subcutaneous tissue, superficial fascia,
muscle, extraperitoneal fascia(deep fascia), peritoneum
Layers of the abdomen, from interior to exterior as follows:
peritoneum, extraperitonealfascia, muscle, deep fascia, superficial
fascia, subcutaneous tissuek and skin.
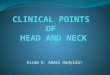
A: Fascial closure, B: Looping the 0-PDS at the vertex, C:
Continuous suture, D: Two PDSmeet in the middle of the incision,
tie together, and cut.
-
8/10/2019 Tissue Layers and Incisions
18/19
The skin is the largest organ of the body, with a total area of
about 20 square feet. The skinprotects us from microbes and the
elements, helps regulate body temperature, and permitsthe
sensations of touch, heat, and cold.Skin has three layers:
The epidermis, the outermost layer of skin, provides a
waterproof barrier andcreates our skin tone. The dermis, beneath
the epidermis, contains tough connective tissue, hair
follicles,
and sweat glands. The deeper subcutaneous tissue (hypodermis) is
made of fat and connective tissue.
The skins color is created by special cells called melanocytes,
which produce the pigmentmelanin. Melanocytes are located in the
epidermis.
The subcutaneous tissue is the third of the three layers of
skin. The subcutaneous layer
contains fat and connective tissue that houses larger blood
vessels and nerves. This layer isimportant is the regulation of
temperature of the skin itself and the body. The size of thislayer
varies throughout the body and from person to person.
Superficial fascia is found in the subcutis in virtually all
regions of the body, blending withthe reticular layer of the
dermis. It is present on the face, over the upper portion ofthe
sternocleidomastoid, at the nape of the neck, and overlying the
sternum. It is mainlyloose areolar connective tissue and adipose
and is the layer that primarily determines theshape of a body. In
addition to its subcutaneous presence, this type of fascia
surroundsorgans and glands, neurovascular bundles, and is found at
many other locations where it
fills otherwise unoccupied space. It serves as storage medium of
fat and water; as apassageway for lymph, nerve and blood vessels;
and as a protective padding to cushion andinsulate
Characteristics of muscle:
excitability - responds to stimuli (e.g., nervous impulses)
contractility - able to shorten in length extensibility - stretches
when pulled elasticity - tends to return to original shape &
length after contraction or extension
Functions of muscle:
motion maintenance of posture heat production
-
8/10/2019 Tissue Layers and Incisions
19/19
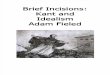
Types of muscle:
skeletal:o attached to bones & moves skeletono also called
striated muscle (because of its appearance under the microscope,as
shown in the photo to the left)o voluntary muscle
smooth (photo on the right)o involuntary muscleo muscle of the
viscera (e.g., in walls of blood vessels, intestine, &
other
'hollow' structures and organs in the body) cardiac:
o muscle of the hearto involuntary
Extraperitoneal fascia (deep fascia) fascial plane of mainly
loose areolar tissue betweenthe parietal peritoneum and the
internal muscular (iliopsoas and inner lamina ofthoracolumbar
fascia) and transversalis fascia of the body wall; its quality and
quantityvary considerably, being very thick and fatty posteriorly,
as pararenal fascia around thekidneys, but thin and fibrous
anteriorly, deep to the linea alba of the anterior
abdominalwall.
The peritoneum is the serous membrane that forms the lining of
the abdominal cavity orthe coelom it covers most of the
intra-abdominal (or coelomic) organs inhigher vertebrates and some
invertebrates (annelids, for instance). It is composed of alayer of
mesothelium supported by a thin layer of connective tissue. The
peritoneum bothsupports the abdominal organs and serves as a
conduit for thei rblood and lymph vesselsand nerves.
http://www.fastbleep.com/medical-notes/surgery/8/8/37
http://www.rnpedia.com/home/notes/medical-surgical-nursing-notes/principles-of-sterility
http://www.wikipedia.org/wiki/Serous_membranehttp://www.wikipedia.org/wiki/Abdomenhttp://www.wikipedia.org/wiki/Coelomhttp://www.wikipedia.org/wiki/Vertebratehttp://www.wikipedia.org/wiki/Invertebratehttp://www.wikipedia.org/wiki/Annelidhttp://www.wikipedia.org/wiki/Mesotheliumhttp://www.wikipedia.org/wiki/Connective_tissuehttp://en.wiktionary.org/wiki/conduithttp://www.wikipedia.org/wiki/Bloodhttp://www.wikipedia.org/wiki/Lymphhttp://www.wikipedia.org/wiki/Nerveshttp://www.fastbleep.com/medical-notes/surgery/8/8/37http://www.rnpedia.com/home/notes/medical-surgical-nursing-notes/principles-of-sterilityhttp://www.rnpedia.com/home/notes/medical-surgical-nursing-notes/principles-of-sterilityhttp://www.rnpedia.com/home/notes/medical-surgical-nursing-notes/principles-of-sterilityhttp://www.rnpedia.com/home/notes/medical-surgical-nursing-notes/principles-of-sterilityhttp://www.fastbleep.com/medical-notes/surgery/8/8/37http://www.wikipedia.org/wiki/Nerveshttp://www.wikipedia.org/wiki/Lymphhttp://www.wikipedia.org/wiki/Bloodhttp://en.wiktionary.org/wiki/conduithttp://www.wikipedia.org/wiki/Connective_tissuehttp://www.wikipedia.org/wiki/Mesotheliumhttp://www.wikipedia.org/wiki/Annelidhttp://www.wikipedia.org/wiki/Invertebratehttp://www.wikipedia.org/wiki/Vertebratehttp://www.wikipedia.org/wiki/Coelomhttp://www.wikipedia.org/wiki/Abdomenhttp://www.wikipedia.org/wiki/Serous_membrane