DISCUSS THORACIC INCISIONS
THORACIC INCISIONSINTRODUCTIONIncision;- Is a surgical wound
made by a surgeon on the skin, with intension of gaining access to
a lesion beneath or cavity.Such wounds created anywhere on the
chest (thoracic) wall is thoracic incisionAnatomy of the chest
CHEST WALLBony rib cage;- manubrum, sternum, 12 pair of rib,
coastal cartilage & thoracic vertebraeSoft tissue covering:-
muscles, neurovascular bundles, other connective tissuesTwo
apertureSuperior=root of the neckInferiorly=separated from
abdominal cavity by diaphragm
Types of thoracic incisionsSternotomyThoracotomyAxillary
thoracotomyAnterior mediastinotomyThoracoabdominal
incisionBilateral Trans-sternal thoracotomy( clam-shell
incision)Extra-thoracic approaches to the thorax
Sternotomy incisionsPartialHemisternotomy (spares 6-8cm
skin)CompleteSuprasternal notchxyphoid processCosmetically
appealing type of incision e.g inframammary (bikini type)
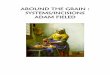
incisionMedian sternotomy incision
Sternal spreader applied
Median sternotomyIndicationsexposure of ant. & middle
mediastlower cervical proceduresTracheal resection&
reconstruction
Indications Excision of thyroid masses & parathyroid
adenomasExcision of cervical oesophageal tumoursExposure of heart
& great vesselsIn cardiopulmonary bypassAdvantagesQuick to
performExcellent exposureSafeHeals quicklyLess incisional
painDisadvantagesMany finds the vertical incision unsighty
Gives limited exposure of the lower chest & posterior
mediastinum
May lead to post-op complications-unsteable sternum,
infections
Technique Standard sternotomy
Open sternotomy
Re-operative sternotomyPartial sternal splitCLOSURE:Interlucking
wire suture technique
Less invasive sternotomy incisionsHemisternotomy- suprasternal
notch,tee-off to the R at interspace 4 or xyphoid,tee-off,R, at
interspace 2Full sternotomy with skin sparingBikini-type
(inframammary) incision- cosmesis Less invasive sternotomy
incisions
COMPLICATIONSAnaesthetic:- arrhythmias, laryngeal spasm
Specific :- Early;haemorrhage,injury to contiguous structures,
pneumothorax, haemothorax, Late;infection, empyema thoracis, post
surgery painComplications Mediastinitis
(S.aureu31%,E.coli3%,enterococcus 2%)Sternal osteomyelitisBrachial
plexus injury,incidence:1.4-6.5%
Thoracotomy Standard thoracotomy incisions
Defined arbitrarily in relation to the position of Latissismus
dorsi muscle,which is laterally sited on the chest wallTypes of
thoracotomy incisionsLateral Anterior
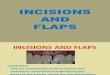
AnterolateralPosterolateralPosteriorothers
The numenclature for std thoracotomy incisions
Indications for posterolateral incisionStandard thoracotomy
incisions can be used for a wide range of surgical procedures
involving;The HeartOesophagusMediastinumIpsilateral lungAdvantages
Flexibility of the incision
Wide range of intra-thoracic exposure
Proven experience with these incisions has made them the
standard thoracic incisional approachDisadvantages Has potential
for poor exposure ,if wrong interspace is chosenUnilateral
hemithorax exposureIncisional painDisability related to division of
chest wall musclesDetrimental effect on pulmonary functionTechnique
(posterolateral)Induction using single/double lumen tube
Appropriate monitoringAnaesthesia-G.A+ETT
Positioning lateral decubitus position
Cleaning/drapping
Crescent or lazy-Sincision, transverselyDissected down &
scapular retractedPleural space enteredPleural/mediastinal
drainageThoracotomy closure
Option for entering the pleural space after posterolateral
thoracotomy
Intercostal approach-incising i.c muscles
Utilizing intercostal incision but to divide one or more ribsTo
resect a rib, enter through its periosteal bed
Anterior & anterolateral thoracotomyIndicationsHas greater
use historicallyUsed for pulmonary resectionCardiac
proceduresManagement of mediastinal massesOesophageal
pathologyTechnique Monittoring
Anaesthesia are same as posterolatral
Supine positionChest elevated at 30-45Curved submammary
incision, extended laterally(anterolateral) Anterolateral
thoracotomy incisions
Lateral thoracotomyWithin confines of latissimus dorsi
Transverse incision
1-2cm inferior to the scapularComplications Post thoracotomy
incision painWound infectionWound dehiscenceBronchopleural
fistula-8%Empyema thoracis-2.2%Muscle-sparing
thoracotomyIndications As in std thoracotomyVariant of std
thoracotomyWell establishedHas less complicationsMuscle sparing
anterolateral thoracotomy incision
Advantages Less early post-op painsGreater shoulder girdle
strengthMost result in quick closurePreserve chest wall
musclePrevent chest wall deformityAxillary
thoracotomyIndications1st rib disectionApical bleb DxMgt of
spontaneous pneumothorax with apical pleurectomy or
pleurodesisStaging of lung cancer
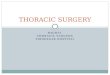
Patient positioning & incision for a vertical axillary
incision
ADVANTAGES Small incisionQuickly performedMuscle
sparingCosmetically appealingIdeal for pt with poor pulmonary
functionDisadv Limited exposureIntercostobrachial nerve
injuryProximal lung thorcic nerve injury
Complications Very minimal
Infection-0.7%
Limited shoulder mobility-0.5%Anterior mediastinotomy
(chamberlain procedure)Used in scalene lymph node biopsy
Exploratory thoracotomy
In cases of lung cancer( inoperable)Anterior
mediastinotomy(Chamberlain)
Thoracosternotomy(Clam shell)
Left thoracoabdominal incisionprovides excellent exposures for
procedures involving the spleenStomach L hemidiaphragm Aorta lower
oesophagusCurrent trendTowards minimally invasive
proceduresThoracic- VATS (video asst thoracoscopic surgery) e.g TEF
LIGATIONCardiac- OPCAB (off-pump coronary art. Bypass)MIDCAB (mini
invas dir coron art. Bypass)
Endoscopic aortic/mitral valve replacement