Embed Size (px)
Citation preview

THYROID DISORDERSAbdelaziz Elamin. MD, PhD, FRCPCHProfessor of Child HealthConsultant Pediatric EndocrinologistSultan Qaboos University, Oman

HYPOTHYROIDISM-EPIDEMIOLOGY
• Neonatal screening reveals incidence that varies between 1-5/1000 live births
• The most common cause of preventable mental retardation in children
• Both acquired & congenital forms are linked to iodine deficiency
• Diagnosis is easy & early treatment is beneficial

ETIOLOGY
•CONGENITALHypoplasia & mal-descentFamilial enzyme defectsIodine deficiency (endemic cretinism)Intake of goitrogens during
pregnancyPituitary defectsIdiopathic

ETIOLOGY /2
•ACQUIREDIodine deficiencyAuto-immune thyroiditisThyroidectomy or RAI therapyTSH or TRH deficiencyMedications (iodide & Cobalt)Idiopathic

KILPATRIK GRADING OF GOITRE
• Grade 0: Not visible neck extended & Not palpable
• Grade 1: Not visible, but palpable• Grade 2: Visible only when neck
is extended & on swallowing,
• Grade 3: Visible in all positions• Grade 4: Large goiter

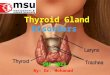
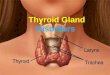
THYROID GLAND
• Derived from pharyngeal endoderm at 4/40
• Migrate from base of the tongue to cover the 2&3 tracheal rings.
• Blood supply from ext. carotid & subclavian and blood flow is twice renal blood flow/g tissue.
• Starts producing thyroxin at 14/40.

OVERVIEW (2)
• Maternal & fetal glands are independent with little transplacental transfer of T4.
• TSH doesn’t cross the placenta.• Fetal brain converts T4 to T3 efficiently.• Average intake of iodine is 500 mg/day.
70% of this is trapped by the gland against a concentration gradient up to 600:1

THYROID HORMONES• Iodine & tyrosine form both T3 & T4 under
TSH stimulation. However, 10% of T4 production is autonomous and is present in patients with central hypothyroidism.
• When released into circulation T4 binds to:Globulin TBG 75%Prealbumin TBPA 20%Albumin TBA 5%

THYROID HORMONES (2)
• Less than 1% of T4 & T3 is free in plasma.
• T4 is deiodinated in the tissues to either T3 (active) or reverse T3 (inactive).
• At birth T4 level approximates maternal level but increases rapidly during the first week of life.
• High TSH in the first 5 days of life can give false positive neonatal screening

TSH Is a Glico-protein with Molecular Wt
of 28000 Secreted by the anterior pituitary
under influence of TRH It stimulates iodine trapping,
oxidation, organification, coupling and proteolysis of T4 & T3
It also has trophic effect on thyroid gland

TSH (2) T4 & T3 are feed-back regulators of TSH TSH is stimulated by a-adrenergic
agonists TSH secretion is inhibited by:
DopamineBromocreptineSomatostatinCorticosteroids

THYROID HORMONES (3)
Conversion of T4 to T3 is decreased by:Acute & chronic illnessesb-adrenergic receptor blockersStarvation & severe PEMCorticosteroidsPropylthiouracilHigh iodine intake (Wolff-Chaikoff effect)

THYROXINE (T4)
Total T4 level is decreased in:Premature infantsHypopituitarismNephrotic syndromeLiver cirrhosisPEMProtein losing entropathy

THYROXINE (2) Total T4 is decreased when the
following drugs are used:SteroidsPhenytoinSalicylatesSulfonamidesTestosteroneMaternal TBII

THYROXINE (3) Total T4 is increased with:
Acute thyroiditisAcute hepatitisEstrogen therapyClofibrateiodidesPregnancyMaternal TSI

FUNCTIONS OF THYROXINE
Thyroid hormones are essential for:Linear growth & pubertal developmentNormal brain development & functionEnergy productionCalcium mobilization from boneIncreasing sensitivity of b-adrenergic
receptors to catecholeamines

CLINICAL FEATURESGestational age > 42 weeksBirth weight > 4 kgOpen posterior fontanelNasal stuffiness & dischargeMacroglossiaConstipation & abdominal
distensionFeeding problems & vomiting

CLINICAL FEATURES (2)• Non pitting edema of lower limbs &
feet• Coarse features• Umbilical hernia• Hoarseness of voice• Anemia• Decreased physical activity• Prolonged (>2/52) neonatal jaundice

CLINICAL FEATURES (3)
• Dry, pale & mottled skin• Low hair line & dry, scanty hair• Hypothermia & peripheral cyanosis• Hypercarotenemia• Growth failure• Retarded bone age• Stumpy fingers & broad hands

CLINICAL FEATURES (5)
• Skeletal abnormalities:Infantile proportionsHip & knee flexionExaggerated lumbar lordosisDelayed teeth eruptionUnder developed mandibleDelayed closure of anterior fontanel

OCCASIONAL FEATURES
• Overt obesity• Myopathy & rheumatic pains• Speech disorder• Impaired night vision• Sleep apnea (central & obstructive)• Anasarca• Achlorhydria & low intrinsic factor

OCCASIONAL FEATURES (2)
• Decreased bone turnover• Decreased VIII, IX & platelets
adhesion• Decreased GFR & hyponatremia• Hypertension• Increased levels of CK, LDH & AST • Abnormal EEG & high CSF protein• Psychiatric manifestations

ASSOCIATIONS
• Autoimmune diseases (Diabetes Mellitus)
• Cardiomyopathy & CHD• Galactorrhoea• Muscular dystrophy +
pseudohypertrophy (Kocher-Debre-Semelaigne)

GOITROGENS•DRUGS
Anti-thyroidCough medicinesSulfonamidesLithiumPhenylbutazonePASOral hypoglycemic agents

GOITROGENS
FOODSoybeansMilletCassavaCabbage

CLINICAL FEATURES (4)
Neurological manifestationsHypotonia & later spasticityLethargyAtaxiaDeafness + MutismMental retardationSlow relaxation of deep tendon jerks

CONGENITAL HYPOTHYRODISM
• Primary thyroid defect: usually associated with goiter.
• Secondary to hypothalamic or pituitary lesions: not associated with goiter.
• 2 distinct types of presentation:Neurological with MR-deafness & ataxiaMyxodematous with dwarfism &
dysmorphism

DIAGNOSIS
• Early detection by neonatal screening
• High index of suspicion in all infants with increased risk
• Overt clinical presentation
• Confirm diagnosis by appropriate lab and radiological tests

LABROTARY FINDINGS• Low (T4, RI uptake & T3 resin uptake)• High TSH in primary hypothyroidism• High serum cholesterol & carotene levels• Anaemia (normo, micro or macrocytic)• High urinary creatinine/hydroxyproline
ratio• CXR: cardiomegaly• ECG: low voltage & bradycardia

IMAGING TESTS
X-ray films can show:Delayed bone age or epiphyseal
dysgenesisAnterior peaking of vertebraeCoxavara & coxa plana
Thyroid radio-isotope scan Thyroid ultrasound CT or MRI

TREATMENT (2)
• L-Thyroxin is the drug of choice. Start with small dose to avoid cardiac strain.
• Dose is 10 g/kg/day in infancy. In older children start with 25 g/day and increase by 25 g every 2 weeks till required dose.
• Monitor clinical progress & hormones level

TREATMENT
Life-long replacement therapy 5 types of preparations are available:
L-thyroxin (T4)Triiodothyronine (T3)Synthetic mixture T4/T3 in 4:1 ratioDesiccated thyroid (38mg T4 & 9mg
T3/grain)Thyroglobulin (36mg T4 & 12mg T3/grain)

THYROID FUNCTION TESTS
1. Peripheral effects:BMR
Deep Tendon Reflex
Cardiovascular indices (pulse, BP, LV function tests)
Serum parameters (high cholesterol, CK, AST, LDH & carcino-embryonic antigen)

THYROID FUNCTION TESTS (2)
2. Thyroid gland economy:Radio iodine uptake
Perchlorate discharge test (+ve in Pendred syndrome & autoimmune thyroiditis)
TSH level
TRH stimulation tests
Thyroid scan

THYROID FUNCTION TESTS (3)
3. Tests for thyroid hormone:
Total & free T4 & T3
Reverse T3 level
T3 Resin Uptake
T3RU x total T4= Thyroid Hormone
Binding Index (formerly Free Thyroxin
Index)

THYROID FUNCTION TESTS (4)
Special Tests:Thyroglobulin levelThyroid Stimulating ImmunoglobulinThyroid antibodiesThyroid radio-isotope scanThyroid ultrasoundCT & MRIThyroid biopsy

PROGNOSIS
Depends on:Early diagnosis
Proper diabetes education
Strict diabetic control
Careful monitoring
Compliance

MYXOEDMATOUS COMA
Impaired sensorium, hypoventilation bradycardia, hypotension & hypothermia
Precipitated by:InfectionsTrauma (including surgery)Exposure to coldCardio-vascular problemsDrugs

PROGNOSIS Is good for linear growth & physical
features even if treatment is delayed, but for mental and intellectual development early treatment is crucial.
Sometimes early treatment may fail to prevent mental subnormality due to severe intra-uterine deficiency of thyroid hormones