Embed Size (px)
Citation preview

Thyroid Disorders
Tapan A. Patel
Cuong Nguyen
Mona Jamaldinian

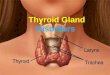
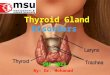
Thyroid Gland Second largest endocrine gland in body Small butterfly shaped gland located at
base of neck below the sternocleidomastoid muscles
Thyroid is controlled
by the hypothalmus
and pituitary

Functions Stimulates & maintains metabolic processes
Produces thyroid hormones T3-triiodothyronine and T4-thyroxine
These hormones regulate metabolism & affect the growth and function of other systems in the body
Secretes calcitonin to lower serum calcium levels
Parathyroid gland secretes PTH to raise serum calcium levels

Functions Metabolic stimulants of:
Neural and skeletal development Oxygen consumption at rest Stimulating bone turnover by increasing formation and
resorption Promoting chronitropic and ionotropic effects Increasing number of catecholamine receptors in heart Increasing production of RBC Altering the metabolism of carbs, fats, and protein

Hormones: T3 & T4
T3 (Triiodothyronine) & T4 (TetraiodothyronineStored in Follicles (round sacs) in the thyroid
filled with thyroglobulin, a thyroid protein. Dietary iodine enters follicles where they are
stored as T3 and T4
T4 is converted to T3 by peripheral organs such as kidney, liver, and spleen
T3 is 10x more active than T 4

Hormones: T4 to T3
Only 20% of total T3 is secreted by thyroid Majority is formed from catalysis of T4 by 5’-
iodthryonine deiodinase (highest activity in liver and kidney)

Hormones: T4 T4-thyroxine contains 4 iodine atoms It is a slow-acting pre-hormone T4 takes 4 days to peak in blood
Half-life 7 days Overall effects take 6 weeks T3 is the active and faster-acting hormone The immediate effects of T3 last 1-2 days
Half-life 1.5 days

Iodine Dietary Iodide is removed from the bloodstream by
means of an active pump The pump can concentrate iodide in the follicular
sacs at 350x greater than the blood concentration Oxidation of iodide by thyroid peroxidase converts
iodide iodine Peripheral de-iodination of T4 to T3 is regulated by
many factors including health, nutritional status, and other hormones

Hormones- TSH TSH
TSH is a pituitary hormone Controlled by TRH-thyrotropin releasing hormone from
hypothalamusFunctions to stimulate thyroid hormone production
May enlarge thyroid (goiter) when under producing
Labs: High TSH indicates low thyroid hormone= hypo Low TSH indicates high thyroid hormone = hyper

Hormones-Calcitonin & PTH
Produced by thyroid to regulate serum calcium levels
Calcitonin stimulates movement of calcium into bone
Parathyroid hormone (PTH) opposite effect of calcitonin

Negative Feedback System
TRH
T3 & T4 Thyroid
TSH
The disruption of any of these mechanisms can cause abnormal levels of T3 and T4 leading to thyroid disease

Diseases Hypothyroidism-Under Activity Prevalence
Affects 5-17% of population Females> Males Higher in >60 years old
Types Hashimoto’s thyroiditis Ord’s thyroiditis Postoperative hypothyroidism Postpartum hypothyroidism Iatrogenic hypothyroidism

Diseases Hyperthyroidism- Over activity Prevalence
Affect 5-17% of population Females> Males More common in younger persons
Types Thyroid storm Graves disease Toxic thyroid nodule Plummers disease Hashitoxicosis De Quervain thryoiditis Iatrogenic hyperthyroidism

Labs
Thyroid Function Test
Measurement Normal Range
Total T4 (TT4) Bound & Free T4 4.5-12.5mg/dL
Free T4 (FT4) Free T4 0.8-1.5 ng/dL
Total T3 (TT3) Bound & Free T3 80-220ng/dL
T3 Resin Uptake Binding capacity of TBG
22-34%
TSH Thyroid stimulating hormone
0.25-6.7U/mL
Total(T3) Bound & Free T3 80-220ng/dL

Labs
HyperthyroidismFT4 TSH
HypothyroidismFT4 TSH

Hyperthyroidism-Types
Graves diseaseMost common form (70-80%)
Autoimmune disorder in which thyroid-stimulating antibodies are circulating in blood. These bind to thyroid cells and activate cells in the same manner as TSH.
7 times greater in womenPeak onset is 20-30’s

Hyperthyroidism-Types
Can be caused by:Toxic multinodular goiterSolitary toxic noduleThyroiditisDrug-induced thryotoxicosisPituitary or trophoblastic tumors

Hyperthyroidism-Symptoms
Weight loss Tachycardia Bulging eyes Nervous/Anxious Insomnia Intolerant of heat Goiter

Goiter A diet deficient in
iodine Increase in thyroid
stimulating hormone (TSH) in response to a defect in normal hormone synthesis within the thyroid gland.

Thyroid Storm Life threatening syndrome Decompensated hyperthyroidism Symptoms
Hyperthyroid symptoms with agitation, confusion, delirium, psychosis
Gastrointestinal: Nausea/Vomiting, Abdominal pain
Tachycardia associated with CHF

Thyroid Storm Treatment Antithyroids
PTU 200-400mg po/NG q4-8h Methimazole 60-120mg/d PO/NG divided q6-8h
Potassium Iodide 2-5 drops PO/NG q6h Lugol Solution-Strong Iodine10 drops po TID Glucorticoids: block conversion of T4 to T3
Hydrocortisone succinate 100-200mg IV q6-8 Dexamethasone 2mg Po/IV q6-8h
BB Esmolol: 500mcg/kg/min Propranolol 20-80mg/dose PO/NG q4-6h

Hyperthyroidism-Treatment
Drug TherapyBeta blocker
Atenolol 50mg-100mg po daily Propranolol 20-40mg po TID
Antithyroids Methimazole 15-30mg po daily Propylthiouracil (PTU) 300mg TID

Hyperthyroid-Treatment
Procedural TherapyRadionuclide albation of thyroid glandTotal thyroidectomy

Methimazole
Methimazole prevents peroxidase enzyme from coupling and iodinating the tyrosine residues on thyroglubulin. Reduces T3 & T4 production.
Dosage15-30mg PO daily

Methimazole Adverse Effects
Skin rashLoss of tasteGI upsetDrowsinessDecreased Platelets
antagonistic properties of Methimazole

Methimazole
Drug Interactions:Discontinue before treatment with radioiodine;
affects uptakeAmiodarone: Increases T3 and T4 serum
levelsWarfarin: enhanced due to vitamin K

Propylthiouracil -PTU Thio-urea derivative Preferred agent in pregnant women DOC for severe thyrotoxicosis Dosage
Adults: 300-450mg/day divided q8h Severe cases: 600-1200mg/day Maintenance dose 100-150mg/day divided q 8-12 hours
Drug Interactions Similar to Methimazole

PTU
Adverse reactionsRash ItchingHivesAgranulocytosisVasculitis

Carbimazole-UK Pro-drug converted to active form -methimazole Dosage
15-40mg PO daily until normal function Reduce to 5-15mg po daily maintenance dose
Adverse EffectsBone marrow suppressionNeutropeniaAgranulocytosis

Sodium Iodide I-131 (Iodotope) Quickly absorbed and taken up by thyroid No other tissue capable of retaining radioactive
iodine therefore low adverse effects Dose
Adult 75-150mCi/g of thyroid x estimated thyroid gland size
24hour radioiodine uptakeDiscontinue antithyroid therapy 3-4days before

Hypothyroidism Types:
Primary hypothyroidism Most common cause Failure of thyroid gland Occurs primarily in women aged 30-50 years old
Chronic autoimmune thyroiditis or Hashimotos disease is the most common primary hypothyroidism AND hypothyroidism overall
Secondary HypothyroidismTertiary HypothyroidismOther causes

Hypothyroidism-Symptoms
Fatigue Weight Gain Depression Dry skin Bradycardia Constipation Intolerant to cold

Hashimoto’s Disease
Autoimmune disorder in which antibodies are directed against a thyroid sites to : Inhibit thyroid peroxidase Inhibit effects of TSHStimulate thyroid growth

Hypothyroidism-Primary Drug induced
Amiodarone, lithium, thiocyanates, phenylbutazone, sulfonylureas, PTU & methimazole
IatrogenicSurgical removal of the thyroid gland and
radiation treatment

Primary Hypothyroidism
Thyroid gland failureDecrease T3 & T4 Increase TRH due to negative feedback Increased TSH due to decreased TRH

Secondary Hypothyroid
Pituitary failure Insufficient TSH release as a result of:
Pituitary tumors Surgery Pituitary radiation Pituitary necrosis Autoimmune mechanisms

Tertiary Hypothyroidism
Hypothalamic Failure- very rare Insufficient TRH release as a result of:
Trauma IrradiationTumors

Hypothyroidism-Treatment Drug Therapy
Levothyroxine Sodium-DOC synthetic T4 Adults 1-1.5mgc/kg/day orally initially, adjust as needed. Average dose
1.6-1.8mcg/kg/day Pediatrics 1-1.5mgc/kg/day. Average 4 mcg/kg/day
Thyroid (Armour) 30mg PO daily, increase 15mg q 2-3 week
Liotrix (Thyrolar) synthetic combo T3 & T4 Thyrolar 1/2 (6.25/25mcg) start1 tab daily , increase PRN q 2-3 weeks.
L-triiodothyronine (Cytomel) synthetic T3 25mcg PO daily/ increase 12.5-25mcg daily every 1-2 weeks

Hypothyroidism-Treatment
Adverse EffectsMIOsteopeniaHA
ContraindicatedAcute MITreatment of obesityUncontrolled HTN

Monitoring
Obtain baseline FT4, TSH, LFT, CBCs before initiation of therapy
Repeat FT4 and TSH after 4-6 weeks on therapy and 4-6 weeks after adjustments
Once euthyroid state obtain thyroid function test after 3-6 months