Embed Size (px)
Citation preview

Thyroid Disorders: 1Thyroiditis, Goitre and Solitory Thyroid Nodules
Professor Tariq WaseemDr. Hina Latif

Kohala Bridge AJK Pakistan

A 28 yrs old PGR in medicine seeks consultant advice for C/O low grade fever along with pain in throat and myalgia for last 1 week.
She also has difficulty in swallowing and hoarseness of voice. Swelling and neck pain was initially on one side of the neck but now involves both sides.
Pain worsens on swallowing and coughing.
Case scenario:1

Moist warm skin Pulse: 110 beats/minute A firm, hot and tender swelling present on the
anterior aspect of the neck with overlying erythema. Lymph nodes…. not enlarged. Diagnosis ?? Acute Thyroiditis
Examination:

A group of individual disorders that all cause thyroidal inflammation and, and result in different clinical presentations.
Can be acute, subacute or chronic.
Thyroiditis:

Hashimoto’s thyroiditis
Subacute thyroiditis
Acute/Infectious thyroiditis
Drug-induced thyroiditis
Radiation induced
Thyroiditis

Supprative thyroidits, Microbial inflammatory thyroiditis, Pyogenic thyroiditis or Bacterial thyroidits
Very rare 0.1-0.7 % of all the thyroiditis
Mostly in children and young adults between the ages of 20-40yrs.
Acute infectious thyroiditis:

Acute Thyroiditis Causes◦Bacterial (S. aureus, S. pyogenes) : 68%◦Fungal : 15% ◦Mycobacterial : 9% ◦Viral
May occur secondary to◦Pyriform sinus fistulae◦Pharyngeal space infections◦Persistent Thyroglossal remnants◦Thyroid surgery wound infections (rare)◦Repeated FNAs◦Upper RTI
More common in HIV

Symptoms
Systemic illness and constitutional symptoms Local symptoms…painful enlargement of the thyroid,
dysphagia, dysphonia and hoarseness of voice (due to compression of esophagus and recurrent laryngeal nerve). Transient signs and symptoms of Hyperthyroidism / Hypothyroidism. Symptoms usually resolve once the infection resolves

ESR WBC count T3, T4, TSH…normal ? Elevated thyroglobulin levels. Decreased radioactive iodine uptake. USG neck…shows abscess or swelling in the thyroid Gallium scan will be positive. Barium Swallow ? fistula connection to pyriform sinus. Fine needle aspiration in case of abscess.
Diagnostic work up:

Antibiotics. Surgical Drainage of abscess….If required. Removal of fistula Lobectomy for antibiotic resistant.
Treatment:

Usually from a viral infection Can be suppurative Presentation is a tender thyroid with fever and malaise Can have transient thyroid test abnormalities If transiently hyperthyroid (mild), sometimes managed
with beta-blockers Usually managed symptomatically
Thyroiditis

A 46 years old female presents in OPD with C/O
Painless midline neck swelling for last 6 months which is gradually increasing in size, she has loss of appetite, constipation, cold intolerance, low mood and generalized weakness.
Her elder sister, maternal cousin and two nieces have been suffering from some thyroid disease.
Diagnosis??
Case scenario:2

Hashimoto's Thyroiditis

Chronic autoimmune thyroiditis. Commonest cause of primary hypothyroidism in U.S Antithyroid antibodies are POSITIVE Antithyroid peroxidase: 90% Anti thyroglobulin “Spontaneous atrophic thyroiditis” term reserved for those with positive TSH receptor-Blocking antibodies Anti Nuclear Factor(ANF) may be positive in those
under 20 years of age.
Hashimoto thyroiditis:

Mostly in young and middle aged females Incidence 3.5 /1000 women vs 0.8/ 1000 men. Small, diffuse, firm or rubbery goitre. 25% hypothyroid at presentation.
Hashimoto thyroiditis:

Periodic follow up: Since hypothyroidism may develop.
For hypothyroidism: levothyroxine Replacement (0.05-0.2 mg orally daily).
Surgery: For compression symptoms.
Treatment:

Subacute thyroiditis Self-limiting thyroid condition.
A triphasic clinical course of hyperthyroidism, hypothyroidism, and return to normal thyroid function.
15-20% of patients presenting with thyrotoxicosis.
10% of patients presenting with hypothyroidism.

Common Recognized Forms of Subacute Thyroiditis.
Subacute granulomatous, subacute painful, or “de
Quervain thyroiditis .”
Lymphocytic thyroiditis (also known as subacute
painless thyroiditis).
Subacute postpartum thyroiditis.

Subacute Granulomatous Thyroiditis(de Quervain’s Thyroiditis)
Self limited disease Mostly post viral (Coxackie, mumps or adenovirus) Enlarged Gland, Tender Initial thyrotoxicosis lasting 4- 6 weeks due to increased
release of stored T3 and T4 from preformed colloid due to inflammation.
A period of hypothyroidism follows for 4-6 months as stores are depleted.
Follicles then recover and Euthyroid state ensues.

Subacute ThyroiditisDeQuervain’s, Granulomatous
Diagnosis◦ Elevated ESR◦Anemia (normochromic, normocytic)◦ Low TSH, Elevated T4 > T3,◦ Low Anti-Thyroid Peroxidase/Anti-Thyroglobulin antibodies.◦ Low Radioactive Iodine uptake (same as silent thyroiditis)

Treatment◦NSAID’s and salicylates.◦Oral steroids in severe cases(Prednisolone 40 mg OD for 3-4 weeks)◦Beta blockers for symptoms of hyperthyroidism, Iopanoic
acid for severe symptoms◦ Symptoms can recur requiring repeat treatment◦Graves’ disease may occasionally develop as a late sequel
Subacute ThyroiditisDeQuervain’s, Granulomatous

Lymphocytic thyroiditis Self limited disease
CAUSE:
Anti-thyroid antibodies, autoimmune disease
CLINICAL FEATURES:
Thyrotoxicosis followed by hypothyroidism.

A 27 year old lady who delivered a live healthy baby 3 months ago presents with restlessness, palpitation, fatigue. She reports 3 kg weight loss over past one month.
O/E Anxious looking young lady Pulse 100 bpm, BP 110/70 mmHg Mild diffuse goitre Non tenderLabs: Raised T4, Low TSHDiagnosis??
Case Scenario: 3

Post-partum thyroiditis Occurs in women after delivery. 2 Phases:
Over Active Phase. 1-4 months of delivery
Under Active Phase. 3- 8 months post partum
Mostly returns to normal state.

May be unmasking of previously unrecognized subclinical autoimmune thyroiditis.
Antithyroid antibodies may be positive in early pregnancy. Negligible Radio Iodine uptake on thyroid scan. Likely to reccur with subsequent pregnancies Eventually progresses to permanent hypothyroidism.
Post-partum thyroiditis

Riedel’s Thyroiditis Rare disease involving fibrosis of the thyroid gland
Diagnosis◦ Thyroid antibodies are present in 2/3◦ Painless goiter “woody”◦Open biopsy often needed ◦Associated with focal sclerosis syndromes (retroperitoneal,
mediastinal, retroorbital, and sclerosing cholangitis)
Treatment◦Resection for compressive symptoms◦ Chemotherapy with Tamoxifen, Methotrexate, or steroids
may be effective◦ Thyroid hormone only for symptoms of hypothyroidism

A 65 year old male presents with unexplained weight loss of 7 Kg over past 6 months, palpitation and sweating. He had a transient ischemic attack 4 years ago and was diagnosed to have lone atrial fibrillation and is taking Amiodarone 200 mg OD, Aspirin 75 mg OD and Warfarin 7.5 mg OD since then.
ECG shows Atrial Fibrillation T3 and T4 are elevated while TSH is undetectable.
Diagnosis??
Case Scenario: 4

Drug-induced thyroiditis CAUSE: Drugs include: amiodarone, lithium, interferons,
cytokines.
CLINICAL FEATURES: Either thyrotoxicosis or hypothyroidism.
DURATION AND RESOLUTION: Often continues as long as the drug is taken.

Amiodarone has structural analogy to T4 Each 200 mg tab has 75 mg of Iodine Normal daily requirement of Iodine is 125 microgram Cytotoxic to thyroid follicles 20% of those taking Amiodarone develop either hypothyriodism or
Thyrotoxicosis. Thyrotoxicosis Classified as Type I : Iodine induced excess hormone synthesis ( Treated with Antithyroid drugs) Type II: Thyroiditis due to cytotoxic effect ( treated with Steroids) Half life 50- 60 days, effects lasts longer Levo thyroxine for Hypothyroidism
Amiodarone induced Thyroiditis

Radiation induced Thyroiditis CAUSE:
1. Follows treatment with radioactive iodine for hyperthyroidism
2. external beam radiation therapy for certain cancers.
CLINICAL FEATURES:3. Occasionally thyrotoxicosis4. more frequently hypothyroidism.

Thyrotoxicosis is transient
hypothyroidism is usually
permanent
DURATION AND RESOLUTION

Bosporus Channel Istanbul Turkey

GOITRE…

Classification of Goitres
Simple goitre:- No hormonal abnormalities and therefore no systemic effects. -Either diffuse or nodular.Simple
Toxic goitre:-Increased in production of thyroid hormones.-Either diffuse (graves dis.) or nodular (single nodule or on the top of multinodular goiter.
Neoplastic goitre:
Either benign (adenoma) or malignant
Inflammatory goitre:As many thyroiditis presentation:-Subacute granulomatous-Autoimmune (hashimot’s)-Reidel-Acute supporative

Goitre Pathogenesis
◦ Iodine deficient areas Heterogeneous response to TSH Chronic stimulation leads to multiple nodules
◦ Iodine replete areas Thyroid follicles are heterogeneous in their growth and
activity potential Autopsy series show MNG >30%.

Thyroid function evaluation◦ TSH, T4, T3◦Overt hyperthyroidism (TSH low, T3/T4 high)◦ Subclinical hyperthyroidism (TSH low, T3/T4 normal)
Determination of thyroid state is key in determining treatment
Goitre

Clinical Assessment of Simple Goiter:
-Benign disease, colloid goiter, euthyroid , female (3rd -5th decade )-Presented as mild enlargement of the gland, most of the time asymptomatic.
-Complication might develop due to mass effect like tracheal compression or voice changes, but mostly asymptomatic.
-Acute development—Hemorrhage or cyst >> acute pain

Goitre: Investigations
1.Thyroid Function Tests2. X-Ray Neck & Chest / CT scan3.Ultrasound Neck4. Isotope Scan 5. FNAC

Isotope scanning:
The uptake by the thyroid of a low dose of either: -Radiolabelled iodine ( I 123)- technetium (Tc 99)will demonstrate distribution of activity in the whole gland.

Prevention and treatment:
1) Iodine uptake: Iodination of salt Food
2) T4 administration.
3) Thyroidectomy

Topkopi Museum Istanbul

SOLITARY NODULE THYROID
DISCRETE SWELLING IN AN OTHERWISE IMPALPABLE GLAND

Solitary thyroid nodule:
Are common, being a feature of many different thyroid diseases
The essential clinical problem, particularly when the lesion is Solitary, is to distinguish between Benign and Malignant disease (nodule).

NORMAL ULTRASOUND BENIGN NODULE ON US
Solitary / Dominant Nodule (Non – toxic)

Benign
◦ Colloid nodule◦Hashimoto’s thyroiditis◦ Simple or hemorrhagic cyst◦ Follicular adenoma◦ Subacute thyroiditis
Solitary Thyroid Nodule

Malignant – PrimaryFollicular cell-derived carcinoma:◦ Papillary Thyroid Carcinoma (PTC) ◦ Follicular Thyroid Carcinoma (FTC) ◦ Anaplastic Thyroid CarcinomaC-cell–derived carcinoma:◦Medullary Thyroid Carcinoma◦ Thyroid Lymphoma
Malignant – Secondary◦Metastatic Carcinoma
Solitary Thyroid Nodule

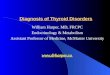
Thyroid Nodule
TSH test
Euthyroid Thyrotoxic
Thyroid scan
FNA Cold nodule Hot nodule
131 I or surgeryBenign Suspicious Malignant Inadequate
Observe or T4-Px Surgery Repeat FNAFU 6-12 M
Suggested strategy for the management of thyroid nodules

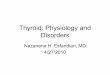
Thyroid scan images:
Cold nodule Hot nodule

Images of a large, asymmetric multinodular goiter. (A) Chest radiography shows marked tracheal deviation to the right (arrow). (B) Chest CT confirmed the presence of a large substernal goiter on the left to the level of tracheal bifurcation.

Other Imaging Techniques
PET scan:◦ 3-dimensional reconstruction images◦ Use in detecting primary and metastatic thyroid cancer◦ The clinical role of PET in pre-OP investigation of thyroid
nodules and in differentiating between benign and malignant lesions is controversial

US guided FNAC Indicated if:◦Palpation-guided FNA non diagnostic◦Complex (solid/cystic) nodule◦Palpable small nodule (<1.5 cm)◦ Impalpable nodule◦Abnormal cervical nodes◦Nodule with suspicious US features

Suspicious Cytology
Diagnosis cannot be made Inculdes: ◦Follicular neoplasms, ◦Hürthle cell neoplasms, ◦Atypical PTC, or ◦Lymphoma

Treatment
Hormone administration Very little evidence to affect benign nodule
Indications for surgeryClinical features and suspicious or definite FNAC
result.If continue enlarge despite TSH suppressionMechanical symptomsCosmetic
54

Emperor Jahangir TombLahore Pakistan