-
8/10/2019 Thyroid Disorders Seminar
1/86
PRESENTER : DR. MWANGA
-
8/10/2019 Thyroid Disorders Seminar
2/86
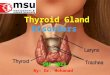
SURGICAL ANATOMY
Thyroid gland = shield like
sitelower part of the anterior and lateral
sides of the neck.
Gland contains right and left lobe joined by
Isthmus.
Vertebral levelC5,6,7,T1.
Each lobe extends from middle of thyroidcartilage to the 4thor
5thtracheal ring.
Isthmus2ndand 3rdtracheal ring.
-
8/10/2019 Thyroid Disorders Seminar
3/86
Contd
Dimensionslobe -5cms x 2.5cm x2.5cm.
Isthmus 1.5cm x1.5cms.
Weight20 to 25 grams in adults. Functional unit is lobule.
Each lobule is supplied by an arteriole.
2 capsulesTrue capsule.False capsule.
-
8/10/2019 Thyroid Disorders Seminar
4/86
-
8/10/2019 Thyroid Disorders Seminar
5/86
-
8/10/2019 Thyroid Disorders Seminar
6/86
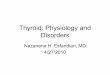
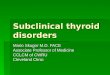
Normal anatomy of the recurrent laryngeal nerve. Note that on
the right
side the recurrent laryngeal nerve hooks around behind the
subclavian
artery, while on the left side this nerve passes around behind
the aortic
arch before ascending in the neck.B) When there is a vascular
anomaly of the right subclavian artery, the r
ecurrent laryngeal nerve no longer "recurs" around this artery
but
proceeds from the vagus nerve in a more transverse direction to
the
larynx. In such a situation, the nerve is much more likely to be
damaged
during operation unless care is taken to visualize its course in
the neck.
(From Skandalakis et al,:4 w ith permission.)
-
8/10/2019 Thyroid Disorders Seminar
7/86
BLOOD SUPPLY
1. Superior thyroid arteryfirst anterior branch of
the external carotid artery.its in close relation
with external laryngeal nerve. It divides in to
anterior and posterior branches. Suppliesupper 1/3rdof lobe and
upper of isthamus.
2. Inferior thyroid arterybranch of thyrocervical
trunck.its terminal part is in close relation with
recurrent laryngeal nerve.supplies lower 2/3rdof lobe and lower
of isthamus.
-
8/10/2019 Thyroid Disorders Seminar
8/86
Venous drainage
Superior thyroid vein drains in to internal
jugular vein or common facial vein.
Middle thyroid veininto internal jugular
vein .
Inferior thyroid veinLt brachiocephalic
vein.
Thyroid vein of kocherin to internal
jugular vein.
-
8/10/2019 Thyroid Disorders Seminar
9/86
Lymphatic drainage
Upper deep cervical lymph nodes .
Lower deep cervical lymph nodes.
NERVE SUPPLY:mainly by middle cervical ganglion and
partly from superior and inferior cervical
ganglia.
-
8/10/2019 Thyroid Disorders Seminar
10/86
PHYSIOLOGY
The hormones T3 and T4 are bound to
thyroglobulin within the colloid.
Synthesis within thyroglobulin complex is
controlled by several enzymes in
different steps1. Trapping
2.oxidation
3.coupling
4.Release
-
8/10/2019 Thyroid Disorders Seminar
11/86
THYROID HORMONES
Iodine & tyrosine form both T3 & T4under TSH
stimulation. However, 10%
of T4 production is autonomous and ispresent in patients with
centralhypothyroidism.
When released into circulation T4binds to:
Globulin TBG 75%
Prealbumin TBPA 20%
-
8/10/2019 Thyroid Disorders Seminar
12/86
THYROID HORMONES (2)
Less than 1% of T4 & T3 is free inplasma.
T4 is deiodinated in the tissues to
either T3 (active) or reverse T3(inactive).
At birth T4 level approximates
maternal level but increases rapidlyduring the first week of
life.
High TSH in the first 5 days of life cangive false positive
neonatal screening
-
8/10/2019 Thyroid Disorders Seminar
13/86
THYROID HORMONES IN SERUM
NAME SYMBOL NORMAL RANGE
Total serum
thyroxine
T4 55150 nmol/I
Total tri
iodothyronine
T3 1.23.1 nmol/I
Free thyroxine t4 826 pmol/I
Free tri-
iodothyronine
t3 39 pmol/I
-
8/10/2019 Thyroid Disorders Seminar
14/86
THYRIOD FUNCTION TEST
1. serum T3, T4.
2. Serum TSH
3. Serum creatinine
4. Serum cholesterol
5. Serum calcitonin
6. Thyroid autoantibody levels.
7. Thyroid scintigraphy .
8. TRH
-
8/10/2019 Thyroid Disorders Seminar
15/86
INVIVO TESTS
1. Radio iodine active uptake test.
2. Thyroid scan.
-
8/10/2019 Thyroid Disorders Seminar
16/86
Thyroid disorders.
1. Hypothyroidism
2. Goitres
3. Hyperthyroidism4. Neoplasams of the thyroid .
5. Thyroiditis .
-
8/10/2019 Thyroid Disorders Seminar
17/86
HYPOTHYROIDISM
ETIOLOGY AND CLASSIFICATION
1. Failure of thyroid development
a. complete- sporadic cretinism.
b.Partial2.Endemic cretinism
3.Iatrogenic a. After thyroidectomy
b.after radio iodine therapy
c.After pituitary ablation
d.Drug induced eg PAS, Iodide
-
8/10/2019 Thyroid Disorders Seminar
18/86
-
8/10/2019 Thyroid Disorders Seminar
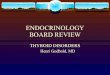
19/86CRETINISM
-
8/10/2019 Thyroid Disorders Seminar
20/86
MYXOEDEMA
A very advanced form of adult hypothyroidism.
CLINICAL FEATURES
SYMPTOMS1.Tiredness
2.mental lethargy
3.cold intolerence
4.increase in weight
5.constipation
6. menstrual disturbances
-
8/10/2019 Thyroid Disorders Seminar
21/86
Contd
Signs:
1. Carpal tunnel syndrome
2. Slow pulse rate
3. Dry skin4. Dry hair
5. Cold extremeties
6. Periorbital puffiness
7. Hoarse voice8. Slow movements
9. Sluggish ankle jerk
-
8/10/2019 Thyroid Disorders Seminar
22/86
-
8/10/2019 Thyroid Disorders Seminar
23/86
Cont.
Investigations:
1. Serum T4 levels below 55 nmol/l
2. Free T4 8 pmol/l
3. Radioiodine studies shows reducedthyroid uptake and increased
renalexcretion- less than 12% at 24 hours is
diagnostic4. ECGT wave flattened or inverted
5. TSH raised
-
8/10/2019 Thyroid Disorders Seminar
24/86
Treatment:
L-thyroxine is curative
A dose of 0.15 -0.2 mg/day
In elderly patients with Myocardialinsufficiency the initial
dose should be as
low as 0.05 mg per day.
If rapid or short lived response is essential,then
triiodothyronine is used
-
8/10/2019 Thyroid Disorders Seminar
25/86
GOITREENLARGED THYROID GLAND
Classifications of goitre
1. SIMPLE GOITRE (EUTHYROID)
Diffuse hyperplastic goitre Nodular goitre
Colloid goitre
Iron deficiency goitre Multinodular goitre
-
8/10/2019 Thyroid Disorders Seminar
26/86
Cont.
2. TOXIC GOITRE
Diffuse toxic goitre (Graves disease)
Toxic nodular goitre Toxic nodule
Secondary thyrotoxicosis in MNG
3. NEOPLASTIC GOITRE (BENIGN &MALIGNANT)
-
8/10/2019 Thyroid Disorders Seminar
27/86
CLASSIFICATION OF THYROID NEOPLASM
MALIGNANT
BENIGN
NEOPLASMS
FOLLICULAR ADENOMA
SECONDARY
METASTATIC
(BLOOD BORNE)
LOCAL INFILTRATION
PRIMARY
MALIGNANT LYMPHOMACARCINOMA MEDULLARY CA
DIFFERRENTIATED UNDIFFERENTIATED(ANAPLASTIC)
PAPILLARY FOLLICULAR
-
8/10/2019 Thyroid Disorders Seminar
28/86
4. INFLAMMATORY GOITRE
AutoimmuneChronic lymphocytic thyroiditis
Hashimotos disease
GranulomatousDe- Quervains thyroiditis
Fibrosing
Riedels thyroiditis
InfectiveAcute
Chronic Others
Amyloid
-
8/10/2019 Thyroid Disorders Seminar
29/86
SIMPLE GOITRE-Due to hyper stimulation of thyroid gland by
anterior
pitutary
Aeitiology
1. Iodine deficiency
-daily iodine requirement is 100-125 mcg-low iodine areas
-goitrogenic area
-failure of intestinal absorption
2. Defects in synthesis of thyroid hormone
-enzyme deficiency within thyroid gland
-goitrogens:- vegetables of brassica family e.g.cabbage, kale,
rap
-
8/10/2019 Thyroid Disorders Seminar
30/86
STAGES IN GOITRE FORMATION
1. Due to fluctuating TSH level a mixed pattern develops(active
and inactive lobules)
2. Active lobules become more vascular and hyperplasticuntil
haemorrhage occurs causing central necrosis andleaving only a
surrounding ring of active follicles
3. Necrotic lobules coalesce to form nodules.4. Persistent TSH
stimulation causes diffuse hyperplasia
and it is reversible if TSH stimulation ceases
5. Continual repetition of this process results in
nodulargoitre
Apart from TSH Growth stimulating immunoglobulin is
alsoresponsible for this process
-
8/10/2019 Thyroid Disorders Seminar
31/86
COLLOID GOITRE-SMOOTH SURFACE AND ROUND BORDERS
-
8/10/2019 Thyroid Disorders Seminar
32/86
DIFFUSE HYPERPLASTIC GOITRE
Children are affected in endemic areas
Sporadic cases in puberty where
metabolic demands are high
Stress and pregnancy
If TSH stimulation ceases the goitre may regress
-
8/10/2019 Thyroid Disorders Seminar
33/86
-
8/10/2019 Thyroid Disorders Seminar
34/86
Multinodular goitre
Is the end stage result of diffuse
hyperplastic goitre
Aetiopathogenesis
-Puberty goitre
-Pregnancy goitre
-Iodine deficiency goitre All these 3 types of goitres if left
untreatred
will change into multinodular goitre
-
8/10/2019 Thyroid Disorders Seminar
35/86
PUBERTY IODINE DEFICIENCY GOITROGENS
GENETIC FACTORS LOW LEVELS OF T3 AND
T4
TSH STIMULATION
MIXED PATTERN NECROSED FOLLICLESDIFFUSED HYPERPLASIA
MULTINODULAR GOITRE
MALIGNANCY TOXIC MULTINODULAR GOITRE
Feed back mechanism
After a few years
-
8/10/2019 Thyroid Disorders Seminar
36/86
Clinical features and diagnosis
Common in females Female : male ratio is 10:1
Age group is 20-40
Long duration of swelling in front of the neck
Dyspnoea, dysphagia
Gland is nodular, firm
Hard areas- calcification; soft areas- necrosis
Sudden increase in size with pain-haemorrhageThe most common
site of a nodule is at the junction of
isthmus with one lobe
-
8/10/2019 Thyroid Disorders Seminar
37/86
Investigations Thyroid profile
X-ray of the neck- AP and lateral view- Calcifications
- Deviation of trachea
- To rule out retrosternal extension-soft tissue
Isotope scan- can demonstrate 3 patterns:
a) Hot nodule- glands no uptake, nodule takes
b) Warm nodule- entire gland takes up isotope e.g typical
ofGraves disease
c) Cold nodule-nodules doesnt take up isotope Only 10% of the
cold nodules are malignant
Ultrasound scan
FNAC
-
8/10/2019 Thyroid Disorders Seminar
38/86
-
8/10/2019 Thyroid Disorders Seminar
39/86
PEMBERTONS SIGN
-
8/10/2019 Thyroid Disorders Seminar
40/86
TOXIC GOITRE
(thyrotoxicosis)
DEFINITION:
Its a complex disorders which occurs dueto increased levels of
thyroid hormones
and manifests clinically with various signs
and symptoms involving many body
systems.
-
8/10/2019 Thyroid Disorders Seminar
41/86
CLINICAL TYPES
Diffuse toxic goitre - Graves disease-
primary thyrotoxicosis
Toxic nodular goitre- secondary
thyrotoxicosis
Toxic nodule
others
-
8/10/2019 Thyroid Disorders Seminar
42/86
GRAVES DISEASE
The exact aetiopathogenesis is not known but
some positive aetiological factors
1. Autoimmune disorder-abnormal thyroid
stimulating antibodies2. Familial
3. Thyroid stimulating immuoglobulins and long
acting thyroid stimulators
4. Exopthalmos- opthalmopathy
5. Female, emotions, stress, young age
-
8/10/2019 Thyroid Disorders Seminar
43/86
-
8/10/2019 Thyroid Disorders Seminar
44/86
CLINICAL FEATURES
Primary thyrotoxicosis is more common in
females than males
Age: 15- 25 yrs
Loss of weight inspite of good apetite
Diarrhoea occurs due to smooth muscle
activity of small intestine
Intolerance to heat
Preference to cold
-
8/10/2019 Thyroid Disorders Seminar
45/86
Cont. Fine tremors
Excitability
Excessive sweating
Oligomenorrhoeafree steroid hormoneslevel decrease in graves
disease, this
results in decreased effective estrogen at
the cellular level which in turn causes
oligomenorrhoea
-
8/10/2019 Thyroid Disorders Seminar
46/86
GRAVES DISEASE
-
8/10/2019 Thyroid Disorders Seminar
47/86
-
8/10/2019 Thyroid Disorders Seminar
48/86
Cont. CNS signs
tremors of the tongue and the tongue is
within the oral cavity
- tremors of the outstretched hand- extensors are weak compared
to flexors
- always a moist warm hand (shake hand
and see)
CVS i
-
8/10/2019 Thyroid Disorders Seminar
49/86
CVS signs:
Pulse rate is always raised and rapid
indicating tachycardia
Depending upon the pulse rate
thyrotoxicosis is classified as follows:
Mild- 90100/ min
Moderate100110/min
Severe - >110/min
Palpitations and extra systoles
Fibrillations and cardiac failure are rare
-
8/10/2019 Thyroid Disorders Seminar
50/86
-
8/10/2019 Thyroid Disorders Seminar
51/86
-
8/10/2019 Thyroid Disorders Seminar
52/86
SEVERE GRAVES OPTHALMOPATHY
-
8/10/2019 Thyroid Disorders Seminar
53/86
THYROTOXIC MYOPATHY
Mild weakness of proximal limb muscles incommondifficulty in
climbing steps do
occur
Weakness of extraocular muscles resultsin double vision
(Diplopia)
Myopathy responds to antithyroid
treatment Features suggestive of myasthenia gravis
and periodic paralysis can be found
-
8/10/2019 Thyroid Disorders Seminar
54/86
SKIN CHANGES
Pretibial myxoedema- non pitting
Pruritis
Palmar erythema
Thinning of hair
Skin is dry and course
Thyroid acropachy
-
8/10/2019 Thyroid Disorders Seminar
55/86
-
8/10/2019 Thyroid Disorders Seminar
56/86
-
8/10/2019 Thyroid Disorders Seminar
57/86
INVESTIGATIONS
Routine inv- CCP, RBG,FBG, post-
prandial Blood sugar, urinalysis, CXR,
neck xray, indirect laryngoscopy
Serum T3, T4 are high and TSH is low
Thyroid antibodies are elevated
Sleeping PR remains high
Thyroid scan will show warm gland
-
8/10/2019 Thyroid Disorders Seminar
58/86
OF PRIMARY THYROTOXICOSIS
AIMS OF TREATMENT
1. To reduce the functioning thyroid mass
to a very critical level (about 6-8 gms of
thyroid tissues)
2. To minimize complications
To restore the patient to euthyroid state:
-
8/10/2019 Thyroid Disorders Seminar
59/86
To restore the patient to euthyroid state:
DRUGS DOSE PRECAUTION & SIDE
EFFECT
Carbimazole 10 mg 6 hrly
*M-10mg 2-3/day
Takes 2-3 wks for its
action
Propranolol 10-20 mg BD / TDS CCF,Bronchial asthma
Lugols iodine 10-20 drops TDS 10
days before surgery
Bitter taste, to be used
with orange juice
Potassiumperchlorate
200 mg TDS* M 200-400 mg OD
Propyl thiouracil 200 mg TDS
*M- maintanance
-
8/10/2019 Thyroid Disorders Seminar
60/86
PLEASE NOTE
Iodine containing anti-arrhythmic drug
AMIODARONEmay worsen
thyrotoxicosis.
Propyl thiouracilis safe in pregnancy withGraves disease.
Role of Lugols iodineis doubtful.
TO REDUCE THE FUNCTIONING
-
8/10/2019 Thyroid Disorders Seminar
61/86
TO REDUCE THE FUNCTIONING
THYROID MASS
Subtotal thyroidectomy
Radio iodine therapy
TO MINIMISE COMPLICATIONS
Good pre-op preparation
-
8/10/2019 Thyroid Disorders Seminar
62/86
ANTITHYROID DRUGS
ADVANTAGES:
No surgery
No radio active materials
DISADVANTAGES:Treatment is prolonged
failure rate is 50%
Some goitres become vascular and
enlarge
rarely dangerous drug reactions
-
8/10/2019 Thyroid Disorders Seminar
63/86
SURGERY
ADVANTAGES
Goitre is removed
cure is rapid
cure rate is high with adequate surgery DISADVANTAGES
Recurrence of thyrotoxicosis in < 5%
Post op thyroid insufficiency in 20 -45%
parathyroid insufficiency < 0.5%
nerve injury (ELN , RLN)
-
8/10/2019 Thyroid Disorders Seminar
64/86
surgery
1. Hemi thyroidectomy
2. Total thyroidectomy
3. Near total thyroidectomy
4. Subtotal thyroidectomy
5. Lobectomy
6. Isthumusectomy
-
8/10/2019 Thyroid Disorders Seminar
65/86
complications
1. Haemorrage
2. Respiratory obstruction
3. Recurrent laryngeal nerve paralysis
4. Thyroid insufficiency5. Parathyroid insuficiency
6. Throtoxic storm
7. Wound infection
8. Keloid scar
9. Stitch granuloma
-
8/10/2019 Thyroid Disorders Seminar
66/86
Post op follow up
1.indirect laryngoscopy
Serum calcitonin at 6 wks
Observation every 6 months for
recurrence
-
8/10/2019 Thyroid Disorders Seminar
67/86
-
8/10/2019 Thyroid Disorders Seminar
68/86
RADIO IODINE
ADVANTAGE:
No surgery
no prolonged drug therapy
DISADVANTAGE:
unavailability
thyroid insufficiency-70-80% after 10yrsan indefinite follow up
is essential
CHOICE OF THERAPY
-
8/10/2019 Thyroid Disorders Seminar
69/86
CHOICE OF THERAPY Diffused toxic goitre
over 45yrs-radioiodine
under 45 yrssurgery for large goitre
drugs for small goitre
Toxic nodular goitresurgery Toxic nodulesurgery is mainstay
radioiodine
for >45yrs
Recurrent thyrotoxicosis after adequate surgery:
> 45 yrsradioiodine,
-
8/10/2019 Thyroid Disorders Seminar
70/86
CLASSIFICATION OF THYROID NEOPLASM
MALIGNANT
BENIGN
NEOPLASMS
FOLLICULAR ADENOMA
SECONDARY
METASTATIC
(BLOOD BORNE)
LOCAL INFILTRATIONPRIMARY
MALIGNANT LYMPHOMACARCINOMA MEDULLARY CA
DIFFERRENTIATED UNDIFFERENTIATED(ANAPLASTIC)
PAPILLARY FOLLICULAR
SUMMARY OF MALIGNANT TUMOUR OF THYROID GLAND
-
8/10/2019 Thyroid Disorders Seminar
71/86
SUMMARY OF MALIGNANT TUMOUR OF THYROID GLAND
PAPILLARY FOLLICULAR ANAPLASTIC MEDULLARY
Etiology Irradiation Endemic goitre Unknown Sporadic
orfamilial
Incidence 60% 17% 13% 6%
Age 20-40 30-50 >50 Middle age
Dx Thyroid swelling
with LN
Thyroid swelling
with metastasis-
bone
Thyroid
swelling, local
fixity, stridor
Difficult to Dx
clinically
Microscop
ic
Orphan Annie-
eyed nuclei,psammoma
bodies
Angioinvasion,
capsular invasion
Poorly
differentiatedcells
Amyloid
stroma-likecarcinoid
Spread Lymphatic Blood Local
infiltration
Lymphatic,
blood
PAPILLARY FOLLICULAR ANAPLASTIC MEDULLARY
-
8/10/2019 Thyroid Disorders Seminar
72/86
Invx FNAC FROZEN
SECTION
FNAC,
BIOPSY
FNAC,
CALCITONIN
Rx of
1ONEAR TOTAL
THYROIDECT
OMY
NEAR TOTAL
THYROIDECTO
MY
ISTHMUSECT
OMY,EXT. RT
TOTAL
THYROIDECTO
MY
Rx of
mets
FUNCTIONAL
BLOCKDISSECTION
I 131OR EXT RT PALLIATIVE
EXT. RT
RADICAL
BLOCKDISSECTION
TSH
depende
nce
YES YES NO NO
Hormonal prod
VERY RARE VERY RARE NO CALCITONIN,
5-HT, ACTH
Px EXCELLENT GOOD WORST BAD
-
8/10/2019 Thyroid Disorders Seminar
73/86
-
8/10/2019 Thyroid Disorders Seminar
74/86
FOLLICULAR NEOPLASM
-
8/10/2019 Thyroid Disorders Seminar
75/86
-
8/10/2019 Thyroid Disorders Seminar
76/86
-
8/10/2019 Thyroid Disorders Seminar
77/86
-
8/10/2019 Thyroid Disorders Seminar
78/86
PAPILLARY CA PRESENTING AS SOLITARY NODULE
-
8/10/2019 Thyroid Disorders Seminar
79/86
PAPILLARY CARCINOMA
-
8/10/2019 Thyroid Disorders Seminar
80/86
-
8/10/2019 Thyroid Disorders Seminar
81/86
ULCERATED SECONDARIES IN THE SCALP BONE FROMFOLLICULAR CARCINOMA
THYROID
-
8/10/2019 Thyroid Disorders Seminar
82/86
-
8/10/2019 Thyroid Disorders Seminar
83/86
-
8/10/2019 Thyroid Disorders Seminar
84/86
SECONDARY DEPOSIT IN THE STERNUM IN A
PATIENT WHO UNDERWENT NEAR TOTAL
THYROIDECTOMY FOR FOLLICULAR CARCINOMA 5
YEARS AGO
Based on BIOLOGICAL AGGRESIVENESS 2 RISK group s:
-
8/10/2019 Thyroid Disorders Seminar
85/86
Based on BIOLOGICAL AGGRESIVENESS, 2 RISK group s:
Low Risk:
(F) < 50, (M) < 40 years
Papillary Ca, Follicular Ca (cytologically suspicious)Tumour
< 1.5 -2 cm, confined to one lobe, no metastases
SURGERY: LOBECTOMY
? Near to tal THYROIDECTOMY
Prognosis: Lobectomy ? Higher recurrence
No significant advantage in survival compared to TT
High Risk:Age: (F) > 50, (M) > 40 years
Larger, bilateral tumours or metastases
Papillary Ca (extrathyroidal)
Follicular Ca (widely invasive)
Medullary Ca
SURGERY: TOTAL THYROIDECTOMY
? Near tot al THYROIDECTOMY
+Lymphno de excis ion o f centra l nod es
+Modif ied radical neck dissect io n
LOW RISK
1.8% Mortality Rate
HIGH RISK
46% Mortality Rate
-
8/10/2019 Thyroid Disorders Seminar
86/86
Men under 41 and Women under 51
without distant metastasesAll patients with distant
metastases
All men over 41 and women over 51 with:
Intra-thyroidal papillarycancer (papillary cancer confined
present only within the thyroid gland) OR follicular
cancer tumor with minor capsular involvement
(the tumor slightly extends into the capsule which
surrounds it) AND
Primary tumor less than 5 cm in diameter AND
No distant metastases
All men over 41 and women over 51 with:
Extra-thyroidalpapillarycancer (extends beyond the
thyroid gland) OR follicular cancer tumor with
major capsular involvement (the tumor extends
significantly into the capsule which surrounds it)
AND/OR
Primary cancer is 5 cm in diameter or larger, regardless
of the extent of the disease
PROGNOSIS