Embed Size (px)
DESCRIPTION
22. P A R T A. The Respiratory System. Questions. 1. Why do we breath oxygen? What is the ultimate role of O2 in the body? 2. Why is the majority of our respiratory system inside our body?. Oxygen’s Journey. - PowerPoint PPT Presentation
Citation preview

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Human Anatomy & PhysiologySEVENTH EDITION
Elaine N. MariebKatja Hoehn
PowerPoint® Lecture Slides prepared by Vince Austin, Bluegrass Technical and Community College
C H
A P
T E
R
22The Respiratory System
P A R T A

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Questions 1. Why do we breath oxygen? What is the ultimate
role of O2 in the body? 2. Why is the majority of our respiratory system
inside our body?

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Oxygen’s Journey 98% of the O2 serves to make ATP by going inside
the mitochondrion and becoming the terminal acceptor of electrons in the Electron Transport Chain
2% unfortunately becomes free radicals causing unwanted oxidation

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 3.2

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 3.17

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 24.5

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 24.7

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 24.9

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 24.8
Cytochrome Oxidase

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Why is the majority of our respiratory system inside our bodies?
When living creatures left the waters and came to the terrestrial (land) environment – the respiratory system had to be internalized or “the respiratory epithelium would dry out.”
But still needed lots of surface area for enough diffusion of oxygen to supply the trillions of body cells in accordance with Fick’s Diffusion Equation
In order to not make body larger but still have lots of diffusion surface area – must branch the respiratory system inside the body – 70 meters squared –tennis court size

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
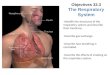
Respiratory System Consists of the respiratory and conducting zones Respiratory zone:
Site of gas exchange Consists of bronchioles, alveolar ducts, and alveoli

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Respiratory System Conducting zone:
Conduits for air to reach the sites of gas exchange Includes all other respiratory structures (e.g., nose,
nasal cavity, pharynx, trachea) Respiratory muscles – diaphragm and other
muscles that promote ventilation
PLAY InterActive Physiology ®: Anatomy Review: Respiratory Structures, page 3

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Respiratory System
Figure 22.1

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Upper vs. Lower Respiratory System The upper respiratory tract consists of the nasal
cavity (nose), pharynx, and the larynx. The "lower respiratory tract" consists of the lower part of the respiratory system. This consists of the trachea (wind pipe), bronchial tubes, bronchioles, and lungs. The upper and lower respiratory tracts make up our whole respiratory system and work in a synchronizing pattern to make it possible to breathe.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
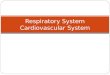
Major Functions of the Respiratory System To supply the body with oxygen and dispose of
carbon dioxide Respiration – four distinct processes must happen
Pulmonary ventilation – moving air into and out of the lungs
External respiration – gas exchange between the lungs and the blood

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Major Functions of the Respiratory System Transport – transport of oxygen and carbon dioxide
between the lungs and tissues Internal respiration – gas exchange between
systemic blood vessels and tissues

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
The Nose Composed of an external part Composed of an internal part – nostrils and other
features

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Function of the Nose The only externally visible part of the respiratory
system that functions by: Providing an airway for respiration Moistening and warming the entering air Filtering inspired air and cleaning it of foreign
matter Serving as a resonating chamber for speech Housing the olfactory receptors

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Structure of the Nose Nose is divided into two regions:
External nose, including the root, bridge, dorsum nasi, and apex
Internal nasal cavity Philtrum – a shallow vertical groove inferior to the
apex The external nares (nostrils) are bounded laterally
by the alae

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Structure of the Nose
Figure 22.2a

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Structure of the Nose
Figure 22.2b

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 7.2a

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 7.10a

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Internal Nose -- Nasal Cavity Lies in and posterior to the external nose Is divided by a midline nasal septum Opens posteriorly into the nasal pharynx via
internal nares The ethmoid and sphenoid bones form the roof The floor is formed by the hard and soft palates

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Inside the Nose 1. When first come into nose (Nasal Vestibule)–
you have the skin of the nose – covered by a non-keratinized stratified squamous epithelium with plenty sweat and oil glands plus Vibrissae (Nose hairs)
2. Come in further and find two types of mucous membranes
Olfactory mucous membrane – smell area
Respiratory mucous membrane – the other membrane

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Respiratory mucous membrane – covered by a ciliated pseudostratified columnar
epithelium with plenty of goblet cells interspersed. The lamina propria had many blood vessels and serous and mucous glands plus lots of lymphatics and white blood cells.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Nasal Mucosae

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Nasal Cavity Vestibule – nasal cavity superior to the nares
Vibrissae – hairs that filter coarse particles from inspired air
Olfactory mucosa Lines the superior nasal cavity Contains smell receptors

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Nasal Cavity Respiratory mucosa
Lines the balance of the nasal cavity Glands secrete mucus containing lysozyme and defensins to help
destroy bacteria Plasma cells that secrete IgE and IgA Mast Cells and other WBC’s Sneeze reflex areas Swell Bodies Kiesselbach’s Area - Capillary and Venous Plexuses

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Kiesselbach’s Area & Swell Bodies Kiesselbach’s Area - a region in the anteroinferior part of the
nasal septum, where four arteries anastomose to form a vascular plexus called Kiesselbach's plexus. usual site for epistaxis as it is exposed to drying effect of inspiratory current. Ninety percent of nose bleeds arise there.
Swell Bodies - The nasal swell body is a widened region of the septum located superior to the inferior turbinates and anterior to the middle turbinates, and of potential importance to the airflow-regulating nasal valve. Although little is known of this structure in terms of vasoreactivity and tendency to limit airflow by vascular engorgement, some consider the swell body to be physiologically analagous to the inferior turbinate.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Kiesselbach’s Area

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Nasal Cavity Inspired air is:
Humidified by the high water content in the nasal cavity
Warmed by rich plexuses of capillaries Ciliated mucosal cells remove contaminated mucus

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Nasal Cavity Superior, medial, and inferior conchae:
Protrude medially from the lateral walls Increase mucosal area Enhance air turbulence and help filter air
Sensitive mucosa triggers sneezing when stimulated by irritating particles

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Nasal Cavity
Figure 22.3b

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 7.7

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Functions of the Nasal Mucosa and Conchae During inhalation the conchae and nasal mucosa:
Filter, heat, and moisten air During exhalation these structures:
Reclaim heat and moisture Minimize heat and moisture loss

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Paranasal Sinuses Sinuses in bones that surround the nasal cavity Sinuses lighten the skull and help to warm and
moisten the air

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 7.11

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Pharynx Funnel-shaped tube of skeletal muscle that
connects to the: Nasal cavity and mouth superiorly Larynx and esophagus inferiorly
Extends from the base of the skull to the level of the sixth cervical vertebra

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Pharynx It is divided into three regions
Nasopharynx Oropharynx Laryngopharynx

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Nasopharynx Lies posterior to the nasal cavity, inferior to the
sphenoid, and superior to the level of the soft palate
Strictly an air passageway Lined with pseudostratified columnar epithelium Four entrances in nasopharynx – two internal nares
and two openings from the eustachian (auditory) tubes
Pharyngeal Tonsil – when enlarged is Adenoid

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15.25a

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Nasal Cavity
Figure 22.3b

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Lymphatics in Nasal and Oral Areas Waldeyer's tonsillar ring is an anatomical term describing the
lymphoid tissue ring located in the pharynx and to the back of the oral cavity.
It was named after the nineteenth century German anatomist Heinrich Wilhelm Gottfried von Waldeyer-Hartz.
The ring consists of (from superior to inferior): Pharyngeal tonsil (also known as 'adenoids' when infected) Tubal tonsils Palatine tonsils (commonly called "the tonsils" in the
vernacular, less commonly termed "faucial tonsils") Lingual tonsils

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Olfactory Mucosae How we smell

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Nasal Cavity
Figure 22.3b

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 7.7

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 15.21

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Nasopharynx Closes during swallowing to prevent food from
entering the nasal cavity The pharyngeal tonsil lies high on the posterior
wall Pharyngotympanic (auditory) tubes open into the
lateral walls

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Oropharynx Extends inferiorly from the level of the soft palate
to the epiglottis Opens to the oral cavity via an archway called the
isthmus of the fauces Serves as a common passageway for food and air

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Oropharynx The epithelial lining is protective stratified
squamous epithelium Palatine tonsils lie in the lateral walls of the fauces Lingual tonsil covers the base of the tongue

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Laryngopharynx Serves as a common passageway for food and air Lies directly posterior to the upright epiglottis Extends to the larynx, where the respiratory and
digestive pathways diverge

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Larynx (Voice Box) Attaches to the hyoid bone and opens into the
laryngopharynx superiorly About 2 inches in length extending from the 3rd to
6th cervical vertebrae Continuous with the trachea posteriorly The three functions of the larynx are:
To provide a patent airway To act as a switching mechanism to route air and
food into the proper channels To function in voice production

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Framework of the Larynx Cartilages (hyaline) of the larynx
Shield-shaped anterosuperior thyroid cartilage with a midline laryngeal prominence (Adam’s apple)
Signet ring–shaped anteroinferior cricoid cartilage Three pairs of small arytenoid, cuneiform, and
corniculate cartilages Epiglottis – elastic cartilage that covers the
laryngeal inlet during swallowing

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Framework of the Larynx
Figure 22.4a, b

Copyright © 2010 Pearson Education, Inc.
Figure 10.8a Muscles of the anterior neck and throat that promote swallowing.
MylohyoidAnteriorbellyPosteriorbelly
Stylohyoid (cut)ThyrohyoidThyroid cartilageof the larynx
Median raphe
Sternothyroid
StylohyoidHyoid boneOmohyoid(superior belly)SternohyoidSternocleido-mastoid Omohyoid(inferior belly)
Digastric
Thyroid gland
(a)

Copyright © 2010 Pearson Education, Inc.
Extrinsic Laryngeal MusclesInfrahyoid Group (Pull larynx and hyoid bone down)• Sternohyoid• Sternothyroid• Thyrohyoid• Omohyoid
Suprahyoid Group• Stylohyoid• Myohyoid• Digastric• Geniohyoid• Stylopharyngeas

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Internal Larynx

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Movements of Vocal Cords
Figure 22.5

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Vocal Ligaments Attach the arytenoid cartilages to the thyroid
cartilage Composed of elastic fibers that form mucosal folds
called true vocal cords The medial opening between them is the glottis They vibrate to produce sound as air rushes up
from the lungs

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Vocal Ligaments False vocal cords
Mucosal folds superior to the true vocal cords Have no part in sound production

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Vocal Production Speech – intermittent release of expired air while
opening and closing the glottis Pitch – determined by the length and tension of the
vocal cords Loudness – depends upon the force at which the air
rushes across the vocal cords The pharynx resonates, amplifies, and enhances
sound quality Sound is “shaped” into language by action of the
pharynx, tongue, soft palate, and lips

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Movements of Vocal Cords
Figure 22.5

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Intrinsic Laryngeal Muscles Cricothyroid muscles lengthen and stretch the vocal folds. Posterior cricoarytenoid muscles abduct and externally rotate
the arytenoid cartilages, resulting in abducted vocal cords. Lateral cricoarytenoid muscles adduct and internally rotate the
arytenoid cartilages, which can result in adducted vocal folds. Transverse arytenoid muscle adducts the arytenoid cartilages,
resulting in adducted vocal cords. Oblique arytenoid muscles narrow the laryngeal inlet by
constricting the distance between the arytenoid cartilages and epiglottis.
Vocalis muscles adjust tension in vocal folds. Thyroarytenoid muscles - sphincter of vestibule, narrowing the
laryngeal inlet.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Wave Description

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Sphincter Functions of the Larynx The larynx is closed during coughing, sneezing, and
Valsalva’s maneuver Valsalva’s maneuver
Air is temporarily held in the lower respiratory tract by closing the glottis
Causes intra-abdominal pressure to rise when abdominal muscles contract
Helps to empty the rectum Acts as a splint to stabilize the trunk when lifting
heavy loads

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Trachea Flexible and mobile tube extending from the
larynx into the mediastinum – about 4 inches long and ¾ inch wide
Composed of three layers Mucosa – made up of goblet cells and ciliated
epithelium Submucosa – connective tissue deep to the mucosa Adventitia – outermost layer made of C-shaped
rings of hyaline cartilage

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Trachea
Figure 22.6a

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Conducting Zone: Bronchi Carina of the last tracheal cartilage marks the end
of the trachea and the beginning of the bronchi Air reaching the bronchi is:
Warm and cleansed of impurities Saturated with water vapor
Bronchi subdivide into secondary bronchi, each supplying a lobe of the lungs
Air passages undergo 23 orders of branching
PLAY InterActive Physiology ®: Anatomy Review: Respiratory Structures, page 6

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Conducting Zone: Bronchial Tree Tissue walls of bronchi mimic that of the trachea As conducting tubes become smaller, structural
changes occur Cartilage support structures change Epithelium types change Amount of smooth muscle increases

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Conducting Zone: Bronchial Tree Bronchioles
Consist of cuboidal epithelium Have a complete layer of circular smooth muscle Lack cartilage support and mucus-producing cells

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Conducting Zones
Figure 22.7

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Respiratory Zone Defined by the presence of alveoli; begins as
terminal bronchioles feed into respiratory bronchioles
Respiratory bronchioles lead to alveolar ducts, then to terminal clusters of alveolar sacs composed of alveoli
Approximately 300 million alveoli: Account for most of the lungs’ volume Provide tremendous surface area for gas exchange

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Respiratory Zone
Figure 22.8a

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Respiratory Zone
Figure 22.8b

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Respiratory Membrane This air-blood barrier is composed of:
Alveolar and capillary walls Their fused basal laminas
Alveolar walls: Are a single layer of type I epithelial cells Permit gas exchange by simple diffusion Secrete angiotensin converting enzyme (ACE)
Type II cells secrete surfactant

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Alveoli Surrounded by fine elastic fibers Contain open pores that:
Connect adjacent alveoli Allow air pressure throughout the lung to be
equalized House macrophages that keep alveolar surfaces
sterile

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Respiratory Membrane
Figure 22.9b

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Respiratory Membrane
Figure 22.9c ,d

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Surfactant is secreted by the type II pneumonocytes Composition Lipids Over 90% of the surfactant is lipids; around half (50%) of
which is dipalmitoylphosphatidylcholine (DPPC). Phosphatidylcholine molecules form ~85% of the lipid in surfactant. Phosphatidylglycerol (PG) forms about 11% of the lipids in surfactant, it has unsaturated fatty acid chains that fluidize the lipid monolayer at the interface. Neutral lipids and cholesterol are also present. The components for these lipids diffuse from the blood into type II alveolar cells where they are assembled and packaged for secretion into secretory organelles called lamellar bodies.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Surfactant Reduces surface tension on alveolar surface Complex mixture of phospholipids, triglycerides,
fatty acids, and proteins Ps = 2T/r
Ps is pressure in a sphere As radius gets smaller the pressure in the sphere
gets greater – thus its air would empty into larger alveoli

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Proteins Proteins make up the remaining 10% of surfactant. Half of this
10% is plasma proteins but the rest is formed by the apoproteins SP-A (SFTPA1), B (SFTPB), C (SFTPC) and D (SFTPD). (SP standing for "surfactant protein".)
SP-A and SP-D confer innate immunity as they have carbohydrate recognition domains that allow them to coat bacteria and viruses promoting phagocytosis by macrophages. SP-A is also thought to be involved in a negative feedback mechanism to control the production of surfactant.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
SP-B and SP-C are hydrophobic membrane proteins that increase the rate that surfactant spreads over the surface. SP-B and SP-C are required for proper biophysical function of the lung. Humans and animals born with a congenital absence of SP-B suffer from intractable respiratory failure whereas those born lacking SP-C tend to develop progressive interstitial pneumonitis.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Numerous agents such as Beta adrenergic agonists, activators of protein Kinase C, leukotrienes and purinergic agonists stimulate secretion of surfactant.
Respiratory Distress of the Newborn is due to lack of surfactant particularly the PG.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Gross Anatomy of the Lungs Lungs occupy all of the thoracic cavity except the
mediastinum Root – site of vascular and bronchial attachments Costal surface – anterior, lateral, and posterior
surfaces in contact with the ribs Apex – narrow superior tip Base – inferior surface that rests on the diaphragm Hilus – indentation that contains pulmonary and
systemic blood vessels

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Organs in the Thoracic Cavity
Figure 22.10a

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Transverse Thoracic Section
Figure 22.10c

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Lungs Cardiac notch (impression) – cavity that
accommodates the heart Left lung – separated into upper and lower lobes
by the oblique fissure Right lung – separated into three lobes by the
oblique and horizontal fissures There are 10 bronchopulmonary segments in each
lung

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Serous Membranes (Peritoneum, Pericardium, Pleura) a serous membrane (or serosa) is a smooth membrane consisting of
a thin layer of cells which secrete serous fluid – lining several body cavities, known as serous cavities, where they secrete a lubricating fluid which reduces friction.
Each serous membrane is composed of a secretory epithelial layer and a connective tissue layer underneath.
The epithelial layer, known as mesothelium, consists of a single layer of avascular flat nucleated cells (simple squamous) which produce the lubricating serous fluid. This fluid has a consistency similar to watery mucus. These cells are bound tightly to the underlying connective tissue.
The connective tissue layer provides the blood vessels and nerves for the overlying secretory cells, and also serves as the binding layer which allows the whole serous membrane to adhere to organs and other structures.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Pleurae Thin, double-layered serosa Parietal pleura
Covers the thoracic wall and superior face of the diaphragm
Continues around heart and between lungs

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Pleurae Visceral pleura covers the external lung surface and the parietal
pleura is stuck to the inside of the chest wall. The space between the two is the pleural space (cavity). It contains pleural fluid.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Blood Supply to Lungs Lungs are perfused by two circulations: pulmonary
and bronchial Pulmonary arteries – supply systemic venous
blood to be oxygenated Branch profusely, along with bronchi Ultimately feed into the pulmonary capillary
network surrounding the alveoli Pulmonary veins – carry oxygenated blood from
respiratory zones to the heart

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Main Pulmonary artery (trunk)
Pulmonary veins

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Blood Supply to Lungs Bronchial arteries – provide systemic blood to the
lung tissue itself (akin to the coronary circulation for the heart – which supplies blood to the heart itself
Arise from aorta and enter the lungs at the hilus Supply all lung tissue except the alveoli
Bronchial veins anastomose with pulmonary veins Pulmonary veins carry most venous blood back to
the heart

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Bronchial arteries come off theAorta
Bronchial veins dump into pulmonary veins

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Important Mathematical Concepts in Respiratory 1. Resistance R = 8ηL/πR4
2. Compliance C = ∆V/∆P 3. Flow Flow = ∆P/ R 4. Diffusion D = A x Dc /t (Co – Ci) 5. Surface Tension of Water ? 6. Ideal Gas Equation ? 7. Boyle’s Law ? 8. Charles Law ? 9. Dalton’s Law of Partial Pressures? 10 . Henry’s Law ?

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Water exerts a surface tension Surface tension is the expression of
intermolecular attraction at the surface of a liquid, in contact with air or another gas, a solid, or another immiscible liquid, tending to pull the liquid inward from its surface.
Water sticks to water and the top of its surface is very, very tight – all of this due to its trillions and trillions of hydrogen bonds – holding the water molecules tightly together.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
The surface tension of water will cause the alveolus to collapse when
the alveolus gets smaller duringexhalation – if it were not forsurfactant (discussed later).

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Ps = 2T/rT = Ps x r/2
Ps – pressure in a sphereT – Tensionr - radius
As radius gets smaller pressureincreases.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Ideal Gas Equation & Boyle’s LawPV = nRT
P – pressure V- Volume n- number of moles R- gas rate constant (8.314472 J·K−1) T – Temperature
in Kelvin Boyles Law: There is an inverse relationship between
Pressure and Volume. Volume is how much space a set amount (number of
atoms or molecules) of gas or liquid occupies. If the volume (space occupied) got larger– but the amount (number of atoms/molecules) stayed the same – the pressure exerted by the gas or liquid would go down.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Charles Law and Dalton’s Law Charles Law: There is a direct relationship
between Volume and Temperature. When a gas is heated it will expand PV = nRT
Dalton’s Law of Partial Pressures: Each type gas in a mixture of gases will exert a pressure independent of the other types of gases in the mixture. The amount of the pressure exerted by each type of gas is in accordance with its percent present in the mixture times the total pressure exerted by all of the gases.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Dalton’s Law Atmospheric Pressure at Sea Level –
760 mmHg/square inch (14.7 lbs./square inch)
Composition of Atmosphere N2 – 78.0826% O2 – 29.94% CO2 - .034%

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Dalton’s Law of Partial Pressures 760 mm Hg x .21 = O2 = 159 mm Hg
760 mm Hg x .0004 = CO2 = .30 mm Hg
760 mm Hg x .79 = N2 = 600.4 mm Hg Percent of other gases = ________________ Total 760 mm Hg

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Henry’s Law The amount of gas that will dissolve in a liquid
depends on the partial pressure of the gas above the liquid (push down force) and the solubility coefficient of the gas for the liquid (pull down force).
Solubility Coefficients of Gases in H2O
(Determination of how much a certain gas likes a certain liquid)
Oxygen --- 0.024 Carbon Dioxide - 0.57 (likes to dissolve in water the best)
Nitrogen – 0.012 Carbon Monoxide – 0.018

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Henry’s Law
Push down force – pressure above the liquid
How much does that particular liquid want to pull into itself that Particular gas. (Determined by Solubility Coefficient)

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Breathing (Inhalation and Exhalation) This process depends on Boyle’s Law – the inverse
relationship between Pressure and Volume A mechanical process that depends on volume
changes in the thoracic cavity Volume changes lead to pressure changes, which lead
to the flow of gases to equalize pressure Breathing, or pulmonary ventilation, consists of two
phases Inspiration (Inhalation) – air flows into the lungs Expiration – (Exhalation )gases exit the lungs

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Factors involved in inhalation and exhalation 1. Terms 2. Muscles involved 3. Volumes of air inhaled and exhaled 4. Compliance

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Terms Normal breath rate is 12 – 20 breaths per minute Fast breath rate – Tachypnea Slow breath rate – Bradypnea Cessation of Breathing - Apnea Average volume during restful inhalation and
exhalation – 500cc (ml.) Deep Breathing – Hyperpnea Shallow Breathing – Hypopnea Quiet Breathing – Eupnea Stressful Breathing - Dyspnea

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Muscles for Breathing It is unusual in the body that although breathing is
an involuntary action – it operates using skeletal muscles – thus using the somatic nervous system rather than the autonomic nervous system
Main muscle for breathing is the Diaphragm Muscles for inhalation – external intercostals,
scalenes, pectoralis minor, sternocleidomastoid, trapezius
Muscles of exhalation – internal intercostals, internal and external obliques, rectus abdominus, transversalis

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Diaphragm
Each hemi-diaphragm is controlled by the Phrenic nerve on itsRespective side. Originates from spinal nerves C3, C4 and C5

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
An average of 10 cm at the top of the dome
When the diaphragm contracts it lowers – thus increasing chest size for inhalation – when it relaxes it domes again – thus decreasing chest sizein exhalation
Hiccups- singultus

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Muscle origin is back of upper rib – insertionfront of rib below – pulls chest outward for inhalation
Origin front of upper rib – insertion is back of rib below – pulls chest Inward for exhalation

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Scalenes raise ribs 1 and 2

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Inhalation musclesPectoralis minor raises ribs 3, 4 and 5

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Trapezius – keeps upper back straight

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Muscles of Exhalation

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Lung Volumes

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Respiratory Volumes Tidal volume (TV) – air that moves into and out of
the lungs with each breath (approximately 500 ml) Inspiratory reserve volume (IRV) – air that can be
inspired forcibly beyond the tidal volume (2100–3200 ml)
Expiratory reserve volume (ERV) – air that can be evacuated from the lungs after a tidal expiration (1000–1200 ml)
Residual volume (RV) – air left in the lungs after strenuous expiration (1200 ml)

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Respiratory Capacities Inspiratory capacity (IC) – total amount of air that
can be inspired after a tidal expiration (IRV + TV) Functional residual capacity (FRC) – amount of air
remaining in the lungs after a tidal expiration (RV + ERV)
Vital capacity (VC) – the total amount of exchangeable air (TV + IRV + ERV)
Total lung capacity (TLC) – sum of all lung volumes (approximately 6000 ml in males)

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Dead Space Anatomical dead space – volume of the conducting
respiratory passages (150 ml) Alveolar dead space – alveoli that cease to act in
gas exchange due to collapse or obstruction Total dead space – sum of alveolar and anatomical
dead spaces

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Respiratory Compliance C = ∆V/∆P There are two compliances involved in breathing.
One is chest wall compliance and other is lung compliance.
Chest wall compliance is due to the ease of movement of the rib cage and the tension of the various skeletal muscles associated with the rib cage. When the lungs are removed from the chest the chest cage springs outward.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Lung Compliance C = ∆V/∆P The ease with which lungs can be expanded Specifically, the measure of the change in lung
volume that occurs with a given change in transpulmonary pressure
Determined by two main factors Distensibility of the lung tissue and surrounding
thoracic cage Surface tension of the alveoli

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Lung Compliance Two forces act to pull the lungs inward - away from the
thoracic wall, promoting lung collapse. These are also the two forces that determine lung compliance
Elasticity (due to elastic fibers) of lungs causes them to assume the smallest possible size
Surface tension of alveolar fluid draws alveoli to their smallest possible size. This is the main force under normal conditions determining lung compliance.
Opposing force – elasticity of the chest wall pulls the thorax outward to enlarge the lungs

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Lung Compliance Curves (Hysteresis) The compliance of the lungis different depending on ifan individual is breathing in (inspiration) versus breathing out -expiration.
When breathing in - it ismore difficult to expand thelungs due mainly to needing to break the surface tension of water.
When breathing out – the surface tension of water helpspull the lungs inward.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Pressure Relationships in the Thoracic Cavity Respiratory pressure is always described relative to
atmospheric pressure Atmospheric pressure (Patm)
Pressure exerted by the air surrounding the body Negative respiratory pressure is less than Patm
Positive respiratory pressure is greater than Patm

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Pressure Relationships in the Thoracic Cavity Intrapulmonary pressure (Ppul) – pressure within
tubes (bronchi, bronchioles and the alveoli Intrapleural pressure (Pip) – pressure within the
pleural cavity

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Pressure Relationships Intrapulmonary pressure and intrapleural pressure
fluctuate with the phases of breathing Intrapulmonary pressure always eventually
equalizes itself with atmospheric pressure Intrapleural pressure is always less than
intrapulmonary pressure and atmospheric pressure

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Pressure Relationships
Figure 22.12

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Lung Collapse (Atelectasis) Caused by equalization of the intrapleural pressure
with the intrapulmonary pressure Transpulmonary pressure keeps the airways open
Transpulmonary pressure – difference between the intrapulmonary and intrapleural pressures (Ppul – Pip)

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Inspiration The diaphragm and external intercostal muscles
(inspiratory muscles) contract and the rib cage rises The lungs are stretched and intrapulmonary
volume increases Intrapulmonary pressure drops below atmospheric
pressure (1 mm Hg) Air flows into the lungs, down its pressure
gradient, until intrapleural pressure = atmospheric pressure

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Inspiration
Figure 22.13.1

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Expiration Inspiratory muscles relax and the rib cage descends
due to gravity Thoracic cavity volume decreases Elastic lungs recoil passively and intrapulmonary
volume decreases Intrapulmonary pressure rises above atmospheric
pressure (+1 mm Hg) Gases flow out of the lungs down the pressure
gradient until intrapulmonary pressure is 0

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Expiration
Figure 22.13.2

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Pulmonary Pressures
Figure 22.14
15 breaths per minute with4 seconds per breath

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
I to E ratio If a person has a breath rate of 12 breaths per
minute – then each breath (both inspiration and expiration) is 5 seconds. If the breath rate is faster the time of each breath is less.
The I (Inspiration) time is generally 2 seconds and the E (Expiration) time is generally 3 seconds – thus and I/E ratio of 2:3 (1:1.5 – 1:2)
The expiration time in actuality is generally no longer than the inspiration time – but it includes the brief moment in time a person is not breathing in or out

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Nonrespiratory Air Movements Most result from reflex action Examples include: coughing, sneezing, crying,
laughing, hiccupping, and yawning

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Alveolar Ventilation
Alveolar ventilation rate (AVR) which is really exchange zone ventilation rate. This measures the flow of fresh gases into and out of the exchange regions of the lungs. The exchange zones include the respiratory bronchiole, alveolar duct, alveolar sac and alveolus
Slow, deep breathing increases AVR and rapid, shallow breathing decreases AVR
AVR = frequency X (TV – dead space)
(ml/min) (breaths/min) (ml/breath)

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Ventilation-Perfusion Coupling Ventilation – the amount of gas reaching the
alveoli Perfusion – the blood flow reaching the alveoli Ventilation and perfusion must be tightly regulated
for efficient gas exchange

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Ventilation-Perfusion Coupling Changes in PCO2 in the alveoli cause changes in the
diameters of the bronchioles Passageways servicing areas where alveolar carbon
dioxide is high dilate Those serving areas where alveolar carbon dioxide
is low constrict

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
V/Q ratio and Dead Space Total ventilation (Vt)is the amount of air coming
into the lungs in a minute (ml./min.) on average 500 cc x 12 breaths per minute = 6 Liters
Exchange zone ventilation (VE) is how much air is going into the exchange zone in a minute. This is the amount of air entering the lungs during inspiration – minus the dead space.
Q is perfusion – thus Q is the blood perfusion rate to the lungs in a minute – which is really the cardiac output - approximately 5 Liters per minute

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Surface Area and Thickness of the Respiratory Membrane (Exchange areas) Respiratory membranes (all membranes where
exchange takes place): only 0.5 to 1 m Alveolus is the thinnest allowing for efficient gas
exchange Have a total surface area (in males) of about 60 m2
(40 times that of one’s skin) Thicken if lungs become waterlogged and
edematous, whereby gas exchange is inadequate and oxygen deprivation results
Decrease in surface area with emphysema, when walls of adjacent alveoli break through

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Respiratory Dead Space The airways in which there is ventilation (air coming in and out) but
the air pipe wall is too thick (all airways prior to the respiratory bronchioles) to allow diffusion of gases (O2, CO2) into and out of the bloodstream. There are two dead spaces – the anatomic and the alveolar - both added together equal the physiologic dead space.
Anatomic Dead Space - the airway pipes prior to the respiratory bronchioles have walls that are too thick to perform exchange of gases between them and the blood. Thus these pipes are conduits (like the arteries and veins in the circulatory system) transferring to the exchange regions (respiratory bronchioles, alveolar ducts, alveolar sacs and alveolus). This is similar to the capillaries which are the exchange vessels in the blood circulation. These airways are termed the anatomic (natural) dead space – in the physiologic demo human – an average of 150 cc.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Physiologic Dead Space = Anatomic Dead Space + Alveolar Dead Space (Alveolar Dead Space is bad airways that should have allowed diffusion into and out of the bloodstream – but for some reason cannot. If an individual has none of these bad airways – the physiologic dead space will equal to the anatomic dead space.
Ideally the exchange zone ventilation rate (air entering) should equal the perfusion rate (blood flow rate) in order to get the best oxygenation of the blood.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Q is perfusion – thus Q is the blood perfusion rate to the lungs in a minute – which is really the cardiac output - approximately 5 Liters per minute
Though the blood supply to lungs as a whole is equal to the cardiac output. Different regions (zones) of the lung get varying blood supplies. Most consider there to be 3 zones. The upper zone which is above the heart gets the least blood – but the best ventilation (high V/Q). The middle zone which is at the level of the heart gets an equal V/Q ratio. The lower zone below the heart gets excellent perfusion but less ventilation – low V/Q.
If the blood can get to an area of the diffusable portion (exchange region) but the ventilation cannot get there – it is termed a shunt.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Ventilation-Perfusion Coupling
Figure 22.19
Reduced alveolar ventilation;excessive perfusion
Reduced alveolar ventilation;reduced perfusion
Pulmonary arteriolesserving these alveoliconstrict
Enhanced alveolar ventilation;inadequate perfusion
Enhanced alveolar ventilation;enhanced perfusion
Pulmonary arteriolesserving these alveolidilate
PO2
PCO2
in alveoli
PO2
PCO2
in alveoli

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Friction is the major nonelastic source of resistance to airflow
The relationship between flow (F), pressure (P), and resistance (R) is:
Physical Factors Influencing Ventilation: Airway Resistance
PRF =
R = 8ηL/πR4

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Resistance to airflow in the respiratory system is composed of three individual resistances; airway resistance, pulmonary (lung) resistance, and chest wall resistance.
Airway resistance is the resistance of the entire airway system from the tip of the nose (for nasal breathing) or mouth (for mouth breathing) to the alveoli.
Pulmonary resistance (lung resistance) is the resistance of the lungs and airways combined.
Chest wall resistance is the resistance of the chest wall and abdominal structures.
Airway resistance is subsumed into upper airway resistance ( nose to glottis) and lower airway resistance (glottis to alveoli)

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
25% - 40% of the total resistance to airflow is located in the upper airways, namely the nose, nasal turbinates, oropharynx, nasopharynx and larynx
Airflow resistance of the lower airways can be divided between the large airways (> 2mm in diameter) – first 8 generations of branchings, the medium sized airways (segmental bronchi, ≥ 2 mm) and the small airways (bronchioles < 2 mm)
It would be thought that the greatest resistance in the airways should be in the smaller airways since their diameters are small. However the smallest airways contribute very little to overall resistance even their individual resistances are high. The greatest resistance is in the medium sized airways.
The reason for this is (1) the cross sectional area of the smaller airways is large – thus the velocity of flow is low and (2) the smaller airways are in parallel arrangement – thus their total resistances is low.

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Resistance in Repiratory Passageways
Figure 22.15
Greatest resistancein the medium sized airways

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Respiratory Zone
Figure 22.8a

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Formulas of Importance Resistance –a force of impedance (holding back) R =
8ηL/πR4 , η is viscosity of the gas or liquid, L is the length of the vessel, and R is the resistance raised to the 4th power
Summation (∑) of Resistances – adding up the resistors in flow arrangement a series arrange
Resistors in series – one resistor in front of another ∑ = R1 + R2 + R3 + ……
Resistors in parallel – a pipe leads into a branching set of pipes ∑ = 1/R1 + 1/R2 + 1/R3 +..
Note: resistors in parallel give less total resistance than those in series (think of the capillary arrangement)

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Formulas of importance Flow = ∆P/ R, ∆P is the change in pressure from one area to
another (P1 – P2) – in the direction of flow, R is the resistance (Note: pressure drops off as a fluid or gas passes further down the pipe – thus the pressure in proximal area 1 (P1) is higher than the pressure is distal area 2. The more pressure drop off the more the flow. Also, the less the resistance the better the flow.
Rate of Flow = amount of gas or liquid/time (example ml/min) Velocity of flow = amount of gas or liquid/time/cross sectional area
(another way of looking at it is Vf = rate of flow/cross sectional area)
example of velocity of flow ml. /min per cm2
Note: Area of a circle (like the inside of a vessel ) = equals pi (π) times the radius squared (π⋅r2), example ml. /min per cm2
Flow formula derived Ohm’s Law

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Resistance in Repiratory Passageways
Figure 22.15
Greatest resistancein the medium sized airways

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Airway Resistance As airway resistance rises, breathing movements
become more strenuous Severely constricted or obstructed bronchioles:
Can prevent life-sustaining ventilation Can occur during acute asthma attacks which stops
ventilation Epinephrine release via the sympathetic nervous
system dilates bronchioles and reduces air resistance

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Alveolar Surface Tension Surface tension – the attraction of liquid molecules
to one another at a liquid-gas interface The liquid coating the alveolar surface is always
acting to reduce the alveoli to the smallest possible size
Surfactant, a detergent-like complex, reduces surface tension and helps keep the alveoli from collapsing

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Lung Compliance The ease with which lungs can be expanded Specifically, the measure of the change in lung
volume that occurs with a given change in transpulmonary pressure
Determined by two main factors Distensibility of the lung tissue and surrounding
thoracic cage Surface tension of the alveoli

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Factors That Diminish Lung Compliance Scar tissue or fibrosis that reduces the natural
resilience of the lungs Blockage of the smaller respiratory passages with
mucus or fluid Reduced production of surfactant Decreased flexibility of the thoracic cage or its
decreased ability to expand

Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings
Factors That Diminish Lung Compliance Examples include:
Deformities of thorax Ossification of the costal cartilage Paralysis of intercostal muscles