Embed Size (px)
DESCRIPTION
Americans need to know the facts of what's to come under Obamacare. Most have no idea of the real facts they only know the candy coated version.
Citation preview

The New World ofOBAMACARE
These copyrighted articles originally appeared in the May 10 and August 30, 2010 issues of THE NEW AMERICAN. Call 1-800-727-TRUE to subscribe today!
!"!"Special Reprint !"!
THAT FREEDOM SHALL NOT PERISHwww.TheNewAmerican.com

by Michael Tennant
By now most Americans are fa-miliar with the broad outline of ObamaCare: Everyone is required
by law to purchase health insurance, with a tax penalty assessed upon those who fail to comply. Insurers may not refuse to cover those with pre-existing conditions nor charge them higher rates. The federal
government is expanding its role in pro-viding health insurance. And did I mention that all of this is supposedly going to re-duce both healthcare costs and the federal deficit?
Of course, with a law that is over 900 pages long and contains hundreds of man-dates, it may be months or even years be-fore all the ramifications of the law are understood. Some of the mandates are al-
ready widely known, such as the require-ment that chain restaurants post nutrition information about their menu items or the 10-percent tax on tanning salon ser-vices. However, it may very well be that the less widely known portions of the law are also the most dangerous, which may
Most Americans know the broad strokes of the new healthcare legislation dubbed ObamaCare, but scratching the surface of the law reveals large-scale unstated changes.
Michael Tennant is a software developer and free-lance writer in Pittsburgh, Pennsylvania.
The New World ofOBAMACARE
2 THE NEW AMERICAN
HEALTHCARE

explain why they were kept out of public view in contravention of candidate Barack Obama’s repeated assurances that the en-tire healthcare debate would be conducted in public and broadcast on C-Span.
Among the obscure but dangerous provisions in the Patient Protection and Affordable Care Act (the official — and disingenuous — name for ObamaCare) are numerous provisions that, said Art Thompson, CEO of The John Birch So-ciety, “will intrude on every aspect of life in America, from cradle to grave.” They include everything from a national healthcare strategy to home visitations by government agents, possibly including forced immunizations, to “Community Transformation Grants” — all designed to alter Americans’ lifestyles to conform to the whims of bureaucrats in Washington.
The law itself is (probably intentional-ly) vague about how all these mandates are to be carried out; the details are left mostly to federal agencies that are much less ac-countable to the voters than Congress. Therefore, many of the suggestions in the following paragraphs as to how these mandates will play out are based not on explicit language in the legislation itself, or (obviously) the yet-to-be-issued regu-lations, but on an informed understanding of how governments can turn seemingly beneficent laws into tools of oppression. If anything, much of what is suggested in this article is actually less radical than what President Obama and fellow Demo-crats have said they wish to accomplish, namely a single-payer* health insurance scheme at the federal level.
Obama himself, in a 2003 speech, said that he’d “like to see” the United States adopt a “single-payer health care plan, a universal health care plan.”
His Secretary of State, Hillary Clinton, of course, attempted to foist a single-payer government healthcare system on Americans back in 1993 and ’94. Many
other Clinton administration figures are prominent members of the Obama administration.
Revolutionary AppointeeObama’s recently appointed head of the Centers for Medicare and Medicaid Ser-vices, Donald Berwick, has openly praised the British National Health Service for not leaving healthcare to “play out in the dark-ness of private enterprise.” Berwick added that “any healthcare that is just, equitable, civilized, and humane must, must redis-tribute wealth from the richer among us to the poorer and the less fortunate. Ex-cellent healthcare is by definition redistri-butional.” Berwick is also a proponent of government rationing† of healthcare, say-ing, “The decision is not whether or not we will ration care. The decision is whether we will ration with our eyes open.” Tellingly, Obama took the occasion of a Senate re-cess to appoint Berwick, by-passing Senate confirmation hearings that would surely have publicized Berwick’s socialized-medicine bona fides and possibly have sunk his nomination.
Thus, it is almost impos-sible to be too alarmist about the intentions of Obama Care
and its proponents. When government controls the healthcare system from top to bottom, it is naturally going to attempt to manipulate every aspect of people’s lives in order to keep costs down; and for those who become ill despite the state’s best efforts to force them to be healthy, care can — and will — be denied. This is already happening in Berwick’s beloved
The “primary function” of existing school-based health centers “is to circumvent parental involvement in the important area of directing a child’s healthcare,” Gregory Hession, a Massachusetts attorney specializing in family and juvenile law, said in an e-mail.
* “Single payer” is the innocuous code for govern-ment-run, bureaucrat-controlled, nationalized, so-cialized medicine.
† Although “rationing” may have a more negative connotation than “single payer,” it is nonetheless euphemistic. What it means in healthcare is that treatment will be determined not by the physician according to the needs of the patient, but according to formulas and edicts issued by the government and carried out by administrators and bureaucrats.
Poking, prodding, and bypassing parents: Section 4101 of ObamaCare provides grants for school-based health centers that offer comprehensive physical and mental care. Though school officials are usually required by law to report worrisome family behavior to authorities, they actually withhold information from parents about high-risk student behaviors and their drugs and medical procedures.
AP Images
www.TheNewAmerican.com 3

British healthcare system, where, for example, life-saving drugs are withheld from patients because the government deems them too costly — and then threatens pa-tients who try to purchase the drugs out of their own pockets with the loss of all their healthcare benefits (see “Paying Patients Test British Health Care System,” the New York Times, Feb. 21, 2008).
Massive New BureaucracyPerhaps the most ominous of the ob-scure-but-dangerous provisions in Obama-Care is found in Sections 3011 through 3015. This portion of the law instructs the Secretary of Health and Human Services to “establish a national strategy to improve the delivery of health care services, patient health outcomes, and population health.” Along with the strategy, the law requires “a comprehensive strategic plan to achieve the priorities” established by Congress. The strategic plan includes “agency-spe-cific strategic plans to achieve national priorities,” “annual benchmarks for each relevant agency,” and “strategies to align public and private payers with regard to quality and patient safety efforts.” In short, the federal government is going to micro-manage the healthcare sector in an effort to achieve its desired outcomes, and it is going to force private insurers to partici-pate in this micromanagement — part of
the price they will pay for having Uncle Sam hand them a captive market.
In order to implement the national strategy, the law instructs the President to “convene a working group to be known as the Interagency Working Group on Health Care Quality.” This new bureaucracy in-cludes senior-level representatives from 23 named federal agencies “and any other Federal agencies and departments … as determined by the President.” Among the agencies included in the working group are the Department of Commerce, the Coast Guard, the Federal Bureau of Prisons, the National Highway Traffic Safety Admin-istration, the Federal Trade Commission, the Department of Labor, the Department of Defense, and the Department of Educa-tion — a strong indication that this is con-cerned with far more than simply ensuring that patients are treated well.
Likewise, Section 4001 of the act in-structs the President to “es-tablish, within the Depart-ment of Health and Human Services, a council to be known as the ‘National Pre-vention, Health Promotion and Public Health Council.’” President Obama issued an executive order to carry out this provision on June 10.
The council is chaired by the Surgeon General and consists of senior-level rep-
resentatives from 12 named federal agencies and “the head of any other Federal agency that the chairperson determines is appropriate.”
The purposes of the council in-clude: (1) to coordinate “preven-tion, wellness and health promotion practices”; (2) to “develop a national prevention, health promotion, public health, and integrative health care strategy”; (3) to “provide recommen-dations to the President and Congress concerning … changes in Federal policy to achieve national wellness, health promotion, and public health goals, including the reduction of to-bacco use, sedentary behavior, and poor nutrition”; and (4) to propose policies “for the promotion of trans-formative models of prevention, in-tegrative health, and public health on individual and community levels across the United States.” There will
be “a list of national priorities” and “spe-cific science-based initiatives” to “address lifestyle behavior modification” with re-gard to “smoking cessation, proper nutri-tion, appropriate exercise, mental health, behavioral health, substance use disorder, and domestic violence screenings.”
“It’s a horror even to think that they would put that in there, that they are going to start regulating personal behavior,” Rep. Ron Paul (R-Texas), himself a physician, told THE NEW AMERICAN. “But these people believe in it, and this is why it’s so bad to allow government to get inside the door.... They get their foot in the door, and then they say, ‘Oh, we’re paying for it, so we’re going to tell you how to live.’”
In other words, ObamaCare has just turned the United States into one giant psy-chiatric laboratory, and Americans are the rats stuck inside and subjected to “behavior modification” until we stop smoking (won-der if this applies to the President, who still hasn’t kicked the habit), take our vaccines and stop eating Twinkies, take up jogging, quit ingesting substances that the big phar-maceutical companies can’t patent, and tell Uncle Sam when we stopped beating our wives. Is this really what all those folks clamoring for healthcare reform wanted? If so, it serves as further proof of H.L. Menck-en’s maxim that “democracy is the theory that the common people know what they want, and deserve to get it good and hard.”
Just what is “emotional wellness,” and how is the government going to see to it that people attain it? Surely it isn’t by cutting bureaucracy and spending, bringing the troops home, and reducing taxes, though those are the surest ways to make (almost) everyone happier.
THE NEW AMERICAN4
HEALTHCARE
Limits to care: Dr. Donald Berwick, who was appointed by President Obama to head the Centers for Medicare and Medicaid Services, has said he will limit medical treatments: “The decision is not whether or not we will ration care — the decision is whether we will ration with our eyes open.”

Section 4101 provides for grants for school-based health centers, which will offer “comprehensive health assessments, diagnosis, and treatment of minor, acute, and chronic medical conditions” and “mental health and substance use disorder assessments, crisis intervention, counsel-ing, treatment, and referral to a continuum of services including emergency psychi-atric care, community support programs, inpatient care, and outpatient programs.”
Will parents’ rights be respected in all this? Will their children be treated without their knowledge?
The “primary function” of existing school-based health centers “is to circum-vent parental involvement in the impor-tant area of directing a child’s healthcare,” Gregory Hession, a Massachusetts attor-ney specializing in family and juvenile law, said in an e-mail. The programs “sex-ualize children with condom giveaways, homosexual advocacy programs, and age-inappropriate instruction to children, even very young ones, about sexual ac-tivity,” said Hession. “These clinics even allow and promote statutory rape” and refer students to abortion clinics and pro-vide transportation to the clinics, Hession added, pointing out that all of this is done “in complete secrecy.”
And what of mental health assessments? Hession stated that much of the mental health screening that already takes place in schools appears to be “fostered by psy-chiatrists with financial ties to large drug companies that offer psychotropic drugs which are almost invariably prescribed for any small perceived personality problem,” the result being “that many children are now required, as a contingency for attend-ing school, to take powerful psychotropic drugs for such invented maladies as atten-tion deficit disorder.”
With school-based health clinics already engaged in such unsavory practices, federal funding and mandates can only lead to even worse, and more widespread, abuses.
Government Into Almost EverythingNothing less than the “transformation” of communities is the modest goal of Section 4201, which creates a grant program for state and local governments and nonprofit organizations “to reduce chronic disease rates, prevent the development of second-ary conditions, address health disparities, and develop a stronger evidence-base of effective prevention programming.” Each grantee must develop a “community trans-formation plan” which may include such things as:
1. creating healthier school environ-ments, including increasing healthy food options, physical activity op-portunities, promotion of healthy lifestyle, emotional wellness, and prevention curricula, and activities to prevent chronic diseases;
2. creating the infrastructure to sup-port active living and access to nu-tritious foods in a safe environment;
3. developing and promoting pro-grams targeting a variety of age levels to increase access to nutri-tion, physical activity and smoking
cessation, improve social and emo-tional wellness, enhance safety in a community, or address any other chronic disease priority area iden-tified by the grantee;
4. assessing and implementing worksite wellness programming and incentives;
5. working to highlight healthy op-tions at restaurants and other food venues;
6. prioritizing strategies to reduce ra-cial and ethnic disparities, including social, economic, and geographic determinants of health; and
7. addressing special populations needs, including all age groups and individuals with disabilities, and individuals in both urban and rural areas.
Imagine telling the Founding Fathers that the federal government would someday be concerning itself with restaurant menus and workplace stress! They would have laughed you right out of Philadelphia. Yet here we are, with the feds doing just that and much, much more.
Long arm of the law: The new healthcare law directs health officials to search out high-risk populations and provide “improvements in parenting skills,” without specifying what is deemed poor parenting. Since religious morals are already targeted by schools as being improper, how will this play out under the new law? AP Images
5Call 1-800-727-TRUE to subscribe today!

Just what is “emotional wellness,” and how is the government going to see to it that people attain it? Surely it isn’t by cutting bureaucracy and spending, bring-ing the troops home, and reducing taxes, though those are the surest ways to make (almost) everyone happier.
President Obama, in a 2007 Democrat-ic primary debate at Dartmouth College, stated his support for a national smok-ing ban if local bans fail to snuff out the habit. It makes sense, then, that his signa-ture achievement would include language plainly calling for “smoking cessation.” When Uncle Sam is footing the bill for Americans’ healthcare, they’d better do as he says or else. Indeed, the British Health Secretary, in charge of that single-payer
system that Berwick so adores, ruled in 2007 that smokers would henceforth “be denied operations unless they give up cigarettes for at least four weeks before-hand,” according to the Daily Mail; their doctors would be in charge of enforcing the rule by making them take blood tests to prove they’ve not lit up for the last month. Surely the ObamaCare adminis-trators can come up with some similarly clever ways of coercing Americans to can their Camels.
Then there’s that business about “reduc-ing disparities.” The intention, undoubt-edly, is to see to it that those who do not have health insurance receive it — and that those who have too much of it, as Wash-ington sees it, are forced to make do with
less; hence the tax penalties applied to so-called Cadillac plans. Subsidizing insurance for some will only encourage them to make more use of the healthcare system, putting upward pressure on prices and hastening the day that Berwick and others of his ilk begin rationing care for them. Punishing those with the best insurance plans will ensure that some of those individu-
als are unable to afford the care they need, which is just rationing by other means. The result: We all end up in the mushy middle, with just as much care as the government deems necessary to keep us from being too much of a strain on the system. For those who do become too ill and therefore too expensive for the government to keep, de-nial of treatment is an easy fix.
Individuals who use community health centers funded by the government may also be given a government-sanctioned “individualized wellness plan” under Sec-tion 4206, which establishes a demonstra-tion project for this purpose. Undoubtedly this will be declared a success, and soon all Americans can expect a Washington-mandated plan for their lives, to control such things as alcohol and tobacco use, weight, blood pressure, nutritional supple-ment usage (but only those supplements “that have health claims approved by the Secretary”), stress, and exercise.
Invading Homes and SchoolsOne need not go to a health clinic to be subjected to federal healthcare intrusions, either. At least two portions of the act actu-ally provide for government agents to come into individuals’ homes to see to it that they are obeying Washington’s directives.
The first of these is Section 2951, en-titled “Maternal, Infant, and Early Child-hood Home Visiting Programs.” This sec-tion requires all states to perform a needs assessment that identifies at-risk com-munities and “the quality and capacity of existing programs or initiatives for early childhood home visitation.” States can then apply for grants to establish early childhood home visitation programs.
The programs will target high-risk com-munities first, with “high-risk” defined as “eligible families who reside in commu-nities in need of such services,” followed by eligible families with low incomes, pregnant women under 21 years old, “a history of child abuse or neglect … or interactions with child welfare services” (not evidence of actual abuse, mind you; just a visit from government agents on an anonymous tip will suffice), “a history of substance abuse,” “users of tobacco prod-ucts” (light up and expect a visit from your friendly neighborhood G-man), “children with low student achievement,” “children with developmental delays or disabilities,”
Gains made in Head Start, the most famous of these government programs, do not last much beyond first grade. Why, then, would anyone expect the government to be able to offer parents expert advice on how to prepare their children for school?
Empathy? President Obama often sold his healthcare prescription to audiences by telling the personal stories of those who are ill, exhibiting a sense of empathy. But as even greater doctor shortages and decreased care are the expected outcome of his law, where is the concern?
AP Images
6 THE NEW AMERICAN
HEALTHCARE

or “individuals who are serving or former-ly served in the Armed Forces.” That just about covers everyone.
“This section of the law is designed to circumvent the Fourth Amendment to the U.S. Constitution, and give government agents a plausible excuse to enter homes without a warrant, with the ultimate goal of reporting the family to child protec-tive services,” said Hession. The child-protection agents then have every incen-tive to take children from their families, as evidenced by the fact that over half a million children are now in child protec-tion agency custody in the United States.
The law lays out specific desired out-comes for individual families, many of which sound good. Who could oppose improvements in mothers’ and babies’ health, children’s development, parent-ing skills, school readiness and academic achievement, crime and domestic vio-lence rates, and family economic self-sufficiency? The detailed regulations es-tablished by federal and state bureaucrats to accomplish these general outcomes, however, may not be so benign.
For example, what specific “improve-ments in parenting skills” might govern-ment agents wish to impose on those they visit? Will spanking children or even speaking sharply to them be permitted? What if parents try to inculcate specific moral or religious precepts in their chil-dren? Hession noted that homeschoolers and parents who believe in corporal pun-ishment are already among the most tar-geted by state child protection agencies.
It is already known that government programs to improve school readiness are of little benefit. Gains made in Head Start, the most famous of these programs, do not last much beyond first grade. Why, then, would anyone expect the government to be able to offer parents expert advice on how to prepare their children for school?
Worse yet, how will “school readiness” and “child academic achievement” be mea-sured? What will happen to families whose children fail to meet the government’s arbi-trary standards? As the Birch Society’s Art Thompson perceptively pointed out,
The idea of school readiness and aca-demic achievement provides the ex-cuse for government agents to nullify parental prerogatives for private and
home schooling. Since they can test the preschool children, mold the tests of how and what the children should be taught, they can use this informa-tion to try and force you to send your children to government institutions.
In fact, school readiness is one of the key reasons boosters of universal pre-kinder-garten cite for their support of extending government schooling to an earlier age. Among those who favor universal pre-kindergarten are Hillary Clinton — she of “It Takes a Village to Raise a Child” and the anti-parental-rights Children’s Defense Fund — and President Obama. Prima facie evidence that it’s a bad idea.
Government has been the greatest enemy of “family economic self-sufficien-cy,” having replaced fathers with welfare checks and having taxed Americans to the
point that both parents frequently must work outside the home just to make ends meet. Government benefits from families who are dependent on it because those same people will almost always vote for even bigger government, as inner-city vot-ing patterns demonstrate.
It is of little comfort that the law re-quires that states provide assurances that “the participation of each eligible family in the program is voluntary.” As Hession said, existing “family visitation programs are about as voluntary as the current IRS tax system, which continues to assert that it is based on voluntary compliance.”
Even if it were the case, at least for now, that families are not required to admit government agents into their homes under this program, given that the target families at the beginning (most likely single mothers, according to Hession)
Choking smokers: Under ObamaCare, the National Prevention, Health Promotion, and Public Health Council is charged with reducing smoking. The law also mandates that smokers go on a list of Americans to get home visitations from federal health officials.
AP
Imag
es
www.TheNewAmerican.com 7

are likely to have less education and fewer resources to fight back, how likely are they to resist a bureaucrat who offers them a check or other assistance just for answering a few questions? Once they are caught in the state’s web, how easily will they be able to extricate themselves? After all, one of the desired outcomes for individual families is that they be more easily referred to “other community re-sources and supports … consistent with State child welfare agency training.” Then how long will it be until the pro-gram is expanded to other families and made mandatory? The dangers here are immense.
As if that weren’t bad enough, Section 4204 actually provides for home visits from government functionaries for the purpose of providing immunizations (a demonstration program for the time being but with the intent “to continue and ex-pand such program”).
The recent H1N1 hoopla demonstrates how the government, with the enthusias-tic backing of vaccine manufacturers, can manufacture a health crisis and then use it to encourage or even force people to be vaccinated. The Washington Post re-
ported on June 4 that two separate reports from Europe “accused the [World Health Organization] of exaggerating the threat posed by the virus and failing to disclose possible influence by the pharmaceutical industry on its recommendations for how countries should respond.” That exag-geration of the so-called pandemic and the WHO’s accompanying recommen-dations led many Americans to be vac-cinated needlessly, including some who were coerced by the government, such as healthcare workers in New York.
Now imagine that same scenario play-ing out under a program in which the fed-eral government gives grants to states to (1) provide “immunization reminders or recalls for target populations,” (2) educate “targeted populations and health care pro-viders concerning immunizations in com-bination with one or more other interven-tions,” (3) subsidize immunizations, (4) promote immunizations, (5) provide for “home visits” that may include “provi-sion of immunization,” and (6) create an electronic database for all states to access immunization records — all provisions of the Patient Protection and Affordable Health Care Act. How easy it would be
for governments to find out who hasn’t volunteered to be vaccinated and to show up at the recalcitrant citizens’ homes to give them their shots right then and there! How profitable it would be for vaccine manufacturers!
Indeed, Dr. Paul said that “one thing that we have found in the past is some of the strongest proponents of massive inoculations” have been funded by phar-maceutical companies. The decision to immunize or not to immunize, he said, “should be strictly a decision made by the doctor and the patient, and never by public health officials.”
Paul expressed particular concern that ObamaCare will come between doc-tors and patients. Decisions about treat-ment, he said, “will be made not by other M.D.’s, but they will be made by people who are pushing a pencil.... And there will be rationing of care … by those people in Washington, the bureaucrats who are looking at a bottom line and not under-standing the situation.”
People Control, Not HealthcareFrom page 1 to page 906, ObamaCare is chock full of expensive, intrusive, and downright scary programs such as these. The law gives the federal and state gov-ernments virtually unlimited power to interfere in Americans’ lives, even within the confines of our own homes. (Hession noted that the act “is marbled with re-quirements that can be accomplished only by entry into private family homes.”) It destroys individual self-reliance and, through a variety of provisions such as school-based health clinics and home visi-tation programs, the family unit. These are the foundations of the American Repub-lic; without them the United States will become a society of helpless, dependent sheep with neither the desire nor the will to resist the state’s relentless encroach-ments on our liberties.
These problems cannot be fixed merely by modifying a clause here and a proviso there. ObamaCare needs to be repealed in full before it can metastasize into a full-blown single-payer system. State-by-state nullification should also be undertaken. Then we can work on dismantling the rest of the federal healthcare behemoth. These are the only cures for what ails the Ameri-can healthcare system. #
Overdose: Health officials will now promote and provide immunizations even to the point of going door to door. With the FDA already being heavily co-opted by the pharmaceutical industry and European governments accusing the WHO of overstating the dangers of H1N1 at the behest of vaccine makers, is this a good idea?
AP Images
8 THE NEW AMERICAN
HEALTHCARE
THE NEW AMERICAN

!"#$%&'('$$)%*+
,-$.'$/0%*�#819*:-;:#/1<-/')6
9
Appleton, WI 54912-8040 • (920) 749-3780 •
“Less government, more responsibility, and — with God’s help — a better world.”

by Thomas R. Eddlem
Americans who want to know how ObamaCare, the recently passed healthcare reform package, will
impact the nation need only look toward Massachusetts. “The Massachusetts law was the model for national reform,” the Massachusetts state government says on
its website. The Bay State passed similar legislation in 2006, mandating all of the major provisions that are present in this year’s ObamaCare:
• Requiring individuals to purchase government-approved health insurance (and fining those who do not comply);
• Requiring employers to offer “afford-able” health insurance to their employees
(and fining employers who do not comply);• Forcing insurers to eliminate “pre-
existing conditions” from their policies;• Allowing young adults to stay on their
parents’ plan until age 26;• Establishing government-regulated
“insurance exchanges”; and• Heavily subsidizing the cost of pur-
chasing insurance for the poor.
Obama’s healthcare law has stiff costs and consequences, including less care, skyrocketing insurance premiums, likely national insolvency, and unchecked government powers.
10 THE NEW AMERICAN
HEALTHCARE
Outcome of ObamaCare

Four years after the Massachusetts reform passed, the healthcare package shepherded by Republican Governor Mitt Romney through the overwhelmingly Democratic legislature is in crisis. Costs to the state government have created a budget deficit and fiscal crisis; insurance costs have spiraled upward, with taxpayers facing the highest premiums in the nation; and the six largest insurance companies are suing the Governor’s Commissioner of Insurance in state court to raise insurance rates and avoid a repeat of the more than $200 million in losses they incurred in 2009. And last sum-mer, the state’s 10-member healthcare ad-visory board proposed healthcare rationing as a means of controlling costs.
This is the model upon which Obama’s national healthcare program was based.
Budget-busting SubsidiesThe Massachusetts fiscal crisis is ex-traordinary because the state has been raking in the bucks from federal stimulus money for its healthcare experiment. The nonpartisan Massachusetts Budget and Policy Center noted:
Nationally, one of the largest single al-locations within the American Recov-ery and Reinvestment Act (ARRA) is more than $128 billion provided to states for health care. Massachusetts will receive ... more than $3.5 bil-lion ... [in] direct health care benefits, funding for health care providers, funding for community-based health care and public health programs, and funding for health care research.”
Massachusetts’ $3.5 billion in federal healthcare subsidies amounts to more than $500 for every man, woman, and child in the Bay State.
But that hasn’t been enough money for the burgeoning Massachusetts healthcare budget, already under assault by high pre-miums for state employees and Medicare and Medicaid premiums.
Massachusetts State Treasurer Tim Ca-hill warns that Romneycare “is bankrupt-ing the state and would have bankrupted our state if not for the federal government being overly generous with Medicaid re-imbursements over these last four years. They’ve really propped the system up to keep it in place.”
Yet, over in Washington, D.C., Demo-cratic leaders trumpeted the similar health-care package on the federal level as a deficit reducer. The White House website claims that the new law “puts our budget and economy on a more stable path by re-ducing the deficit by more than $100 bil-lion over the next 10 years — and more than $1 trillion over the second decade.”
Despite the political promises of deficit reduction, the $938 billion ObamaCare legislation will actually lock in huge deficit spending on healthcare initiatives. ObamaCare does include $525 billion in tax increases and $455 billion in Medicare and Medicaid spending cuts over the next 10 years, but the Congressional Budget Office estimated that the bill would save only $143 billion compared with current law. That may sound like progress, but the key component of that estimate was “com-
pared with current law.” Congression al ap-propriators had already allowed the cur-rent law on Medicare and Medicaid to be on a path toward immense waste and out-of-control spending.
In the face of trillion dollar annual defi-cits projected out into the indefinite future, cutting less than $15 billion per year from expected increases — which ObamaCare would do — won’t substantially change that trajectory.
While some Medicare and Medicaid cuts in the bill would have been positive steps on their own, one of the key means by which the Obama administration claims “savings” in the bill is to cut physician reimburse-ments through Medicare and Medicaid. These payments are already below market costs, and Obama’s own U.S. Centers for Medicare & Medicaid Services concluded that “the estimated savings shown in this
www.TheNewAmerican.com 11
continued on page 14
President Obama and HHS Secretary Kathleen Sebelius will now preside over a healthcare system with deficit spending and higher insurance premiums locked in under the new “reform.”
AP Images

Charting the Murky Waters of ObamaCare
by Michael Tennant
If you think what you’ve seen of ObamaCare thus far is bad, think again. You ain’t seen nothin’ yet.
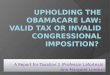
The Republicans of the congressional Joint Eco-nomic Committee, led by Sen. Sam Brownback of Kansas and Rep. Kevin Brady of Texas, have assembled a diagram to show just how all the new mandates, taxes, bureaucra-cies, and other expansions of government power fit to-gether. The result, which “portrays only about one-third of the complexity of the final bill,” according to Brady, is a frightening and impossibly complicated network of rules and regulations that separates patients from doctors and separates both from the actual cost of healthcare.
Brace yourself. The chart is to the right.Even a high-priced Washington attorney with a GPS
couldn’t navigate that mess.Notice how vast the gulf between physicians and pa-
tients is and how many other entities come between them.Notice, too, how one person, the Secretary of Health and
Human Services, seems to be in complete command of the entire healthcare system — as sure a recipe for disaster in the United States as such command-and-control structures were in the former Soviet Union.
Take note of the large number of orange entities; these represent mandates, programs, and agencies with the po-tential to result in rationing of care.
Hexagons represent brand new mandates. This writer counts five of those, but within one (insurance mandate) is contained 17 different mandates. Thus there are actually 21 new mandates represented in the chart, which, again, only shows about a third of the actual ObamaCare system.
Anything outlined in red or green, plus the circles repre-senting bundles of additional entities, means new or expand-ed government. Those, of course, cover most of the chart.
Blue-outlined entities are private entities with new man-dates, regulations, or responsibilities, which account for all private entities on the chart save one: self-insured health plans. How those escaped Congress’ notice is one of the great mysteries of our time.
There are also 19 special-interest provisions, accounted for by the blue triangle in the upper right-hand corner.
Then there is everyone’s favorite government agency, the Internal Revenue Service, which is charged with enforcing the mandates — as if income-tax season weren’t already stressful enough for most Americans.
The chart also portrays $569 billion in higher taxes, $529 billion in Medicare cuts, 16 million more Americans on Medicaid, and “two new bureaucracies with powers to impose future rationing: the Patient-Centered Outcomes Research Institute and the Independent Payments Advisory Board,” says the committee’s web page. #
!"#$%&'(#)*'$+%
,%-"./01'$'22%3."/.#*2
4!!!"#$%&!"#'%&!"#!%&
!$((
5+6'.%7'8%&'/9:#+".)%3."/.#*2
4!!((#'%&)(#"%&)(#$&
7'8%;"1'.$*'$+
**$##(%&(#$$!
*
*$#($
*$##)
**$'#$%&(#$"#
*)$#(
*)$#(
*)+#$
*$'#$%&(#$"#
*$#((
*,##"
*$##(
*$'#$
*$#("
*($#"
*)$#( *)$#(
*'##"
*$##'
*)$#(
*)$#(
*$#")
*$#")
*,##"
**-##-%&(#-#'.&/0123&*('#!
*-##,.&/0123&*('#'
*$##!
**-#(!%&(#-#).&/0123&*('#"
*$'#$
*$#((
*$#($
*,##"
**$##)%&(#$#(
*$##'
&#+0"$0$/%3"+'$+0#:
<#='2%,%>"$'+#.)%-''2?3'$#:+0'2?@9+2
5+6'.%A=(#$20"$2
B$1":1'*'$+%0$%C'#:+6%B$29.#$D'%>#.E'+
&'(.'2'$+2%F9$G:'2%"H%IGG0+0"$#:%A$+0+0'2
>#$G#+'2
<.92+%-9$GJ&#+0"$0$/%3"+'$+0#:K
5+6'.%7'8%<.92+%-9$G2?>"$'+#.)%F'$'H0+2
A=(#$G'G%;"1'.$*'$+;"1'.$*'$+%80+6%A=(#$G'G%I9+6".0+)?%&'2("$20L0:0+)
;"1'.$*'$+%-0$#$D0#:%A$+0+)%80+6%7'8%B$H:"82?59+H:"82
M+#+'?<'..0+".)%80+6%A=(#$G'G%I9+6".0+)?&'2("$20L0:0+)
*$#($*)$#(
*$##+
*(##(%&(#(#(
*$#("
*($$'%&(#(#'
*(!($%&(#(#)
*$##'*$##'*$##'
*$#("
*(#'#-
*'##(
*$'#$%&(#$"#
*,##"
*,##"
**-##-%&(#-#'
*-##,.&/0123&*('#'
*$##!
**$#"(%&(#$#!%&(#$#)*'##(
**$##)%&(#$#(
*'$#!
*,##"
**$##(%&(#$$!
*)$#(
**($((
*)$#(
*'##(
*$'#$%&(#$"#
*('((
**$##(%&(#$$!
*$##'*$##'
*$#((
*$#"(
*$#")
*'##(
*$#($
*)$#(
*)$#(
*'$#!
*(#'#-
*$#((
*$#("
*$$((
*$##!
*$##'
456789:;<=:>78&?;7@;<6
*$##(?ABC>D&4<:<&4>9DC79A;5&EF9:56*$##)%&(#$#(
0766A8>:F=G<95H&0<;5&I;<89>:>789&?;7@;<6*$#")
/79J>:KA<C>:25J7;:>?;7@;<*$##'%&$#
/79J>:<C&076J<;5&L5B9>:5*$##(
/79J>:<CM<CA5=G<95H&?A;DN<9>8@&?;7@;<6**$##(%&(#$$!
058:5;O7;&P5H>D<;5Q&P5H>D<>H&R887S<:>78
**$#"(%&(#$#!%&(#$#)
?NF9>D><8&M<CA5=G<95H&?<F658:&P7H>O>5;
**$##+
388A<C&T55*-##,.&/0123&
*('#'
/79J>:<C9**($((%&$##(%&(#$$!
EU>CC5H&VA;9>8@&T<D>C>:>59**$##)%&(#$(#
**$##)%&(#$#(
36BAC<:7;F&EA;@>D<C&058:5;9
**$##)%&(#$#(
/765&/5<C:N&3@58D>59
*$##)
P5H>D<C&45S>D5&P<8AO<D:A;5;9
**-##-%&(#-#'.&/0123&*('#!
?N<;6<D5A:>D<C&076J<8>59
*-##,.&/0123&*('#'
R8J<:>58:&25N<B>C>:<:>78&T<D>C>:>59
*$##'
/79J>D5&?;7@;<69
*$##'
??E=1W56J:&0<8D5;&/79J>:<C9
*$##!
P5H>D<;5&3H6>8>9:;<:>S5&078:;<D:7;9
*$$((
/5<C:N&R8HA9:;F
P<8H<:59%&25@AC<:>789%&I<W59%&Q&?<F658:&0A:9**($((%&$##(=$##)%&$$((%&-##,%&-##-%&(#$"+%&(#$$(%&(#$$!%&(#-#'.&/0123&
**('#'%&('#!
X78@=I5;60<;5&/79J>:<C9
*$##'
P5H>D<C&45S>D5
1WD>95&I<W**-##-%&(#-#'.&
/0123&*('#!
B3IF*$'#$%&(#$"#
R?3G&0789A65;&3HS>97;F&07A8D>C**$'#$%&(#$"#
P5H>D<;5&?<;:&3&I;A9:&
TA8H*$#")%&$'#$%&)$#(%-#(!
P5H>D<;5&?<;:&G&I;A9:&TA8H*$#")%&)$#(
?ABC>D/5<C:N&KA<C>:F&Q&
1OO>D>58DF&P5<9A;59&45S5C7J658:?;7@;<6**$#($%&(#$#'
/7A;9&7O&E5;S>D5&45:5;6>8<:>78&O7;&0<CDAC<:>8@&
16JC7F5;&P<8H<:5&?58<C:F**(!($%&(#(#)
2AC59&O7;&R89A;<8D5&
0C<>69&3JJ5<C9*(##(%&(#(#(
YOO>D5&7O&?5;97885C&P<8<@5658:
**($$'%&(#(#'
?;59>H58:**&$#("%&$#"'%&$'#$%&'##(%
&,##"%&(#$"#
0A;59&3DD5C5;<:>78&V5:Z7;U&
25S>5Z&G7<;H*(#'#-
VR/**'$#!%&)$#(%&
(#'#-
V<?ABC>D&0<6J
?;5S58:>?;7
*
0A;59&3DD5C5;<:>78&V5:Z7;U*(#'#-
0X3EE&R8H5J58H58D5&TA8H&G7<;H&7O&I;A9:559*,##"
X>O5&R8H5J58H58D5&3DD7A8:9
*,##"
0X3EE&R8H5J58H58D5&
TA8H*,##"
GC<DU&XA8@&G585O>:9&3D:
*(!!)
YOO>D5&7O&PAC:>=E:<:5&KA<C>O>5H&/5<C:N&?C<89*($$'%&(#(#'
?ABC>D/5<C:N&E5;S>D5
**$#((%&'##"%&'$#"
3HS>97;F[;7AJ&78&
?;5S58:>78%&/5<C:N&?;767:>78%&<8H&R8:5@;<:>S5&<8H&?ABC>D&/5<C:N
*'##(
?0Y2R&1WJ5;:&3HS>97;F&?<85C9*)$#(
?0Y2R&P5:N7H7C7@F&0766>::55
*)$#(
?0Y2R&G7<;H&7O&[7S5;87;9
*)$#(
?0Y2RL5B9>:5*)$#(
E:<:5&?;7:5D:>78&Q&3HS7D<DF&EF9:569*,##"
\A9:>D5&45J<;:658:
*)+#$
V<:>78<C&?;5S58:>78%&
/5<C:N&?;767:>78%&Q&?ABC>D&/5<C:N&
07A8D>C*'##(
?;5S58:>78Q&?ABC>D&
/5<C:N&TA8H*'##"
R8:5;<@58DF&L7;U>8@&[;7AJ&78&/5<C:N&0<;5&
KA<C>:F*$#("
?0Y2RI;A9:&TA8H
*)$#(
3@5&B**)$#(%&(#)#"
E7D><CE5DA;>:F&
3H6>8>9:;<:>78*('((
/765C<8H&E5DA;>:F&
45J<;:658:*('((
X<B7;&45J<;:658:
**(##(%&($#"%&($((%&(!((%&(!("%&(!($%&))#!%&(#(#(%&(#(#)
V<:>/5<C:N&44<:<&07C
25J7&EF9*'$
R8:5;<@58DF&?<>8&2595<;DN&077;H>8<:>8@&0766>::55
*'$#!
V<:>78<C/5<C:N&E:;<:5@F&Q&?;>7;>:>59YOO>D5*$#((
>'I>
N"9.%7'8%C'#:+6%@#.'%M)2+'*
V78=/79J>:<
M<CA5=G<9?A;DN<9>8?;7@;<6**$##)%&(#$#
*$##'
**$##"%&(#$"+%&(#$$(
**$##"%&(#$"+%&(#$$(
*$##+
**$##+
?NF9>D><8&KA<C>:F&25J7;:>8@&EF9:56
**$##"%&(#$"+%&(#$$(
36)20D0#$2**($((%&$##"%&$##$%&(#$"+%&(#$$(
HEALTHCARE
12 THE NEW AMERICAN

5+6'.%7'8%F9.'#9D.#D0'2
OO!!('("%&$!#-%&!(#(%
(#(#'%&(#""(%(#$$'%&(#'($%
(#!#(
5+6'.%7'8%P'*"$2+.#+0"$%,%30:"+%3."/.#*2
OQ!!("#(%&"+#'%&"+#!%&"+#)%&"+#+%&$#"$%&$#"'%&$(($%&$('#%&'"#'%&'"#)%&!$#'%&
!!#- %&)((" %&)((' %&(#"("%&(#""(%&(#$(! %&(#$"$ %&(#$") %&(#!#' %&
(#)#+
5+6'.%7'8;.#$+%3."/.#*2
RS!!(##"%&(##$ %&($((%&($""%(!)(%&"-!"%&"-!$ %&$!#( =) %&$!#,%&'(#(%&'(#,%& '"#(%&'"#" %&'$#' %&!(#" %&!"#) %&!"#,%&!$#( =!$#$ %&!$#!%
!$#) %&!$#- %&!$($%&!$(!%&!'#!%& !!#+ =,%
!)#'%&)+#$%(#$#(
(#$"$%&(#$$$%&(#'#, =(#%&(#'($%&(#!#(%&(#!#$
M('D0#:%B$+'.'2+%3."1020"$2
TS!!TTUOV%TOUTV%OUUQV%WTWXV%WOUTV%WWUTV%QUUTV%SUUTV%SUTUV%SUT4V%SUOWV%%TUOUTV%TUWTXV%TUWOWV%TUWO4V%TURUOV%%TUQUTV%TUSUTV%TUSURY%C@A&I% !! TTUTV%%TTUWVTTUQV%TOUWV%T4UQ
G1V1TR0R32R1E]&PA:A<C&7O&&Y6<N<&̂ V1_.4;A@&079.&V\&4;A@&079.332?.& X>BBF&P78:<8<89.
?NF9>D><8=YZ85H&/79J>:<C9.`8>Sa&7O&&0I.&P5H>@<J?C<89.X78@9N7;56<8&/5<C:N&?C<89.&&P5H>D<>H]&/R%&X3%&P3%&IV%&MI.&&&&P5H>D<;5]&0I%&TX%&PR%&PI%&V4
3[R]&3HbA9:5H&[;799&R8D7653/2K]&3@58DF&O7;&/5<C:ND<;5&2595<;DN&<8H&KA<C>:F040]&058:5;9&O7;&4>95<95&078:;7C&Q&?;5S58:>780/R?]&!"#$%&'()*+,'-$."+/(*0&-(1'+2&34&-50X3EE]&0766A8>:F&X>S>8@&399>9:<8D5&E5;S>D59&Q&EAJJ7;:90PE]&058:5;9&O7;&P5H>D<;5&Q&P5H>D<>H&E5;S>D590Y=Y?]&0789A65;&YJ5;<:5H&Q&Y;>58:5H&?;7@;<6TTE]&T55=O7;=E5;S>D5TE3]&TC5W>BC5&EJ58H>8@&3;;<8@5658:[3Y]&[7S5;8658:&3DD7A8:<B>C>:F&YOO>D5/0123]&/5<C:N&0<;5&Q&1HAD<:>78&25D78D>C><:>78&3D://E]&/5<C:N&Q&/A6<8&E5;S>D59&45J<;:658:
/E3]&/5<C:N&E<S>8@9&3DD7A8:R?3G]&R8H5J58H58:&?<F658:&3HS>97;F&G7<;HR2E]&R8:5;8<C&25S58A5&E5;S>D5P3=?4]&P5H>D<;5&3HS<8:<@5&?;59D;>J:>78&4;A@P5H?30]&P5H>D<;5&?<F658:&3HS>97;F&0766>99>78P124]&P5H>D<C&1<;CF&2>9U&45:5D:>7813XY2E]&1W5DA:>S5&3AW>C><;F&X>8U5H&YOO>D5&25@>78<C&EF9:569&P1L3]&PAC:>JC5&16JC7F5;&L5CO<;5&3;;<8@5658:V3R0]&V<:>78<C&3997D><:>78&7O&R89A;<8D5&0766>99>785;9VR/]&V<:>78<C&R89:>:A:59&7O&/5<C:N?0Y2R]&?<:>58:=058:5;5H&YA:D7659&2595<;DN&R89:>:A:5??E]&?;79J5D:>S5&?<F658:&EF9:56
*$#((
*")#"
*!)#!
*'$#"
*")#"
*")#"
*('((
**($$$%&(#(#'
**($'(%&(#(#'
*($((
*('((
*")#"
*$#((
*!)#!
*)+#$
*'##'
*$$((
*,##"
*(##(
*(##(
**-##'%&-##!.&/0123&*('#"
**('#(%&('("%&(#(#!.&/0123&**(##(%&(##'
**(!($%&(#(#).&/0123]&*(##$
*('"(%&(#(#!
**-##(%&(#-#(.&/0123&*('#(
**-#(#%&(#-#!.&/0123&*('#)
*'##"
*)+#$
*($'(%&(#(#'
*($$(%&(#(#'
**(##(%&(#(#(
*'##'
*($"$.&/0123]&*("#'
**($((%&(#(#'
*,##"
**-##(%&(#-#(.&/0123&*('#(
*($((
*($""
*($"$.&/0123]&*("#'
**($((%&(#(#'
*($($%&(#(#'
**($$(%&(#(#'
**('#(%&(#(#!
*($""
*)+#$
**$'#$%&(#$"#
*(#'#+
*$##(
*($$(%&(#(#'
*($($%&(#(#'
**(!#(%&(#(#).&/0123&**(##"%&(##'
**('#"%&('(".&/0123&*(##(
**('#"%&('(".&/0123&*(##(
!"#$%"#&'()*'+,-./'01,.,2-1'3,22-//##4'5#$6(7-1%.'8/%993,.:"#;;2%.'<#=-.'>"%&)4'8#.-,"'?,6;#'5#$6(7-1%.8#.%/,"'8%2'>",@.(%1A4'5%.A-.:'B#2(#"
3#+0'$+%3."+'D+0"$%,%IHH".G#L:'%@#.'%ID+V%3Z!Z%TTT[T4\YC'#:+6%@#.'%,%AG9D#+0"$%&'D"$D0:0#+0"$%ID+V%3Z!Z%TTT[TRO
*('"(%&(#(#!
7'8%&':#+0"$260(2&'/9:#+0"$2?&']90.'*'$+2?>#$G#+'2&'(".+0$/%&']90.'*'$+2
51'.20/6+
>"$')%-:"82@"$29:+#+0"$?IG102".)?B$H"%M6#.0$/M+.9D+9.#:%@"$$'D+0"$2%JB$D:9G'2%A=02+0$/K
3.01#+'
^$D6#$/'G%3.01#+'%A$+0+)
3.01#+'%A$+0+)%80+6%7'8%>#$G#+'2?&'/9:#+0"$2?&'2("$20L0:0+0'2
M('D0#:%B$+'.'2+%3."1020"$2
*$$#(.&/0123&*((#(
**('#(%&('("%&(#(#!.&/0123&**(##(%&(##'
**($$(%&(#(#'
E6<CC&GA9>8599&/5<C:N&YJ:>789&?;7@;<6
*($((
V3R0**($$$%&($'(%&
(#(#'
/0123&*('#"
*$$((
*"+#(
*"+#$
*!)#!
*"+#(
*")#"
*"+#$
**(!($%&(#(#).&/0123&*(##$
*,##"
*)$#(
**$##'%&$##!
*)+#$
*'(#"
**($'(%&(#(#'
*(#'#+
*(#'#+
*"+#(
*($$'%&(#(#'
**$#""%&(#$#+
*,##"
**($#(%&(#(#'
*($$$%&(#(#'
**($'(%&(#(#'
**("#(%&($#(%&($#'
**("#(%&($#(%&($#'
*($'"
*($#(
*(##(
**("#(%&($#(%&($#"
*($$(%&(#(#'*($#"
**($((%&(#(#'
*($'"
*(!((
*(!)(
*('((
*($'"
*'##'
*'##'
*'##'
*'##"
*($((
*)+#$
*)+#$
*$#("
*(!("
*(!((
*'##$
*,##"
*,##"
**-##(%&(#-#(.&/0123&*('#( **-##(%&(#-#(.&/0123&*('#(
**(##(%&(#(#(
*-##'
*-##$
**-#(#%&(#-#!.&/0123&*('#)
*-##"
**-##!%&(#-#".&/0123&*('#$
*(!#(
**($((%&(#(#'
**$(#$%&(#$"#
*($$'%&(#(#'
**($""%&(#(#'
*($$$%&(#(#'
*($("
*)$#(
*$#((
*$#")
*('((
*(##(
**("#(%&($#(%&($#"
*($$(%&(#(#'
*($'(%&(#(#'
*,##"
*(!($%&(#(#)
*))#!
**"##(="##'
**-#(+%&(#-#+
**(!#(%&(#(#).&/0123&**(##"%&(##'
**-#(!%&(#-#).&/0123&*('#" *-#($
*(!((
*(!((
**("#(%&($#(
*($("
I>:C5&RRR
**$"#(%&(#$(,.&/0123&*((#"
**(!('%&(#(#)
*($"(
*"+#$
*!)#!
**($((%&(#(#'
*-##"
*,##"
*('('
*('((
*"+#(
*$'#$%&(#$"#
*)+#$
*($$(%&(#(#'
*")#"
*(!("
**(!('%&(#(#)
*('((
*$#""%&(#$#+
*$#")
*"+#(
*"+#(
*"+#(
*"+#$
*'$#"
*('((
*'##'
*)+#$
*$#((
*$$((
*$$((
*$#"(
*,##"
**($((%&('($
*('((
*($($%&(#(#'
**(##(%&(#(#(
*!)#!
*(!("
*!)#!
KA<C>O>5H&/5<C:N?C<89**($#(%&($#"%($((%&(#(#'
/5<C:N0<;5&0N7>D5&076J<D:9**($$$%&(#(#'
25>89A;<8D5&?;7@;<6**($'(%&(#(#'
M<CA5=G<95H&R89A;<8D5&459>@8&Q&07S5;<@5&7O&?;5S58:>S5&/5<C:N&
E5;S>D59*(##(
YJ:>78<C&G<9>D&/5<C:N&?;7@;<6**($$(%&(#(#'
[3Y**('#(%&$##(%&$'#$%&)$#(%
(#(#!%&(#$"#
076J:;7CC5;&[585;<C**($($%&($""P5H?30
*")#"
E:<:59**($((%($$(%&
($$$%($'(%&(#(#'%&(#'#+
E:<:5&EA;S5F7;9
*)+#$
M>:<C&E:<:>9:>D9&3@58D>59
*(#'#+
`E&I5;;>:7;>59*($"$.&/0123&*("#'
c5FV<:>78<C&
R8H>D<:7;&EF9:56&R6JC5658:<:>78&
R89:>:A:5*!)#!
0766>99>78&78&c5F&R8H>D<:7;9
*!)#!
V<:>78<C&3D<H56F&7O&ED>58D59
*!)#!
@"$/.'22>'*L'.2%
,%3'.2"$#:%M+#HH%>#$G#+']&
Y8CF&1WDN<8@5&07S5;<@5
*($("
V<:>78<CI;<>8>8@&R89:>:A:5&O7;&T5H5;<C&<8H&E:<:5&EA;S5F7;9
*)+#$
3/2K*$#("%&$#($%&)#$(
A22'$+0#:C'#:+6%F'$'H0+2%
3#DE#/'**(##(%("#(%&($#(%
&($#" ?C<:>8A6G;78d5
E>CS5; [7CH
;"1'.$*'$+%C'#:+6%F'$'H0+%A=D6#$/'2**("#(%&($#(%($#"%&($((%&($("%&($($%&($"(%&($"$%&($$'%&('((%&('($%&(#(#'.
/0123&*("#'
R8:5;85:&?7;:<C*($((
4<:<&07CC5D:>78
*($((
//E&R89J5D:7;&[585;<C*($($%&,##"%(#(#'
1C>@>B>C>:F&45:5;6>8<:>789
*('((
?;>S<DF&E:AHF*('((M'D.'+#.)
C'#:+6%,%C9*#$%M'.10D'2
C'#:+6B$29.#$D'@5[53**($""%&(#(#'
0Y=Y?&3HS>97;F&G7<;H*($""%&(#(#'
?;>S<:5&?A;DN<9>8@&07A8D>C
*($""
`E?;5S58:>S5&E5;S>D59&I<9U&T7;D5
*(##(
/5<C:N&E<S>8@9&3DD7A8:9**-##$%&-##'
P5H>D<;5&G585O>D><;>59
*$$((
/5<C:N&R89A;<8D5&?7C>DF&/7CH5;
**(##(%&(#(#(
E6<CC&16JC7F5;9**($#'%&($((%&('"(%&(!("%&
(#(#!
X<;@5&16JC7F5;9**($#'%&(!((%&(!("%&(!($%&
(!('%&(#(#)
P5H>D<;5?<;:&0&Q&?<;:&4&
R89A;5;9*$$((
X<;@5&[;7AJ&P<;U5:
**("#(%&($#(%&(!((
?;56>A6I<W&0;5H>:&EAB9>H>59
**('#(%&('("%&(#(#!.&/0123&**(##(%&
(##'
388A<C&T55**-#(#%&(#-#!.&/0123&*('#)
$a,e&R8S59:658:&R8D765&I<W/0123&*('#"
/E3`95&259:;>D:>78
*-##$
P>9A95&7O/E3&TA8H9
*-##'
6!-%#$$-12$-(*7+8-9**-##(%&(#-#(.&/0123&*('#(
EAB9>H>59]YA:=7O=?7DU5:&1WJ58959**('#"%&('("./0123*(##(
R8H>S>HA<C9
P<8H<:59%&25@AC<:>789%Q&I<W59
**($((%&('((%&(!#(%&-##$=-##!%&-#($%&-#(!%&-#(+%&(#(#)%&(#-#"%&(#-#)%&(#-#+.&
/0123&**(##"%&(##'%&('#"%&('#$
6:91'**#;'+2&3<#.*7**(##(%&(#(#(
3#+0'$+2
P5H>D<;5?<F;7CC&I<W
R8D;5<95]&#a-e**-#(!%&(#-#).&/0123&*('#"
TC5W>BC5&EJ58H>8@&3;;<8@5658:
*-##!%&(#-#".&/0123&*('#$
Y8CF&P5H>D<C&1WJ58959
3B7S5&(#e&7O&R8D765&^3[R_&<;5&I<W&45HAD:>BC5
*-#($
TE3&078:;>BA:>78X>6>:]&f"%!##**-##!%&(#-#".&/0123*('#$
2>9U07;;>H7;9
*($'"
X<;@5&GA9>8599&16JC7F559*(!((%&(!("
E6<CC&GA9>8599&16JC7F559
*(!("
P1L3/5<C:N&?C<89**($#(%&))#!
E5CO=R89A;5H&/5<C:N&?C<89
*($#(
E6<CC&[;7AJ&P<;U5:
*($#(%&($#'%&($'"R8H>S>HA<C&P<;U5:*("#(%&($#(%&($#'%&($'"
(#e&I<W&Y8&
R8H77;&I<88>8@&E5;S>D59]**-#(+%&(#-#+
L"&/5<C:N&
R89A;<8D54>9DC79A;5
*-##"
B$G010G9#:%>#$G#+']&GAF&/5<C:N&R89A;<8D5**(!#(%&(#(#).
/0123&**(##"%&(##'
A*(:")'.%>#$G#+']&
&?;7S>H5&/5<C:N&R89A;<8D5**(!($%&(#(#).&/0123&*(##$
P<8H<:7;F&L7;U5;&3A:7=18;7CC658:
*(!((
E6<CC&GA9>8599
/5<C:N&R89A;<8D5&I<W&0;5H>:
**('"(%&(#(#!
B$29.#$D'%>#$G#+'2&&&
&&&**(##(%&((#(%&&&&&("#(%&("!(%&&&&&&&&&(#(#(%&&&&&&&&&&&&(#(#$.&&&&&&&&&&&&&&&/0123&&&&&&&&&&&&&&&&&&*"$#(
TX
/5<C:N&R89A;<8D5&076J<8>59
P<8H<:59%&25@AC<:>789%&&25gA>;5H&G585O>:9%&Q&
I<W59**(##(%&("#(%&("!"%&($#(%&($$'%&($'(%&$$((%&-##(%&-#(#%&(#(#(%&(#(#'%&(#-#(%&
(#-#!.&/0123&**('#(%&('#)
16JC7F5;9
P<8H<:59%&25@AC<:>789%&Q&I<W59
**(!((%&(!("%&(!($%&-##(%&-##"%&(#(#)%&(#-#(.&/0123&**(##$%&('#(
TTE&3DD7A8:<BC5&
0<;5&Y;@<8>d<:>789&?;7@;<6**$#""%&(#$#+
:<C&:F&>8@&<6##!
P5H>D<>H&/5<C:N&/765&?;7@;<6
*"+#$
T5H5;<C&077;H>8<:5H&/5<C:N&0<;5&YOO>D5*")#"
P5H>D<>H&KA<C>:F&
P5<9A;5658:&?;7@;<6
*"+#(
E:<:5=EJ5D>O>D&3HAC:&/5<C:N&KA<C>:F&P5<9A;59*"+#(
P5H>D<>H&1WJ<89>78]&h()&6>CC>78**"##(="##'
0GY&079:&19:>6<:5%$i"#i(#
E:<:5&P5H>D<>H&3@58D>59**")#"%&"+#(%&"+#$%&
$#((
P5H>D<;50A:9]&f!",a-B8^>8DCAH59&P3&DA:9_
I>:C5&RRR.&0GY&079:&19:>6<:5%
&$i"#i(#
P5H>D<;5&3HS<8:<@5&
0A:9]&f"#!a-B8**$"#(%&(#$(,.&/0123&*((#".&0GY&079:&
19:>6<:5%&$i"#i(#
EAB9>HF]&P5H>D<;5&?<;:&4&4;A@&?;7@;<6&6=3(0.+,3$'7*$$#(.&/0123&
*((#(
/5<C:N&RI&?7C>DF&0766>::55
*(!)(
V<:>78<C&4><B5:59&
25J7;:&0<;H&?;7@;<6*(#'#+
0X3EE&R8H5J58H58D5&G585O>:&?C<8
*,##"
040**(##(%&'##$%&'##'%&
'(#"%&(#'#+V<:>78<C&
?<;:85;9N>J&78&?;5S58:>78&Q&/5<C:N&
?;767:>78*'##'
<:>78<C&1HAD<:>78&J<>@8&78&>78&Q&/5<C:N&767:>78*'##'
0766A8>:F&?;5S58:>S5&E5;S>D59&I<9U&
T7;D5*'##$
V<:>78<C&Y;<C&/5<C:N&?ABC>D&1HAD<:>78&0<6J<>@8
*'(#"
V<:>78<C&4><B5:59&P7;:<C>:F&E:<:>9:>D9&1HAD<:>78&I;<>8>8@&?;7@;<6
*(#'#+
1C>@>B>C>:F&399599658:&EF9:56*,##"
?5;978<C0<;5&3::58H<8:9&L7;UO7;D5&
3HS>97;F&?<85C*,##"
0X3EE&R8H5J58H58D5&3HS>97;F&07A8D>C*,##"
EA;@578&[585;<C*'##(
?;5S58:>78&L5B9>:5*'##'
L5B9>:568&-(*>-&'(1?+#(+@3;'&(5'(.7
*(!!"
0X3EE&?;7@;<6
*,##"
YOO>D57O&I<W&38<CF9>9**($$(%&(#(#'
1CH5;&\A9:>D5&
077;H>8<:>8@&07A8D>C
*)+#$
3HS>97;FG7<;H&78&1CH5;&3BA95%&V5@C5D:%&Q&1WJC7>:<:>78
*)+#$
PAC:>=4>9D>JC>8<;F&?<85C9&78&
R6J;7S>8@&X78@=I5;6&0<;5*)+#$
1CH5;&3BA95%&V5@C5D:%&Q&1WJC7>:<:>78&
T7;589>D&058:5;9*)+#$
B&M**('#(%&('#"%&('((%&('("&('('%
('"(%&(!#(%&-##'%&-##!%(#(#!%&(#-#(.&/0123&
**('#(%&('#"
I;5<9A;F&45J<;:658:**($((%&($$(%&'##"%&
,##"%&(#(#'
>78<C&>9J<;>:>59&CC5D:>78&Q&7;:>8@9:56$#"
/5<C:N0<;5&KA<C>:F&L5B9>:5**$#((%&$#("
>'G0D#0G?@CB3
I>:C5&RR.&**('($%&$#((
'G0D#.'>:C5&RRR%&!"#$"
@>M**$#($%&$#"(%&$#")%&$'#$%&(#$#!%&(#$#)%
(#$"#
P5H>D<;5&?;59D;>J:>78&4;A@&<8H&P3=?4&
076JC<>8:&EF9:56*$$((
0PE&3D:A<;F
**($$(%&$'#$%&(#(#'
078@;599*!($("%&('((%&$$((%&!)#!%&,##"
<C95H&8@&6#(
13Call 1-800-727-TRUE to subscribe today!

memorandum for one category of Medicare proposals may be unrealistic.” The reason was because it would bankrupt or force out of the Medicare market within a decade a fifth of the healthcare providers. The feder-al agency concluded: “Providers for whom Medicare constitutes a substantive portion of their business could find it difficult to remain profitable and, absent legislative in-tervention, might end their participation in the program (possibly jeopardizing access to care for beneficiaries).”
The way Washington politicians are able to claim the new healthcare law cuts the deficit is by engaging in what can only be called creative accounting. This creative accounting might be compared to a family that spent $3,000 on a vaca-tion last year and plans to spend $10,000 on the summer vacation this year despite only having an income to support the same $3,000 vacation. So the wife pro-poses the family makes “cuts” of $500 to the $10,000 vacation plan, arguing that the cuts bring the family closer to their budget. But the reality is that com-mitting to a $9,500 vacation on a $3,000 budget is a foolish path that takes them further from their goal of living within their means. All the bill has done is lock the nation into the path toward insolvency that Obama correctly warned about.
Spiraling Premium CostsThe increased cost to government is only a small part of the problem with the na-tional healthcare law, however. Most of the additional costs will be borne by insurers and their customers, as has happened in Massachusetts. Before the healthcare mandate in Massachusetts, the state gov-ernment picked up the tab for indigent medical care by reimbursing hospitals directly. Now, as in Massachusetts, much of the cost of the subsidies will be foisted
upon insurers, and therefore, upon policyholders. Thus, it shouldn’t be any surprise that the leftist Common-wealth Fund of Massachu-setts recently concluded the Bay State therefore had the highest family health insur-ance premiums in the nation (averaging $13,788 in 2008 and projected to increase to
an estimated $26,730 by 2020).While the Commonwealth of Massachu-
setts has substantial authority to regulate in-surance rates, authority for the federal gov-ernment to regulate health policy rates is not clearly delineated in Obama’s bill. But the Obama administration is already cam-paigning for that power. Obama proposed legislation to grant the executive branch power to regulate rates at a February 2010 “health care summit,” and his Secretary of Health and Human Services, Kathleen Se-belius, has been railing against insurance industry pricing. “If insurance companies are going to raise rates, the least they can do is tell us why,” Sebelius charged in a March letter posted on the HHS website, adding her opinion that insurance industry profits were “wildly excessive.”
A good part of the reason policy rates are increasing in Massachusetts — and will increase nationally under the new federal law — is the requirement that in-surance companies must accept all poli-
cies despite “pre-existing conditions.” People with chronic diseases such as mul-tiple sclerosis or cancer are guaranteed to lose money for insurance companies. The whole purpose of insurance is to pay a small amount that anticipates an unlikely but possible catastrophic healthcare cost; insurance companies plan to make money on most of the insured while losing money on the few who fall sick.
But the ban on exempting pre-existing conditions imposes a different type of burden upon insurance companies. It can be likened to requiring home insurance companies to insure a house against loss while it is on fire. Such a requirement is liable to abuse, as has already happened in Massachusetts.
The Massachusetts system is being “gamed,” according to the Boston Globe, by consumers who purchase insurance for a few months to take care of expensive surgery that they know is coming — such as a knee replacement — and then cancel the coverage after the operations: “Thou-sands of consumers are gaming Massa-chusetts’ 2006 health insurance law by buying insurance when they need to cover pricey medical care, such as fertility treat-ments and knee surgery, and then swiftly dropping coverage, a practice that insur-ance executives say is driving up costs for other people and small businesses.” This can happen because the fine costs less than carrying the insurance.
ObamaCare has no immediate provision for healthcare rationing, but if Massachusetts’ experience is any indicator it will soon be back on the table. There, regulators proposed healthcare rationing as a means of controlling costs.
Knee surgery: Many in Massachusetts are gaming the “no pre-existing conditions” system by buying policies only for the months they need expensive surgeries, such as knee and hip replacements, and then canceling the policies and paying the mandated fine.
AP
Imag
es
14 THE NEW AMERICAN • AUGUST 16, 2010
HEALTHCARE
continued from page 11

The tactic is forcing insurers to register huge losses. “This week Blue Cross Blue Shield reported a big uptick in short-term customers who ran up costs more than four times the average, only to drop the coverage within three months,” the Wall
Street Journal reported on April 9. “Last July, Charlie Baker detailed similar gam-ing at Harvard Pilgrim, the health plan he used to run. Between April 2008 and March 2009, about 40% of its new en-rollees stayed with it for fewer than five
months and on average incurred costs about 600% higher than the company would have otherwise expected.”
Blue Cross Blue Shield of Massachu-setts, a supporter of ObamaCare, is nev-ertheless a party suing the Massachusetts
What the Healthcare Law Means to YouThe new federal healthcare law will impact all Americans
with threats of fines and unprecedented federal interven-tion in regulating the insurance industry, health professionals, and even the family. Art Thompson, CEO of The John Birch Society, explains that the Patient Protection and Affordable Care Act and the reconciliation bill are just a framework to be filled in as bureaucrats add regulations to the new law. “There’s no smoking gun. It’s a cocked pistol that’ll be fired when the regulations come down,” Thompson says, adding that most people “apparently haven’t noticed the fact that this is a pro-gram to reach down into every home.” Here’s the impact in brief:
Doctors and Healthcare Professionals• Pay squeeze: Creates greater dependence upon shrinking gov-
ernment Medicare/Medicaid reimbursements. The bill does nothing to stop recent reimbursement cuts.
• More regulations: Dozens of additional government forms and regulations to follow.
Small Businesses (50 employees or more)• $2,000 per-employee fine: Companies will be fined for not
offering health insurance by 2014. (Section 1513)• $3,000 fine: Employers must subsidize health insurance for
employees who earn up to 400 percent of the poverty level. Employers who fail to do so will be fined $3,000 per incident. (Section 1513)
• File more reports to the federal government: Companies must detail the coverage they offer. (Section 1514)
• Menu nutritional labeling: All restaurants (not just those with at least 50 employees) and vending machines will have to pro-vide nutritional information. (Section 4205)
Insurers• Federal manipulation of the insurance market: Federal offi-
cials will “make recommendations, as appropriate, to the State Exchange about whether particular health insurance issuers should be excluded from participation in the Exchange based on a pattern or practice of excessive or unjustified premium increases.” (Section 2794)
• Require government approval before increasing premiums: The law “shall require health insurance issuers to submit to the Secretary and the relevant State a justification for an unrea-sonable premium increase prior to the implementation of the increase.” (Section 1003)
• Sets executive salaries: Determines maximum salary of $500,000 per year beginning in 2012. (Section 9014)
Individuals and Families• Meddling in your home: Billions of dollars fund new pro-
grams for “home visitation” and other grant-created agencies designed to manage your and your children’s weight, eating habits, exercise routine, and other lifestyle habits — all in the name of controlling healthcare costs to the federal government.
• Fine for noncompliance: By 2016, those who don’t purchase government-approved private health insurance will be assessed $750 on their income tax. (Section 5000A)
• Higher private health insurance premiums: As the financial squeeze is put on doctors and insurers owing to losses on Medi-care/Medicaid patients, the costs for other patients can be expect-ed to rise. Should government respond by requiring below-market reimbursements for all patients, an exodus of qualified doctors will occur and rationing of healthcare services can be expected.
• Medicare/Medicaid patients may have more trouble seeing the doctors of their choice: How can it be otherwise when doctors are forced to accept below-market reimbursements for Medicare/Medicaid patients? #
Quality care endangered: Poor families may soon have more difficulty finding affordable coverage or care. Many doctors have indicated they may stop taking Medicare/Medicaid patients, and in Massachusetts only one insurance company is offering coverage through the state “exchange.”
AP
Imag
es
15www.TheNewAmerican.com

government in court in the hopes of avoid-ing a repeat of their massive 2009 losses, claiming: “We are hopeful these additional funds can be used to offset the impact of the law’s new taxes while addressing the serious problem of cost shifting from pub-lic payers like Medicaid to private payers like Blue Cross Blue Shield of Massachu-setts. This cost shifting, or underpayment to doctors and hospitals by government payers, adds significant costs for private employers and consumers who participate in private health plans.” Blue Cross Blue Shield of Massachusetts, the state’s largest insurer, lost $149.2 million in 2009 — the first such loss in 13 years.
Clearly, the reason rates are increasing in Massachusetts isn’t corporate greed and excessive profits. You can’t make that argument when the insurers are los-ing money. Thus, it’s hardly surprising the Massachusetts Attorney General’s office recently investigated the healthcare sys-tem in the state and concluded that “the
present health care marketplace does not allow employers and consumers to make value-based purchasing decisions.” Of course, a large part of the reason both in-surers and hospitals charge prices for care that have little relation to the actual cost of the care is because they have to make up for their losses incurred as a result of costly government mandates such as the no pre-existing conditions mandate. The Massachusetts Attorney General’s Office concluded: “Our findings show the sys-tem lacks transparency in both price and quality information, which is critical for employers and consumers to be prudent purchasers.” Sadly, that same office failed to notice that the mandates have made that transparency all but impossible.
While the Massachusetts Attorney General’s Office report failed to link the pre-existing conditions mandate as the reason for the disconnect from the actual cost of the services and the price charged, they did conclude that “our preliminary
review has revealed serious system-wide failings in the commercial health care mar-ketplace which, if unaddressed, imperil access to affordable, quality health care.”
ObamaCare, like Romney-care, also relies upon both an individual and corporate tax increase called a “mandate.” The numbers are slightly dif-
ferent between the Massachusetts and Obama system, but the intent is still the same: Fine individuals on their income taxes if they don’t purchase health insur-ance and fine companies that don’t offer “affordable” coverage to employees. The employer mandate is soft in Massachu-setts at $295, but ObamaCare’s employer mandate can cost companies many thou-sands of dollars.
In Massachusetts, the individual man-date can cost a family as much as $1,116 per year in higher taxes. The ObamaCare mandate is smaller at first, just $95 per year in 2014 for failure to purchase insur-ance, increasing to $750 per year by 2016. But Romney’s law started with a penalty of about $100 as well. The Massachusetts penalty is expected to increase to more than $3,500 in coming years, in order to cover half the cost of purchasing the state’s Medicaid program, MassHealth. Once Obama gets the mandate tax started, there’s no telling how high the penalty could go. The tax will certainly rise steep-ly in coming years.
RationingObamaCare has no immediate provision for healthcare rationing, but if Massachu-setts’ experience is any indicator it will soon be back on the table. Even before the current Massachusetts rate war between Governor Deval Patrick and the insur-ance companies began, state regulators in the Special Commission on the Health Care Payment System proposed health-care rationing as a means of controlling costs. “Hospitals and doctors may be put on budget” as the Boston Globe termed it on July 17 last year, noting that “patients could find it harder to get procedures they want but are of questionable benefit if doctors are operating within a budget. And they might find it more difficult to get care wherever they want, if primary doctors push to keep patients within their accountable care organization.”
The Massachusetts commission con-cluded the state should adopt limits on hospital healthcare spending and govern-ment-mandated “evidence-based” stan-dards for distributing medicine. A major part of the cost problem in Massachusetts — as in the rest of the country — has been defensive medicine based upon a broken malpractice system. But the Massachu-
The federal agency concluded: “Providers for whom Medicare constitutes a substantive portion of their business could find it difficult to remain profitable and ... might end their participation in the program.”
16 THE NEW AMERICAN • AUGUST 16, 2010
HEALTHCARE

setts commission failed to take notice of this, just as malpractice reform went unaddressed by the ObamaCare legislation.
Because ObamaCare is a vir-tual carbon copy of Massachu-setts’ Romneycare, the nation will likely suffer a similar fate as the emerging Massachusetts disaster. The Boston Business Journal on April 1 reported “rate hikes that have reached 50 percent for some small businesses.” And the “so-lution” politicians have settled upon is to blame insurance com-panies for the mandates and the rotten system the politicians have set up. But this political postur-ing offers no solution to insur-ance companies that are already bleeding millions. “It’s like tell-ing Dunkin’ Donuts to charge 50 cents for a cup of coffee when all the ingredients and labor add up to a dollar,” Lora Pellegrini, president of the Massachusetts Association of Health Plans, told the Boston Business Journal for March 5. Most insurers in Massachusetts have sim-ply stopped writing new policies in order to cut their losses, a lesson the Bay State should have learned after chasing nearly all national auto insurance companies out of the state after instituting auto-insurance price regulations in the late 1970s (none of the five top nationwide auto insurers would write new policies in Massachusetts for dec ades).
Governor Patrick’s office automatically rejected any healthcare-premium increases of more than 4.8 percent, which is 150 per-cent of the Medical Price Index for 2009, a measure of inflation in the medical in-dustry. When six insurers took the state to court, the Governor’s office yanked the six off the Mass Health Connector, the state health insurance exchange. As of April 12, only a single insurer is offering insurance on the Connector.
The Wall Street Journal for April 9 summed up the position in Massachusetts:
State officials have demanded that the insurers — under the threat of fines and other regulatory punishments — resume offering quotes by today and to revert to year-old base premiums.
Let that one sink in: Mr. Patrick has made the health insurance business so painful the government actually has to order private companies to sell their products (albeit at sub-market costs).
But the federal plan is in some ways worse than the Massachusetts plan in the number of new bureaucracies it creates. The bill includes state grants for “home visitation” and “corrective action plans” and even “improvements in parenting skills” and “improvements in school readiness and child academic achieve-ment.” Though these grants are officially for “at risk,” i.e., inner city, communities, it sets the principle to allow the govern-ment to snoop into every home in Ameri-ca to assess parents’ ability to be parents and manage every American’s lifestyle. In addition to families in “at risk” com-munities, the stated homes to be serviced include residences that have “users of tobacco products in the home,” “families that are or have children with low student achievement,” “families with children with developmental delays or disabili-ties,” and “families who, or that include individuals who, are serving or formerly served in the Armed Forces.”
Another section of the bill calls for cre-ation of a National Prevention and Health Promotion Strategy that would make a “list of national priorities on health pro-motion and disease prevention to address lifestyle behavior modification (smoking cessation, proper nutrition, appropriate exercise, mental health, behavioral health, substance use disorder, and domestic vio-lence screenings) and the prevention mea-sures for the 5 leading disease killers in the United States.”
The bill authorizes “individualized wellness plans” demonstration projects and a billion-dollar “National Health Ser-vice Corps” to see to it that its goals are fulfilled. The bill creates grant authori-ties to supervise lifestyles for all stages of life, from infants and school-age children all the way up to senior citizens. Under Obama’s healthcare package, your pot belly or the Oreo cookie snack you pack for your child at lunch literally becomes a federal issue.
Americans who wish to avoid this mess need to mobilize for a full repeal of the healthcare law by pressuring Con-gress for a full repeal and pressuring state legislators to nullify ObamaCare within their states. #
Hope for repeal: A rising hope for affordable healthcare is that the Obama law is increasingly unpopular and faces a political uprising against the Democratic freshman Congressmen who provided the margin of victory for Obama’s forces.
AP
Imag
es
Call 1-800-727-TRUE to subscribe today! 17

Get involved! Go to JBS.org
ObamaCare 101JBS CEO Art Thompson takes you into the new healthcare law. Find out what’s really in the new law and what you can expect long term. (2010, 23min, sleeved DVD, 1/$1.00; 11-20/$0.90ea; 21-49/$0.80ea; 50-99/$0.75ea; 100-999/$0.70ea; 1000/$0.64ea) DVDO1Ø1(2010, 24min, Audio CD, 1/$1.00; 11-20/$0.90ea; 21-49/$0.80ea; 50-99/$0.75ea; 100-999/$0.70ea; 1000/$0.64ea) CDO1Ø1
ObamaCare and YouThe question of whether ObamaCare will or won’t work has already been answered — in the state of Massachusetts specifically and in doctors’ offices generally. Learn the costs and consequences. (May 10, 2010, 48pp, 1/$2.95, 10/$12.50, 25/$22.50, call for special rates on case lots of 100) TNA100510
Stop ObamaCare Banner Printed indoor/outdoor vinyl banners. Allow for a 2-3 week delivery. ($100.00 POSTPAID)*Also available as downloadable 4 x 8 Banners. ($10.00) EDELBSO, EDELBSOJ
EDELPOSTSO EDELPOSTSOI EDELPOSTSOWEDELPOSTSOC
Intended more for use outside as it includes JBS contact info for ObamaCare campaign. BSO
Use this eye-catching banner as a back-drop for your booth to promote the ObamaCare campaign. BSOJ
Posters24” x 36” downloadable posters ($10.00)

ObamaCare SlimJims(1/$0.28; 100/$0.25ea; 500/$0.20ea) General — SJSOG Seniors — SJSOS Family — SJSOF
BumperstickersBoth versions available in
regular or magnetic formats.
3 x 11 1/2 inch regular bumper sticker (1/$1.00; 100/$0.75ea)
3 x 11 1/2 inch magnetic bumper sticker (1/$2.25; 100/$2.00ea)
BillboardCall to order. ($50.00) BBSO
NullificationLoaded with primary sources among the more than 100 pages of appendices, Thomas Woods’ Nullification should become an action manual for committed activists of the Tea Party movement on the federal healthcare mandates and a host of other issues. (2010, 309pp, hb, $24.95) BKN
Window Cling(1/$2.00; 100/$1.75ea) WCSO
BSSO (regular), BSSOM (magnetic)
BSSOJ (regular), BSSOJM (magnetic)
The New World of ObamaCare ReprintDo you know what the passage of ObamaCare means for you and your family? Much more than health insurance is involved. Find out the truth in this compilation of articles from the May 10 and August 30, 2010 issues of THE NEW AMERICAN. The reprint also includes an orga-nizational chart of the new healthcare system. (2010, 24pp, 1/$1.00; 25/$0.85ea; 100/$0.75ea; 500/$0.65ea; 1,000+/$0.50ea) RPO81Ø
TITLE
000 0000 000 000
0000 0000 0000 0000
0000
!
Name ______________________________________________________________
Address ____________________________________________________________
City _____________________________ State __________ Zip ________________
Phone ____________________________ E-mail ______________________________
" Check " VISA " Discover" Money Order " MasterCard " American Express
# _________________________________________ Exp. Date ________________
Signature ____________________________________________________ RPO810
QUANTITY PRICE TOTAL PRICE
Official Store of The John Birch Society
Credit-card orders call toll-free now! 1-800-342-6491Order Online: www.shopjbs.org
Mail completed form to:ShopJBS • P.O. BOX 8040
APPLETON, WI 54912
VISA/MC/DiscoverThree Digit V-Code
American ExpressFour Digit V-Code
Make checks payable to: ShopJBS ___ ___ ___ ___ ___ ___ ___
SUBTOTAL WI RESIDENTS ADD 5% SALES TAX
SHIPPING/HANDLING(SEE CHART BELOW)
For shipments outside the U.S., please call for rates.
Order Subtotal$0-10.99
$11.00-19.99$20.00-49.99$50.00-99.99
$100.00-149.99$150.00+
Standard Shipping$4.95$7.75$9.95$13.75$15.95
call
Rush Shipping$9.95$12.75$14.95$18.75$20.95
call
Standard: 4-14 business days. Rush: 3-7 business days, no P.O. Boxes, HI/AK add $10.00
TOTAL

by William F. Jasper
Repealing ObamaCare is not an option — it is absolutely essen-tial. It is absolutely essential, that
is, if the United States of America is to survive as a constitutional republic with a federal government of limited powers. Repealing ObamaCare is also absolutely necessary if we hope to avoid national economic collapse.
To those who may think such state-ments are overblown, we strongly advise that they read, in particular, Thomas R. Eddlem’s “Outcome of ObamaCare” in our May 10 issue as well as Michael Ten-nant’s article in this issue (page 10). As they amply demonstrate, the mammoth “health care reform” bill that was rammed through Congress last March and signed by President Obama is jam-packed with dangerous language that will provide fed-
eral bureaucrats with vast new powers that are compatible with totalitarian systems of government, but not with the American tradition of liberty.
ObamaCare, known officially as the Pa-tient Protection and Affordable Care Act, is one of the most revolutionary legislative proposals ever to be enacted in this coun-try. Much of the opposition to it has cen-tered on the horrendous economic costs the gargantuan new program will impose on our already bankrupt federal govern-ment. That, of course, is a major, and very legitimate, concern. However, there are other aspects of ObamaCare that are equally important to, if not more important than, its financial impact.
This is one of the most far-reaching leg-islative efforts ever passed by Congress. It is far more than “mere” nationalized, socialized medicine. It will, if allowed to stand, inaugurate social engineering by “experts” on a scale heretofore unimag-ined … except in the dreams of apostles of the total state. Did the American people demand healthcare “reform” that man-dates federally imposed “lifestyle behav-ior modification” with regard to “proper nutrition,” “appropriate exercise,” “mental health,” and “behavioral health”? Did we envision the invasion of our homes and family privacy to implement “domestic violence screenings,” “childhood home visitation,” and “improvements in parent-ing skills”? How will ObamaCare’s provi-sions on abortion, sex education, vaccina-tions, rationing, and database monitoring play out — if we fail to repeal it?
Analysts for pro-life organizations have charged that the abortion provisions of ObamaCare represent the largest expan-sion of abortion since Roe v. Wade. Other sections of the legislation are sure to prove equally far-reaching.
Multi-pronged Plan of ActionSome of the erstwhile opponents of ObamaCare have assumed the defeat-ist position that attempts to repeal it are hopeless. Adopting the “resistance is fu-tile” stance, they point to the fact that the radical Obama-Reid-Pelosi forces control
Rep. Steve King (R-Iowa), left, looks at a copy of the ObamaCare bill after a rally against the bill on Capitol Hill in Washington, in November 2009.
AP
Imag
es
THE NEW AMERICAN20
HEALTHCARE
Repealing ObamaCare
Since ObamaCare will finish bankrupting our country and gives our government virtually unchecked powers to command Americans to make lifestyle changes, it must be repealed.

the White House and both houses of Con-gress. Nevertheless, ObamaCare is not an irreversible fait accompli; no legislation ever is, as long as dedicated patriots are willing to fight to repeal it.
The question then arises as to the best manner of “undoing” ObamaCare. A wide array of responses — at both the state and federal levels — is being proffered as so-lutions. No sooner had President Obama signed his namesake legislation than Members of Congress were introducing bills to repeal it. The problem is many of these proposals are Republican “repeal and replace” bills to simply substitute less onerous and intrusive “ObamaCare Lite” versions that are also unconstitutional and unacceptable. Top GOP spokesmen (House Minority Whip Eric Cantor, Rep. Charles Boustany, and former Wisconsin Governor and former Bush administration Secretary of Health and Human Services Tommy Thompson) have said they agree with 80 percent of ObamaCare!
Replacing ObamaCare with a slightly lighter version acceptable to these Repub-licans would not be a victory. However, among the confusing profusion of bills are a few well-crafted and viable options that should be supported.
In another approach to undoing Obama-Care, a number of state Attorneys General have launched lawsuits challenging the law in federal court on grounds that it trespasses on the rights of the states. Simi-larly, several state legislatures, responding to grass-roots efforts, are using a “nullifi-cation” strategy to challenge the law on constitutional grounds. Each of these ap-proaches has its merits.
Congressional Repeal: The “cleanest” and most efficient means of repealing ObamaCare is through passage of legisla-tion in both the House and Senate to do just that. Obviously, that will be close to impossible with the current makeup of Congress, and even if that were to occur, President Obama would veto it. Never-theless, the Democrats are likely to lose a sizeable number of congressional seats in the November elections and the Obam-aCare vote will play a significant role in the turnover. In addition to expanding that turnover, forcing another key vote on ObamaCare can also send a strong mes-sage to help build momentum for repeal in the next Congress.
H.R. 4972, introduced by Rep. Steve King (R-Iowa), currently offers the most vi-able, acceptable option for repeal of ObamaCare. At a mere 40 words, it is magnifi-cently simple and straight-forward. It states:
Effective as of the enact-ment of the Patient Pro-tection and Affordable Care Act, such Act is repealed, and the provisions of law amended or repealed by such Act are restored or revived as if such Act had not been enacted.
As of the first week of July, H.R. 4972 had 100 cosponsors. As was to be expected, the Democratic leadership of the House is try-ing to keep the bill bottled up in commit-tee so that they will not have to vote on it and face the consequences from voters in the fall. To circumvent this obstacle, Rep. King has launched a discharge petition ef-fort. By July 14 he had garnered signatures from 130 House members. He needs a total of 218 signatures to force H.R. 4972 out to the House floor for a vote. You can check on the Internet here (http://clerk.house.gov/111/lrc/pd/petitions/Dis11.htm) to see if your Representative has signed the
discharge petition. Write, call, fax, and/or e-mail your Representative, asking him to sign the petition (or extending thanks if he has already done so) as well as urging him to sign on as a cosponsor to H.R. 4972.
Although we offered caveats above con-cerning Republican “repeal and replace” bills, there is at least one bill in that cat-egory that constitutionalists should have no problem supporting: Rep. Ron Paul’s H.R. 5444, “The Private Option Health Care Reform Act.”
In addition to repealing ObamaCare, H.R. 5444 injects a number of genuine, much-needed free-market-oriented re-forms into the equation. Some of the fea-tures of this seven-page bill are:
• Refundable Credit for Health Care Costs
• Strengthening Health Savings Accounts
The primary defect of the state challenge in the federal courts is that it begins with the false premise that a branch of the federal government — the courts — should have the final say on disputes involving federal usurpation of states’ rights.
ObamaCare represents one of the biggest government takeovers in American history, transferring healthcare from a doctor-patient relationship to a patient-government bureaucracy system.
iStock images
21Call 1-800-727-TRUE to subscribe today!

• Repeal of the 7.5 Percent Threshold on Deduction for Medical Expenses
• Purchase of Health Insurance Across State Lines
• Facilitation of Importation of Drugs Approved by the FDA
In addition to being a respected physi-cian, Dr. Ron Paul is widely recognized as the leading constitutionalist in Congress. As such, he understands that more gov-ernment is not the proper prescription for what ails our healthcare system; indeed, it is government taxes, intervention, and regulation that are at the root of our ex-ploding healthcare costs.
State Nullification: One of the most important and encouraging developments in recent times is the reassertion by the states of their sovereign powers against federal usurpation. The Framers of our Constitution well understood the tenden-cies of government toward encroachment and did not intend that the states should be helpless before an inexorable, centralizing national government. The states have the right (and duty) to resist unconstitutional arrogations by Washington of powers con-stitutionally reserved to the states. A prin-cipal form of resistance in this regard is for the state government simply to declare the offending federal law, regulation, or edict null and void and to refuse to enforce or implement it.
This is what happened with regard to the REAL ID Act that was passed by a Re-publican Congress and signed into law in 2005 by then-President George W. Bush. More than two dozen states passed laws or resolutions denouncing the act or refusing to comply with it. As a result, the federal government has been forced to retreat on this unconstitutional grab for power.
Similarly, nearly 25 states have intro-duced some version of the Firearms Free-dom Act (FFA) to nullify federal firearms laws within their state for guns manufac-tured, sold, and used in that state. Seven states have already enacted FFAs: Mon-tana, Tennessee, Utah, Wyoming, South Dakota, Arizona, and Idaho.
Constitutionalists are now using the same strategy to block ObamaCare through state nullification. A “Model Resolution for a State Legislature to Nul-lify the Federal Health Care Bills of 2010” is circulating in the states and can be ac-cessed from the website of The John Birch
Society (www.jbs.org, then type “Model Resolution” in the search box).
State Lawsuits: The Attorneys Gen-eral of 18 states have joined together in a lawsuit which charges that provisions of ObamaCare violate the U.S. Constitution and rights of states by forcing massive new spending on hard-pressed state govern-ments. The lawsuit has served to awaken in many Americans (and many state politi-cians) the realization that the federal gov-ernment does not have carte blanche to enact whatever may be the current whim of the powers-that-be in Washington. However, the judicial process is painfully long, slow, and costly. By the time a deci-sion is rendered — even if it should go in favor of the states — ObamaCare would likely be a firmly established fact. The primary defect of the state challenge in the federal courts is that it begins with the false premise that a branch of the federal government — the courts — should have the final say on disputes involving federal usurpation of states’ rights.
Take ActionAs far as citizen activism goes, there is little that one can do to affect the outcome of the judicial process; lawyers and judges will determine the outcome of the lawsuit. However, regarding congressional repeal
and state nullification efforts, individual citizens can have a tremendous impact. As town-hall meetings, Tea Parties, and opin-ion polls have strongly demonstrated, most Americans are opposed to ObamaCare, and most members of Congress are well aware that they burned up a tremendous amount of political capital to steamroll the legislation through. Many of them are now vulnerable. The repeal and nullifica-tion efforts, besides being aimed directly at undoing ObamaCare, also serve to exact a continuing political price by reminding voters that politicians are responsible for this enormous, costly, unconstitutional, unpopular power grab.
Here’s what you can do:• Urge your Representative to support
Rep. King’s H.R. 4972 to repeal Obama-Care and to support his discharge petition
• Urge your Representative to support Rep. Paul’s H.R. 5444, “The Private Op-tion Health Care Reform Act.”
•Urge your state legislators to introduce, and your Governor to support, state legis-lation (see model legislation mentioned above) to nullify ObamaCare.
• Ask all candidates for the House and Senate, as well as for your state legislative and gubernatorial races, to commit them-selves to a public stand in favor of repeal-ing or nullifying ObamaCare. #
House Speaker Nancy Pelosi (D-Calif.) walks through the Cannon Rotunda after a Democratic Caucus, along with (from left) Reps. Steny Hoyer (D-Md.), John Lewis (D-Ga.), and John Larson (D-Conn.), on March 21, 2010.
AP
Imag
es
THE NEW AMERICAN22
HEALTHCARE

From infancy on, most Americans hear a steady litany of “com-
promise, compromise, com-promise.” Whether parents are breaking up a toddler fight in a sandbox over a big, yellow Tonka truck or a teen scrape between siblings over which child will get to use the home computer, kids hear, “Work it out. Compromise!”
On a certain level that makes sense because compro-mise is better than selfishness, an attitude that leads children to bicker. Compromise usually leads to good ends: Toddler tantrums dissipate (along with the amount of sand that you have to dig out of the wee ones’ eyes, tossed there by retaliatory tots) and household harmony can be quickly reestablished when siblings scream, “Mine!”
But compromise is not all that it’s cracked up to be. For an extreme example, say you’re on the verge of being tortured by our government. For your part, you don’t want to be tortured at all, while the government wants to torture you to the very brink of death. You would not be exhibiting magnanimous behavior, or even good sense, by saying, “I know, let’s compromise. Torture me half to death, and we’ll call it good!”
Just as that would be crazily foolish, there is another type of compromise that can be equally ludicrous, though for some rea-son it is often lauded in the press as a panacea for our country’s political problems: bipartisanship.
Let’s use a real example. When one political party, in this case chiefly Democrats, says in so many words, “We need to water down the First Amendment’s protections on freedom of speech and of the press,” as happened in 2002, if any member of the Republican Party were to compromise one little bit on the First Amendment, that member would also be contributing to the erasure of our freedoms, regardless of his intent. Why? Because once an untouchable right becomes touchable, it soon withers to inconsequence under a sustained assault — unless a major effort is put forth to resurrect the right’s unassailability.
The official title of the 2002 anti-free-speech law is the Biparti-san Campaign Reform Act of 2002. It is commonly known as the McCain-Feingold law. This law allows, among other things, some big corporations, such as newspapers, radio stations, and televi-sion networks, to air their views about candidates any time, while forbidding other corporations, such as the NRA and the Sierra Club, from expressing their views within 60 days of an election.
This censorship came despite the very clear words of the First Amendment: “Congress shall make no law … abridging the freedom of speech or of the press.”
The McCain-Feingold leg-islation is itself the result of a steady progression of creep-ing limits on free speech and press that penalize the Amer-ican people. The Espionage Act of 1917 made it a crime to speak out against the draft in WWI. After its passage, Charles Schenk was arrested for distributing pamphlets opposed to the draft, and he took his free-speech case all the way to the Supreme Court in Charles T. Schenk v. United States, where the U.S. Supreme Court prompt-
ly upheld this clearly unconstitutional law.Of course, the justices “justified” their decision — reasons
are always given for taking away rights. Justice Oliver Wendell Holmes, Jr. wrote: “The question in every case is whether the words used are used in such a circumstance and are of such a nature as to create a clear and present danger that they will bring about the substantive evils that Congress has a right to prevent.”
Holmes likened Schenk’s distribution of pamphlets to shout-ing fire in a crowded theatre and proclaimed that such an action would not fall under the First Amendment. Then free speech was fair game.
Even though the justices tried to formulate phraseology to intelligently categorize speech as legal or not, and despite the unanimous vote in the case, Schenk was overturned in Branden-burg v. Ohio, whereupon a new limit was set on free speech: Speech could now only be banned when it was likely to incite “imminent lawless action.”
Before long, language no longer had to be dangerous to be banned and McCain-Feingold came into existence, as did numer-ous other speech restrictions. Even “free speech” is effectively curtailed because the laws are so convoluted that people who can’t afford to hire a law firm can’t decipher the laws. New reasons to eliminate free speech replaced old reasons. But the reasons were always irrelevant because no limits on free speech were ever really needed. Under U.S. law, one is responsible for one’s ac-tions, and legitimately dangerous actions can be curtailed. For instance, though Congress may not restrict speech, it may outlaw the transference of government secrets. Similarly state and local governments may hold someone responsible for negligently caus-ing bodily harm — such as that caused by a riot in a theatre — and use one’s words in court as evidence of an intent to cause harm.
The lesson is obvious: “Never compromise on freedom!” This is especially relevant as Republicans call to “repeal and replace” ObamaCare. Care must be exercised to make sure the replace-ment isn’t as antithetical to individual rights as is ObamaCare. #
No Compromise on Compromise
www.TheNewAmerican.com
THE LAST WORDTHE LAST WORDBY KURT WILLIAMSEN
23