Embed Size (px)
Citation preview

Project 3 of the Hopkins Center to Eliminate Cardiovascular Health Dispari-ties is now called The 5 Plus Trial.
What does that mean? Five Plus is the catchy study name meaning: Five fruits and vegetables plus nuts and beans. This is a practical application study incor-porating information gathered from other studies done at Johns Hopkins such as The Weight Loss Maintenance Trial. The dietary intervention approach will be based on the DASH Diet.
DASH stands for Dietary Approaches to Stop Hypertension, a multicenter study in which participants were given food and observed during all meals. The study showed that a diet reduced in sodium and rich in other minerals lowered blood pressure to a greater degree than a con-trol diet higher in sodium.
We will be recruiting African-Americans who have blood pressures in the high normal range and those with a diagnosis of hypertension whose blood pressure is controlled by medicines. It is possible that just lowering sodium intake will reduce their blood pressure further even if it is already in the normal range. However, most people are not aware that micronutrients have independent blood pressure lowering effects as well. Micronutrients are substances, such as vitamins or trace elements, essential for healthy development but required only in small amounts. Examples include potas-sium, magnesium and vitamin C. We know that inadequate intake and/or faster loss of these nutrients not only af-fects blood pressure control but has been directly linked to the development of glu-
cose intolerance (poor handling of glucose or sugar by the body) or high levels of uric acid (as seen in conditions like gout).
The control group will receive a 10 minute review of the DASH diet, brief counseling, an info sheet, and (at the end of the study) a gift certificate for $150. Other study par-ticipants will receive dietary counseling for eight weeks on the basic principles of the DASH Diet with a lifestyle interventionist (a person trained to help people change their diet, exercise, and other health be-haviors). Each week, they will also be al-lowed to purchase $30 worth of groceries that are included in that diet, such as fruits, vegetables, beans and nuts that are rich in potassium magnesium, and vitamin C. These foods will be tailored to the indi-vidual’s choices and delivered from a neighborhood grocery market (Santoni’s) that is a partner with the Baltimore City Health Department’s Virtual Supermarket Program called “Baltimarket”. This city program gives low income families access to fresh fruits and vegetables as well as other healthy choice foods. We would like to know if getting help in ordering the gro-ceries and the information about the DASH diet from the interventionist results in better blood pressure control than sim-ply getting the information in a brochure.
Look out for our posters and bro-chures at the selected JHCP site (either East Baltimore Medical Center or Wyman Park) soon!
Project 3, or as We Now Call it, “5 Plus”
Th
e C
en
ter
’s B
ea
t
HO
PK
IN
S
CE
NT
ER
T
O
EL
IM
IN
AT
E
C
AR
DI
OV
AS
CU
LA
R
HE
AL
TH
D
IS
PA
RI
TI
ES
V o l u m e 1 , I s s u e 3
W i n t e r 2 0 1 1 - 1 2
Inside this Issue:Inside this Issue:Inside this Issue:
Community Advisory Board 2
New Team Members 4 Pre-doctoral Fellowship 3
Undergraduate Intern Report 3
By Edgar “Pete” Miller, MD, PhD

Let's talk about “health disparities”. For the past twelve years or so, these have been two of the biggest buzz words of-ten in reference to persons who do not have health insurance or access to healthcare. These persons are either uninsured or under insured. This population of people primarily consists of inner cities minorities who are either unemployed or under em-ployed, persons recently released from prison, homeless per-sons and more recently, the middle class that are unemployed. The only recourse for these people is to go to the hospital emer-gency room and even then, for many, it was too late. It is no surprise that this population of people are the across the board leaders in almost every type of illness, directly correlating to the high rates of disabilities and death.
Thousands of health professionals have traveled all over the country making speeches, holding conferences and even starting new departments in the name of “health disparity”, however few have done anything to address the real problem.
In 1997, I became the Director of the Men's Center, as it was know then. After attending a presentation on health disparities, I held several community focus groups where health care was the major issue. I set out to start a free, holistic health clinic spe-cifically targeted to the needs of the above population. The goal was to not only bring awareness to the problem, but to actually get these people access to healthcare and treatment.
Since the implementation of the health clinic, the lives of hundreds have been improved through pre-screening and early detection. The health clinic has helped prevent strokes, heart attacks and possible death. It has provided treatment for high
cholesterol and hypertension, which are the early warning signs leading to these conditions, as well as diabetes.
I continue to approach clients’ prob-lems holistically through life skills training, pre-employment and case management. These things coupled with health care can affect life altering change. The clinic at the Center at 2222 E. Jefferson St. Baltimore Maryland 21205, is often referred to as the “East Baltimore M*A*S*H unit”. In collaboration with the Charm City Clinic, a group consisting of Johns Hopkins students, we have found a niche. Assessments are provided via the volunteer doctors and nurses. In addition to providing health care services, these indi-viduals help the clients obtain health insurance, which for some is a first time event. There is the study being conducted through the Johns Hopkins Center to Eliminate Cardiovascular Health Disparities where education and treatment are the focus to affect change and reduce health disparities amongst those less fortunate. There are also research projects that are looking to find out what more needs to be done. My motto is that eve-rybody deserves basic healthcare especially in this country where we have so much.
Leon Purnell is the long-term Executive Director of The Men's Center, an organization dedicated to assisting African descendant men and their families in East Baltimore, one of the poorest and most neglected communities in Baltimore City.
Page 2
Community Perspective Leon Purnell
T H E C E N T E R ’ S B E A T
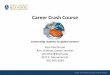
LEGEND:
2012
Jan. Feb. Mar. Apr. May June July Aug. Sep. Oct. Nov. Dec.
EBMC CC/GD
Dietician/PharmD Care Management
Initiative
2012
Jan. Feb. Mar. Apr. May June July Aug. Sep. Oct. Nov. Dec.
EBMC
Patient, Family & Community
Outreach Trial
2012
Jan. Feb. Mar. Apr. May June July Aug. Sep. Oct. Nov. Dec.
EBMC
Five Plus Trial
=
=
Development
CLINICAL SITES:
CC = Canton Crossing
EBMC = East Baltimore
GD = Greater Dundalk
GSS = Green Spring Station
WM = White Marsh
WP = Wyman Park
Implementation
Pilot Study =
*For more information on our research studies visit www.jhsph.edu/cardiodisparities/research
2012
Jan. Feb. Mar. Apr. May June July Aug. Sep. Oct. Nov. Dec.
Six JHCP Sites
Provider Education Initiative
BP Measurement Initiative
Center Research Implementation Timeline*
2012
Jan. Feb. Mar. Apr. May June July Aug. Sep. Oct. Nov. Dec.
WP

V OLU ME 1, ISS UE 3
Greetings. My name is Niajee Washington and I am a junior this fall at Cornell University. This summer I had the privilege of interning at the Center to Eliminate Cardiovascular Health Disparities. During the internship, I visited a plethora of organizations that work to improve the health of underserved Baltimore populations. One of my favorite visits was at the Men and Family Center. The Center, just a few blocks from the Hopkins Medical campus, works to provide health, parenting, employment, and mentorship services to low-income Baltimoreans. On my first visit there, the director told the story of James, one of the young boys in their mentorship program.
While visiting James’ school, an administrator from the mentorship program saw him in the hallway. After speaking with him, he discovered that James was dismissed from class for “laughing too much.” The administrator then spoke with the teacher, asking him why James was in the hallway. The teacher gave the same response. The administrator then explained to the teacher that James’ family life was unstable, thus leaving the young child to care for himself and his siblings without much help. He described how James would feed his siblings breakfast, then after taking them to school, would take himself to school. The ad-ministrator concluded the discussion by explaining that James’ only chance to truly be a child was in the classroom, which likely explained his behavior. The teacher thanked the administrator, explained that he was completely unaware of James’ circum-stances, and dealt with him differently from that day forward. This story helps show that things may not always be as they are per-ceived, and often there are many “invisible” factors that greatly contribute to certain circumstances.
James’ story reflects what we find when looking at health disparities – that it is often the “invisible factors”, the social and eco-nomic conditions that people face, which contribute to poor health outcomes and grave health disparities. I have learned how these social determinants, such as education, access to healthy foods, income, and physical environment, greatly affect people’s health and healthcare. Thus it is critical to approach this epidemic from a multi-dimensional perspective and understand that we can only eliminate these avoidable health inequalities by helping the entire person – not just their diseases.
From sitting in on Baltimore City Health Department meetings, to discussing healthy lifestyle choices with men in a drug recov-ery home, to constructing a research proposal, to learning from brilliant and passionate people who truly believe in eliminating health inequalities, my internship this summer with the Center to Eliminate Cardiovascular Health Disparities has given me a phe-nomenal learning experience that I will never forget and has ultimately led to one of the best summers of my life.
High blood pressure (HBP) is a growing problem among Vietnamese Americans due to rapidly changing life-styles and diets. Compounding that concern, many Viet-namese Americans, like other recent immigrants groups, suffer from insufficient health literacy. This problem se-verely limits their ability to obtain, process and understand information related to their disease. Therefore, the main goal of Ms. Nguyen’s dissertation work is to develop a high blood pressure specific health literacy assessment tool.
Once developed, Ms. Nguyen hopes to use the tool for two purposes. First, it will be used to assess health literacy among Vietnamese Americans with high blood pressure. Second, it will be used to guide interventions that can im-prove health literacy in the context of high blood pressure. Ultimately, Ms. Nguyen hopes that as health literacy im-proves, Vietnamese Americans will become more empow-ered to transform their health experiences and outcomes.
To that end, Ms. Nguyen and her research team have
successfully developed the High Blood Pressure-Health Liter-
acy Scale (HBP-HLS).1 The tool was initially tested on a sam-
ple of Korean Americans with high blood
pressure. Results indicate that the
newly constructed HBP-HLS is valid and
reliable. Ms. Nguyen is currently finish-
ing data collection to cross-validate the
tool on a sample of Vietnamese Ameri-
cans.
Preliminary analyses suggest that
the HBP-HLS is also valid and reliable in the Vietnamese
population. These findings lend early support for the utility
of this tool in diverse populations.
1 Kim MT, Song HJ, Han HR, Song Y, Nam S, Nguyen TH, Lee HB, Kim BK. Development and validation of the high blood pressure-focused health literacy scale. Patient Educ Couns 2011
Pre-Doctoral Trainee Tam Nguyen is a PhD Candidate in the School of Nursing. Dr. Miyong Kim is her primary mentor.
Page 3
Undergraduate Internship Niajee Washington
Training & Career Development Core
High Blood Pressure among Vietnamese Americans Tam Nguyen, RN

The Hopkins Center to Eliminate Cardiovascular Health Disparities is
one of 10 NIH-funded Centers for Population Health and Health Dispari-
ties. The Hopkins Center’s mission is to improve health and eliminate
cardiovascular health disparities among Baltimoreans through innova-
tions in research and training, clinical practice, and patient/community
education. The Center includes 23 faculty from the Schools of Medicine,
Nursing, and Public Health, who are working in collaboration with Johns
Hopkins Community Physicians and focusing initially on improving con-
trol of hypertension in African Americans, who are disproportionately
affected. A 30-member advisory board composed of community mem-
bers representing patients, faith-based and community-based organiza-
tions, neighborhood associations, historically black colleges, practicing
clinicians, and local public health agencies, helps guide the Center to
achieve its research, training and dissemination objectives.
Johns Hopkins School of Medicine
2024 E. Monument Street, Suite 500
Baltimore, Maryland
Baltimore, Maryland 21287
HOPKINS CENTER TO EL IMINATE
CARDIOVASCULAR HEAL TH DISPARIT IES
Center Core Faculty & Staff:
Lisa A Cooper, MD, MPH — Center Director; PI, Project 1
Jill Marsteller , PhD — Co-PI, Project 1
L. Ebony Boulware, MD, MPH — PI, Project 2
Edgar “Pete” Miller, MD, PhD — PI, Project3
Sherita Hill Golden, MD, MHA — Training Director
Phone: 410-614-2412
Fax: 410-614-0588
Creating healthy hearts for all Baltimore residents.
We are on the web!
www.jhsph.edu/cardiodisparities
Welcome Debra Gayles & Sarah Flynn
The Center to Eliminate Cardiovascular Health Disparities is excited to announce two new staff members to our research
Ms. Gayles has accepted the position of Research Project Manager for the Dietary and Supplement Intervention (Plus 5).
Ms. Gayles started her career at Johns Hopkins ProHealth in 2003. She was a lifestyle Interventionist with Dr. Larry Appel's Weight Loss Maintenance Study. The other studies she has worked on include First WIND, a weight loss for post-partum moms with Dr. Wanda Nicholson, The ACHIEVE Pilot and Trial, a weight loss study for people with serious mental illness with Dr. Gail Daumit.
Her new position is Interventionist/Coordinator of the Five Plus Study, encouraging hypertensive African Americans
to eat fruits, vegetable, beans and nuts.
Sarah Flynn will be working as a Re-search Assistant on both the System Level Quality Improvement Intervention (Project 1) and the Patient, Family, and Community Intervention (Project 2).
Sarah has a Bachelor of Arts from Stan-ford University, graduating in June with a major in Human Biology and a minor in Com-parative Studies in Race and Ethnicity. Her coursework and research at Stanford focused on the health of the disadvantaged.
We ask that you join us in welcoming both Debra and Sarah to our research team.
Debra Gayles Sarah Flynn
Richard W. Matens, MDiv — Administrative Director
Kit Carson, ScM — Shared Resources Director
Joy Mays — Research Coordinator
Gary Noronha, MD — Director of Research, JHCP