Embed Size (px)
Citation preview

THE AMAZING KIDNEYS
WESTERN CLINICAL MEDICINE
SP 2012
Systems IV

THE URINARY SYSTEM

WHAT DO THE KIDNEYS DO?
• Extracts metabolic wastes from the blood stream and eliminates it from the body
• Adjusts blood pH by excretion of more or less acid
• Adjusts blood salt concentration by excretion of more or less salt
• Adjusts blood volume and blood pressure by secretion of renin (a hormone)
• Stimulates red blood cell production by excretion of erythropoietin (another hormone)

HOW DO THE KIDNEYS MANAGE TO DO ALL THESE THINGS?
• Due to the amazingly complex anatomy and physiology of the renal system!
• Now, a story…once upon a time there was a large salt water lake…

FIRST WE’LL MEET THE

BLOOD FLOWS RED THROUGH THE GLOMERULUS
• So blood comes along with its toxins, glucose, amino acids, water, electrolytes, etc…enters the kidney via the renal artery
• It then enters afferent arterioles which take the blood into the glomerulus.
• The afferent arteriole contains the juxtaglomerular apparatus (causes renin to be excreted depending on the blood pressure)
• The glomerulus is the FILTER of the system. All water and small particles flow right through, but larger particles like sugar and protein can’t.
• So what makes it through the filter is filtered OUT of the bloodstream and moves into Bowman’s capsule and onto the tubular system…
• What doesn’t get filtered out continues on out the efferent arteriole, which is smaller than the afferent vessel in order to maintain a high pressure system for filtration.



THE TUBULAR SYSTEM
• So the glomerular filtrate moves through the tubules where water and salts/electrolytes are exchanged between the tubular fluid and the blood vessels that run along the tubules.
• What is left over after all the exchanging is done is what is excreted = urine


THE TUBULES
• Most of the water is reabsorbed into the blood. ADH (anti-diuretic hormone) is secreted by the pituitary and controls how much or how little water is reabsorbed based on the osmolarity of the blood.
• Aldosterone (secreted by the adrenals) stimulates potassium to move from blood vessels into the tubule in exchange for sodium.
• The tubule reabsorbs all glucose and amino acids, but if there are too many glucose or AA particles, it can’t reabsorb them all spill into the urine.


URINE
• What is left over after all this occurs.• Contains urea, creatinine (products of protein
metabolism), toxins, and drug metabolites.• Normal urine is acidic because energy
metabolism creates acid which is eliminated in urine and in the breath (CO2)
• Urine also has sodium, potassium, electrolytes that vary depending on diet, exercise, hydration, and metabolism.
• Urine concentration varies according to the body’s need to conserve or excrete water to maintain normal blood osmolarity.

URINE
• Average urine output is 1-1.5 L/day.• The kidney forms 180 L/day of filtrate.• 99% of what the glomerulus filters is
reabsorbed by the tubules. (only 1% ends up as urine)
• It takes 30 min for all the body’s blood volume to be filtered.
• All the blood is cleaned about 50 times each day!

LABORATORY
• BUN = blood urea nitrogen• If the kidneys aren’t working well, there will be more
waste products higher BUN and creatinine in the blood.
• Urinalysis: dipstick, microscopy, culture– Nitrite and leukocyte esterase– Bilirubin– Color/Specific gravity– Protein– Glucose– Red blood cells– Ketones– pH

Urinary System- Recap:
• Kidneys: produce urine• Excretory duct system
– Ureter: conveys urine into bladder by peristalsis– Renal pelvis: expanded upper portion of ureter– Major calyces: subdivisions of renal pelvis– Minor calyces: subdivisions of major calyces into which
renal papillae discharge
• Bladder: stores urine– Discharges urine into urethra during voiding– Anatomic configuration of bladder and ureters normally
prevents reflux of urine into ureters
• Urethra: conveys urine from the bladder for excretion

Kidneys (1 of 2)
• Paired, bean-shaped organs below diaphragm adjacent to vertebral column
• Divided into outer cortex and inner medulla (renal pyramids and columns)
• Excretory organs, functions along with lungs in excreting waste products of food metabolism
• Three basic functions– Excrete waste products of food metabolism
• CO2 and H2O: end-products of carbohydrate and fat metabolism
• Urea and other acids: end-products of protein metabolism that only the kidneys can excrete

Kidneys (2 of 2)
– Regulate mineral and H2O balance
• Excretes excess minerals and H20 ingested and conserves them as required
• Body’s internal environment is determined not by what a person ingests but by what the kidneys retain
– Produces erythropoietin and renin: specialized cells in the kidneys
• Erythropoietin: regulates RBC production in marrow• Renin: helps regulate blood pressure

Nephron (1 of 2)
• Basic structural and functional unit of the kidney• About 1 million nephrons in each kidney• Consists of glomerulus and renal tubule• Glomerulus
– Tuft of capillaries supplied by an afferent glomerular arteriole that recombine into an efferent glomerular
– Material is filtered by a 3-layered glomerular filter• Inner: fenestrated capillary endothelium• Middle: basement membrane• Outer: capillary endothelial cells (with foot processes and filtration
slits)
– Mesangial cells: contractile phagocytic cells that hold the capillary tuft together; regulate caliber of capillaries affecting filtration rate

Nephron (2 of 2)
• Renal tubule: reabsorbs most of filtrate; secretes unwanted components into tubular fluid; regulates H2O balance– Proximal end: Bowman’s capsule– Distal end: empties into collecting tubules
• Requirements for normal renal function– Free flow of blood through the glomerular
capillaries– Normally functioning glomerular filter that
restricts passage of blood cells and protein– Normal outflow of urine

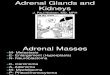
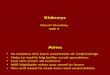
The structure of the renal tubule, illustrating its relationship to the glomerulus and the collecting tubule.

Bowman’s Capsule
© Courtesy of Leonard Crowley, M.D./University of Minnesota Medical School

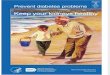
Renal Regulation of Blood Pressure• Renin: released in response to decreased blood
volume, low blood pressure, low sodium• Angiotensin I → angiotensin II by angiotensin
converting enzyme (ACE) as blood flows through the lungs
• Angiotensin II:– Powerful vasoconstrictor: raises blood pressure by
causing peripheral arterioles to constrict– Stimulates aldosterone secretion from adrenal cortex:
increases reabsorption of NaCl and H2O by kidneys
– Net effect: higher blood pressure, increased fluid in vascular system
• System is self-regulating

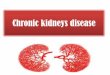
The role of the kidneys in regulation of blood pressure and blood volume.

RENAL VOCABULARY
• Anuria: little or no urine output• Bacteriuria: bacteria in the urine• Diuresis: increased urine output• Dysuria: painful urination• Glycosuria: glucose in the urine• Hematuria: red blood cells in the urine• Nocturia: urination at nighttime• Oliguria: less than normal urine output• Polyuria: more than normal urine output• Proteinuria: protein in the urine

KIDNEY DISEASE
• High blood pressure and diabetes are both common causes of kidney disease.
• Kidneys collect, concentrate, and excrete toxins which can damage them over time.
• The renal tubules are very metabolically active and are therefore vulnerable to toxic damage and oxygen deprivation.

KIDNEY DISEASE
• Disease of one renal structure usually affects others.
• When there is a clinical abnormality, there are frequently several levels of the system that could have gone awry.
• Professional Guide to Diseases next slide

28
CHAPTER 7 PGD
• Congenital Anomalies
– medullary sponge disease and polycystic kidney disorder
• Acute Renal Disorders
– renal failure, pyelonephritis, poststreptococcal glomerulonephritis, tubular necrosis, renal infarction, renal calculi, renal vein thrombosis
• Chronic Renal Disorders
– nephrotic syndrome, chronic glomerulonephritis, renovascular hypertension, hydronephrosis, renal tubular acidosis, chronic renal failure
• Lower Urinary Tract Disorders
– lower UTI, vesicoureteral reflux, neurogenic bladder, congenital anomalies of ureter-bladder-urethra
• Prostate and Epididymis Disorders
– prostatitis, epididymitis, BPH28

29
Congenital Anomalies Ch 7
• Medullary sponge disease -– Medullary sponge kidney is a benign congenital
disorder characterized by dilatation of collecting tubules in 1 or more renal papillae, affecting 1 or both kidneys. Medullary sponge kidney is usually a benign condition, and patients can remain asymptomatic
– The name medullary sponge kidney is misleading because the affected kidney does not resemble a sponge. The names tubular ectasia and cystic dilatation of the collecting ducts have been suggested as alternatives; however, medullary sponge kidney is the most commonly used name for this disorder.
29

30
Congenital, continued
• Polycystic Kidney Disease– Autosomal dominant polycystic kidney disease
(ADPKD) is one of the most common inherited disorders in humans. It is the most frequent genetic cause of renal failure in adults, accounting for 6-8% of patients on dialysis in the United States.
– ADPKD is a multisystemic and progressive disorder characterized by the formation and enlargement of cysts in the kidney (as seen in the image below) and other organs (eg, liver, pancreas, spleen). Clinical features usually begin in the third to fourth decade of life, but cysts may be detectable in childhood and in utero 3
0

31
Polycystic Kidney• Pain—in the abdomen, flank, or back—is the most
common initial complaint, and it is almost universally present in patients with ADPKD (see Clinical). Ultrasonography is the diagnostic procedure of choice (see Workup). Medical therapy is needed to control problems such as hypertension, urinary tract infections, hematuria, and pain. Surgical drainage of cysts may be indicated. Patients who progress to end-stage renal disease (ESRD) may require dialysis or renal transplantation.
31

Other Congenital Abnormalities• Renal agenesis: failure of one or both kidneys to
develop– Bilateral: rare, associated with other congenital
anomalies, incompatible with life– Unilateral: common, asymptomatic; other kidney
enlarges to compensate• Duplications of urinary tract
– Complete duplication: formation of extra ureter and renal pelvis
– Incomplete duplication: only upper part of excretory system is duplicated
• Malposition: one or both kidneys, associated with fusion of kidneys; horseshoe kidney; fusion of upper pole

33
Acute Renal Disorders–acute renal failure–acute pyelonephritis–acute poststreptococcal
glomerulonephritis–acute tubular necrosis–acute renal infarction- not covering–acute renal calculi–acute renal vein thrombosis-not
covering

AZOTEMIA
• Renal failure manifest only by abnormal laboratory tests. No clinical signs of kidney failure are present. Usually elevated BUN and creatinine.

ACUTE RENAL FAILURE
• Acute oliguria or anuria plus azotemia• Most common cause is damage to the renal tubules
(acute tubular necrosis) that occurs during shock (with acute reduction in blood flow to the kidneys due to hemorrhage, infection).
• Other causes include tubular damage from medications or toxins (heavy metals, X-ray contrast), hemolysis or rhabdomyolysis (acute release of intracellular proteins that the kidneys have to filter but can’t). Also acute glomerular or vascular disease
• Usually the tubules can recover if the offending agent is identified and removed.

UREMIA
• Renal failure with clinical signs and symptoms.– Hypertension (retention of salt and water)– Anemia (low erythropoietin)– Edema (retention of salt and water)– Oliguria (low glomerular filtration rate)– Accumulation of toxic metabolic waste
products pericarditis, gastroenteritis, coagulation defects, neuropathy, encephalopathy

Renal Failure (Uremia) (1 of 2)
• Retention of excessive byproducts of protein metabolism in the blood
• Acute renal failure– Causes: tubular necrosis from impaired blood flow to
kidneys or effects of toxic drugs– Renal function usually returns
• Chronic renal failure– From progressive, chronic kidney disease; > 50% from
chronic glomerulonephritis– Others include congenital polycystic kidney disease,
nephrosclerosis, diabetic nephropathy

Renal Failure (Uremia) (2 of 2)
• Clinical manifestations – Weakness, loss of appetite, nausea, vomiting– Anemia– Toxic manifestations from retained waste
products– Edema: retention of salt and water– Hypertension
• Treatment– Hemodialysis– Hypertension

URINARY TRACT INFECTION
• Bacteria and white blood cells in the urine• Infection can be anywhere in the urinary tract
from the kidneys to the urethra.• Can be without symptoms or with dysuria and
fever.• Acute bladder inflammation (cystitis) is the most
common. Risks: sex, catheterization, surgery, back-to-front wiping, urinary reflux, stones
• Pyelonephritis-usually due to ascended cystitis. Flank pain, fever, dysuria, frequency, urgency. Can lead to sepsis and renal failure.

Pyelonephritis
• Involvement of upper urinary tract from– Ascending infection from the bladder (ascending
pyelonephritis)– Carried to the kidneys from the bloodstream
(hematogenous pyelonephritis)
• Clinical manifestations: similar with an acute infection– Localized pain and tenderness over affected kidney– Responds well to antibiotics– Cystitis and pyelonephritis are frequently associated– Some cases become chronic and lead to kidney failure

Glomerulonephritis• Inflammation of the glomeruli caused by antigen-
antibody reaction within the glomeruli• Immune-complex glomerulonephritis
– Usually follows a beta-streptococcal infection (APSGN)– Circulating antigen and antibody complexes are filtered
by glomeruli and incite inflammation– Leukocytes release lysosomal enzymes that cause injury
to the glomeruli– Occurs in SLE; immune complexes trapped in glomeruli– Occurs in IgA nephropathy
• Anti-glomerular basement membrane (anti-GBM) glomerulonephritis: autoantibodies attack glomerular basement membrane

42
Post-Strep Glomerulonephritis
• Acute glomerulonephritis is characterized by the sudden appearance of hematuria, proteinuria, red blood cell casts in the urine, edema, and hypertension with or without oliguria. It can follow streptococcal infections. This illness was first recognized as a complication of the convalescence period of scarlet fever in the 18th century. A link between hemolytic streptococci and acute glomerulonephritis was recognized in the 20th century. (see next two slides for definitions of hematuria and proteinuria, occult)

OCCULT HEMATURIA
• Microscopic hematuria (can’t see the blood but there are red blood cells)
• May be caused by mild or early glomerular disease, or disease elsewhere in the urinary tract.
• A lot of times the cause is unknown

OCCULT PROTEINURIA
• Detectable only on urinalysis• Small amounts of protein may be present
with fever, with urinary tract infection, or following strenuous exercise.
• May be due to glomerular disease or renal damage from hypertension.

45
APSGN• Latent period
◦ A latent period always occurs between the streptococcal infection and the onset of signs and symptoms of acute glomerulonephritis.
◦ In general, the latent period is 1-2 weeks after a throat infection and 3-6 weeks after a skin infection.
◦ The onset of signs and symptoms at the same time as pharyngitis (also called synpharyngitic nephritis) is more likely to be immunoglobulin A (IgA) nephropathy rather than APSGN.
◦ Dark urine (brown-, tea-, or cola-colored)
◦ This is often the first clinical symptom.
◦ Dark urine is caused by hemolysis of red blood cells that have penetrated the glomerular basement membrane and have passed into the tubular system.
45

46
APSGN• Periorbital edema
◦ The onset of puffiness of the face or eyelids is sudden. It is usually prominent upon awakening and, if the patient is active, tends to subside at the end of the day.
◦ In some cases, generalized edema and other features of circulatory congestion, such as dyspnea, may be present.
◦ Edema is a result of a defect in renal excretion of salt and water.
◦ The severity of edema is often disproportionate to the degree of renal impairment.
• Nonspecific symptoms
◦ These can include general malaise, weakness, and anorexia and are present in 50% of patients.
◦ Approximately 15% of patients complain of nausea and vomiting.
46

ACUTE NEPHRITIC SYNDROME• Acute nephritic syndrome presenting as edema, hematuria, and hypertension
with or without oliguria is the most frequent presentation of APSGN. Approximately 95% of clinical cases have at least 2 manifestations, and 40% have the full-blown acute nephritic syndrome.
• Acute glomerular inflammation (glomerulonephritis)• Causes hematuria, hypertension, azotemia, oliguria, and
edema• Almost always caused by acute autoimmune disease.• The inflammation impairs blood flow through the
glomerulus, reducing the filtration rate oliguria and causes leaking of red blood cells through it hematuria
• Not much blood is getting through, so more renin is produced which causes high blood pressure.
• Can occur after strep throat when antibodies made to attack the strep also attack the glomerulus. Usually in kids and appear several weeks after the infection.

48
PE in APSGN
• Acute nephritic (last slide)• Edema• Hypertension• Oliguria• Hematuria• Left Ventricular Dysfunction
48

49
Treatment in APSGN
• Symptomatic therapy is recommended for patients with acute poststreptococcal glomerulonephritis (APSGN), and it should be based on the clinical severity of the illness. The major goal is to control edema and blood pressure.
• Always consider Abx therapy for strep infections 4
9

Renal Tubular Injury/Necrosis
• Pathogenesis– Impaired renal blood flow– Tubular necrosis caused by toxic drugs or
chemicals
• Clinical manifestation– Acute renal failure: oliguria, anuria– Tubular function gradually recovers– Treated by dialysis until function returns

51
ATN
• Acute tubular necrosis (ATN) is the most common cause of acute kidney injury (AKI) in the renal category. AKI is commonly defined as an abrupt decline in renal function, manifested by acute elevation in plasma blood urea nitrogen (BUN) and serum creatinine, occurring in hours to days to weeks, and usually reversible. 5
1

52
ATN-Treatment
• Identify and remove the toxin• Supportive care with fluids and
electrolytes
52

Urinary Obstruction• Blockage of urine outflow leads to progressive
dilatation of urinary tract proximal to obstruction, eventually causes compression atrophy of kidneys
• Manifestations– Hydroureter: dilatation of ureter– Hydronephrosis: dilatation of pelvis and calyces
• Causes– Bilateral: obstruction of bladder neck by enlarged
prostate or urethral stricture– Unilateral: ureteral stricture, calculus, tumor
• Complications: stone formation; infections• Diagnosis and treatment: pyelogram, CT scan

NEPHROLITHIASIS
• Stones in the kidneys• Grain of sand big enough to fill the renal pelvis• Men > women, 20’s-30’s• Hematuria, colicky pain• Can occur once or be recurrent• Calcium stones (75%): due to increased urinary calcium;
hyperparathyroidism• Infection stones/magnesium (15%): precipitate in
alkaline environment created by infection• Uric acid stones (5%): 25% of patients with gout form
them, but most people with these stones don’t have gout

Urinary Calculi (1 of 3)
• Stones may form anywhere in the urinary tract• Predisposing factors
– High concentration of salts in urine saturates urine causing salts to precipitate and form calculi
• Uric acid in gout
• Calcium salts in hyperparathyroidism
– Urinary tract infections reduce solubility of salts in urine; clusters of bacteria are sites where urinary salts may crystallize to form stone
– Urinary tract obstruction causes urine stagnation, promotes stasis and infection, further increasing stone formation

Urinary Calculi (2 of 3)
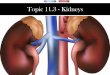
• Staghorn calculus: urinary stones that increase in size to form large branching structures that adopt to the contour of the pelvis and calyces
• Small stones may pass through ureters causing renal colic
• Some become impacted in the ureter and need to be removed
• Manifestations– Renal colic associated with passage of stone– Obstruction of urinary tract causes hydronephrosis-
hydroureter proximal to obstruction

Urinary Calculi (3 of 3)
• Treatment– Cystoscopy: snares and removes stones lodged
in distal ureter– Shock wave lithotripsy: stones lodged in
proximal ureter are broken into fragments that are readily excreted

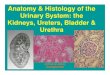
Large staghorn calculus of kidney

59
Next Section
• Chronic Renal Disorders–nephrotic syndrome, chronic
glomerulonephritis, renovascular hypertension, hydronephrosis, renal tubular acidosis, chronic renal failure
59

NEPHROTIC SYNDROME
• Caused by various glomerulus problems• Characterized by lots of protein in the
urine (leaky, damaged glomerulus), low protein in the blood (due to loss in urine), edema (due to loss of protein).
• Diabetic kidney disease is a common cause. Also autoimmune disease which can be caused by Hep B, malaria, drugs, or cancers

GLOMERULAR DISEASE
• Atherosclerotic plaques form in the renal arteries reduce blood flow to the kidney atrophy
• High glomerular pressure in hypertension damages/scars glomeruli. Renin-angiotensin-aldosterone mechanism is triggered by reduced blood flow, which increases blood pressure even more.
• Vasculitis associated with autoimmune diseases (e.g. lupus) can also damage the glomerulus

62
Chronic Glomerulonephritis
• Nearly all forms of acute glomerulonephritis have a tendency to progress to chronic glomerulonephritis. The condition is characterized by irreversible and progressive glomerular and tubulointerstitial fibrosis, ultimately leading to a reduction in the glomerular filtration rate (GFR) and retention of uremic toxins. If disease progression is not halted with therapy, the net results are chronic kidney disease (CKD), end-stage renal disease (ESRD), and cardiovascular disease. The diagnosis of CKD can be made without knowledge of the specific cause
62

63
Chronic Glomerulonephritis
• Dietary education is paramount in managing patients with CKD. The typical dietary restriction is 2 g of sodium, 2 g of potassium, and 40-60 g of protein a day. Additional restrictions may apply for diabetes, hyperlipidemia, and fluid overload.
• Treatment is essentially supportive with the goal to keep blood pressure down and electrolytes normal, as well as preventing heart failure.
63

64
Renovascular Hypertension• RVH is the rise in systemic blood pressure
resulting from stenosis of the major renal arteries or their branches or else from infrarenal atherosclerosis. The narrowing may be partial or complete and the resulting blood pressure elevation may be benign or malignant. (most common secondary hypertension)
• Stenosis or occlusion of the renal artery stimulates the affected kidney to release renin... recall the cascade. 6
4

65
Considerations• Onset of hypertension occurring in patients younger
than 30 years without risk factors
• Abrupt onset of severe (stage II) hypertension (greater than 160/100 in patients older than 55 years)
• Severe or resistant hypertension despite appropriately dosed multidrug (>3 agents) antihypertensive therapy
• Abrupt increase in blood pressure over previously stable baseline in patients with previously well-controlled essential hypertension as well as patients with known RAS
• Negative family history for hypertension
• Two major legs of treatment once underlying cause is identified is compliance on meds and smoking cessation6
5

66
Hydronephrosis
• Defined as an abnormal dialtion of the renal pelvis and the calyces of one or both kidneys, caused by an obstruction of urine flow from the genitourinary tract.
• Caused by obstructive neuropathy like BPH, strictures, calculi, and congenital problems
• Symptoms are those of UTI
66

URINARY TRACT OBSTRUCTION
• Acute and chronic• Prostate enlargement, tumors, scars,
stones• Urine stagnates, collecting system dilates
above the obstruction, bacterial infection can occur
• Can lead to renal failure

CHRONIC RENAL FAILURE
• Low urine output, prolonged symptoms and signs of renal failure
• End stage renal disease = burned out kidneys, shrunken, functionless
• Causes: diabetes, chronic glomerulonephritis (anemia and fatigue, occult proteinuria, hypertension, edema), hypertension account for about 75% of cases.
• Can also be caused by chronic use of aspirin, acetaminophen, codeine, NSAIDs

DIALYSIS• Used in both acute or chronic renal failure• Can sustain patients even when their kidneys aren’t doing their job
and the person would otherwise get quite sick and die.• Hemodialysis creates a circuit of blood that passes from the body
through a machine and back into the body again. In the machine blood passes through tubes with thin walls made of a semipermeable membrane that allows only certain substances to cross into and from blood. The patient’s blood is cleaned, the electrolytes and acid levels are balanced, and wastes are eliminated before sending the blood back into the patient’s body.
• Usually a patient is dialyzed 3 times a week. It takes 3-4 hours.

A NOTE ABOUT DIABETES
• Diabetic kidney disease is the most common cause of renal failure in the U.S.
• About 20% of patients with diabetes develop chronic renal failure.
• Glycoproteins deposit in glomerular capillaries and interfere with glomerular blood flow and damage the barrier function that prevents protein from entering the glomerular filtrate.

A note onTUMORS OF THE KIDNEY
• Most tumors of the kidney are malignant• More common with increasing age• Renal cell carcinoma: 90% of renal
cancers, affects the epithelium of the tubules. Smokers have twice the risk. Flank pain, hematuria. Tx: removal of kidney