Embed Size (px)
Citation preview

Running Head: Diabetes in Thahin 1
Assessment of Individual Dietary Behavior and Diabetes Health Status among Adults in Thahin,
Thailand: A Correlational Study.
Public Health Field Practicum: Research Proposal
Khon Kaen University
Caroline de Bie, Desbelet Berhe, Diane Jang, Anisa Sanghrajka

Diabetes in Thahin 2
Executive Summary
Rapid globalization is occurring in almost every country, and Thailand is no exception.
As Thailand has experienced economic growth, it has also seen a shift in diet, from more
traditional dishes to more processed, high sugar and high fat foods. As a result, lifestyle related
diseases such as hypertension, obesity and diabetes have become increasingly more common. In
addition to the many people who are diagnosed as diabetic, there are thousands more who go
undiagnosed until symptoms are severe enough to seek care. Our research aims to measure the
susceptibility to diabetes among individuals in the Thahin community of Khon Kaen province.
By distributing questionnaires, we are seeking to find the correlation between dietary habits and
diabetes. With this information, we hope to design an appropriate intervention surrounding
nutrition and the prevention of type II DM. This may take the form of a nutrition seminar, a
cooking class or another educational program in the community.

Diabetes in Thahin 3
Topic
Within the last few decades, Thailand has experienced rapid economic and social change.
With this change comes a change in dietary patterns, a nutrition transition from traditional foods
to a more Western diet. This has lead to a rapid increase in the prevalence of type II DM.
Almost 10% of Thai adults have been diagnosed with the disease (World Health Organization,
2012). Although this chronic disease is usually not very intrusive in everyday life, it can be very
dangerous and can cause diabetic comas, eye problems and circulation issues when left
unchecked. It also can increase an individual’s risk for heart disease, stroke and kidney failure
(WebMD).
In the Thahin community specifically, diabetes has been expressed as a great concern by
community members. During an interview conducted by CIEE students in the fall of 2013, a
village health volunteer responded that diabetes was one of the most important health concerns in
the community. Additionally, because there is a strong relationship with this community from
previous visits, Thahin is well-suited for research and interventions relating to diabetes.
Objectives
Prior to collecting data for the upcoming intervention in Thahin, it is essential to clearly
think through personal and group objectives. By administering a minimum of 30 questionnaires
to adults above the age of 18 throughout the community, we wish to assess the dietary behaviors
by measuring the frequency of specific food item intake. By measuring the prevalence and
susceptibility of diabetes in individuals, through data collected in the questionnaire, specific
interventions can be shaped for the near future. By assessing the community wants and needs, we
will be able to lay a solid foundation as to the approach of our intervention as well. Lastly,
building strong community relationships is extremely important, not only in the success of our

Diabetes in Thahin 4
intervention, but also in the continuing of the strong relationship between CIEE, Khon Kaen
University’s Faculty of Public Health, and Thahin.
Research Question
The research question that will be explored is, “What is the correlation between dietary
behaviors and type II DM status among adults in Thahin?” We will measure dietary behaviors by
asking questions about food consumption, food purchasing, food preparation and dietary
restrictions. Because diet has been shown to be a risk factor for diabetes, we will distribute 30
questionnaires to show that individuals with high saturated fat, carbohydrates, and salt intake
have higher prevalence and susceptibility to type II DM among adults in Thahin.
Rationale for Study
CIEE Public Health students have had the opportunity of visiting Thahin numerous times
over the past several years, which has continued to give students insight into some of the health
issues that face the community. In an interview conducted with a village health volunteer in the
Fall 2013 semester, diabetes was identified as being one of the most pressing public health
issues. Looking more broadly, at Thailand and the northeast Isaan region, it is evident that this is
the case. By studying diabetes more in depth and gaining an understanding of its impact in
Thahin specifically, an effective intervention can be organized and conducted.
Literature Review
Background
Diabetes, or also known as diabetes mellitus, describes a group of metabolic diseases in
which an individual has high blood sugar due to the inability to process insulin effectively.
Approximately 90% of diabetes cases worldwide are classified as type II DM. Individuals with
type II DM produce insulin, however there is not enough being produced, or it is not effective.

Diabetes in Thahin 5
Insulin is defined as a protein hormone synthesized in and secreted by the pancreas to regulate
blood glucose levels. Most commonly in type II DM, cells become insulin resistant which causes
blood glucose levels to uncontrollably increase. Carefully monitoring daily glucose levels,
nutrition, and exercise are crucial in keeping diabetes symptoms under control.
Risk Factors
In the Progress of Diabetes Control in Thailand, the World Health Organization reported
that 1 in 13 Thai’s are diagnosed with diabetes mellitus. A previous literature review on diabetes
management in Thailand, specifically focusing on the burden, costs, and outcomes, provided that
non-communicable disease in Thailand were estimated to account for 71% of all deaths:
cardiovascular diseases representing 27%, cancers 12%, and diabetes 6%. According to the
National Health Examination Survey 2009, the prevalence of diabetes was higher in urban areas
than rural areas. An important problem of diabetes in Thailand is the under-diagnosis therefore
delaying the treatment and care for the patient. Consequently, those with diabetes living in rural
parts of Thailand may face more health implications due to a late diagnosis.
The lack of exercise, smoking, drinking alcohol, unsuitable food consumption, and stress,
including in association with environmental problems, all contribute to the prevalence of
hypertension and diabetes mellitus in Thailand (Nakagasien). These risk factors are more
commonly associated with undiagnosed diabetes, and are a determinant of cardiovascular
disease. In an ethnographic study in Thailand, Dr. Nakagasien reported that the greatest number
of people with diabetes live in the Northeast region, and known as the Isaan region. Dr.
Nakagasien stated that “understanding the process of diabetes mellitus knowledge management
of people in the community is essential” to support the process of knowledge management.

Diabetes in Thahin 6
Naemiratch and Manderson (2006), explored a previous ethnographic study conducted in
Bangkok, Thailand to uncover the perceptions of diabetes and its control, later finding the
importance of diabetes impacting everyday life. It is not until diabetes becomes visible and
intrusive, when patients start to worry and exercise control. For example, extreme rises in blood
sugar levels in an indicator that the patient should see the doctor more often in order to stabilize
their condition (Naemiratch and Manderson, 2006).
In the International collaborative study of Cardiovascular Disease in Asia, researchers
aimed to compare the prevalence and management of diabetes and the association of diabetes
with cardiovascular risk factors. After collecting data through a structured interview, a brief
examination, and a blood sample from 5,105 Thai adults age 35 and older (Aekplakorn, et al.) .
As a result, researchers concluded that the national prevalence of diabetes of Thai adults was
9.6% (2.4 million people), including 4.8%of though previously diagnosed and 4.8% of those
newly diagnosed. The issue of diabetes in Thailand is not the treatment accessible to the patients,
but rather the fact that only half of all cases are undiagnosed (Aekplakorn, et al). Since diagnosed
diabetes is treatable with low-cost, preventive therapies, research suggest that initiative focusing
on diagnosis rates would most likely produce health benefits in Thailand.
Diabetes is a growing global health issue. In 2025, it is projected that the number of
individuals with diabetes will rise to 300 million, with the greatest increases in developing
nations, including Thailand (Aekplakorn, et al.). In order to control the prevalence of diabetes
mellitus in Thailand, there is a need for health education on nutrition, an increase of screening in
high risk populations, identifying factors that affect poor treatment outcomes, and providing an
effective framework to track the progress. Furthermore, by executing an intervention in the
Thahin community in the Khon Kaen province, we plan on leaving middle-aged adults with

Diabetes in Thahin 7
basic knowledge about the health risks of diabetes and nutrition, and changes they could
implement in their diet in order to reduce the onset of severe diabetes related symptoms.
Although there have been past research focusing on diabetes management and control
and teaching programs, there is still a failed attempt at uncovering the behaviors and trends
associated with people who have the condition but are not proactive in treatment. There are
thousands of Thais living in rural and isolated parts of Thailand who may not even know they
have diabetes until their condition has worsened enough to then see a doctor. Therefore, by
observing the Thai food chain and understanding the role of nutrition in diabetes mellitus, the
population can be provided with effective knowledge on how adapt to a healthier lifestyle.
Symptoms
Diabetes if not kept under control can lead to the development of more severe symptoms.
Some of these symptoms include increased hunger and thirst, frequent urination, unexplained
weight loss, fatigue, blurred vision, numbness or tingling of the hands or feet, slow healing sores
and cuts, dry and itchy skin, and frequent yeast infections. These symptoms can decrease one’s
quality of life and it is therefore important to control glucose levels before symptoms continue to
get worse. Other more overarching health concerns that are closely related to diabetes include:
mental health issues, hearing loss, hypertension, neuropathy, peripheral arterial disease, coma,
and stroke for example.
Dietary Intake
Individual diabetics need to keep in mind their dietary intake, as they as individuals must
keep their glucose levels in check. The American Diabetes Association outlined food suggestions
for type II diabetics suggesting that individuals should enrich their diet with calcium, potassium,
fiber, magnesium, and vitamins A, C, and E in correct portion sizes. Some of the “super-foods”

Diabetes in Thahin 8
that are highly recommended include beans, dark leafy vegetables, citrus fruit, sweet potatoes,
berries, fish high in Omega-3 and fatty acids, whole grains, and fat-free milk and yogurt.
High sugar and alcohol intake can negatively impact the glucose control of a diabetic
patient. In order to make this process easier, there are several diet trackers and programs which
help to facilitate patient progress (American Diabetes Association, 2013).
Goals outlined in Diabetes Care discuss the short and long-term goals that should be
followed in order to reduce the impacts of diabetes. The goals are listed below:
1. To attain and maintain optimal metabolic outcomes specifically blood glucose levels,
lipoprotein profile, and blood pressure
2. To prevent and treat the chronic complications of diabetes by modifying personal lifestyle as
appropriate for the prevention and treatment of other diseases
3. To improve overall health through healthy food choices
4. To take into consideration personal and cultural barriers, including recognizing wish to change
and adapt (Diabetes Journal, 2013).
Using the above information, it is clear that individual food intake combined with other
factors, greatly impact diabetes in general. We plan on designing an intervention on the nutrition
within the Thahin community.
Cultural Eating Behaviors in Thailand
As previously mentioned, diet is a key factor in the development of type II DM. The
modern diet of northeastern Thailand in particular is highly likely to lead to this condition.
According to research done by Vongsulvat Kosulwat, the typical Isaan diet consists of dishes
such as sticky rice, grilled and fried meats, papaya salad, soups and ready-to-eat snacks. In more
urban areas like Bangkok, Thai staples are being replaced with pre-made, processed foods.

Diabetes in Thahin 9
Across the country, the consumption of carbohydrates and fats has been steadily increasing since
the 1990s (2002). Additionally, the diversity of the Thai diet has greatly increased: there are
many more fruits, vegetables and animal products available at the markets (Dixon et. al., 2006).
The high consumption of sugars and fats across the entire country clearly correlate to the steady
increase in prevalence of diabetes.
Aside from the food itself, food purchasing and consumption practices greatly affect
one's health. The total amount of money spent on food in Isaan is a fair amount higher than the
amount of money spent in urban areas. The typical Isaan household spent approximately 37% of
their total budget on food in 1999, while urban families spent only 29% of their budget on food.
Also, the money spent on food from markets and convenience stores, which can be very high in
sugar and fat, has greatly increased over all of Thailand. In the northeast, the total proportion
almost doubled from 12.2% of food expenditures in 1990 to 21.7% in 1999. In urban areas, this
number is much higher, at about 50% of total food expenses. When food is prepared in the home,
it is most commonly either stewed, grilled or fried. Traditionally, dishes are served all at once
and shared amongst everyone (Kosulwat, 2002). Such practices have significantly impacted the
prevalence of diabetes mellitus in Thailand overall, but northeastern Thailand in particular has
seen the most rapid growth in this disease. Previous research has indicated that this is a serious
problem, and the reasons for higher growth in the Isaan region must be explored further.
Rationale for Questionnaire
For numerous previous research projects, researchers utilized Simplified Food Frequency
Questionnaire to assess participants’ individual dietary behaviors. Simplified Food Frequency
Questionnaire is consisted of a list of questions that ask about participants’ consumption
frequencies of foods and beverages. Then the nutrient intake can be estimated by multiplying the

Diabetes in Thahin 10
frequency of each food by the amount of nutrients. We decided to base our questionnaires on the
Simplified Food Frequency Questionnaire because it is very easy to administer, represents the
usual intake of the participants, and has high validity despite the fact that Simplified Food
Frequency Questionnaire is relatively short and does not take into portion sizes. When Simplified
Food Frequency Questionnaire was compared with 7-day Estimated Diet Records, the
researchers found out that Simplified Food Frequency Questionnaire yields similar responses and
conclusions as 7-day Estimated Diet Records. The results were valid across most food groups
across different gender and age groups. The results for grains and sauces were only slightly
different (De Keyzer et al., 2013). There was also another study that assessed the validity of
Simplified Food Frequency Questionnaire conducted on Taiwanese elderly. They then compared
the responses with the 24-hour Dietary Recall and Biomarkers. Their results showed that the
responses from both dietary assessment tools are very similar, thus making the Simplified Food
Frequency Questionnaire valid. Also, the validity was high for dairy, fish, and fruit intakes for
both genders (Huang, Lee, & Wahlqvist. 2011). Therefore, we incorporated question types from
the Simplified Food Frequency into our questionnaires to increase the validity of our assessment
of individuals’ dietary behaviors.

Diabetes in Thahin 11
Conceptual Framework
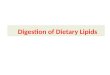
Figure 1. Conceptual Framework of Research in Thahin
The above diagram breaks down the conceptual framework that we have developed in the
design of our research. To start, our variables include individual dietary practices including the
intake of fats, carbohydrates, sugar, and salt, as well as measuring dependent variables including
prevalence and susceptibility by looking at family history, medical records, BMI, and blood
pressure. The objective of this research is to be able to measure the susceptibility of diabetes in
Thahin after collecting thirty surveys. The research question that will be focused on is, What is
the correlation between dietary behaviors and type II DM status among adults in Thailand. From
this research question, we expect to find that adults who consume high amounts of fats,
carbohydrates, sugars, and salt, will have a higher susceptibility of getting diabetes. The

Diabetes in Thahin 12
reasoning behind focusing our research in this way is because the problem in Thahin, which we
are identifying is that poor nutritional behaviors can negatively impact an individual’s health,
specifically those who are susceptible to diabetes.
Methods
In this research study, data collectors will conduct questionnaires through interviews. We
will be targeting our questionnaires at the adult population in the Thahin community. Prior to the
interviews, we plan to introduce ourselves and the reasoning for our research. Interviews will be
conducted in the presence of a translator in order eliminate any language barriers. The translators
in this study will receive the survey ahead of time to be translated in Thai. The research that will
be conducted in the Thahin community includes both qualitative and qualitative methodologies
in our data collection. In accordance to the characteristics of quantitative and qualitative
methodologies presented in the Public Health Field Practicum Reading Packet, CIEE 2013, our
purpose is to measure actions, tendencies, and levels of knowledge carried out by our objectives
and variables (International Planned Parenthood Foundation, 2002).
Although the survey, found in the appendix A, is majority quantitative consisting of
close-ended questions carried out by predefined variables before data collection, we will also
utilize a qualitative approach in obtaining information on family history and medical records.
Implementing qualitative and quantitative strategies in the data collection will strengthen the
evaluation design and data analysis.
As shown in Figure 1, our objective is to measure the susceptibility of diabetes in the
Thahin community by looking at specific variables. In this study, the independent variable is the
individual dietary practices and the dependent variable is the prevalence and susceptibility. By
asking how one prepares their food, ingredients they use, frequencies and the amount, the data

Diabetes in Thahin 13
collectors will use this evidence to better understand how their diets affects their health status
and susceptibility to diabetes.
Participants
The participants will be Thai men and women ages 18 and over from the Thahin Village,
Khon Kaen, Thailand. There is no participant requirement other than age. The participants can
either have or not have type II DM. Data collectors aim to reach a total of 30 participants,
recruited by convenience sampling method. One translator and four data collectors will walk
around the village and survey anyone who meets the age requirement. The surveys will be
conducted on the basis of the participants’ permission and comfortability.
Measures
Prevalence and susceptibility of type II DM. Participants’ demographic information
such as sex, age, and type II diabetic health status will be measured with simple survey
questions. The participants’ height and weight will be measured to calculate their Body Mass
Index (BMI). Also, with the help of Village Health Volunteers, we will measure the blood
pressure of each participant after conducting the questionnaire. Lastly, the participants will be
asked about the family history of type II DM and how often they exercise in order to assess
susceptibility of type II DM.
Dietary assessment. The questions that assess individual dietary behaviors are based on
the Simplified Food Frequency Questionnaire by Dr.Willet and his team at the Harvard School
of Public Health (2003). For questionnaires, please refer to Appendix 1.Through the survey
questions, the participants’ food intake frequencies will be assessed by recalling how many
times they ate certain food described in the questionnaires in the past week. Then, the individual
dietary behavior will be defined by dietary score based on the assigned scores for the frequency

Diabetes in Thahin 14
of each food consumed (Question #16, Appendix A). Data collectors will also use a visible
representation to better gauge the amount of ingredients used in their foods, as indicated by the
following answer options : a little bit, moderate amount, a lot or none (Question #15, Appendix
A). With the use of a tablespoon and a measuring cup, we can better understand the amount of
these foods into ones diets, which will be helpful in our data analysis. For example, less than a
tablespoon indicates “a little bit,” a tablespoon is a moderate amount, and more than a tablespoon
is “a lot.” All of the responses for both measures will be anonymous to ensure participants’
privacy.
Data Analysis
It is important to note that we are assuming participants to answer the questionnaires as
honestly and accurately as possible. After gathering all the responses from the questionnaires,
descriptive statistics will be used to report participants’ demographic information and type II
diabetic status. According to a study conducted in a health check-up clinic in Khon Kaen,
Thailand, men who have a Body Mass Index (BMI) of ¿27, and women who are > 25 will be
classified as obese (Pongchaiyakul, et al., n.d.). The individual dietary score will be measured
according to the scores that we assigned to each food group (Appendix B).
The salt, sugar, and fat intake will be calculated by combining the amount of intake for
each group based on the participants’ responses for question number 15 (R. MSG, salt, and soy/
fish sauce will be categorized into salt group, sugar and condensed milk into sugar group, and
vegetable oil and butter into the fat group. For the dietary score, A (none) will score 4, B (little)
will score 3, C (moderate) 2, and then D (a lot) with 1. All the scores will be added up to yield
final score for each participant to assess their dietary behavior.

Diabetes in Thahin 15
Then we will conduct correlation statistics to see what correlations exist between the the
individual dietary scores and Type II Diabetic health status. All quantitative data will be
analyzed using SPSS and Microsoft Excel. The qualitative data will be used as supplemental
information that will better prepare data collectors with the necessary tools and knowledge for a
future intervention project.
Discussion
After our research in the Thahin community is complete, it is expected that the data will
show a positive correlation between high fat, carbohydrate, sugar and salt intake and
susceptibility of diabetes. Our survey will ask questions about a variety of factors that can lead to
diabetes, such as food consumption and preparation, exercise patterns, and family history. These
questions will give us sufficient insight into each individual’s susceptibility to diabetes. In order
to make sure that our results are useful, as a group we will try to keep things as consistent as
possible so that the data is externally and internally valid. We will also take full advantage of the
time and resources given to us. We will try to successfully target subjects who will respond in
such a way that will clearly illustrate a relationship between the dependent and independent
variables in question without selection bias.
With the information collected, we will design an intervention to suit the needs of the
community while keeping in mind our own limitations, both in terms of time and resources. If
we find no correlation, we will deliberate on the next steps, conduct further research in the
community and decide on another feasible intervention that reflects the true needs of the
community. If we do find a positive correlation, we will potentially create education programs
based on cooking and nutrition to involve the whole community and have maximum impact. If a
nutrition program is not an expressed desire, we may incorporate exercise into an intervention

Diabetes in Thahin 16
plan, which has also been shown to positively impact the course of diabetes and prevention.
Because diabetes has been expressed as a health concern in the community, an intervention
targeted at this topic will most likely be very well-received.

Diabetes in Thahin 17
References
Aekplakorn, W., Suriyawongpaisal, P., Stolk, R., Neal, B., Woodward, M., Chongsuvivatwong,
V., & Cheepudomwit, S. (2003). The prevalence and management of diabetes in Thai
adults: The International Collaborative Study of Cardiovascular Disease in Asia.
Diabetes Care, 26(10), 2758-2763.
American Diabetes Association. (2013). What Can I Eat. Retrieved from
http://www.diabetes.org/?loc=logo
De Keyzer, W., Dekkers, A., Van Vlaslaer, V., Ottevaere, C., Van Oyen, H., De Henauw, S., &
Huybrechts, I. (2013). Relative validity of a short qualitative food frequency
questionnaire for use in food consumption surveys. European Journal Of Public Health,
23(5),737-742.
Deerochanawong, C., & Ferrario, A. (2013). Diabetes management in Thailand: a
literature review of the burden, costs, and outcomes. Globalization & Health, 9(1), 1-18.
Dixon, J., Banwell, C., Kanponai, W., Friel, S., Seubsman, S., & MacLennan, R. (2007). Dietary
diversity in Khon Kaen, Thailand, 1988-2006. International Journal Of Epidemiology,
36(3), 518-521.
Huang, Y., Lee, M., Pan, W., & Wahlqvist, M. (2011). Validation of a Simplified Food
Frequency Questionnaire as Used in the Nutrition and Health Survey in Taiwan
(NAHSIT) for the Elderly. Asia Pacific Journal Of Clinical Nutrition, 20(1), 134.
International Planned Parenthood Foundation (2002). Guide for Designing Results-Oriented
Projects and Writing Successful Proposals. Public Health Field Practicum Reading
Result, CIEE.
Kosulwat, V. (2002). The nutrition and health transition in Thailand. Public Health

Diabetes in Thahin 18
Nutrition, 5(1A), 183-189.
Naemiratch, B., & Manderson, L. (2006). Control and adherence: living with diabetes in
Bangkok, Thailand. Social Science & Medicine, (5), 1147.
Nakagasien, P. (n.d.) Diabetes Mellitus Knowledge Management in the Rural Community: An
Ethnographic Study in Thailand. International Seminar Population and Development.
Nutrition Principles and Recommendations in Diabetes. (2004).American Diabetes Association.
Diabetes Care, 27S36-S46.
Pongchaiyakul, C., Nguyen, T.V., Wanothayaroj, E., Krusun, N., Klungboonkrong, V. (2007).
Prevalence of Metabolic Syndrome and Its Relationship to Weight in the Thai
Population. Journal for the Medical Association of Thailand, 90 (3), 459-467.
Tee, E., Dop, M., & Winichagoon, P. (2004). Proceedings of the workshop on food-consumption
surveys in developing countries: future challenges. Food And Nutrition Bulletin, 25(4),
407-414.
Type II DM (n.d.) Diabetes Health Center. WedMD. Retrieved from
http://diabetes.webmd.com/guide/diabetes_symptoms_types
Willett, W. (2003). Nurses’ Health Study II, Harvard School of Public Health and Harvard
Medical School. Retrieved from http://www.channing.harvard.edu/nhs/
World Health Organization (2004). Age-standardized Disability-adjusted Life Years (DALYs):
Diabetes Mellitus by Country.

Diabetes in Thahin 19
Appendices
Appendix A. Questionnaire Diabetes in ThahinNovember 23, 2013
Good morning! Today, as American public health students studying at Khon Kaen University, we are trying to understand the impact of diabetes within the Thahin community. We greatly appreciate your participation in this survey. All of your responses will be anonymous.Please feel free to direct any questions you may have to our team.
Demographic
1. How old are you (years)? _________ years old
2. How much do you weigh (kg)? __________ kg
3. How tall are you (cm)? _________ cm
4. Do you have diabetes? Yes No
If yes, please kindly answer the following questions:
4a. Which type of diabetes do you have? Type I Type II Gestational Unknown
4b. How long have you been diagnosed with diabetes (in years)? ___________ years
4c. How often do you visit your doctor? _____________________
5. Do you have high blood pressure? Yes No
Family History
6. Does anyone in your immediate family (parents, grandparents, siblings) have diabetes? Yes No
7. Does anyone in your immediate family have high blood pressure? Yes No(parents, grandparents, siblings) Exercise

Diabetes in Thahin 20
8. How often do you get physical activity (voluntarily or/and occupationally) ?
ퟀ a. Never ퟀ b. 1 - 2 a week ퟀ c. 3 - 6 times a week ퟀ d. Everyday ퟀ e. Other. Please specify _________________
Nutrition
9. Have you had any exposure to a nutritional program in the past? Yes No
If yes, please specify when: __________________
10. Do you have any dietary restrictions? Yes No
If yes, please specify ______________________
11. Do you think diabetes is a big issue in this community? Yes No
12. Where do you get most of your food from? __________________________________
13. Every week, how many times do you buy food to eat? _________ times
14. Every week, how many times do you cook for yourself? ____________ times
15. How much of the following ingredients do you cook with on a regular basis?

Diabetes in Thahin 21
Ingredient A B C D
MSG
Salt
Sugar
Vegetable Oil
Butter
Condensed Milk
Soy/ Fish Sauce
A: NoneB: A lit bitC: A moderate amountD: A lot
16. Last week, how often did you consume the following foods?

Diabetes in Thahin 22
Food Never Once 2-3 times 4-5 times 6-7 times
Dairy (cow milk, soy milk, yogurt)
Fruits
Boiled/steamed Vegetables
Stir-fried Vegetables
Deep-fried Vegetables
Boiled/steamed Meat/ Fish
Grilled Meat/Fish
Stir-fried Meat/Fish
Deep-fried Meat/Fish
Fried Egg
Deep-fried Egg
Boiled Egg
Rice/Noodles
Sticky rice
Soda
Alcohol

Diabetes in Thahin 23
Chocolate, Candy, Chips
Appendix B. Dietary Scores. 4 being the healthiest to 0 being the least healthy
Food Never Once 2-3 times
4-5 times
6-7 times
Dairy (cow milk, soy milk, yogurt)
0 1 2 3 4
Fruits 0 1 2 3 4
Boiled/steamed Vegetables 0 2 3 4 4
Stir-fried Vegetables 0 2 3 2 0
Deep-fried Vegetables 4 3 2 1 0
Boiled/steamed Meat/ Fish 0 1 2 3 4
Grilled Meat/Fish 0 1 2 3 3
Stir-fried Meat/Fish 0 1 2 1 0
Deep-fried Meat/Fish 4 3 2 1 0
Fried Egg 2 4 3 2 1
Deep-fried Egg 4 3 2 1 0
Boiled Egg 0 1 2 3 4
Rice/Noodles - - - - -

Diabetes in Thahin 24
Sticky rice 4 3 2 1 0
Soda 4 3 2 1 0
Alcohol 4 3 2 1 0
Chocolate, Candy, Chips 4 3 2 1 0