Embed Size (px)
Citation preview

Terapia Neoadiuvante nella malattia HER-2 positiva:Trasferibilità nella pratica clinica
Vincenzo Adamo Vincenzo Adamo
UOC Terapie Integrate in OncologiaAOU Policlinico ”G.Martino” MessinaUOC Terapie Integrate in OncologiaAOU Policlinico ”G.Martino” Messina

Sequence of Treatment for Primary Breast Cancer
Diagnosis and Staging
Surgical Resection
Adjuvant systemic treatment
Diagnosis and Staging
Neoadjuvant systemic therapy
Surgical Resection
Adjuvant therapy
The Rational for Neoadjuvant Therapy in Breast Cancer: Which Patients?
Traditionally: Neoadjuvant systemic therapy should be considered for patients inoperable at onset: T4, clinical N2-N3
New data: supporting preoperative or neoadjuvant systemic therapy in primary operable breast cancer patients
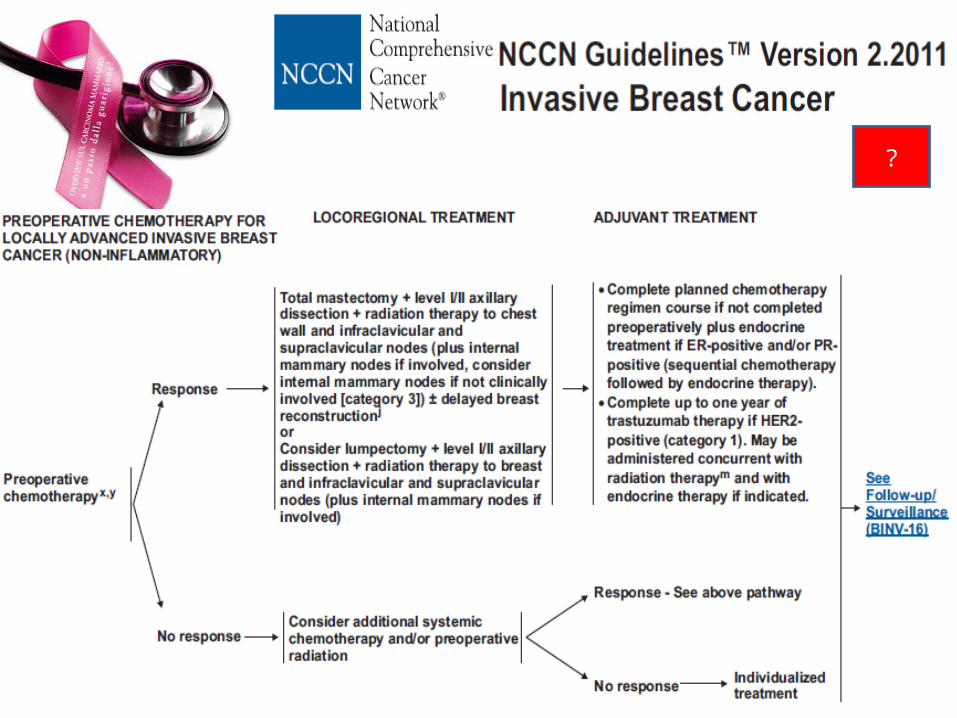
NCCN Guidelines 2011:neoadjuvant chemotherapy or trastuzumab plus chemotherapy should be considered for HER2+ patients


Goals of Neoadjuvant Theapy in Breast Cancer
Make tumours more operable, increase the rate of breast conserving surgeries
Improve prognosis of certain disease subtypes (i.e. HER2+)
Have a better idea of prognosis based on response to neoadjuvant treatment
Allow patients to start treatment earlier
Reduce the extent of surgery required in breast and axylla
Improve DFS and OS using pathological response rate for selection of subsequent treatment in individual patients

Parametres to assessed in clinical practice
pCR and Treatment Outcomes
Status lymph node (sentinel node biopsy)
Instrumental evaluation with MRI and PET
Toxicity
Definition of pCR
Different definition of pCR are in use:
- Absence of invasive cancer in the breast
- Absence of invasive cancer in the breast and in the axillary lymph nodes.
- Absence of invasive and in situ cancer cells in the breast and in the axillary nodes
There is high degree of concordance between the different definition
With very definition pCR identifies cases with favorable disease
Marchiò C. & Sapino A. JNCI Monogr 2011;43:86–90
Putative Predictive Factors of pCR
Tumor size & Tumor grade
Histological type
ER/PgR
Her2/neu
Proliferative markers ( Ki-67/MIB-1, PCNA)
Treatment & MDR-1/pgp
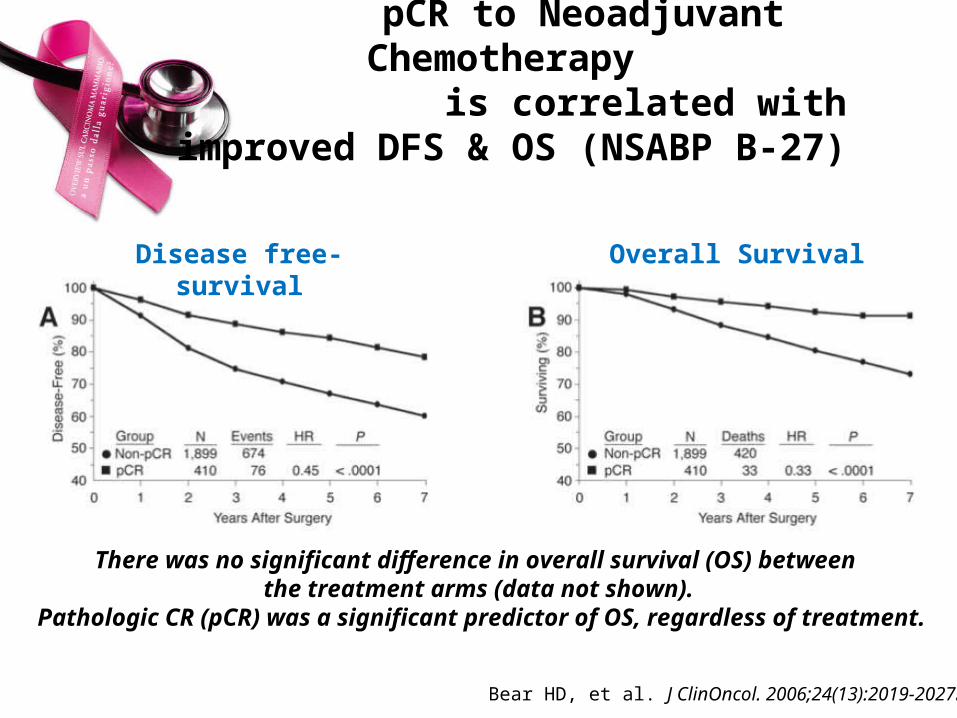
There was no significant difference in overall survival (OS) between the treatment arms (data not shown).
Pathologic CR (pCR) was a significant predictor of OS, regardless of treatment.
Bear HD, et al. J ClinOncol. 2006;24(13):2019-2027.
Disease free-survival Overall Survival
pCR to Neoadjuvant Chemotherapy is correlated with improved DFS & OS
(NSABP B-27)

Outcomes of Neoadjuvant Trials with unselected tumor characteristics
Mazouni C, et al. J Clin Oncol. 2007
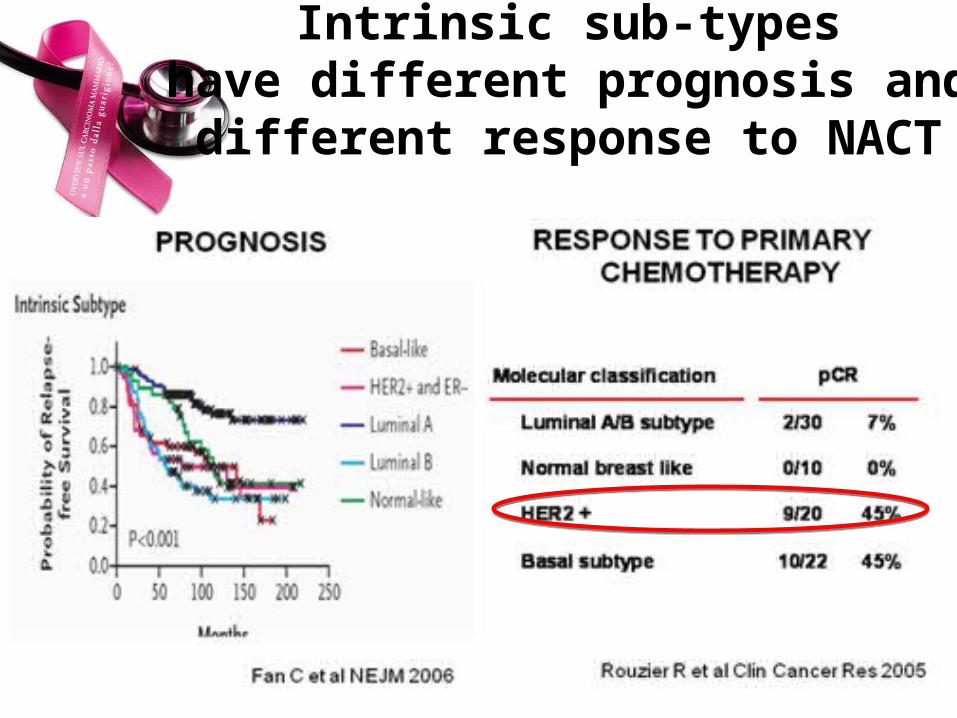
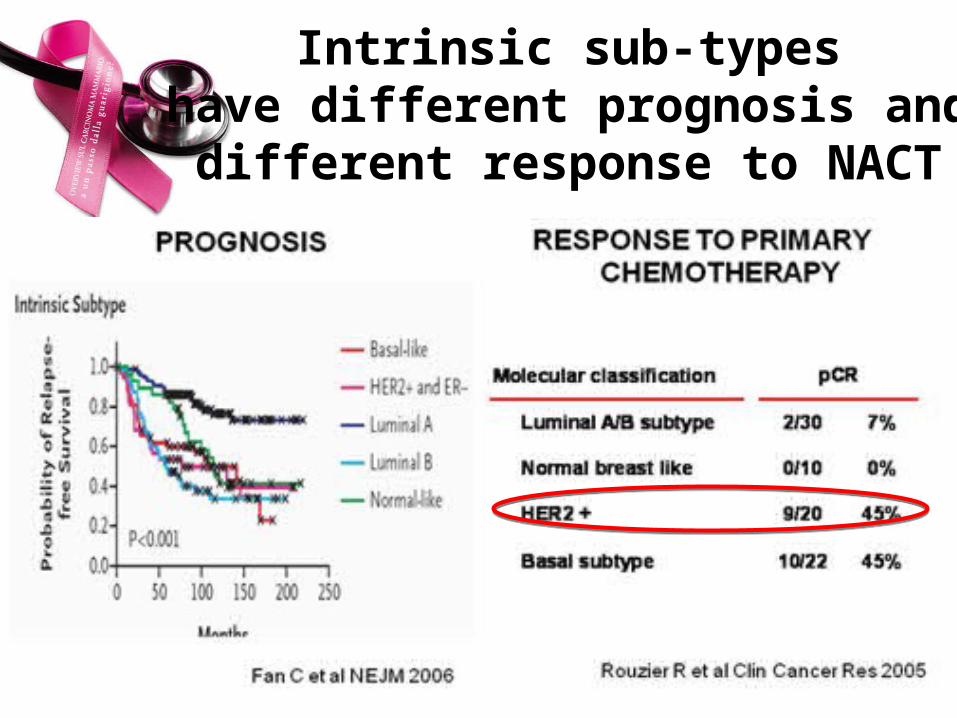
Intrinsic sub-types have different prognosis and
different response to NACT
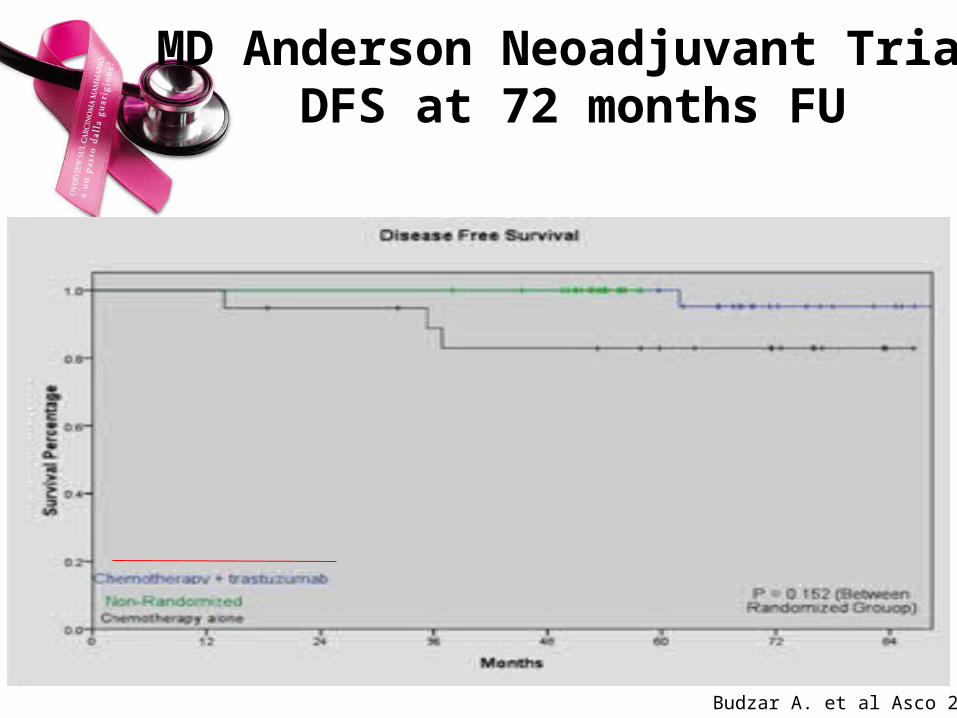
MD Anderson Neoadjuvant TrialDFS at 72 months FU
Budzar A. et al Asco 2009
“ ..if indicated, the majority of the Panel considered that the neoadjuvant chemotherapy regimen should include both a taxane and an anthracycline and(for HER2-positive disease) an anti-HER2 drug.Thus, the choice of a regimen for adjuvant or neoadjuvant chemotherapy might be made using similar criteria..’’
Goldhirsch A, et al. Ann Oncol. 2009;20(8):1319-1329.

Impact of treatment characteristics on the pCR
Untch M. et al J Nat Cancer Inst Monogr
2011.

Impact of treatment characteristics on the pCR
Untch M. et al J Nat Cancer Inst Monogr
2011.
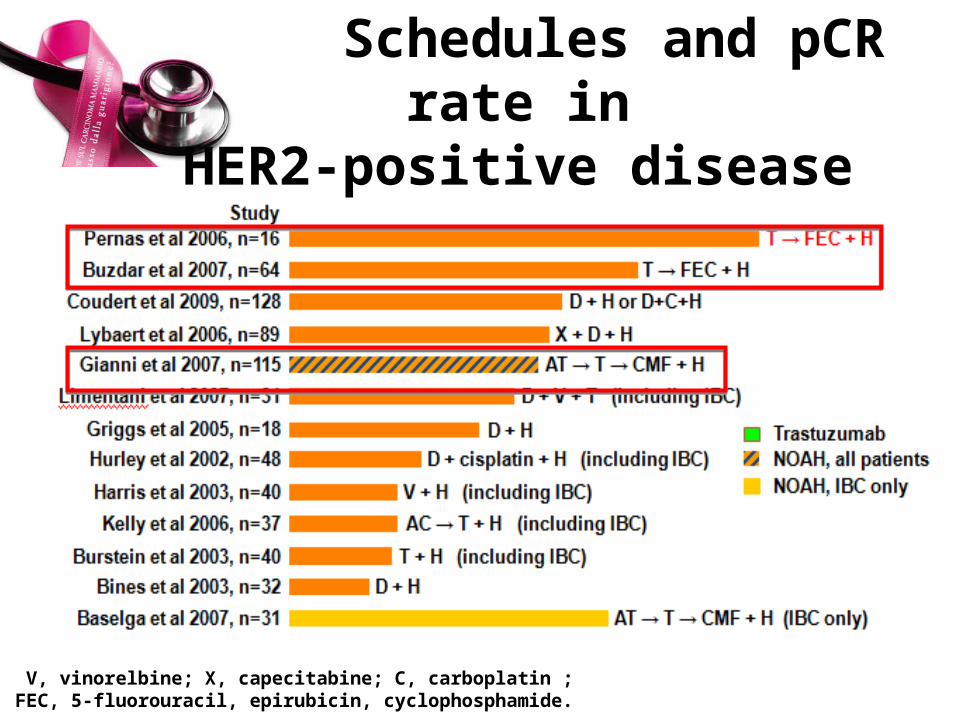
V, vinorelbine; X, capecitabine; C, carboplatin ;FEC, 5-fluorouracil, epirubicin, cyclophosphamide.
Schedules and pCR rate in HER2-positive disease

Pre and Post-operative Chemotherapy plus Trastuzumab Improve DSF

… Future Clinical Practice….

Anti-HER2 Treatment:Mechanisms of action
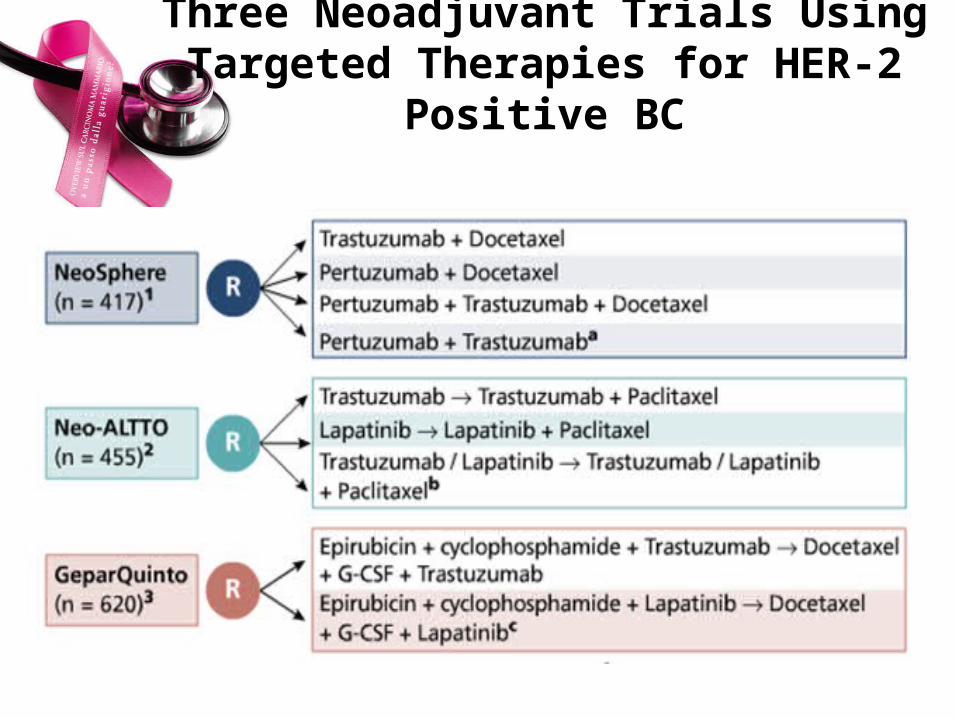
Three Neoadjuvant Trials Using Targeted Therapies for HER-2 Positive BC

pCRS in Three Trials with Target Therapies
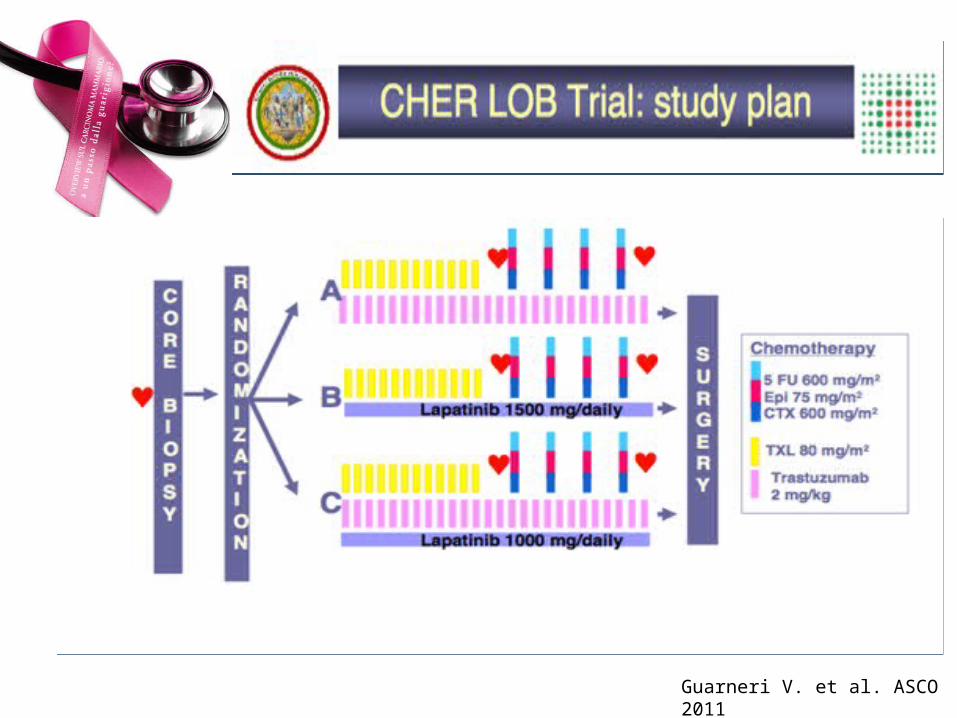
Guarneri V. et al. ASCO 2011

Efficacy: Breast and Axillary pCR Rate
Guarneri V. et al. ASCO 2011

Status lymph node (sentinel node biopsy)
SLNB in relation to neoadjuvant therapy
Which is the aim of SLNB in breast cancer patients?
Which patients are usually receiving neoadjuvant?
Is there a role of SLNB in patients undergoing neoadjuvant therapy?
Should SLNB be performed before or after neoadjuvant therapy?
Are there sufficient data supporting either approach ?
St Gallen 2007, Annals of Oncol 18: 1133–1144, 2007

SLN Biopsy Prior to Therapy
Disadvantages• Two operations• Potentially delays start of chemotherapy
Advantages• Higher identification rate• Lower false negative rate
St Gallen 2007, Annals of Oncol 18: 1133–1144, 2007
The Role of SNLB
Inflammatory breast cancer not indicated– breast lymphedema, due to occluded lymphatics by metastatic
cells
inadequate lymphatic drainage
mapping agents would also be trapped and not travel to the SLN
false-negative rate very high
Locally Advanced (large tumor size)- Palpable lymphadenopathy FNA –No Role for SNLB
- Non palpable or Clinically negative LNs SLNB is acceptable
- Before or after neo-adjuvant chemotherapy ?
St Gallen 2007, Annals of Oncol 18: 1133–1144, 2007

Marchiò C. & Sapino A. JNCI Monogr 2011;43:86–90

St Gallen 2011:SN and ALND

Downstaging Axilla & Complete Axillary Response
Strong prognostic factor
Axillary pCR: 93%
Residual disease: 60%
Hennessey BT, et al. J Clin Oncol.2005;23(36):9304-9311.

Instrumental evaluation: MRI and PET and Neoadjuvant Chemo in HER2BC

MRI: Evaluation Neoadjuvant Chemotherapy
MRI highest accurracy for monitoring chemotherapy Change in (residual) tumor size, signal intensity, and
contrast kinetics Underestimation possible!
Mc Guire K.P. et al.Ann Surg Oncol 2011

MRI Staging after NACT : Does Tumor Biology Affect Accuracy?
MRI response versus pathologic response by tumor subtype. Discrimination and predictive value (a) overall, (b) luminal A/B, and (c) HER2+/TN
Mc Guire K.P. et al.Ann Surg Oncol 2011
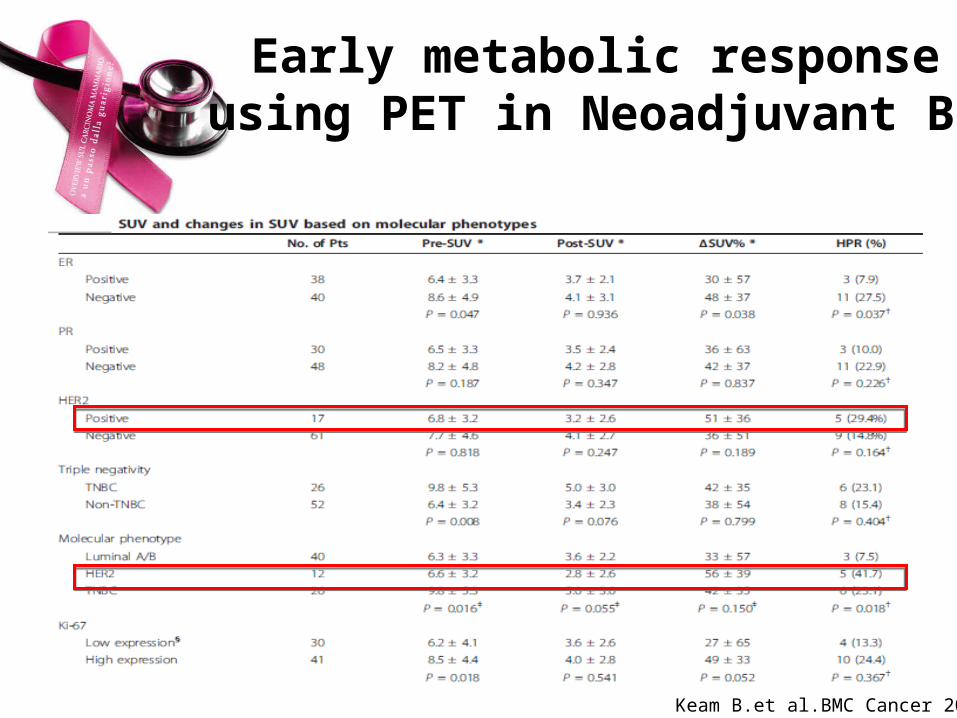
Early metabolic responseusing PET in Neoadjuvant BC
Keam B.et al.BMC Cancer 2011
Toxicity and neoadjuvant Chemotherapy in HER2BC
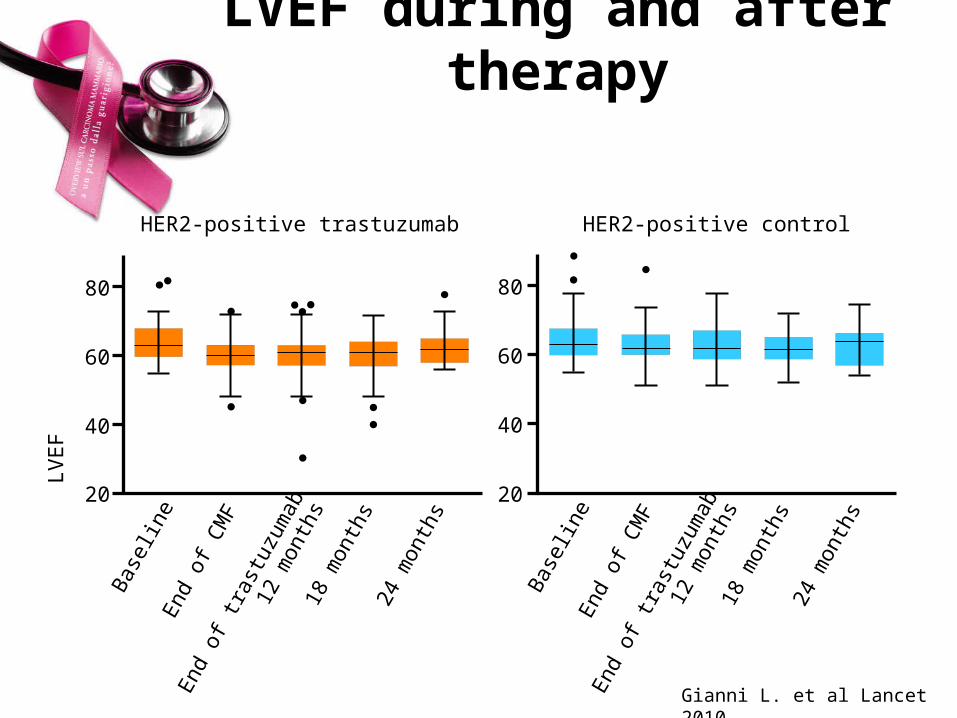
LVEF during and after therapy
HER2-positive control
End
of C
MF
18 m
onth
s24
mon
ths
Bas
elin
e
20
40
60
80
HER2-positive trastuzumab
End
of C
MF
18 m
onth
s24
mon
ths
Bas
elin
e
20
40
60
80
LVE
F
End
of t
rast
uzum
ab12
mon
ths
End
of t
rast
uzum
ab12
mon
ths
Gianni L. et al Lancet 2010
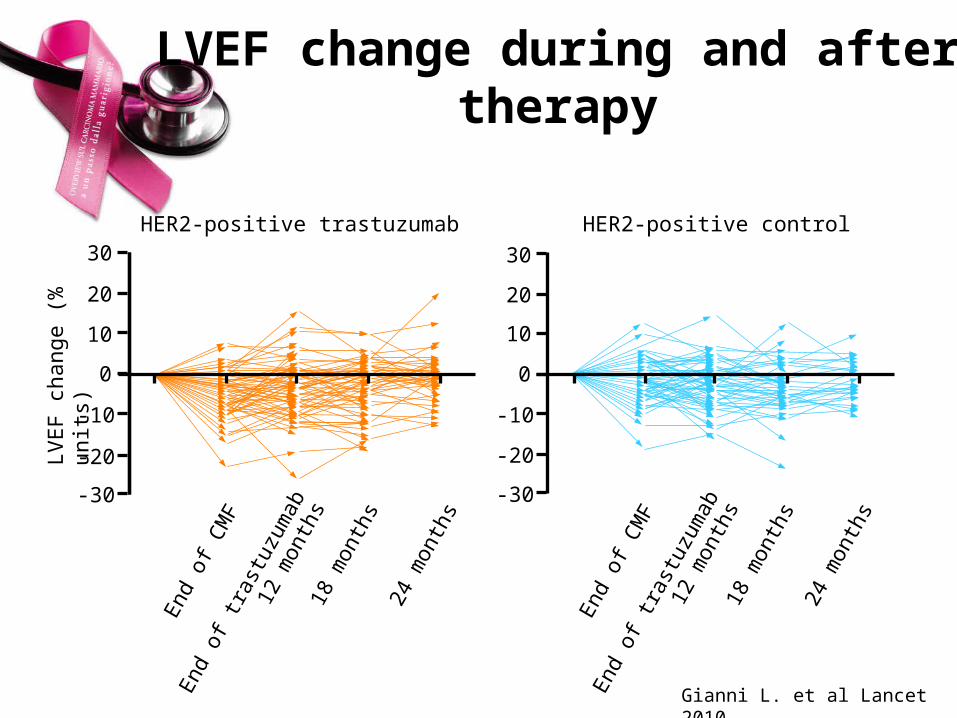
LVEF change during and after therapy
End
of C
MF
18 m
onth
s
24 m
onth
s
30
20
10
0
-10
-20
-30
LVE
F c
hang
e (%
uni
ts)
End
of C
MF
18 m
onth
s
24 m
onth
s
30
20
10
0
-10
-20
-30
HER2-positive controlHER2-positive trastuzumabE
nd o
f tra
stuz
umab
12 m
onth
s
End
of t
rast
uzum
ab12
mon
ths
Gianni L. et al Lancet 2010
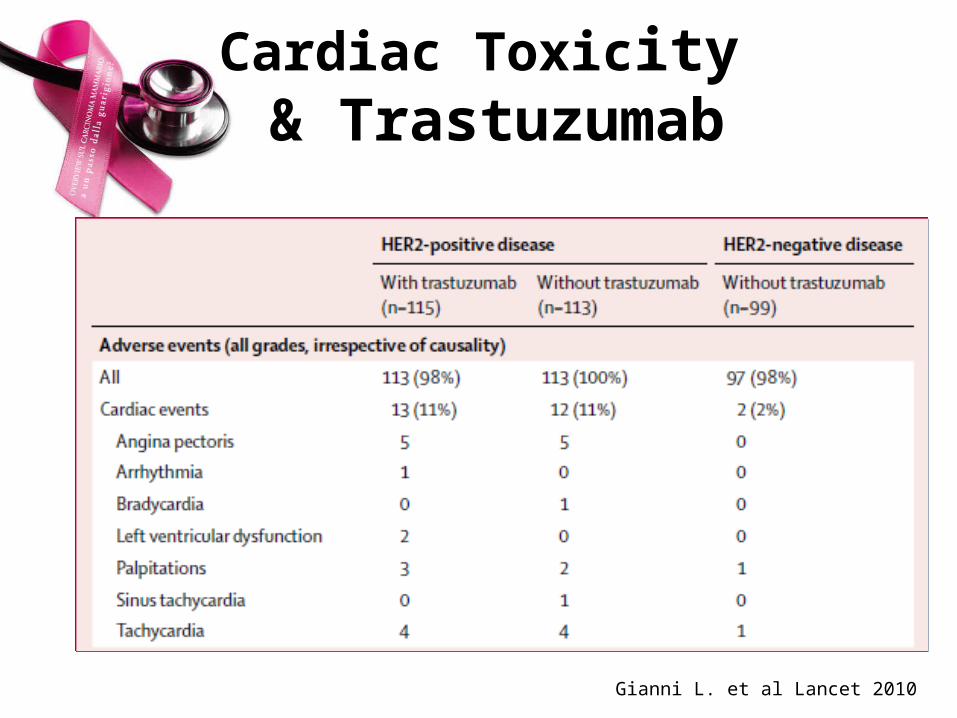
Cardiac Toxicity & Trastuzumab
Gianni L. et al Lancet 2010

Cardiac monitoring guidance: Trastuzumab
• All patients for Herceptin treatment should undergo baseline cardiac assessment prior to treatment initiation
• For patients with EBC, cardiac assessment should be performed every 3 months during treatment and at 6, 12 and 24 months following cessation of treatment
• For patients with MBC, cardiac function should be monitored during treatment (eg every 3 months)
• Patients who develop asymptomatic cardiac dysfunction may benefit from more frequent monitoring (eg every 6-8 weeks)
CGCC, Cardiac Guidelines Consensus Committee;EMEA, European Medicines Evaluation Agency
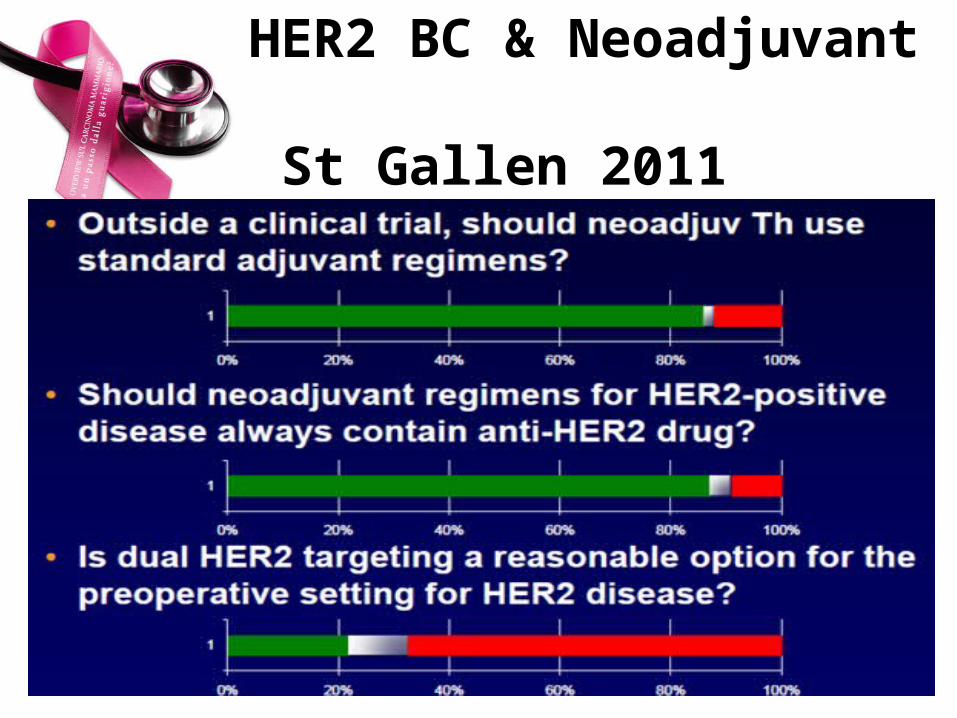
HER2 BC & Neoadjuvant St Gallen 2011
Intrinsic sub-types have different prognosis and
different response to NACT
Conclusive comments • NACT should be considered as an option for every woman as
far as the indication for adjuvant treatment has been confirmed• Many good quality clinical trials suggest that trastuzumab
should be incorporated in the preoperative treatment of women with HER2-pos (..NCCN guidelines).
open questions• the preferred combination chemotherapy with trastuzumab• the optimal duration of trastuzumab in pts who achieve a pCR
after preoperative chemotherapy.
Comments and questions


The end
• Stop here
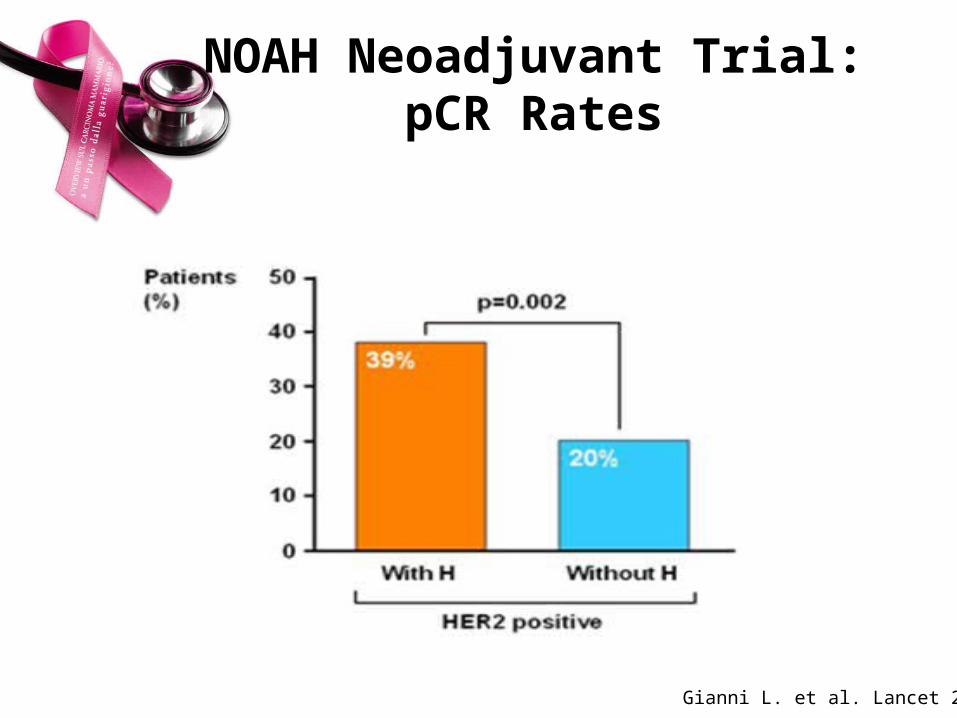
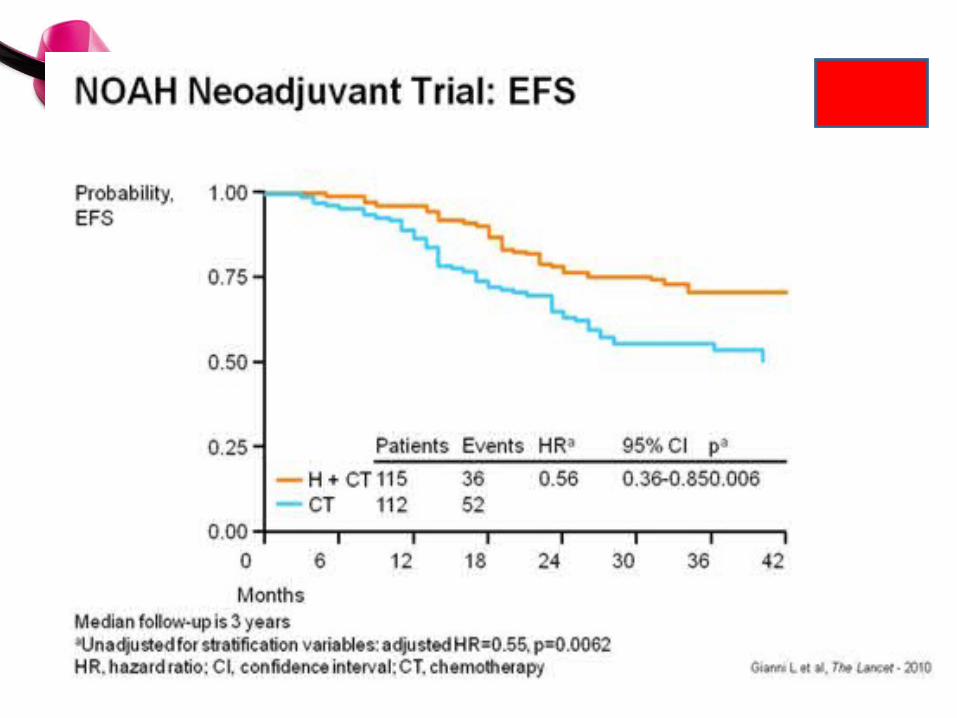
NOAH Neoadjuvant Trial:pCR Rates
Gianni L. et al. Lancet 2010

pCR After NACT Plus Trastuzumab Predicts Favorable Survival in HER2+ BC:
Results From the TECHNO
Untch M. et al, JCO 2011

Neoadjuvant Therapy (NAT):Potential Advantages
Improved Tumor Downstaging Inoperable Operable Mastectomy BCS
Provides in vivo assessment of anti-tumor effects
Provides opportunity to assess surrogate biological endpoints
Early initiation of systemic therapy
Inhibition of post-surgical growth spurt
May expedite new drug development
no
pCR and Treatment Outcome
pCR is a robust measure of therapeutic effects and surrogate a DFS in responder
Increase pCR rate should correspond to improved efficacy in the overall patient population
Prediction of pCR should predict for benefit and allow for tailoring treatment to indivudual tumor characteristics
no
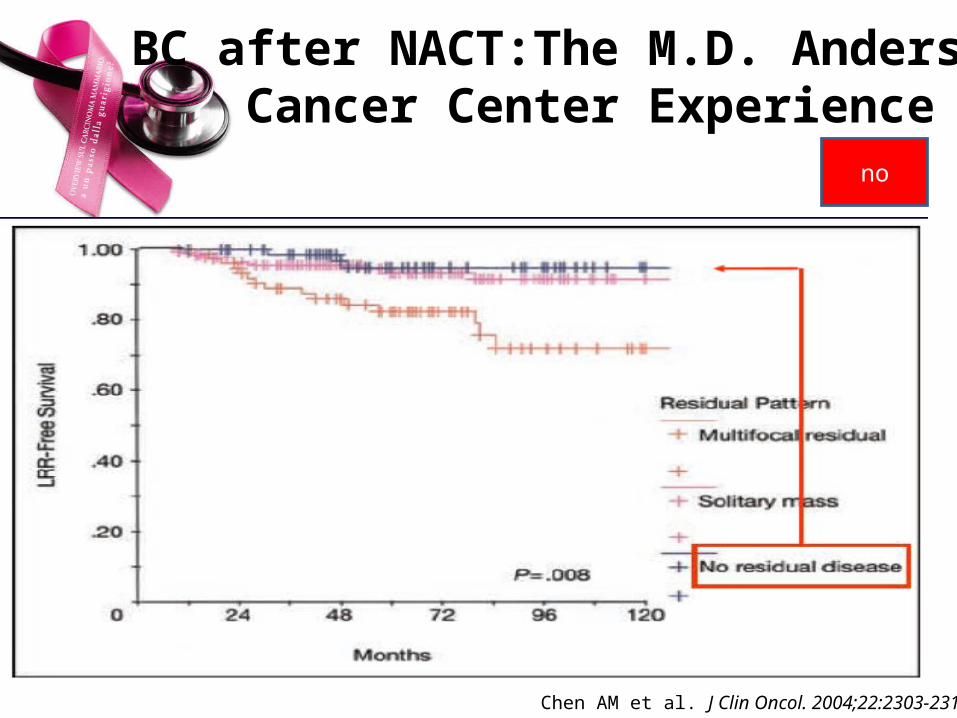
BC after NACT:The M.D. Anderson Cancer Center Experience
Chen AM et al. J Clin Oncol. 2004;22:2303-2312.
no
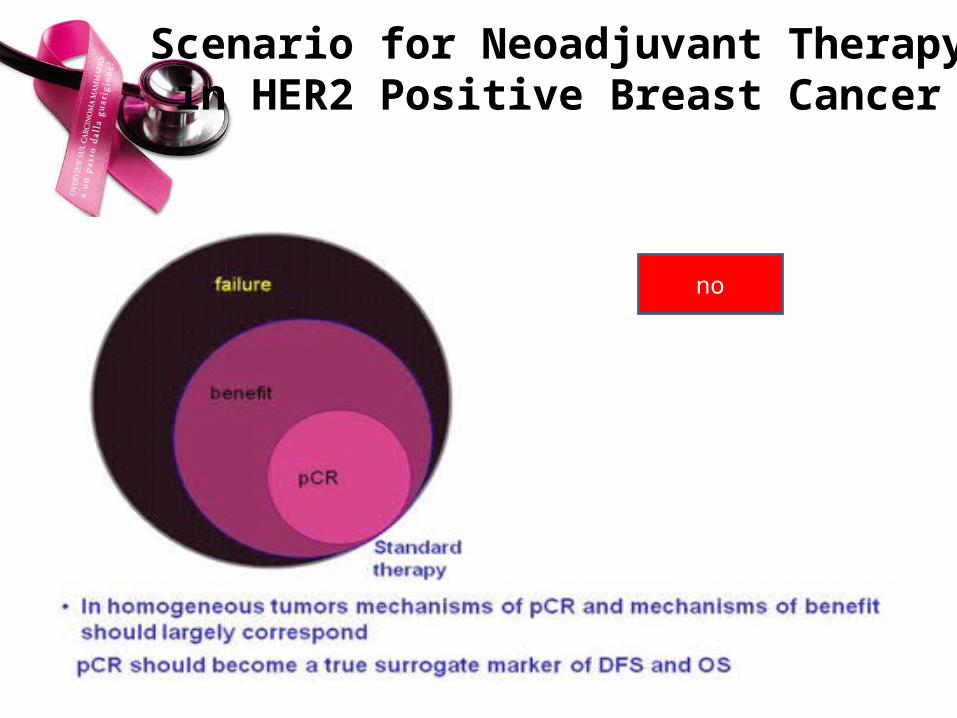
Scenario for Neoadjuvant Therapy in HER2 Positive Breast Cancer
no

Trastuzumab in NACT – pCR
T-FEC T-FEC + H
pCR 26.3 % 66.7 %
pCR ER pos 27 % 61 %
pCR ER neg 25 % 70 %
pN0 78.9 % 90.3 %
Buzdar AU et al, PASCO 2004 ; Clin Cancer Res 2007
Study closed after first 42 pts due to the strong advantage for H combination H stopped at the end of NACT (6 months)
no
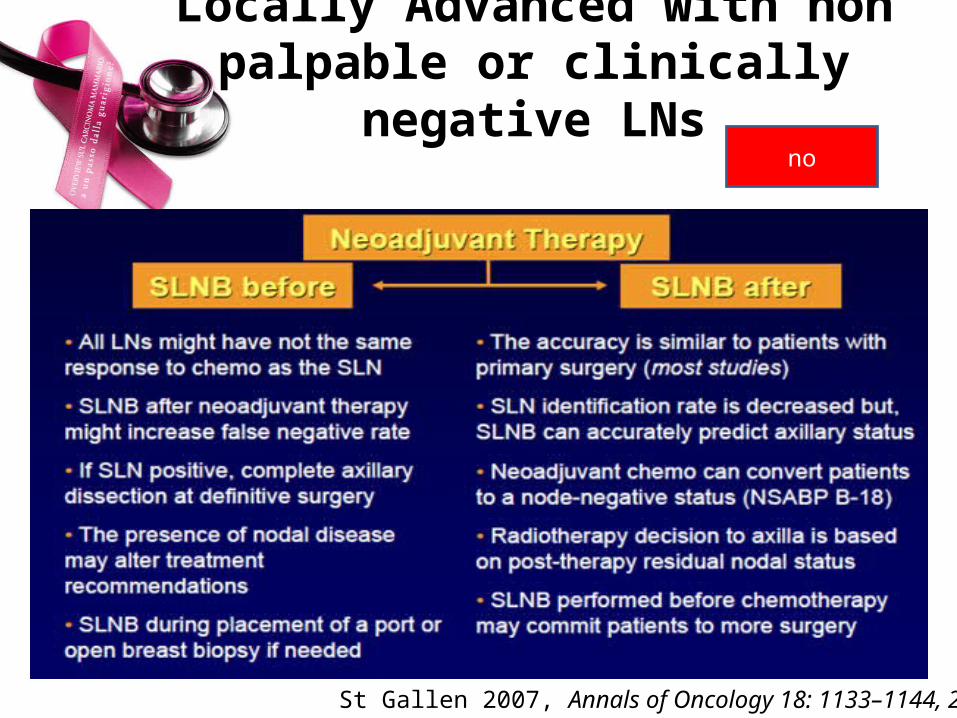
Locally Advanced with non palpable or clinically negative LNs
no
St Gallen 2007, Annals of Oncology 18: 1133–1144, 2007

Sentinel Lymph Node Biopsy in BC patients Treated With NACT
Pecha V. et al. Cancer 2011
no
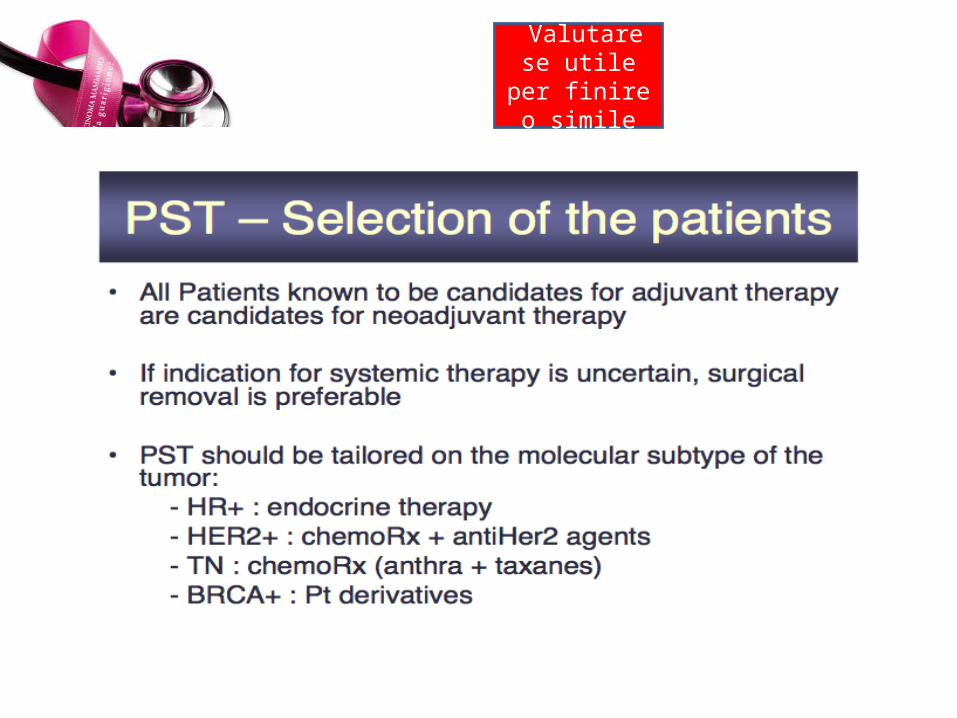
Valutare se utile per finire
o simile
Timing of SLNB
Hunt KK, et al. Ann Surg. 2009;250(4):558-566
Vedere il lavoro di Sapino e mettere lo schema interessante

PET and Neoadjuvant Chemotherapy

…Open Question in Clinical Practice…?
?