Embed Size (px)
Citation preview

LA MALATTIA MINIMA RESIDUA NELLA
LEUCEMIA ACUTA MIELOIDE
Francesco Lo-Coco Università Tor Vergata, Roma
Progetto di Formazione Nazionale SIE Napoli, 25 Ottobre 2018

Disclosures
Norelevantconflictsofinteresttodeclare ResearchSupport/P.I.
Employee Norelevantconflictsofinteresttodeclare
Norelevantconflictsofinteresttodeclare Stockholder
Consultant Teva,Orsenix
AdvisoryBoard Novar5s,Teva,Orsenix
SpeakersBureau Novar5s,Teva
Other(Specify) Norelevantconflictsofinteresttodeclare

• Advancedmedianage(70yrs)• Currenttherapypoorlytoleratedinelderly• Dismalprognosis(50-80%relapserate)
• Targetedtherapystronglyneeded
AcuteMyeloidLeukemia

Age CR% ED% Cure%
<15 90 <5 >60
<60 75 <10 45
>60 50 ~20 <15
AMLTreatmentOutcome

Gene=cheterogeneityofAML
Dohner et al, European LeukemiaNet, 2017

HeterogeneityofNKAML
Schlenk et al. N Engl J Med 2008

Muta=onalpaDerninAMLbyWGS
The Cancer Genome Atlas Research Network. N Engl J Med 2013

MolecularComplexityofAMLasdefinedbyNGS:Implica=onsforTreatment
• Inhibitorsagainstonetargetwillnotsuppressallleukemogenicclones
• ClearingallmutaUonsincreasesoverallsurvival
Patel, et. al. NEJM 2012

ComprehensiveprognosisassessmentinAML
• Pre-treatment prognostic factors • Karyotype • Molecular genetics • Clinical parameters
• Post-treatment prognostic factors • MRD detection
• Flow-cytometry • Molecular biology

Prognos=cfactorsinAMLandtypeoffailure
Characteristic Unfavorable
category Early death
Death during
remission Resistance/
Relapse Age Older × × Performance status >2 × × Comorbidities increasing × × Previous HD/t-AML Yes × Cytogenetics Unfavorable × Mutational status* FLT3-ITD; KMT2A × WBC count Hyperleucocytosis × × Quality of response MRD+ × *Other mutations have been recently added : RUNX1, ASXL1, TP53

CanMRDimproveoutcomedetermina=oninAML?
Thismodalitymaynotonlycapturedifferencesintreatmentresponsethatreflecttheunderlyingmolecularheterogeneity,butalsointer-
pa=entvariabilityindrugavailabilityandmetabolism,whichmayalsosignificantlyinfluenceoutcome
10 12
10 10
10 8
10 6
10 4
10 2
10 0
Time
No.
of l
euke
mic
cel
ls
Relapse
Cure
CR
MRD
Grimwade, Best Pract Hematol 2012

Hourigan, et al, Nature Reviews Clinical Oncology 2013
Measurable Residual Disease
Differences according to ! disease type ! drug availability ! individual metabolism
NGS: ! Clonal heterogeneity and evolution
dD-PCR
QRT-PCR

Ding L, et al. Nature 2012
ClonalHeterogeneityandClonalEvolu=on
-> one subclone within the founding clone evolved to become the dominant clone at relapse by acquiring additional mutations

Technical Platforms for MRD detection in AML
! PCR, RT-PCR
! RQ-PCR
! Digital PCR
! NGS
! Flow cytometry

MRDdetec=oninAML:PCRvsMPFC
PRO CONTRA SENSITIVITY APPLICABILITY
Flow(MPFC)
1. Fast,lessexpensive
2. Singlecellanalysis3. Cellviability
1. Lessleukemiaspecific2. Subclonesexpansion3. Phenotypicshi\4. Complexanalysis
104-105 Wide(>90%)
PCR/RQ-PCR
1. HighDNAstability2. Specific3. Verylow
backgroundinnormalcells
4. QuanUtaUon
1. Timeconsuming,expensive
2. FalseposiUve3. RNAinstability(sample
quality)4. Cellviabilitynot
determinable
104-106 Specificsubgroups:(~60%)
CBF-AML,NPM1mutWT1
Modified from Buccisano, CCO 2009

E2A/PBX1
MLL/AF4
BCR/ABL
TEL/AML1
PML/RARα
SIL/TAL
CBFb/MYH11
RUNX1/ RUNX1T1
Standardiza=onofQ-PCRforfusiontranscripts
Gabert et al., Leukemia 2003

• NPM1
• RUNX1
• ASXL1
• MLL-PTD
• CEBPA ?
• FLT3 ?
• DNMT3a ?
MoleculartargetsforMRDinAML
• PML-RARA
• CBFB-MYH11
• RUNX1-RUNX1T1
• MLL-fusion partner
• DEK-NUP214
• BCR-ABL
• Others
• WT1
• BAALC
• ERG
• MN1
Fusion genes Mutations Overexpression

MRDdetermina=oninCBF-AMLpredictsrelapse
• Upfront genetics and MRD determination in CBF acute myeloid leukemia. • 198 patients • RQ-PCR transcripts determination after first consolidation • a less than 3-log MRD reduction or a level <0.1% was associated with
a higher specific hazard of relapse
Jourdan et al, Blood 2013

RecurrentTransloca=ons:t(8;21)(RUNX1-RUNX1T1)CBF2006trial,n=94pts
Willekens et al, Haematologica 2016
! MRD>0.001%consideredposiUve! BMpersistently+at2yrsin8%ofpt! PBattheendofconsolidaUonpredicUve,anUcipaUngrelapse
by4mos! Duringfollow-up:100%relapserateinBM>500copies,PB>100copies! RisingMRDlevelsaccuratelypredict
relapse(AML-MRC15,LiuYin,Blood2012)
CIR OS
BM
PB

Kronke et al, JCO 2009
RQ-PCRforNPM1mut:impactofMRDonsurvival

NPM1muta=onsMRDbyRQ-PCRinPBa\er2CyclesofCHT
ThepresenceofMRDbyquan=ta=onofNPM1-mutatedtranscriptsprovidedpowerfulprognos=cinforma=onindependentofotherriskfactors.
Ivey A et al., NEJM 2016
Overall Survival Cumulative incidence of relapse

MRDasaPredictorofOutcomeinDevelopmentandValida=onCohorts
Ivey A et al, NEJM 2016

NPM1mutisastablemarker,DNMT3AmutandFLT3ITDarenot
Ottone et al, Am J Hematol 2018

1
10
100
1000
10000
100000
1 2 3 4
NPM1
DNMT3A
• Texto1
! Texto21
10
100
1000
10000
100000
Esordio Induz ione P ostc ons
NPM1
DNMT3A
1
10
100
1000
10000
100000
E sor dio Induzione Postcons
NPM1
DNMT 3A
UPN_243
UPN_277
UPN_82
0,1
1
10
100
1000
10000
100000
Esordio Induzione Post cons Relapse
NPM1
DNMT3A
UPN_43
Relapsed Relapsed
ParalelMRDassessmentofDNMT3AandNPM1

ClonalHematopoiesisandBlood-CancerRiskInferredfromBloodDNASequence
Giulio Genovese, Ph.D., Anna K. Kähler, Ph.D., Robert E. Handsaker, B.S., Johan Lindberg, Ph.D., Samuel A. Rose, B.S., Samuel F. Bakhoum, M.D., Ph.D., Kimberly
Chambert, M.S., Eran Mick, B.S., Benjamin M. Neale, Ph.D., Menachem Fromer, Ph.D., Shaun M. Purcell, Ph.D., Oscar Svantesson, M.S., Mikael
Landén, Ph.D., Martin Höglund, M.D., Ph.D., Sören Lehmann, M.D., Ph.D., Stacey B. Gabriel, Ph.D., Jennifer L. Moran, Ph.D., Eric S. Lander, Ph.D., Patrick F.
Sullivan, M.D., Pamela Sklar, M.D., Ph.D., Henrik Grönberg, M.D., Ph.D., Christina M. Hultman, Ph.D., and Steven A. McCarroll, Ph.D.
N Engl J Med Volume 371(26):2477-2487
December 25, 2014
Weanalyzeddatafromwhole-exomesequencingofDNAinperipheral-bloodcellsfrom12,380persons,unselectedforcancerorhematologicphenotypes.

Clonalhematopoiesiswithsoma=cmuta=onsin:
• DNMT3A,ASXL1,andTET2,genesimplicatedinhematologiccancers.
• Riskofhematologiccancerincreasedintheseindividuals
Genovese G, Jaiswal G, et al. N Engl J Med 2014
NGSandClonalhematopoiesis(CHIP)

UPN Karyotype FLT3-ITD NPM1 Karyotype FLT3-ITD NPM1 routine RT-PCR
routine RT-PCR
104 46,XY negative positive 46,XY positive positive 213 46,XX negative positive 46,XX positive positive 241 46,XX negative positive 46,XX positive positive
DIAGNOSIS RELAPSE
FLT3-ITD patient-specific RQ-PCR
UPN FLT3-ITD FLT3-ITD/ABLx104 routine RT-PCR RQ-PCR
104 negative 82.00 213 negative 37.98 241 negative 1719.21
Exon 14 Exon 15 ITD
Primer forward Patients specific
Primer reverse
Probe
Clonal evolution of FLT3-ITD mutations in AML

Iden=fica=onofan=gensassociatedwithFLT3-ITD(MPFCanalysisoftotalBMcellsfromFLT3-ITDmutpts)
*Pearson's chi-squared test
Antigen FLT3 mutated FLT3 wt p value* (% of pts/tot) (% of pts/tot)
CD99 73% (27/37) 48% (44/91) 0.02
CD123 100% (38/38) 83% (75/90) 0.02
CD11b 92% (35/38) 66% (59/90) 0.004
CD7 68% (26/38) 46% (41/89) 0.003
CD25 87% (33/38) 40% (36/90) 0.000003
Battistini, Ottone et al, Clin Cancer Res 2015

Athresholdof11.7%cellsstainingposi=veforthisan=genicprofilepredictsFLT3
mutwithspecificityandsensi=vity>90%
ReceiverOpera=ngCharacteris=c(ROC)curve
analysis
Battistini, Ottone et al, Clin Cancer Res 2015

ITD-mutations Exons 14/15
Suitability of alterations for MRD detection
Preleukemic Leukemic Post-Onset Drivers
FLT3-ITD FLT3-TKD RAS PTPN11 KIT
DNMT3A TET2 IDH1/2 SF3B1
NPM1 Translocations RUNX1 CEBPA
Sensitive Potentially unspecific
Specific Lost in 10-90%
Sensitive specific
by courtesy of C. Thiede

Are MRD studies still valuable and cost effective in APL ?


J Clin Oncol 2003

MRDtodirectpre-emp=vetreatmentinAPL
Lo-Coco et al. Blood, 1999 Esteve et al. Leukemia, 2006
0 1 2 3 4 5 6 7 8
Years
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pro
babi
lity
Hematological relapse (n=33; 24 events)
Molecular failure (n=16; 5 events)
p=0.008
0 1 2 3 4 5 6 7 8
Years
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pro
babi
lity
Hematological relapse (n=33; 24 events)
Molecular failure (n=16; 5 events)
p=0.008

Grimwade et al, JCO 2009
Pre-emptive ATO therapy
MRCAML-15TrialforNewlyDiagnosedAPL

Cicconietal,Leukemia2016
Diagnosis
Post-induc=on
PostIIIconsolida=on
Kine=csofPML/RARaclearanceinAPL0406
PML/RARA +ve patients by RQ-PCR

PrimaryEndpoint:Rateofmolecularcompleteremission
SecondaryEndpoints: 2yearEFS,Safety,QoL
ORH-2014 in APL: Pivotal Registration Study A Randomized, Multi-center, Phase III Study to Compare
ORH-2014 and i.v. ATO in Low-Intermediate Risk APL
Agreement with FDA on study design, population, and endpoints

ATRA-CHTATRA-ATOWT1FLT3 -ITDDNMT3AETV6FLT3-TKDTET2ASXL1JAK2RUNX1SRSF2TP53U2AF1PMLRARA
single mutation
wild-type
multiple mutations
not analysed
Muta=onalpaDerninrelapsedAPL

PMLandRARAmuta=onsatrelapse
B2 LBD PML RARA
A216V (2)
A216T
(1)
L224I
(1)
T291A (1)
T285I
(1)
C235F (1)
F286del (1)
R272Q (1)
I222_D223insE (1)
W225C (1)
S287L
(1)
B2 PML
A216V (2)
A216T
(1)
E224G (1)
L220P (1)
L290V (1)
Madan et al, Leukemia 2016
Iaccarino et al, BJH 2016 Zhu et al, NEJM 2014
Lehmann-Che et al, NEJM 2014 Goto et al, Blood 2011

Earlyandsensi=vedetec=onofPMLA216VbyddPCR
posiUvebyddPCR
posiUvebySanger
negaUvebyddPCR
negaUvebySanger

41
• WT1overexpressedin>90%AMLs
• Suitable“universal”MRDmarkerforAML• ComparisonofsensiUvity&specifiUyof9differentRQ-PCRassaysby11Europeanlabs(LeukemiaNet)
Op=mizedRQ-PCRofWT1(Cillonietal,JCO2009)

1
10
100
1000
10000
100000
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
Normal range (<20 copies/104 copies of ABL)
WT1levelinPBofAMLpa=entsattheendoftheinduc=ontherapypredictsforrelapse
Cilloni et al, Haematologica 2008

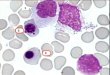
GlobalimmunophenotypicapproachtoAML
Multiple staining at diagnosis
Identification of “leukemia-associated” phenotypes
Definition of a patient’s “immunologic fingerprint”
Immunologic fingerprint used during follow-up
Venditti, Blood 2000; Venditti, Leukemia 2003; Buccisano, Leukemia 2006; Maurillo, JCO 2008; Buccisano, Blood 2010

Leukemia-associatedImmunophenotypes
LAIPtype Examples
Asynchronousan=genexpression
CD34+CD14+CD34+CD15+CD33+
Lackofan=genexpressionCD34+CD13-CD33+Hla-DR-CD34+CD13+
Cross-lineagean=genexpression
CD34+CD13+CD19+
CD34+CD13+CD2+
An=genoverexpression
HLA-DR++CD34+++CD13++
CD64++CD4++CD45++
Average3LAIPperpa=ent
• 85%ofpediatricAML
• 80-95%ofadultAML
Pitfalls: immunophenotypic shifts, complex analysis

Laboratory diagnostics of hematological malignancies has three major applications:
• Diagnosis • Prognostic (sub)classification • Evaluation of treatment effectiveness via detection of MRD
MPFC

MRDAssessmentbyFlowCytometryinAML
Terwijn M et al, JCO 2013

AML02:Aprospec=ve,mul=centerstudyofrisk/MRD-directedtherapy
• LevelsofMRDwereusedtoallocateGOandtodeterminetheUmingofinducUon2
• BothMRDandgeneUcabnormaliUesatdiagnosiswereusedtodeterminethefinalriskclassificaUon
SR (with donor)
HR
Enrollment, Randomization, Initial Risk Assignment
H-ADE ADE ± GO
Final Risk Assignment
SCT
CI CII CIII
ADE
MRD MRD
LR SR (w/o donor)
SR (with donor)
HR
Rubnitz et al, Lancet Oncology 2010

AML02:Mainconclusions
71% ± 4%OS
63% ± 4% EFS
00.10.20.30.40.50.60.70.80.9
1
0 1 2 3 4 5 6 7
19% ± 3%
Years on Study
9% ± 2%
Relapse
Death
• Risk- and MRD-adapted therapy resulted in 71% OS • Day 22 MRD >1% significantly associated with worse OS, EFS, CIR
N=230 CR rate 94% MDR+ 37% (Ind1) MDR+ 20% (Ind2) St. Jude AML Trials
(Rubnitz et al, Lancet Oncology 2010

IntegratedRisk-Score(TorVergata)
Low-Risk High-Risk
Favorable K / MRD-
Int K / MRD-
Adverse K FLT3+ Good K / MRD+
Int K / MRD+
Buccisano et. al. Blood 2010

GIMEMAAML1310:astudyofrisk-adaptedandMRD-directedtherapyforadultAML
Low-risk: CBF/Kitwt; NPM1+/FLT3- Int-risk: all others High-risk: Adverse K; FLT3+
Diagnosis
Low-risk
Int-risk
High-risk
MRD-
MRD+
MRD marker LAIP Risk stratif
CG, molecular MRD assess
LAIP
FLA-Ida salvage No CR CR
CR In
duct
ion
(1 o
r 2 c
ours
es)
Con
solid
atio
n 1
autoSCT
alloSCT
alloSCT: MRD, MUD, UCB, HRD

GIMEMA AML1310
342 post consolidation
177 candidates to AutoSCT
110 (62%) received AutoSCT
165 candidates to AlloSCT
110 (67%) received AlloSCT
81 not in CR post induction
23 (CR post salvage) candidates to
AlloSCT
16 (70%) received AlloSCT
AML1310: results

GIMEMA AML1310
52
AML1310: intermediate-risk OS and DFS by MRD status
Venditti A et al, submitted

Responseto
therapy
CRMRD-asanewresponsecriterion
MolecularMRD:ELN2017recommenda=onsforAML
Transcripts
-NPM1-RUNX1-RUNX1T1-CBFB-MYH11-PML-RARA
When
-aoer2cyclesofstandardinduc=on/consolida=on-aoertheendoftreatment-every3monthsfor24monthsaoerendoftreatment
ModifiedfromSchuurhuisGJ,etalELN-MRDWP,Blood2018
Source
-inPBandBMorPBevery4-6weeks
! PBinsteadofBM?Inpar=cularatprolongedfollow-up?! Absolutecopynumbersshouldalsobereported
Defini=onoffailure
-FailuretoachieveMRD-nega=veCR(molecularresistance)-RisingMRDlevels(>1Log)duringoraoertherapy(molecularprogression)-Molecularrelapse

Clinical Impact of MRD in AML is Increasingly Recognized

Anetworkoflaboratorieslicencedforthe
moleculardiagnosisofAML
Aimingatdefiningandspreadingdiagnos=c
standardsforAML,includingmoleculargene=cs,
cytogene=cs,andimmunophenotype
Researchprojects
LabnetAML

Diagnos=caLAM:PannelloBase
Cario=po • G-banding
QRT-PCRQ-LAMP
• PML/RARA(bcr1-2ebcr3)
• BCR/ABL(p190ep210)
• RUNX1/RUNX1T1• CBFb/MYH11
PCR-ECPCR-RLFP
• FLT3-ITD• FLT3-D835eI836• NPM1
Tempi
15gg
24ore
72-96ore
72-96ore

ProssimiStep:PannelloAvanzato
!

Risulta=StandardizzazioneMRD
BCR-ABL p190
BCR-ABL p210 b3a2
PML-RARA bcr1
PML-RARA bcr3
CBFb/MYH11 type A
RUNX1/RUNX1T1
NPM1
Undiluited
10-2
10-3
10-1

Conclusive remarks (I)
• NGS may provide in the future more comprehensive data on clonal heterogeneity / evolution and overall effects of treatments
• MRD assessment by MPFC / RQ-PCR allows better strategies for delivering treatment in AML
• RQ-PCR provides valuable prognostic information in CBF and NPM1 +ve AML

Conclusive remarks (II)
• MRD –ve remission as a new treatment objective in AML to accelerate drug approval
• Importance of reference laboratories

TorVergataTeam
LauraCicconi MariadomenicaDivonaTizianaOpone SerenaLavorgnaEmilianoFabiani GiuliaFalconiNélidaI.Noguera ValenUnaAlfonsoSerenaTravaglini LiciaIaccarino
AdrianoVendir FrancescoBuccisano
MariaTeresaVoso