Embed Size (px)
DESCRIPTION
terapi gbs
Citation preview

Management ofManagement ofGuillainGuillain--Barre Barre SyndromeSyndrome
Peter LinR3 Neurology Resident

GuillainGuillain--Barre Barre SyndromeSyndromenn First described in 1916 byFirst described in 1916 by Guillain Guillain,, Barre Barre, and, and Strohl Strohl
nn Characterized by rapidly ascending paralysis,Characterized by rapidly ascending paralysis,hyporeflexia hyporeflexia and CSFand CSF cytoalbuminologic cytoalbuminologic dissociationdissociation
nn Pathology studies showedPathology studies showed demyelination demyelination andandmononuclear infiltration in nerve rootsmononuclear infiltration in nerve roots
nn Thought to be acuteThought to be acute demyelinating demyelinating neuropathyneuropathy
nn Clinical spectrum has expanded over last decade toClinical spectrum has expanded over last decade toinclude a wide range of variantsinclude a wide range of variants

EpidemiologyEpidemiologynn Most common cause of acquired generalized paralysisMost common cause of acquired generalized paralysisnn 1-4 per 100,000 per year 1-4 per 100,000 per yearnn All ages are affected All ages are affectednn Slight male preponderance Slight male preponderancenn Mean age of occurrence 40 Mean age of occurrence 40nn Mortality fallen from 33% to < 5% with ICU care Mortality fallen from 33% to < 5% with ICU carenn Most common causes of death are ARDS, sepsis, Most common causes of death are ARDS, sepsis,dysautonomiadysautonomiann Presentations vary depending on countryPresentations vary depending on country

TriggersTriggersnn 60-70% of cases preceded by a trigger infection such as60-70% of cases preceded by a trigger infection such as
gastroenteritis or URIgastroenteritis or URI
nn Trigger event precedes symptoms by 1-3 weeksTrigger event precedes symptoms by 1-3 weeks
nn Typically, viral upper respiratory infectionsTypically, viral upper respiratory infections
nn Certain pathogens predominate as triggersCertain pathogens predominate as triggersnn C. C. jejunijejuninn CMVCMVnn EBVEBVnn MycoplasmaMycoplasma

Other associated triggersOther associated triggersnn VaccinationsVaccinations
nn SurgerySurgery
nn Cancer (HodgkinCancer (Hodgkin’’s disease)s disease)
nn PregnancyPregnancy
nn 1/3 of patients have no preceding illness1/3 of patients have no preceding illness

PathogenesisPathogenesisnn Initially thought to be caused by an immune attack onInitially thought to be caused by an immune attack on
myelinmyelin
nn Peripheral nerve histology shows Peripheral nerve histology shows endoneurialendoneurialperivascular monocyte perivascular monocyte infiltration and infiltration and multifocalmultifocaldemyelinationdemyelination
nn Nerves may be affected at all levels from roots to distalNerves may be affected at all levels from roots to distalnerve endings (nerve endings (polyradiculoneuropathypolyradiculoneuropathy))
nn A similar disease can be induced in animals byA similar disease can be induced in animals byimmunization with nerve preparations enriched inimmunization with nerve preparations enriched inmyelin (Experimental autoimmune neuritis)myelin (Experimental autoimmune neuritis)

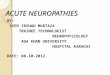
Immune injury in AIDPImmune injury in AIDP
Bosch and Smith, from NICP, 3rd edition

PathogenesisPathogenesisnn Immune theoriesImmune theories
nn Molecular mimicry of microbial structures andMolecular mimicry of microbial structures and gangliosides gangliosidesnn Humoral Humoral factors (antibodies tofactors (antibodies to gangliosides gangliosides))nn Cell-mediated responses (Macrophage activation)Cell-mediated responses (Macrophage activation)
nn Further characterizations of variants showed that thereFurther characterizations of variants showed that thereare are demyelinating demyelinating and axonal variants of GBSand axonal variants of GBS
nn Result from immune-mediated processes directedResult from immune-mediated processes directedagainst different antigensagainst different antigens
nn A large number of reports have reported antibodies toA large number of reports have reported antibodies toglycolipidsglycolipids, including GM1, GQ1b, various other, including GM1, GQ1b, various othergangliosidesgangliosides, all components of the axonal membrane, all components of the axonal membrane

Clinical presentationClinical presentation
nn Paresthesias Paresthesias and pain usually are first symptomsand pain usually are first symptomsnn PainPain
nn Usually a deep aching pain in lower back, may radiate toUsually a deep aching pain in lower back, may radiate tobuttocks, thighs, calvesbuttocks, thighs, calves
nn May complain of burning, tingling, shock-like sensationsMay complain of burning, tingling, shock-like sensationsnn WeaknessWeakness
nn Follows sensory symptoms, beginning typically in legs andFollows sensory symptoms, beginning typically in legs andascending to armsascending to arms
nn 10% begin with arm weakness10% begin with arm weaknessnn Rarely weakness begins in face (cervical-pharyngeal-brachial)Rarely weakness begins in face (cervical-pharyngeal-brachial)nn Facial weakness occurs in at least 50% of patients and is usuallyFacial weakness occurs in at least 50% of patients and is usually
bilateralbilateralnn ReflexesReflexes
nn Absent or depressed in virtually all casesAbsent or depressed in virtually all cases

Clinical findingsClinical findingsnn Eye movement abnormalitiesEye movement abnormalities
nn Oculomotor Oculomotor paresis in 15% of patientsparesis in 15% of patientsnn Ptosis Ptosis andand pupillary pupillary abnormalities can be seenabnormalities can be seen
nn Sensory lossSensory lossnn VariableVariablenn May be minimal or have severe kinesthetic lossMay be minimal or have severe kinesthetic lossnn Panmodality Panmodality sensory loss in stocking-glove is typicalsensory loss in stocking-glove is typical
nn Autonomic dysfunctionAutonomic dysfunctionnn More frequent in severely affected patientsMore frequent in severely affected patientsnn 65% of patients had65% of patients had dysautonomia dysautonomia in some studiesin some studiesnn Blood pressureBlood pressure lability labilitynn Cardiac arrhythmiasCardiac arrhythmiasnn Urinary retentionUrinary retentionnn ConstipationConstipation

Clinical courseClinical coursenn Disease progresses for days to 4 weeksDisease progresses for days to 4 weeksnn Typical course (90% of patients) is steady progression toTypical course (90% of patients) is steady progression to
nadir within 3 weeks from onset of nadir within 3 weeks from onset of paresthesiasparesthesiasnn Plateau phase ranges from days to 6 monthsPlateau phase ranges from days to 6 monthsnn Occasional patients will have stuttering or stepwiseOccasional patients will have stuttering or stepwise
coursecoursenn Comprises variants which have unifying features ofComprises variants which have unifying features of
clinical time course, CSF and clinical time course, CSF and electrodiagnostic electrodiagnostic findings,findings,and antecedent triggersand antecedent triggers

Clinical-pathologic spectrumClinical-pathologic spectrumnn Acute inflammatory Acute inflammatory demyelinatingdemyelinating
polyradiculoneuropathy polyradiculoneuropathy (AIDP)(AIDP)
nn Axonal variantsAxonal variantsnn Acute Motor Axonal Neuropathy (AMAN)Acute Motor Axonal Neuropathy (AMAN)nn Acute Motor Sensory Axonal Neuropathy (AMSAN)Acute Motor Sensory Axonal Neuropathy (AMSAN)
nn Without predominant weaknessWithout predominant weaknessnn Acute Acute pandysautonomiapandysautonomiann Pure sensory neuropathyPure sensory neuropathynn Miller-Fisher syndromeMiller-Fisher syndrome

GuillainGuillain--Barre Barre MimicsMimics
nn Transverse Transverse myelitismyelitisnn Myasthenia GravisMyasthenia Gravisnn Vasculitic Vasculitic neuropathyneuropathynn Porphyric Porphyric neuropathyneuropathynn Toxic neuropathies (thallium, arsenic, hexane)Toxic neuropathies (thallium, arsenic, hexane)nn Tick paralysisTick paralysisnn Inflammatory Inflammatory meningoradiculopathies meningoradiculopathies ((LymeLyme’’ss,,
CMV, HIV)CMV, HIV)

Lumbar punctureLumbar puncturenn CSFCSF
nn Classically, Classically, albuminocytologic albuminocytologic dissociationdissociationnn 90% of patients demonstrate protein elevation90% of patients demonstrate protein elevation
without without leukocytosis leukocytosis at time of maximal weaknessat time of maximal weaknessnn Normal cell counts and increased proteinNormal cell counts and increased proteinnn 5% of patients have 5% of patients have pleocytosis pleocytosis of 10-20 cellsof 10-20 cellsnn Abnormal findings level off after 1 monthAbnormal findings level off after 1 monthnn Pleocytosis Pleocytosis > 20 associated with HIV, > 20 associated with HIV, LymeLyme’’ssnn May be normal early on < 7 days, or in GBS variantsMay be normal early on < 7 days, or in GBS variants

Serum TestsSerum Testsnn Usually not helpfulUsually not helpful
nn LFTLFT’’s s may be abnormal in coexisting hepatitismay be abnormal in coexisting hepatitis
nn CK may be elevated in patients with severe painCK may be elevated in patients with severe pain
nn Hyponatremia Hyponatremia may occur due to SIADHmay occur due to SIADH

AntibodiesAntibodies
nn Measurement of antibodies is not common practiceMeasurement of antibodies is not common practicenn May have implications for prognosisMay have implications for prognosisnn GM1 is associated with a severe pure motor variantGM1 is associated with a severe pure motor variantnn GM1b associated with GM1b associated with C. C. jejunijejuni - severe progression- severe progressionnn GQ1b - Miller Fisher VariantGQ1b - Miller Fisher Variantnn Does not change therapeutic approachDoes not change therapeutic approachnn Correlation of antibodies with variants and clinicalCorrelation of antibodies with variants and clinical
courses is ongoingcourses is ongoing

MRIMRInn MRI of brain is normalMRI of brain is normalnn Cranial nerve enhancement with gad has beenCranial nerve enhancement with gad has been
seenseennn Enhancement of spinal roots, Enhancement of spinal roots, conusconus, , caudacauda
equina equina has been reported in severe caseshas been reported in severe casesnn Findings are nonspecific and are not helpful inFindings are nonspecific and are not helpful in
confirming diagnosisconfirming diagnosisnn Rare patients with predominantly lower limbRare patients with predominantly lower limb
involvement may benefit to rule outinvolvement may benefit to rule outcompressive cord lesioncompressive cord lesion

ElectrodiagnosisElectrodiagnosisnn Most sensitive test in evaluating GBSMost sensitive test in evaluating GBSnn Patterns:Patterns:
nn Motor conduction blockMotor conduction blocknn Prolonged distal latenciesProlonged distal latenciesnn Temporal dispersionTemporal dispersionnn Slowing of nerve conductionSlowing of nerve conductionnn Increased F-wave latencyIncreased F-wave latencynn Operator-dependentOperator-dependentnn Depends on variant (Depends on variant (demyelinating demyelinating vs. axonal)vs. axonal)nn Normal NCV after several days of symptoms inNormal NCV after several days of symptoms in
setting of severe weakness makes diagnosis unlikelysetting of severe weakness makes diagnosis unlikely

Goals of TreatmentGoals of Treatment
nn To reduce the inflammatory attack earlyTo reduce the inflammatory attack earlynn ImmunomodulationImmunomodulation
nn Reduce morbidityReduce morbiditynn Disease relatedDisease relatednn Secondary complicationsSecondary complications
nn Improve final outcomeImprove final outcome

Treatment OptionsTreatment Options
nn PlasmapheresisPlasmapheresis
nn IVIgIVIg
nn CSF FiltrationCSF Filtration
nn SteroidsSteroids

Clinical TrialsClinical Trialsnn Most trials examined those unable to ambulateMost trials examined those unable to ambulate
unaided or with respiratory progressionunaided or with respiratory progressionnn EndpointsEndpoints
nn Time to onset of motor recoveryTime to onset of motor recoverynn Duration of time for mechanical ventilationDuration of time for mechanical ventilationnn Hughes Disability Scale at 1 month, 6 months, 1 yearHughes Disability Scale at 1 month, 6 months, 1 year
nn 0 = normal to 6 = deceased with 3 = able to walk 5 meters0 = normal to 6 = deceased with 3 = able to walk 5 meterswith walker or supportwith walker or support
nn Many studies randomized only patients unable to walkMany studies randomized only patients unable to walkindependently Hughes > 3 referred to as moderateindependently Hughes > 3 referred to as moderate
nn Mean improvement at 4 weeks was main primary outcome Mean improvement at 4 weeks was main primary outcomemeasure for most major trialsmeasure for most major trials

Plasma Exchange TrialsPlasma Exchange Trialsnn Evidence suggesting that circulatingEvidence suggesting that circulating humoral humoral factorsfactors
inducedinduced demyelination demyelination led to study of led to study of plasmapheresisplasmapheresisnn The first treatment shown to be beneficialThe first treatment shown to be beneficialnn North American (North American (GuillainGuillain--BarreBarre Study Group, Study Group, NeurologyNeurology,,
1985)1985)nn 245 patients treated within first 2 weeks with severe245 patients treated within first 2 weeks with severenn FindingsFindings
nn Improvement in function at 4 weeksImprovement in function at 4 weeksnn Decreased time to improve one clinical gradeDecreased time to improve one clinical gradenn Decreased time to independent walking (53 vs. 85 days)Decreased time to independent walking (53 vs. 85 days)nn Improved outcome at 6 monthsImproved outcome at 6 monthsnn Decreased number of days on ventilator (24 vs. 48 days)Decreased number of days on ventilator (24 vs. 48 days)

Plasma Exchange TrialsPlasma Exchange Trialsnn French Cooperative Group (French Cooperative Group (AnnAnn Neurol Neurol, 1987), 1987)
nn 220 patients220 patientsnn Findings:Findings:
nn Decreased number of days to walk with assistanceDecreased number of days to walk with assistancenn 71% full recover at 1 year follow-up vs. 52% supportive71% full recover at 1 year follow-up vs. 52% supportive
nn Second French study 1997Second French study 1997nn 556 patients556 patientsnn Studied PE in mild patients (able to walk but not run)Studied PE in mild patients (able to walk but not run)nn Concluded that mild patients benefited from 2 exchangesConcluded that mild patients benefited from 2 exchangesnn Moderate and severe benefited from 4 but not 6Moderate and severe benefited from 4 but not 6
nn In the 1980In the 1980’’s PE was the treatment of choices PE was the treatment of choice

Plasma Exchange ProtocolPlasma Exchange Protocolnn Standard regimen is 5 exchanges (Standard regimen is 5 exchanges (totalling totalling 200-250200-250
mLmL/kg) on alternate days/kg) on alternate days
nn Preferred replacement fluid is 5% albuminPreferred replacement fluid is 5% albumin
nn Need to monitor BP, fibrinogen, PT, PTTNeed to monitor BP, fibrinogen, PT, PTT
nn Contraindications:Contraindications:nn septic shock, recent MI, marked septic shock, recent MI, marked dysautonomia dysautonomia and activeand active
bleedingbleeding
nn Side effectsSide effectsnn Vasovagal Vasovagal reactions,reactions, hypovolemia hypovolemia, , hemolysis hemolysis from tube kinking,from tube kinking,
air air embolizationembolization, , hematomashematomasnn Anaphylactoid Anaphylactoid reactions, reactions, hypocalcemiahypocalcemia, thrombocytopenia,, thrombocytopenia,
hypothermia, hypothermia, hypokalemiahypokalemia, depletion of coagulation factors, depletion of coagulation factors

Plasma Exchange: ConsensusPlasma Exchange: Consensus
nn Optimum number of exchanges is unknownOptimum number of exchanges is unknownnn Volume of plasma removed is not knownVolume of plasma removed is not knownnn Cochrane Database Meta-analysis 2002Cochrane Database Meta-analysis 2002
nn Six eligible trials with 649 patientsSix eligible trials with 649 patientsnn ConclusionsConclusions
nn Plasmapheresis Plasmapheresis is only proven treatment and should beis only proven treatment and should becompared to as gold standardcompared to as gold standard
nn In mild GBS, 2 exchanges are superior to noneIn mild GBS, 2 exchanges are superior to nonenn In moderate GBS, 4 exchanges are superior to 2In moderate GBS, 4 exchanges are superior to 2nn In severe GBS, 6 are no better than 4In severe GBS, 6 are no better than 4nn More beneficial when started within 7 days of onsetMore beneficial when started within 7 days of onsetnn Is still beneficial in patients treated up to 30 days afterIs still beneficial in patients treated up to 30 days after

IVIgIVIgnn Prepared from pooled plasma from donorsPrepared from pooled plasma from donors
nn Contains entire array of variable region of antibodies inContains entire array of variable region of antibodies innormal serumnormal serum
nn Complex mode of actionComplex mode of actionnn Modulation of function of Fc receptorsModulation of function of Fc receptorsnn Interference with activation of complementInterference with activation of complementnn ProvidingProviding antiidiotypic antiidiotypic antibodiesantibodiesnn Modulation of functions of T and B cellsModulation of functions of T and B cells

IVIg IVIg TrialsTrialsnn Dutch trial 1992 (vanDutch trial 1992 (van der Meche der Meche, , NEJMNEJM, 1992), 1992)nn 150 GBS patients unable to walk independently150 GBS patients unable to walk independently
randomized to randomized to IVIg IVIg vs. PE within 2 weeks of onsetvs. PE within 2 weeks of onsetnn At 4 weeks more patients showed improvement withAt 4 weeks more patients showed improvement with
IVIg IVIg (53% vs. 34%)(53% vs. 34%)nn Median time to improve one grade on Hughes scale wasMedian time to improve one grade on Hughes scale was
less in less in IVIg IVIg group (27 days) vs. PE (41 days)group (27 days) vs. PE (41 days)nn CriticismsCriticisms
nn Plasma exchange group did not do as well as in North AmericanPlasma exchange group did not do as well as in North Americantrialtrial
nn Mean duration of disease prior to entry different (6 days vs. 11)Mean duration of disease prior to entry different (6 days vs. 11)nn Relapse rate in Relapse rate in IVIg IVIg treated patients was highertreated patients was higher

Plasmapheresis Plasmapheresis vs. vs. IVIgIVIgnn Plasma Exchange/Plasma Exchange/Sandoglobulin Sandoglobulin GBS Trial GroupGBS Trial Group
((Lancet, Lancet, 1997)1997)nn Compared PE with Compared PE with IVIg IVIg and PE/and PE/IVIg IVIg 383 patients383 patientsnn No significant difference between treatments at 4 weeks fromNo significant difference between treatments at 4 weeks from
randomisation randomisation on Hughes scaleon Hughes scalenn No difference in secondary measures including time to recoverNo difference in secondary measures including time to recover
unaided walking, time to d/c vent, recovery from disability at 48unaided walking, time to d/c vent, recovery from disability at 48weeksweeks
nn No difference in the incidence of relapse after treatmentNo difference in the incidence of relapse after treatmentnn Conclusions:Conclusions:
nn PE and PE and IVIg IVIg have equivalent efficacyhave equivalent efficacynn No benefit from combined treatments over individualNo benefit from combined treatments over individualnn Equivalent risk of relapseEquivalent risk of relapse

IVIg IVIg ProtocolProtocolnn Costs less and is easier to useCosts less and is easier to usenn No need for central accessNo need for central accessnn Standard dose is 0.4 g/kg for 5 daysStandard dose is 0.4 g/kg for 5 daysnn Half-life is 3 to 6 weeksHalf-life is 3 to 6 weeksnn Adverse effects include aseptic meningitis, acuteAdverse effects include aseptic meningitis, acute
renal failure, ischemic stroke, anaphylactic shockrenal failure, ischemic stroke, anaphylactic shocknn Need to monitor Need to monitor creatinine creatinine levelslevelsnn No data on mild patients (ambulatory)No data on mild patients (ambulatory)

Preferred TreatmentPreferred Treatmentnn Choice ofChoice of IVIg IVIg or PE is a matter of convenienceor PE is a matter of convenience
and practicalityand practicalitynn IVIg IVIg preferred in rural areas, hospitals where PEpreferred in rural areas, hospitals where PE
not available, and in patients withnot available, and in patients withcontraindications to PEcontraindications to PE
nn In all other cases, data support no superiority ofIn all other cases, data support no superiority ofone over otherone over other
nn No clear data on efficacy of treatments in GBSNo clear data on efficacy of treatments in GBSvariants, mild disease (ambulatory)variants, mild disease (ambulatory)

Progression with treatmentProgression with treatmentnn 18% of patients will continue to deteriorate after18% of patients will continue to deteriorate after
receiving full course of receiving full course of IVIg IVIg or or plasmapheresisplasmapheresisnn 10% of patients will improve and then deteriorate10% of patients will improve and then deteriorate
(relapse)(relapse)nn Associated medical conditions appear to correlate bestAssociated medical conditions appear to correlate best
with increased risks of relapse, whereas earlier treatmentwith increased risks of relapse, whereas earlier treatmentonset is associated with decreased relapseonset is associated with decreased relapse
nn Anecdotal evidence for second course of same therapyAnecdotal evidence for second course of same therapyshowing benefitshowing benefit
nn Unclear whether improvement secondary to therapyUnclear whether improvement secondary to therapyversus natural history of diseaseversus natural history of disease
nn Controlled trials are in the planning phaseControlled trials are in the planning phase

CSF FiltrationCSF Filtrationnn Soluble Soluble pathogenetic pathogenetic factors can be removedfactors can be removed
from site where nerve conduction impeded orfrom site where nerve conduction impeded ornerve damage inflictednerve damage inflicted
nn 30 to 50 30 to 50 mL mL of CSF filtered and of CSF filtered and reinfusedreinfusednn No difference in outcome vs. plasma exchangeNo difference in outcome vs. plasma exchange
in one small study (in one small study (WollinskyWollinsky, , NeurologyNeurology, 2001), 2001)nn Underpowered to establish equivalenceUnderpowered to establish equivalencenn Experimental only at this timeExperimental only at this time

SteroidsSteroidsnn Corticosteroids alone are of no benefitCorticosteroids alone are of no benefitnn GBS Steroid Trial Group, GBS Steroid Trial Group, LancetLancet, 1993, 1993
nn 242 patients on242 patients on Solumedrol Solumedrol 500 mg for 5 days500 mg for 5 daysnn Ineffective in altering natural history of GBSIneffective in altering natural history of GBSnn May increase rate of relapseMay increase rate of relapse
nn OngoingOngoing multicenter multicenter trial is taking place to see benefit oftrial is taking place to see benefit ofIV steroids and IV steroids and IVIg IVIg simultaneouslysimultaneously
nn Pilot observations suggested beneficial interactionPilot observations suggested beneficial interactionnn Steroids are of benefit in management of CIDPSteroids are of benefit in management of CIDP

ICU AdmissionICU Admission
nn Patients with rapid progression (< 7 days)Patients with rapid progression (< 7 days)nn Neck weakness with inability to raiseNeck weakness with inability to raise
head against gravityhead against gravitynn Bulbar dysfunctionBulbar dysfunctionnn Bilateral facial weaknessBilateral facial weaknessnn SignificantSignificant dysautonomia dysautonomiann AspirationAspiration

ICU ManagementICU Managementnn Respiratory supportRespiratory supportnn FluidsFluidsnn Bowel/bladder careBowel/bladder carenn Autonomic dysfunctionAutonomic dysfunctionnn Skin, eye, mouth careSkin, eye, mouth carenn Pain managementPain managementnn NutritionNutritionnn DVT prophylaxisDVT prophylaxisnn Psychologic Psychologic supportsupport

Respiratory FailureRespiratory Failurenn Respiratory failure usually occurs within 1 week afterRespiratory failure usually occurs within 1 week after
onset of onset of paresthesiasparesthesiasnn 1/3 of patients will eventually require ventilator1/3 of patients will eventually require ventilatornn Unusual for diaphragmatic failure to develop > 2 weeksUnusual for diaphragmatic failure to develop > 2 weeks
into illnessinto illnessnn Evident by interrupted speech, inability to count to 20Evident by interrupted speech, inability to count to 20nn May be accompanied by tachycardia and sweatingMay be accompanied by tachycardia and sweatingnn Rapid decline may occur unexpectedlyRapid decline may occur unexpectedlynn Serial measurements are helpful in anticipatingSerial measurements are helpful in anticipating
mechanical ventilationmechanical ventilation

Respiratory ManagementRespiratory Managementnn At risk for At risk for atelectasis atelectasis due to diaphragmaticdue to diaphragmatic
akinesisakinesisnn Chest PT and frequent oral suctioning in thoseChest PT and frequent oral suctioning in those
with impaired coughwith impaired coughnn Respiratory measurementsRespiratory measurements
nn FVCFVCnn MIFMIF
nn Lung expansion techniquesLung expansion techniquesnn Incentive Incentive spirometryspirometrynn Maximal inspiration with cough maneuversMaximal inspiration with cough maneuvers

Decision to Decision to intubateintubate
nn Vital capacity less than 15 Vital capacity less than 15 mLmL/kg/kgnn PaO2 < 70 PaO2 < 70nn Inability to protect airway Inability to protect airwaynn 20-30-40 rule (Lawn et al., 20-30-40 rule (Lawn et al., Arch Arch NeurolNeurol 2001)2001)nn Vital capacity < 20 Vital capacity < 20 mLmL/kg/kgnn MIF < 30 cm H2O MIF < 30 cm H2Onn Max exp. Pressure < 40 cm H2O Max exp. Pressure < 40 cm H2Onn Change from > 30% from baseline Change from > 30% from baseline

WeaningWeaningnn Preferred approach is to reduce IMV rate withPreferred approach is to reduce IMV rate with
maximum pressure-supportmaximum pressure-supportnn Start once vital cap 15 Start once vital cap 15 mLmL/kg and tidal volumes of 10-/kg and tidal volumes of 10-
12 12 mLmL/kg/kgnn Pressure support is reduced to 5 cm H2OPressure support is reduced to 5 cm H2Onn Diaphragm weakness improves even beforeDiaphragm weakness improves even before
improvement in limbsimprovement in limbsnn Should not attempt weaning when Should not attempt weaning when dysautonomia dysautonomia isis
still presentstill presentnn Weaning should be expected in 20 to 30 daysWeaning should be expected in 20 to 30 days

FluidsFluids
nn Isotonic saline infusion 2 liters dailyIsotonic saline infusion 2 liters dailynn Should be adjusted once enteric feedingShould be adjusted once enteric feeding
startedstartednn Larger volumes needed in those onLarger volumes needed in those on
ventilators and with feversventilators and with fevers

Bowel/bladder IssuesBowel/bladder Issues
nn ConstipationConstipationnn Slowing of bowel activity due to Slowing of bowel activity due to bedrestbedrestnn Stool softenersStool softenersnn Adynamic ileus Adynamic ileus may occur but raremay occur but rare
nn Bladder paralysisBladder paralysisnn Indwelling catheterIndwelling catheter

DysautonomiaDysautonomiann Autonomic storms occur commonly in rapidlyAutonomic storms occur commonly in rapidly
progressive GBS but may be present with mild weaknessprogressive GBS but may be present with mild weaknessnn Common manifestations are spontaneous BP changesCommon manifestations are spontaneous BP changes
and cardiac arrhythmiasand cardiac arrhythmiasnn Wide fluctuations over minutesWide fluctuations over minutesnn Due to impaired Due to impaired baroreceptor baroreceptor bufferingbufferingnn Spontaneous fluctuations in blood pressure should beSpontaneous fluctuations in blood pressure should be
left aloneleft alonenn Antihypertensive and Antihypertensive and pressors pressors should be used withshould be used with
cautioncautionnn Persistent hypotension can be treated withPersistent hypotension can be treated with
Trendelenburg Trendelenburg positioning and albumin infusionpositioning and albumin infusion

ArrhythmiasArrhythmiasnn Sinus bradycardia and tachycardiaSinus bradycardia and tachycardia
nn Can have sinus arrest and AV blockCan have sinus arrest and AV block
nn Tracheal suctioning may provokeTracheal suctioning may provoke
nn Complete heart block may occurComplete heart block may occur

Pain managementPain management
nn Hot packsHot packsnn Oral orOral or parenteral opioids parenteral opioidsnn NSAIDs NSAIDs for back andfor back and radicular radicular painpainnn Epidural morphineEpidural morphinenn Recovery phase Recovery phase neuropathic neuropathic painpain
responds to responds to Elavil Elavil or or MexiletineMexiletine

General careGeneral carenn Skin should be kept drySkin should be kept drynn Eyedrops Eyedrops for those who cannot close eyesfor those who cannot close eyes
completelycompletelynn May need taping of eyelids at nightMay need taping of eyelids at nightnn Mouth care including Mouth care including toothbrushing toothbrushing andand
inspection for inspection for candidiasiscandidiasisnn Regular turning, positioning and paddingRegular turning, positioning and paddingnn Splints, foot boards to prevent contracturesSplints, foot boards to prevent contracturesnn Early physical therapy to maintain ROMEarly physical therapy to maintain ROM

NutritionNutritionnn Enteral Enteral nutrition should be started in those withnutrition should be started in those with
diminished swallowing mechanics,diminished swallowing mechanics, intubated intubated
nn Contraindicated in Contraindicated in adynamic ileusadynamic ileus
nn Ileus Ileus occurs in minority of patientsoccurs in minority of patients
nn Should be treated with suctioning, IVShould be treated with suctioning, IVadministration, placement of flatus tubeadministration, placement of flatus tube

Other care issuesOther care issuesnn Psychologic Psychologic supportsupportnn Frequent discussion with patientFrequent discussion with patientnn Clear projection of future courseClear projection of future course
nn Stress ulcersStress ulcersnn Proton pump inhibitors for ventilated patientsProton pump inhibitors for ventilated patients
nn DVT prophylaxisDVT prophylaxisnn Many patients cannot tolerate Many patients cannot tolerate SCDsSCDs/TEDS/TEDSnn Subcutaneous HeparinSubcutaneous Heparin

OutcomeOutcomenn GBS is GBS is monophasic monophasic in majority of patientsin majority of patientsnn Recurrence very unusual, but have been knownRecurrence very unusual, but have been known
to occur after long asymptomatic interval (up toto occur after long asymptomatic interval (up to36 years)36 years)
nn Predictors of poor outcome:Predictors of poor outcome:nn C. C. jejunijejuni infection, antecedent diarrheal illnessinfection, antecedent diarrheal illnessnn Old ageOld agenn Comorbid Comorbid lung diseaselung diseasenn Degree of axonal degeneration on EMG/NCVDegree of axonal degeneration on EMG/NCVnn ProlongedProlonged ventilatory ventilatory supportsupportnn Rapidly progressive weakness prior to presentation < 7 daysRapidly progressive weakness prior to presentation < 7 days

RecoveryRecoverynn 80% of patients recover within 6 months80% of patients recover within 6 months
nn 15% recover completely15% recover completelynn 65% recover with minor deficits that do not interfere65% recover with minor deficits that do not interfere
with with ADLsADLsnn 5-10% have persistent motor weakness5-10% have persistent motor weaknessnn 3-5% die despite intensive care3-5% die despite intensive care
nn In patients with persistent motor weakness ,In patients with persistent motor weakness ,improvement can continue up to 2 yearsimprovement can continue up to 2 years