Embed Size (px)
Citation preview
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 1/43
TUBERCULOUS MENINGITIS
Supervisor:
dr. Ridwan M Daulay, Sp.A(K)
Presentator:
Lee Wei Lun 080100419
CASE REPORT
PEDIATRICS DEPARTMENT
FACULTY OF MEDICINE
UNIVERSITY OF NORTH SUMATERA
HAJI ADAM MALIK GENERAL HOSPITAL CENTER
MEDAN 2013
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 2/43
Definition
The disease caused by the inflammation of
the protective membranes covering the
brain and spinal cord known as the
meninges
EtiologyBacterial, Viral, Fungal, Parasitic,
Noninfectious
Risk Factor
- Immunodeficiency associated with young age,aging, malnutrition etc
- Immunosuppressed individuals
- Defect complemen system (C5-C8) in Eskimos.
- Congenital or acquired CSF leakage (may be
due to trauma)
Definition, Etiology and Risk Factors
of meningitis
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 3/43
Tuberculous
Meningitis
Infection of the meninges by
Mycobacterium tuberculosis.
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 4/43
Pathogenesis
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 5/43
Pathophysiology
Bacterialseeding
Increasedpearmeability BBB
Cerebraledema
Presenceof toxic
mediator s
Inflammationof spinal
nerves androots
Meningeal signs
Inflammationof cranialnerves
Cranialneurophatie
s
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 6/43
Diagnosis
Nonspecific
symptoms:Fever, Irritability,
Drowsiness, and
Malaise
Confusion,
meningeal
signs,
seizures
Coma,
Hemiparesis,
Nerves palsies
Lumbal Puncture Blood Culture
Radiology
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 7/43
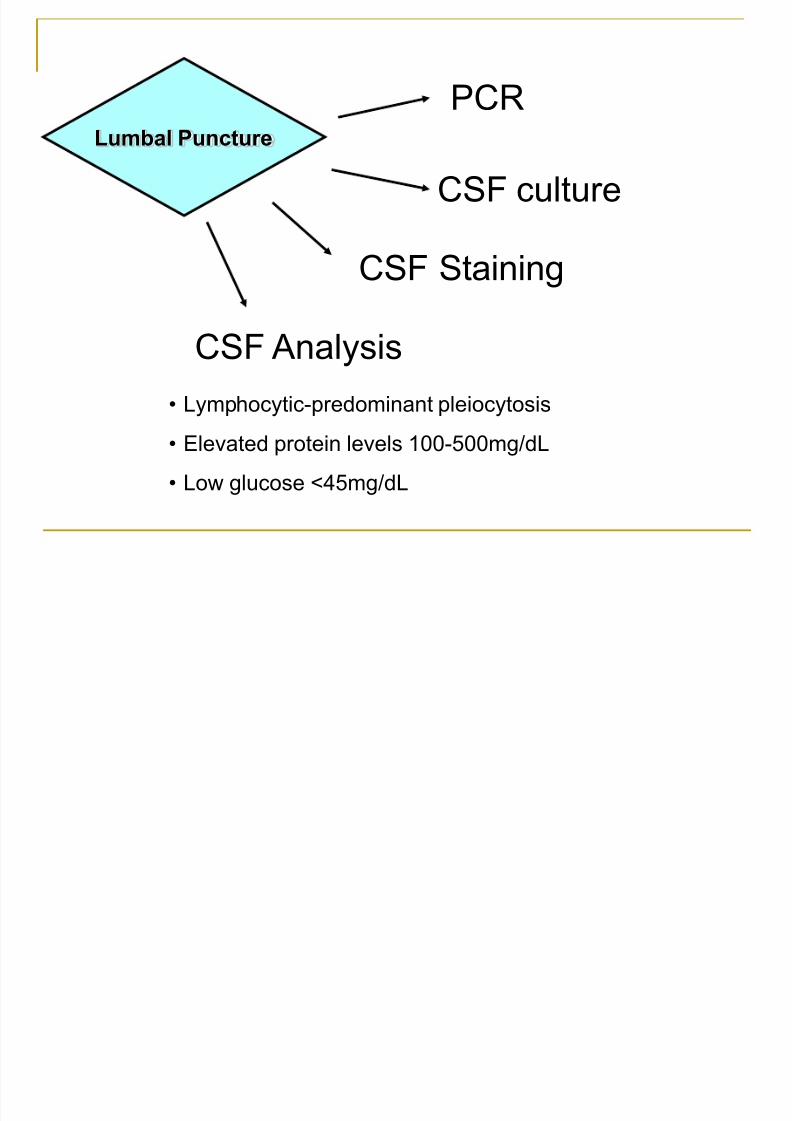
Lumbal Puncture
PCR
CSF culture
CSF Staining
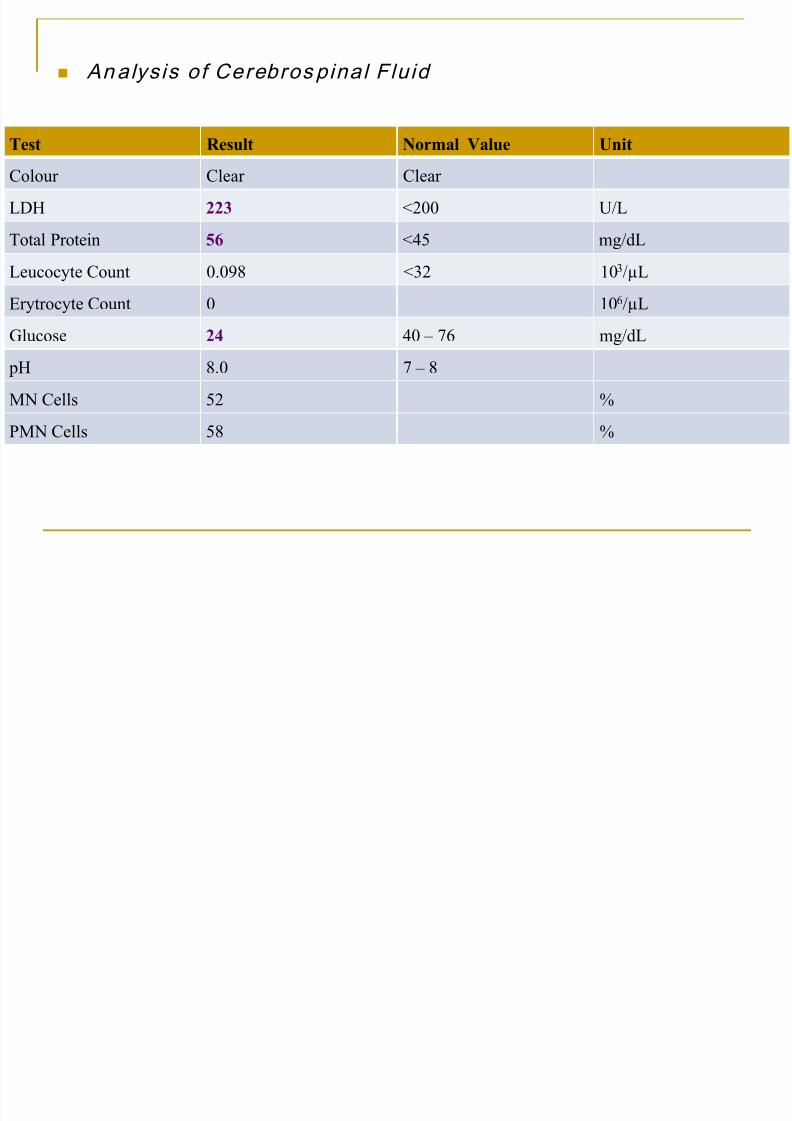
CSF Analysis
• Lymphocytic-predominant pleiocytosis• Elevated protein levels 100-500mg/dL
• Low glucose <45mg/dL

8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 8/43
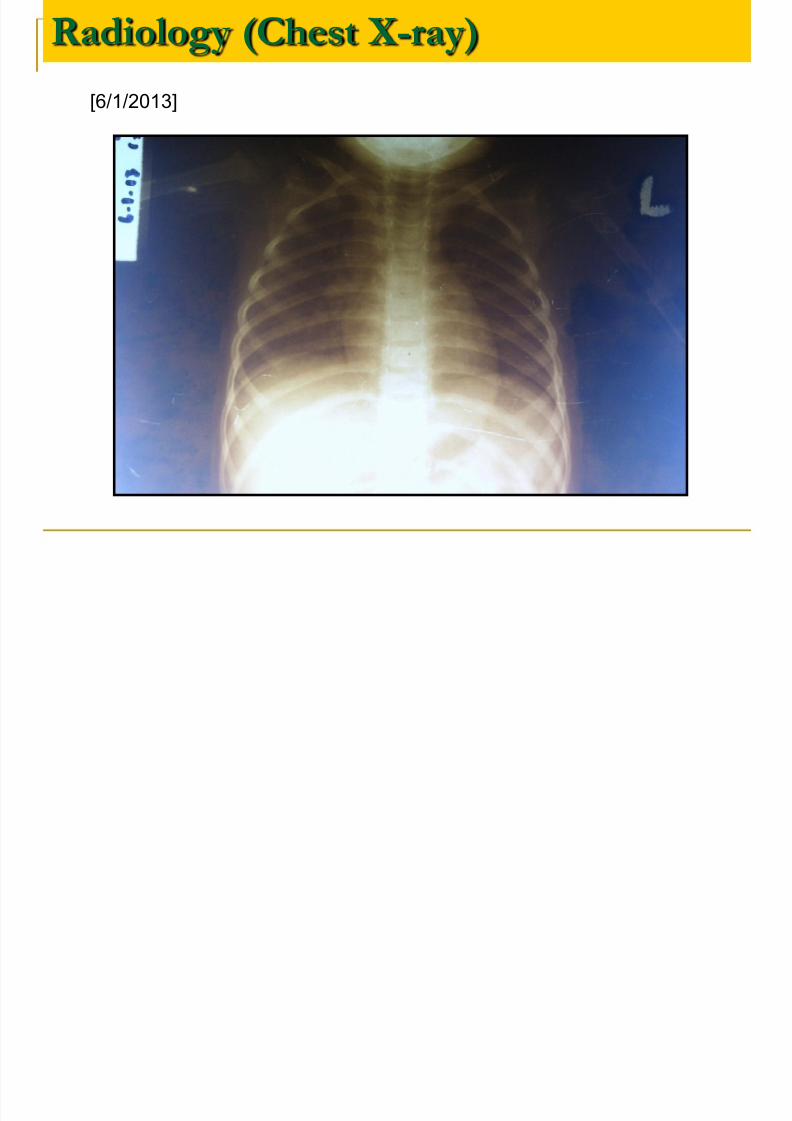
Radiology
• Suggesting active or previous
pulmonary tuberculosis
• 10% have milliary disease
Brain CT-Scan
Chest X-ray
• Hydrocephalus
• Tuberculomas
• Infarctions
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 9/43
Management
Antibiotic
Glucocorticoid
• Evidence thatinflammatorycytokines
• Adjunctivetherapy was
reducedaudiologic andneurologicsequelae
Antituberculousdrugs
• INH ( 10 mg/kgBB/day)
• Rifampicin (10-20mg/kgBB/day)
• Pyrazinamide (15-30mg/ kgBB /day
• Ethambutol (15-25mg/ kgBB/day)
• Streptomycin (20-40mg/ kgBB/day)
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 10/43
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 11/43
CASE REPORT
Name : PF
Age : 1 year 10 months Sex : Female
MR : 54.33.98
Address : Desa Batu Lapan, Deli
Serdang
Date of Admission : January 06th 2013
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 12/43
CHIEF COMPLAINT:
Altered level of consciousness
HISTORY:
It started 2 days ago and was preceded by an episode of seizure. Theseizure was generalized, with stiffening and rigidity of all four extremitiesand the patient’s eyeballs appeared to be rolled upwards. The seizure onlyoccurred once with duration of 1 hour and the patient was unconscioussince then. The patient does not have any history of seizure before this.
Fever(+) for the past 1 week with fluctuating body temperature, bodytemperature tends to decrease with consumption of antipyretic drugs.
Cough(+) for the past 1 week, unproductive. History of coming into contactwith any person with chronic coughs was not found.
2 days ago, before the seizure occurred, the patient experienced 2episodes of vomit. Contents of the vomits are the foods and drinks
ingested.Previous traumatic event was not found.
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 13/43
Pregnancy history : 2nd child of the family,
history of sickness during pregnancy (-), diabetes (-),
hypertension (-), consumption of medications (-),
consumption of herbal drinks (-).
Delivering history : Born at home with the helpof a midwife, aterm, cried immediately, birth weight:
3000gram and body length: 50cm. bluish appearance
(-), seizures (-) .
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 14/43
History of Growth &Development:
Sitting : 8 month
Walking : 1 yearCurrently patient can mention certain words like:‘mama’, ‘bapak’, ‘kakek’ and ‘nenek’
History of Feeding:
Birth – 5 mo : Breast milk only
5 mo – 1 yr : Breast milk + conventional
milk + porridge
1 year – present : conventional milk + soft rice
History of Immunization: Unclear
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 15/43
History of previous illness:
Patient was initially treated in Kabupaten A.Tamiang General Hospital for two days with thediagnosis: Encephalitis with bronchopneumonia.
History of previous medications:
Injection of Metamizole Sodium, Ampicillin,Gentamycin and Phenytoin
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 16/43
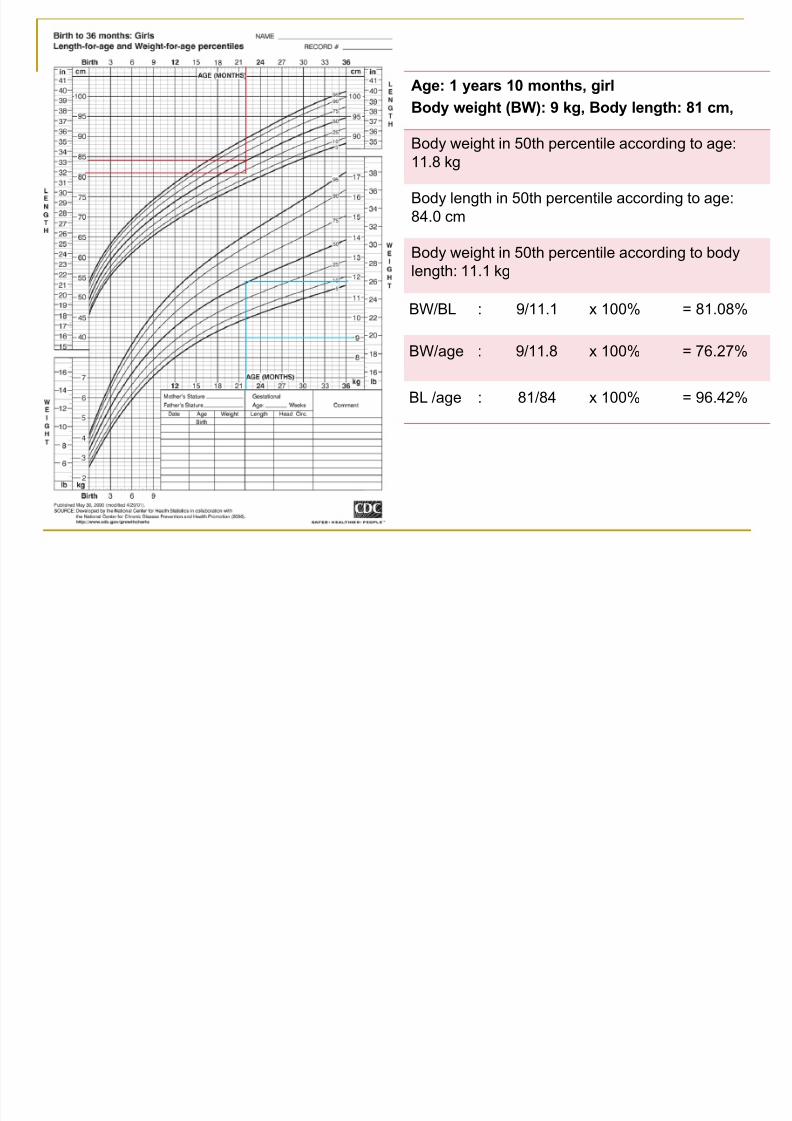
Age: 1 years 10 months, girl
Body weight (BW): 9 kg, Body length: 81 cm,
Body weight in 50th percentile according to age:11.8 kg
Body length in 50th percentile according to age:
84.0 cm
Body weight in 50th percentile according to body
length: 11.1 kg
BW/BL : 9/11.1 x 100% = 81.08%
BW/age : 9/11.8 x 100% = 76.27%
BL /age : 81/84 x 100% = 96.42%
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 17/43
Presence Status:
Sensorium: GCS 9 (E3V2M4)
BP = 90/60 mmHgHR = 120 x/i
RR = 26 x/i,
T = 38.5°C
Body weight (BW) : 9.0 kg
Body length (BL) : 81 cm
Head Circumference (HC): 43 cm
Anemic (-), icteric (-), dyspnea (-)cyanotic (-), edema (-).
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 18/43
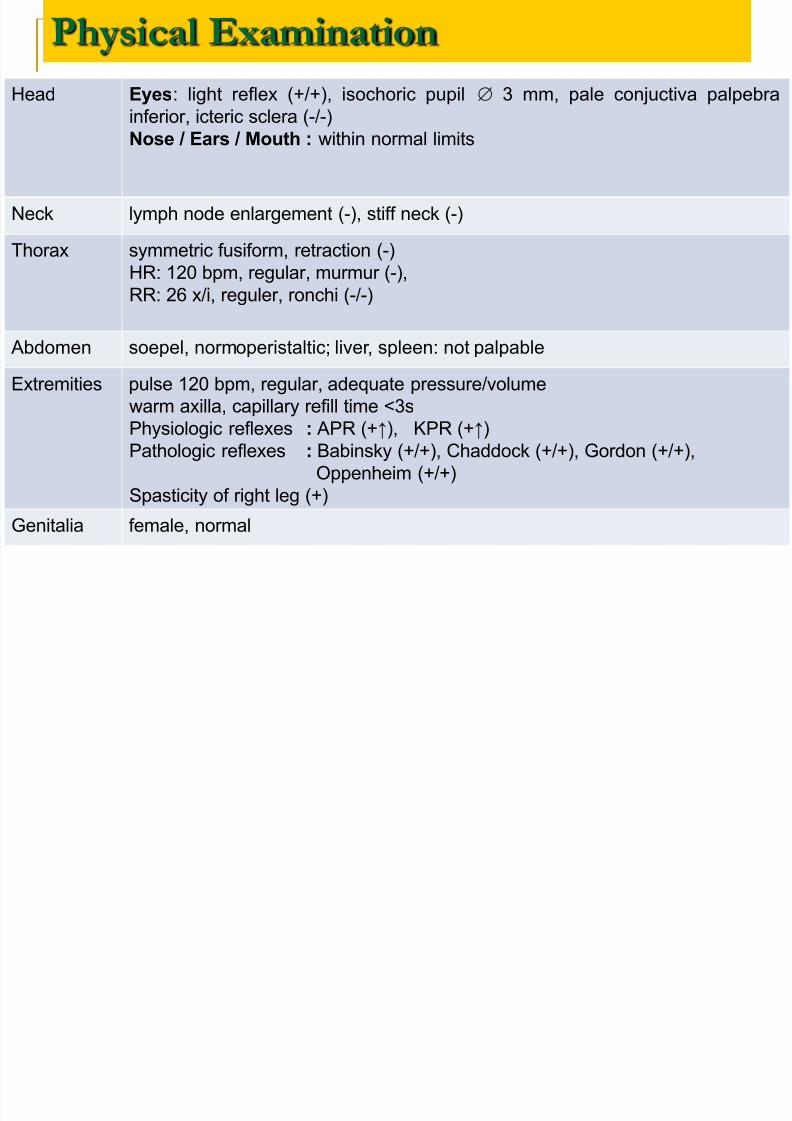
Physical Examination
Head Eyes: light reflex (+/+), isochoric pupil 3 mm, pale conjuctiva palpebra
inferior, icteric sclera (-/-)
Nose / Ears / Mouth : within normal limits
Neck lymph node enlargement (-), stiff neck (-)
Thorax symmetric fusiform, retraction (-)
HR: 120 bpm, regular, murmur (-),RR: 26 x/i, reguler, ronchi (-/-)
Abdomen soepel, normoperistaltic; liver, spleen: not palpable
Extremities pulse 120 bpm, regular, adequate pressure/volume
warm axilla, capillary refill time <3s
Physiologic reflexes : APR (+↑), KPR (+↑)
Pathologic reflexes : Babinsky (+/+), Chaddock (+/+), Gordon (+/+),
Oppenheim (+/+)
Spasticity of right leg (+)
Genitalia female, normal
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 19/43
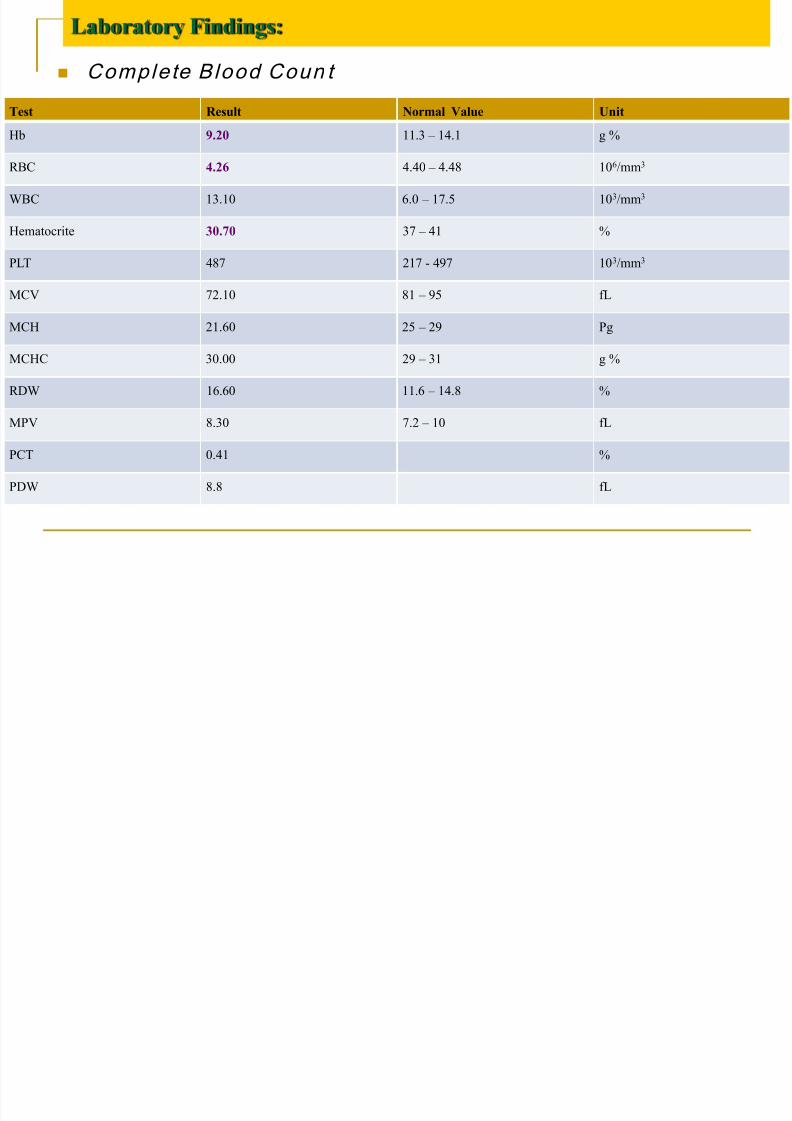
Laboratory Findings:
Complete Blood Coun t
Test Result Normal Value Unit
Hb 9.20 11.3 –
14.1 g %
RBC 4.26 4.40 – 4.48 106/mm3
WBC 13.10 6.0 – 17.5 103/mm3
Hematocrite 30.70 37 – 41 %
PLT 487 217 - 497 103/mm3
MCV 72.10 81 – 95 fL
MCH 21.60 25 – 29 Pg
MCHC 30.00 29 – 31 g %
RDW 16.60 11.6 – 14.8 %
MPV 8.30 7.2 –
10 fL
PCT 0.41 %
PDW 8.8 fL
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 20/43
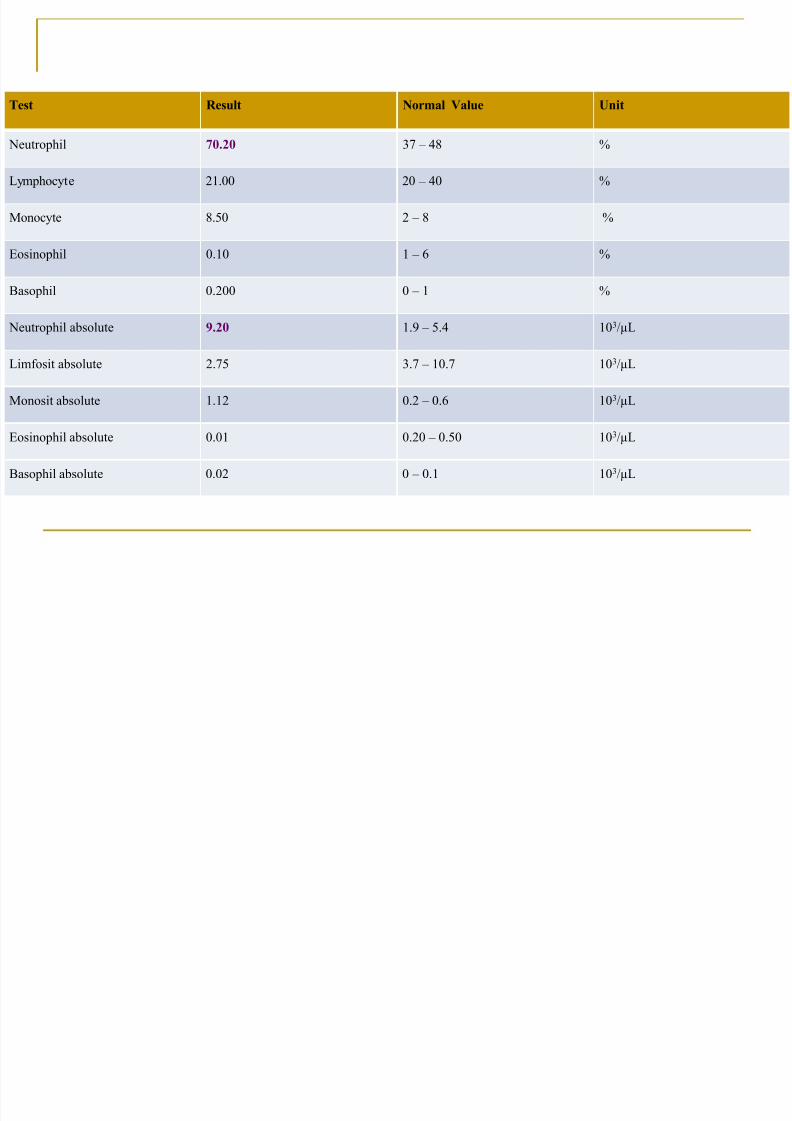
Test Result Normal Value Unit
Neutrophil 70.20 37 –
48 %
Lymphocyte 21.00 20 – 40 %
Monocyte 8.50 2 – 8 %
Eosinophil 0.10 1 – 6 %
Basophil 0.200 0 – 1 %
Neutrophil absolute 9.20 1.9 – 5.4 103/µL
Limfosit absolute 2.75 3.7 – 10.7 103/µL
Monosit absolute 1.12 0.2 – 0.6 103/µL
Eosinophil absolute 0.01 0.20 – 0.50 103/µL
Basophil absolute 0.02 0 – 0.1 103/µL
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 21/43
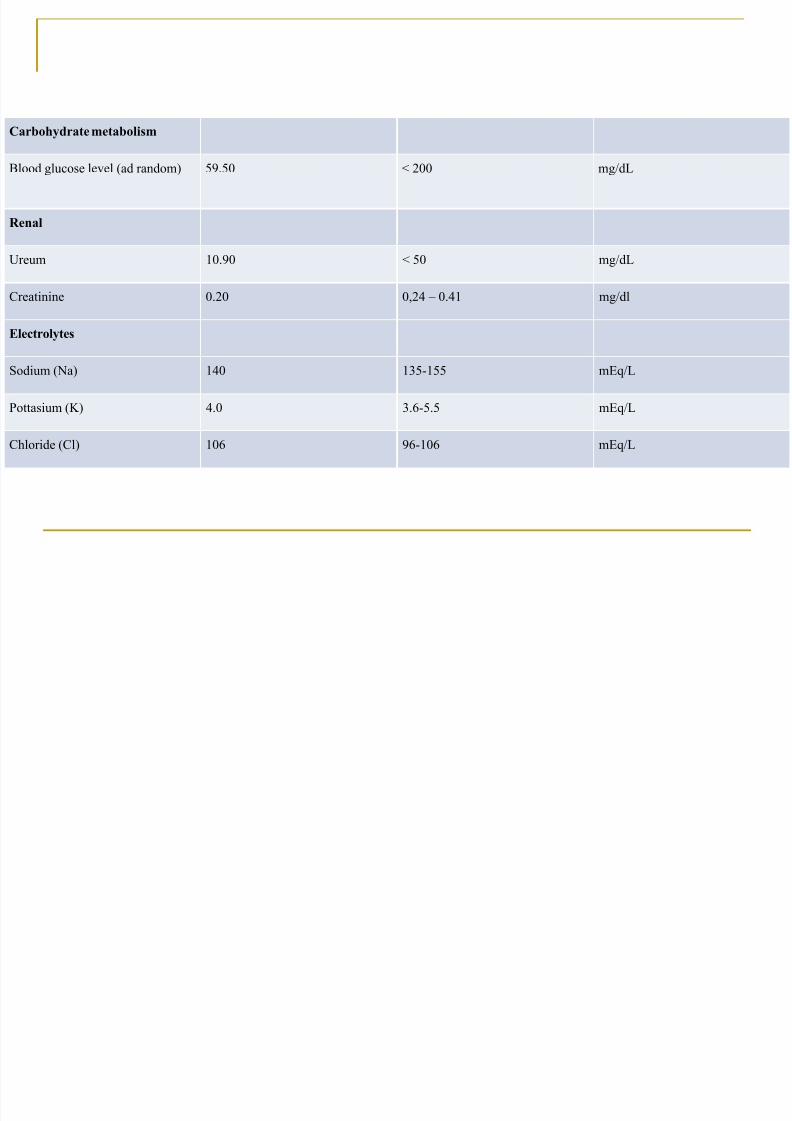
Carbohydrate metabolism
Blood glucose level (ad random) 59.50 < 200 mg/dL
Renal
Ureum 10.90 < 50 mg/dL
Creatinine 0.20 0,24 – 0.41 mg/dl
Electrolytes
Sodium (Na) 140 135-155 mEq/L
Pottasium (K) 4.0 3.6-5.5 mEq/L
Chloride (Cl) 106 96-106 mEq/L
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 22/43
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 23/43
Radiology (Chest X-ray)
[6/1/2013]
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 24/43
Differential Diagnosis:
Encephalitis
Meningoencephalitis
Meningitis
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 25/43
Management:
- Bed rest with 30º head elevation
- O2 1 liter/minute via nasal canule
- IVFD D5% NaCl 0,45% 19 gtt/i (micro)- Diet SV 900 kcal with 18g protein
- Inj. Phenytoin 25mg/12hours in 5cc D5% in 20 minutes
- Inj. Ceftriaxone 450 mg/12 hours/IV
- Inj. Ampicillin 450 mg/6 hours/IV
- Paracetamol 3x100 mg
Diagnostic Planning:
Consult Neurology Division
Head CT-Scan Mantoux test done on left volar, read on 9th January
Blood culture
J 7th 2013
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 26/43
January 7th 2013
S Decreased level of consciousness (+), fever(+)
O
Sens: GCS 9 (E3V2M4), T= 38.3°C
Head: Eyes: light reflex (+/+), isochoric pupil 3 mm, pale
conjuctiva palpebra inferior, icteric sclera (-/-)
Nose: nasal canule (+)
Ears / Mouth : within normal limits
Neck : lymph node enlargement (-), stiff neck (-)
Thorax: symmetric fusiform, retraction (-), HR: 110 bpm,
regular, murmur (-)
RR: 24 x/i, reguler, ronchi (-/-)Abdomen: soepel, normoperistaltic; liver, spleen, and
renal are not palpable
Extremities: pulse 110 bpm, regular, adequate
pressure/volume, warm acral, capillary refill time <3’’
Physiologic reflexes : APR (+↑), KPR (+↑)
Pathologic reflexes : Babinsky (+/+), Chaddock
(+/+), Gordon (+/+), Oppenheim (+/+)
A DD: 1. Encephalitis
2. Meningoencephalitis
3. Meningitis
P
Management:
- Bed rest with 30º head elevation
- O2
1 liter/minute via nasal canule
- IVFD D5% NaCl 0,45% 19 gtt/i (micro)
- Diet SV 900 kcal with 18g protein
- Inj. Phenytoin 25mg/12hours in 5cc D5% in 20minutes
- Inj. Ceftriaxone 450 mg/12 hours/IV (H1)
- Inj. Ampicillin 450 mg/6 hours/IV (H1)
- Inj. Dexamethasone 9mg/6hours/IV
- Paracetamol 3x100 mg
Pediatric Neurologist Consultation:
Working Diagnosis: Encephalitis
Treatment: IVFD NaCl 3%/12 hours done in 2 hours
time
Liver Function Test
AST/SGOT: 45U/L (N: <32)
ALT/SGPT: 17 U/L (N: <31)
Ferritin: results pending
Iron (Fe): 25 mg/dL (N: 61 – 157)
TIBC: 153 mcg/dL (N: 112 – 346)
January 8th 2013
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 27/43
January 8th 2013
S Decreased level of consciousness (+), fever(+)
O
Sens: GCS 9 (E3V2M4), T= 38.6°C
Head: Eyes: light reflex (+/+), isochoric pupil 2 mm, pale
conjuctiva palpebra inferior, icteric sclera (-/-)
Nose: nasal canule (+)
Ears / Mouth : within normal limits
Neck : lymph node enlargement (-), stiff neck (-)
Thorax: symmetric fusiform, retraction (-), HR: 106 bpm,
regular, murmur (-)
RR: 30 x/i, reguler, ronchi (-/-)Abdomen: soepel, normoperistaltic; liver, spleen, and
renal are not palpable
Extremities: pulse 106 bpm, regular, adequate
pressure/volume, warm acral, capillary refill time <3’’
Physiologic reflexes : APR (+↑), KPR (+↑)
Pathologic reflexes : Babinsky (+/+), Chaddock
(+/+), Gordon (+/+), Oppenheim (+/+)
A DD: 1. Encephalitis
2. Meningoencephalitis
3. Meningitis
P
Management:
- Bed rest with 30º head elevation
- O2 1 liter/minute via nasal canule
- IVFD D5% NaCl 0,45% 19 gtt/i micro
- IVFD NaCl 3% 90cc 45 gtt/i micro/ 12 hours
- Diet SV 900 kcal with 18g protein
- Inj. Phenytoin 25mg/12hours in 5cc D5% in 20minutes
- Inj. Ceftriaxone 450 mg/12 hours/IV (H2)
- Inj. Ampicillin 450 mg/6 hours/IV (H2)
- Inj. Dexamethasone 9mg/6hours/IV- Paracetamol 3x100 mg
Gastric Aspiration was done and samples taken for
microbiology and acid-fast test.
Results from blood culture using Bactec:
Staphylococcus saprophyticus
Balance: I: 850cc; O:670cc = 180cc
Urine Dipstick:
Leu Nit Uro Prot pH Blo Sg Ket Bil Glu
- - 0.2± 5.0 - 1.005 - - -
January 9th 2013
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 28/43
January 9th 2013
S Decreased level of consciousness (+), fever(+)
O
Sens: GCS 9 (E3V2M4), T= 38.5°C
Head: Eyes: light reflex (+/+), isochoric pupil 2 mm, pale
conjuctiva palpebra inferior, icteric sclera (-/-)
Nose: nasal canule (+)
Ears / Mouth : within normal limits
Neck : lymph node enlargement (-), stiff neck (-)
Thorax: symmetric fusiform, retraction (-), HR: 106 bpm,
regular, murmur (-)
RR: 28 x/i, reguler, ronchi (-/-)Abdomen: soepel, normoperistaltic; liver, spleen, and
renal are not palpable
Extremities: pulse 106 bpm, regular, adequate
pressure/volume, warm acral, capillary refill time <3’’
Physiologic reflexes : APR (+↑), KPR (+↑)
Pathologic reflexes : Babinsky (+/+), Chaddock
(+/+), Gordon (+/+), Oppenheim (+/+)
A DD: 1. Encephalitis + Suspect Sepsis
2. Meningoencephalitis
3. Meningitis
P
Management:
- Bed rest with 30º head elevation
- O2 1 liter/minute via nasal canule
- IVFD D5% NaCl 0,45% 19 gtt/i micro- IVFD NaCl 3% 90cc 45 gtt/i micro/ 12 hours
- Diet SV 900 kcal with 18g protein
- Inj. Phenytoin 25mg/12hours in 5cc D5% in 20minutes
- Inj. Ceftriaxone 450 mg/12 hours/IV (H3)
- Inj. Ampicillin 450 mg/6 hours/IV (H3)
- Inj. Dexamethasone 9mg/6hours/IV- Paracetamol 3x100 mg
Results of Mantoux Test: negative
Results from microbiology on gastric aspirates:
Epithelial: 0-1/lpbLeucocytes: 0-1/lpb
BTA: negative
Fungal: negative
Gastric Aspiration was repeated.
Immunoserology
Qualitative CRP: positive
Procalcitonin: 1.24ng/mL (N:<0.05)
January 10th 2013
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 29/43
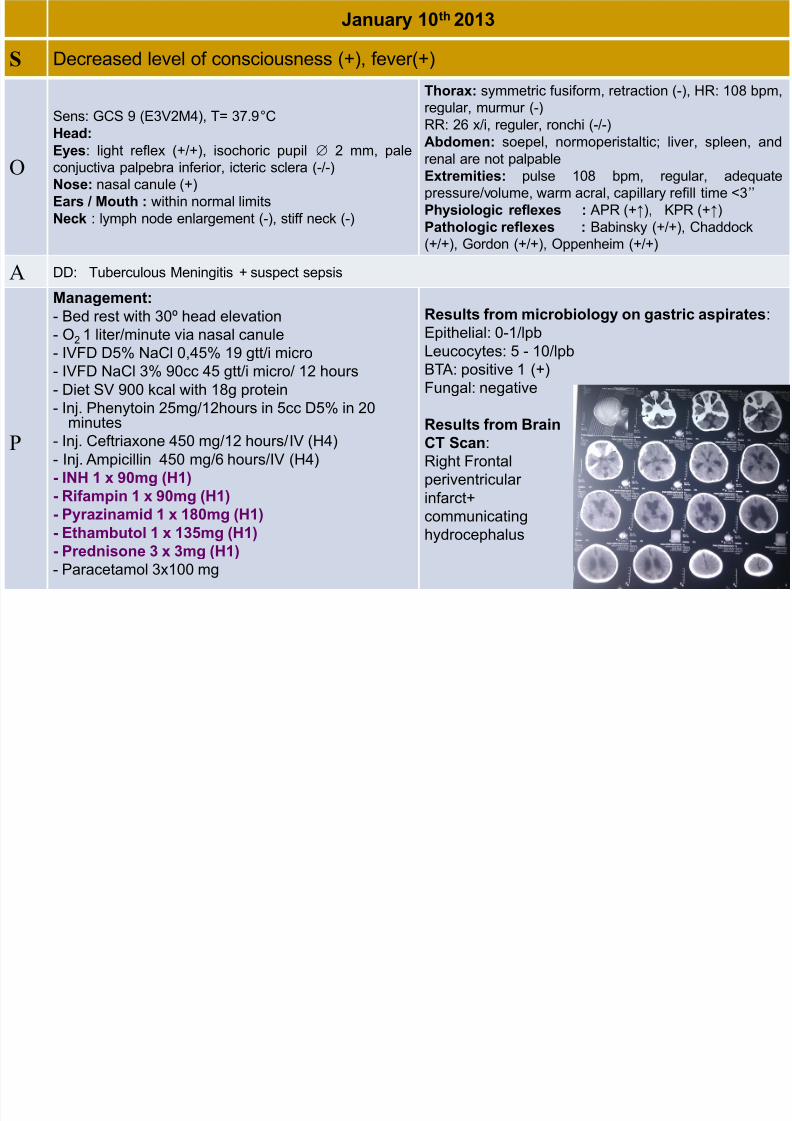
January 10th 2013
S Decreased level of consciousness (+), fever(+)
O
Sens: GCS 9 (E3V2M4), T= 37.9°C
Head:
Eyes: light reflex (+/+), isochoric pupil 2 mm, pale
conjuctiva palpebra inferior, icteric sclera (-/-)
Nose: nasal canule (+)
Ears / Mouth : within normal limits
Neck : lymph node enlargement (-), stiff neck (-)
Thorax: symmetric fusiform, retraction (-), HR: 108 bpm,
regular, murmur (-)
RR: 26 x/i, reguler, ronchi (-/-)
Abdomen: soepel, normoperistaltic; liver, spleen, andrenal are not palpable
Extremities: pulse 108 bpm, regular, adequate
pressure/volume, warm acral, capillary refill time <3’’
Physiologic reflexes : APR (+↑), KPR (+↑)
Pathologic reflexes : Babinsky (+/+), Chaddock
(+/+), Gordon (+/+), Oppenheim (+/+)
A DD: Tuberculous Meningitis + suspect sepsis
P
Management:
- Bed rest with 30º head elevation
- O2 1 liter/minute via nasal canule
- IVFD D5% NaCl 0,45% 19 gtt/i micro
- IVFD NaCl 3% 90cc 45 gtt/i micro/ 12 hours
- Diet SV 900 kcal with 18g protein
- Inj. Phenytoin 25mg/12hours in 5cc D5% in 20minutes
- Inj. Ceftriaxone 450 mg/12 hours/IV (H4)
- Inj. Ampicillin 450 mg/6 hours/IV (H4)
- INH 1 x 90mg (H1)
- Rifampin 1 x 90mg (H1)
- Pyrazinamid 1 x 180mg (H1)
- Ethambutol 1 x 135mg (H1)
- Prednisone 3 x 3mg (H1)- Paracetamol 3x100 mg
Results from microbiology on gastric aspirates:
Epithelial: 0-1/lpb
Leucocytes: 5 - 10/lpb
BTA: positive 1 (+)
Fungal: negative
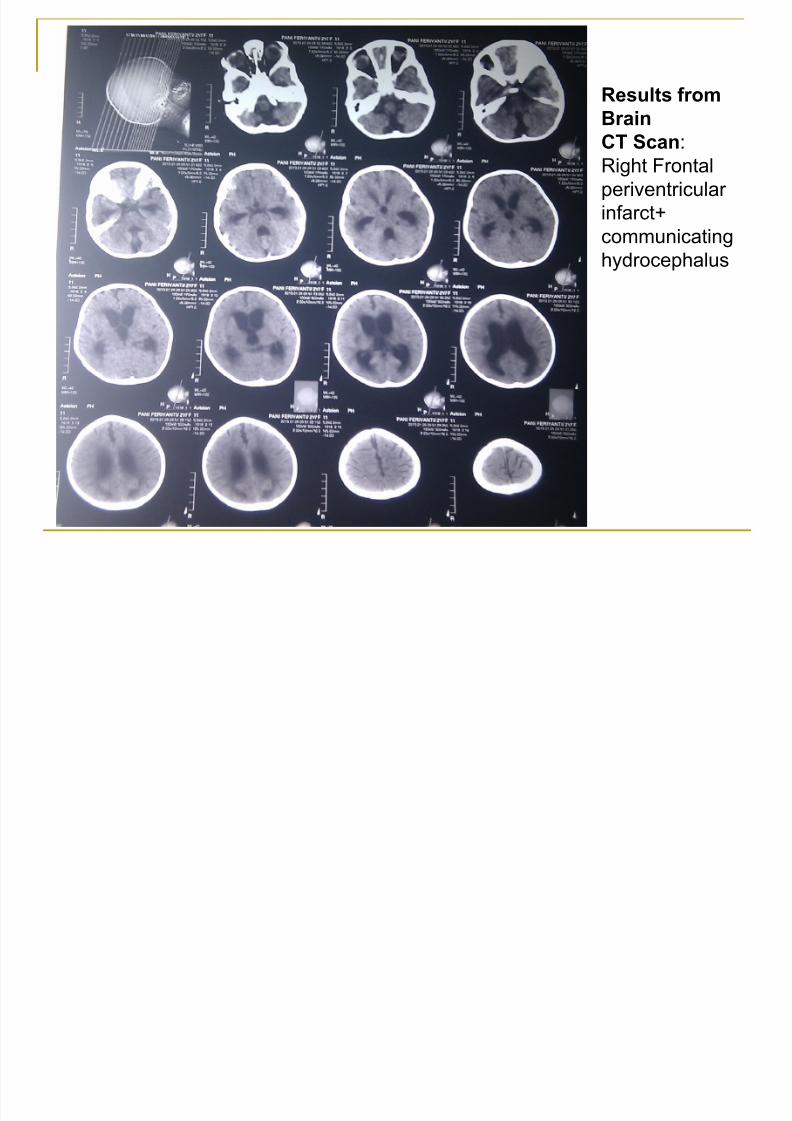
Results from Brain
CT Scan:
Right Frontal
periventricular
infarct+
communicating
hydrocephalus
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 30/43
Results from
Brain
CT Scan:Right Frontal
periventricular
infarct+
communicating
hydrocephalus
January 11th 2013
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 31/43
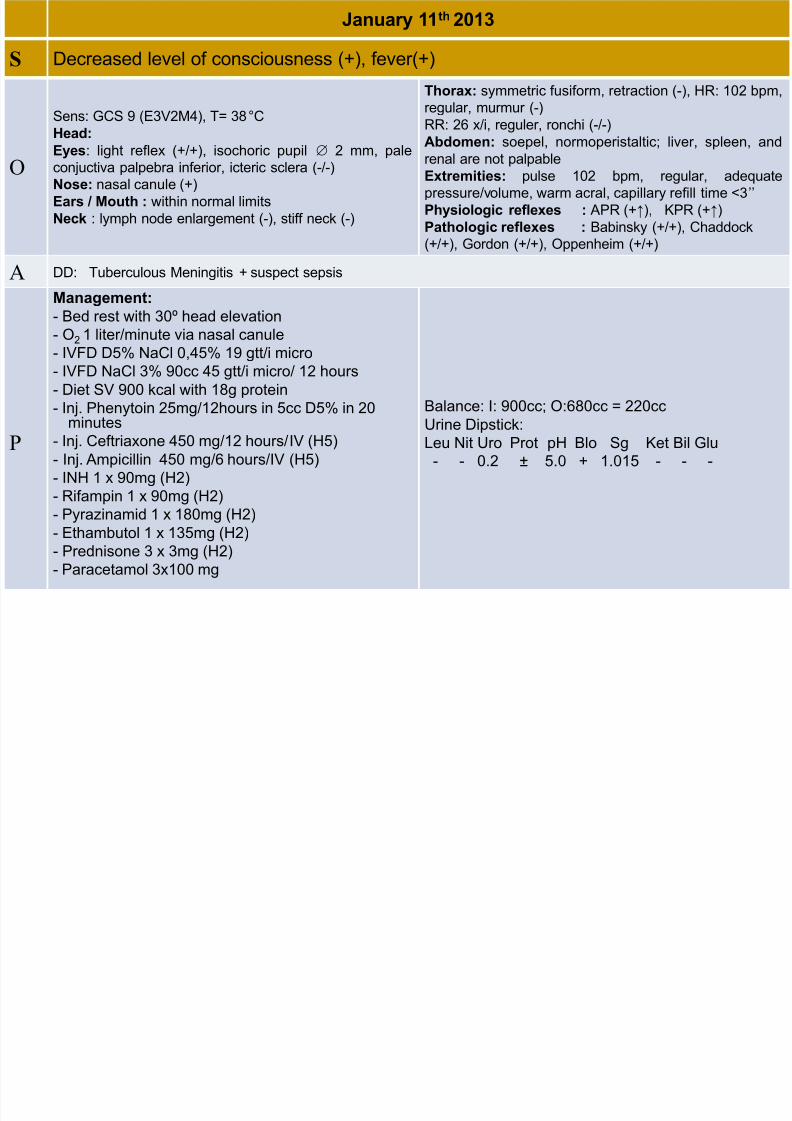
January 11 2013
S Decreased level of consciousness (+), fever(+)
O
Sens: GCS 9 (E3V2M4), T= 38°C
Head:
Eyes: light reflex (+/+), isochoric pupil 2 mm, pale
conjuctiva palpebra inferior, icteric sclera (-/-)
Nose: nasal canule (+)
Ears / Mouth : within normal limits
Neck : lymph node enlargement (-), stiff neck (-)
Thorax: symmetric fusiform, retraction (-), HR: 102 bpm,
regular, murmur (-)
RR: 26 x/i, reguler, ronchi (-/-)
Abdomen: soepel, normoperistaltic; liver, spleen, andrenal are not palpable
Extremities: pulse 102 bpm, regular, adequate
pressure/volume, warm acral, capillary refill time <3’’
Physiologic reflexes : APR (+↑), KPR (+↑)
Pathologic reflexes : Babinsky (+/+), Chaddock
(+/+), Gordon (+/+), Oppenheim (+/+)
A DD: Tuberculous Meningitis + suspect sepsis
P
Management:
- Bed rest with 30º head elevation
- O2 1 liter/minute via nasal canule
- IVFD D5% NaCl 0,45% 19 gtt/i micro
- IVFD NaCl 3% 90cc 45 gtt/i micro/ 12 hours
- Diet SV 900 kcal with 18g protein
- Inj. Phenytoin 25mg/12hours in 5cc D5% in 20minutes
- Inj. Ceftriaxone 450 mg/12 hours/IV (H5)
- Inj. Ampicillin 450 mg/6 hours/IV (H5)
- INH 1 x 90mg (H2)
- Rifampin 1 x 90mg (H2)
- Pyrazinamid 1 x 180mg (H2)
- Ethambutol 1 x 135mg (H2)
- Prednisone 3 x 3mg (H2)- Paracetamol 3x100 mg
Balance: I: 900cc; O:680cc = 220cc
Urine Dipstick:Leu Nit Uro Prot pH Blo Sg Ket Bil Glu
- - 0.2 ± 5.0 + 1.015 - - -
January 12th 2013
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 32/43
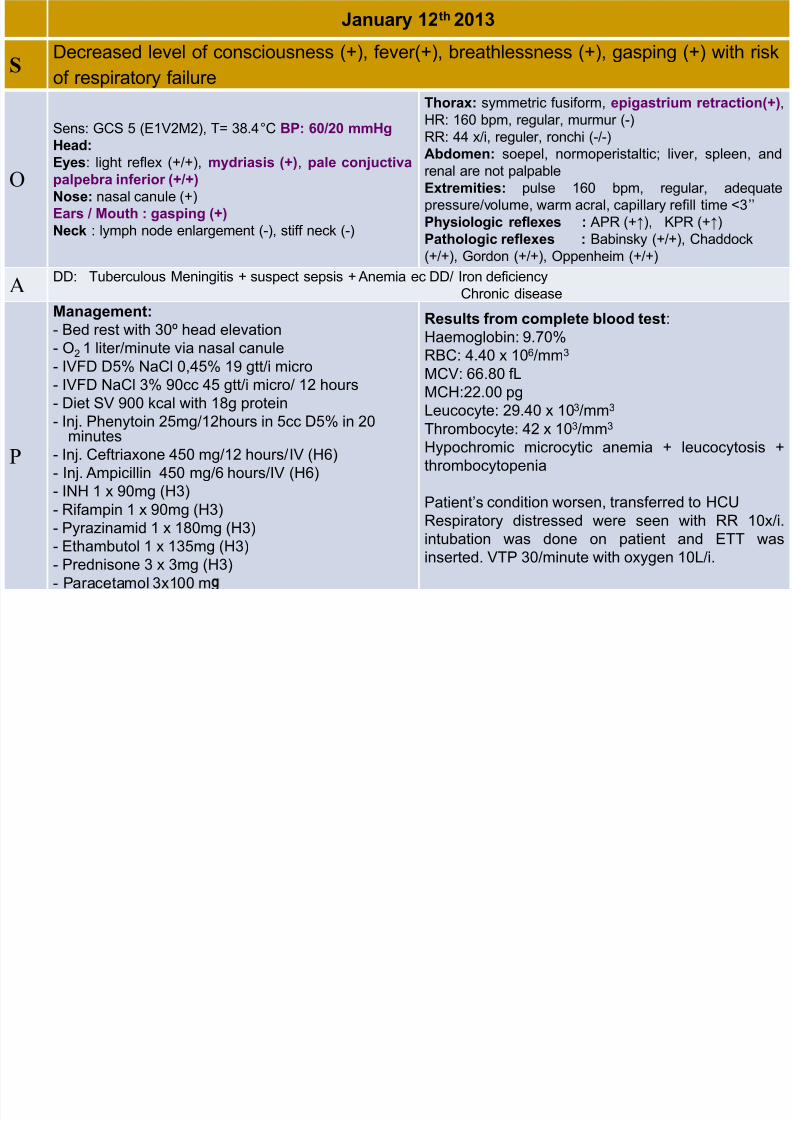
January 12 2013
S Decreased level of consciousness (+), fever(+), breathlessness (+), gasping (+) with risk
of respiratory failure
O
Sens: GCS 5 (E1V2M2), T= 38.4°C BP: 60/20 mmHg
Head: Eyes: light reflex (+/+), mydriasis (+), pale conjuctiva
palpebra inferior (+/+)
Nose: nasal canule (+)
Ears / Mouth : gasping (+)
Neck : lymph node enlargement (-), stiff neck (-)
Thorax: symmetric fusiform, epigastrium retraction(+),
HR: 160 bpm, regular, murmur (-)
RR: 44 x/i, reguler, ronchi (-/-)Abdomen: soepel, normoperistaltic; liver, spleen, and
renal are not palpable
Extremities: pulse 160 bpm, regular, adequate
pressure/volume, warm acral, capillary refill time <3’’
Physiologic reflexes : APR (+↑), KPR (+↑)
Pathologic reflexes : Babinsky (+/+), Chaddock
(+/+), Gordon (+/+), Oppenheim (+/+)
A DD: Tuberculous Meningitis + suspect sepsis + Anemia ec DD/ Iron deficiencyChronic disease
P
Management:
- Bed rest with 30º head elevation
- O2 1 liter/minute via nasal canule
- IVFD D5% NaCl 0,45% 19 gtt/i micro
- IVFD NaCl 3% 90cc 45 gtt/i micro/ 12 hours
- Diet SV 900 kcal with 18g protein
- Inj. Phenytoin 25mg/12hours in 5cc D5% in 20minutes
- Inj. Ceftriaxone 450 mg/12 hours/IV (H6)
- Inj. Ampicillin 450 mg/6 hours/IV (H6)
- INH 1 x 90mg (H3)
- Rifampin 1 x 90mg (H3)
- Pyrazinamid 1 x 180mg (H3)
- Ethambutol 1 x 135mg (H3)
- Prednisone 3 x 3mg (H3)
- Paracetamol 3x100 m
Results from complete blood test:
Haemoglobin: 9.70%
RBC: 4.40 x 106/mm3
MCV: 66.80 fL
MCH:22.00 pg
Leucocyte: 29.40 x 103/mm3
Thrombocyte: 42 x 103/mm3
Hypochromic microcytic anemia + leucocytosis +
thrombocytopenia
Patient’s condition worsen, transferred to HCU
Respiratory distressed were seen with RR 10x/i.
intubation was done on patient and ETT was
inserted. VTP 30/minute with oxygen 10L/i.
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 33/43
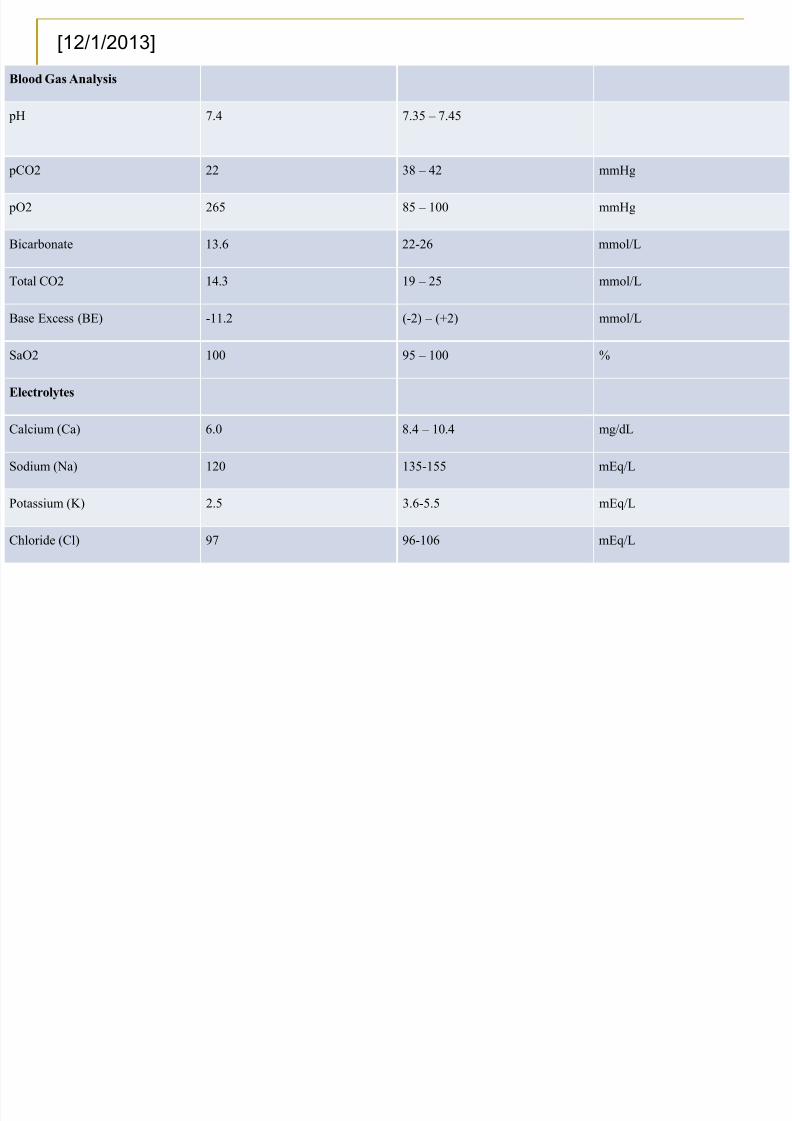
Blood Gas Analysis
pH 7.4 7.35 – 7.45
pCO2 22 38 – 42 mmHg
pO2 265 85 – 100 mmHg
Bicarbonate 13.6 22-26 mmol/L
Total CO2 14.3 19 –
25 mmol/L
Base Excess (BE) -11.2 (-2) – (+2) mmol/L
SaO2 100 95 – 100 %
Electrolytes
Calcium (Ca) 6.0 8.4 – 10.4 mg/dL
Sodium (Na) 120 135-155 mEq/L
Potassium (K) 2.5 3.6-5.5 mEq/L
Chloride (Cl) 97 96-106 mEq/L
[12/1/2013]
January 13th 2013
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 34/43
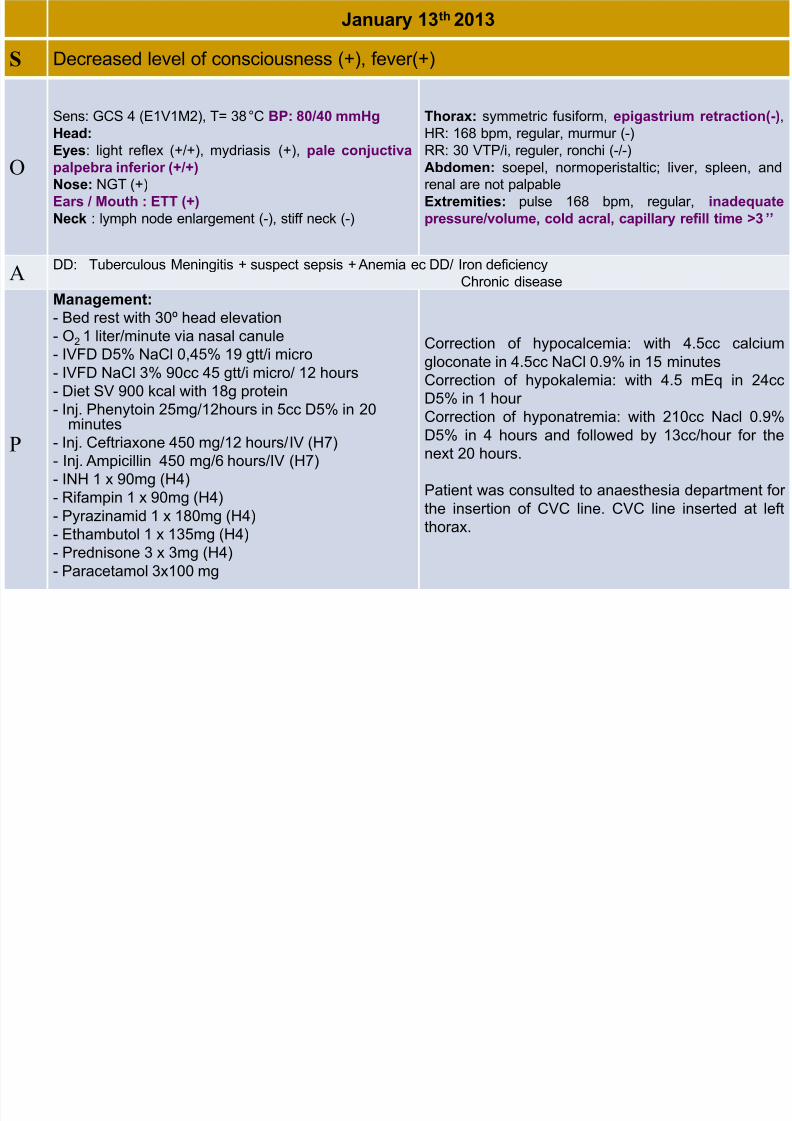
January 13 2013
S Decreased level of consciousness (+), fever(+)
O
Sens: GCS 4 (E1V1M2), T= 38°C BP: 80/40 mmHg
Head:
Eyes: light reflex (+/+), mydriasis (+), pale conjuctiva
palpebra inferior (+/+)
Nose: NGT (+)
Ears / Mouth : ETT (+)
Neck : lymph node enlargement (-), stiff neck (-)
Thorax: symmetric fusiform, epigastrium retraction(-),
HR: 168 bpm, regular, murmur (-)
RR: 30 VTP/i, reguler, ronchi (-/-)
Abdomen: soepel, normoperistaltic; liver, spleen, and
renal are not palpable
Extremities: pulse 168 bpm, regular, inadequate
pressure/volume, cold acral, capillary refill time >3’’
A
DD: Tuberculous Meningitis + suspect sepsis + Anemia ec DD/ Iron deficiency
Chronic disease
P
Management:
- Bed rest with 30º head elevation
- O2 1 liter/minute via nasal canule
- IVFD D5% NaCl 0,45% 19 gtt/i micro
- IVFD NaCl 3% 90cc 45 gtt/i micro/ 12 hours
- Diet SV 900 kcal with 18g protein
- Inj. Phenytoin 25mg/12hours in 5cc D5% in 20minutes
- Inj. Ceftriaxone 450 mg/12 hours/IV (H7)
- Inj. Ampicillin 450 mg/6 hours/IV (H7)
- INH 1 x 90mg (H4)
- Rifampin 1 x 90mg (H4)
- Pyrazinamid 1 x 180mg (H4)
- Ethambutol 1 x 135mg (H4)
- Prednisone 3 x 3mg (H4)- Paracetamol 3x100 mg
Correction of hypocalcemia: with 4.5cc calcium
gloconate in 4.5cc NaCl 0.9% in 15 minutes
Correction of hypokalemia: with 4.5 mEq in 24cc
D5% in 1 hour
Correction of hyponatremia: with 210cc Nacl 0.9%D5% in 4 hours and followed by 13cc/hour for the
next 20 hours.
Patient was consulted to anaesthesia department for
the insertion of CVC line. CVC line inserted at left
thorax.
January 14th 2013
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 35/43
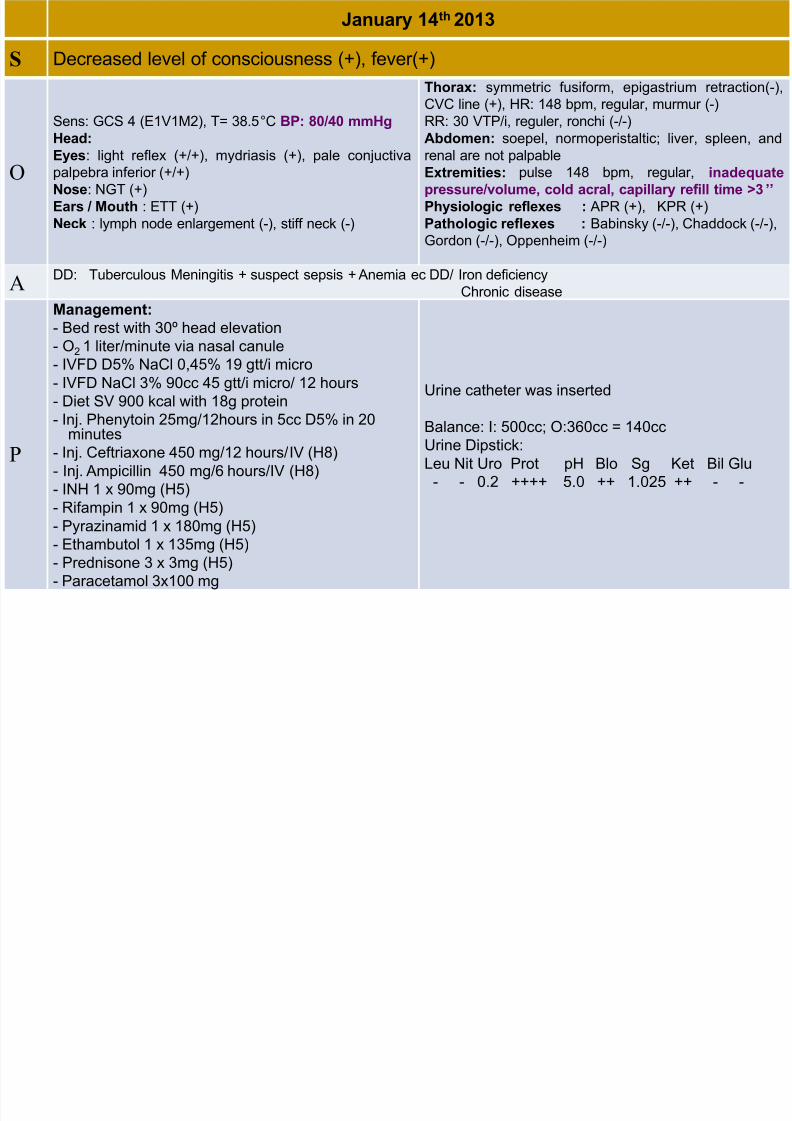
January 14 2013
S Decreased level of consciousness (+), fever(+)
O
Sens: GCS 4 (E1V1M2), T= 38.5°C BP: 80/40 mmHg
Head: Eyes: light reflex (+/+), mydriasis (+), pale conjuctiva
palpebra inferior (+/+)
Nose: NGT (+)
Ears / Mouth : ETT (+)
Neck : lymph node enlargement (-), stiff neck (-)
Thorax: symmetric fusiform, epigastrium retraction(-),
CVC line (+), HR: 148 bpm, regular, murmur (-)
RR: 30 VTP/i, reguler, ronchi (-/-)
Abdomen: soepel, normoperistaltic; liver, spleen, andrenal are not palpable
Extremities: pulse 148 bpm, regular, inadequate
pressure/volume, cold acral, capillary refill time >3’’
Physiologic reflexes : APR (+), KPR (+)
Pathologic reflexes : Babinsky (-/-), Chaddock (-/-),
Gordon (-/-), Oppenheim (-/-)
A DD: Tuberculous Meningitis + suspect sepsis + Anemia ec DD/ Iron deficiencyChronic disease
P
Management:
- Bed rest with 30º head elevation
- O2 1 liter/minute via nasal canule
- IVFD D5% NaCl 0,45% 19 gtt/i micro
- IVFD NaCl 3% 90cc 45 gtt/i micro/ 12 hours
- Diet SV 900 kcal with 18g protein
- Inj. Phenytoin 25mg/12hours in 5cc D5% in 20minutes
- Inj. Ceftriaxone 450 mg/12 hours/IV (H8)
- Inj. Ampicillin 450 mg/6 hours/IV (H8)
- INH 1 x 90mg (H5)
- Rifampin 1 x 90mg (H5)
- Pyrazinamid 1 x 180mg (H5)
- Ethambutol 1 x 135mg (H5)
- Prednisone 3 x 3mg (H5)- Paracetamol 3x100 mg
Urine catheter was inserted
Balance: I: 500cc; O:360cc = 140cc
Urine Dipstick:
Leu Nit Uro Prot pH Blo Sg Ket Bil Glu
- - 0.2 ++++ 5.0 ++ 1.025 ++ - -
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 36/43
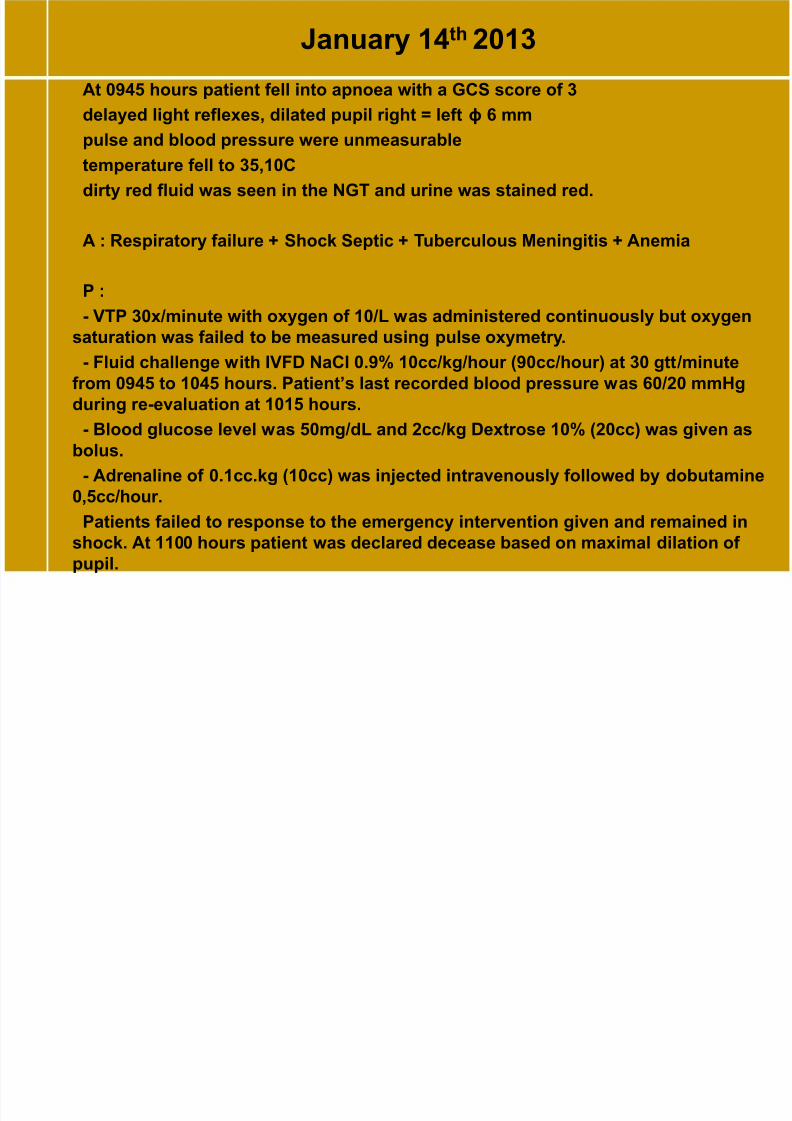
January 14th 2013
At 0945 hours patient fell into apnoea with a GCS score of 3
delayed light reflexes, dilated pupil right = left ϕ 6 mm
pulse and blood pressure were unmeasurabletemperature fell to 35,10C
dirty red fluid was seen in the NGT and urine was stained red.
A : Respiratory failure + Shock Septic + Tuberculous Meningitis + Anemia
P :
- VTP 30x/minute with oxygen of 10/L was administered continuously but oxygen
saturation was failed to be measured using pulse oxymetry.
- Fluid challenge with IVFD NaCl 0.9% 10cc/kg/hour (90cc/hour) at 30 gtt/minute
from 0945 to 1045 hours. Patient’s last recorded blood pressure was 60/20 mmHg
during re-evaluation at 1015 hours.
- Blood glucose level was 50mg/dL and 2cc/kg Dextrose 10% (20cc) was given as
bolus.
- Adrenaline of 0.1cc.kg (10cc) was injected intravenously followed by dobutamine
0,5cc/hour.
Patients failed to response to the emergency intervention given and remained in
shock. At 1100 hours patient was declared decease based on maximal dilation of
pupil.

8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 37/43
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 38/43
DISCUSSION
THEORYIn tuberculous meningitis, a prodromal phase of low-grade fever, malaise,
headache, dizziness and vomiting may persist for a few weeks, after whichpatients can then develop more severe headache, altered mental status,
stroke, hydrocephalus, and cranial neuropathies. Seizures occurs in about
50% of child tuberculous meningitis.
CASE
PF, was admitted with the chief complain of altered mentalstatus. Symptoms that preceded the decrease of
consciousness includes fever, vomiting and an episode ofseizure.
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 39/43
DISCUSSION
THEORYCharacteristic CSF findings of tuberculous meningitis include:
(i) Clear fluid
(ii) Lymphocytic-predominant pleiocytosis. Total white cell counts are
usually between 100 and 500 cells/ μ L. MN>PMN
(iii) Elevated protein levels, typically between 100 and 500 mg/dL,
(iv) Low glucose, usually less than 45mg/dL or CSF: plasma ratio <50%
CASE
CSF analysis shows a clear colored fluid, slight increase in proteins level: 56mg/dLand decrease level of CSF glucose: 24mg/dL. Pleiocytosis was not found. MN 52%,
PMN 58%.Atypical CSF findings are well described, particularly in immune-suppressed
patients, and the CSF can be acellular or contain a predominance of neutrophils .
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 40/43
DISCUSSION
THEORY
Gastric aspirates and bone marrow aspirates may assist indetecting extra-neural tuberculosis in children
CASE
Gastric aspiration was done twice. On the second time, resultsshows that acid-fast bacilli was found to be positive 1 (+1) on
smear.
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 41/43
DISCUSSION
THEORYThe commonest cerebral CT features of tuberculous meningitis are
hydrocephalus and basal contrast enhancing exudates. Both features are
more common in children ( 80%). Infarctions as a result of ongoingvasculitis or tuberculoma are found in approximately 20% of patients.
CASE
results of CT-scan from the radiologist: Right frontalperiventricular infarct with communicating hydrocephalus
possibly due to meningitis
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 42/43
PF, 1 year 10 months, female who first entered with thediagnosis of encephalitis was diagnosed withtuberculous meningitis with sepsis.
The diagnosis was established based on history taking,
clinical manifestations, laboratory and radiologicalfindings.
Patient was treated for 9 days.
The condition of the patient worsen after 2 days intoantituberculosis drugs and finally pass away on the 5th day of antituberculosis therapy due to respiratory failure.
8/13/2019 TBM Case Report (tuberculose meningitis)
http://slidepdf.com/reader/full/tbm-case-report-tuberculose-meningitis 43/43
hank you























![Tuberculose guia de vigilancia epidemiologica]](https://img.pdfslide.us/doc/110x75/5568c449d8b42a7c7d8b5158/tuberculose-guia-de-vigilancia-epidemiologica.jpg)




