Embed Size (px)
Citation preview

Surveillance of Colorectal Cancer Effectiveness of Early Detect ion of Intraluminal Recurrences on Prognosis and Survival of Patients Treated for Cure
P. Barillari, M.D., G. Ramacciato, M.D., G. Manetti, M.D., A. Bovino, M.D., P. Sammartino, M.D., V. Stipa, M.D.
From the First Department of Surgery, University of Rome "La Sapienza, "Rome, Italy
PURPOSE: The authors evaluate the effectiveness of routine colonoscopy and marker evaluation in diagnosis of intralu- minal recurrent cancer. METHODS: Chart review was con- ducted on 481 patients who underwent curative resection for colorectal cancer between 1980 and 1990. Clinical visits were scheduled and carcinoembryonic antigen evaluation was performed every three months, and colonoscopy was performed preoperatively, 12 to 15 months after surgical treatment, and then with intervals of 12 to 24 months or when symptoms appeared. RESULTS: About 10 percent of patients developed intraluminal recurrences. More than one-half of metachronous lesions arose within the first 24 months, and median time to diagnosis was 25 months. Patients with left-sited tumors in the advanced stage had a higher risk of developing recurrent intraluminal disease. Twenty-nine patients underwent a second surgical opera- tion, of which 17 cases were radical. In this group, the five-year survival was 70.6 percent, although no nonradi- caUy treated or nonresected patients survived longer than 31 months. Twenty-two patients were asymptomatic at time of diagnosis of recurrence, and of these, 12 patients underwent radical operation; on the other hand, of the 24 symptomatic patients, only 5 were treated radically. Carci- noembryonic antigen was the first sign of recurrence in eight cases. Colonoscopy must be performed within the first 12 to 15 months after operation, whereas an interval of 24 months between examinations seems sufficient to guar- antee early detection of metachronous lesions. CONCLU- SION: Serial tumor marker evaluation is of help in earlier diagnosis of local recurrences. Asymptomatic patients more frequently undergo another operation for cure and thus have a better survival rate. [Key words: Colorectal cancer; Local recurrence; Colonoscopy; Carcinoembryonic antigen (CEA)]
Barillari P, Ramacciato G, Manetti G, Bovino A, Sanmaartino P, Stipa V. Surveillance of colorectal cancer: effectiveness of early detection of intraluminal recurrences on prognosis and survival of patients treated for cure. Dis Colon Rectum 1996;38:388-393.
p atients t reated for colorectal cancer have an in-
creased risk of developing metachronous tu-
mors, polyps, or anastomotic recurrences. 1-7 Gener-
ally, it is accepted that local recurrences are curable
only by surgical resection, and radiotherapy and che-
motherapy usually offer little as far as survival is
concerned. Thus, early detect ion of asymptomatic re-
Address reprint requests to Dr. Barillari: Via della Camilluccia 589/c, 00135 Rome, Italy.
currences may offer the possibility of a second radical
operat ion and, hence, a further chance of permanent
cure. 8-1s Several long-term studies have, however,
indicated that intensive follow-up is not worth the
effort and expense, because up to 60 percent of new
lesions are detected only when patients are symptom-
atic. s-l~ Optimal type of follow-up care of these post-
operative patients has not yet been established.
Colonoscopy seems to be superior to bar ium enema
in detecting small polyps, and it also allows their
removal. 19 On the other hand, there is no consensus
about timing and duration of postoperat ive follow-up.
Aims of this study were 1) to evaluate effectiveness of
co lonoscopy in early detect ion of metachronous le-
sions in patients treated for colorectal cancer, 2) to
analyze timing and duration of postoperat ive follow-
up, and 3) to evaluate effectiveness of such fol low-up
programs in terms of incidence of resection for cure
and survival rates.
MATERIALS A N D M E T H O D S
The study included 607 patients who were treated
for colorectal cancer be tween 1980 and 1990 at the
First Depar tment of Surgery of the University of Rome
"La Sapienza." Data recorded for each case included
age, sex, preoperat ive examinations, site and stage of
primary neoplasm, and site and number of synchro-
nous polyps. We excluded patients with familial pol-
yposis or ulcerative colitis.
All patients underwent preoperat ive co lonoscopy
and, if a complete co lonoscopy was not feasible be-
cause of obstruction, patient was excluded from the
study. Microscopically proven hyperplastic polyps
were excluded from this review. Curative resection
was defined as the absence of local or metastatic
cancer and as the presence of "tumor-free" margins of
resection. Follow-up included clinical visits and car-
c inoembryonic antigen (CEA) evaluations every three
months and co lonoscopy every year or when patient
became symptomatic. During the last six years, 212
388

Vol 39, 4 SURVEILLANCE OF
patients were randomized into two similar groups (Table 1). First group included those who underwent
a first postoperative colonoscopy within 12 months
and then at mean intervals of 12 months. Second group was comprised of patients who underwent a
first postoperative colonoscopy within 12 months and then at mean intervals of 24 months. Randomization
was performed after surgery. If inclusion criteria for the study were satisfied, patients were assigned to the
first or second group and were given a numbered, sealed envelope containing the follow-up schedule. Follow-up schedules were determined by random numbers, which were generated on a personal com- puter. Colonoscopies were performed by fellows in
colon and rectal surgery and staff colon and rectal surgeons. M1 examinations were evaluated by two
observers, one of whom was always a staff colon and rectal surgeon. Most patients were given intravenous
sedation and narcotic analgesics during the proce- dure.
An "anastomotic recurrence" was defined as an intraluminal lesion occurring within 5 cm from the surgical anastomosis. A "methachronous tumor" was defined as neoplasm arising more than 5 cm from anastomosis and more than one year after surgical treatment.
Metastatic disease included involvement of the liver, lung, brain, peritoneal carcinomatosis and any other extraperitoneal organ. Chi-squared test (Yates'
correction), compared proportion Z test (Yates' cor- rection), and Fisher's exact test were used to assess differences.
RESULTS
Of 607 patients who underwent surgery, 61 had abdominoperineal resections, 34 were unresectable or had residual tumor at operation, and 31 other
Table 1. Characteristics of Two Randomized Groups
Group 1 Group 2
Localization Right colon 38 37 Left colon 34 37 Rectum 34 32
Stage T1 ,NO 5 4 T2,N0 25 25 T3,N0 27 28 T2,N1 29 28 T3,N1 2O 21
COLORECTAL CANCER 389
patients had an incomplete follow-up and thus were excluded from the study. Complete records and fol-
low-up information were available for 481 patients.
There were 251 men and 230 women, and mean age
was 65.2 (range, 29-89) years. Sixteen (3.3 percent) patients presented two or more synchronous tumors. Distribution of primary neoplasms with regard to
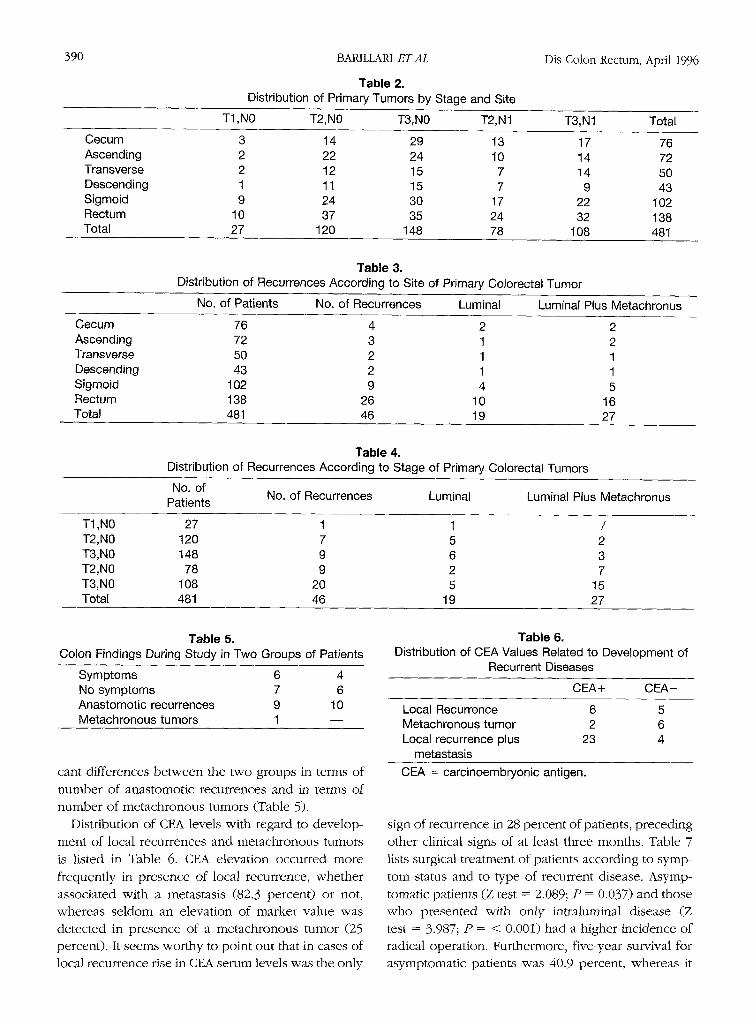
stage and localization is listed in Table 2; 50.1 percent of tumors were located in distal portion of the large
bowel, 53.2 percent were considered T3 neoplasms, and 38.7 percent were node-positive carcinomas.
Mean follow-up period per patient was 62 (range, 37-142) months. Of 481 patients, 46 (9.6 percent) were subsequently diagnosed with intraluminal recur-
rences. Of these, 34 were local recurrences from rectal
cancer, and 12 were metachronous tumors. Mean time to diagnosis was 25 (range, 10-73) months. Fifty-
two percent of recurrences was detected within the
first two years, whereas only 29.5 percent of polyps was discovered over the same period of time. Of 46 patients who developed recurrent disease, 22 (47.6 percent) had recurrences that were detected while the patient was asymptomatic and 24 while the patient was symptomatic. Rectal recurrences were easily de-
tectable by digital rectal examination, even if asymp- tomatic, and most of these (80.8 percent) were de- tected within the first 18 months.
Concerning the 12 metachronous lesions, 4 devel- oped at the level of hepatic or splenic flexure, 5 were
discovered in patients who failed to repeat colonos- copy at regular interval, and finally 3 were diagnosed in patients who underwent incomplete colonoscopy, which was not repeated after a short period of time (poor bowel preparation, patient intolerance). Meta- chronous lesions were grouped according to TNM classification: five neoplasms were Stage T1,N0, two
were Stage T2,N0, two were Stage T3,N0, two were stage T2,N1, and one was Stage T3,N1. In four cases,
synchronous hepatic metastases were present at the time of the second surgical procedure. Of 34 local
recurrences, 10 (29.4 percent) developed only within the lumen, whereas 24 (70.6 percent) involved adja- cent structures or were associated with metastatic disease. Distribution of recurrences with regard to stage and localization is listed in Tables 3 and 4; 56.5 percent of recurrences developed after anterior resec- tion for rectal cancer (chi-squared = 8.361; P =
0.004), and 15.6 percent arose in patients affected with primary node-positive tumors (chi-squared =
11.631; P = <0.001). According to frequency at which colonoscopy was performed, there were no signifi-
390 BARILLARI ET AL
Table 2. Distribution of Primary Tumors by Stage and Site
Dis Colon Rectum, April 1996
T1 ,NO T2,N0 T3,N0 T2,N1 T3,N1 Total
Cecum 3 14 29 13 17 76 Ascending 2 22 24 10 14 72 Transverse 2 12 15 7 14 50 Descending 1 11 15 7 9 43 Sigmoid 9 24 30 17 22 102 Rectum 10 37 35 24 32 138 Total 27 120 148 78 108 481
Table 3. Distribution of Recurrences According to Site of Primary Colorectal Tumor
No. of Patients No. of Recurrences Luminal Luminal Plus Metachronus
Cecum 76 4 2 2 Ascending 72 3 1 2 Transverse 50 2 1 1 Descending 43 2 1 1 Sigmoid 102 9 4 5 Rectum 138 26 10 16 Total 481 46 19 27
Table 4. Distribution of Recurrences According to Stage of Primary Colorectal Tumors
No. of No. of Recurrences Luminal Luminal Plus Metachronus Patients
T1 ,NO 27 1 1 / T2,N0 120 7 5 2 T3,N0 148 9 6 3 T2,N0 78 9 2 7 T3,N0 108 20 5 15 Total 481 46 19 27
Table 5. Colon Findings During Study in Two Groups of Patients
Symptoms 6 4 No symptoms 7 6 Anastomotic recurrences 9 10 Metachronous tumors 1 - -
cant differences between the two groups in terms of
number of anastomotic recurrences and in terms of
number of metachronous tumors (Table 5).
Distribution of CEA levels with regard to develop-
ment of local recurrences and metachronous tumors
is listed in Table 6. CEA elevation occurred more
frequently in presence of local recurrence, whether
associated with a metastasis (82.3 percen0 or not,
whereas seldom an elevation of marker value was
detected in presence of a metachronous tumor (25
percent). It seems worthy to point out that in cases of local recurrence rise in CEA serum levels was the only
Table 6. Distribution of CEA Values Related to Development of
Recurrent Diseases
CEA+ CEA-
Local Recurrence 6 5 Metachronous tumor 2 6 Local recurrence plus 23 4
metastasis
CEA = carcinoembryonic antigen.
sign of recurrence in 28 percent of patients, preceding
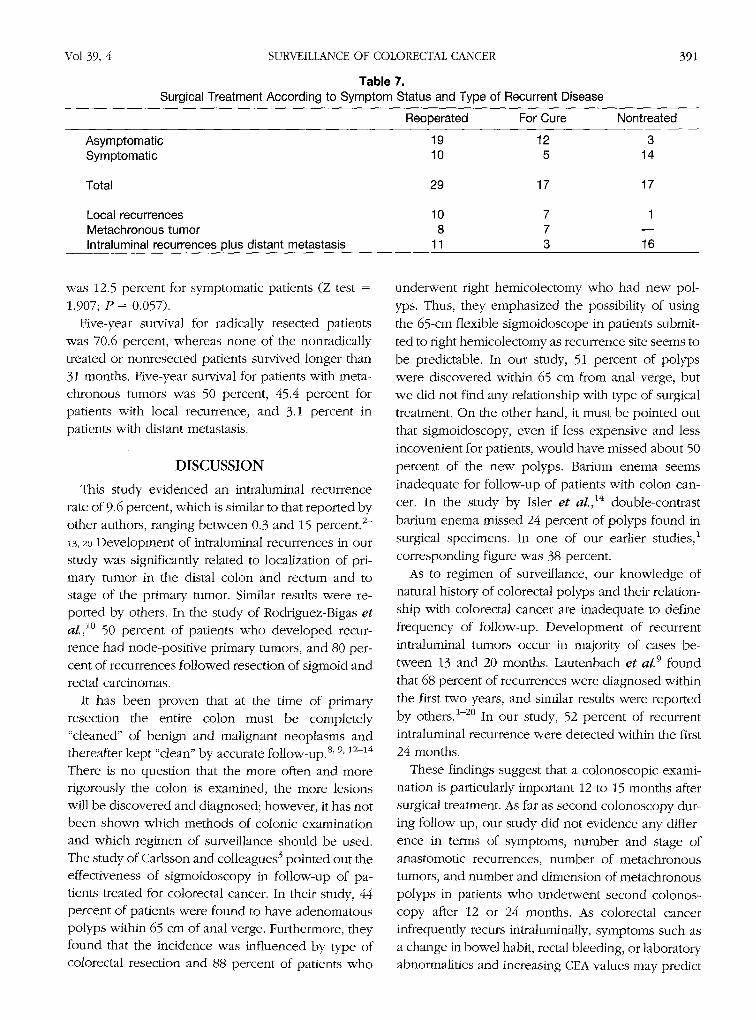
other clinical signs of at least three months. Table 7
lists surgical treatment of patients according to symp-
tom stares and to type of recurrent disease. Asymp-
tomatic patients (Z test = 2.089; P = 0.037) and those who presented with only intraluminal disease (Z
test = 3.987; P = < 0.001) had a higher incidence of
radical operation. Furthermore, five-year survival for
asymptomatic patients was 40.9 percent, whereas it
Vol 39, 4 SURVEILLANCE OF COLORECTAL CANCER
Table 7. Surgical Treatment According to Symptom Status and Type of Recurrent Disease
391
Reoperated For Cure Nontreated
Asymptomatic Symptomatic
Total
Local recurrences Metachronous tumor Intraluminal recurrences plus distant metastasis
19 12 3 10 5 14
29 17 17
10 7 1 8 7
11 3 16
was 12.5 percent for symptomatic patients (Z test =
1.907; P = 0.057). Five-year survival for radically resected patients
was 70.6 percent, whereas none of the nonradically treated or nonresected patients survived longer than 31 months. Five-year survival for patients with meta- chronous tumors was 50 percent, 45.4 percent for patients with local recurrence, and 3.1 percent in patients with distant metastasis.
D I S C U S S I O N
This study evidenced an intraluminal recurrence rate of 9.6 percent, which is similar to that reported by
other authors, ranging between 0.3 and 15 percent. 2- ,3, 2o Development of intraluminal recurrences in our study was significantly related to localization of pri- mary tumor in the distal colon and rectum and to stage of the primary tumor. Similar results were re- ported by others. In the study of Rodriguez-Bigas e t
al., 1~ 50 percent of patients who developed recur- rence had node-positive primary tumors, and 80 per- cent of recurrences followed resection of sigmoid and rectal carcinomas.
It has been proven that at the time of primary resection the entire colon must be completely "cleaned" of benign and malignant neoplasms and thereafter kept "clean" by accurate follow-up. 8' 9, 12-14
There is no question that the more often and more rigorously the colon is examined, the more lesions will be discovered and diagnosed; however, it has not been shown which methods of colonic examination and which regimen of surveillance should be used. The study of Carlsson and colleagues 3 pointed out the effectiveness of sigmoidoscopy in follow-up of pa- tients treated for colorectal cancer. In their study, 44 percent of patients were found to have adenomatous polyps within 65 cm of anal verge. Furthermore, they found that the incidence was influenced by type of colorectal resection and 88 percent of patients who
underwent right hemicolectomy who had new pol-
yps. Thus, they emphasized the possibility of using
the 65-cm flexible sigmoidoscope in patients submit-
ted to right hemicolectomy as recurrence site seems to
be predictable. In our study, 51 percent of polyps were discovered within 65 cm from anal verge, but
we did not find any relationship with type of surgical
treatment. On the other hand, it must be pointed out that sigmoidoscopy, even if less expensive and less
incovenient for patients, would have missed about 50
percent of the new polyps. Barium enema seems
inadequate for follow-up of patients with colon can- cer. In the study by Isler e t aL, 14 double-contrast
barium enema missed 24 percent of polyps found in surgical specimens. In one of our earlier studies, 1
corresponding figure was 38 percent.
As to regimen of surveillance, our knowledge of natural history of colorecta] polyps and their relation-
ship with colorectal cancer are inadequate to define
frequency of follow-up. Development of recurrent
intraluminal tumors occur in majority of cases be- tween 13 and 20 months. Lautenbach et al. 9 found
that 68 percent of recurrences were diagnosed within
the first two years, and similar results were reported
by others. 1-2~ In our study, 52 percent of recurrent
intraluminal recurrence were detected within the first 24 months.
These findings suggest that a colonoscopic exami- nation is particularly important 12 to 15 months after
surgical treatment. As far as second colonoscopy dur-
ing follow-up, our study did not evidence any differ- ence in terms of symptoms, number and stage of
anastomotic recurrences, number of metachronous
tumors, and number and dimension of metachronous
polyps in patients who underwent second colonos-
copy after 12 or 24 months. As colorectal cancer infrequently recurs intraluminally, symptoms such as
a change in bowel habit, rectal bleeding, or laboratory abnormalities and increasing CEA values may predict

392 BARILLARI ET AL Dis Colon Rectum, April 1996
appearance of recurrent disease; however, aggressive follow-up protocols 2~ found that approximately 50
percent of patients were asymptomatic for recurrent
disease. In our study, 47.8 percent of patients had
recurrences although asymptomatic, and 86.3 percent
were able to undergo a second resection that was
radical in 63.1 percent of cases. In the group of symp-
tomatic patients, only 41 percent underwent second
surgical treatment, which was radical in 50 percent of
cases. Survival rate for symptomatic and asymptom-
atic patients was 12.5 percent and 40.9 percent, re-
spectively. Similar data were reported by Lautenbach
e t aL,9 who showed that of patients diagnosed while
asymptomatic, 75 percent were able to undergo cur-
ative resection, whereas this was possible only in 16
percent of patients who were symptomatic on presen-
tation.
CEA evaluation presents a good sensitivity in pres-
ence of local recurrence, and this sensitivity might
increase using other markers in association with CEA. 24 In this study, eight (17 percen0 recurrences
were diagnosed only on the basis of CEA rise.
Incidence of metachronous tumors ranges be tween 0.6 and 3.6 percent; 1' 3-7, 20, 21 however, a large num-
ber of these polyps, called "early metachronous" tu-
mors, were detected precociously after the operation;
they had been misdiagnosed in preoperat ive exami-
nations. In our study, no early metachronous tumor
was detected, and this is attributable, in our opinion,
to preoperat ive colonoscopy, which permits detec-
tion of synchronous tumors that, with other examina-
tions, would have been misdiagnosed and later on
identified as metachronous. Furthermore, during fol-
low-up, early excision of polyps would avoid degen-
eration into carcinoma. In our study, 12 metachro-
nous tumors developed, and, in our opinion, it was
because of a mistake by the endoscopist in four cases (because of insidious localization of tumor at level of
hepatic flexure in two cases and behind a colonic
valve in the other two) and because of patient care-
lessness in the other eight cases. Data compiled from
the present study show that detection of intraluminal recurrence while patients are asymptomatic is related
to better resectability and survival rate. Patients with
left-sited tumor in the advanced stage have a higher risk of developing recurrent intraluminal disease.
More than one-half of metachronous lesions arose within the first 24 months. Therefore, there is a need for more sensitive and direct examination, which is provided by colonoscopy and must be performed
within the first 12 to 15 months after the operation,
whereas an interval of 24 months be tween each ex
amination seems sufficient to guarantee early detec-
tion of metachronous lesions. Serial tumor marker
evaluation is helpful in earlier diagnosis of local re- currences.
REFERENCES
1. Barillari P, Ramacciato G, De Angelis R, et al. Effect of preoperative colonoscopy on the incidence of synchro- nous and metachronous neoplasms. Acta Chit Scand 1990; 156:163-6.
2. Carlsson G, Petrelli JN, Nava H, Herrera L, Mittelman A. The value of colonoscopic surveillance after curative resection for colorectal cancer or synchronous adeno- matous polyps. Arch Surg 1987;122:1261-3.
3. Carlsson G, Petrelli JN, Nava H, Herrera L, Mittelman A. Endoscopic surveillance of patients following curative resection for colorectal cancer. J Surg Oncol 1988;38: 80-2.
4, Evers BM, Mullins RJ, Matthews TH, Broghamer WL, Polk HC Jr. Multiple adenocarcinomas of the colon and rectum: an analysis of incidence and current trends. Dis Colon Rectum 1988;31:518-22.
5. Kiefer PJ, Thorson AG, Christensen MA. Metachronous colorectal cancer: time interval to presentation of a meta- chronous cancer. Dis Colon Rectum 1986;29:378-82.
6. Lee TK, Barringer M, Meyers T, Sterchi JM. Multiple primary carcinomas of the colon and associated extra- colonic primary malignant tumors. Ann Surg 1982;195: 501-7.
7. Luchtefeld MA, Ross DS, Zander JD, Folse JR. Late development of metachronous colorectal cancer. Dis Colon Rectum 1987;30:180-4.
8. Berge I, Ekelund C, Mellner BP. Carcinoma of the colon and rectum in a defined population: an epidemiological clinical and post mortem investigation of colorectal can- cer and coexisting polyps in Malmo Sweden. Acta Chir Scand 1972;438:1-86.
9. Lautenbach E, Forde K, Neugut A. Benefits of colonos- copy surveillance after curative resection of colorectal cancer. Ann Surg t994;220:206-11.
10. Rodriguez-Bigas MA, Stulc JP, Davidson B, Petrelli NJ. Prognostic significance of anastomotic recurrence from colorectal adenocarcinoma. Dis Colon Rectum 1992;35: 838-42.
11. Byrd RL, Boggs HW Jr, Slagle GW, Cole PA. Reliability of colonoscopy. Dis Colon Rectum 1989;32:1023-5.
12. Fowler DL, Hedberg SE. Follow-up colonoscopy after polypectomy [abstract. Gastrointest Endosc 1980;19:
655-9. 13. Holtzman R, Poulard JB, Bank S, et al. Repeat colonos-
copy after endoscopic polypectomy. Dis Colon Rectum 1987;30:185-8.
14. Islet JT, Brown PC, Lewis FG, Billingham RP. The role
Vol 39, 4
of preoperative colonoscopy in colorectal cancer. Dis Colon Rectum 1987;30:435-9.
15. Reilly JC, Rusin LC, Theuerkauf FJ Jr. Colonoscopy: its role in cancer of the colon and rectum. Dis Colon Rectum 1982;25:532-8.
16. Juhl G, Larson MG, Mullins R, Bond S, Polk CH. SL'v-year results of annual colonoscopy after resection of colo- rectal cancer. World J Surg 1990;14:255-61.
17. Williams CB, Hunt RH, Loose H, Riddel RH, Sakay Y, Swarbit ET. Colonoscopy in the management of colon polyps. Br J Surg 1974;61:673-82.
18. Woolfson IK, Eckholdt GJ, Wetzel CR, et al. Usefulness of performing colonoscopy one year after endoscopic polypectomy. Dis Colon Rectum 1990;33:389-93.
19. Pagana TJ, Ledesma ES, Mittelman A, Nava HR. The use of colonoscopy in the study of synchronous colorectal neoplasms. Cancer 1984;53:356-9.
SURVEILLANCE OF COLORECTAL CANCER 393
20. Dasmahapatra KS, Lopyan K. Rationale for agressive colonoscopy in patients with colorectal neoplasia. Arch Surg 1989;124:63-6.
21. Larson MG, Bond JS, Shallcross C, Mullins R, Polk CH. Colonoscopy after curative resection of colorectal can- cer. Arch Surg 1986;121:535~40.
22. Barkin JS, Cohen ME, Flaxman M, et al. Value of a routine follow-up endoscopy program for the detection of recurrent colorectal carcinoma. Am J Gastroenterol 1988;88:1355-60.
23. Buhler H, Seefeld U, Deyle P, et aL Endoscopic fol- low-up after colorectal cancer surgery. Cancer 1984;54: 791-3.
24. Barillari P, Bolognese A, Chirletti P, Cardi M, Sammartino P, Stipa V. Role of CEA, TPA, and Ca 1:9-9 in the early detection of localized and diffuse recurrent rectal cancer. Dis Colon Rectum 1992;35:471-6.
XVIth Biennial of the
International Society Colon and Rectal
Congress
of University Surgeons
Lisbon, Portugal April 14-18, 1996