-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
1/18
2012 MFMER | slide-1/21
Workflow-based Data Reconciliation for
Clinical Decision Support: Case of
Colorectal Cancer Screening andSurveillance
Kavishwar Wagholikar, MBBS PhD1, Sunghwan Sohn, PhD1,
Stephen Wu, PhD1,Vinod Kaggal1, Sheila Buehler, RN CNP2,
Robert A. Greenes, MD PhD3,8, Tsung-Teh Wu, MD4,David Larson, MD
MBA5, Hongfang Liu, PhD1,
Rajeev Chaudhry, MBBS MPH6, Lisa Boardman, MD7
1Biomedical Statistics and Informatics, 2Internal
Medicine,4Anatomic Pathology, 5Colon and Rectal Surgery, 6Primary
Care
Internal Medicine, 7Gastroenterology and Hepatology,
Mayo Clinic Rochester, MN3Biomedical Informatics, Arizona State
University, Scottsdale, AZ;
8Health Science Research, Mayo Clinic, Scottsdale, AZ
AMIA-CRI 2013,
San Francisco CA,
21 March 2013
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
2/18
2012 MFMER | slide-2/21
CDSS
Data quality
Workflow analysis
Data reconciliation
Formative evaluation
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
3/18
2012 MFMER | slide-3/21
Data Quality and CDS
Deficient data quality can impact the clinical
decisions and consequently health outcomes
Data quality: completeness, accuracy,
Stetson et al. Assessing Electronic Note Quality Using the
Physician Documentation Quality Instrument
(PDQI-9). Appl Clin Inform. 2012;3(2):164-74.
Weiskopf et al. Methods and dimensions of electronic health
record data quality assessment: enabling
reuse for clinical research. J Am Med Inform Assoc. 2012 Jun
25.
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
4/18
2012 MFMER | slide-4/21
Data quality and data use
Factors influencing data quality:
motivation or purpose for the document
time available for documentation
use of schemas
expertise and qualifications of the documenter
documentation tools
Deeper understanding of the document is critical todetermine if
the data is suitable for a particular task.
e.g. diagnostic coding by abstractors for insurancereimbursement
lack sufficient accuracy and completenessfor clinical decision
making.
Reiser SJ. The clinical record in medicine. Part 2: Reforming
content and purpose. Ann Intern Med. 1991 Jun
1;114(11):980-5.
Rosenbloom ST, et al. Data from clinical notes: a perspective on
the tension between structure and flexible
documentation. JAMIA. 2011 Mar-Apr;18(2):181-6.
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
5/18
2012 MFMER | slide-5/21
Workflow study to determine data quality
use workflow analysis :
i) to identify data sources
ii) and to design data reconciliation processes
in a CDSS for colorectal cancer prevention
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
6/18
2012 MFMER | slide-6/21
Challenges for the CRC CDSS
i) several parameters and logical decision stepsare involved
ii) the documentation is of inadequate quality or
iii) is in free-text form
iv) high degree of decision accuracy
Wagholikar K, et al. Clinical Decision Support for Colonoscopy
Surveillance Using Natural Language Processing. IEEE
Healthcare Informatics, Imaging, and Systems Biology Conference.
University of California, San Diego, CA; 2012.
http://dx.doi.org/10.1109/HISB.2012.11http://dx.doi.org/10.1109/HISB.2012.11http://dx.doi.org/10.1109/HISB.2012.11http://dx.doi.org/10.1109/HISB.2012.11http://dx.doi.org/10.1109/HISB.2012.11http://dx.doi.org/10.1109/HISB.2012.11
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
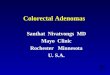
7/18
h/o IBD
CRCancer
yes
Colonoscopy.
Preparation
poor,
inadequate
Repeat in 1 or 2
days
PolypType
adequate,
good,
excellentno
hyperplastic
Adenomatous:
tubular, serrated
adenomaAdenomatous:
tubulovillous,
villous, SSA
Risk
Colonoscopy now
no
yes
>=40y
>=50yAge
Age Colonoscopy now
h/o CRCancer
Colonoscopy at 3yrs after thetime CRcancer was detected
no
yes IBD-consult if no
addendum
no
yes GI consult
no
h/o CRC
=1yr
1 year
Hyperplastic
polyp
group2group1
RecentCRPath is recent
Colorectal Endoscopy Pathology
Recommendation for colonoscopy are
indicated in years from Recent CRPath
CRrisk
10y 5y
no yes
>=50y && =40y
Age atRecent
cololoscopy
+10y
Age at Recentcolonoscopy
+5y
h/o CRCancer
no
yes
3y
h/o CRCsyndromeyes GI-consult if no
addendum
no
8h/o CRC
since
no
yes
Recent.Poylpyes
Recurrentloop
=10 monthsTimeSincePreviousColonoscopy (withadequate prep)
Recent
Colonoscopy.
Time
reportAbsent
>0 years
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
8/182012 MFMER | slide-8/21
Methods
Studied workflow analysis
Designed several processes for data reconciliation
To determine the utility of these processes,quantitative
analysis after selectively
adding/removing each of reconciliation processes.Two
parameters:
i. accuracy gain of the patient parameter reconciledby the
process, and
ii. accuracy gain of the recommendations computedby the
CDSS.
106 cases
Unertl KM,et al. Traversing the many paths of workflow research:
developing a conceptual framework of workflow
terminology through a systematic literature review. JAMIA. 2010
May-Jun;17(3):265-73.
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
9/18
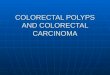
Demographics
Coded Problem List
Free text Problem section
in Clinical notes
Coded Patient response
Questionnaire System
Pathology report
templatized free-text
Endoscopists dictated
free-text procedure note
GI Dept.
system
Pathology dept. system
findings
indications
Patient
RFID tag on biopsy
Referring
Care
provider
EHR
Endoscopist
R.Nurse
Pathologist
during procedure
before procedure
Care
providers
Annual
Questionnaire
Registration
Previous
Hospital Visits
Colonoscopy
visit
Biopsy
specimen
CDSS
Natural Language
Processing
Structured Data
Guideline rules
Recommendation
Data reconciliation
Workflow
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
10/182012 MFMER | slide-10/21
Colonoscopy
TV
TV
Clipart from Microsoft Office
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
11/182012 MFMER | slide-11/21
Colonoscopy
Structured event information
Specimen label
TV
TV
20-30 mins
Clipart from Microsoft Office
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
12/182012 MFMER | slide-12/21
Colonoscopy
Endoscopy
dictation
TV
TV
Clipart from Microsoft Office
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
13/182012 MFMER | slide-13/21
Results
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
14/182012 MFMER | slide-14/21
Conventionally, software engineering practicesinvolve workflow
studies, when the software isprimarily for workflow support.
Our study demonstrates that when there is lackof adequate data
quality, workflow studies of thedocumentation phase can help
discover datareconciliation strategies that can resolve the
data deficiencies
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
15/182012 MFMER | slide-15/21
Lack of NLP sensitivity can be overcome withmulti-source data
reconciliation. e.g. NLP on theendoscopy note for polyp size was
effectivewhen supplemented with structured GI findings.
Findings of the workflow analysis obviated thelaborious effort
to develop NLP for someinformation. e.g. the RNs structured
recording
obviated NLP for detecting number of polypsfrom endoscopy
note.
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
16/182012 MFMER | slide-16/21
Conclusion
Workflow analysis was useful to identify datareconciliation
strategies to addressdocumentation gaps, which improved
CDSSperformance.
Workflow-based data reconciliation can play animportant role in
designing new-generationCDSS based on complex guideline models
and
NLP.
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
17/182012 MFMER | slide-17/21
Questions
Contact and related resources: waghskATgmail.com
http://scholar.google.com/citations?user=_MlaqMsAAAAJ&hl=enhttp://scholar.google.com/citations?user=_MlaqMsAAAAJ&hl=en
-
7/28/2019 Workflow-Based Data Reconciliation for Clinical
Decision Support-Case of Colorectal Cancer Screening and
Surveillance
18/18
References
Stetson et al. Assessing Electronic Note Quality Using the
Physician Documentation Quality Instrument (PDQI-9).Appl Clin
Inform. 2012;3(2):164-74.
Weiskopf et al. Methods and dimensions of electronic health
record data quality assessment: enabling reuse forclinical
research. J Am Med Inform Assoc. 2012 Jun 25
Reiser SJ. The clinical record in medicine. Part 2: Reforming
content and purpose. Ann Intern Med. 1991 Jun1;114(11):980-5.
Rosenbloom ST, et al. Data from clinical notes: a perspective on
the tension between structure and flexibledocumentation. J Am Med
Inform Assoc. 2011 Mar-Apr;18(2):181-6.
Unertl KM,et al. Traversing the many paths of workflow research:
developing a conceptual framework of workflowterminology through a
systematic literature review. J Am Med Inform Assoc. 2010
May-Jun;17(3):265-73.
Wagholikar K, et al. Clinical Decision Support for Colonoscopy
Surveillance Using Natural Language Processing.IEEE Healthcare
Informatics, Imaging, and Systems Biology Conference. University of
California, San Diego, CA;2012.
Wagholikar K, et al. Clinical decision support with automated
text processing for cervical cancer screening. J AmMed Inform
Assoc. 2012; 19 (5), 833-839,
Wagholikar K ,et al. Formative evaluation of the accuracy of a
clinical decision support system for cervical cancerscreening. J Am
Med Inform Assoc. 2013. (in press)
http://dx.doi.org/10.1109/HISB.2012.11http://dx.doi.org/10.1109/HISB.2012.11http://dx.doi.org/10.1109/HISB.2012.11http://www.ncbi.nlm.nih.gov/pubmed/22542812http://www.ncbi.nlm.nih.gov/pubmed/22542812http://jamia.bmj.com/content/early/2013/04/04/amiajnl-2013-001613.fullhttp://jamia.bmj.com/content/early/2013/04/04/amiajnl-2013-001613.fullhttp://jamia.bmj.com/content/early/2013/04/04/amiajnl-2013-001613.fullhttp://jamia.bmj.com/content/early/2013/04/04/amiajnl-2013-001613.fullhttp://jamia.bmj.com/content/early/2013/04/04/amiajnl-2013-001613.fullhttp://jamia.bmj.com/content/early/2013/04/04/amiajnl-2013-001613.fullhttp://jamia.bmj.com/content/early/2013/04/04/amiajnl-2013-001613.fullhttp://www.ncbi.nlm.nih.gov/pubmed/22542812http://www.ncbi.nlm.nih.gov/pubmed/22542812http://www.ncbi.nlm.nih.gov/pubmed/22542812http://www.ncbi.nlm.nih.gov/pubmed/22542812http://www.ncbi.nlm.nih.gov/pubmed/22542812http://www.ncbi.nlm.nih.gov/pubmed/22542812http://www.ncbi.nlm.nih.gov/pubmed/22542812http://www.ncbi.nlm.nih.gov/pubmed/22542812http://www.ncbi.nlm.nih.gov/pubmed/22542812http://www.ncbi.nlm.nih.gov/pubmed/22542812http://dx.doi.org/10.1109/HISB.2012.11http://dx.doi.org/10.1109/HISB.2012.11http://dx.doi.org/10.1109/HISB.2012.11http://dx.doi.org/10.1109/HISB.2012.11http://dx.doi.org/10.1109/HISB.2012.11http://dx.doi.org/10.1109/HISB.2012.11