Embed Size (px)
Citation preview
BritishJournal ofOphthalmology, 1991,75,698-701
Intraocular involvement with subretinal pigmentepithelium infiltrates by mycosis fungoides
Barbara C Erny, Peter R Egbert, Irene M Peat, K Shorrock, A Ralph Rosenthal
AbstractWe report a case of intraocular mycosisfungoides in a 48-year-old man. The patientpresented with decreased visual acuity, whitesubretinal lesions, and vitritis. Post-mortemhistopathology revealed malignant T cell in-filtrates consistent with mycosis fungoides inthe retina, vitreous, and between the retinalpigment epithelium (RPE) and Bruch's mem-brane. Focal atrophy of the RPE, along withthe sub-RPE infiltrates, correlated with theclinically visible fundus lesions.
Mycosis fungoides is a cutaneous T celllymphoma, which can progress to generaliseddisease. ' It commonly presents with a long phaseof 'premycotic' skin lesions. These progress topatches on the skin, which may or may notbecome plaques, and eventually tumours.2 Theclinical course of skin involvement varies fromchronic to rapidly progressive, and is unpredict-able.3 Systemic involvement is late in the courseof the disease, and usually involves the lymphnodes, liver, spleen, and/or central nervoussystem.4 Because the majority of patientsdevelop the disease between the ages of 40 and60, many of them die of unrelated causes beforethe disease becomes widespread.
Eyelid and conjunctival involvement is notunusual in the course of mycosis fungoides.'Other external ocular involvement has beenreported, including cornea,6 caruncle,7 sclera,6and orbit.8 Intraocular lesions are rare, and onlya few individual cases have been reported. Onlyone of the previous reports records both theclinical and pathological appearance of intra-ocular mycosis fungoides.9We present here a patient followed up closely
for an ocular disease that resembled fungalendophthalmitis but was histologically proved tobe mycosis fungoides.
left. The left eye showed anterior uveitis, andsevere vitritis with active retinitis in the posteriorpole (Fig 2). The left eye had also developed aconjunctival perilimbal nodular yellow infiltrate(Fig 3). A presumed diagnosis of candida chorio-retinitis was made, and the patient was treatedwith intravitreal amphotericin and oral keto-conazole. Cultures and stains of vitreous biopsieswere negative, and oral ketocanazole was con-tinued. By 5 December the right eye alsodeveloped a small white lesion in the macula(Fig 4), a limbal lesion, and conjunctivalinfiltrates.At the same time the patient was admitted to
hospital for control of pain and a newly dis-covered left sided abdominal mass. He died on21 December 1989, with a diagnosis of mycosisfungoides and widespread lymphoma.
POST MORTEM FINDINGSThe body was covered with numerous crustingskin lesions up to 2 cm in diameter. There wasevidence of extensive involvement of the lymphnodes by lymphoma, which also appeared to beinfiltrating retroperitoneal tissues.
Stanford UniversityDepartment ofOphthalmology,Stanford, California,USAB C ErnyP R Egbert
Leicester RoyalInfirmary, Leicester,EnglandI M PeatK ShorrockA R RosenthalCorrespondence to:Barbara C Erny, MD, StanfordUniversity Department ofOphthalmology, Room A-157,Stanford University MedicalCenter, Stanford, California94305, USA.Accepted for publication4 April 1991
Case reportThe patient was a 48-year-old white man knownto have had mycosis fungoides for 30 years. Hehad disseminated skin lesions for which hereceived topical steroids, psoralen and ultra-violet light (PUVA), superficial x ray therapy,and in 1989 intermittent oral chlorambucil(Leukerad). In 1983 he had undergone surgeryfor a subarachnoid haemorrhage.On 1 November 1989 the patient complained
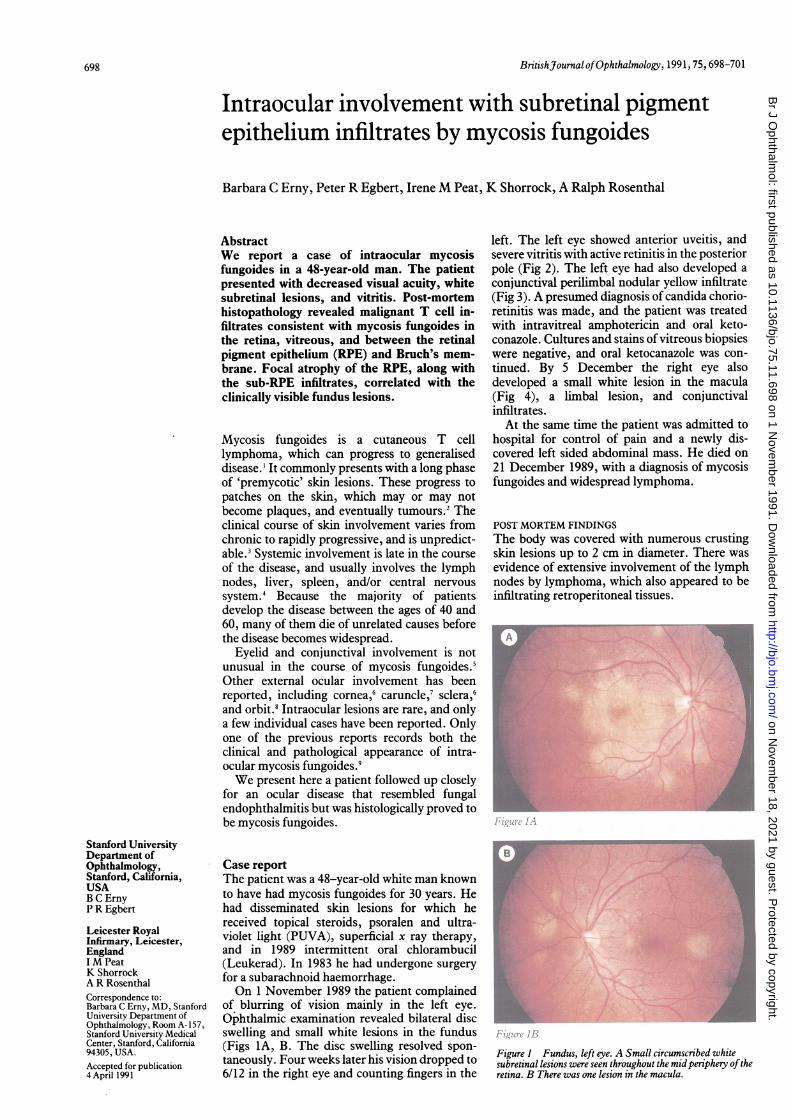
of blurring of vision mainly in the left eye.Ophthalmic examination revealed bilateral discswelling and small white lesions in the fundus(Figs 1A, B. The disc swelling resolved spon-taneously. Four weeks later his vision dropped to6/12 in the right eye and counting fingers in the
Figure I Fundus, left eye. A Small circumscribed whitesubretinal lesions were seen throughout the mid periphery oftheretina. B There was one lesion in the macula.
698
on Novem
ber 18, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.75.11.698 on 1 Novem
ber 1991. Dow
nloaded from
Intraocular involvement with subretinal pigment epithelium infiltrates by mycosisfungoides
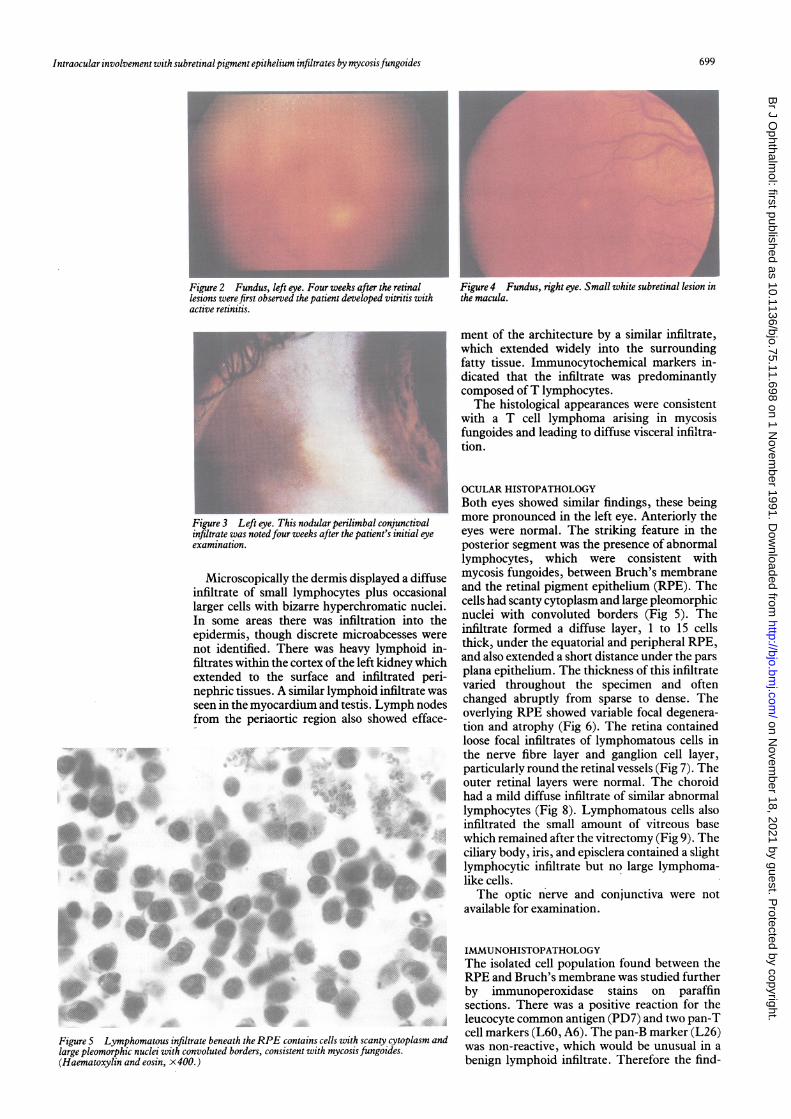
Figure 2 Fundus, left eye. Four weeks after the retinallesions were first observed the patient developed vitritis withactive retinitis.
Figure 3 Left eye. This nodular perilimbal conjunctivalinfiltrate was notedfour weeks after the patient's initial eyeexamination.
Microscopically the dermis displayed a diffuseinfiltrate of small lymphocytes plus occasionallarger cells with bizarre hyperchromatic nuclei.In some areas there was infiltration into theepidermis, though discrete microabcesses werenot identified. There was heavy lymphoid in-filtrates within the cortex ofthe left kidney whichextended to the surface and infiltrated peri-nephric tissues. A similar lymphoid infiltrate wasseen in the myocardium and testis. Lymph nodesfrom the periaortic region also showed efface-
........~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~....
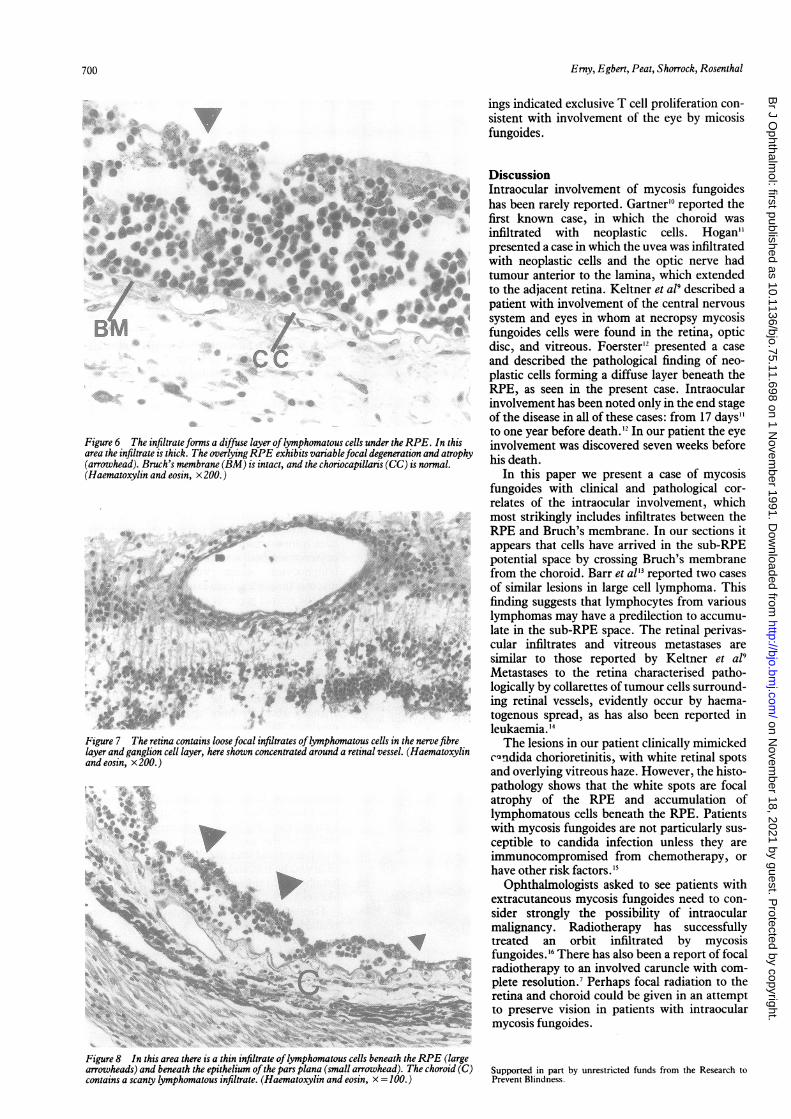
Figure 5 Lymphomatous infiltrate beneath theRPE contains cells with scanty cytoplasm andlarge pleomorphic nuclei with convoluted borders, consistent with mycosis fungoides.(Haematoxylin and eosin, x 400.)
Figure 4 Fundus, right eye. Small white subretinal lesion inthe macula.
ment of the architecture by a similar infiltrate,which extended widely into the surroundingfatty tissue. Immunocytochemical markers in-dicated that the infiltrate was predominantlycomposed ofT lymphocytes.The histological appearances were consistent
with a T cell lymphoma arising in mycosisfungoides and leading to diffuse visceral infiltra-tion.
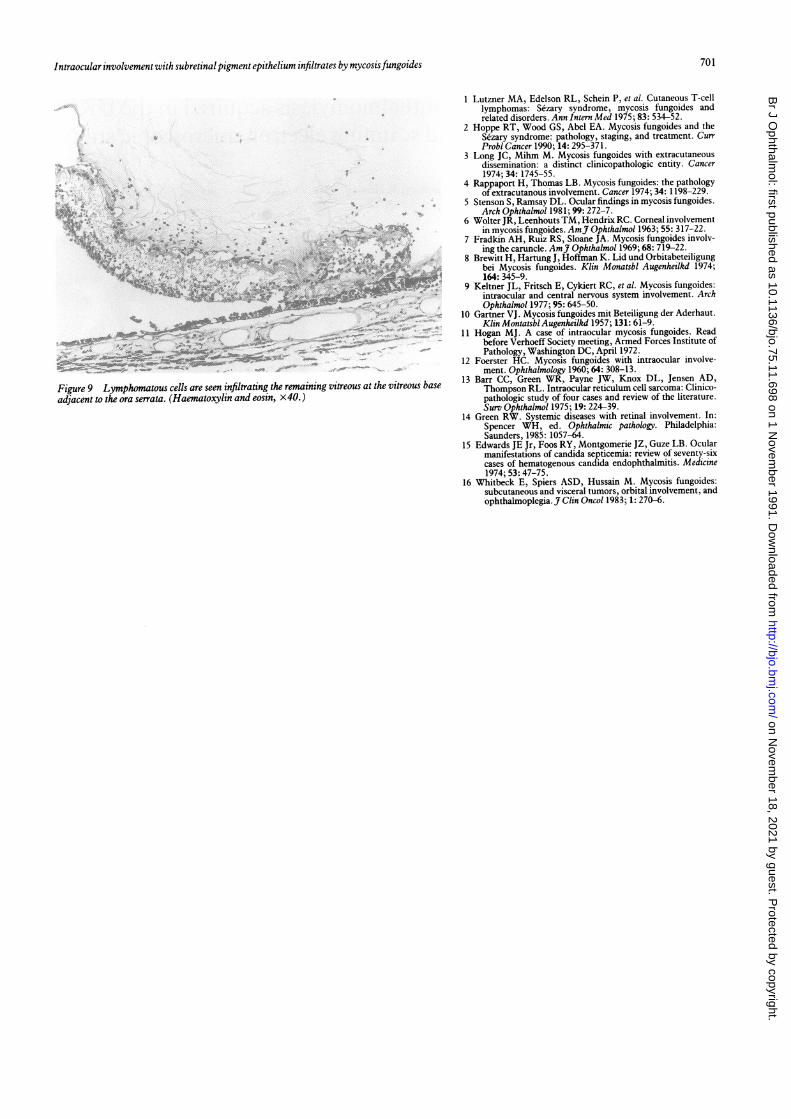
OCULAR HISTOPATHOLOGYBoth eyes showed similar findings, these beingmore pronounced in the left eye. Anteriorly theeyes were normal. The striking feature in theposterior segment was the presence of abnormallymphocytes, which were consistent withmycosis fungoides, between Bruch's membraneand the retinal pigment epithelium (RPE). Thecells had scanty cytoplasm and large pleomorphicnuclei with convoluted borders (Fig 5). Theinfiltrate formed a diffuse layer, 1 to 15 cellsthick, under the equatorial and peripheral RPE,and also extended a short distance under the parsplana epithelium. The thickness of this infiltratevaried throughout the specimen and oftenchanged abruptly from sparse to dense. Theoverlying RPE showed variable focal degenera-tion and atrophy (Fig 6). The retina containedloose focal infiltrates of lymphomatous cells inthe nerve fibre layer and ganglion cell layer,particularly round the retinal vessels (Fig 7). Theouter retinal layers were normal. The choroidhad a mild diffuse infiltrate of similar abnormallymphocytes (Fig 8). Lymphomatous cells alsoinfiltrated the small amount of vitreous basewhich remained after the vitrectomy (Fig 9). Theciliary body, iris, and episclera contained a slightlymphocytic infiltrate but no large lymphoma-like cells.The optic nerve and conjunctiva were not
available for examination.
IMMUNOHISTOPATHOLOGYThe isolated cell population found between theRPE and Bruch's membrane was studied furtherby immunoperoxidase stains on paraffinsections. There was a positive reaction for theleucocyte common antigen (PD7) and two pan-Tcell markers (L60, A6). The pan-B marker (L26)was non-reactive, which would be unusual in abenign lymphoid infiltrate. Therefore the find-
699
on Novem
ber 18, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.75.11.698 on 1 Novem
ber 1991. Dow
nloaded from
Erny, Egbert, Peat, Shorrock, Rosenthal
ings indicated exclusive T cell proliferation con-sistent with involvement of the eye by micosisfungoides.
4,~~~~~~~~"
;,... .. 1, }
F
*eoh,t~
MP ..* .SR....
4 A
*.1 -!
Figure 6 The infiltrate forms a diffuse layer oflymphomatous cells under the RPE. Itarea the infiltrate is thick. The overlyingRPE exhibits variablefocal degeneration and i
(arrowhead). Bruch's membrane (BM) is intact, and the choriocapillaris (CC) is norms(Haematoxylin and eosin, x 200.)
4t
* .;!bi. ir
r j 1.:: r ,:
3
Sty* I 8 ;>F frill +
ial ... ..i;..A~~~~~~y~
Figure 7 The retina contains loosefocal infiltrates oflymphomatous cells in the nerve)layer and ganglion cell layer, here shown concentrated around a retinal vessel. (Haemaiand eosin, x 200. )
*.: .- .-
-.';-t Y :J
Figure 8 In this area there is a thin infiltrate oflymphomatous cells beneath the RPEarrowheads) and beneath the epithelium ofthe pars plana (small arrowhead). The chotcontains a scanty lymphomatous infiltrate. (Haematoxylin and eosin, x = 100.)
DiscussionO. Intraocular involvement of mycosis fungoides
has been rarely reported. Gartner'0 reported thefirst known case, in which the choroid was
infiltrated with neoplastic cells. Hogan"presented a case in which the uvea was infiltratedwith neoplastic cells and the optic nerve had
is* tumour anterior to the lamina, which extendedto the adjacent retina. Keltner et al' described a
patient with involvement of the central nervous
system and eyes in whom at necropsy mycosisfungoides cells were found in the retina, opticdisc, and vitreous. Foerster'2 presented a case
and described the pathological finding of neo-
plastic cells forming a diffuse layer beneath theRPE, as seen in the present case. Intraocularinvolvement has been noted only in the end stageof the disease in all of these cases: from 17 days"to one year before death.'2 In our patient the eye
this involvement was discovered seven weeks beforeatrohaophy his death.
In this paper we present a case of mycosisfungoides with clinical and pathological cor-
relates of the intraocular involvement, whichmost strikingly includes infiltrates between theRPE and Bruch's membrane. In our sections itappears that cells have arrived in the sub-RPEpotential space by crossing Bruch's membranefrom the choroid. Barr et al" reported two cases
of similar lesions in large cell lymphoma. Thisfinding suggests that lymphocytes from variouslymphomas may have a predilection to accumu-late in the sub-RPE space. The retinal perivas-cular infiltrates and vitreous metastases are
similar to those reported by Keltner et a19Metastases to the retina characterised patho-logically by collarettes of tumour cells surround-ing retinal vessels, evidently occur by haema-togenous spread, as has also been reported inleukaemia. 14
fibre The lesions in our patient clinically mimickedtoxylin cQndida chorioretinitis, with white retinal spots
and overlying vitreous haze. However, the histo-pathology shows that the white spots are focalatrophy of the RPE and accumulation oflymphomatous cells beneath the RPE. Patientswith mycosis fungoides are not particularly sus-
ceptible to candida infection unless they are
immunocompromised from chemotherapy, or
have other risk factors. '1Ophthalmologists asked to see patients with
extracutaneous mycosis fungoides need to con-
sider strongly the possibility of intraocularmalignancy. Radiotherapy has successfullytreated an orbit infiltrated by mycosisfungoides. 16 There has also been a report of focalradiotherapy to an involved caruncle with com-
plete resolution.7 Perhaps focal radiation to theretina and choroid could be given in an attemptto preserve vision in patients with intraocular
He -~ mycosis fungoides.
(largeroid (C) Supported in part by unrestricted funds from the Research to
Prevent Blindness.
It
700
P.,
lk,jp
:7
-
,. S_
on Novem
ber 18, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.75.11.698 on 1 Novem
ber 1991. Dow
nloaded from
Intraocular involvement with subretinal pigment epithelium infiltrates by mycosisfungoides
-#~~~~~~~~~~~~~~~~~~~~~~~.444
~~~~~~~~~~.*'r't""'3! -':
Figure 9 Lymphomatous cells are seen infiltrating the remaining vitreous at the vitreous baseadjacent to the ora serrata (Haematoxylin and eosin, x40.)
1 Lutzner MA, Edelson RL, Schein P, et al. Cutaneous T-celllymphomas: S6zary syndrome, mycosis fungoides andrelated disorders. Ann Intern Med 1975; 83: 534-52.
2 Hoppe RT, Wood GS, Abel EA. Mycosis fungoides and theS6zary syndrome: pathology, staging, and treatment. CurrProbl Cancer 1990; 14: 295-371.
3 Long JC, Mihm M. Mycosis fungoides with extracutaneousdissemination: a distinct clinicopathologic entity. Cancer1974; 34: 1745-55.
4 Rappaport H, Thomas LB. Mycosis fungoides: the pathologyof extracutanous involvement. Cancer 1974; 34: 1198-229.
5 Stenson S, Ramsay DL. Ocular findings in mycosis fungoides.Arch Ophthalmol 1981; 99: 272-7.
6 Wolter JR, Leenhouts TM, Hendrix RC. Corneal involvementin mycosis fungoides. AmJ7 Ophthalmol 1963; 55: 317-22.
7 Fradkin AH, Ruiz RS, Sloane JA. Mycosis fungoides involv-ing the caruncle. AmJ7 Ophthalmol 1969; 68: 719-22.
8 Brewitt H, Hartung J, Hoffman K. Lid und Orbitabeteiligungbei Mycosis fungoides. Klin Monatsbl Augenheilkd 1974;164: 345-9.
9 Keltner JL, Fritsch E, Cykiert RC, et al. Mycosis fungoides:intraocular and central nervous system involvement. ArchOphthalmol 1977; 95: 645-50.
10 Gartner VJ. Mycosis fungoides mit Beteiligung der Aderhaut.Klin Montatsbl Augenheilkd 1957; 131: 61-9.
11 Hogan MJ. A case of intraocular mycosis fungoides. Readbefore Verhoeff Society meeting, Armed Forces Institute ofPathology, Washington DC, April 1972.
12 Foerster HC. Mycosis fungoides with intraocular involve-ment. Ophthalmology 1960; 64: 308-13.
13 Barr CC, Green WR, Payne JW, Knox DL, Jensen AD,Thompson RL. Intraocular reticulum cell sarcoma: Clinico-pathologic study of four cases and review of the literature.Surv Ophthalmol 1975; 19: 224-39.
14 Green RW. Systemic diseases with retinal involvement. In:Spencer WH, ed. Ophthalmic pathology. Philadelphia:Saunders, 1985: 1057-64.
15 Edwards JE Jr, Foos RY, Montgomerie JZ, Guze LB. Ocularmanifestations of candida septicemia: review of seventy-sixcases of hematogenous candida endophthalmitis. Medicine1974; 53: 47-75.
16 Whitbeck E, Spiers ASD, Hussain M. Mycosis fungoides:subcutaneous and visceral tumors, orbital involvement, andophthalmoplegia. J Clin Oncol 1983; 1: 270-6.
701
on Novem
ber 18, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.75.11.698 on 1 Novem
ber 1991. Dow
nloaded from





























