Childhood Onset Schizophrenia and other Psychotic Disorders, and
Substance Abuse Disorder
Childhood Onset Schizophrenia And Other Psychotic DisordersAnne
Cristine D. Guevarra, MDChild Psychiatry Rotator
Children and adolescents experience the same range and types of
psychotic symptoms as do adults. They can lose the connections
between their thoughts (formal thought disorder) and have
perceptions without external stimuli (hallucinations).
Psychosis Mental life has been disrupted in its capacities or
forms, as a result of a process that generates new forms of
psychological experience.McHugh PR, Slavney PR. The perspectives of
psychiatry. Baltimore:Johns Hopkins University Press, 1998.The
appearance of psychotic symptoms in childhood, albeit rare, is an
important clinical entity. This importance extends beyond their
clinical prevalence and has begun to influence our understanding of
the principal psychotic conditions.What does it mean when a child
reports experiencing hallucinations or delusions?When one examines
a 5-year old child who claims that he is superman and can fly, the
challenge is to determine whether the child has a delusion.
Similarly, in a child who complains about hearing a voice telling
her to do bad things, one must determine whether she is talking
about her conscience or is experiencing auditory
hallucinations.From a cognitive and developmental standpoint,
certain clinical features in children create diagnostic challenges.
One problem is distinguishing true psychotic phenomena in children
from nonpsychotic idiosyncratic thinking, perceptions caused by
developmental delays, exposure to disturbing and traumatic events,
and overactive and vivid imaginations.Organic PsychosesNeurologic
ConditionsSeizure DisorderDeteriorative Neurologic DisordersCentral
Nervous System LesionsMetabolic and Hormonal DisturbancesToxic
Psychoses
Functional PsychosesChildhood Onset SchizophreniaMood
DisordersBrief Reactive PsychosisAnxiety DisordersClinician-Rated
Dimensions ofPsychosis Symptom Severity
Instead, an eight-symptom Clinician-Rated Dimensions of
PsychosisSymptom Severity scale for determining severity of
psychosis across many psychotic illnesses is included in Section
III of the DSM-5.Symptom domains rated in this scale include the
following: hallucinations, delusions, disorganized speech, abnormal
psychomotor behavior,negative symptoms (restricted emotional
expression or avolition), impaired cognition, depression, and
mania.
Scoring and InterpretationEach item on the measure is rated on a
5-point scale (O=none; l=equivocal; 2=present, butmild; 3=present
and moderate; and 4=present and severe) with a symptom-specific
definitionof each rating level. The clinician may review all of the
individual's available informationand, based on clinical judgment,
select (by circling) the level that most accuratelydescribes the
severity of the individual's condition. The clinician then
indicates the scorefor each item in the "Score" column
provided.Frequency of UseTo track changes in the individual's
symptom severity over time, the measure may becompleted at regular
intervals as clinically indicated, depending on the stability of
the individual'ssymptoms and treatment status. Consistently high
scores on a particular domainmay indicate significant and
problematic areas for the individual that might warrantfurther
assessment, treatment, and follow-up. Clinical judgment should
guide decisionmaking.8Clinician-Rated Dimensions ofPsychosis
Symptom Severity
Instead, an eight-symptom Clinician-Rated Dimensions of
PsychosisSymptom Severity scale for determining severity of
psychosis across many psychotic illnesses is included in Section
III of the DSM-5.Symptom domains rated in this scale include the
following: hallucinations, delusions, disorganized speech, abnormal
psychomotor behavior,negative symptoms (restricted emotional
expression or avolition), impaired cognition, depression, and
mania.
Scoring and InterpretationEach item on the measure is rated on a
5-point scale (O=none; l=equivocal; 2=present, butmild; 3=present
and moderate; and 4=present and severe) with a symptom-specific
definitionof each rating level. The clinician may review all of the
individual's available informationand, based on clinical judgment,
select (by circling) the level that most accuratelydescribes the
severity of the individual's condition. The clinician then
indicates the scorefor each item in the "Score" column
provided.Frequency of UseTo track changes in the individual's
symptom severity over time, the measure may becompleted at regular
intervals as clinically indicated, depending on the stability of
the individual'ssymptoms and treatment status. Consistently high
scores on a particular domainmay indicate significant and
problematic areas for the individual that might warrantfurther
assessment, treatment, and follow-up. Clinical judgment should
guide decisionmaking.9Factors to ConsiderMisdiagnosis remain due to
symptom overlapAnxiety and stress are probably the most common
causes of hallucinations in preschool children with benign
prognosisPsychotic phenomena in school age children generally tend
to be more persistent, and are more likely to be associated with
drug toxicity or significant mental illnessLewiss Child &
Adolescent Psychiatry: A Comprehensive Textbook 4th
EditionCognitive impairments, particularly impaired concentration
and ability to focus, usually accompany psychosis in children.When
the psychosis is secondary to an organic origin, there is often
accompanying impairment in the sensorium presenting as confusion
and disorientation, as is typical of delirium.shyness, and
disturbances in adaptive social behavior seem to be the first signs
of dysfunctional premorbid developmentEarly language deficits and
motor impairmentsDiagnostic ChallengesDistinguishing true psychotic
phenomena in children from nonpsychotic: idiosyncratic thinking,
perceptions caused by developmental delays, exposure to disturbing
and traumatic events, and overactive and vivid
imaginationsDifferentiating between the premorbid state and the
active psychotic stateDistinguishing true psychotic phenomena in
children from nonpsychotic idiosyncratic thinking, perceptions
caused by developmental delays, exposure to disturbing and
traumatic events, and overactive and vivid imaginations.
12Childhood Psychosis Adult Schizophrenia (?)
Childhood Onset Schizophrenia Adult Schizophrenia
Childhood Onset Schizophrenia = Adult SchizophreniaLewiss Child
& Adolescent Psychiatry: A Comprehensive Textbook 4th
EditionCOS vs Adult SchizophreniaSimilar to that of poor outcome
adult casesPsychosis of COS can usually be distinguished by its
severe and pervasive nature and its nonepisodic, unremitting
courseChildren show poorer premorbid functioning in social, motor,
and language domains, learning disabilities, and disruptive
behavior disordersTransient autistic symptoms such as hand flapping
and echolalia in toddler years are common, probably reflecting more
compromised early brain development.Lewiss Child & Adolescent
Psychiatry: A Comprehensive Textbook 4th EditionHistoryMaudsley
first wrote a description of the insanity of early life in his
textbook, Physiology and Pathology of Minddevelopmental approachthe
mental faculty of children was not organized, and hence the
insanity in children must be of the simplest kind, influenced more
by reason of bad descent or of baneful influences during uterine
life.
15HistoryDe Sanctis may be credited first with setting out
childhood schizophrenia as different from mental deficiency and
from certain neurologic disorders, such as epilepsy or
postinfectious encephalopathyHistoryKraeplin introduced the concept
of dementia praecox and noted its onset in late childhood and
adolescenceSuggested that 3.5% of patients with schizophrenia had
the onset of their illness before the age of 10 years. This led to
an increased interest in understanding the developmental aspects of
psychosis.HistoryThe term psychosis was used so broadly in children
that a spectrum of behavioral disorders and autism were grouped
together under the category of childhood schizophrenia.Before the
1960s, the term childhood psychosis was applied to a heterogeneous
group of children, many of whom exhibited autism spectrumdisorder
symptoms without hallucinations and delusions. In the late 1960s
and 1970s, reports of children with evidence of a profoundpsychotic
disturbance very early in life included observations of
intellectual disabilities, social deficits, and severe
communication andlanguage impairments, and no family history of
schizophrenia. Children whose psychoses emerged after the age of 5
years, however, moreoften exhibited auditory hallucinations,
delusions, inappropriate affect, thought disorder, normal
intellectual function, and a positive familyhistory of
schizophrenia.18HistoryThe landmark studies of Kolvin first
established the clinical distinction between autism and other
psychotic disorders of childhood19HistorySchizophrenia with
childhood onset was formally separated from autistic disorderIn the
1980s, schizophrenia with childhood onset was formally separated
from what was then termed autistic disorder, and currentlytermed
autism spectrum disorder.
20Controversy & Confusion after SeparationResearch
documented a small group of children with autism spectrum disorder
who developed schizophrenia in later childhood or adolescenceMany
children with childhood-onset schizophrenia exhibit
neurodevelopmental abnormalities, some of which are also evident in
children with autism spectrum disorderAccording to the DSM-5,
schizophrenia can be diagnosed in the presence of autism spectrum
disorder, provided that the diagnosis of schizophrenia is
specifically differentiated from autism spectrum disorder.
However, even after the separation of the disorders, controversy
and confusion remained as to the distinctiveness in the long-term
courses ofthese disorders. First, research documented a small group
of children with autism spectrum disorder who developed
schizophrenia in laterchildhood or adolescence. Second, many
children with childhood-onset schizophrenia exhibit
neurodevelopmental abnormalities, some ofwhich are also evident in
children with autism spectrum disorder. Children with autism
spectrum disorder and those with childhood-onsetschizophrenia are
typically impaired in multiple areas of adaptive functioning from
relatively early in life. However, in autism spectrumdisorder, the
onset is almost always before 3 years of age, whereas the onset of
childhood-onset schizophrenia occurs before the age of 13years, but
most often is not recognizable in children until after the age of 3
years. Childhood-onset schizophrenia is signicantly less
frequentthan adolescent-onset or onset in young adulthood, and few
reports document cases of schizophrenia onset before 5 years of
age. Accordingto the DSM-5, schizophrenia can be diagnosed in the
presence of autism spectrum disorder, provided that the diagnosis
of schizophrenia isspecifically differentiated from autism spectrum
disorder.21Early-Onset Schizophreniaonset of disease before the age
of 18 years, including childhood-onset as well as adolescent-onset
schizophreniaassociated with severe clinical course, poor
psychosocial functioning, and increased severity of brain
abnormalitycurrent evidence supports the efficacy of both
psychosocial and pharmacological interventions
Early-onset schizophrenia comprises childhood-onset and
adolescent-onset schizophrenia. Childhood-onset schizophrenia is a
very rare andvirulent form of schizophrenia now recognized as a
progressive neurodevelopmental disorder. Childhood onset is
characterized by a morechronic course, with severe social and
cognitive consequences and increased negative symptoms compared to
adult-onset schizophrenia.Childhood-onset schizophrenia is dened by
an onset of psychotic symptoms before the age of 13 years, believed
to represent a subgroup ofpatients with schizophrenia with an
increased heritable etiology, and evidence of widespread
abnormalities in the development of brainstructures including the
cerebral cortex, white matter, hippocampus and cerebellum. Children
diagnosed with childhood-onset schizophreniahave higher than normal
rates of premorbid developmental abnormalities that appear to be
nonspecic markers of abnormal braindevelopment. Early-onset
schizophrenia is dened as an onset of disease before the age of 18
years, including childhood-onset as well asadolescent-onset
schizophrenia. Early-onset schizophrenia is associated with severe
clinical course, poor psychosocial functioning, andincreased
severity of brain abnormality. Despite the more severe course,
current evidence supports the ecacy of both psychosocial
andpharmacological interventions in the management of
childhood-onset and, particularly, adolescent-onset
schizophrenia.22Childhood-Onset Schizophreniaa very rare and
virulent form of schizophrenia now recognized as a progressive
neurodevelopmental disordermore chronic course, with severe social
and cognitive consequences and increased negative symptoms compared
to adult-onset schizophrenia.onset of psychotic symptoms before the
age of 13 years, increased heritable etiology, and evidence of
widespread abnormalities in the development of brain structures
including the cerebral cortex, white matter, hippocampus and
cerebellum. Have higher than normal rates of premorbid
developmental abnormalities nonspecific markers of abnormal brain
development.a very rare andvirulent form of schizophrenia now
recognized as a progressive neurodevelopmental disorder. Childhood
onset is characterized by a morechronic course, with severe social
and cognitive consequences and increased negative symptoms compared
to adult-onset schizophrenia.Childhood-onset schizophrenia is dened
by an onset of psychotic symptoms before the age of 13 years,
believed to represent a subgroup ofpatients with schizophrenia with
an increased heritable etiology, and evidence of widespread
abnormalities in the development of brainstructures including the
cerebral cortex, white matter, hippocampus and cerebellum. Children
diagnosed with childhood-onset schizophreniahave higher than normal
rates of premorbid developmental abnormalities that appear to be
nonspecic markers of abnormal braindevelopment.23Childhood-Onset
Schizophreniamore significant deficits in measures of intelligence
quotient (IQ), memory, and tests of perceptuomotor skills compared
with adolescent-onset schizophreniaincreased impairment of
cognitive measures such as IQ, working memory, and perceptuomotor
skills premorbid markers of illness rather than sequelae, of the
disorder. Although cognitive impairments are greater in younger
patients with schizophrenia, clinicalpresentation of schizophrenia
remains remarkably similar across the agesthe diagnosis of
childhood-onset schizophrenia is continuous with that in
adolescents and adults, with one exception: In childhood-onset
schizophrenia a failure to achieve expected social and academic
functioning may replace a deterioration in functioning.24Diagnosis
of SchizophreniaActive PhaseAt least one of the following:
delusions, hallucinations, disorganized speechAt least one
additional symptom present most of the time for a month: delusions,
hallucinations, disorganized speech, grossly disorganized or
catatonic behavior, or negative symptoms (i.e. diminished emotional
expression or avolition)Symptoms are present for a significant
amount of time during a single month AND cause impairment (social,
academic, occupational)To meet full criteria for schizophrenia,
continuous signs of disturbance must persist for at least 6
months.To meet full criteria for schizophrenia, continuous signs of
disturbance must persist for at least 6 months. Social, academic,
or occupational impairment must be present. In contrast to previous
diagnostic criteria, the subtypes of schizophrenia (paranoid,
disorganized, catatonic, undifferentiated, and residual) have been
eliminated due to their lack of diagnostic validity and
reliability. Instead, an eight-symptom Clinician-Rated Dimensions
of PsychosisSymptom Severity scale for determining severity of
psychosis across many psychotic illnesses is included in Section
III of the DSM-5.Symptom domains rated in this scale include the
following: hallucinations, delusions, disorganized speech, abnormal
psychomotor behavior,negative symptoms (restricted emotional
expression or avolition), impaired cognition, depression, and
mania.25EpidemiologyFrequency of COS is less than one case in about
40,000 children, whereas among adolescents between the ages of 13
and 18 years, the frequency of schizophrenia is increased by a
factor of at least 50resembles the more severe, chronic, and
treatment-refractory adult-onset schizophrenic subgroups, in that
the same core phenomenological features are presentCo-morbid
disorders: ADHD, depressive disorders, anxiety disorders, speech
& language disorders, motor disturbances
The frequency of childhood-onset schizophrenia is reported to be
less than one case in about 40,000 children, whereas among
adolescentsbetween the ages of 13 and 18 years, the frequency of
schizophrenia is increased by a factor of at least 50.
Schizophrenia with childhoodonset resembles the more severe,
chronic, and treatment-refractory adult-onset schizophrenic
subgroups, in that the same corephenomenological features are
present; however, in childhood-onset schizophrenia, extremely high
rates of comorbidities are present,including
attention-deficit/hyperactivity disorder (ADHD), depressive
disorders, anxiety disorders, speech and language disorders, and
motordisturbances. 26EpidemiologyIn adolescents, the prevalence of
schizophrenia is estimated to be 50 times that in younger children,
with probable rates of 1 tom2 per 1,000. Male 1.67: 1
FemaleSchizophrenia rarely is diagnosed in children younger than 5
years of age. The prevalence of schizophrenia among the parents of
children with schizophrenia is about 8%, which is about twice the
prevalence in the parents of patients with adult-onset
schizophrenia.In adolescents, the prevalence of schizophrenia is
estimated to be 50 times that in younger children, with probable
rates of 1 to2 per 1,000. Boys seem to have a slight preponderance
among children diagnosed with schizophrenia, with an estimated
ratio of about 1.67boys to 1 girl. Boys often become identified at
a younger age than girls do. Schizophrenia rarely is diagnosed in
children younger than 5years of age. The prevalence of
schizophrenia among the parents of children with schizophrenia is
about 8 percent, which is about twice theprevalence in the parents
of patients with adult-onset schizophrenia.27Etiologya
neurodevelopmental disorder
GENES + ENVIRONMENT Abnormal Early Brain Development
white matter abnormalities and disturbances lead to abnormal
connectivityChildhood-onset schizophrenia is a neurodevelopmental
disorder in which complex interactions between genes and the
environment arepresumed to result in abnormal early brain
development. The consequences of the aberrant brain development in
schizophrenia may not befully evident until adolescence or early
adulthood; however, data support the hypothesis that white matter
abnormalities and disturbances inmyelination in childhood, lead to
abnormal connectivity between brain regions. The aberrant
connectivity in various regions of the brain isbelieved to be an
important contributing factor in the psychotic symptoms and
cognitive deficits in childhood-onset schizophrenia.28Genetic
FactorsHeritability estimates at 80%8x more prevalent among first
degree relatives with schizophreniaHigher concordance rates among
monozygotic twins than in dizygotic twinsHigher rates among
relatives of childhood-onset schizophrenia than in adult-onset
schizophreniaNo reliable method can identify persons at the highest
risk for schizophrenia in a given family.Estimates of heritability
for childhood-onset schizophrenia have been as high as 80 percent.
The precise mechanisms of transmission ofschizophrenia are still
not well understood. Schizophrenia is known to be up to eight times
more prevalent among rst-degree relatives ofthose with
schizophrenia than in the general population. Adoption studies of
patients with adult-onset schizophrenia have shown
thatschizophrenia occurs in the biological relatives, not the
adoptive relatives. Additional genetic evidence is supported by
higher concordancerates for schizophrenia in monozygotic twins than
in dizygotic twins. Higher rates of schizophrenia have been
established among relatives ofthose with childhood-onset
schizophrenia than in the relatives of those with adult-onset
schizophrenia.29
MRI Studiesprogressive loss of gray matterdelayed and disrupted
white matter growthdecline in cerebellar volumeGray matter
abnormalities were normalized over time in the siblings, indicating
a protective mechanism in siblings that was not present in those
children with childhood-onset schizophrenia. hippocampal volume
loss across the age span appears to be static among children with
childhood-onset schizophreniaA National Institute of Mental Health
(NIMH) prospective study of more than 100 patients with
childhood-onset schizophrenia and theirtypically developing
siblings has demonstrated progressive loss of gray matter, delayed
and disrupted white matter growth, and a decline incerebellar
volume in those with childhood-onset schizophrenia. Although
siblings of children with childhood-onset schizophrenia alsoshowed
some of these brain disruptions, the gray matter abnormalities were
normalized over time in the siblings, indicating a
protectivemechanism in siblings that was not present in those
children with childhood-onset schizophrenia. Furthermore, the
hippocampal volumeloss across the age span appears to be static
among children with childhood-onset schizophrenia. An MRI NIMH
study of more than 100children with childhood-onset schizophrenia
and their typically developing siblings, studied for about two
decades, documented that inchildhood-onset schizophrenia,
progressive brain gray matter loss occurs continuously over time.
This gray matter shrinkage occurs withventricular increases, with a
pattern of loss originating in the parietal region and proceeding
frontally to dorsolateral prefrontal andtemporal cortices,
including superior temporal gyri. Studies of childhood-onset
schizophrenia at the NIMH provided evidence that early lossof
parietal gray matter followed by frontal and parietal gray matter
loss is more pronounced in childhood-onset schizophrenia than
inschizophrenia with later onset. Other research utilized diusion
tensor images from children with childhood-onset schizophrenia
versuscontrols and found increased diusivities in the posterior
corona radiata in children with childhood-onset schizophrenia,
which implicatedabnormal connectivity with the parietal lobes.
These results contrasted with ndings among subjects with later
onset of schizophrenia inwhom there were more abnormalities in the
frontal lobes.34MRI NIMH StudyAn MRI NIMH study of more than
100children with childhood-onset schizophrenia and their typically
developing siblings, studied for about two decades, documented that
inchildhood-onset schizophrenia, progressive brain gray matter loss
occurs continuously over time. This gray matter shrinkage occurs
withventricular increases, with a pattern of loss originating in
the parietal region and proceeding frontally to dorsolateral
prefrontal andtemporal cortices, including superior temporal gyri.
Studies of childhood-onset schizophrenia at the NIMH provided
evidence that early lossof parietal gray matter followed by frontal
and parietal gray matter loss is more pronounced in childhood-onset
schizophrenia than inschizophrenia with later onset. Other research
utilized diusion tensor images from children with childhood-onset
schizophrenia versuscontrols and found increased diusivities in the
posterior corona radiata in children with childhood-onset
schizophrenia, which implicatedabnormal connectivity with the
parietal lobes. These results contrasted with ndings among subjects
with later onset of schizophrenia inwhom there were more
abnormalities in the frontal lobes.35Phenomenology and Neurobiology
of COSPremorbid Developmenthigher rates of early language, social,
and motor developmental abnormalities, possibly reflecting greater
impairment in early brain developmentLewiss Child & Adolescent
Psychiatry: A Comprehensive Textbook 4th EditionPhenomenology and
Neurobiology of COSRisk FactorsParental Age and Obstetric
Complicationsno correlation with maternal or paternal ageincidence
of obstetric complications in COS patients did not differ from that
for the healthy sibling control groupEye Trackinggenetic factors
underlying eyetracking dysfunction (Smooth pursuit eye movement)
may be more salient for COS than AOSFamilial Schizophrenia Spectrum
Disordersrate of familial schizophrenia spectrum disorders was
higher for COS than AOS, and both were higher than community
controlsFamilial Neurocognitive FunctioningCOS siblings had
significantly poorer performance than community controls, although
the rates of neuropsychological abnormalities for COS were not
significantly higher than for AOSLewiss Child & Adolescent
Psychiatry: A Comprehensive Textbook 4th EditionPervasive
Developmental Disorder and COSPDD in COS may be a nonspecific
marker of more severe early abnormal neurodevelopmentLewiss Child
& Adolescent Psychiatry: A Comprehensive Textbook 4th
EditionNeurocognitive Functioning in COS Probandsperform poorly on
tasks involving fine motor coordination, attention, short-term and
working memoryEvoked-potential studies show diminished amplitude of
brain electrical activity during these tasks, suggesting that
allocation of necessary attentional resources is deficient, which
is also shared by adults with schizophreniathere was no evidence
for a longer term degenerative cognitive process in COS, at least
through early adulthood
Lewiss Child & Adolescent Psychiatry: A Comprehensive
Textbook 4th EditionComorbid Disordersdepression
(54%)obsessive-compulsive disorder (OCD;21%)generalized anxiety
disorder (GAD; 15%)attention deficit hyperactivity disorder (ADHD;
15%)Lewiss Child & Adolescent Psychiatry: A Comprehensive
Textbook 4th EditionBrain Development in COSincreasing ventricular
volume and decreasing total cortical, frontal, medial temporal, and
parietal gray matter volumes at 2, 4, and 6 years after initial
scan
Lewiss Child & Adolescent Psychiatry: A Comprehensive
Textbook 4th EditionWhat is the Pattern of GM Loss in COS and its
Relationship with Normal Development?back to front tissue loss,
with early parietal gray matter loss followed by frontal and
temporal gray matter loss later in adolescencetop-down fashion on
the medial surfaceGM loss in COS may reflect an exaggeration of
normal maturational process of synaptic/dendritic pruning during
adolescenceLewiss Child & Adolescent Psychiatry: A
Comprehensive Textbook 4th EditionDoes the Cortical GM Loss in COS
EventuallyResemble the Adult Onset Pattern when Subjects
Mature?Cortical thickness analyses in adult onset schizophrenia
document GM loss mostly in prefrontal and temporal corticesas COS
subjects mature, the robust and global GM loss during the
adolescent years becomes limited to prefrontal and superior
temporal cortices by age 24, thus mimicking a pattern seen in adult
patientsLewiss Child & Adolescent Psychiatry: A Comprehensive
Textbook 4th Edition
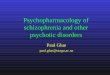
Comparison of the Patterns of Cortical Gray Matter (GM) Loss in
Childhood-Onset Schizophrenia (COS) (Between Ages 12 and 16 Years)
to That Seen in Normal Cortical Maturation (Between Ages 4 and 22
Years). A. Right lateral view of the dynamic sequences of cortical
GM maturation in healthy children between ages 4 and 22 years (n=
13, 54 scans, upper panel) rescanned every 2 years. Scale bar shows
GM amount at each of the 65 536 cortical points across the entire
cortex represented using a color scale (red to pinkmore GM, blueGM
Loss). Cortical GM maturation appears to progress in a
"back-to-front" (parietotemporal) manner.[49]B. Right lateral view
of the dynamic sequence of cortical GM maturation in COS between
ages 12 and 16 years compared with age- and sex-matched healthy
controls (n= 12, 36 scans in each group), where children are
rescanned every 2 years. Dynamic maps representPvalues for the
difference in GM amount between COS and controls at each of the 65
536 cortical points, andPvalues are represented using a color scale
(eg, pink,P< .00002). Cortical GM loss in COS also appears to
follow in a "back-to-front" direction on the lateral surface, thus
suggesting that the COS pattern is an exaggeration of the normal GM
maturation.[50]Asterisk represents data on childhood schizophrenia
only age 1216 years. Adapted fromProc Natl Acad Sci
USA2004;101:8178 andProc Natl Acad Sci USA2001;98:11652.44
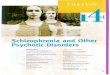
Progression of Cortical Gray Matter (GM) Loss in Childhood-Onset
Schizophrenia (COS) (n= 70, 162 scans) Relative to Age-, Sex-, and
Scan IntervalMatched Healthy Controls (n= 72, 168 Scans) From
Adolescence to Young Adulthood (age 1224 years). Analyses were done
using mixed model regression statistics and covaried from mean
cortical thickness. Side bar showststatistic with threshold to
control for multiple comparisons using the false discovery rate
procedure withq= 0.05. Differences are from mixed model regression
with age centered at approximate 3-year intervals for middle 80% of
the age range, and colors represent areas of statistically
significant thinning in COS.81 Adapted fromJ Child Psychol
Psychiatry2006;47:1007.45
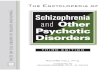
Cortical Gray Matter (GM) Thickness in Healthy Childhood-Onset
Schizophrenia (COS) Siblings (n= 52, 110 scans) Compared With Age-,
Sex-, and Scan IntervalMatched Healthy Controls (n= 52, 108 scans)
Between Ages 8 Through 28 Years. Healthy COS siblings show
significant GM deficits in left prefrontal and bilateral temporal
cortices and smaller deficits in right prefrontal and inferior
parietal cortices. These deficits in healthy siblings normalize
with age with no abnormalities remaining by age 20 years. Side bar
showststatistic with threshold to control for multiple comparisons
using the false discovery rate procedure withq= 0.05. Differences
are from mixed model regression with age centered at approximate
3-year intervals for middle 80% of the age range, and colors
represent areas of statistically significant thinning in COS
siblings.Adapted from Arch Gen Psychiatry. 2007;64:774.46
Is the GM Loss in COS a Medication Effect?The GM findings in COS
appeared to be due to schizophrenia and not due to medicationsIs
the GM Loss in COS Diagnostically Specific?The GM findings in COS
appeared to be due to schizophrenia and not due to
medicationsLewiss Child & Adolescent Psychiatry: A
Comprehensive Textbook 4th EditionNATURE VS. NURTURE NATURE &
NURTURE
Deficits in measures of IQ, memory, and tests of perceptuomotor
skills
Children > Adolescents > Adults
Suggests that these deficits are NOT sequelae of the disorder,
but are MARKERS of brain dysfunction even before the onset of
illnessPsychosocial stressors are known to influence the course of
schizophrenia, and the same stressors may possibly interact with
biological risk factors in the emergence of the disorder, given
that children who are diagnosed with COS have marked
neuropsychological deficits in a wide range of brain functions,
including attention, working memory, and executive functions.
Similar defects have been demonstrated in adolescents and adults
with schizophrenia; however, children with schizophrenia have been
shown to have more significant deficits in measures of intelligence
quotient (IQ), memory, and tests of perceptuomotor skills compared
with adolescent onset of schizophrenia and adolescents had greater
deficits in these areas than adults with schizophrenia. Differences
in these cognitive measures of IQ, memory, and perceptuomotor
skills in persons with schizophrenia of different ages of onset
suggests that these deficits may not be a sequelae of the disorder,
but are markers of brain dysfunction even before the onset of the
illness.52Vulnerability Factorsshyness, and disturbances in
adaptive social behaviorearly language deficits and motor
impairmentsIntellectual delays
a socially odd child is not usually schizophrenicDiagnosis &
Clinical Featurespremorbid history of social rejection, poor peer
relationships, clingy withdrawn behavior, and academic trouble,
delayed motor milestones and language acquisitionOnset is
insidious, starting with inappropriate affect or unusual
behaviorAuditory hallucinationsVisual hallucinations associated
with lower IQ and earlier age at onsetVisual, tactile, and
olfactory hallucinations may be a marker of more severe
psychosisDiagnosis & Clinical FeaturesDelusions increase in
frequency with increased ageBlunted or inappropriate
affectInappropriate giggling and cryingFormal thought disorders,
including loosening of associations and thought blockingIllogical
thinking and poverty of thoughtdo not have poverty of speech
content, but they speak less than other children and ambiguous in
the way they refer to persons, objects, and eventsDiagnosis &
Clinical FeaturesCommunication deficits: unpredictably changing the
topic of conversation without introducing the new topic to the
listener (loose associations)illogical thinking and speaking and
tend to underuse self-initiated repair strategies to aid in their
communicationfail to aid communication with revision, fillers, or
starting over NEGATIVE SYMPTOMSDiagnosis & Clinical FeaturesThe
clinical presentation of schizophrenia remains remarkably similar
across the ageSchizophrenia in prepubertal children includes the
presence of at least two of the following:
hallucinationsdelusionsgrossly disorganized speech or
behaviorsevere withdrawal for at least 1 monthsocial or academic
dysfunction must be presentcontinuous signs of the disturbance must
persist for at least 6 monthsThe diagnostic criteria for
schizophrenia in children are identical to the criteria for the
adult form, except that instead of showing deteriorating
functioning, children may fail to achieve their expected levels of
social and academic functioning.The clinical presentation of
schizophrenia, however, taking into consideration developmental
level of the child, remains remarkably similar across the ages.
Schizophrenia in prepubertal children includes the presence of at
least two of the following: hallucinations, delusions, grossly
disorganized speech or behavior, and severe withdrawal for at least
1 month. Social or academic dysfunction must be present, and
continuous signs of the disturbance must persist for at least 6
months. The diagnostic criteria for schizophrenia in children are
identical to the criteria for the adult form, except that instead
of showing deteriorating functioning, children may fail to achieve
their expected levels of social and academic
functioning.57DifferentialsLewiss Child & Adolescent
Psychiatry: A Comprehensive Textbook 4th EditionDifferentialsLewiss
Child & Adolescent Psychiatry: A Comprehensive Textbook 4th
EditionCourse and PrognosisImportant predictors of course and
outcome:childs premorbid level of functioningthe age of
onsetIQresponse to psychosocial and pharmacological
interventionsdegree of remission after the first psychotic
episodedegree of family supportLess treatment responsive:Early age
at onsetwith comorbid developmental delayslearning disorderslower
IQpremorbid behavioral disorders, such as ADHD and conduct
disorderCourse and PrognosisPredictors of a poorer course:family
history of schizophreniayoung age and insidious onsetdevelopmental
delayslower level of premorbid functionchronic or length of first
psychotic episodeAn important factor in outcome is the accuracy and
stability of the diagnosis of schizophrenia.Management &
TreatmentStage 1 (prodromal phase): The child may experience some
period of deteriorating function, which may include social
isolation, idiosyncratic preoccupations and behaviors, and academic
difficulties.
Stage 2(acute phase): This is usually the time when the child
comes to the attention of a mental health professional, when the
clinical picture is dominated by frank delusions and hallucinations
and other positive symptoms such as a formal thought disorder or
strange and idiosyncratic behaviors.
Management & TreatmentStage 3 (recovery phase): The symptoms
usually begin to remit and dissipate. However, often there may
still be the presence of some psychotic symptoms, although they are
less disturbing to the child. In this phase, the child may continue
to experience some levels of confusion, disorganization, or
lability in mood.
Stage 4 (residual phase): The positive symptoms continue to
subside, but the child continues to experience apathy, lack of
motivation, withdrawal, and restricted or flat affect.
Pathology & Laboratory ExaminationsNo specific laboratory
tests are diagnostically specific for childhood-onset
schizophreniaAlthough data exist to suggest that hypoprolinemia is
associated with the risk of schizoaffective disorder due to an
alteration on chromosome 22q11, no association of hyperprolinemia
with childhood-onset schizophrenia has been identified.Management
& TreatmentIntegrated Psychological Interventions:Cognitive
behavioral therapygroup skills trainingcognitive remediation
therapymultifamily psychoeducationsupportive counseling on the
prevention of psychosisMore effective than standard treatments in
delaying the onset of psychosis over a 2-year follow-up
periodChildren may have less robust responses to antipsychotic
medications than adolescents and adultManagement &
TreatmentPharmacotherapy is instituted in an attempt to treat the
underlying cause of the psychosis, or for symptom control, in those
children who have psychotic symptoms secondary to a known
origin.
Informed consent from the parents or guardian should be obtained
before treatment with psychopharmacologic agents is
instituted.Pharmacotherapysome efficacy:Risperidone up to 3 mg per
dayOlanzapinerandomized 6-week controlled trial of olanzapine in
adolescents with schizophrenia found that it was more efficacious
than placebo.AripiprazoleAt two fixed doses, superior to placebo in
the treatment of positive symptoms of adolescent schizophrenia;
however, more than 40 percent of subjects in the active medication
group did not achieve remission.Clozapinemore effective than
haloperidol in improving both positive and negative symptoms in
treatment resistant schizophrenia in youthPharmacotherapyClozapine
vs high dose Olanzapineresponse rates were about twice as great for
clozapine as olanzapine (66% vs. 33%)clozapine was found to be
associated with a significant reduction in all outcome measures,
whereas olanzapine showed improvement on some measures but not on
allclozapine was superior to olanzapine in alleviating negative
symptomsClozapine was associated with more adverse events, such as
lipid abnormalities and a seizure in one patient.
Management & TreatmentPsychosocial interventions should
include working with both the parents and the child.Improving
family functioning, problem solving, communication skills, and
relapse prevention have been shown to decrease relapse rates in
adultsSocial skills training and may require specialized
educational programs, academic adjustments, and support at
schoolOngoing illness teaching and medication education, are
important to promote compliance with treatment and to help in
coping with the daily and sometimes long-term implications of the
childs illness.Psychosicial InterventionsPsychotherapists who work
with children with schizophrenia must take into account a childs
developmental level in order to support the childs reality testing
and be sensitive to the childs sense of self. Long-term supportive
family interventions and cognitive behavioral and remediation
interventions combined with pharmacotherapy are likely to be the
most effective approach to early-onset schizophrenia.Management
& TreatmentTreatment strategies need to focus on the clinical
symptoms and morbidity of the underlying disorder, while also
addressing any comorbid disorders or biopsychosocial stressors.The
assessment of the child with psychotic symptoms should include a
careful, comprehensive, and thoughtful evaluation