Embed Size (px)
Citation preview
© Cengage Learning 2016 © Cengage Learning 2016
Eric J. MashDavid A. Wolfe
Autism Spectrum Disorder andChildhood-Onset Schizophrenia
6
© Cengage Learning 2016
• A complex neurodevelopmental disorder characterized by abnormalities in social behavior, language and communication skills, and unusual behaviors and interests
Autism Spectrum Disorders (ASD)
© Cengage Learning 2016
• ASD refers to pervasive developmental disorders (PDDs) characterized by significant impairments in social and communication skills, and by stereotyped patterns of interests and behaviors
Description and History
© Cengage Learning 2016
• Kanner (1943) coined the term “early infantile autism” to describe young children with autistic symptoms
• Asperger (1944) defined a milder form of autism ► Asperger’s disorder
• Autism is a biologically-based lifelong neurodevelopmental disability present in the first few years of life
Description and History (cont’d.)
© Cengage Learning 2016
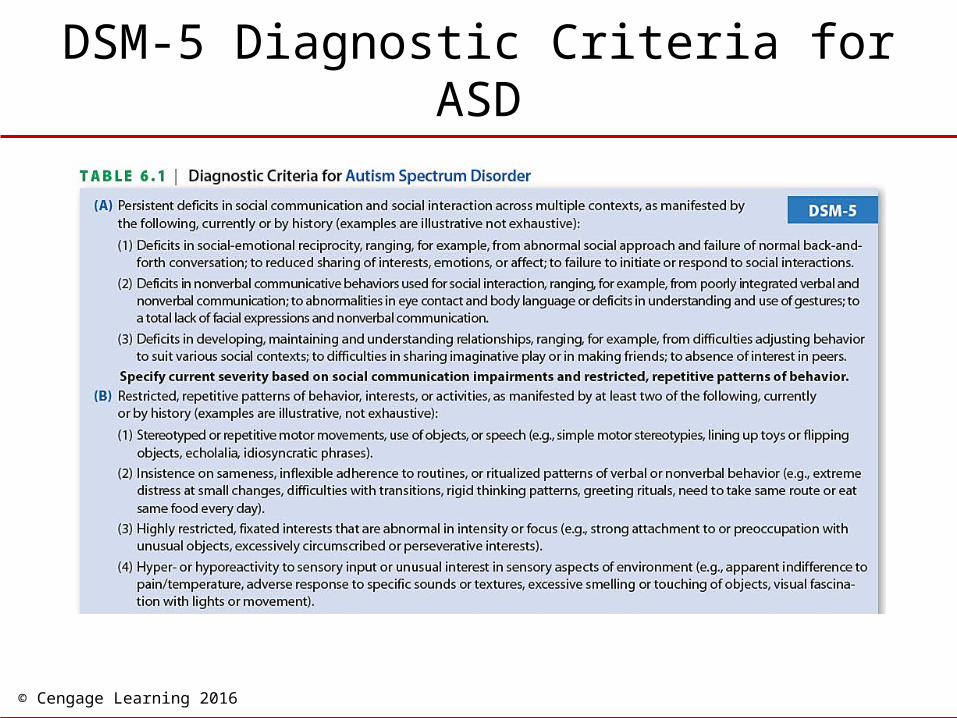
• Impairments in social interaction
• Impairments in communication
• Restricted repetitive and stereotyped patterns of behavior, interests, and activities
DSM-5 Defining Features of ASD
© Cengage Learning 2016
DSM-5 Diagnostic Criteria for ASD
© Cengage Learning 2016
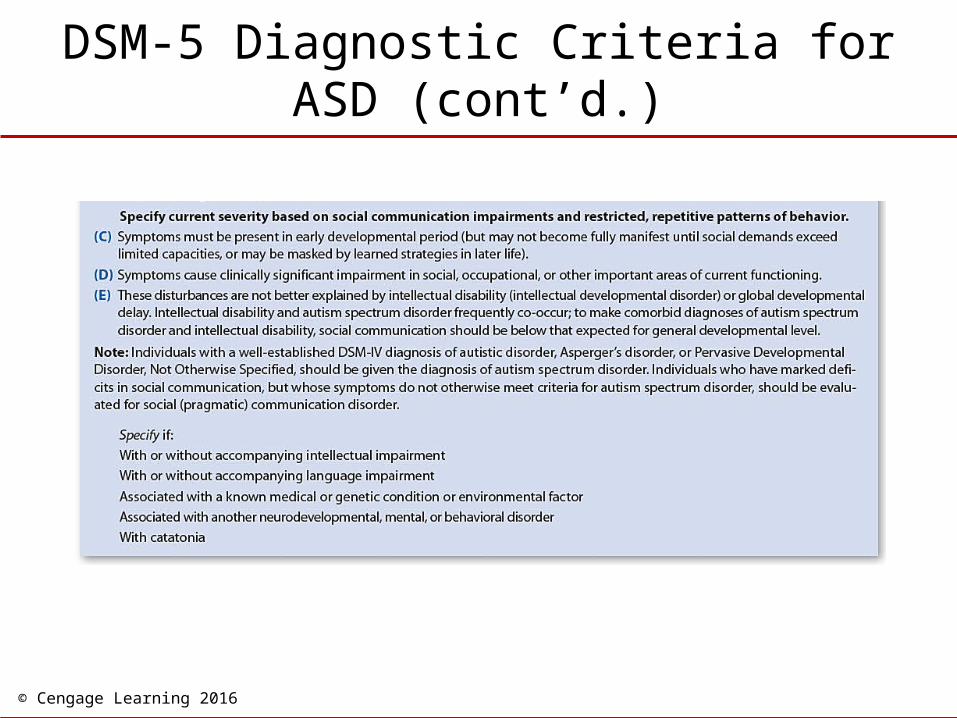
DSM-5 Diagnostic Criteria for ASD (cont’d.)
© Cengage Learning 2016
• Three factors contribute to the spectrum nature of autism– Children with autism may differ in level of
intellectual ability, from profound disability to above-average intelligence
– Children with autism vary in the severity of their language problems
– The behavior of children with autism changes with age
Autism Across the Spectrum
© Cengage Learning 2016
• Debate about core deficits of ASD
• Several deficits likely affect the child’s:– Social-emotional development
– Language development
– Cognitive development
• These aspects of development are interconnected
Core Deficits of ASD
© Cengage Learning 2016
• Deficits in social and emotional reciprocity
• Unusual nonverbal behaviors
• Social imitation, sharing focus of attention, make-believe play
• Limited social expressiveness
• Atypical processing of faces and facial expressions
• Joint attention
Social Interaction Impairments
© Cengage Learning 2016
• One of the first signs of language impairment is inconsistent use of early preverbal communications– Use protoimperative gestures rather than not
protodeclarative gestures
– Miss other declarative gestures, such as showing gesture
– About 50% do not develop any useful language
Communication Impairments
© Cengage Learning 2016
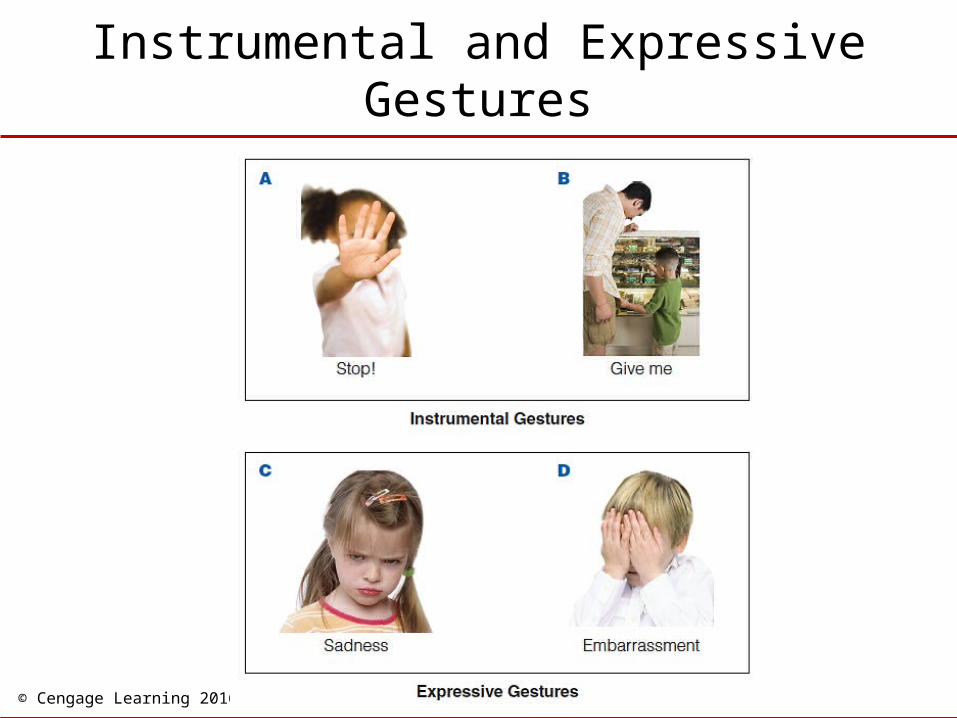
Instrumental and Expressive Gestures
© Cengage Learning 2016
• Those who begin to speak may regress between 12-30 months
• Children with ASD who develop language usually do so before age 5
• Qualitative language impairments – Pronoun reversals
– Echolalia
– Perseverative speech
– Impairments in pragmatics
Communication Impairments (cont’d.)
© Cengage Learning 2016
Difficulty with Pragmatic Use of Language
© Cengage Learning 2016
• Stereotyped body movements– Repetitive sensory and motor behaviors
– Insistence on sameness behaviors
• Self-stimulatory behavior– Different theories
• A craving for stimulation to excite their nervous system
• A way of blocking out and controlling unwanted stimulation from environment that is too stimulating
• Maintained by sensory reinforcement it provides
Restricted and Repetitive Behaviors and Interests
© Cengage Learning 2016
• Children with ASD display a number of associated characteristics– Intellectual deficits and strengths
– Sensory and perceptual impairments
– Cognitive and motivational deficits
– Medical conditions and physical characteristics
Associated Characteristics of ASD
© Cengage Learning 2016
• About 70% of autistic children with autism have co-occurring intellectual impairment
• A common pattern is low verbal scores and high nonverbal scores
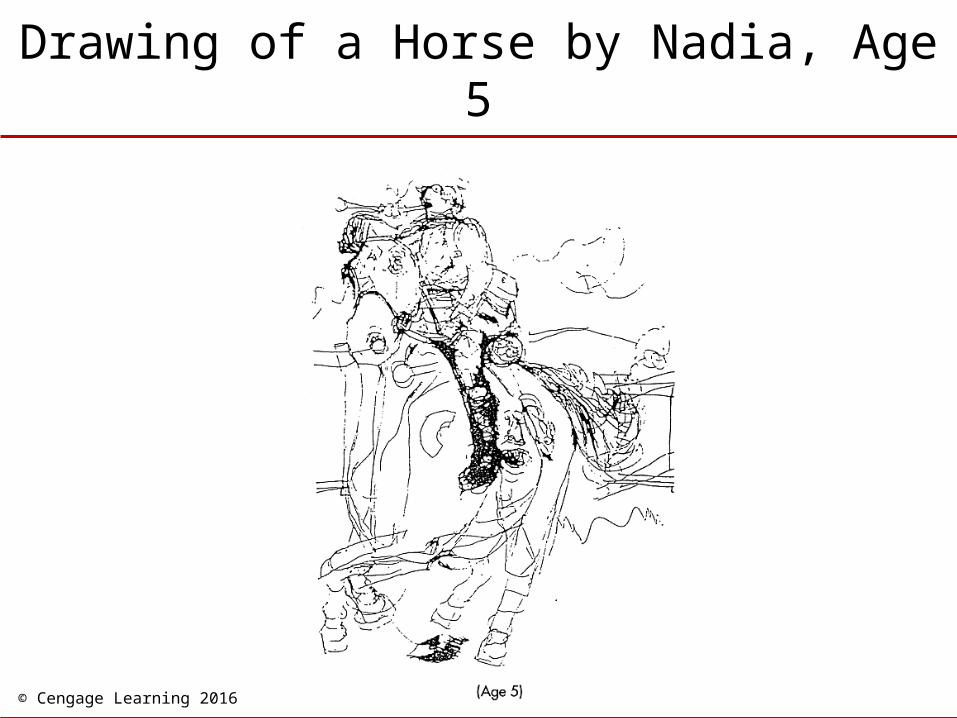
• About 25% have splinter skills or islets of ability
• 5% (autistic savants) display isolated and remarkable talents
Intellectual Deficits and Strengths
© Cengage Learning 2016
Drawing of a Horse by Nadia, Age 5
© Cengage Learning 2016
• Oversensitivities or undersensitivities to certain stimuli
• Overselective and impaired shifting of attention to sensory input
• Impairments in mixing across sensory modalities
• Sensory dominance
• Stimulus overselectivity
Sensory and Perceptual Impairments
© Cengage Learning 2016
• Deficits in processing social-emotional information– Difficulty in situations that require social
understanding
– Do not understand pretense or engage in pretend play
– Deficit in mentalization or theory of mind (ToM) - difficulty understanding others’ and their own mental states
• Do not understand false-belief tests
Cognitive and Motivational Deficits
© Cengage Learning 2016
• Executive functions (higher-order planning and regulatory behaviors)
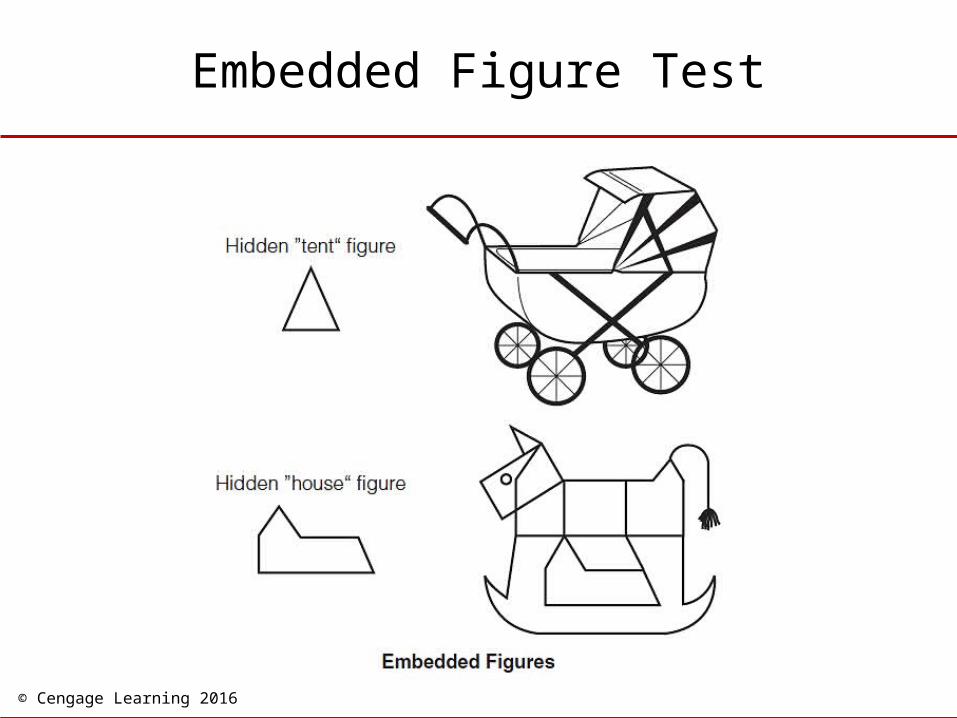
• Weak drive for central coherence (strong human tendency to interpret stimuli in a relatively global way to account for broader context)– Do well on tasks requiring focus on parts of
stimulus
General Deficits
© Cengage Learning 2016
Embedded Figure Test
© Cengage Learning 2016
• Lack of ToM is one of the most specific to ASD– Deficits in processing socio-emotional
information and executive functioning deficits are less specific to ASD
What is Specific to ASD?
© Cengage Learning 2016
• A single cognitive abnormality cannot explain all the deficits present in in children with ASD
• There is a view that children with ASD have an underlying impairment in social motivation
Are Cognitive Deficits Found in All ASD?
© Cengage Learning 2016
• About 10% of children with ASD have a coexisting medical condition– Motor and sensory impairments, seizures,
immunological and metabolic abnormalities
• Sleep disturbances occur in 65%
• Gastrointestinal symptoms occur in 50%
• About 20% have a significantly larger-than-normal head size—more common in those who are higher functioning
Medical Conditions and Physical Characteristics
© Cengage Learning 2016
• Two most common disorders– Intellectual disability
– Epilepsy
• Other disorders - ADHD, conduct problems, anxieties and fears, and mood problems
• May engage in extreme and sometimes potentially life-threatening self-injurious behaviors (SIB)
Accompanying Disorders and Symptoms
© Cengage Learning 2016
• Worldwide: 100 children per 10,000 may suffer from some form of autism – Autistic disorder - 22 of 10,000
– PPD-NOS - 33 of 10,000
– Asperger’s disorder - 10 of 10,000
– One million or more individuals in the United States
– Occurs in all social classes and identified worldwide
Prevalence and Course of ASD
© Cengage Learning 2016
• Most often identified by parents in the months preceding child’s second birthday– Diagnosis is made in preschool period or later
• Earliest point in development for reliable detection period is from 12-18 months– Diagnoses made around 2-3 years are
generally stable
– AAP recommends that all children be screened at 18-24 months
Age of Onset
© Cengage Learning 2016
• Children with ASD may develop along different pathways
• Often gradual improvements with age,– Likely to continue to experience many
problems
– Symptoms may worsen in adolescence
• Complex obsessive-compulsive rituals may develop in late adolescence and adulthood
Course and Outcome
© Cengage Learning 2016
• It is now generally accepted that autism is a biologically based neurodevelopmental disorder with multiple causes– Problems in early development
– Genetic influences
– Brain abnormalities
– A disorder of risk and adaptation
Causes of ASD
© Cengage Learning 2016
• Children with ASD experience more health problems during pregnancy, at birth, or immediately following birth
• Prenatal and neonatal complications have been identified in a small percentage of children with ASD– Examples: parental age, in vitro fertilization,
and maternal use of drugs
Problems in Early Development
© Cengage Learning 2016
• Chromosomal and gene disorders – Fragile-X anomaly occurs in 2-3% of children
with ASD
– ASD individuals have a 5% elevated risk for chromosomal anomalies
– About 25% of children with tuberous sclerosis have ASD
Genetic Influences
© Cengage Learning 2016
• 15-20% of siblings of individuals with ASD have the disorder– Broader autism phenotype
• Concordance rates– 70-90% in identical twins
– Near 0% for fraternal twins
– Heritability of an underlying liability for ASD is 90%
Family and Twin Studies
© Cengage Learning 2016
• Points to particular areas on many different chromosomes as possible locations for genes for ASD– Causally implicated but not a direct cause
– ASD is likely to be a complex genetic disorder
– Expression of ASD genes may be influenced by environmental factors occurring primarily during fetal brain development
– Epigenetic dysregulation may be a factor
Molecular Genetics
© Cengage Learning 2016
• Behavioral features of ASD may result from abnormalities in brain structures– Lack of normal connectivity and
communication across brain networks
– Multiple brain regions may be involved
Brain Abnormalities
© Cengage Learning 2016
• Cerebral gray and white matter overgrowth Structural abnormalities:– In the cerebellum and medial temporal lobe
and related limbic system structures
• Decreased blood flow in the frontal and temporal lobes
• Elevated blood serotonin in 33% of cases
• Atypical patterns of connectivity in default mode network
Brain Abnormalities – Biological Findings
© Cengage Learning 2016
• The relationship between the child’s early risk for ASD and later outcomes– Is mediated by alterations in how the child
interacts with and adapts to his or her environment
• Different children will follow different developmental pathways
ASD as a Disorder of Risk and Adaptation
© Cengage Learning 2016
• There are about 400 different treatments for ASD
• There is no known cure
• Treatment goals– Minimize core problems
– Maximize independence and quality of life
– Help the child and family cope more effectively with the disorder
Treatment of ASD
© Cengage Learning 2016
• Engaging children in treatment
• Decreasing disruptive behaviors
• Teaching appropriate social behavior
• Increasing functional, spontaneous communication
• Promoting cognitive skills
• Teaching adaptive skills to increase responsibility and independence
Overview of Treatment Strategies
© Cengage Learning 2016
• Initial stages focus on building rapport and teaching learning-readiness skills– Discrete trial training involves a step-by-step
approach to presenting stimulus and requiring a specific response
– Incidental training strengthens behavior by capitalizing on naturally occurring opportunities
Treatment Strategies: Initial Stages
© Cengage Learning 2016
• Intensive 25 hours a week and 12 months a year
• Low student-teacher ratio
• High structure
• Family inclusion
• Peer interactions
• Generalization
Early Intervention
© Cengage Learning 2016
• Many children with ASD receive psychotropic medications– Antidepressants, stimulants, and tranquilizers/
antipsychotics
– Benefits are limited• Variable from child to child
• Core deficits of these children are not altered
– Risks, benefits, and costs must be carefully evaluated
Medications
© Cengage Learning 2016
• Schizophrenia is a neurodevelopmental disorder of the brain - expressed in abnormal mental functions and disturbed behavior– Characterized by severe psychotic symptoms
bizarre delusions, hallucinations, thought disturbances, grossly disorganized behavior or catatonic behavior, extremely inappropriate or flat affect, and significant deterioration or impairment in functioning
Childhood-Onset Schizophrenia (COS)
© Cengage Learning 2016
• COS is a rarer and possibly more severe (not distinct) form of schizophrenia
• Key features– Occurs during childhood
– Has a gradual, rather than sudden onset
– Is likely to persist into adolescence and adulthood
– Has profound negative impact on developing social and academic competence
Childhood-Onset Schizophrenia (cont’d.)
© Cengage Learning 2016
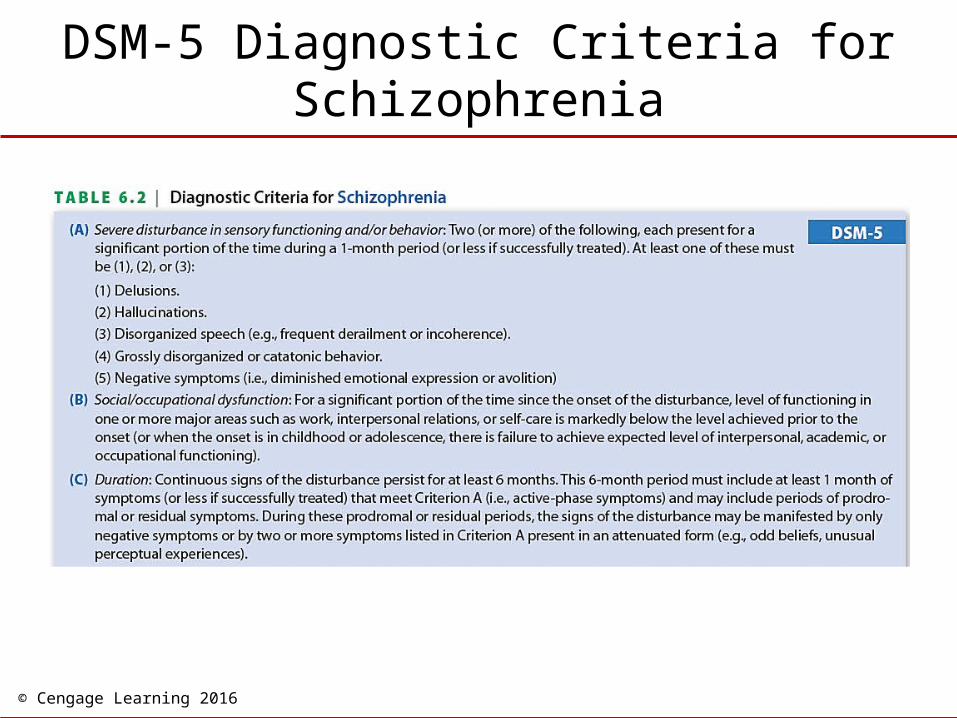
• Positive symptoms – Delusions
– Hallucinations most common for children are auditory - occur in 80% of cases with onset prior to age 11
• 40 to 60% experience visual hallucinations, delusions, and thought disorder
• Negative symptoms – Slowed thinking, speech, movement;
emotional apathy; and lack of drive
DSM-5 Positive and Negative Symptoms
© Cengage Learning 2016
DSM-5 Diagnostic Criteria for Schizophrenia
© Cengage Learning 2016
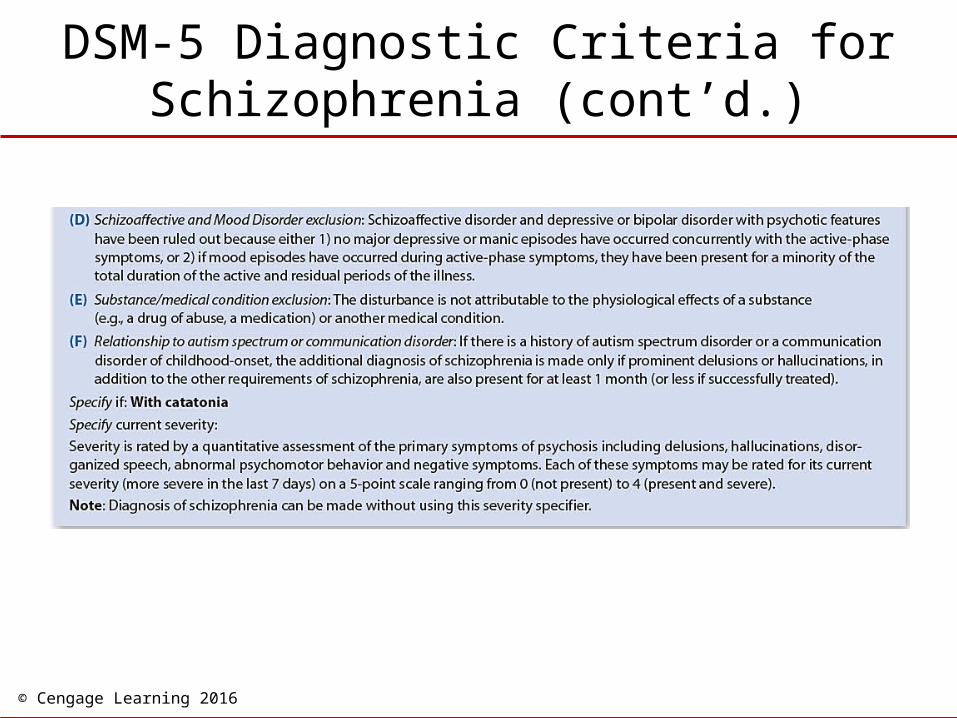
DSM-5 Diagnostic Criteria for Schizophrenia (cont’d.)
© Cengage Learning 2016
• Gradual onset
• Almost 95% have history of behavioral, social, and psychiatric disturbances before onset of psychosis
• Developmental precursors
• Other symptoms/disorders– 70% meet criteria for another diagnosis -
most commonly mood disorder or ODD/CD
– COS and ASD may not be linked
Precursors and Comorbidities
© Cengage Learning 2016
• Extremely rare in children under age 12
• Dramatic increase in adolescence, with a modal onset around 22 years of age
• Estimated prevalence is less than 1 per 10,000 children
• COS has an earlier age of onset in boys by two to four years– Gender differences disappear in adolescence
Prevalence
© Cengage Learning 2016
• Neurodevelopmental model– Defective neural circuitry increases a child’s
vulnerability to stress
• Biological factors – Strong genetic contribution
• Molecular genetic studies have identified several potential susceptibility genes
– CNS dysfunction and improvements with medication suggest it is a disorder of the brain
Causes of COS
© Cengage Learning 2016
• Environmental factors – Familial disorder and nongenetic factors may
play a role through interaction with a genetic susceptibility
– High communication deviance
– Stress, distress, and personal tragedy experienced by families of children with schizophrenia
Causes of COS (cont’d.)
© Cengage Learning 2016
• COS is a chronic disorder with a poor long-term prognosis
• Current treatments emphasize use of antipsychotic medications combined with psychotherapy and social and educational support programs
• Medications help control psychotic symptoms– There can be serious side effects
Treatment of COS