Embed Size (px)
Citation preview
STATE OF CALIFORNIA - HEALTH AND HUMAN SERVICES AGENCY
FACILITY EVALUATION REPORT
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES COMMUNITY CARE LICENSING DIVISION
CCLD Regional Office, 2580 N FIRST STREET, STE. 300 SAN JOSE, CA 95131
FACILITY NAME: SHEPHERD OF THE VALLEY LUTHERAN CHURCH ADMINISTRATOR: TANYA KENNEDY
FACILITY NUMBER: FACILITY TYPE:
430702694 850
(408) 997-4846 95120
10/02/2013 08:15AM 09:35AM
ADDRESS: 1281 REDMOND AVENUE TELEPHONE: CITY: SAN JOSE STATE: CA ZIP CODE: CAPACITY: 75 CENSUS: 62 DATE: TYPE OF VISIT: POC UNANNOUNCED TIME BEGAN: MET WITH: Tanya Kennedy TIME COMPLETED:
NARRATIVE 1 A follow up visit was made to the facility to verify correction to deficiencies cited on 09/05/13. Toured class 2 rooms and observed parents signing their children in . today, number of children in care matched with sign in 3 sheet. 4 Play ground has been fix, they removed protruding nails on the side of the storage shed. Sand box frame 5 has been fixed and painted. 6 All deficiencies cited on 09/05/13 have been fixed and no new one noted. 7 Notice of site visit was posted . 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
SUPERVISOR'S NAME: Sandy Knight
LICENSING EVALUATOR NAME: Roya Shahkarami
LICENSING EVALUATOR SIGNATURE:
TELEPHONE: (408) 324-2148
TELEPHONE: (408) 334-8312
DATE: 10/02/2013
I acknowledge receipt of this form and understand my licensing appeal rights as explained and received.
FACILITY REPRESENTATIVE SIGNATURE:
~I DATE: 10/02/2013
This report must be available at Child Care and Group Home facilities for public review for 3 years.
LIC809 (FAS) - (06/04) Page: 1 of 1
All POC Have Been Cleared STATE OF CALIFORNIA - HEALTH AND HUMAN SERVICES AG ENCY
CLEARED DEFICIENCIES
FACILITY NAME: SHEPHERD OF THE VALLEY LUTHERAN CHURCH
POC Due Date I PLAN OF CORRECTIONS(POCs) Section Number
09/20/2013 1
1 01238.2(d)(2) 2 3 4 ifhey need to hammer down all the nai ls. 5 6 7
09/20/2013 1 Section Cited 2
3 1 01238.2(d)(2) 4 r-hey need to sand and paint the sand box's frame.09 5 6 7
09/20/2013 1
Section Cited 2 3 101229.1 4 [They need to monitor sign in/ sign out sheet. 5 6 7
1
Section Cited 2 3 4 5 6 7
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES COMMUNITY CARE LICENSING DIVISION
CCLD Regional Office, 2580 N FIRST STREET, STE. 300 SAN JOSE, CA 95131
FACILITY NUMBER: 430702694
VISIT DATE: 09/05/201 3
Date Cleared I Comments
1 2 1 0/02/2013
3 Cleared By Visit
4
1 . 1 0/02/2013
~ Cleared By Visit
4
1 10/02/2013
~ Cleared By Vis it
4
1 2 3 4
STATE OF CALIFORNIA - HEALTH AND HUMAN SERVICES AGENCY CALIFORNIA DEPARTMENT OF SOCIAL SERVICES COMMUNITY CARE LICENSING DIVISION
FACILITY EVALUATION REPORT CCLD Regional Office, 2580 N FIRST STREET, STE. 300 SAN JOSE, CA 95131
FACILITY NAME: SHEPHERD OF THE VALLEY LUTHERAN CHURCH ADMINISTRATOR: TANYA KENNEDY ADDRESS: 1281 REDMOND AVENUE CITY: SAN JOSE CAPACITY: TYPE OF VISIT: MET WITH:
1 2
75 Annual/Random Tania Kennedy
STATE:CA CENSUS: 60 UNANNOUNCED
NARRATIVE
FACILITY NUMBER: FACILITY TYPE: TELEPHONE: ZIP CODE: DATE: TIME BEGAN: TIME COMPLETED:
430702694 850
(408) 997-4846 95120
09/05/2013 08:20AM 11:15 AM
2 An unannounced Annual / Random visit was made to the facility. Waited 10 minutes in parking lot since office 3 is open from 8:30AM. Observed arrival of the children . Met with director and toured facility. Today, they had a 4 book fa ir. 5 Toured 5 rooms, observed supervision and ratio. Tanya stated that she has a floater that helps children and 6 staff with escorting the ch ildren to bathroom. Supervision was correct during today's visit. 7 Reviewed sign in/ sign out sheet. All required posters, Parents Rights , facil ity license, daily activities and 8 Personal Rights were posted . 9 Observed children during arrival, free play time and making snack. 10 Reviewed posted snack menu. Children bring in their lunches. They have a kitchen for food preparation . 11 Kitchen observed to be clean , has hoU cold running water, refrigerator and sanitizer. Garbage cans have tight 12 fitting lids. They serve 1% milk and no juice is being served to children . 13 Children nap at th is program. Each child has their own mat and bedding . The facility provides children's 14 bedding and they wash ch ildren's bedding by weekly. 15 Observed children being escorted to the inside bathroom. One teacher stands outside and help children as 16 needed. 17 They do administer medication. Medication are kept in the kitchen. At this time they do not have any children 18 on medication . Discussed isolation of sick child . Office is used for isolation of a sick child. They have 19 accessible drinking water in the class rooms and in their playground. 20 Chi ldren's bathroom observed to be clean . Soap, toilet papers and paper towels were available for children . 21 Toured their playground. They have age appropriate equipment for children . They have enough shaded areas 22 for ch ildren. Tanya stated that she designated one staff for each area of the playground to assure visual 23 supervision at all time. Reviewed sampling of staff and children's records. staff have current CPR training. 24 They are planning to conduct their drills on 09/10 and 09/11/2013. They have fire drill, earthquake drill and 25 code red drill.
Discussed regulations regarding zero tolerance citation and penalty associated to the citation.
SUPERVISOR'S NAME: Sandy Knight
LICENSING EVALUATOR NAME: Roya Shahkarami
LICENSING EVALUATOR SIGNATURE:
TELEPHONE: (408) 324-2148
TELEPHONE: (408) 334-8312
DATE: 09/05/2013
I acknowledge receipt of this form and understand my licensing appeal rights as explained and received.
FACILITY REPRESENTATIVE SIGNATURE:
DATE: 09/05/2013
This report must be available at Child Care and Group Home facilities for public review for 3 years.
LIC809 (FAS) • (06/04) Page: 1 of 3
STATE OF CALIFORNIA- HEALTH AND HUMAN SERVICES AGENCY
FACILITY EVALUATION REPORT (Cont)
FACILITY NAME: SHEPHERD OF THE VALLEY LUTHERAN CHURCH
NARRATIVE
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES COMMUNITY CARE LICENSING DIVISION
CCLD Regional Office, 2580 N FIRST STREET, STE. 300 SAN JOSE, CA 95131
FACILITY NUMBER: 430702694
VISIT DATE: 09/05/2013
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
They have different schedules and their program runs from 8:45AM to 3:30 PM. Majority of the children leave around 11 :45 AM. A review of staff records on 09/05/13 indicates that all facility staff or other individuals who requires caregiver background checks have received criminal record and child abuse index clearances or exemptions. "NOTICE OF SITE VISIT" Document was posted & must remain posted for 30 days adjacent to the main entry doorway.
The following type B deficiencies are cited:
SUPERVISOR'S NAME: Sandy Knight
LICENSING EVALUATOR NAME: Roya Shahkarami
LICENSING EVALUATOR SIGNATURE:
TELEPHONE: (408) 324-2148
TELEPHONE: (408) 334-8312
DATE: 09/05/2013
I acknowledge receipt of this form and understand my appeal rights as explained and received.
FACILITY REPRESENTATIVE SIGNATURE:
DATE: 09/05/2013
LIC809 (FAS) - (06/04) Page: 3 of 3
STATE OF CALIFORNIA· HEALTH AND HUMAN SERVICES AGENCY
FACILITY EVALUATION REPORT (Cont)
FACILITY NAME: SHEPHERD OF THE VALLEY LUTHERAN CHURCH DEFICIENCY INFORMATION FOR THIS PAGE:
Deficiency Type POC Due Date I DEFICIENCIES Section Number
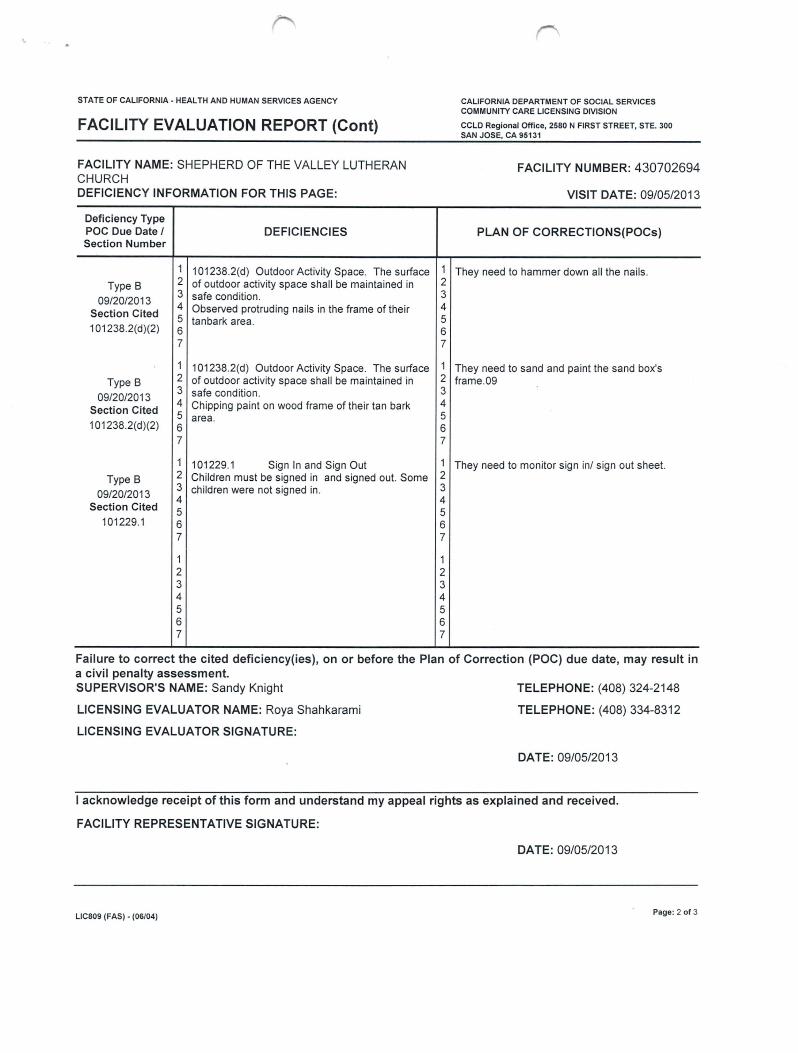
1 1 01238.2(d) Outdoor Activity Space. The surface Type B 2 of outdoor activity space shall be maintained in
09/20/2013 3 safe condition .
Section Cited 4 Observed protruding nails in the frame of their 5 tanbark area.
1 01238.2(d)(2) 6 7
1 1 01238.2(d) Outdoor Activity Space. The surface Type B 2 of outdoor activity space shall be maintained in
09/20/2013 3 safe cond ition.
Section Cited 4 Chipping paint on wood frame of their tan bark 5 area.
1 01238.2(d)(2) 6 7
1 101229.1 Sign In and Sign Out Type B 2 Children must be signed in and signed out. Some
09/20/2013 3 children were not signed in .
Section Cited 4 5
101229.1 6 7
1 2 3 4 5 6 7
1 2 3 4 5 6 7
1 2 3 4 5 6 7
1 2 3 4 5 6 7
1 2 3 4 5 6 7
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES COMMUNITY CARE LICENSING DIVISION
CCLD Regional Office, 2580 N FIRST STREET, STE. 300 SAN JOSE, CA 95131
FACILITY NUMBER: 430702694
VISIT DATE: 09/05/2013
PLAN OF CORRECTIONS(POCs)
They need to hammer down all the nails.
They need to sand and paint the sand box's frame.09
They need to monitor sign in/ sign out sheet.
Failure to correct the cited deficiency(ies), on or before the Plan of Correction (POC) due date, may result in a civil penalty assessment. SUPERVISOR'S NAME: Sandy Knight
LICENSING EVALUATOR NAME: Roya Shahkarami
LICENSING EVALUATOR SIGNATURE:
TELEPHONE: (408) 324-2148
TELEPHONE: (408) 334-8312
DATE: 09/05/2013
I acknowledge receipt of this form and understand my appeal rights as explained and received.
FACILITY REPRESENTATIVE SIGNATURE:
DATE: 09/05/2013
LIC809 (FAS) - (06/04) Page: 2 of 3
SJm: ZOe CAUFORNIA- HEALTH AND HUMAN SERVICES AGENCY CALIFORNIA DEPARTMENT OF SOCIAL SERVICES
' AA . LJAL LICENSE VISIT CHECKLIST CHR..D CARE CENTERS AND INFANT CENTERS
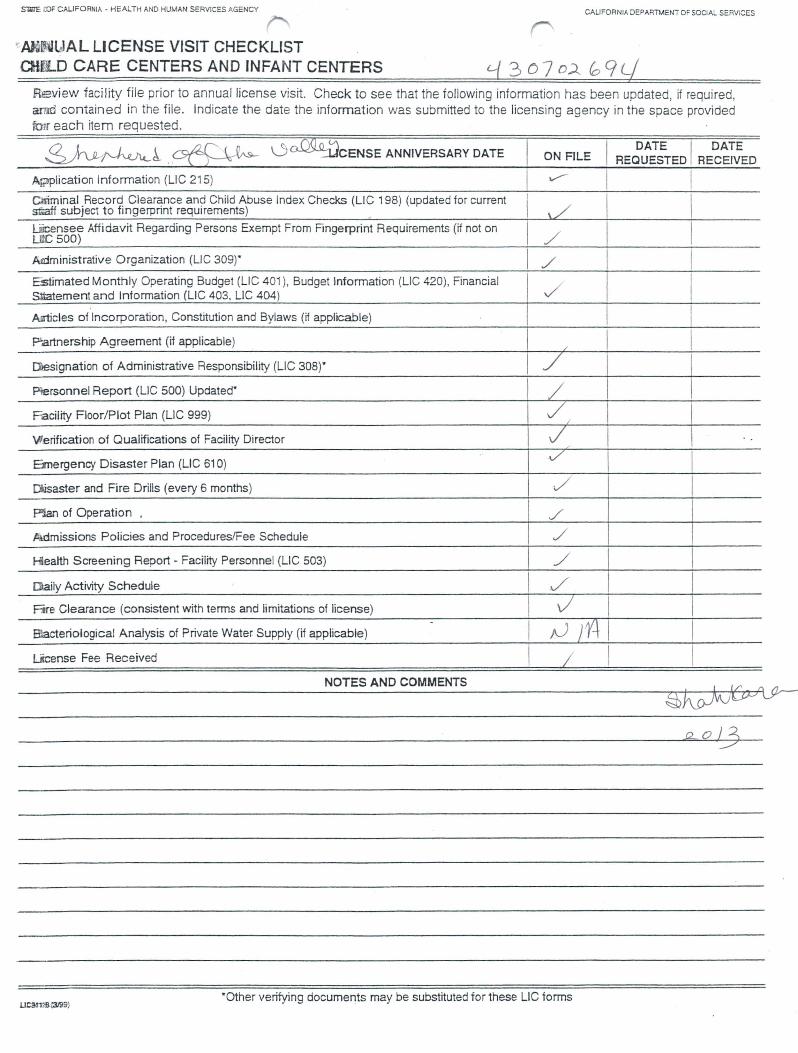
Reeview facility file prior to annual license visit. Check to see that the following information has been updated, if required, arnrl contained in the file. Indicate the date the information was submitted to the licensing agency in the space provided fm.r each item requested.
0 o::o9:@cENSE ANNIVERSARY DATE
A~?Piication Information (LIC 215)
Grominai_Record. Clearance and Child Abuse Index Checks (LIC 198) (updated for current ~ff subJect to fmgerpnnt requirements) ~
Uicensee Affidavit Regarding Persons Exempt From Fingerprint Requirements (if not on U C SOD)
Atdministrative Organization (LIC 309)"
Estimated Monthly Operating Budget (LIC 401 ), Budget lnfonmation (LIC 420), Financial Sltatement and Information (LIC 403, LIC 404)
Aaticles of Incorporation, Constitution and Bylaws (if applicable)
P.artnership Agreement (if applicable)
r::»esignation of Administrative Responsibility (LIC 308)"
Plersonnel Report (LIC 500) Updated·
Facility Floor/Plot Plan (LIC 999)
Vlerification of Qualifications of Facility Director
Emergency Disaster Plan (LIC 61 0)
Ciisaster and Fire Drills (every 6 months)
Pllan of Operation .
Admissions Policies and Procedures/Fee Schedule
Hl.ealth Screening Report - Facility Personnel (LIC 503)
[l}aily Activity Schedule
Fire Clearance (consistent with terms and limitations of license)
Blacteriological Analysis of Private Water Supply (if applicable)
L«cense Fee Received
NOTES AND COMMENTS
ON FILE
/ /
I / / I
I ./ J' v I /
./ / I
I /
'A I
·Other verifying documents may be substituted for these LIC tonms
DATE I DATE REQUESTED RECEIVED
I
I I
I
STATE OF CALIFORNIA· HEALTH AND HUMAN SERVICES AGENCY
FACILITY EVALUATION REPORT
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES COMMUNITY CARE LICENSING DIVISION
CCLD Regional Office, 2580 N FIRST STREET, STE. 300 SAN JOSE, CA 95131
FACILITY NAME: SHEPHERD OF THE VALLEY LUTHERAN CHURCH ADMINISTRATOR: TANYA KENNEDY
FACILITY NUMBER: FACILITY TYPE:
430702694 850
(408) 997-4846 95120
03/09/2012 02:30PM 03:17PM
ADDRESS: 1281 REDMOND AVENUE TELEPHONE: CITY: SAN JOSE STATE: CA ZIP CODE: CAPACITY: 75 CENSUS: 30 DATE: TYPE OF VISIT: Case Management UNANNOUNCED TIME BEGAN: MET WITH: Tania Kennedy TIME COMPLETED:
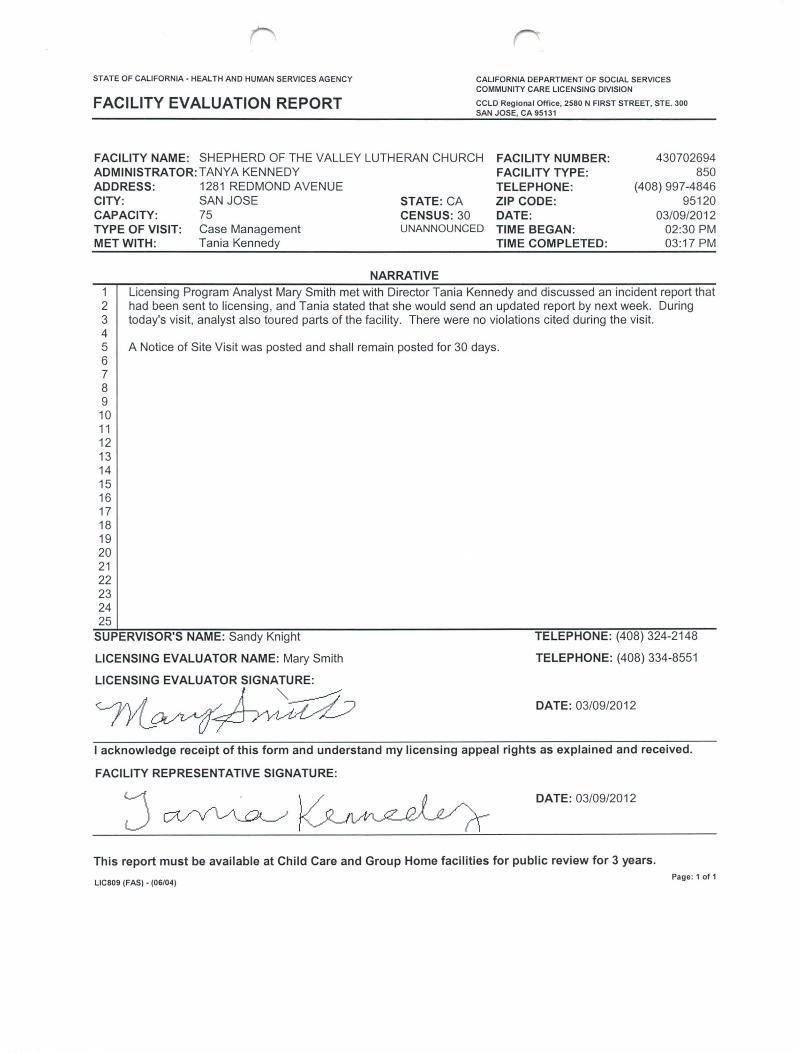
NARRATIVE 1 Licensing Program Analyst Mary Smith met with Director Tania Kennedy and discussed an incident report that 2 had been sent to licensing , and Tania stated that she would send an updated report by next week. During 3 today's visit, analyst also toured parts of the facility. There were no violations cited during the visit. 4 5 A Notice of Site Visit was posted and shall remain posted for 30 days. 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
SUPERVISOR'S NAME: Sandy Knight
LICENSING EVALUATOR NAME: Mary Smith
LICENSING EVALUATOR SIGNATURE:
!YLovv(~
TELEPHONE: (408) 324-2148
TELEPHONE: (408) 334-8551
DATE: 03/09/2012
I acknowledge receipt of this form and understand my licensing appeal rights as explained and received.
FACILITY REPRESENTATIVE SIGNATURE:
DATE: 03/09/2012
This report must be available at Child Care and Group Home facilities for public review for 3 years.
LIC809 (FAS) • (06/04) Page : 1 of 1
All POC Have Been Cleared STATE OF CALIFORNIA - HEALTH AND HUMAN SERVICES AGENCY
CLEARED DEFICIENCIES
FACILITY NAME: SHEPHERD OF THE VALLEY LUTHERAN CHURCH
POC Due Date I PLAN OF CORRECTIONS(POCs) Section Number
01 /30/2011 1
101 217 (a) 2 3 4 One staff person did not have all required forms . 5 6 7
1
Section Cited 2 3 4 5 6 7
1
Section Cited 2 3 4 5 6 7
1
Section Cited 2 3 4 5 6 7
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES COMMUNITY CARE LICENSING DIVISION
CCLD Regional Offi ce, 2580 N FIRST STREET, STE. 300 SAN JOSE, CA 95131
FACILITY NUMBER: 430702694
VISIT DATE: 01 /10/2011
Date Cleared I Comments
1 2 02/02/2011
3 Cleared By Visit
4
1 2 3 4
1 2 3 4
1 2 3 4
STATE OF CALIFORNIA· HEALTH AND HUMAN SERVICES AGENCY
FACILITY EVALUATION REPORT
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES COMMUNITY CARE LICENSING DIVISION
CCLD Regional Office, 2580 N FIRST STREET, STE. 300 SAN JOSE, CA 95131
FACILITY NAME: SHEPHERD OF THE VALLEY LUTHERAN CHURCH ADMINISTRATOR: LEATHERMAN , SANDRA
FACILITY NUMBER: FACILITY TYPE:
~30702694
850 (408) 997-4846
95120 02/02/2011
02:35PM 03:30PM
ADDRESS: 1281 REDMOND AVENUE CITY: SAN JOSE CAPACITY: 75 TYPE OF VISIT: POC MET WITH: Tanya
STATE:CA CENSUS: 13 UNANNOUNCED
NARRATIVE
TELEPHONE: ZIP CODE: · DATE: TIME BEGAN: TIME COMPLETED:
1 A fo llow up visit was made to the facil ity to verify correction to deficiency cited on 01/10/11. Analyst toured 2 facility and observed 13 children to two staff. Reviewed staff's records and issued two teacher's passports. All 3 staff records were complete and up to date. Deficiency cited has been corrected and no new one noted. 4 Notice of site visit was posted. 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
SUPERVISOR'S NAME: Sandy Knight
LICENSING EVALUATOR NAME: Roya Shahkarami
LICENSING EVALUATOR SIGNATURE:
TELEPHONE: (408) 324-2148
TELEPHONE: (408) 334-8312
DATE: 02/02/2011
I acknowledge receipt of this form and understand my licensing appeal rights as explained and received.
FACILITY REPRESENTATIVE SIGNATURE:
DATE: 02/02/2011
This report must be available at Child Care and Group Home facilities for public review for 3 years.
LIC809 (FAS) • (06/04) Page: 1 of 1
STATE OF CALIFORNIA· HEALTH AND HUMAN SERVICES AGENCY CALIFORNIA DEPARTMENT OF SOCIAL SERVICES COMMUNITY CARE LICENSING DIVISION
FACILITY EVALUATION REPORT CCLD Reg ional Office, 2580 N FIRST STREET, STE. 300 SAN JOSE, CA 95131
FACILITY NAME: SHEPHERD OF THE VALLEY LUTHERAN CHURCH ADMINISTRATOR: LEATHERMAN, SANDRA
FACILITY NUMBER: FACILITY TYPE:
~3070269
850 (408) 997-4846
95120 01/10/2011
12:40 PM 03:20PM
ADDRESS: 1281 REDMOND AVENUE TELEPHONE: CITY: SAN JOSE STATE:CA
CENSUS: 13 UNANNOUNCED
ZIP CODE: CAPACITY: 75 DATE: TYPE OF VISIT: Required - 5 Year
Tanya Kennedy TIME BEGAN:
MET WITH: TIME COMPLETED:
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
NARRATIVE
An unannounced Required/ 5 year visit was made. Met with newly hired Director, Tanya Kennedy and toured facility ( Luke,John, Genesis, Mark and Matthew). Analyst observed children during their group time and circle time. During today's visit the ratio and supervision was correct. They have two sets of toilets , 3 toilets and 3 sinks in each bathrooms. Children's bathroom observed to have soap containers , toilet papers and paper towels . Reviewed sign in/ sign out sheet for each class room . The facility provides one snack. Toured kitchen checked food storage area. They have dishwasher, refrigerator and freezer. Reviewed posted snack menu. All required posters, Parents Rights , facility license,daily activities and Personal Rights were posted. Children do not nap at this facility. They do not administer medication . Observed drinking water in the class room and in the playground. Toured playground and they have age appropriate equipment for children . They have enough shaded areas for children. They have cemented walk way, sand, tanbark and grass areas in their playgrounds. Reviewed sampling of staff and children's records. Issued 7 passports. Their last emergency and fire drills were on 01/16/2010. They have a complete first aide kit.
A review of the staff records on 01/10/11 indicates that all facility staff or other individuals who require caregiver background checks have received criminal record and child abuse index clearances or exemptions. "NOTICE OF SITE VISIT" Document was posted & must remain posted for 30 days adjacent to the main entry doorway. The following type B deficiencies is cited.
SUPERVISOR'S NAME: Sandy Knight TELEPHONE: (408) 324-2148
TELEPHONE: (408) 334-8312 LICENSING EVALUATOR NAME: Roya Shahkarami
LICENSING EVALUATOR SIGNATURE:
DATE: 01/10/2011
I acknowledge receipt of this form and understand my licensing appeal rights as explained and received.
FACILITY REPRESENTATIVE SIGNATURE:
DATE: 01/10/2011
This report must be available at Child Care and Group Home facilities for public review for 3 years.
LIC809 (FAS) • (06/04) Page: 1 of 2
STATE OF CALIFORNIA· HEALTH AND HUMAN SERVICES AGENCY
FACILITY EVALUATION REPORT (Cont)
FACILITY NAME: SHEPHERD OF THE VALLEY LUTHERAN CHURCH DEFICIENCY INFORMATION FOR THIS PAGE:
Deficiency Type POC Due Date I DEFICIENCIES Section Number
1 101217(a) Personnel Records. Personnel records Type B 2 shall be maintained on the licensee, administrator,
01/30/2011 3 and each employee, and shall contain specified
Section Cited 4 information. 5 Violation of Title 22.
101217 (a) 6 7
1 2 3 4 5 6 7
1 2 3 4 5 6 7
1 2 3 4 5 6 7
1 2 3 4 5 6 7
1 2 3 4 5 6 7
1 2 3 4 5 6 7
1 2 3 4 5 6 7
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES COMMUNITY CARE LICENSING DIVISION
CCLD Regional Office, 2580 N FIRST STREET, STE. 300 SAN JOSE, CA 95131
FACILITY NUMBER: 430702694
VISIT DATE: 01/10/2011
PLAN OF CORRECTIONS(POCs)
One staff person did not have all required forms.
Failure to correct the cited deficiency(ies), on or before the Plan of Correction (POC) due date, may result in a civil penalty assessment.
SUPERVISOR'S NAME: Sandy Knight
LICENSING EVALUATOR NAME: Roya Shahkarami
LICENSING EVALUATOR SIGNATURE:
TELEPHONE: (408) 324-2148
TELEPHONE: (408) 334-8312
DATE: 01/10/2011
I acknowledge receipt of this form and understand my appeal rights as explained and received.
FACILITY REPRESENTATIVE SIGNATURE:
0~~ DATE: 01/10/2011
LIC809 (FAS) • (06/04) Page: 2 of 2
OF CALIFORNIA- HEALTH AND HUMAN SERVICES AGENCY
CALIFORNIA DEPARTM:NT OF SOCIAL SERVI~ES
UNUAL LICENSE VISIT CHECKL._ r tYILD CARE CENTERS AND INFANT CENTERS
Review facility file prior to annual license visit Check to see that the following information has been updated, if required, and contained in the file . Indicate the date the information was submitted to the licensing agency in the space provided for each item requested .
Criminal Record Clearance and Child Abuse Index Checks (LIC 1 98) (updated for current staff subject to fingerprint requirements)
Licensee Affidavit Regarding Persons Exempt From Fingerprint Requirements (if not on LIC 500)
Administrative Organization (LIC 3o9r Estimated Monthly Operating Budget (LIC 401 ), Budget Information (LIC 420), Financial Statement ahd lnfonnation (LIC 403, LIC 404)
Articles of Incorporation, Constitution and Bylaws (if applicable)
Partnership Agreement (if applicable)
Designation of Administrative Responsibility (LIC 308)"
Personnel Report (LIC 500) Updated•
Facility Floor/Plot Plan (LIC 999)
Verification of Qualifications of Facility Director
Emergency Disaster Plan (LIC 61 0)
Disaster, and Fire Drills (every 6 months)
Plan of Operation
Admissions Policies and Procedures/Fee Schedule
Health Screening Report - Facility Personnel (LIC 503)
Daily Activity Schedule
Fire Clearance (consistent with terms and limitations of license) -
Bacteriological Analysis of Private Water Supply (if applicable)
Ucense Fee Received
NOTES AND COMMENTS
ON FILE
I ----~./"
I ./
I ........--
..... _./ '
/
~
./ _/
/ 1 ./
I ~ ~ I ~
LIC 9118 (3199) ·Other verifying documents may be substituted for these LIC forms
DATE DATE REQUESTED RECEIVED
I I I I I I
I I
I
I I
I I I
.. -STATE OF CALIFORNIA- HEALTH AND HUMAN SERVICES AGENCY COMMUNITY CARE LICENSING
DEPARTMENT OF SOCIAL SERVICES
•
Date 3/5/06
Director Sandy Leatherman L.i,.Cjlnse~ ;:snepnerd of the Valley Lutheran Church
1\tat;ne of FaciliJY ~nephera of the Valley Lutheran Preschool
Addrj!SS 12~1 Redmond Ave. , San Jose, CA 95120
City, State, Zip Code
SUBJECT: Waiver Request
Discussion and/or Limit~tions -of Waiver (Reason for Denial):
THIS DOCUMENT MUST BE MADE AVAILABLE FOR REVIEW ON THE FACILITY PREMISES
Waiver:
0 Denied
0 Granted
Inside gym is used for preschool space. The inside gym is set up with a series of stations that the children can choose to explore. The space is sectioned off with a series of rolling carts that contain blocks, manipulatives & arts/craft materials. Child size tables and chairs are in the gym space for snack, cooking projects, and glitter/glue projects and used for a variety of other activities. The children's art work is displayed on the gym walls at the childs eye level.
Shepherd provides a three hour preschool program. The last 10 to 15 minutes before dismisal the rolling carts are closed in the gym and the children are released after they are signed out from circle time in the Matthew, Mark, Luke, John classrooms to their parents or caregiver.
-The inside gym is also used for large motor movement such as music and rainy day recess. The classes are stagered.
This Waiver is subject to periodic review and may be terminated at the discretion of the licensing agency.
LIC 956 (1 0/99) (PUBLIC)
r--.,, ~.'::~: ...... 1::··~~~
"~~r···
~·· .... ,~) ...
:....~)
I I..JC•
,., It'
i~
......... N
Authorized Signature Community Care Licensing Division
0 t../"!1 l!.i'•t
('') I~') ,.-(/1 1 ..... ;.:i!J! (J
STATE OF CAUFORNIA- HEALTH AND HUMAN SERVICES AGENCY
FACILITY EVALUATION REPORT
CAUFORNIA DEPARTMENT OF SOCIAL SERVICES COMMUNilY CARE UCENSING DMSION
San Jose Child Care, 111 N Marl<et, #300 San Jose, CA 95113
FACILITY NAME:
SHEPHERD OF THE VALLEY LUTHERAN CHURCH FACILITY NUMBER: 430702694
DIRECTOR: LEATHERMAN, SANDRA 1281 REDMOND AVENUE SAN JOSE
FACILITY TYPE: 850 (408) 997-4846
95120 ADDRESS: TELEPHONE: CITY: STATE:CA ZIP CODE:
CAPACITY: 60 CENSUS: 0 DATE: 02/23/2006 08:15AM 02:30PM
TYPE OF VISIT: AnnuaVRandom UNANNOUNCED TIME BEGAN: MET WITH: Sandra Leatherman TIME COMPLETED:
DEFICIENCY INFORMATION FOR THIS PAGE: CIVIL PENALTY INFORMATION:
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
Not Applicable
COMMENTS/DEFICIENCIES
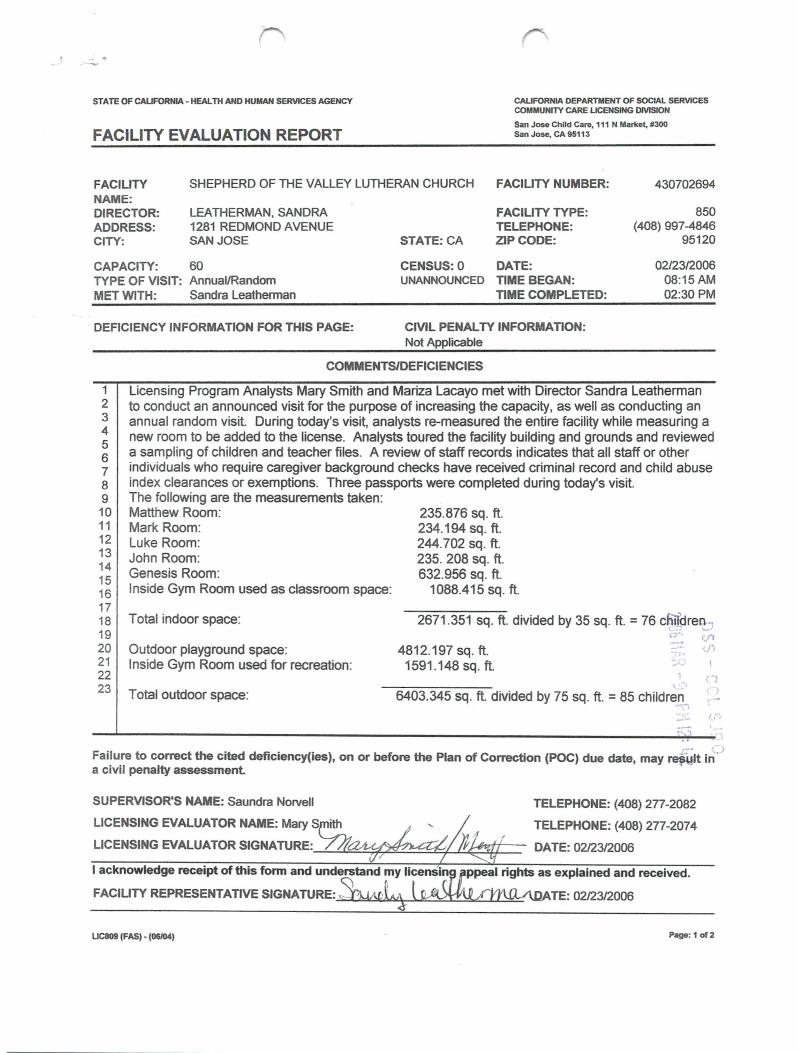
Licensing Program Analysts Mary Smith and Mariza Lacayo met with Director Sandra Leatherman to conduct an announced visit for the purpose of increasing the capacity, as well as conducting an annual random visit. During today's visit, analysts re-measured the entire facility while measuring a new room to be added to the license. Analysts toured the facility building and grounds and reviewed a sampling of children and teacher files. A review of staff records indicates that all staff or other individuals who require caregiver background checks have received criminal record and child abuse index clearances or exemptions. Three passports were completed during today's visit. The following are the measurements tak~n: Matthew Room: Mark Room: Luke Room: John Room: Genesis Room: Inside Gym Room used as classroom space:
Total indoor space:
Outdoor playground space: Inside Gym Room used for recreation:
Total outdoor space:
235.876 sq. ft. 234.194 sq. ft. 244.702 sq. ft. 235. 208 sq. ft. 632.956 sq. ft.
1088.415 sq. ft.
2671 .351 sq. ft. divided by 35 sq. ft. = 76 c~ttJreGJ-...:..1 4812.197 sq. ft.
1591 .148 sq. ft.
::·.: t!./l ..,.,L<rlok ·~/'~
~~·:~; n
,,,,C)
6403.345 sq. ft. divided by 75 sq. ft. = 85 children ·"''\',"\ -· . .... ,.'~.~<
Failure to correct the cited deficiency(ies}, on or before the Plan of Correction (POC} due date, may re~~lt i~:J a civil penalty assessment
SUPERVISOR'S NAME: Saundra Norvell TELEPHONE: (408) 277-2082
LICENSING EVALUATOR NAME: MaryS TELEPHONE: (408) 277-2074
LICENSING EVALUATOR SIGNATURE:_£..~~~~~~~.1.!.1;,'-::.~1J'==~ DATE: 02/23/2006
I acknowledge receipt of this form and understand my lie~ explained and received.
FACILITY REPRESENTATIVE SIGNATURE: ~4l TE: 02123/2006
UC809 (FAS) - (06104) Page: 1 of2
STATE OF CAUFORNIA - HEALTH AND HUMAN SERVICES AGENCY
FACILITY EVALUATION REPORT
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES COMMUNITY CARE LICENSING DMSION
San Jose Child Care, 111 N Marl<et, #300 San Jose, CA 95113
FACILITY NAME:
SHEPHERD OF THE VALLEY LUTHERAN CHURCH FACILITY NUMBER: 430702694
DIRECTOR: ADDRESS: CITY:
LEATHERMAN, SANDRA 1281 REDMOND AVENUE SAN JOSE
CAPACITY: 60 TYPE OF VISIT: Annual/Random MET WITH: Sandra Leatherman
DEFICIENCY INFORMATION FOR THIS PAGE:
FACILITY TYPE: TELEPHONE:
STATE:CA ZIP CODE:
CENSUS:O DATE: UNANNOUNCED TIME BEGAN:
TIME COMPLETED:
CIVIL PENALTY INFORMATION: Not Applicable
850 (408) 997-4846
95120
02/23/2006 08:15AM 02:30PM
COMMENTS/DEFICIENCIES
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
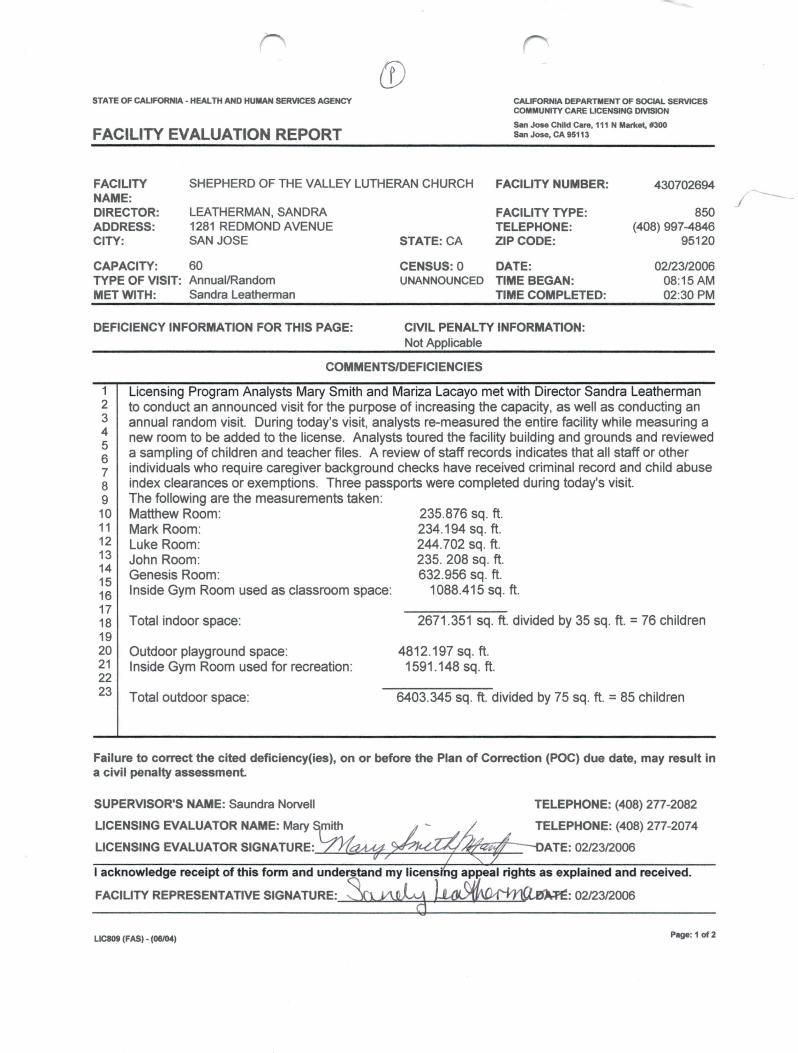
Licensing Program Analysts Mary Smith and Mariza Lacayo met with Director Sandra Leatherman to conduct an announced visit for the purpose of increasing the capacity, as well as conducting an annual random visit. During today's visit, analysts re-measured the entire facility while measuring a new room to be added to the license. Analysts toured the facility building and grounds and reviewed a sampling of children and teacher files. A review of staff records indicates that all staff or other individuals who require caregiver background checks have received criminal record and child abuse index clearances or exemptions. Three passports were completed during today's visit. The following are the measurements taken: Matthew Room: Mark Room: Luke Room: John Room: Genesis Room: Inside Gym Room used as classroom space:
Total indoor space:
Outdoor playground space: Inside Gym Room used for recreation :
Total outdoor space:
235.876 sq. ft. 234.194 sq. ft. 244.702 sq. ft. 235. 208 sq. ft. 632.956 sq. ft.
1088.415 sq. ft.
2671.351 sq. ft. divided by 35 sq. ft. = 76 children
4812.197 sq. ft. 1591.148 sq. ft.
6403.345 sq. ft. divided by 75 sq. ft. = 85 children
Failure to correct the cited deficiency(ies}, on or before the Plan of Correction (POC) due date, may result in a civil penalty assessment
SUPERVISOR'S NAME: Saundra Norvell
LICENSING EVALUATOR NAME: Mary mith
LICENSING EVALUATOR SIGNATURE:_L:...t..f.;;Z:11;¢.,;z_~~~~~~
LIC809 (FAS) - (06/04)
TELEPHONE: (408) 277-2082
TELEPHONE: (408) 277-2074
Page: 1 of2
---_/
STATE OF CALIFORNIA - HEALTH AND HUMAN SERVICES AGENCY CAUFORNIA DEPARTMENT OF SOCIAL SERVICES COMMUNITY CARE LICENSING DIVISION
FACILITY EVALUATION REPORT (Cont) San Jose Child Care, 111 N Marl<et, 1¥300 San Jose, CA 95113
FACILITY NAME: SHEPHERD OF THE VALLEY LUTHERAN CHURCH DEFICIENCY INFORMATION FOR THIS PAGE: VISIT DATE: 02/23/2006
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
NARRATIVE/COMMENTS
There are no waivers for this site. During today's visit, analysts observed the following : Facility is on a winter break and there were no children present; CPR/First Aid for at least one staff person were on file; sign in and out sheets were revieWed; all required forms were posted and up to date; drinking water is available indoors and outdoors; there is adequate storage for children's belongings; staff and children 's bathroom are clean and in good working order; paper products are available; snack menus are posted and in compliance; kitchen has a sink with hot and cold running water; cleaning supplies are inaccessible to children and stored separately from any food; first aid supplies are available and properly maintained; medication procedures were reviewed and in compliance; furniture and equipment is age appropriate and in good repair; children do not nap at the facility; outdoor equipment is age appropriate, in good repair and resilient material is adequate; facility is clean, safe, sanitary and in good repair today. Director was advised that three of the gates surrounding the playground be locked, as they led to a driveway and a parking lot. Also, the carpet in the Genesis room needs to be thoroughly cleaned. The new fire clearance needed to increase the capacity and add the Genesis room has been received by licensing. Capacity is increased to 75 children as of today's date.
Today this facility is found to be in compliance with Title 22 regulations and no deficiencies are being cited.
A copy of "Notice of Site Visit" was posted and will remain posted for 30 days.
Failure to correct the cited deficiency(ies), on or before the Plan of Correction (POC) due date, may result in a civil penalty assessment
SUPERVISOR'S NAME: Saundra Norvell
LICENSING EVALUATOR NAME: Mary mith
LICENSING EVALUATOR SIGNATURE:-<-<u.=~""""".,;....:..;;.;;...;:..:.'-+--+"--"""""l;z:s...>.--
TELEPHONE: (408) 277-2082
TELEPHONE: (408) 277-2074
DATE: 02123/2006
I acknowledge receipt of this form and understand my appeal rights as explained and received.
FACILITY REPRESENTATIVE SIGNATURE: .s ATE: 02/23/2006
LIC809 (FAS) - (06/04) Page: 2 of 2
CALIFORNIA- HEALTH AND HUMAN SERVICES AGENCY ·· CALIFORNIA OEPARTMEI'rr OF SOCIAL SERVICES
COMMUNI1Y CARE LICENSING
~CILITY EVALUATION REPORT . REFER TO -. >ee other side for explanation of form. ACILITY NAME
.ODAESS
JEFICIENCY INFORMATION FOR TJ:!IS.PA~~: j 0 Type A 0 No DefiV'fJfl.fj t,17'--r~ 0 T eB ·
DUE TO DISTRICT STAFF SHORTAGES, THE A~U~ FACILITY EVALUATION DUE ON lsjJ.? /JtJ.A.-8-NOT COMPLETED.
• • .. . I
• ~ 1. I
POC DUE DATE
Failure to correct the above cited deficiency(!es), on or before the· Plan of COrrection ·(POC) due date1 may result In a civil penalty assessment of $50 per day (Family Child Care Homes, Foster Family Homes and all governmental agencies are exempt).
NAME
AGENCY COPY
I understand my licensing appe;!al rights as ex lained on the back of this form. ·
DATE
Page ___ of ___ pages __