Embed Size (px)
DESCRIPTION
Sidney Kimmel Medical College at Thomas Jefferson University alumni Bulletin.
Citation preview

A L U M N i B U L L e T i N
SiDNey KiMMeL MeDiCAL CoLLege AT THoMAS JeFFeRSoN UNiveRSiTy • SUMMeR 2014
Jefferson Receives Its
from Sidney Kimmel FoundationLargest-Ever Gift

Calling all ’4s and ’9s!ALUMNi WEEKEND 2014 • OCTOBER 24-25
oCToBeR 24 FridayeveNiNg
“Jefferson Pride” Welcome Reception Join fellow alumni on campus for a casual and entertaining evening with light fare and drinks. Sit back and relax as the Jefferson Chamber Orchestra, led by Bruce Fenderson, PhD, professor of pathology, anatomy and cell biology, performs. Stroll down memory lane and enjoy photos and yearbooks from our University Archives and Special Collections.
Come early on Friday to take advantage of a complimentary CME program and lunch.
oCToBeR 25 SaturdayMoRNiNg/AFTeRNooN• Legacy admissions workshop
• Campus tours highlighting the Dr. Robert and Dorothy Rector Clinical Skills & Simulation Center and Jefferson’s new anatomy lab
• “Taste of Philadelphia” luncheon hosted by Dean Mark L. Tykocinski, MD, who will deliver his annual “State of the College” address
eveNiNg (THE UNiON LEAGUE OF PHiLADELPHiA)• Class photos and cocktail receptions
• Three-course sit-down dinner
• Presentation of Alumni Achievement Award
Register online:Advancement.Jefferson.edu/AlumniWeekend2014
For more information: contact the Office of Alumni Relations at 215-955-7750 or [email protected].
Hotel rooms are blocked at the following locations. Don’t forget to mention “Jefferson Alumni Weekend” when booking to get these special discounted rates!
Inn at the Union League215-587-5570Single/Double: $229/nightSuite: $279/nightReservation deadline: Sept. 25
Ritz-Carlton Philadelphia 1-888-505-3914Single: $245/nightReservation deadline: Sept. 23

Contents
Jefferson Alumni Bulletin Summer 2014 Volume 63, Number 3
Senior Vice President: Elizabeth A. Dale, EdD
Editor: Gail Luciani
Associate Editor: Karen L. Brooks
Design: Jefferson Creative Services
Bulletin Committee William V. Harrer, MD ’62 Chair James Harrop, MD ’95 Cynthia Hill, MD ’87 Larry Kim, MD ’91 Phillip J. Marone, MD ’57, MS ’07 Joseph Sokolowski, MD ’62
Quarterly magazine published continuously since 1922.
Address correspondence to: Editor, Alumni Bulletin Office of Institutional Advancement Thomas Jefferson University 125 S. 9th Street, Suite 700 Philadelphia, PA 19107-4216
215-955-7920 Fax: 215-503-5084 Advancement.Jefferson.edu Alumni Relations: 215-955-7750
The Jefferson community and supporters are welcome to receive the Alumni Bulletin on a regular basis; please contact the address above. Postmaster: send address changes to the address above. iSSN-0021-5821
Copyright© Thomas Jefferson University. All Rights Reserved.
Cover: Jefferson President and CEO Stephen Klasko, MD, MBA, with Sidney and Caroline Kimmel and Jefferson Provost Mark Tykocinski. Photo by Matt Lester.
CS 14-1937
FEATURES
8 Jefferson Receives Its Largest-Ever Gift from Sidney Kimmel Foundation
10 Surgery or Surveillance? BRCA Mutation Carriers Weigh Their Options
14 The New Face of Surgery
DEPARTMENTS
2 DeAN’S CoLUMN
6 FiNDiNgS Focused Ultrasound Reduces Cancer Pain
18 ALUMNUS PRoFiLe 10 Questions with . . . Walter L. McConnell, MD ’59
20 FACULTy PRoFiLe Joseph F. Majdan, MD, CV '81: Alumni Association Welcomes New President
22 PeoPLe
23 CLASS NoTeS
25 iN MeMoRiAM
29 By THe NUMBeRS
ALUMNi WEEKEND 2014 • OCTOBER 24-25

2 Sidney Kimmel medicAl college Alumni Bulletin
On May 29, 2014, Dean Mark L.
Tykocinski, MD, shared the following
comments with graduates at Jefferson’s
190th commencement ceremony at the
Kimmel Center for Performing Arts.
His remarks appear here, adapted, in
lieu of his usual column. A video of his
address is available on our website at
Advancement.Jefferson.edu.
As graduates of our distinguished medical
college, you are emboldened by four years of
hard-earned medical knowledge and
know-how. While celebrating this most
impressive achievement, i’d like to temper
your sense of empowerment just a bit and
urge you to retain a healthy dose of humility
— enabled, yes, but not all-knowing. you will
be lured, at times virtually forced, to project
an air of total confidence, expected to play
the highly intelligent and informed
physician. my message to you today is simple
— resist this tug, hold back — and
importantly, never start with talking. Always
start with listening. the power is in the
listening — hone this as an art and
understand all its dimensions.
the first dimension? listen with ears
wide open. Assimilate and be guided by
what you actually hear, by the facts, and
importantly, do not prejudge what is
possible or impossible. in our world of
biomedicine, the impossible morphs into
the possible at a dizzying pace — we are
dazzled by fundamentally new ways of
perceiving things and by new, sometimes
radically different, solutions to challenges
that yesterday seemed intractable. Just this
past year:
• For the visually impaired, next-generation
google glass that converts into words
what the eyeglasses see.
• For the immobile, wheelchairs that
descend stairs.
• For the cancer-ridden, injectable nano-
satellites that propel themselves to tumor
beds and heat them into oblivion.
• For the amputee, an artificial hand that
transmits the sensation of touch to its
user’s brain.
• For the injured, bio-printed tissue patches
— mini organs, if you will.
• For gene defects, a technology that allows
one to modify broken genes, with the hint
of someday repairing them.
• And right here at Jefferson, the discovery,
via high-power computational analytics,
that there are far, far more small genetic
elements floating inside our cells than we
had ever imagined, opening an exciting
The Dean’s Column
avenue to unravel the mysteries of small
RnA-regulated gene control.
So be receptive to new ideas. the
improbable can materialize — the
impossible can become possible. though we
have pressed you to be critical thinkers,
don’t wall yourselves off as relentless
skeptics.
A second dimension to the art of
listening: listen in high fidelity, without
bias. We are hard-wired to force-fit what we
hear into our preconceived notions and
convenient narratives. Psychologists speak
of this as “confirmation bias” — a cognitive
process whereby we conform what we hear,

SummeR 2014 3
to enshrine what we hold sacred. We look
for and find confirming evidence in our
beliefs, ignoring or rationalizing away all
disconfirming evidence. We remember in
great detail studies that support our
preferences, forgetting all counter-
examples. We befriend people who think
like us, further reinforcing our beliefs.
in “the unpersuadables,” Will Storr tours
the world interviewing enemies of science,
those with the craziest of irrational beliefs,
from Holocaust deniers to homeopaths.
confirmation bias, Storr concludes, is what
locks people into their hopelessly distorted
worldviews, what makes them
unpersuadable.
it turns out many research results, even
those published in the most prestigious
journals, are hard to reproduce. And
“many” is in fact a gross understatement.
A few years ago, scientists at Amgen were
able to replicate only six of 53 studies
considered landmarks in the basic science
of cancer, even though they cooperated
closely with original researchers to ensure
consistency in methodology. months earlier,
Bayer Healthcare reported that it had
successfully reproduced published results
in only one-quarter of 67 seminal studies.
the implications of this inconvenient truth
— if companies cannot rely on academic
research, the pipeline artery for new drug
development clogs up and dwindles away.
the failure to meet the basic standard of
reproducibility has been attributed to the
publish-or-perish culture in academia,
which pushes scientists to publish more
quickly than may be wise. While outright
fraud is rare, questionable research
practices are more common. Statistical
mistakes are widespread. Sample sizes are
often insufficient. imperfections in the data
are glossed over. the list goes on.
i suggest a more essential root cause —
that is, confirmation bias — all the more
dangerous when it insinuates itself into our
own research work product. experimental
models can be “tuned” to enable
researchers to perceive a pattern where
none exists and over-fit their data.
intriguingly, the very choice of hypotheses
can invite confirmation bias. to boost
chances of publication in high-profile
journals, scientists want surprising and
exciting results, and so they formulate and
test hypotheses that are “unlikely.” But
guess what — the unlikely is more likely to
be untrue, and thus irreproducible. the
pressure to muffle the sounds of the likely
and suppress the data’s actual message can
be overwhelming. We deafen ourselves
through bias.
A third dimension: listen with your
heart. Where real human lives are at risk
of being tossed about and set adrift, allow
yourselves to hear the human cry, and set
aside personal or institutional ego and
narcissism.
case in point — 15-year-old Justina
Pelletier, treated at tufts medical center
for a rare mitochondrial disease affecting
cellular energy production. When
wheelchair-bound Justina began
experiencing some gi symptoms, she was
referred back to her former
gastroenterologist at Harvard’s Boston
children’s Hospital. When she arrived by
ambulance that snowy night, the resident
on call brought in a Harvard psychologist
who hastily diagnosed Justina with a rare
somatoform disorder, a mental condition in
which real symptoms have no physical or
biological explanation. the family’s plea to
have her seen by the gastroenterologist,
and then returned to tufts to be treated for
the mitochondrial disease, was ignored.
So ensued a very public legal clash
between tufts and Boston children’s. the
state swiftly took custody of Justina away
from her parents, concluding that by
rejecting the new psychiatric diagnosis the
parents had committed medical child
abuse. Alan dershowitz of Harvard law
was retained to prosecute the case on
behalf of the family.
one can’t help but think that two Boston
academic powerhouses should somehow
have been able to listen to the patient’s
needs at a different frequency — one

4 Sidney Kimmel medicAl college Alumni Bulletin
resonating with their hearts — and
to put aside institutional arrogance
and agendas to prevent the
fracturing of a family. listening
from the heart means allowing some
subjectivity into the mix — at times,
humanity can trump hard-nosed
scientific opinion.
Another dimension to the art of
listening: listen for sounds, but also
stay attuned to the absence of
sounds. the masterful conductor
claudio Abbado spoke lyrically of a
“certain sound to snow … a falling
sound, fading away to nothing,
pianissimo, like a breath. you could
hear it only if you listened to what
some supposed was silence.” And he
characterized the magical silence at
the end of Bruckner’s ninth, when
the final three minutes fade away to
nothingness, as “trembling with
possibility, like the falling of snow.”
this provocative metaphor
speaks to me in framing the
different dimensions of listening —
from hidden music to hidden
messages. Hear not just what is
articulated, but also what is not
said. the unsaid is fraught with
meaning and context. there is
power in silence. this past
november, my wife and i sat in this
symphony hall, in the presence of itzhak
Perlman, one of the world’s magnificent
violin virtuosos, who was guest-
conducting. the music was wonderful, of
course, but what most grabbed my
attention that evening was watching
Perlman climb the conductor’s platform,
which was literally situated where i am
now standing. i was totally mesmerized by
the slow motion tableaux as this victim of
polio, at age 4, ascended the platform steps,
crutches in hand. Absolute silence gripped
the audience, as Perlman swung each
crutch forward, pivot after pivot, clawing
up the steps. He was, no doubt, conveying
an even deeper, subliminal message to the
hushed audience, by having no one at his
side, no one even within catching distance.
Perlman was drawing upon the power of
silence to turn his personal challenge into
strength — no rush up the steps, he alone
controls the pace, all must wait patiently,
listen to clanging of crutches and
intermittent silences during a tenuous
ascent.
Perlman conducted Beethoven’s
Symphony no. 2 that evening, a work that
Berlioz characterized as “smiling
throughout,” with its humor and vitality.
ironically, this piece was composed at a
bleak phase of Beethoven’s life, when he
penned a famous unsent letter to his
brothers, in which he expressed utter
despair over his loss of hearing and
contemplated suicide. “only my art held me
back,” he wrote. “it seemed to me impossible to
leave the world until i had produced all i felt was
within me.” Beethoven would continue to
triumph and create the most magnificent sounds
of music even as he himself was sadly entering a
world of silence.
And lastly, a fifth dimension to the art of
listening — keep an ear to the future —
anticipate the next sounds, some of which may
be approaching from sideways. call it “peripheral
hearing,” if you like. Just when you start to feel
smug, when you think you’ve arrived at the
destination, keep listening for more — vigilant
for opportunities or complications down the
road. every end is only a beginning. What you
know now is incomplete — there will always be
more. in the words of t.S. eliot: “never cease
from exploration, and at the end of all exploring
you arrive where you started and know the place
for the very first time.”
listening to the future can lead us to entirely
new platforms. take “predictive intelligence” —
an emerging concept in web search: anticipating
what information users will need, based on
context and past behavior, and providing it
before they have even asked for it. this is
listening on steroids, sensing the future. imagine
the impact of predictive intelligence on health
care — listening that is attuned to the patient’s
future wants. listen not only in the present, but
also for what is barely in hearing shot.

SummeR 2014 5
So in closing, class of 2014, my message
to you — master the art of listening, and
stay attuned to all its sundry dimensions:
• Retain humility, and reinforce a reflex to
first listen, and then speak — unlike
icarus, who hurled toward the sun, with
unbridled over-confidence and
enthusiasm. you always have more to
learn and hear.
• Listen critically, but also listen with an
open mind. Be ready to rely on what you
actually hear and be guided by the facts;
remain open to the heterodox and the
out-of-the-box; who knows where the
next frontier will take us.
• While open to the new and
transformational, fight confirmation bias
that taints the unpersuadables and makes
scientific research irreproducible; listen
to your own data, even if it contradicts
your most interesting hypotheses.
• Listen with your heart, and let it trump
your brain when humanity calls for it.
• Listen attentively for that which is not
said, for the context and information that
is being conveyed through silence;
appreciate the power of silence; and i
might add, recognize that those who
speak little can carry a big stick.
• And lastly, leave all questions open, don’t
lock your concepts in stone, don’t encase
your narratives in cement — endings are
only beginnings, and the quest for new
knowledge should be never-ending.
class of 2014, thomas Jefferson spoke of
“generational revolutions” — you are living
through one now. times of change, like
these, demand hyper-acute listening.
graduates, be willing to frame new
possibilities, new mindsets, built around
strong principles, and do this through
relentless listening.
you were the first class of the medical
college to have experienced the dean’s
concert Series, a program designed to
expose you to world-class performers — a
noontime break to indulge in listening. But,
class of 2014, your listening prowess
became wonderfully evident this past fall
in another, more profound way. in a
moment of class crisis — when your
classmate greg Snyder was battling the
early sequelae of his accident, you heard
the need, and mobilized all to revive
Jefferson’s Black and Blue Ball tradition,
but with a specific mission — to dedicate
proceeds to help a classmate at a critical
moment. you listened with your hearts.
And to greg, who is celebrating with you
here today — while your formal graduation
may have been delayed until next year, you
are forever in the hearts of the class of
2014, and in my own heart as well. you are
a listener supreme who i am confident will,
like Perlman, wield sounds and silences to
do great things in this world.
As you now take the sacred oath of
Hippocrates, hear the profession’s ancient
call to service, heed its admonitions and
affirm your commitment to others in the
most professional and altruistic ways. And
permit yourselves to listen with intelligence
and feeling to those in need around you.
We salute all those who brought you to
this point in life — your parents and family
who nurtured and supported your passion
for service and inquiry. As you cross this
stage, it is indeed the dreams of all of us
here today that accompany you. you enter
a long tradition that dates from
Hippocrates, to mcclellan and gross,
through gibbon, and now to you. it is your
turn to join, to continue, and to enhance
Jefferson’s legacy of service, and to
perpetuate that desire to make a
difference that brought you to Jefferson
four years ago.
mark l. tykocinski, md Provost and Executive Vice President for Academic AffairsAnthony F. and Gertrude M. DePalma Dean Sidney Kimmel Medical College at Thomas Jefferson University

6 JeFFeRson MedicAL coLLege ALuMni BuLLetin
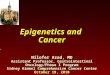
When cancer progresses and spreads to the bone, patients often suffer debilitating pain. now, a new phase iii clinical trial shows that non-invasive magnetic resonance-guided focused ultrasound treatment, which heats the cancer within the bone, relieves pain and improves function for most patients when other options are limited.
magnetic resonance-guided focused ultrasound surgery (MRgFus) has been used safely to treat thousands of women with uterine fibroids. However, “this is the first phase iii study to use this technology in the treatment of cancer,” says prin-cipal investigator and lead author mark Hurwitz, md, vice chairman of quality, safety and performance excellence and director of thermal oncology in Jefferson’s department of Radiation oncology.
Although radiation therapy is commonly used to treat bone-related
Focused Ultrasound Reduces Cancer PainNon-invasive focused ultrasound thermal therapy reduces pain from bone metastases
Findings6 Sidney Kimmel medicAl college Alumni Bulletin
pain, not all patients experience relief, and those who do may have recurrence of pain. in addition, the maximum safe radiation dose does not always control patients’ pain.
A total of 147 patients from 17 centers in the united States, canada, israel, italy and Russia were enrolled in the study and randomized to undergo MRgFus or a sham treatment. Patients in the treat-ment group received focused ultrasound precisely targeted to their bone tumors to heat the tumor tissue to between 65 and 85 degrees celsius, resulting in its destruction. during each treatment, patients were monitored in real time via mRi to ensure the right tissue was targeted and the right temperatures were reached while ensuring heat in surrounding normal tissues and organs remained at safe levels. the control group underwent the same procedure but
without the ultrasound device turned on. Finally, patients who did not respond to the placebo treatment within two weeks were allowed to be unblinded and offered MRgFus.
Patients responded well to treatment, with 64 percent experiencing either no pain or significant pain reduction, and many were able to reduce or stop use of opioid medications. most patients experi-enced relief within days of treatment.
the next steps in this line of research, Hurwitz says, are to refine the treat-ment technique to get an even greater response rate and to apply radiation and thermal therapy together in treatment of bone metastases. Jefferson has launched a new program for thermal oncology within the department of Radiation oncology to provide patients with access to thermal therapies that have been shown to augment radiation treatment.
Bone metastasis usually occurs in patients who are suffering from another form of cancer, like lung cancer. The cancer spreads to the bone and forms tumors within the bone.

SummeR 2014 7
Denervation
Magnetic resonance-guided focused ultrasound surgery (MRgFUS) treatment targets the area of the bone metastasis. Reduction in pain can occur by several mechanisms. In addition to periosteal denervation, tumor debulking may also play a clinically significant role in symptom relief.
Tumor Debulking

8 Sidney Kimmel medicAl college Alumni Bulletin
Jefferson Receives its Largest-Ever Gift from Sidney Kimmel Foundation
With a nod to his hometown as well as his faith in Jefferson’s ability to revolutionize health care nationwide, philanthropist Sidney Kimmel and his wife, Caroline,
through the Sidney Kimmel Foundation, have given $110 million— the largest gift in Jefferson’s 190-year history — to benefit Jefferson Medical College, which has been renamed the Sidney Kimmel Medical College at Thomas Jefferson University.
“My heart has always been in Philadelphia, and Jefferson is the soul of this city,“ said Mr. Kimmel when making the investment in June 2014.
Over the past year, Jefferson has begun a journey to transform the way medicine is taught, patient care is delivered and breakthrough treatments are discovered. The gift will provide critical support in the pursuit of these goals.
Sidney Kimmel was born and raised in Philadelphia and was the founder and chairman of Jones Apparel Group, one of the world’s leading designers and marketers of branded apparel, footwear and accessories. Since 1993, the Sidney Kimmel Foundation and its subsidiary, the Sidney Kimmel Foundation for Cancer Research, have committed more than $750 million to philanthropic causes.
Nearly three-quarters of these gifts have benefited cancer research through the establishment of cancer centers, including Jefferson’s Sidney Kimmel Cancer Center.
Of the nation’s 140 accredited medical colleges, only 10 have been named as a result of endowed gifts of $100 million or more. This gift from the Sidney Kimmel Foundation places Jefferson among the top five and is also a vote of confidence as the institution prepares to launch a comprehensive fundraising campaign. Alumni can take pride in knowing that their medical college will have the resources to continue to grow in stature, quality and reputation in today’s highly competitive environment.
Jefferson celebrated the Kimmels’ generosity with an event on campus June 18. A special alumni informational session and reception was hosted July 21 by Dean Mark L. Tykocinski, MD; President and CEO Stephen K. Klasko, MD, MBA; and Alumni Association President Joseph F. Majdan, MD, CV '81. if you were unable to attend these events and have questions about the gift and name change, please feel free to contact Majdan at 215-503-4226 (o), 215-801-6791 (m) or [email protected].
Jefferson President and CEO Stephen Klasko, MD, MBA, with Caroline and Sidney Kimmel; Mark Tykocinski, MD, Anthony F. and Gertrude M. DePalma Dean of the Sidney Kimmel Medical College at Thomas Jefferson University and Joseph Majdan, MD, CV'81, SKMC Alumni Association President. Photo by Matt Lester.

From the Deanin 1790, Edmund Burke, a contemporary of Thomas Jefferson, spoke eloquently of his ideal for the state, and his words translate readily to a magnificent institution such as ours:
“It is a partnership in all science; a partnership in all art; a part-nership in every virtue and in all perfection … a partnership not only between those who are living, but between those who are living, those who are dead and those who are to be born.”
Jefferson is a partnership of art plus science; it is a partnership of past plus present plus future.
As stewards of a remarkable 190-year legacy, we at Jefferson understand that stewardship is not merely preservation; it does not equate to stasis or inflexibility. Stewardship respects the past by embracing the future — it begs for nimbleness and adaptability, invites evolving visions and recognizes that an institution’s survival, let alone its vibrancy, demands openness to creative thought and transformative action.
Philanthropic giving is the lifeblood of such dynamic stewardship. Sidney and Caroline Kimmel’s inspirational giving empowers Jefferson’s leaders to be effective stewards. Committed to preserving the best of what has made Jefferson distinctive, we can leverage their gift to cultivate a community of scholars and clinicians who remain relevant for the century ahead of us and a campus sparkling with learning and discovery.
Jefferson has too often been referred to as one of the nation’s best-kept secrets. The Kimmels’ generosity ensures that we will be a secret no more. Our trajectory these past few years has already caught the attention of many — our flagship hospital, empowered by its associated physician practices, has risen to national prominence; our faculty create new scientific paradigms; our medical students shine, in their unparalleled community service and their clinical abilities when they enter the most competitive residency programs.
Now, the speed of Jefferson’s ascent will accelerate. This gift will be a catalyst for more giving, and we will use this financial leverage wisely — investing in our human capital, faculty and students in ways that carry us to new heights in the years to come. As the future unfolds here at the Sidney Kimmel Medical College at Thomas Jefferson University, we will create a faculty of the future that trains a new kind of medical student — 21st-century leaders who pioneer healthcare delivery and discovery for our communities and society at large.
Mark L. Tykocinski, MD Provost and Executive Vice President for Academic Affairs Anthony F. and Gertrude M. DePalma Dean Sidney Kimmel Medical College at Thomas Jefferson University
SummeR 2014 9
How Will the Funds Be Used?
The Sidney Kimmel Foundation’s investment will enable Jefferson to continue attracting the most talented medical students and faculty, drive scientific research that inspires medical innovation and foster an entrepreneurial approach to healthcare education that meets the future needs of our society.
We will create a pathways program that will pioneer a ground-breaking “Beyond Flexner” approach to 21st-century medical education. The Caroline Kimmel Endowment Fund for Scholarships will allow us to attract top medical students who exhibit both high intellectual and emotional intelligence and who have degrees in cross-cutting fields, such as architectural design, computational science and social sciences.
We will also create an Institute for Advanced Study to support a collegium of elite research faculty. The Sidney Kimmel Innovation and Research Fund and the Sidney Kimmel Presidential Endowment Fund will provide professorships for domain experts and world-class authorities across programmatic research theme areas that are deemed “fields of the future” in the biomedical sciences.
The Sidney Kimmel Capital Fund will support the creation of a state-of-the-art conference and think-tank facility that will allow us to implement a robust visiting-scholars program, hosting field leaders from the United States and abroad.
Jefferson Receives its Largest-Ever Gift from Sidney Kimmel Foundation
Above: Klasko; Matt DeCaro, MD ‘80; Stanton Miller, MD '80; and Philip Nimoityn, MD ‘76. Below: Tykocinski; Howard Weitz, MD '78; Charles Pohl, MD '87; and Geno Merli, MD '75. Photos by Matt Lester.

10 Sidney Kimmel medicAl college Alumni Bulletin
SURGeRySurveillance?
or

SummeR 2014 11
last year, 37-year-old actress Angelina Jolie generated global headlines by revealing she’d had a double mastectomy to reduce her risk of breast cancer. Jolie, who carries a mutation in the BRcA1 gene and lost her mother to ovarian cancer in 2007, again made news this spring when she announced plans for another cancer-prevention surgery: removal of her ovaries.
Physicians around the world reported seeing an immediate “Jolie effect” after the star publicized her medical situation. many women, particularly young ones, developed a sudden interest in genetic testing and be-came inspired to learn more about options
for controlling their own cancer risks.Preventing cancer through surgery is not
a new phenomenon; for years, physicians have advised BRcA1 and 2 mutation carri-ers to consider prophylactic mastectomies and oophorectomies, or removal of the ovaries. About 70 percent of women who learn they have the mutations opt to have an oophorectomy, and up to 40 percent have a mastectomy. But these procedures are not right for every woman.
massimo cristofanilli, md, director of the Jefferson Breast care center, says that while an increase in awareness of genetic counseling is a good thing, the downside to publicity is that patients sometimes act out of fear and make uninformed decisions.
“Since Angelina Jolie’s story, all women want to know if they have BRcA mutations. the media can confuse them by imparting so much information about a role model doing something so drastic. Surgery is a very personal decision, and we must help each patient properly assess her risk and approach cancer prevention in the way that is most appropriate,” cristofanilli says.
BRCA Genes: What Are They?BRcA1 and 2 genes (BReast cAncer genes 1 and 2) are inherited mutations that significantly increase a woman’s risk of developing breast and ovarian cancer. According to the national cancer institute, these mutations account for 5 to 10 percent of breast cancers and 15 percent of ovarian cancers.
the nci says that fewer than 2 percent of all women develop ovarian cancer
during their lifetimes, but 39 percent of BRcA1 carriers and up to 17 percent of BRcA2 carriers do. About 12 percent of women develop breast cancer, but a BRcA mutation raises the risk four- to fivefold.
Past studies have shown removal of the ovaries and fallopian tubes in premenopausal women with BRcA muta-tions lowers risk for ovarian cancer by up to 95 percent and breast cancer by up to 60 percent, since the ovaries produce hormones that drive breast tumor growth. ovarian cancer is especially deadly, and there is no reliable method for early detection like there is for breast cancer — so physicians often recommend that women with a BRcA1 mutation, which generally leads to cancer at a younger age, have their ovaries removed as soon as they are finished having children.
New Recommendations for SurgeryA canadian study released in February 2014 was the largest ever to capture the protective powers of ovarian removal for BRcA1 and 2 mutation carriers and the first to break down different recommenda-tions for each gene. overall, researchers found that women who had oophorecto-mies reduced their risk of ovarian cancer by 80 percent and their risk of death before age 70 from any cause by 77 percent. in the study, oophorectomy benefits varied based on the gene involved. BRcA1 carriers got the clearest advan-tage if surgery was performed by age 35, reducing their lifetime cancer risk
STORy SUMMARy
• Mutations in the genes BRCA1 and BRCA2 sharply increase the risk of breast and ovarian cancers.
• About 70 percent of carriers opt to have their ovaries removed and up to 40 percent have their breasts removed to reduce cancer risk.
• A new study suggests that BRCA1 carriers should pursue ovary removal by age 35 and BRCA2 carriers by age 40, although some physicians hesitate to adopt such stringent rules.
• Surgery is a personal decision, and women must work with their health- care providers to determine their cancer risk and choose the best approach to prevention.
BRCA Mutation Carriers Weigh Their OptionsBy Karen L. Brooks

12 Sidney Kimmel medicAl college Alumni Bulletin
to about 1 percent — similar to women without mutations. the findings revealed no ovarian cancers in BRcA2 carriers under 40, suggesting those women can safely delay surgery an extra five years. current guidelines from the American college of obstetrics and gynecology recommend prophylactic oophorectomy for both BRcA1 and 2 carriers by age 40, but the study’s authors are pushing for 35 or younger to become the new universal standard for the procedure in BRcA1 carriers. Some physicians are hesitant to adopt such rigid guidelines. “it is extremely difficult to agree on a strict recommendation for age regarding this procedure,” cristofanilli says. “yes, there is an indication that a BRcA1 mutation can cause cancer earlier, and these women need to think about ovarian
removal as a preventive measure. But there are so many factors that must be considered, especially family history and family planning. in certain cases, it is appropriate to delay surgery as much as possible. A hard rule of ages 35 and 40 — i don’t know that it is right for everyone.” theodore n. tsangaris, md, surgical director at the Jefferson Breast care center, agrees, explaining that the findings could frighten women into acting before they’re ready. “everyone has different takes on the information that’s given to them, and no matter what procedure you’re talking about — oophorectomy or mastectomy — the optimal timing has to be determined individually. neither of these surgeries can be undertaken without significant compro-mises that patients have to consider, even
though we do know they are very effective and result in a very low risk of cancer,” tsangaris says. Bilateral mastectomy, which was not examined in the canadian study, has previously been shown to reduce breast cancer risk by 95 percent in women with BRcA1 and 2 mutations. As with all major surgeries, prophylactic mastectomy and oophorectomy carry potential complications such as bleeding and infection. many women have babies through their late 30s, and ovary removal sends patients into abrupt menopause with symptoms that can be severe. the risk of bone-thinning osteoporosis also increases, although it can be controlled through diet, exercise and supplements. Breast removal can cause anxiety by affecting a woman’s body image.
• BRCA1 and BRCA2 mutations are
uncommon (occurring in 1 of every
300 to 800 women, according to the
American College of Obstetricians
and Gynecologists) but are thought
to account for 5 to 10 percent of all
breast cancers and about 15 percent of
ovarian cancers.
• If multiple family members have had
breast or ovarian cancer, particularly
at a young age, the U.S. Preventive
Services Task Force says a woman
should discuss with a health profes-
sional if she’s at increased risk. A genetic
counselor can help her decide whether
to have a blood test to see if she inher-
ited faulty genes.
• Physicians advise women with BRCA
mutations to undergo frequent screen-
ings for breast cancer and to consider
having their ovaries removed between
ages 35 and 40 or when childbearing
is complete (recent research suggests
BRCA1 carriers should pursue surgery at
the earlier age).
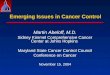
A Look at the Genes that Raise the Risk of Breast and Ovarian Cancer
BRCA Mutation Increases the Risk of Cancer
BRCA Mutation Carriers
General Population
<2%
Ovarian Cancerby Age 70
50
33%–50%
7%
27%–44%
56%–87%
Breast Cancerby Age 50 Breast Cancer
by Age 70
40
30
20
10
0
<2%

SummeR 2014 13
“tamoxifen is certainly something to consider for breast cancer prevention, but you don’t know how many years you’ll stay on it. this can turn into a lifelong treatment with a drug that has side effects. And if a patient is of reproductive age, she cannot have children while taking tamoxifen,” cristofanilli says. For postmenopausal women, the drug raloxifene is another option for cutting breast cancer risk.
Any BRcA mutation carrier who does not want to undergo a mastectomy should be closely monitored with frequent screenings.
“if someone is a carrier but doesn’t want to have surgery, she should have annual mammography and annual mRi, and we like to stagger it so she’s getting some form of imaging every six months,” lazar says. “the national comprehensive cancer network also recommends breast aware-ness starting at age 18 and a clinical breast exam every six to 12 months.”
unfortunately, there are no reliable methods for early detection of ovarian cancer.
“We do know of some markers, but there has not been success in developing a screening test,” cristofanilli says. “Women with a BRcA mutation do have to plan their families earlier rather than later and be prepared to make a major decision regarding ovary removal at a relatively young age.”
Jefferson Eyes New High-Risk Clinictsangaris says faculty members at Jefferson aim to establish a special service for women who have a high cancer risk, whether due to a BRcA mutation, strong family history or other factors. currently, he says, most services force these patients to get their information piecemeal.
“First, a woman might talk to the geneticist. And then, depending on what the geneticist tells her, she’s faced with some major decisions. if she’s genetically positive but doesn’t have cancer, what should she do? increase her screening? take a preventive like tamoxifen? or go ahead and have surgery?” tsangaris says. “We want to take away the confu-sion by creating a comprehensive clinic where women can get all the information they need from the appropriate experts— geneticists, oncologists, surgeons — in a streamlined way and then make intelligent decisions that are right for them.”
Key to the clinic’s success, he says, will be a full-time coordinator who will manage patients’ experiences from genetic testing to screening to prophylactic or therapeutic treatment.
“What Angelina Jolie did is not right for every woman, and after the Jolie effect, you need to help women put their risk in perspective. this is one of the top specialty clinics we’d like to offer, and we are currently looking for philanthropic invest-ments to support it. nobody else in our area is bringing coordinated, high-risk cancer care together like this, and women deserve clear information to determine what course of action makes the most sense.”
For more information about plans for a high-risk cancer service or to support the initiative, contact Paul Gunther, Director of Development for Oncology, at [email protected] or 215-955-9446.
Regardless of these drawbacks, says Jefferson breast surgeon melissa A. lazar, md ’06, the majority of BRcA mutation carriers are eager to move forward with prophylactic surgery. “most women who carry mutations have seen relatives experience cancer. they’ve seen loved ones go through treatments like chemo-therapy and have probably seen some pass away from the disease. i think their fear of developing cancer outweighs some of the negatives of surgery, and providing patients with resources for psychological support is important,” lazar says.
Alternatives to SurgeryFor mutation carriers who are strongly opposed to having surgery, other preventive measures can be taken. drugs like tamoxifen can cut a woman’s risk of breast cancer by up to half, as can ordinary oral contraceptives.
Tamoxifen
53%+
Mastectomy
90%
Oral ContraceptivesUP TO
60%
OophorectomyUP TO
96%
OophorectomyUP TO
68%
Proactive Cancer Management Reduces the Risk PRevenTIve MeASUReS
Breast Cancer
+ In contralateral breast cancer
Ovarian Cancer
CAnCeR RISK RedUCTIOn100806040200
HBOC is caused by BRCA1 and 2 gene mutations and is characterized by the following features in a family:
• Early age of onset of breast cancer (often before age 50)
• Family history of breast and ovarian cancer
• Increased chance of bilateral cancers (cancer that develop in both breasts, or both ovaries, independently) or an individual with both breast and ovarian cancer
• An autosomal dominant pattern of inheri-tance (vertical transmission through either the mother or father’s side)
• An increased incidence of tumors of other specific organs, such as the prostate
Other factors that increase the chance that a family has HBOC syndrome include:
• Family history of male breast cancer
• Ashkenazi Jewish ancestry
What is Hereditary Breast Ovarian Cancer (HBOC) Syndrome?

14 Sidney Kimmel medicAl college Alumni Bulletin
The
new Face of SuRgeRy
E. J. Caterson, MD, PhD '03, and Stephanie Caterson, MD '99, in surgery. Photo courtesy of Brigham and Women's Hospital.

SummeR 2014 15
Touch your forehead. Touch your cheek. Touch your chin. imagine doing that and feeling the skin of another person. imagine losing your face — and imagine receiving someone else’s.
the world’s first face transplant was performed in France in 2005. the recipient was a 38-year-old woman whose face had been mauled by her dog. Her surgeons had to overcome both the challenges of a complex experimental procedure that had never been done and the opposition of pres-tigious medical societies, which declared the transplant unethical and immoral.
nearly a decade later, 28 face trans-plants have been performed in seven countries, including six at Boston’s Brigham and Women’s Hospital, where e.J. caterson, md, Phd ’03, and Stephanie Houser caterson, md ’99, are members of an elite team that performs the rare procedure.
“our first transplant patient was trach dependent. He couldn’t speak, couldn’t smell and couldn’t taste his food,” says e.J. caterson. “After he recovered from his transplant, he could speak and he could smell; because he could smell, he could taste his food, which increased his nutrition level. He was no longer trach dependent, and his facial muscles moved so he could interact with the outside world. that was a huge improvement for that individual patient.”
With the rewards of transplanta-tion come risks before, during and after surgery. From the immunosuppression perspective, all transplant patients risk infection and adverse reactions to toxic anti-rejection drugs. “We transplant organs that are critical in terms of func-tion, because if it’s a not vital organ, is the transplant worth the potential risk?” asks Steven copit, md ’88, director of plastic surgery at Jefferson. “does the morbidity
of not having the transplant outweigh the morbidity of the treatment?”
Although still under investigation, the immunosuppression regimen for a face transplant is about the same as the one for an internal organ transplant. Because solid organ transplants are performed to replace a vital function, organs can be procured from a compatible donor and delivered to a suitable waiting patient. However, face transplants must be tailored to the defect of the recipient, and finding a donor who matches these very specific physical needs is a challenge. Potential donors are screened based upon sex, age, skin color, facial size and oral health. And the recipi-ents may be some of the most rigorously screened patients for surgery in the world.
“one of the true keys to a good result is proper donor selection,” says e.J. caterson. “Another reason that donors are hard to match is immunologic. PRA, which stands for Panel Reactive Antibodies, is, in a normal healthy male, quite low. Some of the PRAs we’ve had on our transplant patients have been over 85 percent. that means that we could pick donors from only 15 percent of the donor pool, so it can take a very long time.”
carmen tarleton is a case in point. in 2007, tarleton’s estranged husband broke into her home and beat her with a baseball bat, fracturing an eye socket and breaking her arm. He then sprayed her with indus-trial-strength lye, resulting in burns over 92 percent of her body; little of her face remained.
While tarleton was screened and approved for a face transplant, it took six years for doctors to find a suitable donor. A 20-hour surgery gave her the face of 56-year-old woman who had died after slipping into a coma following a massive stroke. “every case is different,” e.J. caterson says. “For carmen, the transplant was mainly soft tissue — her forehead, cheeks, nose, mouth and lips, without the boney component.”
tarleton’s appearance is still evolving, but her face is a composite — it doesn’t look like her pre-burn face, but it doesn’t look like the woman who donated it, either. “there is an aesthetic component not needed in internal organ transplants, because the face is clearly visible to the outside world,” he adds. “We have to insert a face so that it fits or transplants to the recipient without a mismatch. that’s the sort of art that’s still being worked out.”
The Facial Nerveconnecting the facial nerve part is considered the most important part of the surgery. “you can attach a face, but if you don’t animate it, if the patients can’t move their lips well or smile or open and close their eyes appropriately, that makes a huge difference in the ultimate functional and cosmetic result,” Stephanie caterson explains. “Hooking up the facial nerve that controls those independent actions is the last part of the operation — we could be 20 hours into the operation when we get to it.”
this independent function of the facial nerve is enhanced by tacrolimus, or FK-506, an immunosuppressive drug that is used mainly after an allogeneic organ transplant to reduce the activity of the patient’s immune system and lower the risk of organ rejection. “it has also been shown to improve nerve growth in a significant number of animal models in the lab,” he says. “So by putting the patient on immunosuppression drugs you can actually get the nerves to grow faster — sensory nerves as well as motor nerves that move the face. We put non-transplant patients who have lost the facial nerve and are undergoing facial reconstruction on a short window of immunosuppression. And we are getting excellent results because of the lessons we learned in the face trans-plant world. it’s a nice reverse innovation that is a result of our relationships with the facial transplant patients.”
By Gail Luciani
“There is an aesthetic component not needed in internal organ transplants, because the face is clearly visible to the outside world.”
- e.J. Caterson, Md, Phd '03

16 Sidney Kimmel medicAl college Alumni Bulletin
A Foundation from JeffersonWhen i was a student at Jefferson, i ran the
local Operation Smile chapter. The late Dr.
John Moore was the faculty advisor, and he
got me interested in plastic surgery because
of the humanitarian aspect of congenital
surgery (cleft lip and palate) that we could
do around the world.
Once I got into plastic surgery, I realized that
to repair a cleft lip and palate, I needed to do
a fellowship in craniofacial surgery. As a
result of that training, I learned how to take
the face apart and then put it back together.
I developed a skill set for dealing with cranial
facial trauma that allowed me to naturally
progress toward very complex cases.
i’ve been fortunate to have had wonderful
plastic surgeons as teachers. Drs. Steve
Copit, Jim Fox and John Moore gave me a
wonderful education at Jefferson and were
an inspiration. Now, my mentor is Dr. Julian
Pribaz, one of the best facial reconstruction
experts in the world. Working with him
inspires everyone on the team to go to the
next level.
E.J. Caterson, MD, PhD '03
My grandfather, father and sister all went to
Jefferson. But I wanted to be an astronaut,
not a doctor. So I went to the University of
Colorado and studied aerospace engi-
neering. I resisted going to medical school,
but my advisor told me that to be an astro-
naut, I would need a certain number of
higher education years. I could have done a
PhD, but because of my family, i was
familiar with medicine, and I was interested
in how the body changes in microgravity. I
thought okay, i’ll do it, but i’m definitely still
applying to be an astronaut.
i went to Jefferson and met Dr. John Moore.
He was so inspiring, i signed up for plastic
surgery as my third-year clinical rotation.
And i fell in love with it. There is a lot of
overlap between plastic surgery and engi-
neering; they are both about problem
solving. I started to think seriously about
plastic surgery even though it conflicted
with my dream of becoming an astronaut. I
decided to do five years of general surgery
and then apply for astronaut training. But in
2003, the space shuttle Columbia disinte-
grated as it reentered Earth’s atmosphere,
killing all seven crew members. The new
astronaut program was stopped. So I applied
for a plastic surgery fellowship and did
training at the Lahey Clinic in Boston. It
became evident that this was going to be
my path. I love it, and I have no regrets, but
it was circuitous how I got to where I am
today.
And i would not be here if it weren’t for the
people at Jefferson. I have a lot of respect
for them, especially the plastic surgeons.
Drs. Fox, Moore and Copit have been
incredibly supportive of me at every step. I
hear them in my head sometimes still. Dr.
Copit taught me how to hold a scalpel when
I was a third-year medical student, and I
teach my medical students the same way.
Stephanie Houser Caterson, MD ’99
E.J. and Stephanie Caterson with sons Ned and Henry.

SummeR 2014 17
The Future of Face Transplantsin 1998, Jefferson started a Phd program for cell and tissue engineering, the first in the country. And the first recipient of a Phd in that program was e.J. caterson. there has been progress toward the goal of using engineering principles to create tissue form and function, but organs can’t be created in a clinical laboratory. “i don’t anticipate that happening in the near future. So i look at transplants as a bridge to buy us time until we can grow organs in a laboratory that are free from the neces-sary evils of immunosuppression,” he says. “While we are trying to work toward using tissue engineering, we’re more likely to
make headway in the realm of immunosup-pression. We’ll be able to either have the antigen tied from the immune system in an organ or facial transplant or engineer the transplant to present to the immune system that it is not something that should be rejected. i think that’s where the first big breakthrough will come from before tissue engineering becomes a reality.”
As in other areas of medicine, teamwork is a critical component of success, and surgery is becoming more of a team effort. “drs. Julian Pribaz and Bohdan Pomahac are the leaders of face transplant program. i am the only cranial-facial surgeon on the face transplant team, and Stephanie is a premier microsurgeon and plastic surgeon,” he says.
While almost everyone on the face transplant program has some level of experience in microsurgery, Stephanie caterson is the microsurgeon with the highest patient volume in her division, performing about three procedures a
week in her breast reconstruction practice. “the blood vessels we connect are small, and the suture is no bigger than a human hair,” she explains. “microsurgery is very delicate, very technical and you need to have steady hands to do it.”
Face transplants require eight to 12 people on a team, rotating in and out, some working with the donor and others preparing the recipient. Several phases of the surgery require microsurgery, and that is her niche. She says that the most chal-lenging part of the procedure is preparing the recipient, because patients often have a lot of scar tissue from multiple attempts at reconstruction.
“We do the surgery as a team because we get a higher level of precision by having more than one attending surgeon working on a patient. that’s a new paradigm for the future of surgery. there will more collaborative opportunities with experts in other fields. it all comes together for a greater outcome,” he says. the catersons are also members of the team that does non-transplant facial reconstructive surgeries.
A recent report published online by The Lancet finds while the procedure is still experimental, risky and expensive, face transplants are generally safe and feasible. For victims of genetic disorders, gunshots, burns and other traumatic accidents, face transplants can be life changing, if not life saving. “none of our patients has any regrets, and some wish they could have had it done sooner,” she says.
While not all patients are appropriate candidates for facial transplantation, many may benefit from conventional reconstruction. “if we know that even with 10-15 operations we’re not going to get the results that we want, we may use the face transplant earlier,” he says. “However, when you have exhausted all recon-structive possibilities, a face transplant becomes the best option.”
While medical insurance may pay for the immunosuppressive regimen and associated medications, it doesn’t pay for the actual surgery. Still a rare event, it is unlikely to become a common procedure. “the real number of transplant cases is
actually quite low, and they will remain a relatively rare event in medicine. Based on input from the military, we estimate that there are probably only about 200 potential patients in the united States,” he says.
“i believe that we should provide conventional facial reconstruction as part of our practice. Face transplants are at the top of the reconstruction ladder. Are they experimental? yes, and we need to monitor and track our patients because we are trying to gain further experience. But in the end, they are simply another tool for providing the best results for our patients.”
“When you have exhausted all reconstructive possibilities, a face transplant becomes the best option.”
Read more about face transplant surgeries on the web at Advancement.Jefferson.edu/ facetransplant.

18 Sidney Kimmel medicAl college Alumni Bulletin
10 Questions with Walter L. McConnell, MD ’59 As part of its spring 2014 senior lecture series, SUNY Adirondack invited resi-dents in the Lake George area of upstate New York to campus every Tuesday from April 22 to May 13 to hear faculty and local experts speak on various topics. There were lessons in history, anthropology, local ornithology and one titled “Around the World — 10 Most Favorite Places.”
With the stamps of 110 countries in his passport, Walter McConnell, MD ’59, was a fitting speaker to compile such a ranking.
McConnell’s list includes the Tuscany region of Italy, Iguazu Falls in Argentina and Nepal, a country to which he has had close ties for nearly 40 years. In the late 1970s when he and his wife, Isabel, first visited the home of Mount Everest, McConnell caught the climbing bug.
In spring 1989, he returned to Nepal to ascend 29,029 feet above sea level to Everest’s summit. McConnell and his climbing team set off on May 16 for the final push toward the peak. With his teammates out of sight and his head-light not working, he fell behind, waiting until sunrise to continue. He forgot to turn on his radio, so when the others realized he was not with them, they called base camp to say he was missing. After sunrise, McConnell climbed to 27,000 feet before turning back as he realized he would not reach the summit in a safe time.
His climbing mates continued to the summit, but on the descent the lead guide, Phudorje Sherpa, fell to his death. He left behind a 14-month-old son.
McConnell has since returned to the Himalayas a dozen times. In 1992 and 1993, he attempted Everest again from Tibet, but conditions didn’t allow for a
climb to the summit. During his other trips to Nepal, McConnell has given back as a volunteer physician. He has worked in remote villages, delivering babies and caring for sick people and their animals.
McConnell has kept in contact with Phudorje’s son, Dorje Sherpa, now 26, supporting him to ensure he received an education. In May 2014, Dorje, along with two women from Nepal, traveled to the United States to spend the summer at McConnell’s home in the No. 1 most favorite place on his list, Lake George.
“We first came up to Lake George in 1962, and I said to my wife, ‘this is where we’re going to retire,’” he says. When he stepped down in 1996 as director of emergency medicine at Dover General Hospital in Dover, N.J., they retreated to Bolton Landing, N.Y.
“It’s absolutely beautiful here,” he says.
To read a complete list of McConnell’s 10 favorite places, log on to Advancement.Jefferson.edu/mcconnell
1. What drew you to your specialty? I think Jefferson was responsible for me going into primary care. It was empha-sized when I was going to school there, and a lot of my classmates went into primary care. Over time, my practice group got too big. We got taken over by carpetbaggers who only cared about the bottom line. That’s not why I got into practice. I ended up leaving and going into emergency medicine.
2. If you could work for a year in any location in the world, where would you do it? Nepal. I’ve gone there 12 times. Once I helped with the Nepal Ministry of Health on a medical study and twice for the Himalayan Rescue Association
in the remote village of Manang. I gave altitude lectures, delivered babies and even took care of their animals. I’ve gone back to the village and recon-nected with kids I delivered, people I took care of and even a horse I took care of. It was 10 years after I cared for the horse, and the owner brought him to where I was staying, and he rubbed my face against mine. He hadn’t forgotten me.
3. What was your first job? My dad set an example to work hard. From a young age, I took care of lawns, shoveled snow, parked cars at the local theater, then worked as a soda jerk at the local soda shop.
4. What’s on your bucket list (person-ally or professionally)? I have a few countries I haven’t been to: Cambodia, Laos and Vietnam.
5. If you had a theme song, what would it be? My favorite song is Frank Sinatra’s “I Did It My Way.” That’s how I’ve tried to live my life.
6. What is the best decision you ever made? I met my wife the first week in college. When we went out on our first date, I dropped her off and said “let’s go steady.” We got married the week after graduation in 1953.
7. What is the most adventurous thing you have ever done? Going to Everest. I went in 1989 from Nepal and twice from Tibet in 1992 and 1993. My climbing leader Scott Fischer in 1989 died on Everest in 1996 along with a well-respected guide from New Zealand, Rob Hall, whom I met in 1989.
Alumnus Profile

SUMMER 2014 19
No one summited either of those trips from Tibet.
8. What gets you out of bed in the morning? My morning bike rides or runs. When I was 30 years old, I was 65 pounds over-weight and smoked. I didn’t want to live like that, so I started running and I’ve been running ever since, all over the world.
9. What is your biggest pet peeve? Where our country is going with health care. I was the executive producer of a documentary called “Money-Driven
Medicine,” which was produced by Alex Gibney and shown on “Nightline” on ABC and “Bill Moyers Journal” on PBS. We had the opportunity to show the documentary in the Capitol audi-torium, and we invited every member of Congress. Only one senator showed up. The rest sent their assistants so we had a full house. As is discussed in the film, I believe we need to start looking at a patient as an individual and teaching wellness and prevention. I think our healthcare system needs a lot of work, and we need a big change in Washington.
10. What is the proudest moment of your career? While I was practicing in my hometown, Dover, N.J., I had five high-school teachers choose me as their primary care physician. I had the opportunity to deliver the chil-dren of five classmates and saw at least half of my high-school class while I was a primary care doctor. My proudest moment, though, was watching my son Jeffrey graduate from Jefferson in 1985.
— Stacey Miller
Photo by M. Cheri Bordelon

20 Sidney Kimmel medicAl college Alumni Bulletin
Sidney Kimmel Medical College Alumni Association Welcomes New President Joseph F. Majdan, MD, CV '81 Joseph F. Majdan, MD, CV '81, was elected president of the Sidney Kimmel Medical College Alumni Association in April 2014. Born in Hackensack, N.J., he was the only child of Polish immigrants. At 5, he moved with his parents to Bucks County, Pa., and later attended Holy Ghost Preparatory School. He then attended LaSalle University, where he obtained a Bachelor of Arts in history and biology. He received his doctor of medicine degree at the University of Pennsylvania School of Medicine and completed his resi-dency in internal medicine at the Presbyterian-University of Pennsylvania Medical Center. Majdan came to Jefferson in 1981 for a fellowship in cardiovascular medicine and is still here 33 years later.
The Alumni Association reminds us of our noble heri-tage and challenges each and every one of us to be a living example of all that has been, is and must always define a Jefferson physician. There was something about Jefferson that touched me when I first came here and still does so to this very day, for Jefferson is more than an iconic institution of learning and healing. Its greatness has been and continues to be perpetuated by the people who were its past and are its present. And I thought, “This is a family that I so wanted to be a part of.” I wake up every day and am so thankful for having been given the opportunity to teach and practice here. I am so proud to be able to say “I am a Jeffersonian.”
I still remember the doctor I had as a child; he was a Jefferson graduate. His name was Dr. Francis X. Thomas. He was the epitome of kindness and gentleness. At 7 years of age I told him I wanted to be a doctor and that I wanted to be just like him. He smiled, then gave me a letter opener from his desk to save for the day when I would become a doctor. He told me to “always care and respect your patients.” I was in awe. That letter opener from Dr. Thomas sits on my desk to this very day.
Today, when people ask me what I do, I tell them I am a teacher. It is my vocation. Teaching is a way of life, a calling. I still do physical diagnosis rounds with students, and I serve as
their mentor. The cornerstone of medicine must always be the doctor-patient relationship. At the bedside is where this profes-sional relationship is forged. At the bedside is where medicine is truly taught. At the bedside is where the skills of a Jefferson physician must always be developed. My door is always open to our students, just as it will always be open to alumni.
I look forward with great hope and enthusiasm to working with our president, Dr. Klasko, and with our dean, Dr. Tykocinski. I firmly believe that a new and better day is dawning for our alumni association. I want you to have faith in that promise. Across the United States in small towns and in large cities, with our graduates serving in institutions from academic medical centers to the Armed Forces, you are reading this article. I want each and every one of you to know that I need your faith, your resolve, your support, your help to make our alumni association rise again and become the best it can be. I give you my solemn pledge that I will do all I can to perpetuate the ideals of our Jefferson heritage and to make our alumni association the best it has ever been. I hope to meet as many alumni as I can and to reunite with many of my former students and residents. This is our medical school, our institution, our family, our Jefferson.
Joseph F. Majdan, MD, CV '81 [email protected] 215-503-4226
To read more about Majdan, please visit: Advancement.Jefferson.edu/physicaldiagnosis
Dear fellow alumni,Many thanks for entrusting me with the position of president of our association for the past two years. It was an honor and a pleasure to serve in this role and to begin new traditions including “Jeff at the Beach” and the annual alumnae brunch, and equally rewarding to revive former traditions such as the “Black and Blue Ball” and the dean’s dinner with alumni reunion class chairs.
Another success we can all be proud of is the return of the reproduction of “The Gross Clinic” to the Medical College; it will be hung at the top of the staircase where the original work resided for
so many decades. When returned to its rightful home, “The Clinic” will serve as the heart of the college and will be a reminder of all Jefferson physicians’ goal of healing with compassion.
With joyful anticipation, i pass the baton to our new president, Joseph Majdan, MD, CV ’81. i know i speak for all alumni in pledging our faithful support and genuine good wishes. Congratulations, Joe!
— Marianne T. Ritchie, MD '80

SummeR 2014 21
Photo by Ed Cunicelli

22 Sidney Kimmel medicAl college Alumni Bulletin
the members of Jefferson’s physician liaison team serve as a direct line of communication between Jefferson and
the broader physician community, helping physicians across the region navigate the referral process and facilitating interactions between referring physicians and Jefferson specialists in cardiovascular medicine, gastroenterology, oncology and neurology/neurosurgery.
Our liaisons strive to ensure the referral process goes as smoothly as possible. They welcome inquiries from you and your staff to help you maintain a meaningful relationship with Jefferson while connecting your patients with the best care available. Call or email them at any time.
Simon gratz Prize– Call for NominationsEvery three years, the Simon Gratz Prize is awarded to
two medical college alumni whose work has furthered the
advancement of medical or surgical treatment of disease
or for research work that has been of practical value. The
work must have been completed within the past five years.
The two alumni, one of whom must also be a current
faculty member, will each receive a cash prize of $10,000.
Postgraduate alumni are not eligible.
How to Apply
Email the following material to [email protected]:
1. Contact information, including your name, title, class
year, affiliation, mailing address, daytime phone and
email address.
2. An up-to-date copy of your curriculum vitae.
3. A one-page summary of your research within the past
five years.
4. Copies (PDFs) or links to any relevant publications.
In addition, two letters of reference (from colleagues in
your field describing your contributions to research within
the past five years) should be sent directly to the committee
Selection Procedure
Recipients will be chosen by the selection committee,
whose decision will be final. The award recipients will be
announced in spring 2015.
Deadline
Applications and supporting documents must be received
no later than Wednesday, Dec. 31, 2014.
Questions may be addressed to Karen Novielli, MD ‘87, vice
dean, faculty affairs, at 215-955-2361 or via email at
People
ellen doubet Service area: South Jersey [email protected] 215-200-9193
laurie geositsService areas: Center City Philadelphia; South Philadelphia; Main Line, Pa.; Delaware County, Pa.; Chester County, Pa.; Lehigh Valley, Pa.; Montgomery County, Pa. (northwest of Norristown); Scranton, Pa.; State of Delaware laurie.geosits@ jefferson.edu 215-200-9458
Vicki JonesService areas: Northeast Philadelphia; Bucks County, Pa.; Mercer County, N.J. victoria.jones@ jefferson.edu 215-200-4889
• Mark L. Tykocinski, MD, SKMC dean, has been named Provost and Executive Vice President
for Academic Affairs, Thomas Jefferson University.
• david McQuaid, President and CEO, Thomas Jefferson University Hospitals, has been named
Executive Vice President for Clinical Affairs, Jefferson Health System.
• Salvatore Mangione, MD, director of Jefferson’s physical diagnosis course, has won the
2013 Vesalius Prize for his brief, “Leonardo and the Reinvention of Anatomy.”
Referring a Patient to Jefferson? Meet Our Physician Liaison Team

SummeR 2014 23
ClassNotes’61 Joseph J. Cirotti has been designated emeritus chairman of the department of Pediatrics at Abington memorial Hospital. cirotti served as chairman of the department from 1988 to 2002. He lives in Ambler, Pa.
’64Leroy S. Clark writes that “after doing radiology for almost 50 years, it was time to put away the fluoroscopy equipment and retire.” clark has seven grandchildren “who need yelling at their ballgames and help with their homework.” He lives in tarzana, calif., and hopes to attend his 50th Jefferson reunion in october.
’67Allan M. Arbeter retired from clinical medicine in June 2012 as former chair of pediatrics at Albert einstein medical center in Philadelphia. He now teaches microbiology to second-year students at SKmc and to pediatric residents, students and faculty at einstein. He also studies piano and art. He and his wife, tammy, live in Philadelphia and have 11 grandchildren.
’70Arnold J. Willis has been named dean of clinical studies at Aureus university School of medicine in Aruba. Willis is still practicing urology in the Washington, d.c., area and is medical director for greenbelt urology institute. in addition to presenting papers related to epigenetic changes in prostate cancer nationally and internationally, including in Paris and Prague, he has continued to teach about minimally invasive prostate
cancer treatments in the Scandinavian countries.
’71 Edward B. Ruby is an assistant professor of medicine in the division of endocrinology at SKmc and was selected to receive a dean’s Award for excellence in education in may 2014. Ruby also received a lifetime Achievement Award from mercy catholic medical center, where he has served as chief of endocrinology, in June. He lives in Fort Washington, Pa.
’72Arthur A. Kunkle retired after 37 years of practicing pediatrics in Roanoke, Va., and writes that “it’s great having weekends and holidays off and enjoying our six grandchildren. my wife and i are enjoying travel and using the lake house.”
’74Burton H. Danoff lives in Weston, Fla., and is proud to report that his daughter, madison Paige, is beginning her first year at duke university’s Pratt School of engineering, where she will study biomedical engineering.
David and Stephen Karasick will celebrate their 40th class reunion this fall. they have been on the radiology staff at Jefferson since 1980. david’s two sons are both medical students at Jefferson. Andrew is a fourth-year student and will receive his md and mBA next year; michael is a first-year student.
John P. Lubicky is still in full-time academic practice of pediatric orthopaedic and spine surgery at West Virginia university. After being the only pediatric orthopaedic
surgeon in the state for nearly five years, he will be getting a partner in September. lubicky lvies in morgantown, W.Va.
’77 Robert S. Boova is a professor of surgery at temple university School of medicine and chief of cardiovascular surgery at Jeanes Hospital. He previously was associate professor of surgery at case Western Reserve university School of medicine and a member of the division of cardiac Surgery, Harrington Heart and Vascular institute, university Hospitals, case medical center, in cleveland.
’78Harold J. Davis is an associate clinical professor of obstetrics and gynecology at the commonwealth medical college and is serving as regional coordinator of ob/gyn services. davis also is director of gynecology at moses taylor Hospital in Scranton, Pa. He lives in clarks green, Pa.
’79Harry A. Hamburger has been appointed an adjunct clinical professor by the interAmerican university of Puerto Rico. He has also been asked to be on the advisory board of doctors Rx/Allergy testing inc. and was recently chosen as a Special master ime examiner by the state of Florida. He recently published a book of illustrated chassidic poetry, “i See only light.” Hamburger lives in Pinecrest, Fla.
Sandra Willingmyre was recently widowed. She continues to practice in tucson, Ariz.
’49Stanley F. Nabity received the 2013 saint Francis Medical center Physician lifetime Achievement Award in recognition of his “exemplary qualities, contributions to health care in grand island, neb., and to the community and medical staff of Saint Francis Medical center.”
’54Warren W. Brubaker retired in 1992 after 21 years as corporate medical director for the Hershey Foods corp. He previously did solo general practice in Annville, Pa., from 1955 to 1971. Brubaker and his wife, mary, live in Hershey, Pa., and have two children and three grandchildren.
’59Murray Feingold continues to practice medicine after 55 years and recently was appointed clinical professor of pediatrics at Harvard medical school. Feingold lives in Bourne, mass.
Claude J. Miller and his wife, Jean (a Jefferson medical technician graduate), live in cleona, Pa., but spend winters in Ft. Lauderdale, Fla., where they enjoy playing bridge, singing in a church choir and attending functions at the local performing arts center. miller says he is happy to see a fellow Ft. Lauderdale resident and Jefferson alumnus, Robert Catanzaro, MD ’72, even though their specialties are very different. catanzaro is an orthopaedist, while miller retired from practicing dermatology 15 years ago.

24 Sidney Kimmel medicAl college Alumni Bulletin
’80Mark D. Chilton has stopped taking eR calls and performing spine surgery after 28 years but continues to practice general orthopaedics and act as an examiner for the American Board of orthopaedic Surgery. He lives in Frederick, Md.
’81David M. Mannino was recognized by the American thoracic Society and expertscape as the top expert in the united States for chronic obstructive pulmonary disease (coPd) in december 2013. He lives in lexington, Ky.
Richard F. Spaide, an ophthalmologist with Vitreous-Retina-macula consultants
of new york, has co-authored numerous books about issues related to myopia, macular degeneration and retinal imaging. An updated edition of his book “Age-Related macular degeneration” was published in 2012, and a new book, “Pathologic myopia,” was published this year. this September, he will travel to Paris to receive the gabriel coscas Prize for excellence in research of the retina, and last year he received the Paul Henkind Award from the macula Society. in 2012, the Retina Society presented him with its Award of merit, the specialty’s biggest honor, which comes with a $50,000 prize. Spaide frequently presents named lectures in ophthalmology and recently had a patent issued for widefield mapping of the retina.
’84John W. Spurlock continues to enjoy solo private practice in Bethlehem, Pa., and writes that he was pleased to pass his board certification in the first group to sit for the boards in female medicine and pelvic reconstructive surgery (formerly known as urogynecology). spurlock and his wife, lisa, recently
welcomed their first grandson, John.
’87Gregory C. Kane, interim director of the department of medicine and the Jane and leonard Korman Professor of Pulmonary medicine at Jefferson, began a four-year term as governor of the Pennsylvania Southern chapter of the American college of Physicians, the national organization of internists, in April 2014. Working with a local council, Kane will help supervise AcP chapter activities, appoint members to local committees and preside at regional meetings. He lives in devon, Pa.
Steven A. Maser, an orthopaedic hand surgeon, was elected by his peers as president of the medical staff of morristown medical center in morristown, n.J. He began his term as president on Jan. 1, 2014. maser lives in livingston, n.J.
’89Robert A. Kitei partnering with his daughters, invented and marketed Supercleat, a patent-pending product that repels mud from adhering to sports cleats. Supercleat
has been sold to mission Athletecare, a global sporting goods brand that re-launched the product as cleat grip and sells it to retailers worldwide. Kitei lives in doylestown, Pa.
Raj K. Sinha is president of S.t.A.R. othopaedics and founder of Joint Replacement Hospitals of America, inc. His son Abhi is an actor on the ABc Family television show “chasing life,” and he has two other children, Ava and Sid. Sinha lives in Palm desert, calif.
’91Pamela Tecce Johnson has been appointed radiology residency program director and promoted to associate professor at Johns Hopkins Hospital. She lives in Baltimore.
’04Jonathan M. Fenkel edited a book, “Quick Reference dictionary for gi and Hepatology,” which was released in April 2014. Fenkel lives in Bryn mawr, Pa.
Michael Pucci has been appointed assistant professor in the department of Surgery at Jefferson. He lives in Huntingdon Valley, Pa.
Philadelphia County Medical Society Recognizes AlumniOn June 14, 2014, the Philadelphia County Medical Society installed Anthony M. Padula, MD ’67, as its 153rd president. Padula, who completed both his residency and internship at Jefferson, was a faculty member from 1975 to 1995, and his sons Anthony (MD ’98) and Michael (MD ’00), are both alumni.
At the event marking Padula’s installation, the Society also presented awards to three members of the SKMC community in recognition of their 50 years of medical service: alumni Robert W. Kalish, MD ’64, and Edward C. Leonard, MD ’64, as well as emeritus chairman of the Department of Radiology David C. Levin, MD. in addition, Harris R. Clearfield, MD ’59, past president of the Society, received the Cristol Award, which is given to a member who “has shown great leadership and unselfish dedication in furthering and enhancing the educational, scientific and charitable goals, purposes and functions of organized medicine.”
Send us your personal and professional updates for the Bulletin’s Class Notes!
Contact the Office of Institutional Advancement at 215-955-7751 or [email protected].
Mail to: Office of Institutional Advancement 125 S. 9th Street, Suite 700 Philadelphia, PA 19107
What’s New?

SummeR 2014 25
In Memoriamgames of ice hockey with his children and their friends. He especially enjoyed time at his family cottage in dick’s dam, Pa., and summers at the Jersey shore. Jordan is survived by his wife of 62 years, lauretta; two sons, Herb iii and Bob; two daughters, laurie and Jan; six grandchildren; and five great-grandchildren.
Leon Levintow, 92, died march 11, 2014, at home in Kentfield, calif. levintow was professor emeritus of microbiology and immunology at the university of california, san Francisco, and served as chairman of the department from 1978 until his retirement in 1993. After graduating from Jefferson, he served in the u.S. Army medical corps, stationed in germany. He served his residency at massachusetts general Hospital in Boston but found he preferred scientific research to medical practice. He joined the u.S. Public Health Service and worked at the national institutes of Health in Bethesda, md., researching the biochemistry of animal cells and studying the viruses that attack them. He was invited to join the ucsF faculty in 1965.
in addition to his research, levintow had an exceptional ability to recognize, recruit and nurture top-level scientific talent. during his tenure, the microbiology and immunology department — previously considered a remote outpost — became a world-renowned center for cell research. in 1989, his colleagues J. michael Bishop, whom he had personally recruited and
mentored both at niH and ucsF, and Harold Varmus were awarded nobel Prizes in Medicine, the first ucsF scientists ever to receive that honor.
He is survived by his wife of 54 years, Regina; his brother david; three sons, michael, Stephen and daniel; and three grandchildren. Another son, Robert Paul, predeceased him. James V. Mackell, 94, of Stone Harbor, n.J., died may 3, 2014. mackell, former chairman of the pediatrics department at Holy Redeemer Hospital in meadowbrook, Pa., was class agent for the Jmc class of 1946 for more than 60 years. He served in the military at an Army hospital in Heidelberg, germany, and was appointed to the medical staff at Holy Redeemer in 1958. in the 1960s, he was president of the medical staff there and a founding member of its pediatrics department, of which he was chairman for 26 years. From the 1960s into the 1980s, he was a clinical associate professor of pediatrics at Jefferson. He also maintained a private practice until retiring in 1989.
mackell ran about three miles on the beach every day, even in his 90s. At St. Paul church in Stone Harbor, he was a trustee and president of the parish council. A trustee of the Stone Harbor Property owners Association, he also was a member of the American legion.
mackell is survived by his wife of 72 years, Rosemary; two sons, thomas and James V. Jr.; four daughters, Rosemary, Sally, margaret and Jane; 31 grandchildren; five step-grandchildren; and two great-grandchildren.
’48 Edwin Gordy, 88, died nov. 20, 2013, in newtonville, mass. Born and raised in Philadelphia, gordy earned his undergraduate degree from Harvard university and dSc degree from the university of Pennsylvania. He spent two years in the u.S. Army as a researcher at Walter Reed Army Hospital, after which he set up the medical instrumentation section of Roswell Park cancer center in Buffalo, n.y. He worked as a researcher at the Worcester institute and the American electronics institute in the Boston area. He spent much of his life working in medical instruments, but also had a medical practice in newtonville, mass. gordy is survived by his wife, mary; sons Roger and matthew; daughter, Alison; and sister, charlotte glauser.
John Edwin Weyher, Jr., 89, died march 5, 2014, in Wilmington, n.c. After completing his internship at Jefferson davis Hospital in Houston, Weyher served two years in the u.S. navy. He completed a residency in urology at Kennedy Veterans Administration Hospital in memphis, tenn. He was certified by the American Board of urology and was a member of the American urological Association and the north carolina medical Society. He practiced urology in goldsboro, n.c., for 28 years, was a member of the Wayne county medical Society and was on the staff at Wayne memorial Hospital. Following his retirement in 1985, he moved to topsail Beach, n.c., and later moved
’45 Benson Krieger, of Philadelphia, died may 16, 2014. He is survived by his wife, natalie; two children, myles and Anna; four grandchildren, Arthur, eric, nano and Ziggy; and four great-grandchildren, Wyatt, nati, yanni and Aubrey.
’46 Herbert V. Jordan, Jr., 92, of mechanicsburg, Pa., died Feb. 12, 2014. Jordan attended Jefferson under the Army Specialized training Program. After completing his internship at Harrisburg general Hospital in 1947, he served two years as a captain in the u.S. Army Medical corps at Fort mcKinley, manila, Philippine islands. He then returned to Harrisburg Hospital and completed residencies in surgery and ob/gyn. He held academic appointments at several institutions including Hahnemann Hospital, the Harrisburg Hospital School of nursing and the medical college of Penn State university in Hershey, Pa. He was a past president of Harrisburg Hospital medical staff and the central PA Academy of medicine and past chairman of obstetrics and gynecology at Harrisburg Hospital. He practiced for many years with Jordan, mccall and Associates and was later a consulting physician at e.g. Frederick Health center in millersburg, Pa. He was a member of the American medical Association and American college of obstetrics and gynecology. Jordan enjoyed traveling, skiing, tennis and

26 Sidney Kimmel medicAl college Alumni Bulletin
to Wilmington in 2000. Weyher is survived by his wife of 62 years, Patsy; two daughters, Karen and melissa; four grandchildren, John, matthew, Joseph and grace; a sister, Rachel; and many nieces and nephews. in addition to his parents, he was preceded in death by his son, John, and a sister, louise.
’49 Thomas C. Piekenbrock, 90, of dubuque, iowa, died march 15, 2014. in 1956, after serving as a flight surgeon for three years, he joined his uncle in practicing psychiatry in dubuque, where he was a leader in the mental healthcare community for over 60 years. He served as chief of staff at mercy medical center and was a leader in developing the gannon center for community mental Health. He continued to care for mental health patients until his retirement at the age of 89. His service was recognized by many accolades including the American Psychiatric Association 50-year distinguished life member medallion; he was the 105th physician to achieve this award out of more than 34,000 members. He also received the nancy Hill Award from Hillcrest Family services in recognition of special services to the organization.
He is survived by his wife, Pat; five children, Barbara, ellen, charles, Roger and Kara; 10 grandchildren, martha, eric, Patrick, Kalie, Jack, natalie, Audrey, olivia, ellie and Susie; two great-grandchildren, madie and morgan; 12 stepchildren, lenda, michael, mark, Beth, mary Jo, Sara, Ann, eric, Amy,
ellen, Kathleen and Andy; and many nieces and nephews.
He was preceded in death by his wife Peggy, his wife imelda; and his brothers Jack and Bob.
’50 Murray A. Kessler, 86, died Jan. 26, 2014, in lakewood, n.J. Kessler surmounted a great physical handicap to become a physician; at age 7, he had a stroke that left him partially paralyzed on one side. Following his internship and residency, he became a pediatrician and practiced full time in long Branch and Freehold, n.J. While maintaining his practice, he continued his education in allergy and immunology, the field in which he eventually practiced exclusively. He was a diplomat of the American Academy of Pediatrics and the American Academy of Allergy and immunology. upon retiring, he enjoyed gardening and playing bridge, ultimately achieving the rank of life master.
Kessler is survived by his wife of 62 years, Phyllis; three children, Joel, connie and Dan, MD ’86; and six grandchildren.
’52 Albert Lethiecq Babcock, of duxbury, mass., died April 23, 2014. Babcock worked in the greater Hartford area as a plastic surgeon for 45 years and used his expertise to help people in need internationally. in 1975, his first volunteer assignment was on the hospital ship HoPe in tunisia, and his greatest personal satisfaction came from his many volunteer trips to
Brazil through the esperanza Project. He also relished his many ties to his home state of maine and enjoyed time outdoors on mt. desert island and the wilderness areas of Baxter State Park. Babcock is survived by his companion, Antonia colby Shoham; five children, linda, Jonathan, david, daniel and Janna; six grandchildren david Jr., ted, Kelly, Abigail, Jacob and grace; a great-grandson, Jameson; four nieces and nephews, Brit, ted, Hannah and christopher; a sister, Jane; and a step-daughter, Susan.
’53 Earl W. “Doc” Wharton, 88, of charlo, mont., died march 11, 2014. Before pursuing his medical degree, Wharton was an engineering officer for the u.S. navy; he was honorably discharged in September 1946. After graduating from Jefferson, Wharton completed his training in internal medicine at Akron city Hospital in ohio. He opened a private practice, which he maintained for 35 years.
Wharton published two books: “Why Weight,” a book on obesity, and “the Sword and the Scalpel,” about life as a surgeon during the civil War. one of his proudest moments was his induction into the Summit county Professional Boxing Hall of Fame; he was the physician for the golden gloves as well as for professional boxing in Akron and cleveland for more than 30 years and became acquainted with some of the great fighters of the 20th century: muhammad Ali, Joe Frazier, ernie shavers, george Foreman,
larry Holmes and Joe “the Brown Bomber” louis. in his retirement, Wharton built or renovated two homesteads in ohio and montana. He was an accomplished artist and painter.
Wharton is survived by his wife of 47 years, Betty; two daughters, Ruth Ann and carol; a son, Steven; four grandchildren, Vanessa, Josh, laura and monica; and a sister, Ann. He was preceded in death by a son, Joseph.
Harold R. Weidaw, 87, died march 12, 2013, in Pinehurst, n.c. Weidaw served in the u.S. Army from 1944 to 1947. He started his first practice in Pennsylvania in general medicine and worked there for about 10 years. He then opened an allergy practice in Pinehurst in 1985 and worked there until he was 80 years old, when he suffered a stroke and had to retire. He is survived by his wife, Betty; a son, James; a grandson; and a great-grandson.
’56 Philip S. Green, 82, of San Jose, calif., died may 15, 2013. green completed an ob/gyn residency at martland medical center in newark, n.J., and practiced for 35 years in Scotch Plains and Somerville, n.J., after serving two years in the u.s. Air Force. He was an associate professor at the Robert Wood Johnson medical School and retired to San Jose, to be near family. He is survived by his wife of 59 years, Roma; two daughters, lisa and Sara; and two granddaughters, Amanda and Alexandra.
continued on page 28

SummeR 2014 27
John M. Fenlin, MD ’63
John Major Fenlin, MD ’63, longtime Jefferson faculty member, died May 11, 2014.
Fenlin completed his internship and surgical residency at Jefferson and stayed on campus throughout his entire 46-year career as an orthopaedic surgeon. He devoted the last 25 years of his practice to shoulder surgery and earned the nickname “Dr. Shoulder” across the Philadelphia medical community. He started Jefferson’s shoulder and elbow service, which under his leadership gained international recognition.
A recipient of the prestigious Charles S. Neer Award for clinical research, he published 37 peer-reviewed articles on shoulder surgery, served as president of the American Shoulder and Elbow Surgeons and designed the first reverse shoulder replacement for glenohumeral arthritis, forever changing the way shoulder replacement surgery is performed. With humor and humility, he always focused on giving his patients the best surgical outcomes possible.
Earlier this year, Fenlin’s colleagues at the Rothman Institute recognized his influence and accomplishments by establishing a new professorship fund in his name, and Gerald R. Williams, Jr., MD, was invested as the first John M. Fenlin, Jr., MD, Professor of Shoulder and Elbow Surgery in June.
“John Fenlin is synonymous with Jefferson in general and shoulder surgery in particular. He left his imprint on all of us on the shoulder and elbow service, and I am honored and humbled to be the recipient of his endowed chair,” Williams said.
Fenlin is survived by his wife, Naomi; 10 children; and nine grandchildren. Donations in his name may be made to the John M. Fenlin, Jr., MD, Professorship in Shoulder and Elbow Surgery, Jefferson Office of Institutional Advancement, Suite 700, 125 S. 9th St., Philadelphia, PA 19107 or online at Advancement.Jefferson.edu/fenlin.
Jefferson Community Mourns Two Longtime Orthopaedic Leaders
Jerome M. Cotler, MD ’52
Jerome M. “Jerry” Cotler, MD ’52, 85, director of orthopaedic surgery at Jefferson from 1986 to 1995, died April 10, 2014.
After completing his surgical and orthopaedic residencies at Jefferson, Cotler stayed on as an instructor and associate orthopaedic surgeon. He later became director of orthopaedic surgery and the orthopaedic residency program and was named the Dr. Everett J. and Marian Gordon Professor of Orthopaedic Surgery.
For more than a decade, Cotler shared an office with Phillip Marone, MD ’57, former orthopaedic surgeon and associate dean of alumni affairs at JMC. Marone recalls him as “a great guy, the nicest man you’ll ever find.”
Cotler also was affiliated with numerous facilities in South Jersey and Southeastern Pennsylvania, including Bridgeton Hospital, Salem County Memorial Hospital, Elmer Community Hospital, Magee Rehabilitation Hospital and Elizabethtown Hospital for Crippled Children and Youth, where he was president of the medical staff from 1971 to 1975.
Cotler served as president of the American Board of Orthopaedic Surgery and vice president of the American Orthopaedic Association. He co-authored numerous clinical research papers and orthopaedic textbooks and lectured throughout the world at scientific conferences. His many honors and awards included the American Spinal Injury Association’s Lifetime Achievement Award; Ursinus College’s Alumni Award; the Jewish National Fund’s Man of the Year; the Lindback Award for Distinguished Teaching; the Garland Award for Excellence in Resident Education; and the Sir John Charnley Award from the Arthritis Foundation of Eastern Pennsylvania.
Cotler is survived by his wife of 62 years, Florence; two children, Howard, MD ’79, and Michele; four grandchildren, Mitchell, Amanda, Laura and Elizabeth; and a great-grandson, Jacob. Donations in his name may be made to the Parkinson’s and Movement Disorders Program, Jefferson Office of institutional Advancement, Suite 700, 125 S. 9th St., Philadelphia, PA 19107 or online at Advancement.Jefferson.edu/movementdisorders.

SummeR 2014 28
’59 Alan H. Weigand, 79, of Jupiter, Fla., died June 26, 2013. After graduating from Jefferson, he attended law school at temple university. He later completed a residency in rehabilitation medicine at Albert einstein college of medicine in new york. He and his wife, tina, shared a successful private practice in Ho-Ho-Kus and Ridgewood, n.J.
Weigand became head of rehabilitation medicine at the university of medicine and dentistry of new Jersey and was nationally recognized as the “Best electromyographer on the east coast.” He trained residents to detect and treat neuromuscular diseases. He also served as director of rehabilitation and physical medicine at the VA Hospital in east orange, n.J., for 20 years. Weigand was an accomplished musician who wrote music and played the piano, violin and accordion. His greatest love, though, was the Hammond organ; whenever he played, his italian greyhound Pinot grigio, the “canine tenor,” would accompany him loudly.
in addition to his wife, Weigand is survived by his
daughters, Kathryn and Angela; and his granddaughters, emily, Reagan and Aine.
’63 Charles Markosi, Jr., 76, of Hamburg, Pa., died April 25, 2014. markosi served his internship at Fitzgerald Mercy Hospital in darby, Pa., and later worked in the emergency room at Allentown general Hospital. He was a u.S. navy veteran of the Vietnam War. While serving in the military, he was a physician at chelsea naval Hospital in Boston. markosi was in private practice at tannersville Family Practice for 25 years, later working for the penal system in Pennsylvania and then for Wernersville State Hospital. He was a member of the American medical Association and a life member of cambridge Who’s Who; in 2011, he received the Professional of the year Award in Family Medicine from cambridge Who’s Who. He also was inducted into elite American Physicians in February 2013. He was a member of St. mary Roman catholic church and loved to
continued from page 26
fish and work in his garden.markosi is survived by
his wife of 51 years, irene; one son, charles iii; three daughters, lauren, tanya and mary; and six grandchildren, tara, Stefanie, charles iV, Anastasia, c.J. and damon. He was predeceased by a sister, lorraine.
’69 Philip Henry Geetter, 68, of Pipersville, Pa., died Aug. 12, 2012. geetter completed his internship at mercy Hospital and medical center in San diego, later returning to Jefferson for his ophthalmological residency. in 1974, he founded Bucks mont eye Associates in Sellersville, Pa. He was active on the medical staff of grand View Hospital, St. luke’s Quakertown Hospital and Wills eye Hospital. Board certified in ophthalmology, he was a fellow of the American and the Pennsylvania Academy of ophthalmology and the American implant Society. He was past president of the grand View Hospital medical staff and the inter-county ophthalmic Society
as well as a member of the American Society of cataract and Refractive Surgery and an honorary member of the Wills eye Society.
geetter shared his love of travel with his family, taking his children and grandchildren on special excursions every year. He loved spending time in his garden, fishing, chasing hurricanes and relaxing in his hammock. He is survived by his wife of 42 years, Helene; four children, erik, todd, chad and courtney; three grandchildren, Audrey, Zachary and troy; his father, nathan; a sister, diane; two nephews, david and Joshua; two grand-nieces, isadora and lillian; and two dogs, gracie and carly.
The names of Steven A. Katz, MD ’84,
and Jonathan S. Daitch, MD ’84,
were misspelled in the spring issue of
the Bulletin. The Bulletin regrets any
inconvenience this may have caused.
Mitochondrial Disease and the MitoCare Center at Jefferson
in January 2014, Jefferson launched the MitoCare Center for Mitochondrial Imaging Research and Diagnostics, a new research center focused on characterizing the role of mitochondrial dysfunction in disease. Housed in the Department of Pathology, Anatomy and Cell Biology, the Center employs cutting-edge technology and multidisciplinary researchers to examine how changes in mitochondrial biology can contribute to a wide range of diseases.
Mitochondria have an evolutionary history that derives from ancient organisms that adapted to permanent residence in eukaryotic cells, bringing more efficient energy management and the coordination of diverse cell functions including decision-making related to survival and death. When mitochondria break down, a cell and its related tissues lose much of their capacity to produce energy and fail to function efficiently.
Recent research suggests that malfunctioning mitochondria contribute to many common ailments in adults and older individuals including neurodegenerative diseases, metabolic diseases, heart disease and cancer.
MitoCare Center scientists are working closely with faculty from Wills Eye Hospital, the Kimmel Cancer Center, the Center for Translational Medicine, and the departments of neurology, neuroscience,
emergency medicine and biochemistry.
For facts about mitochondrial disease, see By the Numbers on the following page.
For more information about the MitoCare Center at Jefferson, contact Gyorgy Hajnoczky, MD, PhD, at [email protected].

SummeR 2014 29
*Figures from the United Mitochondrial Disease Foundation and MitoAction.
Mitochondrial DiseaseMitochondrial defects cause a range of degenerative diseases
often evident in children, although some patients are also
diagnosed as adults. More and more primary mitochondrial
diseases are being diagnosed as genetic screening improves and
basic research continues to uncover new gene functions. Here
are some facts about mitochondria and mitochondrial disease:
number of organ systems mito-
chondrial diseases typically affect:
At least 3
Incidence of primary mitochondrial
disease in the United States:
1 in every 3,000 to 4,000 individuals
existing effective mitochondrial
disease treatments: 0
(related symptoms, such as seizures
or attention problems, can be
managed with various medications,
but the mitochondrial disease itself
remains unchanged)
existing reliable and consistent
means of mitochondrial disease
diagnosis: 0
Percentage of cellular energy
generated by mitochondria.
number of people with a
mutation that could develop into
mitochondrial disease at some
point in their lifetime: 1 in 200M
Children born with a primary
mitochondrial disorder every year:
1,000 to 4,000
Children who will develop mito-
chondrial disease by age 10:
1 in 2,000
By tH
e numbers
numbers of mitochondria in a cell:
1 to 10,000, depending on
the type of cell.
90%

Non-Profit Org. US Postage
PAID Permit #276
Philadelphia, PA
125 S. 9th Street, Suite 700 Philadelphia, PA 19107
Change Service Requested
Printed on FSC (Forest Stewardship Council) certified paper, which supports the growth of responsible forest management
worldwide through its international standards.
What Every Healthcare Professional Should Know: A General Medical UpdateFebruary 1-5, 2015
The Four Seasons, Jackson HoleSpend a week with Jefferson faculty at the annual alumni winter CME symposium. Renowned experts from several specialties will present.
Featuring: Jefferson President Stephen Klasko, MD, MBA, and Provost Mark Tykocinski, MD, Anthony F. and Gertrude M. DePalma Dean, Sidney Kimmel Medical College at Thomas Jefferson University
Updates and Clinical Pearls in:• Cardiac and Vascular Disease• Geriatric Medicine • Complementary and
Alternative Medicine
• Treatment of Hepatitis C• and more!
Registration Fee:Beginning at $595 (see website for details) fee includes• All education sessions and CME credit• Welcome Superbowl reception (Feb. 1)• Breakfast and afternoon snacks (Feb. 2-5)• One dinner ticket (Feb. 4)*• Access to additional area discounts
See the full schedule of presenters and topics at: Jefferson.edu/jeffcme/AlumniCME Register Online Now!
Questions? Contact the SKMC Office of CME at 1-888-JEFF-CME or [email protected]*Guests welcome at dinner with additional ticket purchase
New LoCATioNThe Four Seasons, Jackson Hole, wyomingRoom rates are $325 for a king bed or two double beds and $695 for a suite. To reserve a room, please call the Four Seasons directly and request the Reservations Department at 1-800-295-5281. Please note room rates will be honored for course registrants only.
Sidney Kimmel Medical College at Thomas Jefferson University is accredited by the ACCME to provide continuing medical education for physicians.