Embed Size (px)
Citation preview
New Directions in the Management of Chemotherapy-Induced Nausea and Vomiting
David S. Ettinger, MDAlex Grass Professor of Oncology
Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins
Disclosure of Conflicts of Interest
David S. Ettinger, MD, discloses that he has served as an advisor/consultant for Gilead, Roche/Genentech, Boehringer Ingelheim, Biodesix, Lilly, and Helsinn Therapeutics.
Learning Objectives
Describe the pathophysiology of chemotherapy-induced nausea and vomiting (CINV)
Assess the risk for nausea and vomiting in cancer patients scheduled to receive chemotherapy
Differentiate antiemetic strategies for delayed, breakthrough, and refractory nausea and vomiting
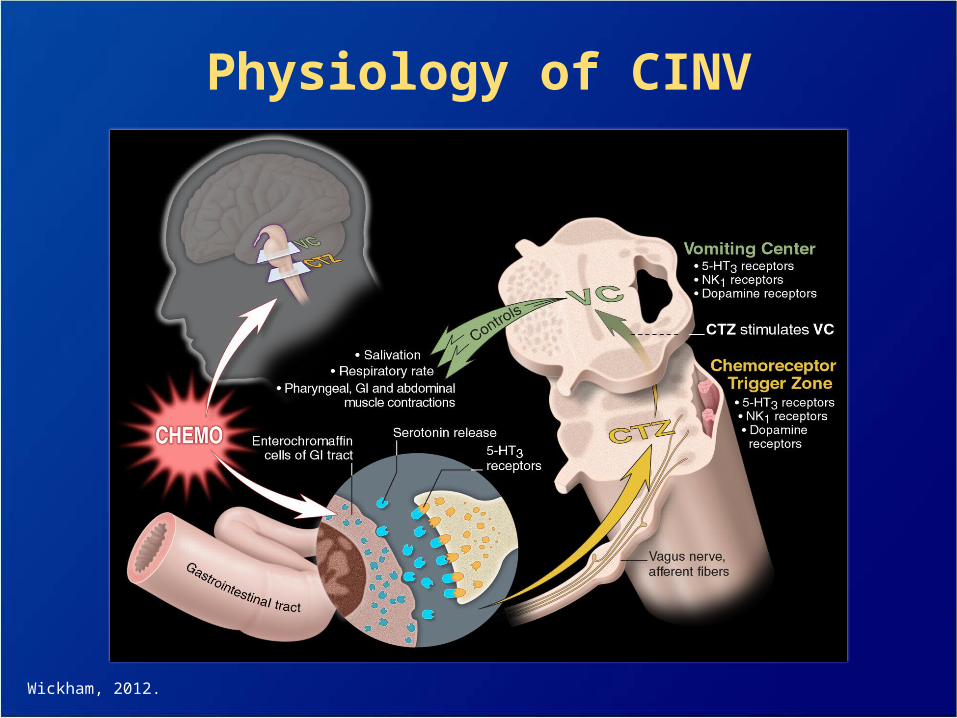
Physiology of CINV
Wickham, 2012.
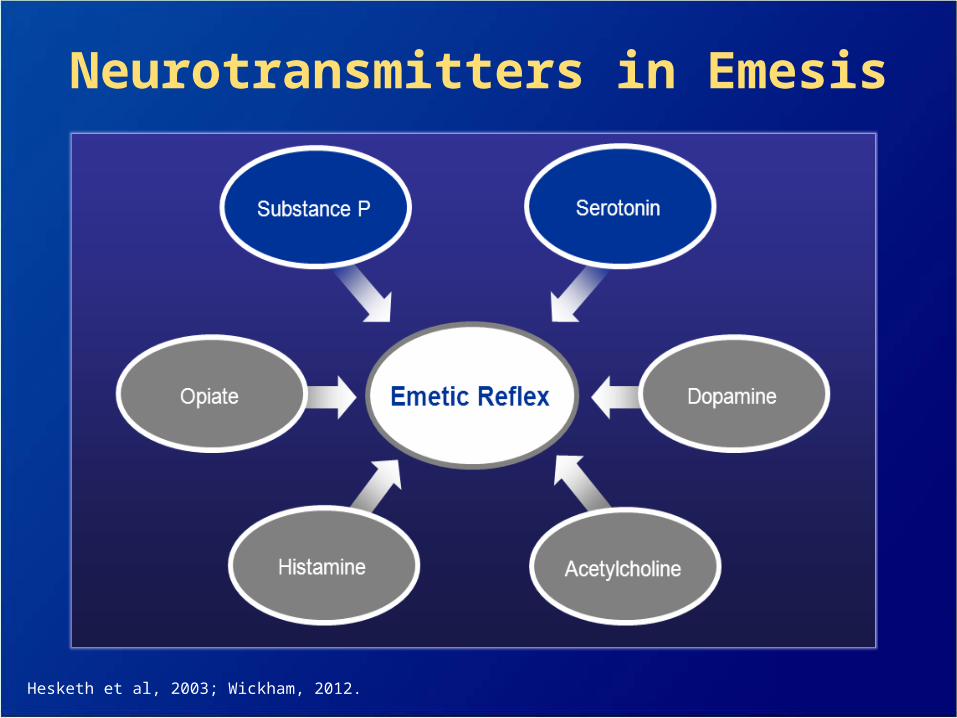
Neurotransmitters in Emesis
Hesketh et al, 2003; Wickham, 2012.
Serotonin and the 5-HT3 Receptor Pathway
Pathway first recognized with high-dose metoclopramide
Introduction of 5-hydroxytryptamine (5-HT3) receptor antagonists offered an improved treatment option– Effective in acute vomiting; variable efficacy for
delayed events
Primary mechanism of action appears to be peripheral
Miner & Sanger, 1986; Andrews et al, 1998; Hesketh et al, 2003; Wickham, 2012.
Substance P and the NK1 Receptor Pathway
Substance P relays noxious sensory information to the brain (ie, modulates nociception)
High density of substance P/neurokinin-1 (NK1) receptors located in brain regions is implicated in the emetic reflex
Primary mechanism of NK1 receptor blockade action appears to be central– Effective for both acute and delayed events
– Augments antiemetic activity of a 5-HT3 receptor antagonist and a corticosteroid
DeVane, 2001; Hargreaves, 2002; Hesketh et al, 2003; Hesketh, 2001; Tattersall et al, 1996; Wickham, 2012.
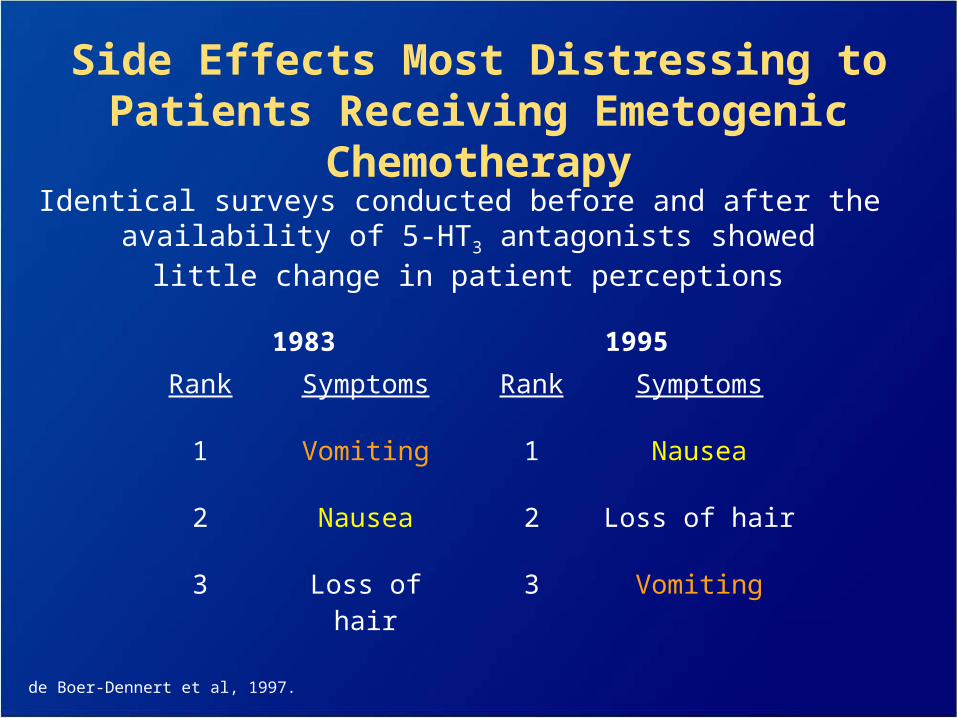
Identical surveys conducted before and after the availability of 5-HT3 antagonists showed
little change in patient perceptions
1983 1995
Rank Symptoms Rank Symptoms
1 Vomiting 1 Nausea
2 Nausea 2 Loss of hair
3 Loss of hair 3 Vomiting
Side Effects Most Distressing to Patients Receiving Emetogenic Chemotherapy
de Boer-Dennert et al, 1997.
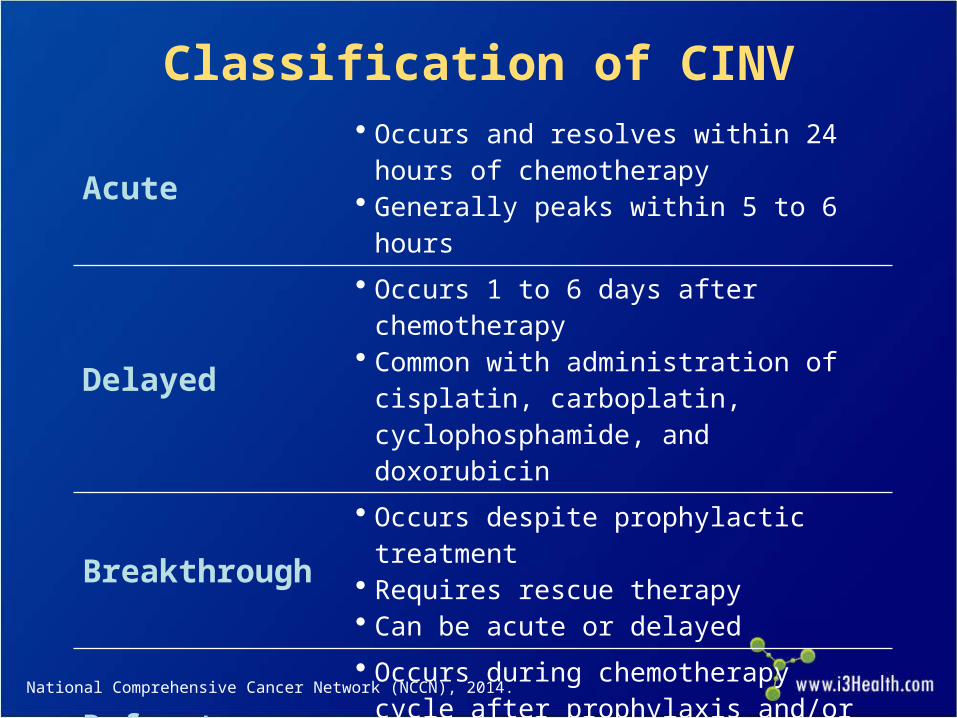
Acute• Occurs and resolves within 24 hours of
chemotherapy• Generally peaks within 5 to 6 hours
Delayed
• Occurs 1 to 6 days after chemotherapy• Common with administration of cisplatin,
carboplatin, cyclophosphamide, and doxorubicin
Breakthrough• Occurs despite prophylactic treatment• Requires rescue therapy• Can be acute or delayed
Refractory• Occurs during chemotherapy cycle after
prophylaxis and/or rescue therapy has failed in earlier cycles
Classification of CINV
National Comprehensive Cancer Network (NCCN), 2014.
Characterizing Nausea
Less understood at neurochemical level than vomiting
Results of direct treatment not as effective as treating vomiting
Impact of nausea on quality of life (QOL) often overlooked
Grunberg, 2012.
Characterizing Nausea (cont.)
Vomiting an objective event Nausea a subjective symptom Nausea commonly suffered in silence
(difficult to grade)
Grunberg, 2012.
Impact of Nausea on QOL
Nausea has more of a deleterious effect on QOL and sense of well-being than emesis
Patients rate severe nausea worse for QOL than vomiting with or without nausea
Börjeson et al, 2002; Bloechl-Daum et al, 2006; Sun et al, 2005; Grunberg, 2012.
The Importance of Treating Nausea
Nausea duration may result in even greater distress and altered QOL than severity of nausea
Reduction of nausea rather than emesis has been shown to guide patient preference in antiemetic treatment
Grunberg, 2012.
CINV Risk Factors
Treatment-related risk factors– High emetogenicity of chemotherapy drugs
– High drug dose
Patient-related risk factors– Younger age
– Female gender
– No/minimal history of alcohol use
– Susceptibility to motion sickness
– Poor control with prior chemotherapy
– AnxietyNCCN, 2014.
CINV Risk Factors (cont.)
Medical procedures such as surgery and radiation Medications such as digitalis derivatives, opioids,
nonsteroidal anti-inflammatory drugs (NSAIDs), and antibiotics
Uremia Hypercalcemia Hepatic dysfunction Increased intracranial pressure Gastrointestinal abnormalities: obstruction, ascites,
hepatomegaly, paraneoplastic syndrome, gastroparesis, gastric outlet syndrome
NCCN, 2014.
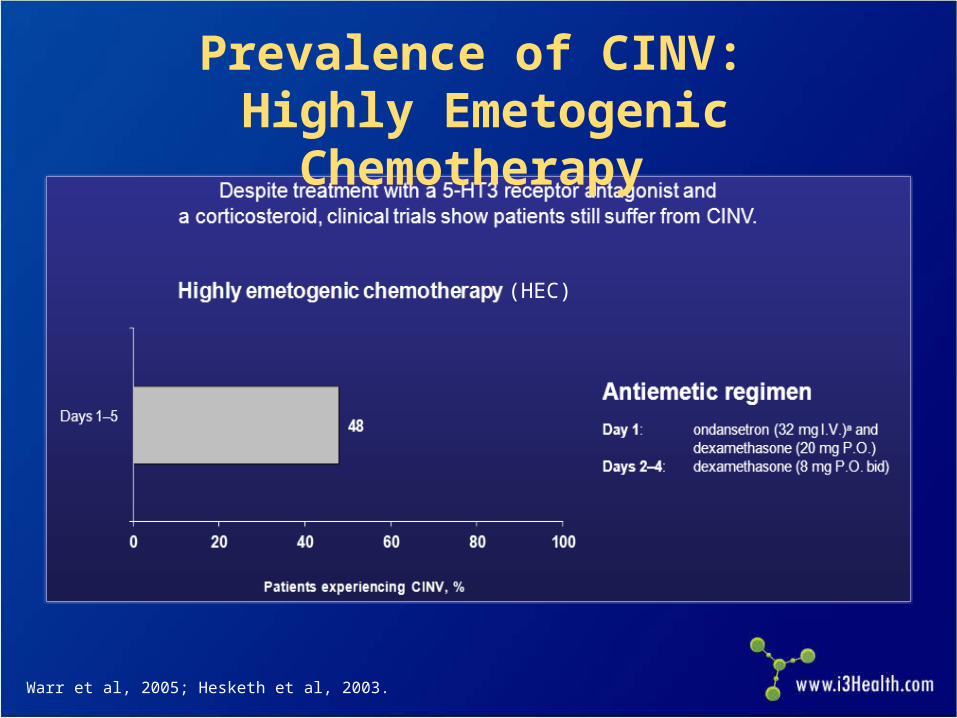
Prevalence of CINV: Highly Emetogenic Chemotherapy
Warr et al, 2005; Hesketh et al, 2003.
(HEC)
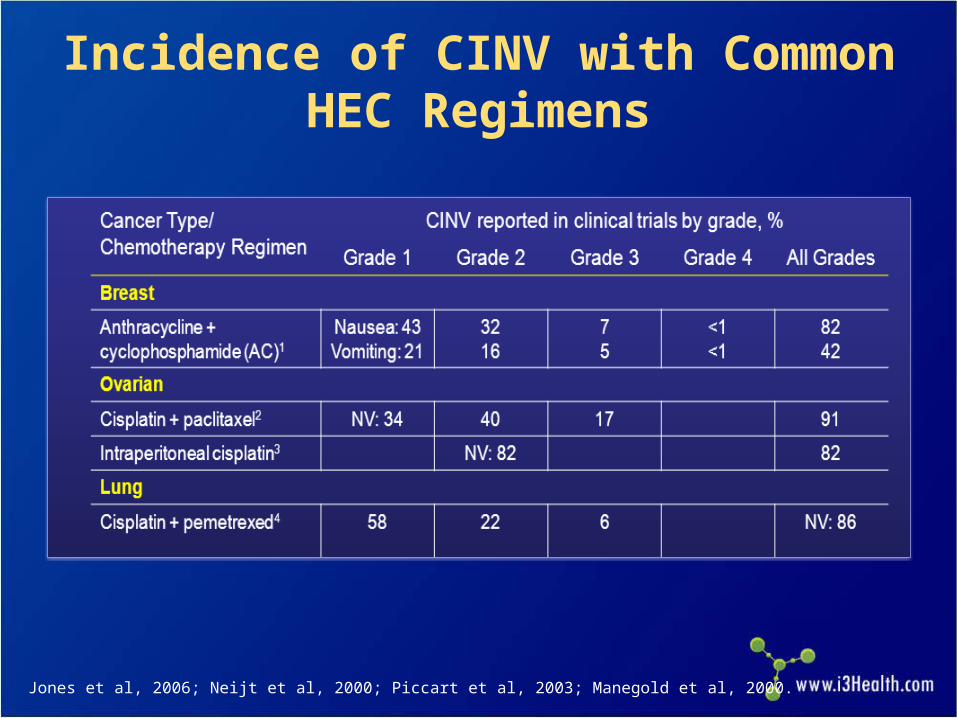
Incidence of CINV with Common HEC Regimens
Jones et al, 2006; Neijt et al, 2000; Piccart et al, 2003; Manegold et al, 2000.
CINV: Predictability and Preventability
CINV is a common, often predictable, and often preventable adverse reaction to chemotherapy
Consider using preventive measures for CINV with cycle 1 of chemotherapy
CINV negatively affects patients’ overall chemotherapy experience
Preventing CINV on first exposure to chemotherapy can reduce the risk for developing anticipatory CINV in subsequent cycles
Lau et al, 2004; Basch et al, 2011; Osoba, Zee, Warr, et al, 1997; Aapro et al, 2005; Fernández-Ortega et al, 2012.
Risk Factors for CINV: Chemotherapy-Specific
Use of emetogenic regimens such as:– AC (anthracycline + cyclophosphamide)
– Carboplatin-based regimens
– Cisplatin-based regimens
– Cyclophosphamide-based regimens
– FOLFOX/FOLFIRI (oxaliplatin + leucovorin + 5-fluorouracil/irinotecan + leucovorin + 5-fluorouracil)
– ABVD (doxorubicin + bleomycin + vinblastine + dacarbazine)
Short IV infusion time Repeated cycles of chemotherapy
NCCN, 2014a; Basch et al, 2011.
Cisplatin: Prototypical Highly Emetogenic Chemotherapy
Cisplatin is the cornerstone of therapy for many cancers
Risk of emesis is universal– Agent causes emesis in all patients (there is >99%
risk without antiemetics)
Well-characterized emetogenic profile serves as a model for antiemetic testing– Efficacy shown with cisplatin is predictive of
antiemetic efficacy with other chemotherapy drugs
Basch et al, 2011.
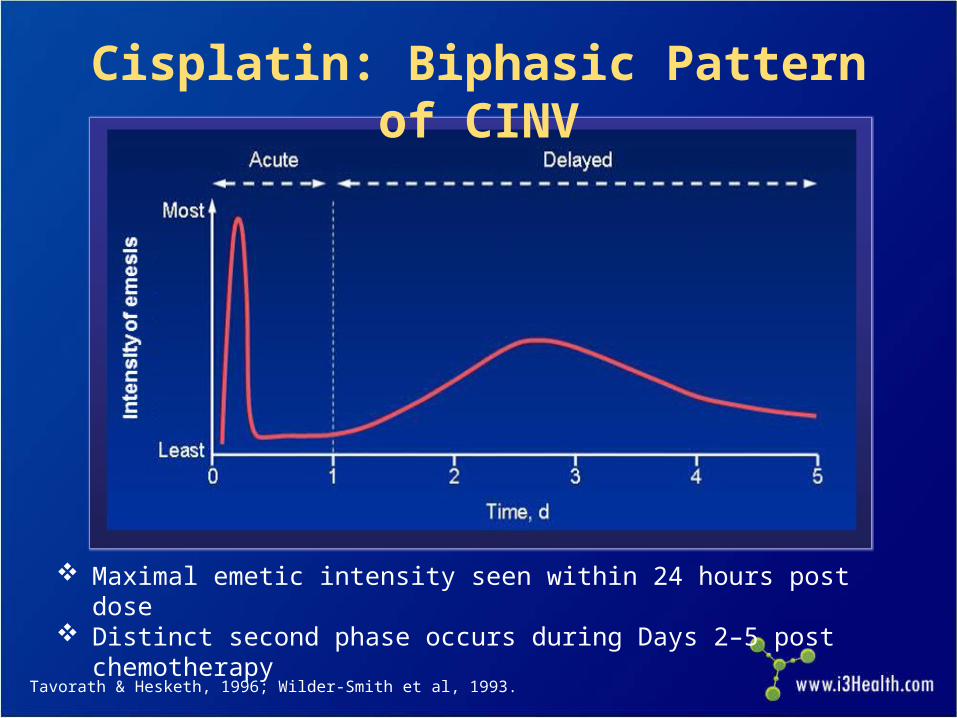
Maximal emetic intensity seen within 24 hours post dose Distinct second phase occurs during Days 2–5 post chemotherapy
Cisplatin: Biphasic Pattern of CINV
Tavorath & Hesketh, 1996; Wilder-Smith et al, 1993.
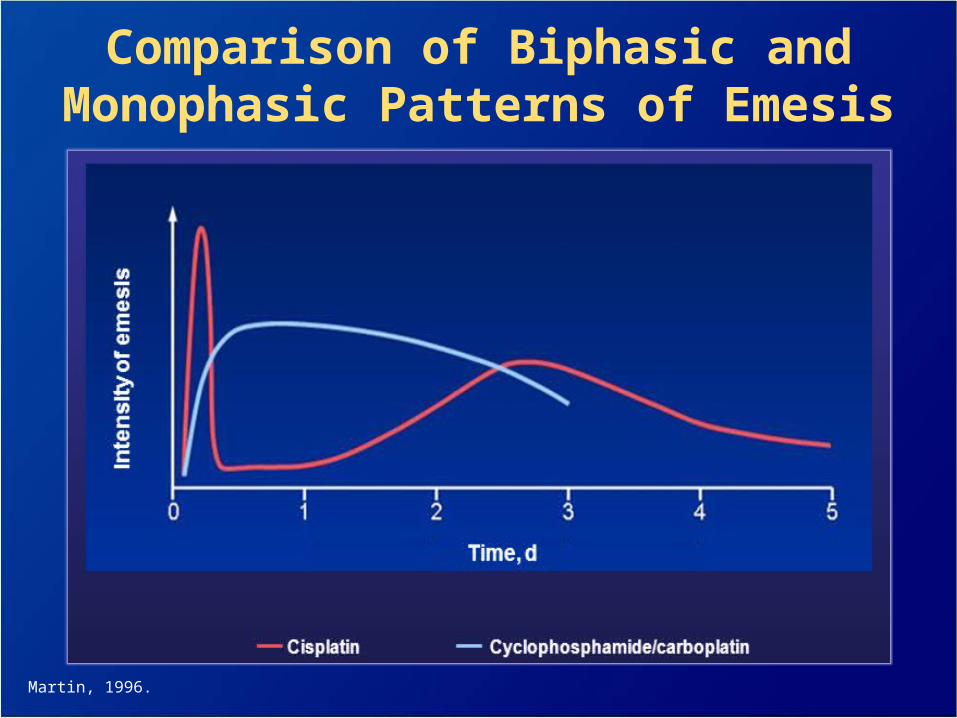
Comparison of Biphasic and Monophasic Patterns of Emesis
Martin, 1996.
Considerations While Selecting the Right Initial Antiemetic
Emetogenicity of chemotherapeutic regimen Side-effect profile of antiemetic(s) Other symptoms Cost Ease of administration
High Emetogenic Potential of Selected Antineoplastic Agents
Drugs with >90% emetic risk:– Cisplatin
– Dacarbazine
– Streptozocin
– Cyclophosphamide ≥1,500 mg/m2
– Ifosfamide ≥2 g/m2 per dose
– Doxorubicin ≥60 mg/m2
– Adriamycin cyclophosphamide (AC) combination defined as either doxorubicin or epirubicin with cyclophosphamide
NCCN, 2014; Basch et al, 2011; Roila et al, 2010.
Moderate Emetogenic Potential of Selected Antineoplastic Agents
Drugs with 30–90% emetic risk:– Oxaliplatin
– Cyclophosphamide ≤1500 mg/m2
– Carboplatin
– Ifosfamide <2 g/m2 per dose
– Irinotecan
– Cytarabine >200 mg/m2
– Anthracyclines (doxorubicin, daunorubicin, epirubicin, idarubicin)
– Methotrexate ≥250 mg/m2NCCN, 2014; Basch et al, 2011; Roila et al, 2010.
Low Emetogenic Potential of Selected Antineoplastic Agents
Drugs with 10–30% emetic risk:– Cytarabine (low dose)
– Gemcitabine
– Topotecan
– Paclitaxel
– Docetaxel
– Pemetrexed
NCCN, 2014; Basch et al, 2011; Roila et al, 2010.
Minimal Emetogenic Potential of Selected Antineoplastic Agents
Drugs with <10% emetic risk:– Vincristine
– Vinblastine
– Vinorelbine
– Fludarabine
– Bleomycin
– Rituximab
– Bevacizumab
– Trastuzumab
– CetuximabNCCN, 2014; Basch et al, 2011; Roila et al, 2010.
Anticholinergics: scopolamine transdermal patch Antihistamines: diphenhydramine Barbiturates: pentobarbital, secobarbital Benzodiazepines: lorazepam Butyrophenones: droperidol, haloperidol Cannabinoids: dronabinol, nabilone Phenothiazines: prochlorperazine,
chlorpromazine, promethazine Atypical antipsychotics: olanzapine
Antiemetics Used in CINV Management
NCCN, 2014; Basch et al, 2011; Roila et al, 2010.
Antiemetics Used in CINV Management (cont.)
NK1 inhibitors: aprepitant, fosaprepitant
Serotonin antagonists: ondansetron, granisetron, dolasetron mesylate, palonosetron
Steroids: dexamethasone, methylprednisolone Substituted benzamines: metoclopramide
NCCN, 2014; Basch et al, 2011; Roila et al, 2010.
Potential Side Effects of Antiemetics
Anticholinergics: dry mouth, drowsiness, blurred vision, disorientation, restlessness, confusion
Antihistamines: drowsiness, restlessness (eg, restless legs), confusion, dizziness, blurred vision/diplopia, tinnitus, dry mouth/nose/throat, urinary retention, frequency, rash, hypotension, palpitations
Wickham, 2012.
Potential Side Effects of Antiemetics (cont.)
Barbiturates: drowsiness, lethargy, hangover, respiratory depression, Stevens-Johnson syndrome, angioedema
Benzodiazepines: drowsiness, sedation, disorientation
Butyrophenones: restlessness, sedation, extrapyramidal reactions, respiratory depression, tachycardia, hypotension, prolonged QT interval (time between Q wave and T wave, inversely proportional to heart rate)
Wickham, 2012.
Potential Side Effects of Antiemetics (cont.)
Cannabinoids: mood changes; disorientation; dizziness; brief impairment of perception, coordination, and sensory functions; tachycardia; hypotension
NK1 inhibitors: weakness, dizziness, diarrhea, constipation, flatus, abdominal discomfort, reflux symptoms, hiccups, headache
Serotonin antagonists: diarrhea, constipation, headache, increased liver function tests
Wickham, 2012.
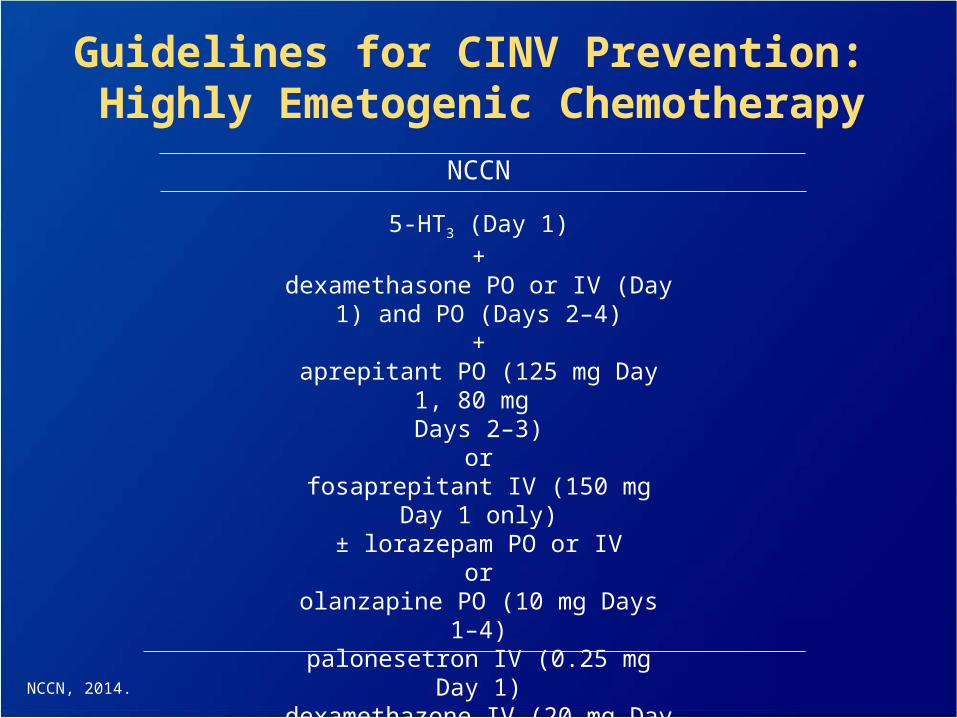
NCCN
5-HT3 (Day 1)+
dexamethasone PO or IV (Day 1) and PO (Days 2–4)
+aprepitant PO (125 mg Day 1, 80 mg
Days 2–3)or
fosaprepitant IV (150 mg Day 1 only)± lorazepam PO or IV
orolanzapine PO (10 mg Days 1–4)palonesetron IV (0.25 mg Day 1)dexamethazone IV (20 mg Day 1)
± lorazepam
Guidelines for CINV Prevention: Highly Emetogenic Chemotherapy
NCCN, 2014.
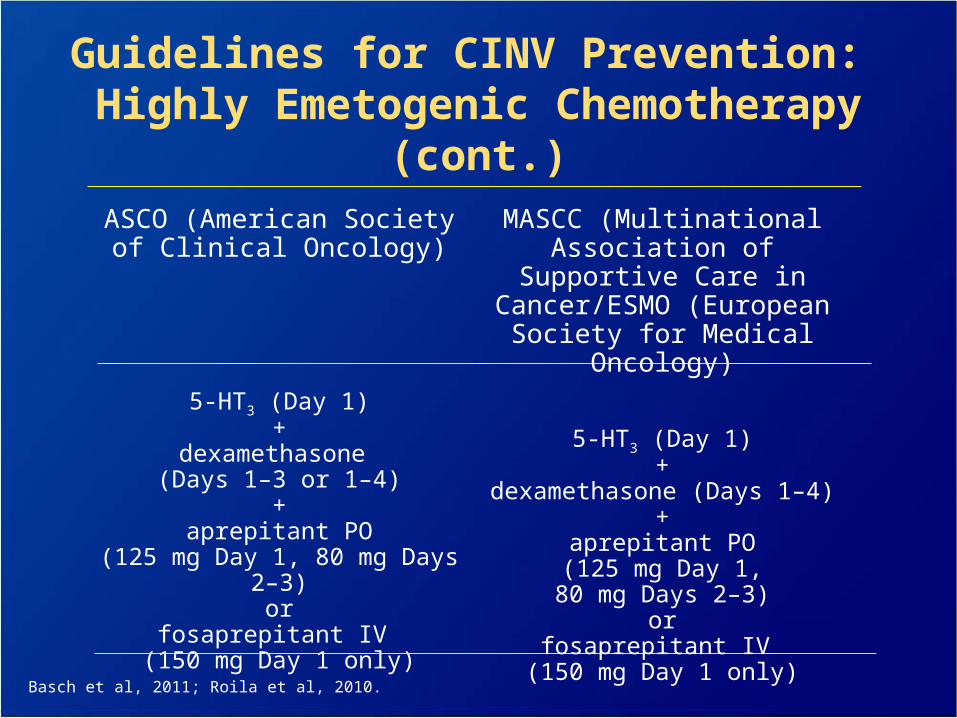
Basch et al, 2011; Roila et al, 2010.
ASCO (American Society of Clinical Oncology)
5-HT3 (Day 1)+
dexamethasone (Days 1–3 or 1–4)
+aprepitant PO
(125 mg Day 1, 80 mg Days 2–3)or
fosaprepitant IV (150 mg Day 1 only)
MASCC (Multinational Association of Supportive
Care in Cancer/ESMO (European Society for
Medical Oncology)
5-HT3 (Day 1)+
dexamethasone (Days 1–4)+
aprepitant PO (125 mg Day 1, 80 mg Days 2–3)
orfosaprepitant IV
(150 mg Day 1 only)
Guidelines for CINV Prevention: Highly Emetogenic Chemotherapy (cont.)
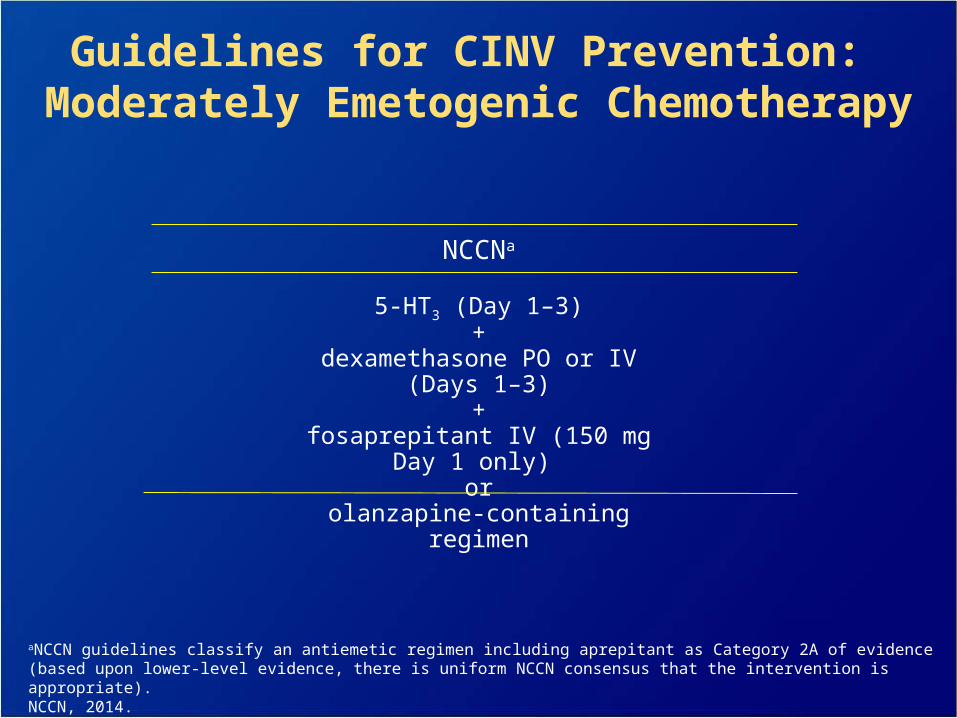
NCCNa
5-HT3 (Day 1–3)+
dexamethasone PO or IV (Days 1–3)+
fosaprepitant IV (150 mg Day 1 only) or
olanzapine-containing regimen
Guidelines for CINV Prevention: Moderately Emetogenic Chemotherapy
aNCCN guidelines classify an antiemetic regimen including aprepitant as Category 2A of evidence (based upon lower-level evidence, there is uniform NCCN consensus that the intervention is appropriate).NCCN, 2014.
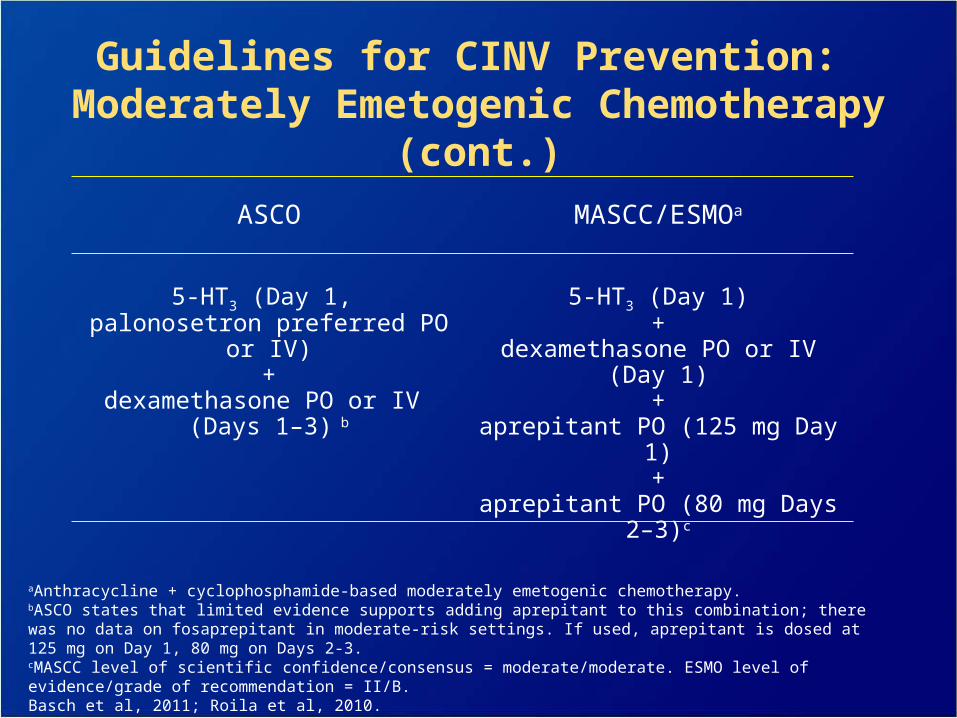
ASCO
5-HT3 (Day 1, palonosetron preferred PO or IV)
+dexamethasone PO or IV
(Days 1–3) b
MASCC/ESMOa
5-HT3 (Day 1)+
dexamethasone PO or IV (Day 1)+
aprepitant PO (125 mg Day 1)+
aprepitant PO (80 mg Days 2–3)c
Guidelines for CINV Prevention: Moderately Emetogenic Chemotherapy (cont.)
aAnthracycline + cyclophosphamide-based moderately emetogenic chemotherapy.bASCO states that limited evidence supports adding aprepitant to this combination; there was no data on fosaprepitant in moderate-risk settings. If used, aprepitant is dosed at 125 mg on Day 1, 80 mg on Days 2-3. cMASCC level of scientific confidence/consensus = moderate/moderate. ESMO level of evidence/grade of recommendation = II/B.Basch et al, 2011; Roila et al, 2010.
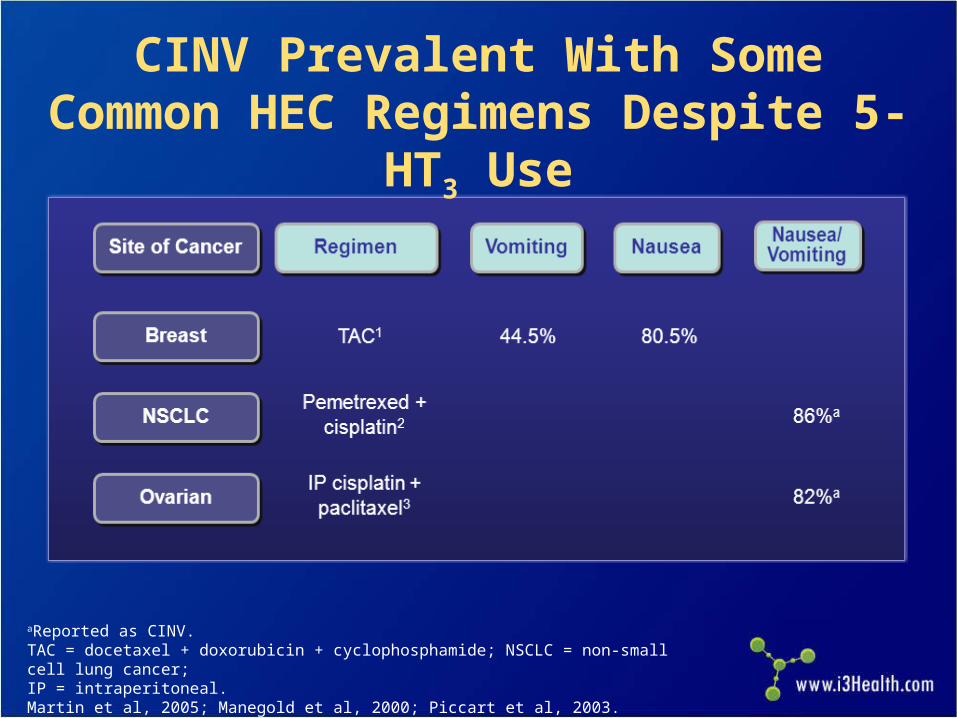
CINV Prevalent With Some Common HEC Regimens Despite 5-HT3 Use
aReported as CINV.TAC = docetaxel + doxorubicin + cyclophosphamide; NSCLC = non-small cell lung cancer; IP = intraperitoneal. Martin et al, 2005; Manegold et al, 2000; Piccart et al, 2003.
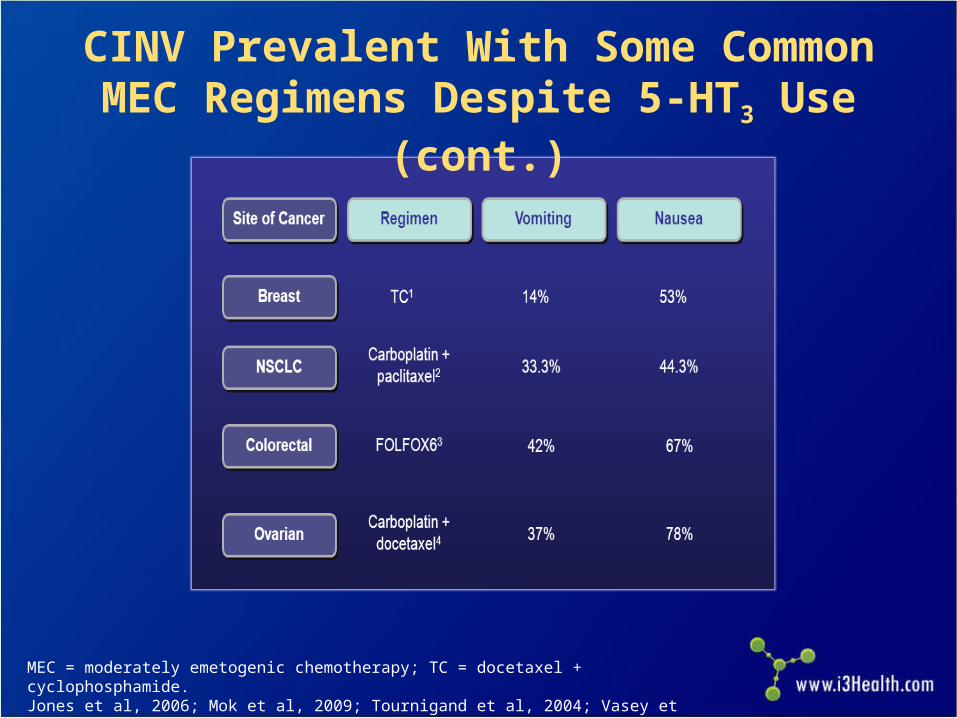
CINV Prevalent With Some Common MEC Regimens Despite 5-HT3 Use (cont.)
MEC = moderately emetogenic chemotherapy; TC = docetaxel + cyclophosphamide.Jones et al, 2006; Mok et al, 2009; Tournigand et al, 2004; Vasey et al, 2004.
Around-the-clock (ATC) a better option than as needed (prn)
Use drug(s) from different class than previously used
NCCN guidelines list specific choices from multiple classes of agents
Management of Breakthrough of Nausea and Vomiting
NCCN, 2014.
Atypical antipsychotic– Olanzapine
– Benzodiazepine
– Lorazepam
Cannabinoid– Dronabinol
– Nabilone
Other– Haloperidol
– Metoclopramide
– ScopolamineNCCN, 2014.
Treatment for Breakthrough Nausea and Vomiting
Treatment for Breakthrough Nausea and Vomiting (cont.)
Phenothiazine– Prochlorperazine
– Promethazine
Serotonin 5-HT3 antagonists
– Dolasetron
– Granisetron
– Ondansetron
Steroid– Dexamethasone
NCCN, 2014.
Prevention and Treatment of Anticipatory Emesis
Prevention is key Use optimal antiemetic therapy
– Behavioral therapy
– Relaxation/systemic desensitization
– Hypnosis/guided imagery
– Music therapy
– Acupuncture/acupressure
Alprazolam or lorazepam
NCCN, 2014.
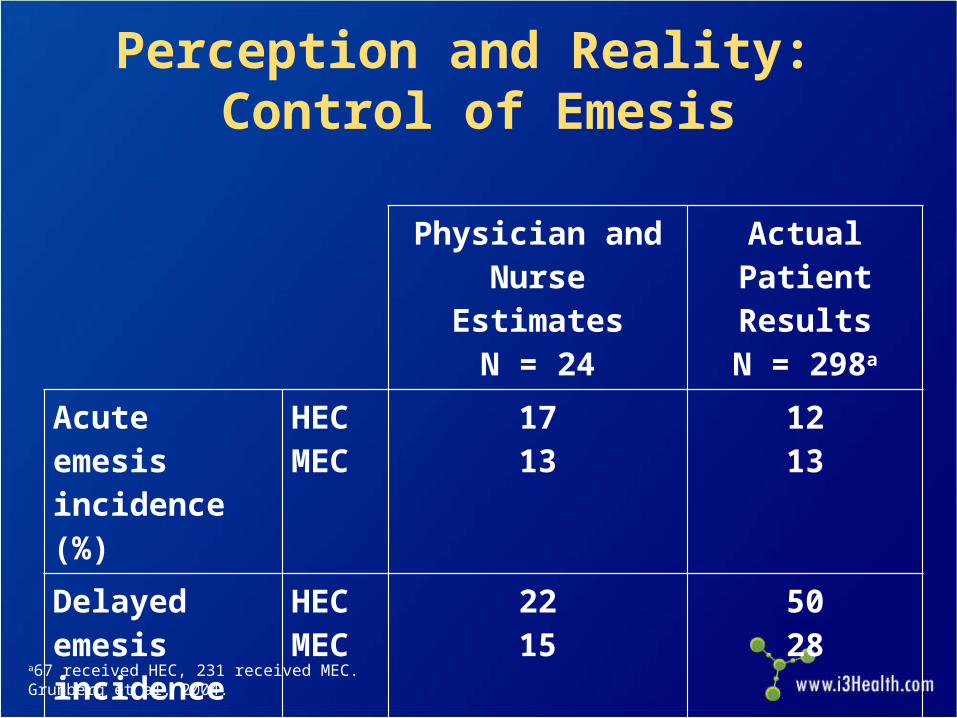
Physician andNurse Estimates
N = 24
Actual PatientResultsN = 298a
Acute emesis incidence (%)
HECMEC
1713
1213
Delayed emesis incidence (%)
HECMEC
2215
5028
Perception and Reality: Control of Emesis
a67 received HEC, 231 received MEC.Grunberg et al, 2004.
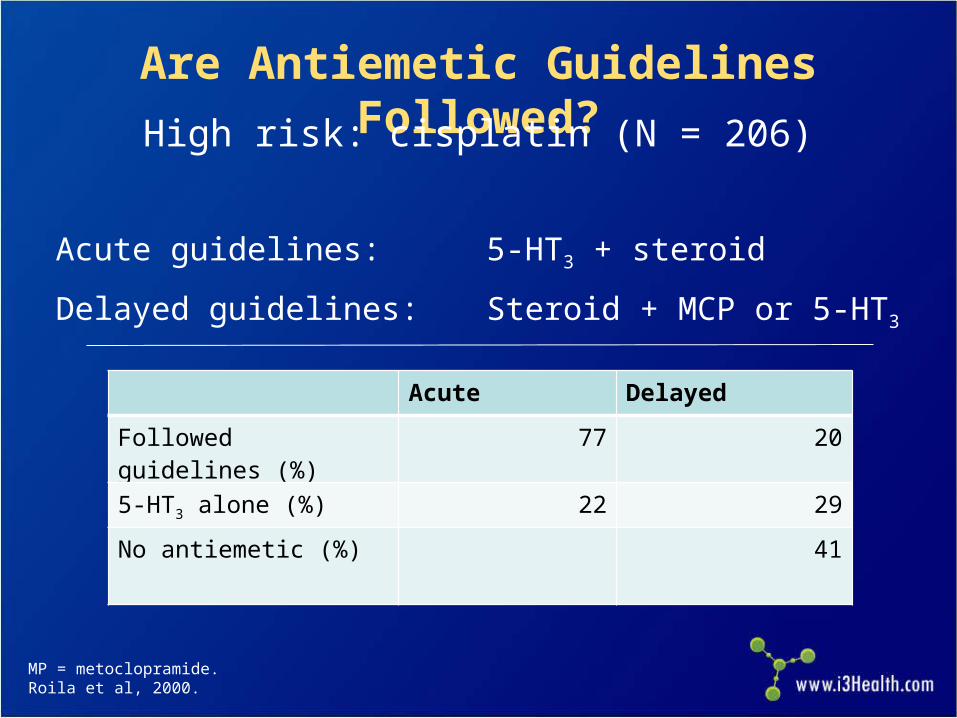
MP = metoclopramide.Roila et al, 2000.
Acute guidelines: 5-HT3 + steroid
Delayed guidelines: Steroid + MCP or 5-HT3
Are Antiemetic Guidelines Followed?
High risk: cisplatin (N = 206)
Acute Delayed
Followed guidelines (%) 77 20
5-HT3 alone (%) 22 29
No antiemetic (%) 41
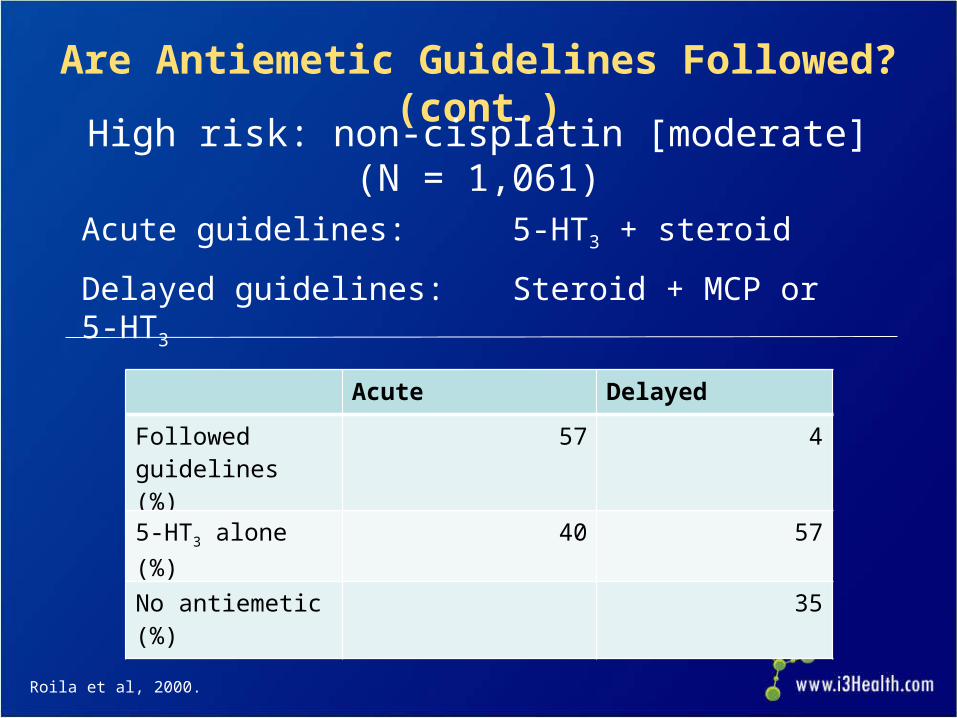
Acute guidelines: 5-HT3 + steroid
Delayed guidelines: Steroid + MCP or 5-HT3
Are Antiemetic Guidelines Followed? (cont.)
High risk: non-cisplatin [moderate] (N = 1,061)
Roila et al, 2000.
Acute Delayed
Followed guidelines (%)
57 4
5-HT3 alone (%) 40 57
No antiemetic (%) 35
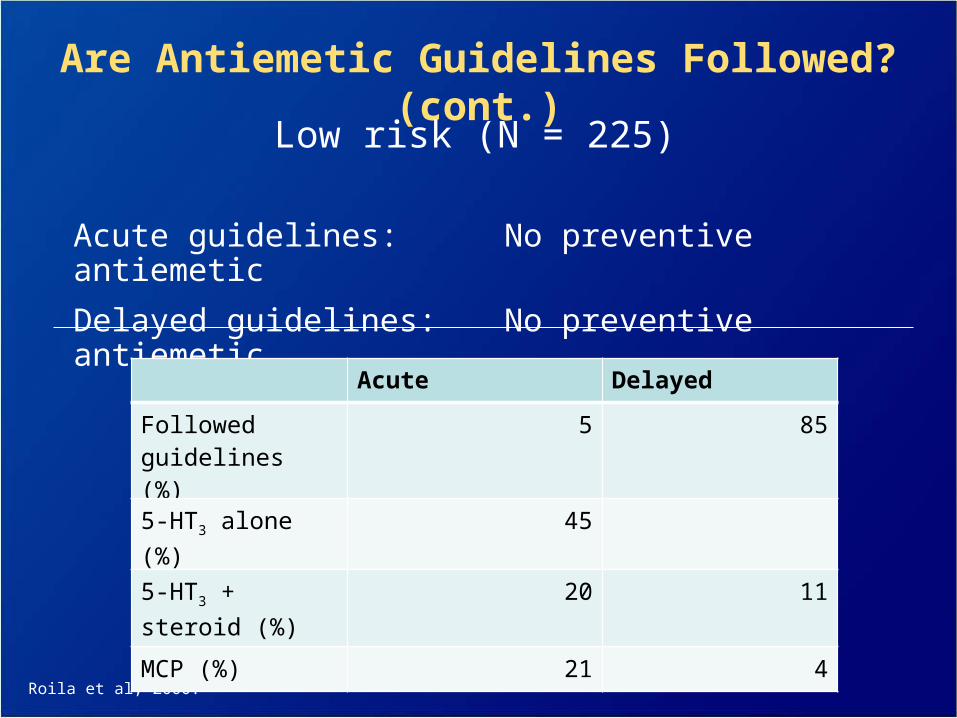
Acute guidelines: No preventive antiemetic
Delayed guidelines: No preventive antiemetic
Roila et al, 2000.
Are Antiemetic Guidelines Followed? (cont.)
Low risk (N = 225)
Acute Delayed
Followed guidelines (%)
5 85
5-HT3 alone (%) 45
5-HT3 + steroid (%)
20 11
MCP (%) 21 4
NCCN Guidelines:Principles of CINV Control
Current NCCN guidelines include the following principles: – Prevention is the goal
– Risk of CINV lasts for at least 3 days with HEC and 2 days with MEC
– Consider the toxicity of specific antiemetic(s)
– Choose antiemetic(s) based on emetogenicity of therapy and patient factors
– Consider other potential causes of emesis in cancer patients (eg, bowel obstruction, electrolyte imbalance, brain metastases)
NCCN, 2014.
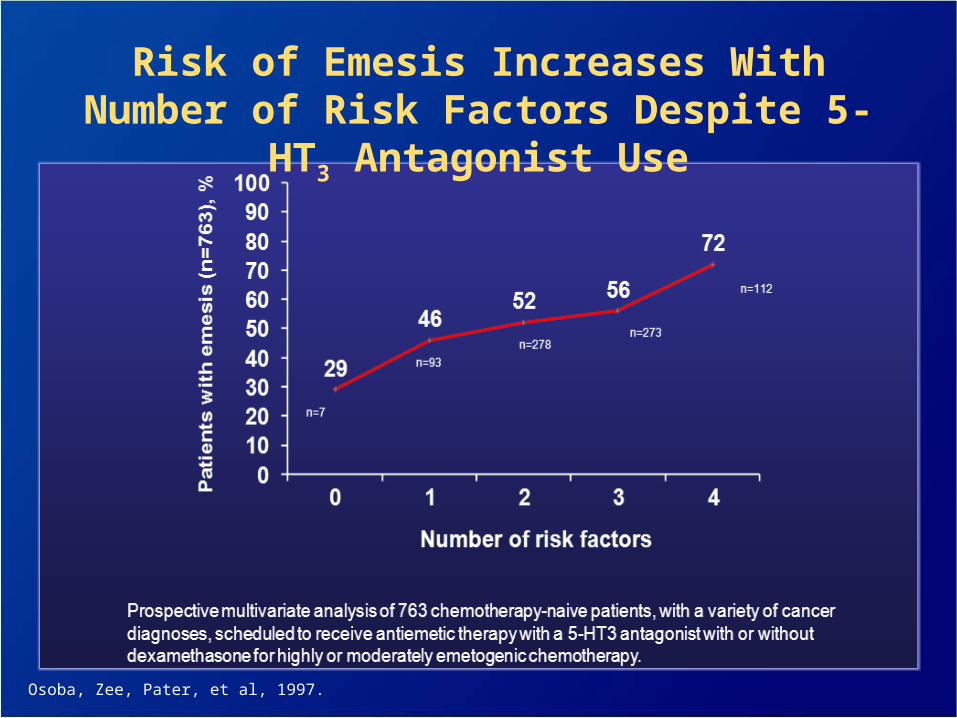
Risk of Emesis Increases With Number of Risk Factors Despite 5-HT3 Antagonist Use
Osoba, Zee, Pater, et al, 1997.
CINV: Aim for Prevention
Prevention of CINV is the goal
– Patients need protection for the full period of CINV risk
– Assess patient and chemotherapy factors related to CINV risk
– The choice of antiemetic(s) should be based on emetogenicity of
therapy and patient risk factors
Provide patient education and counseling tools for both in-
office and take-home use
– They should be simple and easy to understand
– Consider a visual analog scale for nausea and patient diaries for
vomiting
– MASCC Antiemesis Tool is available online at
http://www.mascc.org/matNCCN, 2014; Basch et al, 2011; Roila et al, 2010; Boogaerts et al, 2000; Osoba, Zee, Pater, et al, 1997.
Case Study 1: Delayed CINV
Ms. DL is a 49-year-old attorney with node-positive invasive ductal carcinoma of the breast, estrogen and progesterone receptor positive, and human epidermal growth factor receptor 2 (HER2) negative. She undergoes a lumpectomy
Oncologist recommends adjuvant chemotherapy with four cycles of AC chemotherapy: doxorubicin 60 mg/m2 and cyclophosphamide 600 mg/m2 IV Day 1, every 3 weeks
Patient is anxious and concerned about any side effects that might keep her from working
Case Study 1 (cont.)
Which chemotherapy-induced side effects may be particularly important for this patient?
a. Nausea and vomiting
b. Alopecia
c. Neutropenia
d. All of the above
Case Study 1 (cont.)
Which patient characteristic can increase the risk for CINV?
a. Female sex
b. Age <50 years
c. Anxiety
d. All of the above
Case Study 1 (cont.)
What other risk factors for CINV might be important in this patient?– History of motion sickness
– History of morning sickness
– History of low alcohol intake (<1.5 oz/d)
Case Study 1 (cont.)
What steps can be taken to prevent CINV in this patient?– Make prevention a goal of treatment
– Implement optimal prophylaxis to prevent both acute and delayed CINV
– Start antiemetic therapy before chemotherapy
Case Study 2: Breakthrough CINV
Mr. CW is a 72-year-old engineer with stage IIA adenocarcinoma of the lung; status post right-upper lobectomy and mediastinal lymphadenopathy
Oncologist recommends adjuvant chemotherapy with docetaxel 75 mg/m2 IV and cisplatin 75 mg/m2 IV Day 1, every 3 weeks for four cycles
Case Study 2 (cont.)
Mr. CW’s regimen is considered highly emetogenic.
a. True
b. False
Case Study 2 (cont.)
Oncologist reviews side effects associated with chemotherapy regimen
Tells patient that 75% of patients experience some nausea and vomiting (grades 1 and 2) while approximately 24% experience severe nausea and vomiting (grades 3 and 4)
Patient states he is very anxious about occurrence of nausea and vomiting
Case Study 2 (cont.)
Since patient is receiving a regimen considered highly emetogenic, oncologist gives patient the following antiemetic regimen prior to starting chemotherapy:
– Fosaprepitant 150 mg IV Day 1
– Palonosetron 0.25 mg IV Day 1
– Dexamethasone 12 mg IV Day 1 and 8 mg PO Day 2, then 8 mg PO twice daily Days 3–4
Patient also given lorazepam 0.5 mg PO every 6 hours Days 1–4
Case Study 2 (cont.)
Mr. CW experiences some nausea without vomiting during first 24 hours after chemotherapy
Experiences progressive nausea and vomiting for next 96 hours
Forty-eight hours after he received chemotherapy, patient calls oncology nurse, who recommends additional antiemetics for breakthrough nausea and vomiting
Case Study 2 (cont.)
What regimen would you recommend for Mr. CW’s breakthrough nausea and vomiting?– Add one agent from a different class to current
regimen
– Consider increasing dose of lorazepam
Case Study 3: Refractory CINV
Ms. WB is a 56-year-old woman with stage IV ovarian carcinoma with bulky abdominal metastases as well as liver metastases– ECOG (Eastern Cooperative Oncology Group)
performance status 2
– Complains of abdominal pain for which she is receiving narcotics
Started on paclitaxel 175 mg/m2 IV Day 1 and carboplatin with area under the curve (AUC) 6 IV Day 1 given every 3 weeks
Case Study 3 (cont.)
With the first cycle of chemotherapy, Ms. WB received palonosetron 0.25 mg IV Day 1 and dexamethasone 12 mg IV Day 1– Developed nausea and vomiting on the evening of Day 1
extending through Day 2
With the second cycle, fosaprepitant 150 mg IV Day 1 was added to the previous antiemetic regimen– Developed more nausea and vomiting that continued for a
week
Case Study 3 (cont.)
What is the appropriate management of refractory nausea and vomiting?
a. Investigate other causes of nausea and vomiting (eg, liver metastases, bowel obstruction)
b. Increase doses of antiemetics
c. Switch antiemetics
d. a and c
Antiemetic Treatment: Current Status and Future Considerations
Marked advances in antiemetic therapy have occurred over past few decades and recently
Best antiemetic control occurs when efficacy from clinical trials is emulated in clinical practice
Advances have had major impact on patient QOL and patterns of treatment (move to ambulatory chemotherapy)
Future studies need to concentrate on mechanisms of resistance and identification of patients at risk
Research is needed on understanding and controlling nausea
New agents are needed
Aapro MS, Molassiotis A, and Olver I (2005). Anticipatory nausea and vomiting. Support Care Cancer, 13(2):117-121.Andrews PLR, Naylor RJ, and Joss RA (1998). Neuropharmocology of emesis and its relevance to anti-emetic therapy.
Consensus and controversies. Support Care Cancer, 6(3):197-203.Basch E, Prestrud AA, Hesketh PJ, et al (2011). Antiemetics: American Society of Clinical Oncology clinical practice
guideline update. J Clin Oncol, 29(31):4189-4198. DOI:10.1200/JCO.2010.34.4614.Bloechl-Daum B, Deuson RR, Mavros P, et al (2006). Delayed nausea and vomiting continue to reduce patients’ quality
of life after highly and moderately emetogenic chemotherapy despite antiemetic treatment. J Clin Oncol, 24(27):4472-4478.
Boogaerts JG, Vanacker, E, Seidel L, et al (2000). Assessment of postoperative nausea using a visual analogue scale. Acta Anaesthesiol Scand, 44(4)470-474.
Börjeson S, Hursti TJ, Tishelman C, et al (2002). Treatment of nausea and emesis during cancer chemotherapy. Discrepancies between antiemetic effect and well-being. J Pain Symptom Manage, 24(3):345-358.
de Boer-Dennert M, de Wit R, Schmitz PI, et al (1997). Patient perceptions of the side-effects of chemotherapy: the influence of 5HT3 antagonists. Br J Cancer, 76(8):1057.
DeVane CL (2001). Substance P: a new era, a new role. Pharmacotherapy, 21(9):1061-1069. Fernández-Ortega P, Caloto MT, Chirveches E, et al (2012). Chemotherapy-induced nausea and vomiting in clinical
practice: impact on patients' quality of life. Support Care Cancer, 20(12):3141-3148. Grunberg SM (2012). Patient-centered management of chemotherapy-induced nausea and vomiting . Cancer Control,
19(suppl):10-15. Grunberg SM, Deuson RR, Mavros P, et al (2004). Incidence of chemotherapy-induced nausea and emesis after
modern antiemetics. Cancer, 100(10):2261-2268.Hargreaves R (2002). Imaging substance P receptors (NK1) in the living human brain using positron emission
tomography. J Clin Psychiatry, 63(suppl 11):18-24.Hesketh PJ (2001). Potential role of the NK1 receptor antagonists in chemotherapy-induced nausea and vomiting.
Support Care Cancer, 9(5):350-354.
References
Hesketh PJ, Van Belle S, Aapro M et al (2003). Differential involvement of neurotransmitters through the time course of cisplatin-induced emesis as revealed by therapy with specific receptor antagonists. Eur J Cancer, 39(8):1074-1080.
Jones SE, Savin MA, Holmes FA, et al (2006). Phase III trial comparing doxorubicin plus cyclophosphamide with docetaxel plus cyclophosphamide as adjuvant therapy for operable breast cancer. J Clin Oncol, 24(31):5381-5387.
Lau PM, Stewart K, and Dooley M (2004). The ten most common adverse drug reactions (ADRs) in oncology patients: do they matter to you? Support Care Cancer, 12(9):626-633.
Manegold C, Gatzemeier U, von Pawel J, et al (2000). Front-line treatment of advanced non-small-cell lung cancer with MTA (LY231514, pemetrexed disodium, ALIMTA) and cisplatin: a multicenter phase II trial. Ann Oncol, 11(4):435-440.
Martin M (1996). The severity and pattern of emesis following cytotoxic agents. Oncology, 53(suppl 1):26-31.Martin M, Pienkowski T, Mackey J, et al (2005). Adjuvant docetaxel for node-positive breast cancer. N Engl J Med,
352(22):2302-2313.Miner WD and Sanger GJ (1986). Inhibition of cisplatin-induced vomiting by selective 5-hydroxytryptamine M-receptor
antagonism. Br J Pharmacol, 88(3):497-499.Mok TS, Wu YL, Thongprasert S, et al (2009). Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl
J Med, 361:947-957. DOI:10.1056/NEJMoa0810699National Comprehensive Cancer Network (2014). NCCN Clinical Practice Guidelines in Oncology: Antiemesis.
Accessed on: March 21, 2014. Available at: http://www.nccn.org/professionals/physician_gls/pdf/antiemesis.pdfNeijt JP, Engelholm SA, Tuxen MK, et al (2000). Exploratory phase III study of paclitaxel and cisplatin versus paclitaxel
and carboplatin in advanced ovarian cancer. J Clin Oncol, 18(17):3084-3092.Osoba D, Zee B, Pater J, et al (1997). Determinants of postchemotherapy nausea and vomiting in patients with cancer.
J Clin Oncol, 15(1):116-123.
References
Osoba D, Zee B, Warr D, et al (1997). Effect of postchemotherapy nausea and vomiting on health-related quality of life. Support Care Cancer, 5(4):307-313.
Piccart MJ, Floquet A, Scarfone G, et al (2003). Intraperitoneal cisplatin versus no further treatment: 8-year results of EORTC 55875, a randomized phase III study in ovarian cancer patients with a pathologically complete remission after platinum-based intravenous chemotherapy. Int J Gynecol Cancer, 13(suppl 2):196-203.
Roila F, De Angelis V, Patola L, et al (2000). Antiemetic prescriptions in 77 Italian oncological centers after the MASCC Consensus Conference. Support Care Cancer, 8:241.
Roila F, Herrstedt J, Aapro M, et al (2010). Guideline update for MASCC and ESMO in the prevention of chemotherapy and radiotherapy-induced nausea and vomiting: results of the Perugia consensus conference. Ann Oncol, 21(suppl 5):v232-v243.
Sun CC, Bodurka DC, Weaver CB, et al (2005). Rankings and symptom assessments of side effects from chemotherapy: insights from experienced patients with ovarian cancer. Support Care Cancer, 13(4):219-227.
Tattersall FD, Rycroft W, Francis B, et al (1996). Tachykinin NK1 receptor antagonists act centrally to inhibit emesis induced by the chemotherapeutic agent cisplatin in ferrets. Neuropharmacology, 35(8):1121-1129.
Tavorath R and Hesketh PJ (1996). Drug treatment of chemotherapy-induced delayed emesis. Drugs, 52(5):639-648.Tournigand C, André T, Achille E, et al (2004). FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced
colorectal cancer: a randomized GERCOR study. J Clin Oncol, 22(2):229-237Vasey PA, Jayson GC, Gordon A, et al (2004). Phase III randomized trial of docetaxel-carboplatin versus paclitaxel-
carboplatin as first-line chemotherapy for ovarian carcinoma. J Natl Cancer Inst, 96(22):1682-1691.Wickham R (2012). Evolving treatment paradigms for chemotherapy-induced nausea and vomiting . Cancer Control,
19(2 suppl):3-9.Wilder-Smith OH, Borgeat A, Chappuis P, et al (1993). Urinary serotonin metabolite excretion during cisplatin
chemotherapy. Cancer, 72(7):2239-2241.
References