Embed Size (px)
Citation preview
Epigenetics and Epigenetics and CancerCancer
++
Nilofer Azad, MDNilofer Azad, MDAssistant Professor, Gastrointestinal Oncology/Phase I ProgramAssistant Professor, Gastrointestinal Oncology/Phase I Program
Sidney Kimmel Comprehensive Cancer CenterSidney Kimmel Comprehensive Cancer CenterOctober 19, 2010October 19, 2010
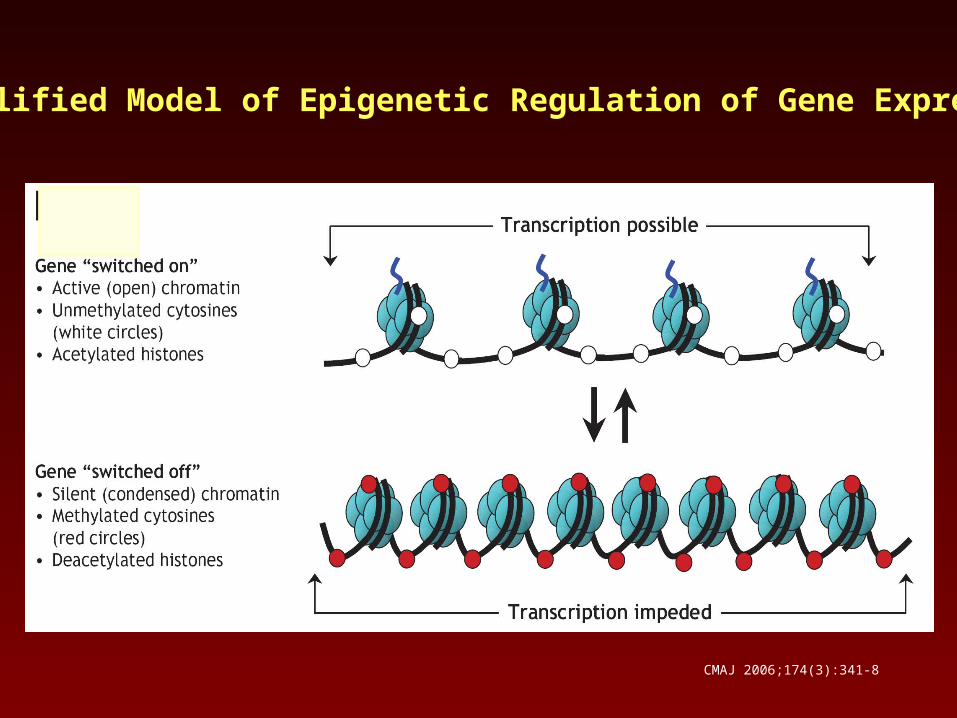
CMAJ 2006;174(3):341-8
Simplified Model of Epigenetic Regulation of Gene Expression
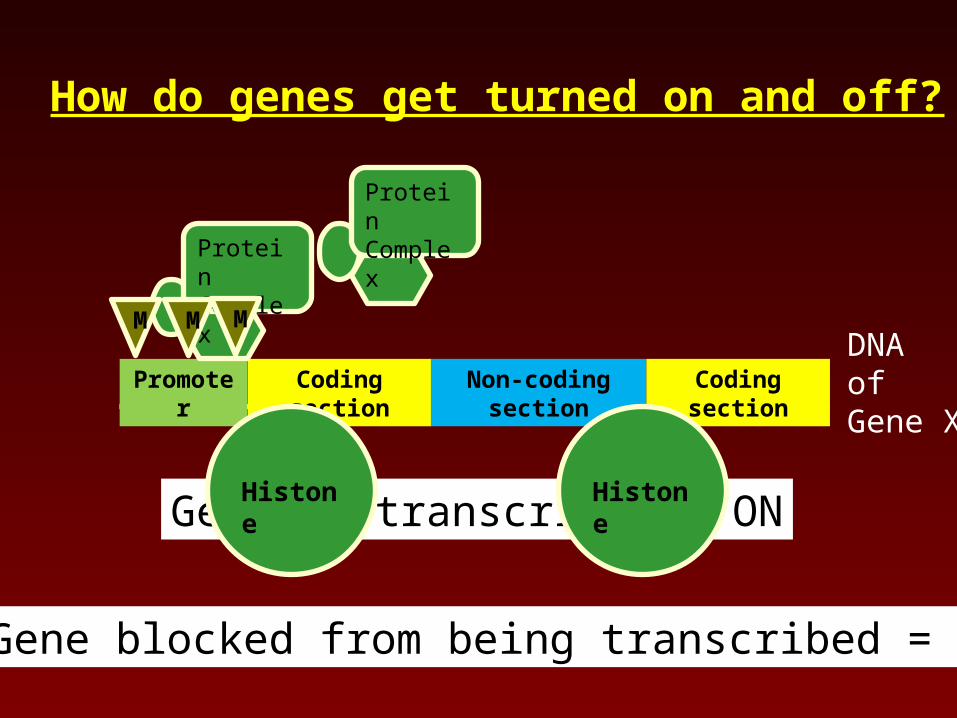
Promoter Coding section Non-coding section Coding section
Protein Complex
How do genes get turned on and off?
DNAofGene X
M M M
Gene is transcribed = ON
Gene blocked from being transcribed = OFF
Histone Histone
Protein Complex
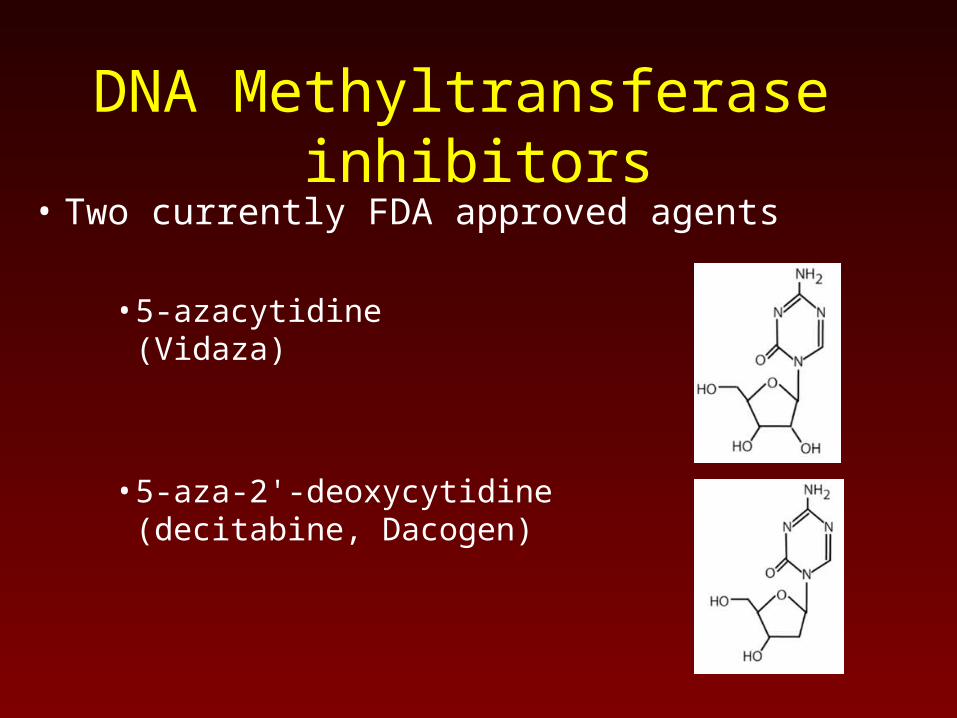
DNA Methyltransferase inhibitors
• Two currently FDA approved agents
• 5-azacytidine(Vidaza)
• 5-aza-2'-deoxycytidine (decitabine, Dacogen)
5-azacitidine
• FDA approved in 2004 for myelodysplasia
• Dose: 75 mg/m2 SQ daily x 7 d / 28 d cycle
• Mechanism of action: Incorporated into DNA → suicide inhibitor of DNMTInduces global hypomethylation
• Time to clinical response: Average = 4 months
Histone deacetylase inhibitors• Three currently FDA approved agents
• Vorinostat (Pan-HDACi)(SAHA, Zolinza) Oral agentApproved for cutaneous T-cell lymphoma
• Depsipeptide (Pan-HDACi)(Istodax) Intravenous agent
Approved for cutaneous T-cell lymphoma
• Valproic acid (weak inhibitor) anti-seizure
LUNG CANCER
Rationale for double epigenetic blockage in lung cancer
• Epigenetic gene silencing mediated by DNA methylation and histone deaceylation is a key contributor to lung carcinogenesis
• Preclinical studies suggest that combining DMNTi with HDACi synergistically enhances expression of silenced tumor suppressor genes
• Clinical studies combining DMNTi and HDACi have shown remarkable clinical activity in MDS/AML
• Hypothesis: similar effect in NSCLC
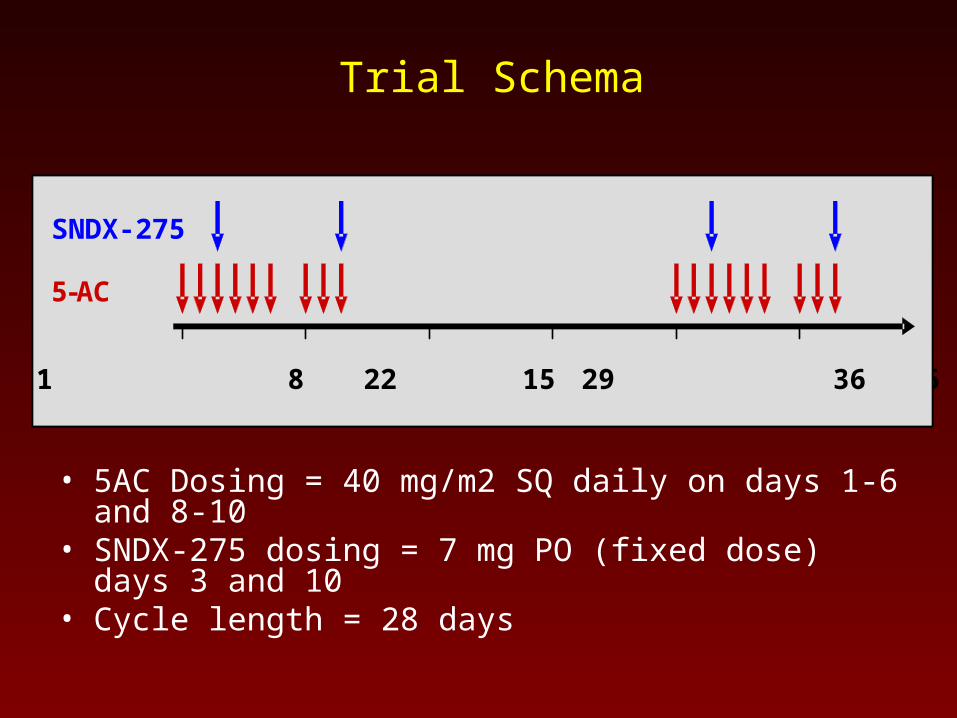
Trial Schema
• 5AC Dosing = 40 mg/m2 SQ daily on days 1-6 and 8-10• SNDX-275 dosing = 7 mg PO (fixed dose) days 3 and 10• Cycle length = 28 days
MS275
5-Aza
Day 1 8 15 22 29 36
SNDX-275
5-AC
Day 1 8 15 22 29 36
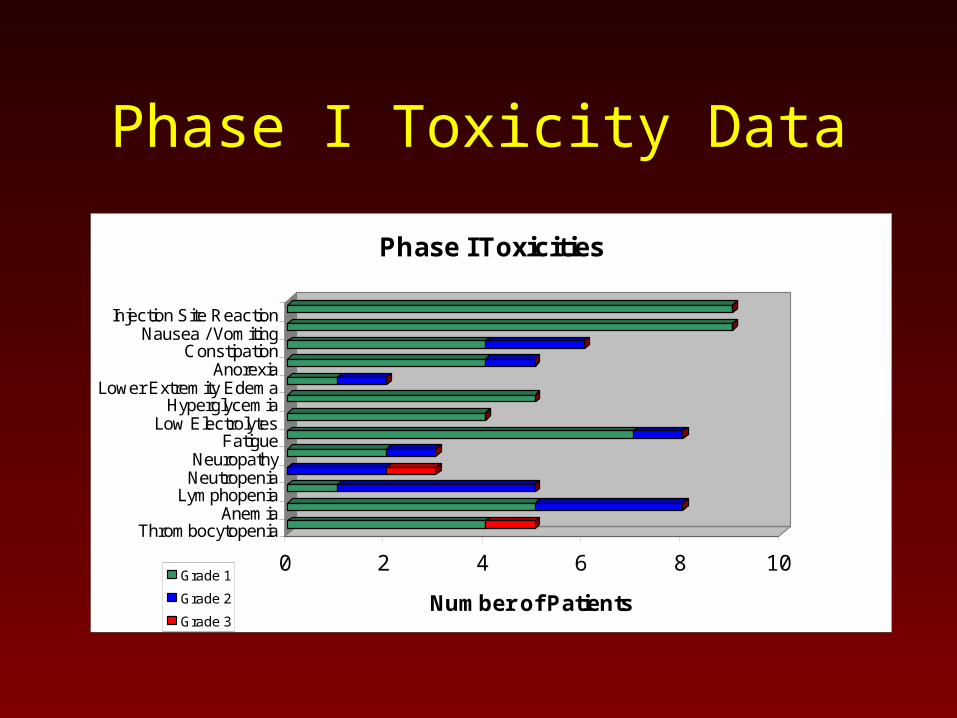
Phase I Toxicity Data
0 2 4 6 8 10
Number of Patients
Injection Site ReactionNausea / Vomiting
ConstipationAnorexia
Lower Extremity EdemaHyperglycemia
Low ElectrolytesFatigue
NeuropathyNeutropenia
LymphopeniaAnemia
Thrombocytopenia
Phase I Toxicities
Grade 1
Grade 2
Grade 3
Updated Response Data28 Evaluable Patients
• 1 Complete Response – On treatment for 14 months
• 1 Partial Response
Responded for 8 months – then new SCLC
Still no progression of his NSCLC 9 months off epigenetic therapy
• 8 Stable Disease One on treatment for 18 months; Five treated for 4 months
One treated for 3 months then stopped due to schedule
One still being treated (on cycle 12 now)
• 17 Progressive Disease
• 8 Not evaluable (finished less than 1 cycle)
• 5 Actively being treated
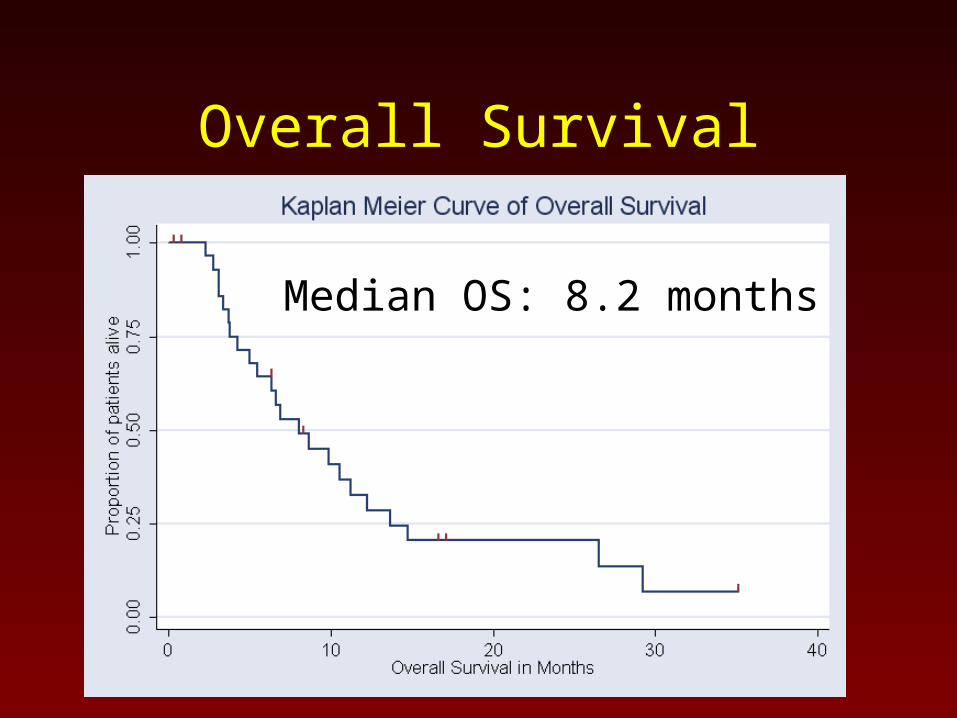
Overall Survival
Median OS: 8.2 months

Images of Patient with Complete Response
56 year old woman with stage I lung cancer that was resected and treated with adjuvant chemotherapy.She progressed after salvage chemotherapy with radiation at relapse.She had a response after 2 cycles, continued improvement after 4; 14 cycles were given. She had 3 prior therapies for advanced disease.
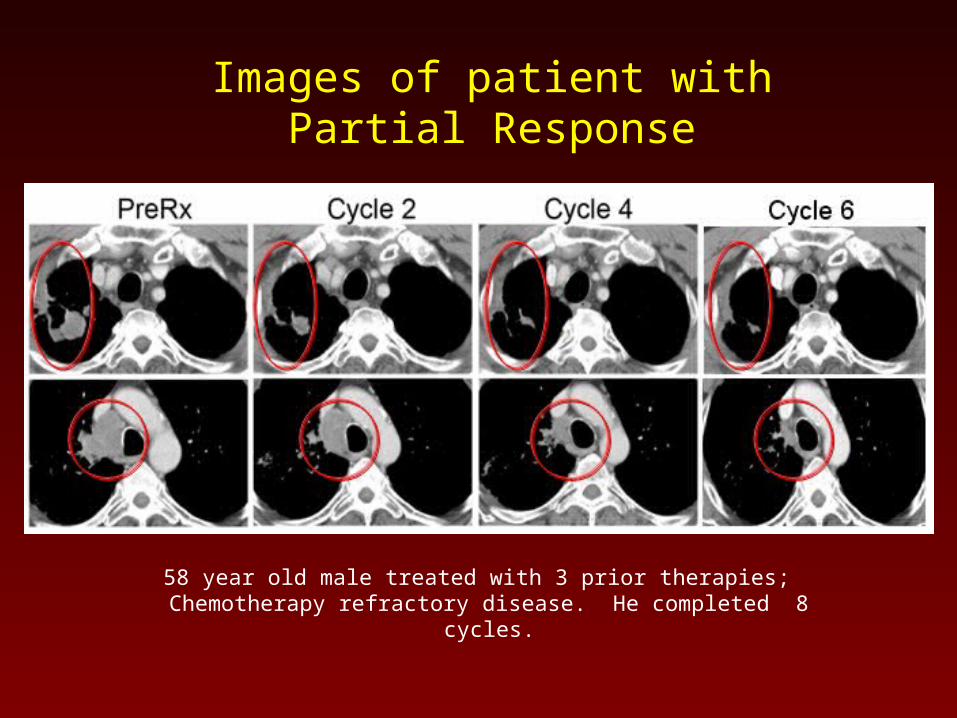
Images of patient withPartial Response
58 year old male treated with 3 prior therapies; Chemotherapy refractory disease. He completed 8 cycles.
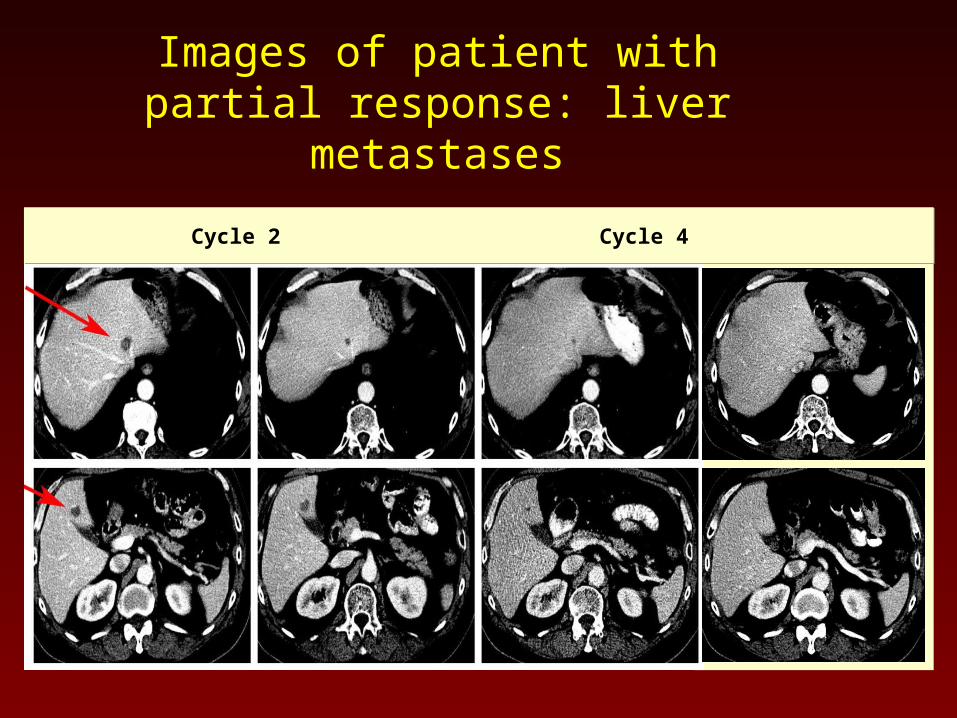
Images of patient with partial response: liver metastases
Pre-treatment Cycle 2 Cycle 4 Cycle 8 Pre-treatment Cycle 2 Cycle 4 Cycle 8
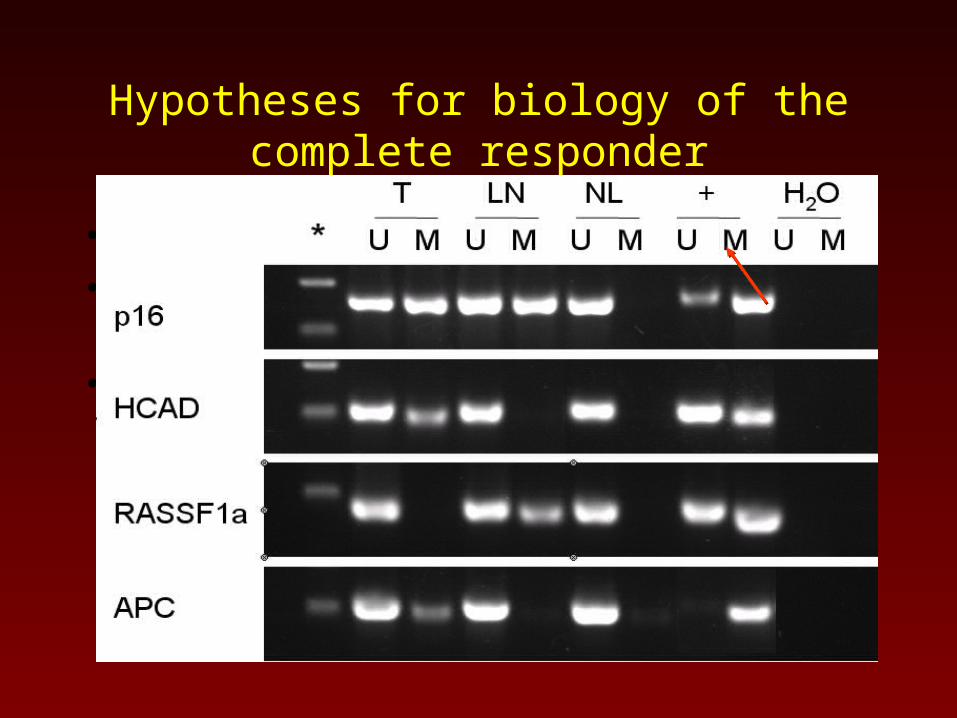
Hypotheses for biology of the complete responder
• Fewer number of previous therapies…
• Higher serum level of 5-azacitidine…
• Epigenetics…• Responding patient was a previously resected stage
I NSCLC patient
• Analysis of her tumor and mediastinal lymph nodes found a methylation pattern that predicted she was at high risk for early recurrence
Response
PD NE SD CR
5A
C C
ma
x (n
g/m
L)
0
500
1000
1500
2000
14500
15000
15500
0 1 2 3 4 5
0.00
0.25
0.50
0.75
1.00
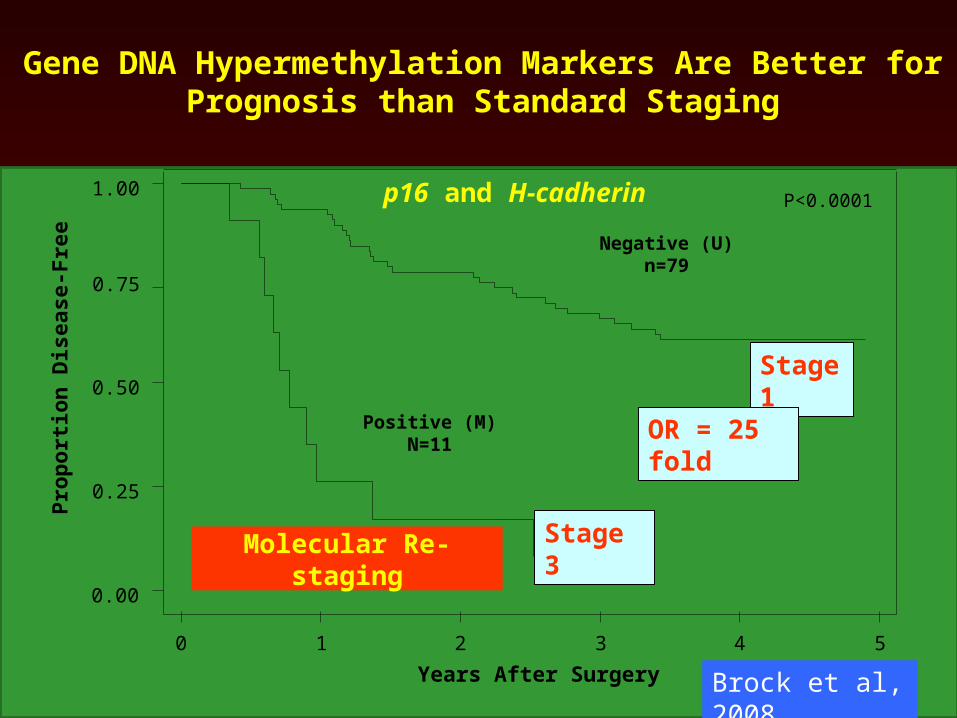
Negative (U)n=79
Positive (M)N=11
P<0.0001
Stage 1
Stage 3
Gene DNA Hypermethylation Markers Are Better for Prognosis than Standard Staging
Prop
ortio
n D
isea
se-F
ree
Years After Surgery
OR = 25 fold
p16 and H-cadherin
Brock et al, 2008
Molecular Re-staging
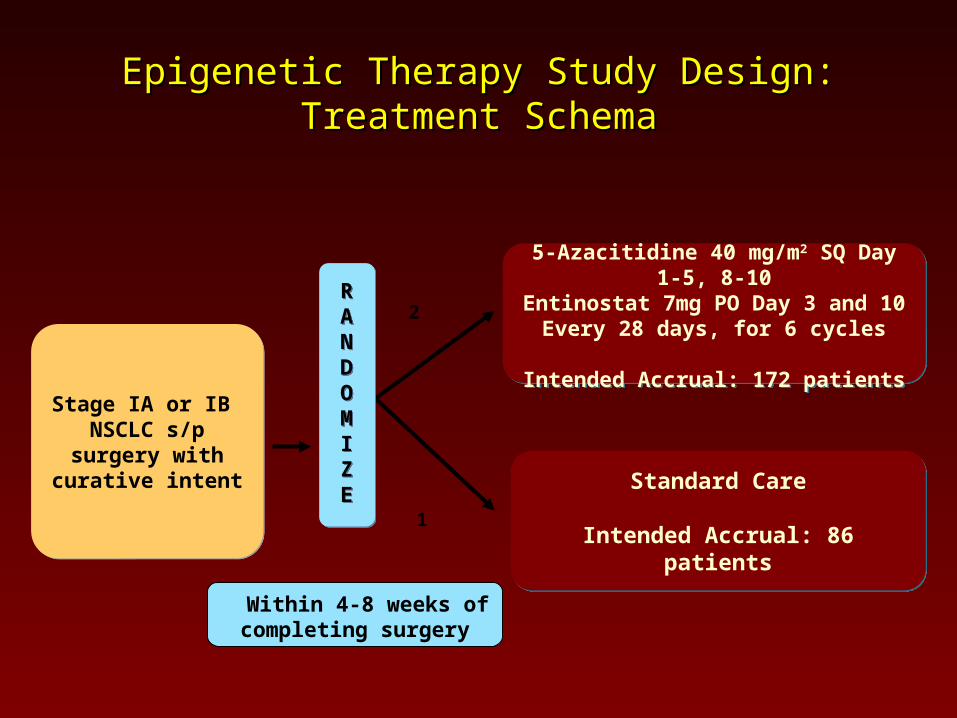
Epigenetic Therapy Study Design: Treatment Epigenetic Therapy Study Design: Treatment SchemaSchema
2
1
5-Azacitidine 40 mg/m2 SQ Day 1-5, 8-10Entinostat 7mg PO Day 3 and 10
Every 28 days, for 6 cycles
Intended Accrual: 172 patients
5-Azacitidine 40 mg/m2 SQ Day 1-5, 8-10Entinostat 7mg PO Day 3 and 10
Every 28 days, for 6 cycles
Intended Accrual: 172 patients
Stage IA or IB NSCLC s/p surgery with curative intent
Stage IA or IB NSCLC s/p surgery with curative intent
RANDOMIZE
RANDOMIZE Standard Care
Intended Accrual: 86 patients
Standard Care
Intended Accrual: 86 patients
Within 4-8 weeks of completing surgery
COLON CANCER
Men294,120
Women271,530
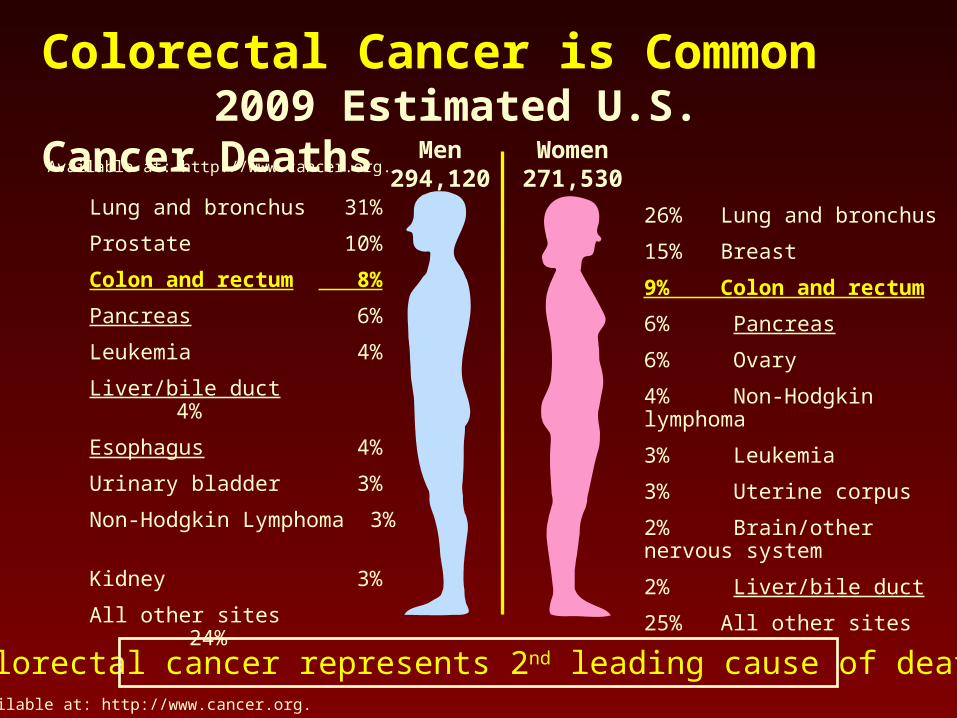
Available at: http://www.cancer.org.
Colorectal Cancer is Common 2009 Estimated U.S. Cancer Deaths
Colorectal cancer represents 2nd leading cause of death
Lung and bronchus 31%
Prostate 10%
Colon and rectum 8%
Pancreas 6%
Leukemia 4%
Liver/bile duct 4%
Esophagus 4%
Urinary bladder 3%
Non-Hodgkin Lymphoma 3%
Kidney 3%
All other sites 24%
26% Lung and bronchus
15% Breast
9% Colon and rectum
6% Pancreas
6% Ovary
4% Non-Hodgkin lymphoma
3% Leukemia
3% Uterine corpus
2% Brain/other nervous system
2% Liver/bile duct
25% All other sites
Available at: http://www.cancer.org.
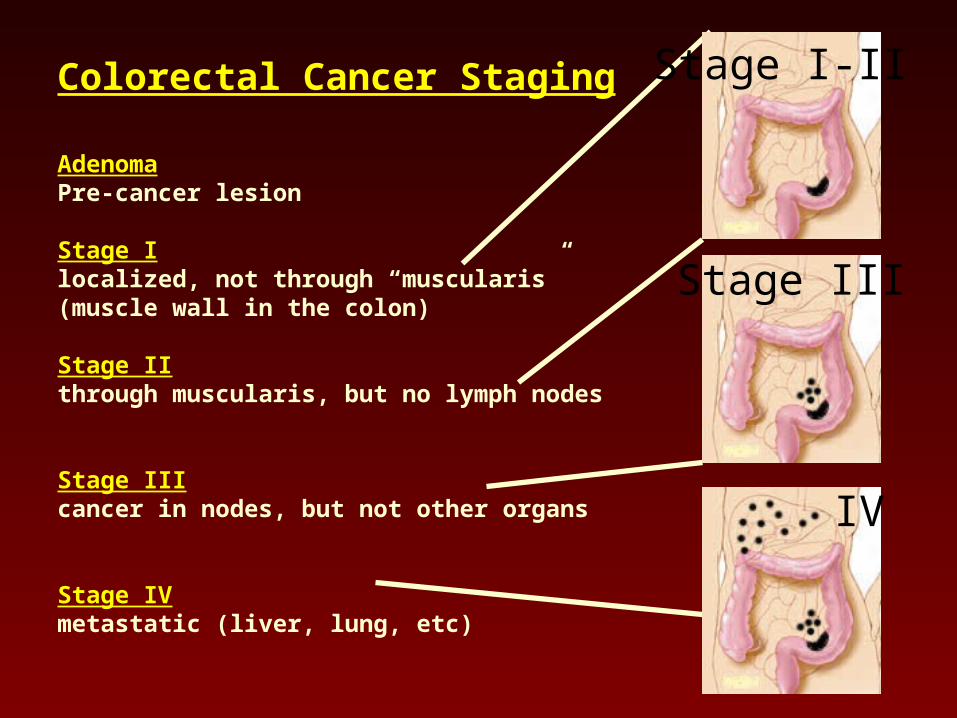
Colorectal Cancer Staging
AdenomaPre-cancer lesion
Stage Ilocalized, not through “muscularis”(muscle wall in the colon)
Stage IIthrough muscularis, but no lymph nodes
Stage IIIcancer in nodes, but not other organs
Stage IVmetastatic (liver, lung, etc)
Stage III
Stage I-II
IV
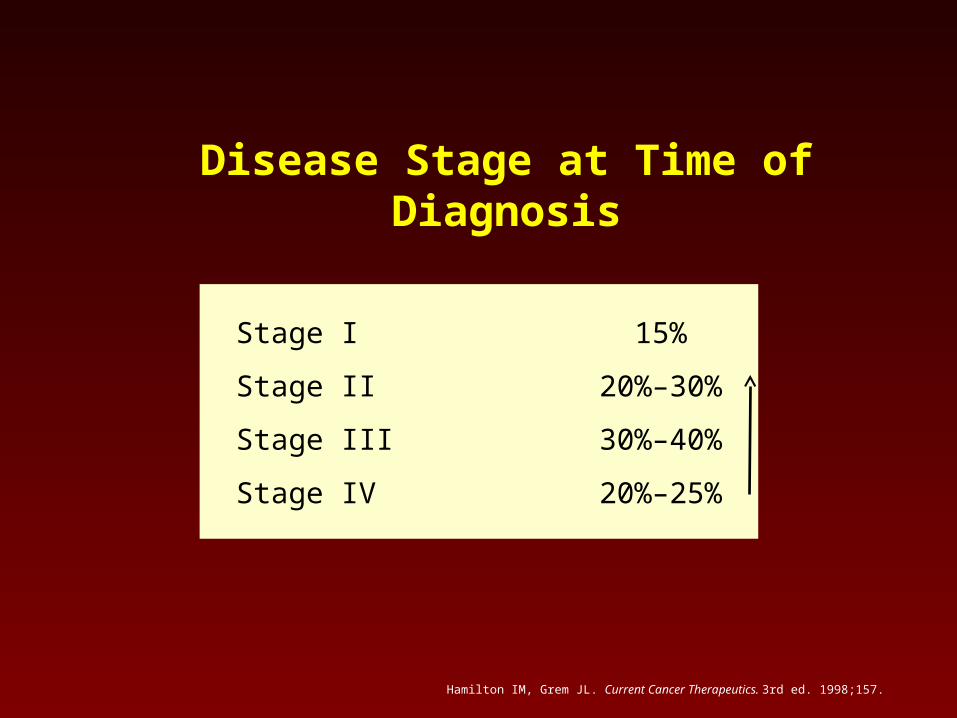
Stage I 15%
Stage II 20%–30%
Stage III 30%–40%
Stage IV 20%–25%
Disease Stage at Time of Diagnosis
Hamilton IM, Grem JL. Current Cancer Therapeutics. 3rd ed. 1998;157.
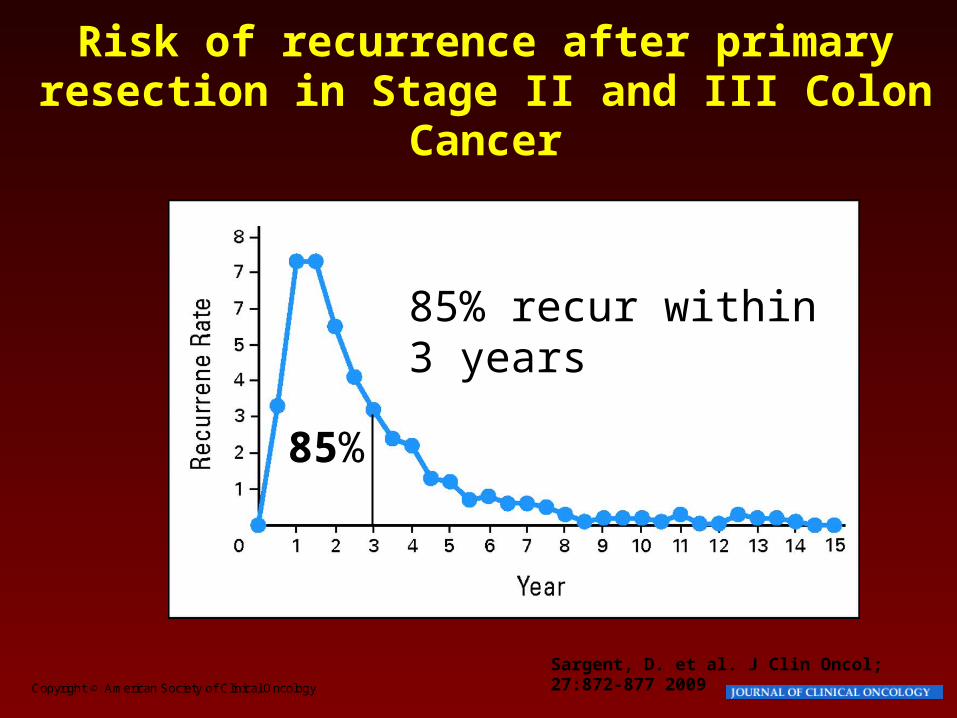
Copyright © American Society of Clinical Oncology
Sargent, D. et al. J Clin Oncol; 27:872-877 2009
Risk of recurrence after primary resection in Stage II and III Colon
Cancer
85% recur within 3 years
85%

Metastatic Disease
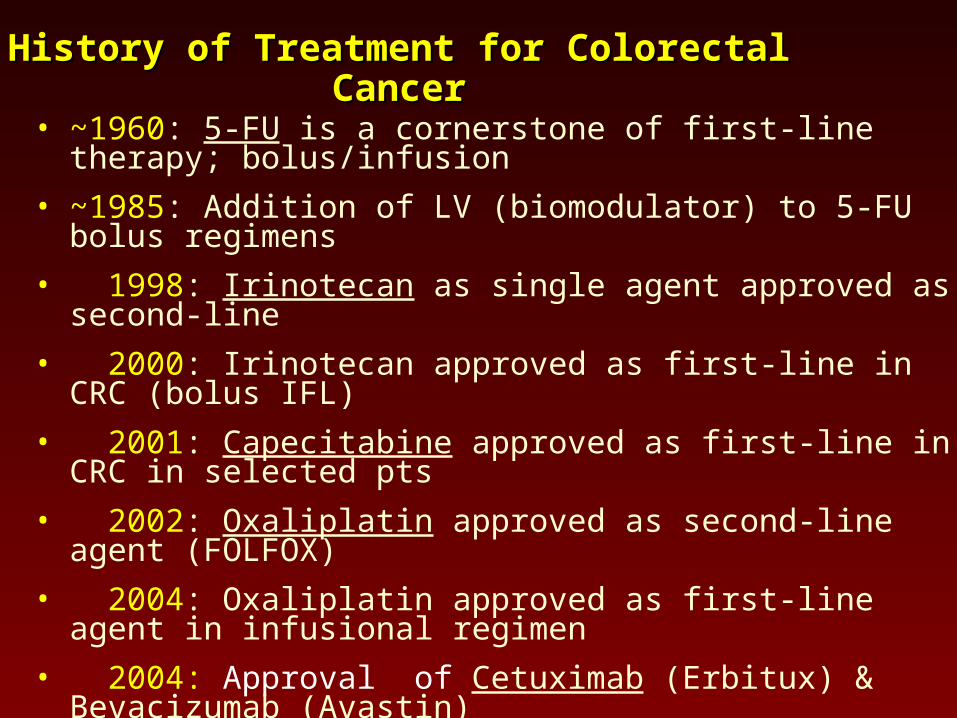
History of Treatment for Colorectal CancerHistory of Treatment for Colorectal Cancer
• ~1960: 5-FU is a cornerstone of first-line therapy; bolus/infusion
• ~1985: Addition of LV (biomodulator) to 5-FU bolus regimens
• 1998: Irinotecan as single agent approved as second-line
• 2000: Irinotecan approved as first-line in CRC (bolus IFL)
• 2001: Capecitabine approved as first-line in CRC in selected pts
• 2002: Oxaliplatin approved as second-line agent (FOLFOX)
• 2004: Oxaliplatin approved as first-line agent in infusional regimen
• 2004: Approval of Cetuximab (Erbitux) & Bevacizumab (Avastin)
• 2006: Approval of Panitumumab (Vectibix)
• 2008: KRAS mutations predict lack of benefit of EGFR mAb’s
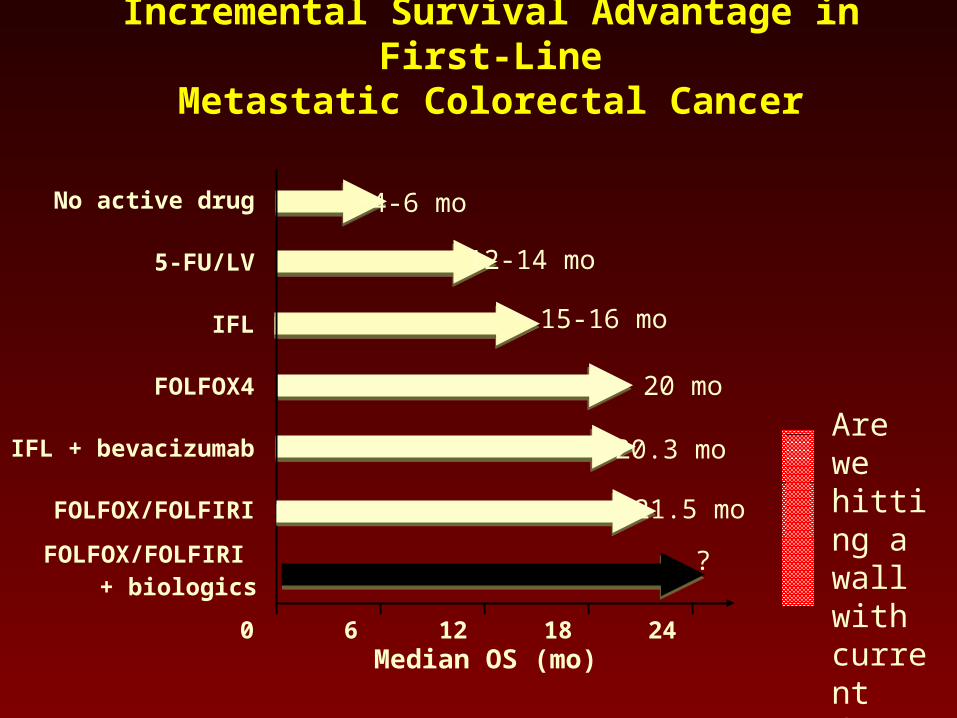
Incremental Survival Advantage in First-LineMetastatic Colorectal Cancer
No active drug
0 6 12 18 24Median OS (mo)
~4-6 mo
12-14 mo
~ 15-16 mo
20.3 mo
?
~ 20 mo
5-FU/LV
FOLFOX4
IFL + bevacizumab
IFL
21.5 moFOLFOX/FOLFIRI
FOLFOX/FOLFIRI
+ biologics
Are we hitting a wall with current drugs?
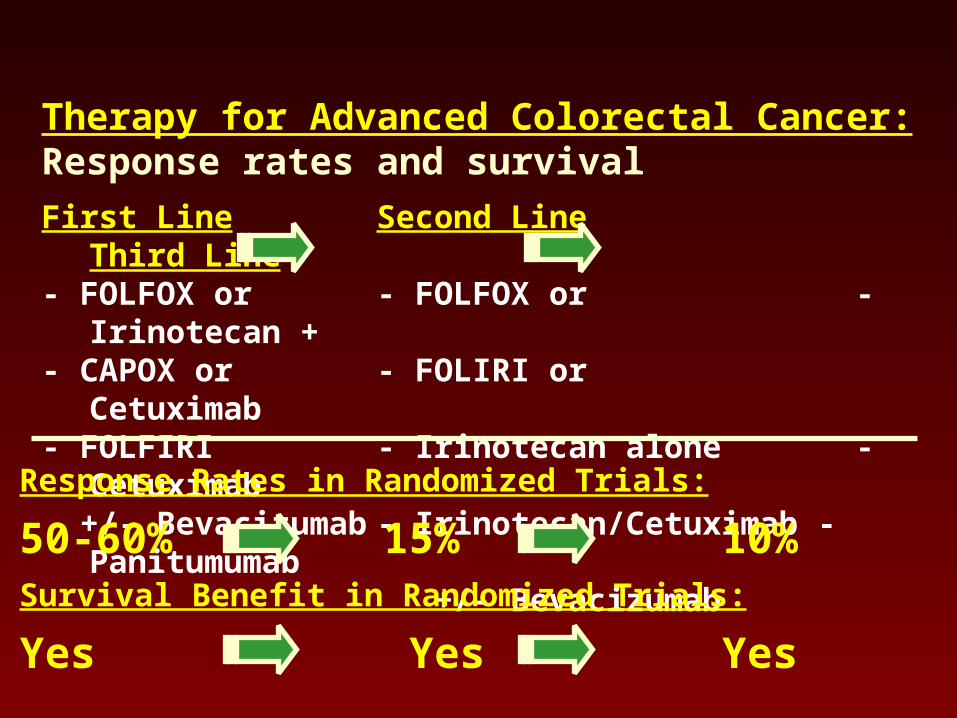
Therapy for Advanced Colorectal Cancer: Response rates and survival
First Line Second Line Third Line- FOLFOX or - FOLFOX or - Irinotecan +- CAPOX or - FOLIRI or Cetuximab - FOLFIRI - Irinotecan alone - Cetuximab +/- Bevacizumab - Irinotecan/Cetuximab - Panitumumab
+/- Bevacizumab
Response Rates in Randomized Trials:
50-60% 15% 10%Survival Benefit in Randomized Trials:
Yes Yes Yes
Epigenetics in CRC• Many genes have silenced expression due to epigenetic
changes
• Targeting epigenetically abnormal tumors may be more effective than targeting abnormal mutations in genes
• CRC may be uniquely appropriate for this strategy
• A subset of colon cancer have more gene promoter methylation
Ahuja et al.
Combination Epigenetic Therapy• First study of epigenetic therapy in CRC
• Primary Objective:
• To determine the preliminary efficacy via tumor shrinkage rate of the combination of 5-azacitadine and entinostat in patients with metastatic colorectal cancer
• Secondary Objective:
• To see what is happening in the tumor itself and circulating cells in blood before and after treatment with these drugs
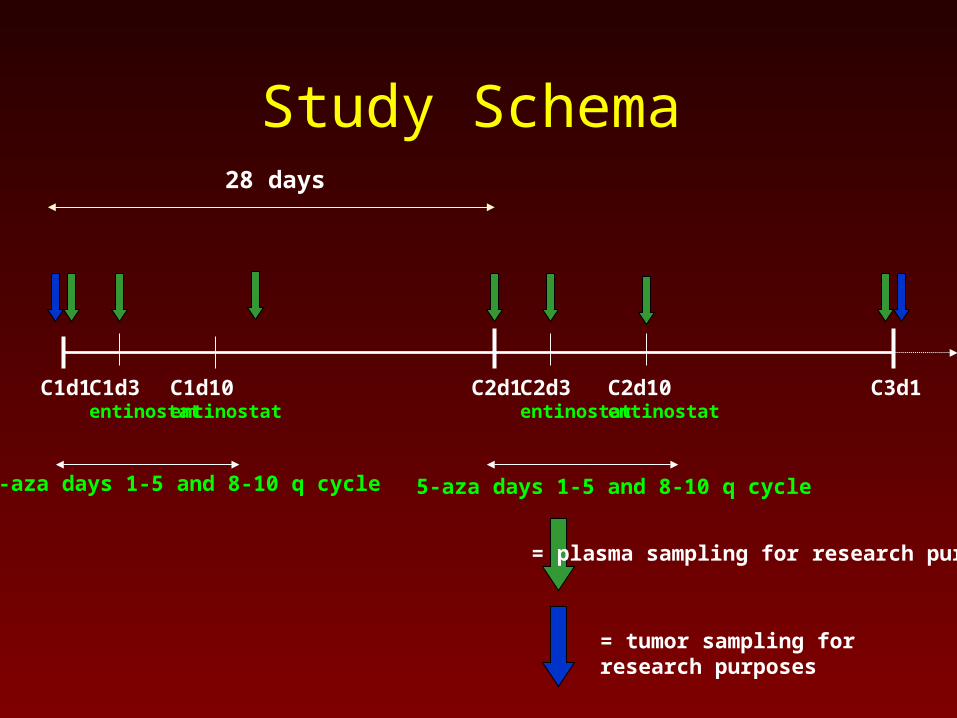
Study Schema28 days
C2d1C1d3entinostat
C1d1 C1d10entinostat
C2d3entinostat
C2d10entinostat
C3d1
= plasma sampling for research purposes
= tumor sampling for research purposes
5-aza days 1-5 and 8-10 q cycle5-aza days 1-5 and 8-10 q cycle
Ongoing and Upcoming Studies
• Lung Cancer– New schedule– Adjuvant treatment of early stage disease
• Breast– Same schedule in triple negative and hormone
resistant metastatic cancer
Conclusions
• Despite progress, colon cancer is a still leading source of death
• Epigenetic therapy offers a novel way to approach treating cancer, based on the abnormal gene expression seen in cancers compared to normal cells
• We are presently enrolling a trial of patients with late-stage colon cancer an treating them with epigenetic agents, 5-azacitidine and entinostat

BREAST CANCER
Epigenetics and breast cancer
• Multiple genes are methylated and thus silenced in breast cancer1
• ER, RAR beta, cyclin D, Twist, RASSF1A, and HIN-1
1 Pu RT. Mod Pathol 2003;16(11):1095-101.
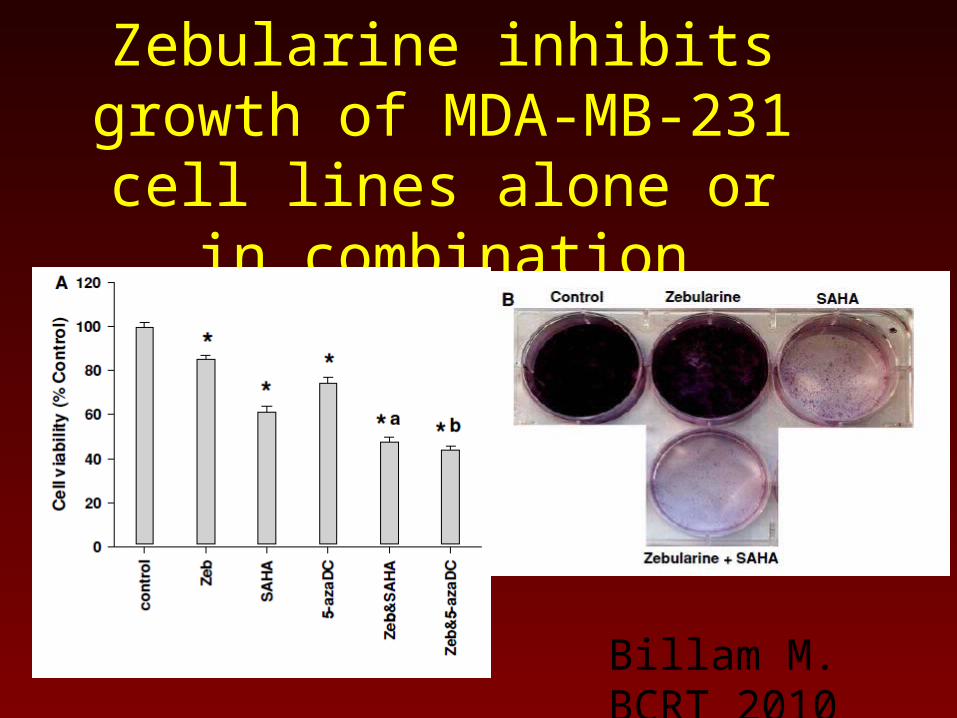
Zebularine inhibits growth of MDA-MB-231 cell lines alone
or in combination
Billam M. BCRT 2010
Clinical studies: Vorinostat in MBC
• Phase 2
SKCCC J0785/TBCRC 008A Multi-Institutional Randomized Phase II Study Evaluating Response and Surrogate Biomarkers to
Carboplatin and nab-Paclitaxel (CP) with or without Vorinostat (SAHA) in HER2- Negative Breast
Cancer
Principal Investigator: Vered Stearns, MDFellow: Roisin Connolly, MB.BCh
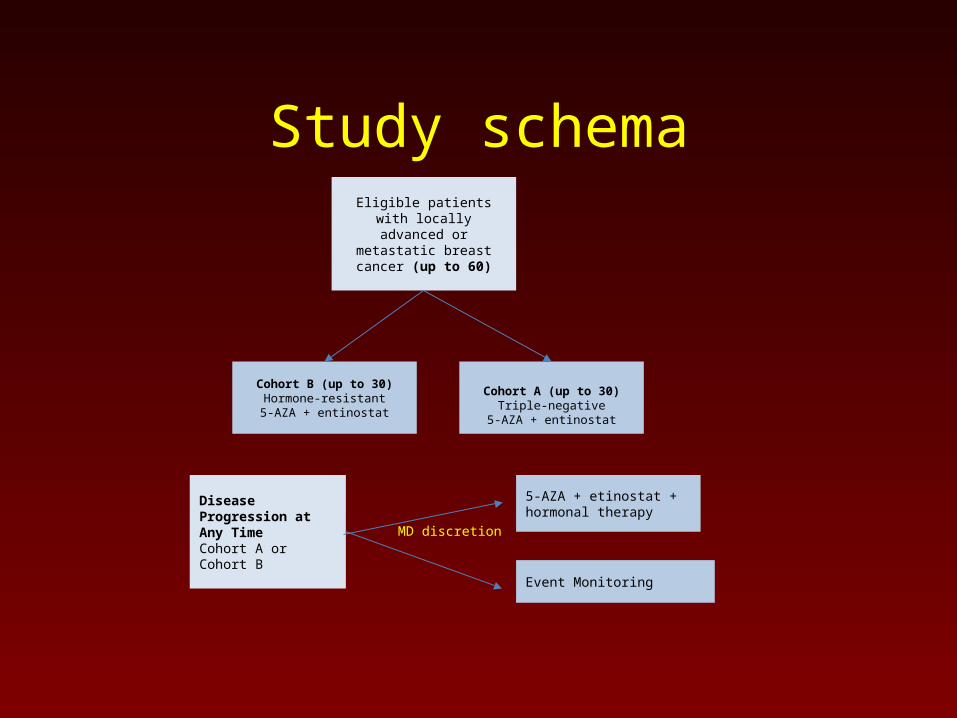
Eligible patients with locally advanced or metastatic breast cancer (up to 60)
Cohort A (up to 30)Triple-negative
5-AZA + entinostat
Cohort B (up to 30)Hormone-resistant5-AZA + entinostat
Disease Progression at Any Time Cohort A or Cohort B
5-AZA + etinostat + hormonal therapy
Event Monitoring
MD discretion
Study schema
Conclusions
• Epigenetics is a new way to look at cancer biology and therapy
• Ongoing trials in major tumor types in the metastatic setting
• Plans to move therapy into earlier stage disease may be even more successful
Acknowledgements
• First and foremost, our patients
• SU2C researchers
• Research support staff at all our institutions





























