Embed Size (px)
Citation preview

RET
Multiple Endocrine Neoplasia Type 2 (MEN2)
Brooke Martin
3/20/08

History of RET
• Discovered in 1985 by the transfection of NIH3T3 cells with DNA from T cell lymphoma cells
• RET stands for– rearranged during transfection
• Can have either loss of function or gain of function mutations

RET Properties
• Transmembrane protein and RTK• Mainly found in precursors of the urogenital
system and neural crest• Has 3 isoforms
– short (RET9), middle(RET43), and long (RET51)
• Homodimer– Also pairs with GFR (growth factor
receptor)α 1, 2, 3, and 4• Ligands
– GDNF (glial-derived neurotrophic factor), neurturin (NTN), persephin (PSP), and artemin

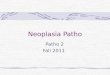
GDNF Family with Receptors SIGMA-ALDRICH

RET Properties Continued
•Gene found on long arm of chromosome 10 at 11.2•Gene has 21 exons•Cadherin part must bind with Ca2+ in order for RET to work•5 phosphotyrosine residues
–2 more in long isoform

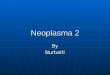
Protein Structures of RET
Unphosphorylated
Phosphorylated
J. Biol. Chem. v281, p.33577-33587

What Does RET Do Normally?
• Helps with kidney development and enteric nervous system
• Also implicated in cell differentiation and apoptosis

Knockout Mice
• Knockouts had no neurons in the gut, superior cervical ganglia, no kidneys at all or malformed and malfunctioning
• RET null mutation die shortly after birth
• No endocrine organs affected in MEN 2
• Heterozygotes have no apparent defects

MEN 2-multiple endocrine neoplasia type 2
• Inherited form of cancer and very rare• First to be discovered in 1993 that MEN 2 was
caused by germline mutations• Three subtypes
– MEN 2A and MEN 2B– Familial medullary thyroid carcinoma (FMTC)
• Autosomal dominant• RET constitutively active • Endocrine glands affected
– Adrenal, parathyroid, and thyroid• Gain of function mutations

MEN 2A
Codons effected 630, 634,(exon 11) or 609, 611, 618, 620 (exon10)
Mutation to 634 worst90% of MEN 2A have this. 50% have change from a cysteine to argenine
How RET is activeLigand-independent dimerization, loss of disulfide bond between dimers
Tumors developed Pheochromocytoma, MTC
Incidence100% get MTC, 50% pheochromocytoma, 15-30% parathyroid hyperplasia

MEN 2B
Codons affected
918, change from methionine to threonine (exon 16)883 in TK domain but rare (5%)
Most aggressive of the three
95% have the M918T mutation
What keeps RET active
Made to look unlike an RTK from mutation, changes autophosphorylation
Tumors developed and incidence
100% MTC, 50% pheochromocytoma, very rare parathyroid hyperplasia
Pattern of phosphorylation
The proteins phosphorylated differs form MEN 2A

FMTC
• Have the same mutations as 2A in extracellular domain but also can be in TK domain at 768, 790, 791,(exon 13); 804, 844,(exon 14); or 891 (exon15)
• Have mild C cell disease• Low transforming activity can
predispose to FMTC rather than MEN 2A

Treatment and Testing
• Thyroidectomy– Before age 6 or 6-12 depending on mutation– If MEN 2B, needed before a year old– Have to take thyroid for the rest of life
• Chemotherapy not effective• Microarray (best)• Direct sequencing or single-strand
conformational polymorphism• Drugs being tested to disrupt RET
kinase activity– Needs a higher concentration though

Questions?