Embed Size (px)
Citation preview

جو ےسنامےكاهللاربان ہم
ےهواالےكرنرحماور
الرحيم الرحمن اهللا بسم
ا ڑب
24-11-2008
Neoplasia
2
Differentiation refers to the extent to which neoplastic cells resemble comparable normal cells, both morphologically and functionally.
Anaplasia is lack of differentiation
3
Morphologic Features of Anaplasia, Lack of Differentiation
• Pleomorphism: (pleo = more) (Variation in size & shape of the cells and nuclei) Some cells/nuclei may be many times larger compared to their neighbors
and some other may be small and primitive.
• Abnormal nuclear morphology: The nuclei contain an abundance of DNA, are hyperchromatic and
larger and show higher nucleo-cytoplasmic ratio. Nuclei vary in shape and chromatin is clumped along the nuclear membrane. Nucleoli are enlarged and prominent.
• Mitoses: Atypical and bizarre mitotic figures with multipolar spindles are features of anaplasia. (Increased number of normal mitotic figures are seen in bone marrow and hyperplastic tissue.) 4
• Loss of polarity: Orientation of anaplastic cells is markedly disturbed. Sheets and large masses of tumor cells grow in anarchic, disorganized fashion.
• Tumor giant cells: Cancer giant cells are common in some malignant growth. These have large
hyperchromatic pleomorphic nuclei varying in size and shape. Cancer giant cells may have single or multiple nuclei. (Macrophage derived multinucleated
Langhans and foreign body giant cells have normal nuclei).
• Areas of ischemic necrosis may be seen in the malignant growth as blood supply falls short of the need for rapid growth.
Morphologic Features of Anaplasia, continued
5
• Poorly differentiated anaplastic tumors also demonstrate a total disarray of tissue architecture as in
anaplastic cervical malignancy, the normal orientation of squamous epithelial cells relative to each other is lost.
• Well differentiated tumors, whether benign or malignant, tend to retain the functional characteristics of their normal counterparts. Thus there may be hormone production by endocrine tumors or keratinproduction by squamous epithelial tumors.
6
Dysplasia• Dysplasia literally means “disordered growth”
• Dysplasia is disorderly but non-neoplastic growth.
• It is usually encountered in epithelia (usually in ut. cervix)
• Pleomorphism, hyperchromasia, loss of normal orientation and mitotic activity may occur short of malignancy. The lesion is reversible if the cause is removed. Dysplasia may be mild, moderate or severe.
• When dysplastic changes are marked and involves the entire thickness of the epithelium, the lesion is considered a preinvasive intraepithelial neoplasm (Carcinoma in situ).
• Cervical Intraepithelial Neoplasia (CIN) may be described as CIN I, CIN II, CIN III (Carcinoma in situ)
7
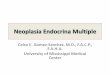
BA
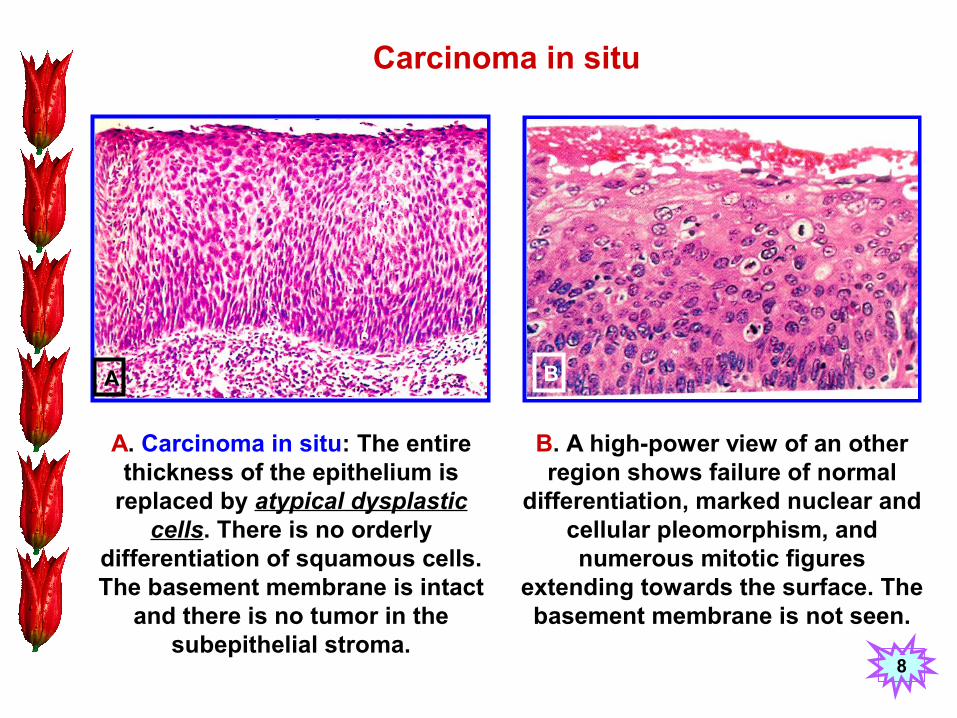
A. Carcinoma in situ: The entire thickness of the epithelium is
replaced by atypical dysplastic cells. There is no orderly
differentiation of squamous cells. The basement membrane is intact
and there is no tumor in the subepithelial stroma.
B. A high-power view of an other region shows failure of normal
differentiation, marked nuclear and cellular pleomorphism, and numerous mitotic figures
extending towards the surface. The basement membrane is not seen.
Carcinoma in situ
8
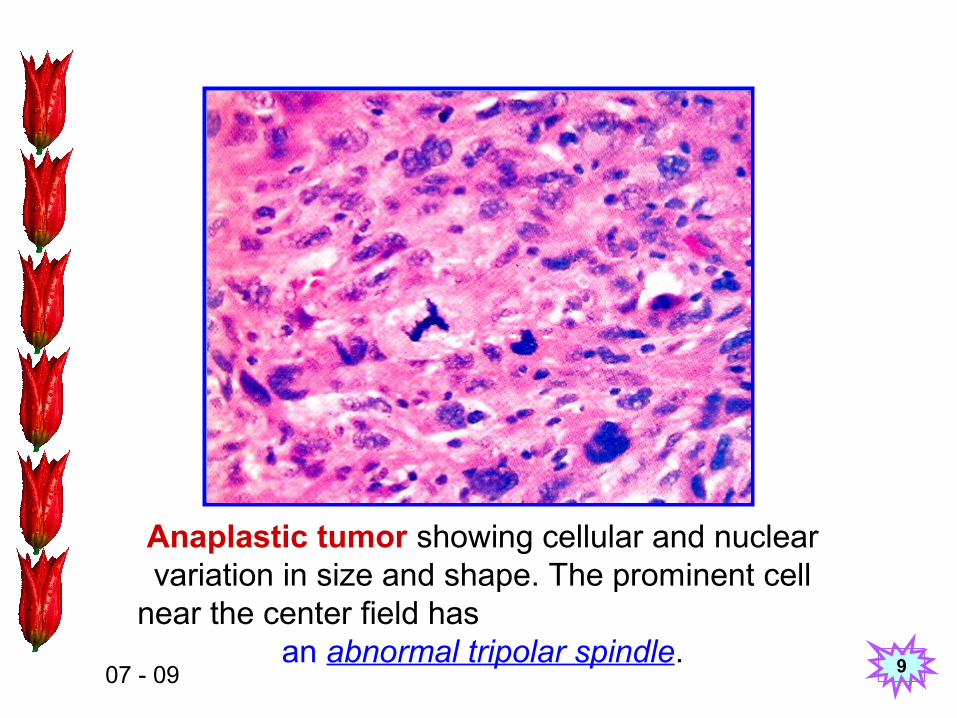
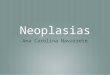
Anaplastic tumor showing cellular and nuclear variation in size and shape. The prominent cell
near the center field has an abnormal tripolar spindle.
07 - 09 9
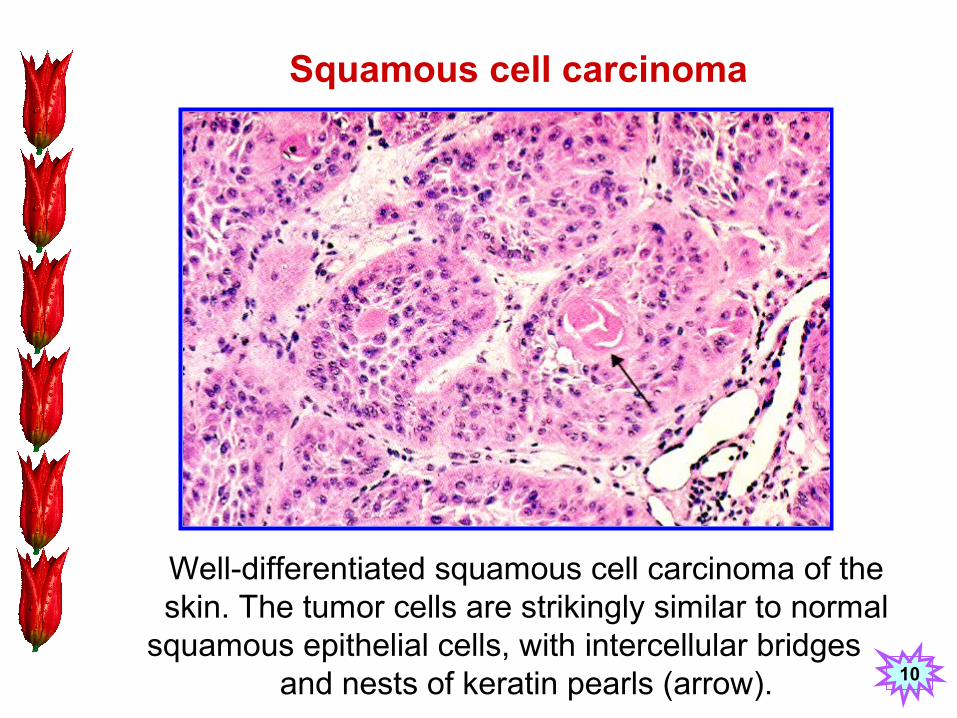
Squamous cell carcinoma
Well-differentiated squamous cell carcinoma of the skin. The tumor cells are strikingly similar to normal
squamous epithelial cells, with intercellular bridges and nests of keratin pearls (arrow). 10
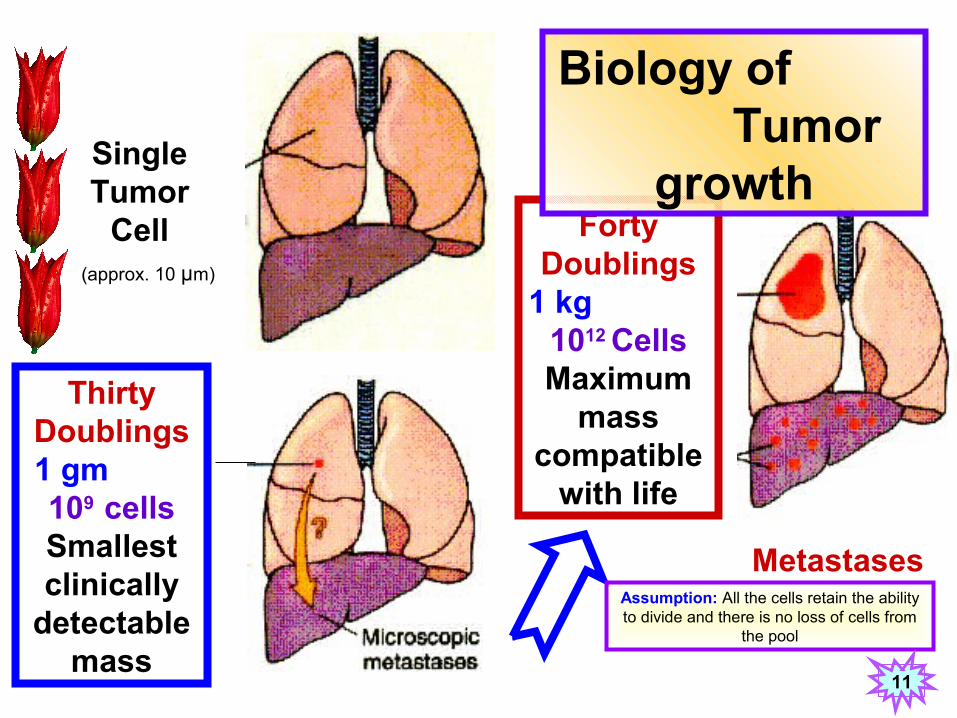
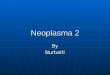
Single Tumor
Cell Forty Doublings
1 kg 1012 Cells Maximum
mass compatible
with life
Metastases
Biology of Tumor
growth
Thirty Doublings 1 gm 109 cells Smallest clinically
detectable mass
(approx. 10 μm)
Assumption: All the cells retain the ability to divide and there is no loss of cells from
the pool
11
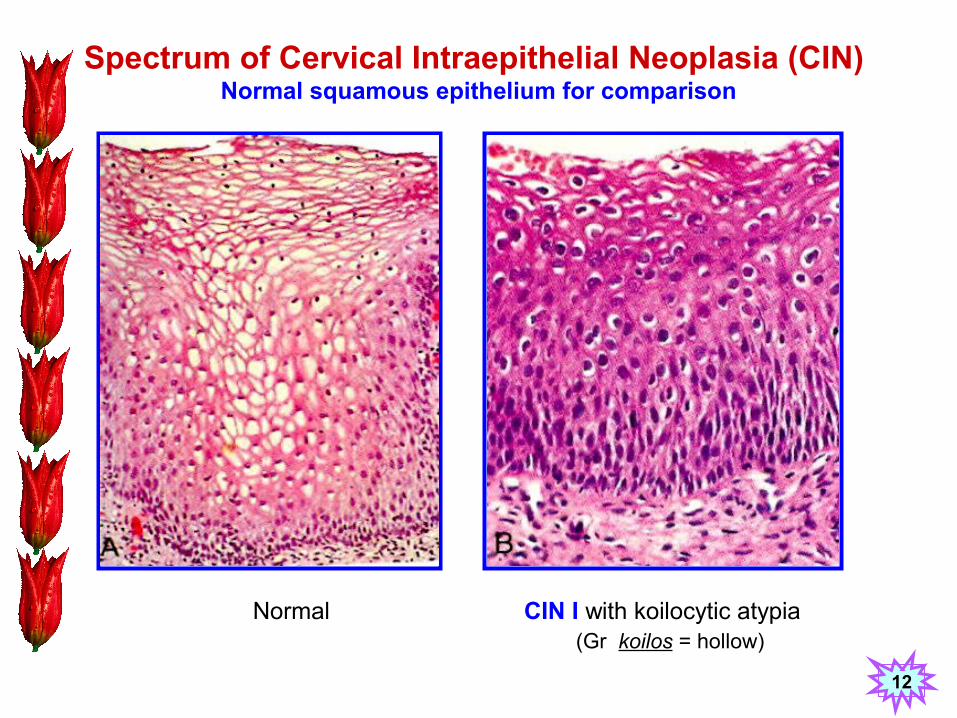
Spectrum of Cervical Intraepithelial Neoplasia (CIN) Normal squamous epithelium for comparison
Normal CIN I with koilocytic atypia(Gr koilos = hollow)
12
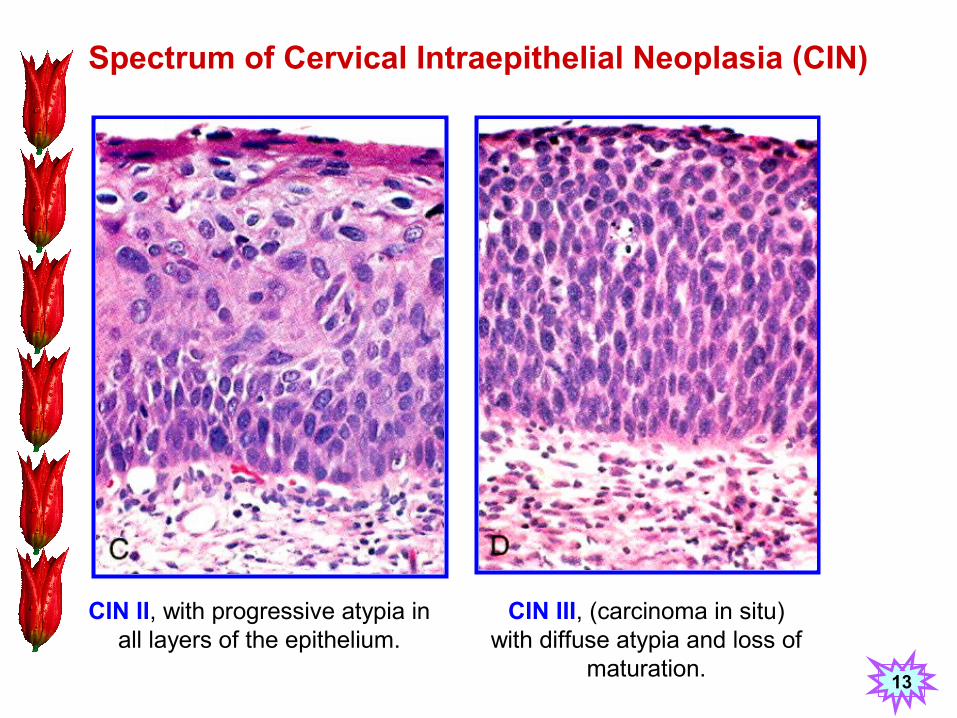
Spectrum of Cervical Intraepithelial Neoplasia (CIN)
CIN II, with progressive atypia in all layers of the epithelium.
CIN III, (carcinoma in situ) with diffuse atypia and loss of
maturation.13
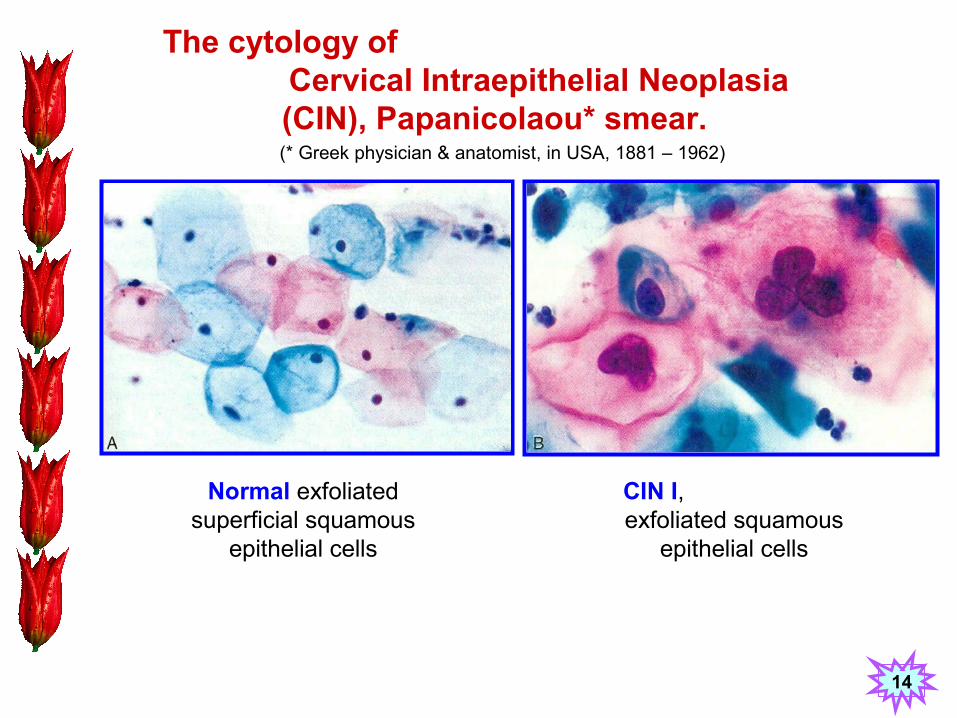
The cytology of Cervical Intraepithelial Neoplasia
(CIN), Papanicolaou* smear.
Normal exfoliated superficial squamous
epithelial cells
CIN I, exfoliated squamous
epithelial cells
(* Greek physician & anatomist, in USA, 1881 – 1962)
14
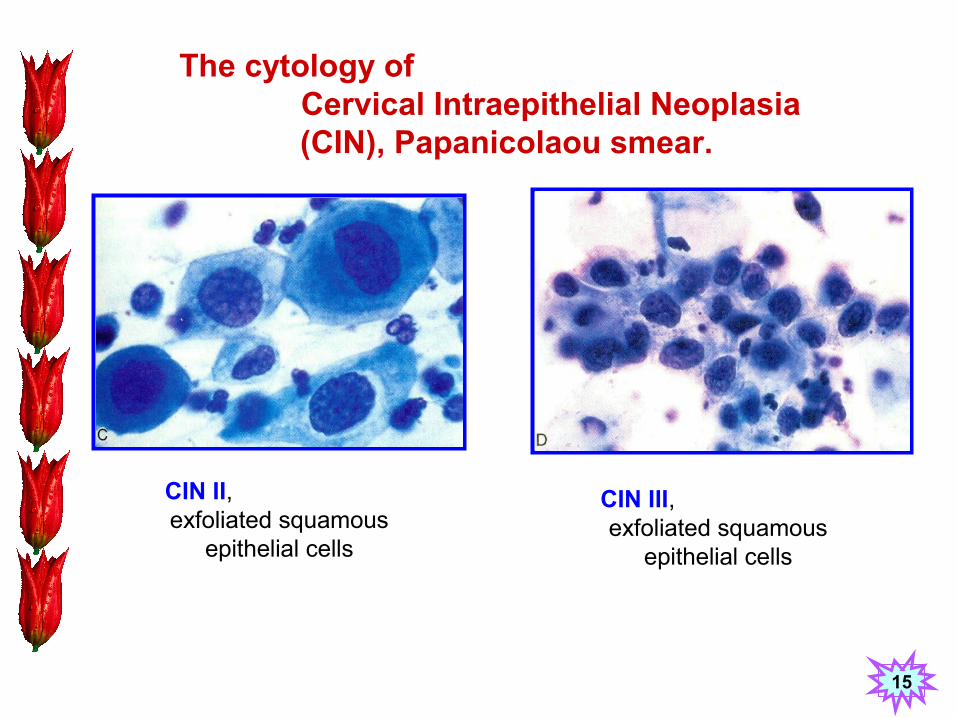
The cytology of Cervical Intraepithelial Neoplasia
(CIN), Papanicolaou smear.
CIN III, exfoliated squamous
epithelial cells
CIN II, exfoliated squamous
epithelial cells
15
Spread of Tumors
16
Dissemination of cancer may occur through one of three pathways:
1. Lymphatic spread
2. Hematogenous spread
3. Seeding of body cavities and surface
• Seeding of body cavities & surfaces: This occurs when carcinoma penetrate to reach the surface of a viscus, most often peritoneal cavity but also pleural, pericardial, subarachnoid and joint space. Such seeding is usually seen in carcinoma of the ovaries coating the surface of the peritoneum. Appendiceal mucinous carcinoma may spread to peritoneum forming pseudomyxoma peritonei.
17
• Lymphatic Spread: is the most common pathway for initial spread of carcinomas. Sarcomas may also use this route. The pattern of lymph node involvement follows the natural routes of lymphatic drainage.
Sentinal node: The first node in a regional lymphatic basin that receives lymph flow from a primary tumor.
In many cases the regional nodes serve as effective barrier for some time.
Drainage of tumor cell debris and/or tumor antigens also induces reactive changes in the nodes with their enlargement.
Thus regional node enlargement does not always mean dissemination of the primary lesion.
• Hematogenous Spread: is typical of sarcomas but is also seen with carcinomas.
◘ The liver and the lungs are most frequently involved secondarily in hematogenous dissemination.
All portal area drainage flows to the liver and
All caval blood flows to the lungs.
◘ Cancers arising close to the vertebral column often embolize through paravertebral vascular
plexus (Vertebral metastasis from prostate and thyroid).
◘ Certain cancers may invade veins. Renal cell carcinoma and hepatocellular carcinoma may
involve branches of renal vein and portal / hepatic veins respectively.
18
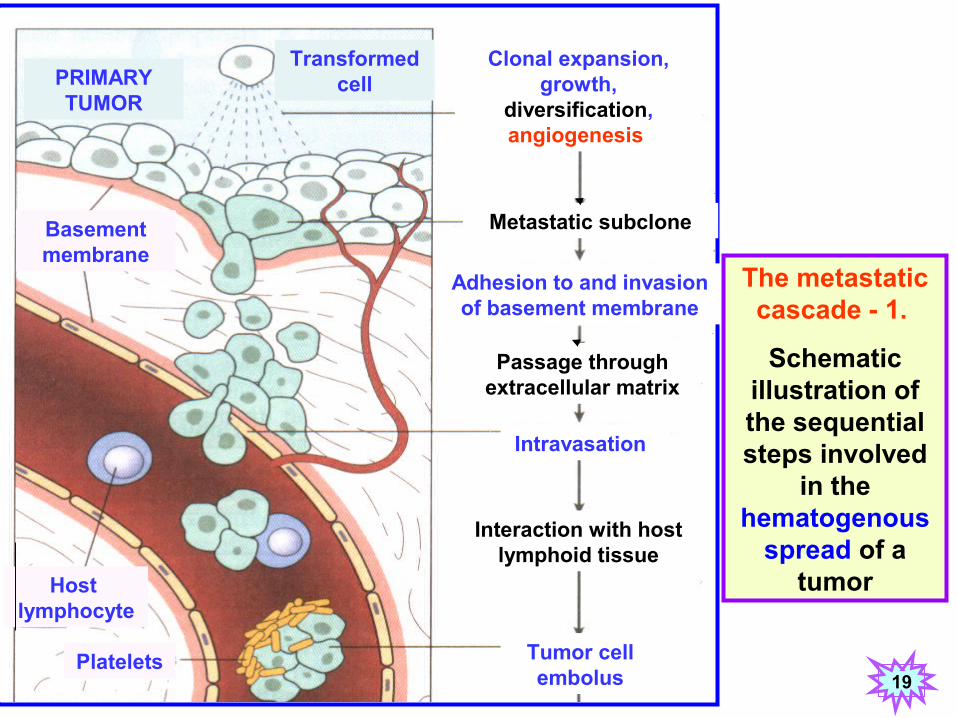
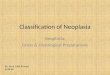
Clonal expansion, growth,
diversification, angiogenesis
PRIMARY TUMOR
Transformed cell
Metastatic subclone
Adhesion to and invasion of basement membrane
Passage through extracellular matrix
Intravasation
Interaction with host lymphoid tissue
Tumor cell embolus
Basement membrane
Host lymphocyte
Platelets
The metastatic cascade - 1.
Schematic illustration of the sequential steps involved
in the hematogenous
spread of a tumor
19
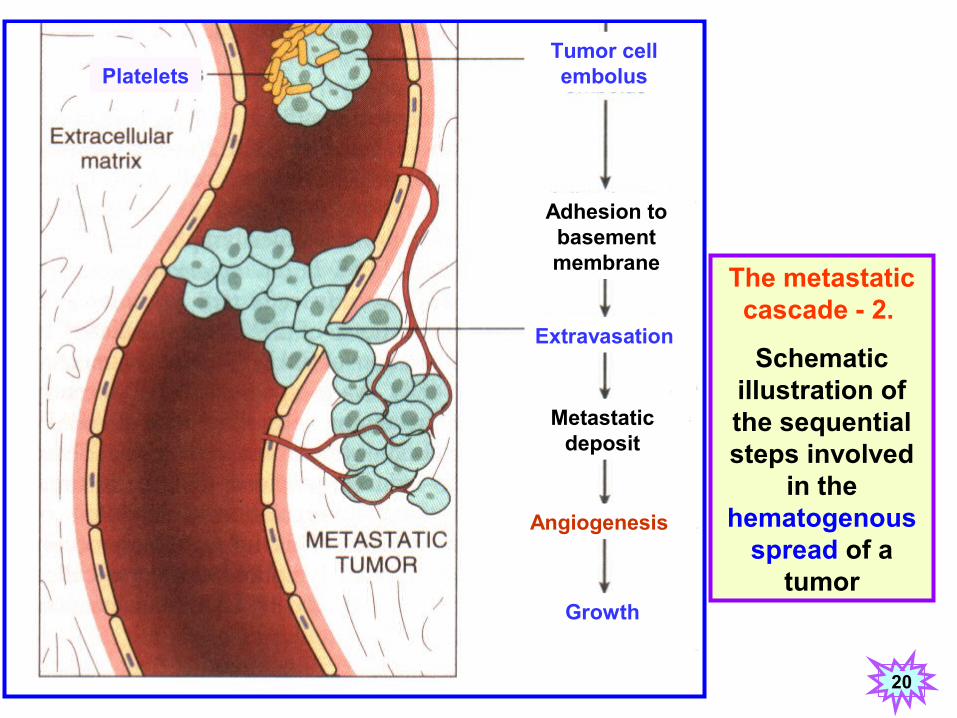
The metastatic cascade - 2.
Schematic illustration of the sequential steps involved
in the hematogenous
spread of a tumor
PlateletsTumor cell embolus
Adhesion to basement membrane
Extravasation
Metastatic deposit
Angiogenesis
Growth
20
شكريه