Embed Size (px)
Citation preview
- ACTA OPHTHALMOLOGICA SCANDINAVICA 1996
Results of treatment of amblyopia with a screening program for early detection Gunnar Lennerstrand and Agneta Rydberg
Department of Ophthalmology, Karolinska Institute, Huddinge University Hospital, Huddinge, Sweden
ABSTRACT. The Swedish program for early intervention in children with visual dysfunction, was evaluated with respect to the results of treat- ment of amblyopia. One hundred and seventy-two amblyopic children were examined before and at 6,12 and 18 months after the beginning of treatment. The mean visual acuity of the amblyopic eye was 0.76 and the mean ratio of visual acuity between the two eyes was 0.75 or better in all types of amblyopia. Children with strabismic amblyopia showed slightly poorer treatment results than the other types, in spite of the fact that their amblyopia had been detected earlier than the others. The results at- test to the importance of careful screening of monocular visual acuity in all children, which in Sweden occurs at 4 years of age. This provides a good basis for detection and treatment of amblyopia. Only one child in the group had a visual acuity at 0.2 and may therefore be at risk for visual handicap if the better eye should be lost later in life.
Key words: amblyopia - strabismus - anisometropia - refractive error - treatment results - vis- ual acuity - screening program - testing at 4 years of age.
Acta Ophthalmol. Scand. 1996: 74 (Suppl219): 42-45
mblyopia is defined as reduced vis- A ual acuity without visible damage to structures in the eye or the visual system (von Noorden 1990). It is one of the most common conditions in pediatric ophthalmology, and the de- tection and treatment of amblyopia is of great concern to pediatricians and ophthalmologists.
Amblyopia is regarded as a devel- opmental abnormality of the visual functions represented in the visual cor- tex, particularly form vision and bino- cular vision (Campos 1995). The period during which these abnor- malities may occur extends from about 4-6 months of age until about 8-10 years of age, the so called plastic period of visual development.
The results of amblyopia treatment are usually excellent if the condition is discovered at an early age, and treat- ment is instituted without delay and with good compliance of the child and the parents (Oliver et al. 1986; Lithan- der & Sjostrand 1991; Unwin 1991). The results of treatment are regarded very poor after 8 years of age (Campos 1995).
In order to discover amblyopia early, different screening programs have been introduced (Lennerstrand et al. 1995). The most extensive screen- ing programs with the highest attend- ence rates of the child population, are the ones used in the Scandinavian countries. In Sweden the screening consists of two parts and is carried out
at the regular visits that the children make to the Child Health Care Cen- ters. The attendance rates of these vi- sits are very hgh and the screening in- volves almost all (99%) of the popula- tion. The first part of screening consists of general inspection of the eyes for structural abnormalities and ocular motility disorders, such as strabismus and nystagmus. When ocular and vis- ual dysfunction is suspected, also from the reports of the parents, the child is referred to the nearest department of pediatric ophthalmology for further evaluation. The second part of the screening program consists of mono- cular visual acuity screening at the age of 4 years.
Children who fail screening, after 1 or 2 retests, are immediately referred to the pediatric ophthalmology depart- ments. Although the system is con- sidered to function well, the results of amblyopia treatment in a population of amblyopic children detected by the screening system have not yet been properly reported.
Material and Methods The children included in this study were 172 consecutive patients with amblyopia referred from the Child Health Care Centers to two depart- ments of pediatric ophthalmology in Stockholm during a period of about one year.
All children had orthoptic and oph- thalmologic examinations, and their cycloplegic refraction was determined. Visual acuity was tested, when pos-
42
ACTA OPHTHALMOLOGICA SCANDINAVICA 1996 -
Number of patients
40
0 1 2
Number of patients
30 1 group1
group2 M S H A
0 S+A
B R 20
10
0 vears
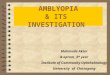
bars) and group 2 (filled bars). Fig. 1. The age distribution at start of treatment for group 1 (open Fig. 2. Age distribution of children in group 1, separated into am-
blyopia types: strabismic amblyopia (S), anisometropic amblyopia (A), combined amblyopia (S +A), refractive amblyopia (R).
sible, with the HVOT-test (Hedin et al. 1980). Treatment was instituted as soon as the diagnosis of amblyopia was made, and the treatment consisted of glasses and/or occlusion. The treat- ment was prescribed according to the practice of the departments that are very similar to each other.
At follow-up visits the visual acuity was measured if possible, the oculo- motor and binocular functions were evaluated, and cycloplegic refraction was performed when needed. The re- sults obtained after treatment for about 6, 12 and 18 months have been further analyzed, although visits were generally more frequent than at these intervals. The patients were divided
into two groups. Group 1 consisted of all the children, and group 2 of only those children who could already be tested for visual acuity at the start of treatment. The age distribution at the start of treatment in each group is shown in Fig. 1.
Results 1. Types of amblyopia The underlying cause of the amblyopia was determined from knowledge of the type and characteristics of the strabis- mus and of the refractive error of each eye. The type of amblyopia was divided into strabismic (S), anisometropic (A),
combined strabismic and anisome- tropic (S + A) and purely refractive (R). Strabismus was of the manifest or inter- mittent type. Anisometropia was defined as a difference in refraction be- tween eyes of 2D and more of spherical value and/or 1D or more of astigmatic value. Patients with appreciable spheri- cal and/or astigmatic refractive error but no anisometropia or strabismus were considered having refractive am- blyopia. The age distribution of child- ren with different types of amblyopia in group 1 is shown in Fig. 2. Generally the children with strabismic amblyopia and with combined strabismic and anisometropic amblyopia were dis- covered earlier and their treatment
Visual amblyopic eye Ratio
L O 1 acuity
$ 9 0 1 non-amblyopic eye
0 6 12 18 months
Treatment period
0 6 12 18 months Treatment period
Fig. 3. Mean values of visual acuity in the amblyopic and the non-amblyopic eyes of children in group 1 at different times of treatment.
Fig. 4. Mean ratios of visual acuity for the amblyopichon-amblyopic eye at different times during treatment in Group 1, in strabismic (S), anisome- tropic (A), combined (S + A) and refractive (R) amblyopia.
43 -
- ACTA OPHTHALMOLOGICA SCANDINAVICA 1996
g 1 . 0 -
0 . 8 :
.- E
z m 0.6- - 3 0 .4 - - 1 0 . 2 - 5
0 , O l
A Strablsmic amblyopia B Anisometropic amblyopia
u) 5 1 , o - 0 0. 0 0 0 0
5! 0 .
0 . 0 0 0 0 0 00 0
0 0 0 00 0 0 0 0 . 6 1 0 0 0 0. : goo O 0 .
- 0 5 0 , 6 -
0 0 0 j 0 * 4 - 0 ,- 2.
- f 0 . 2 -
5 . I . I . I . , ' I ' 7 o , o , . I . a I ' I ' 1 ' I
C Strsblsmic and anisomatropic amblyopia D Refractive amblyopia
8 8 8 . 8
B 8
8
0 , O - l , I . I . I . I . I ' I 0.0 0 .2 0.4 0 , 8 0.8 1,0 1.2 0 , O 0 .2 0.4 0.6 0 , 8 1,0 1,2
Visual acuity at 0 months Visual acuity at 0 months
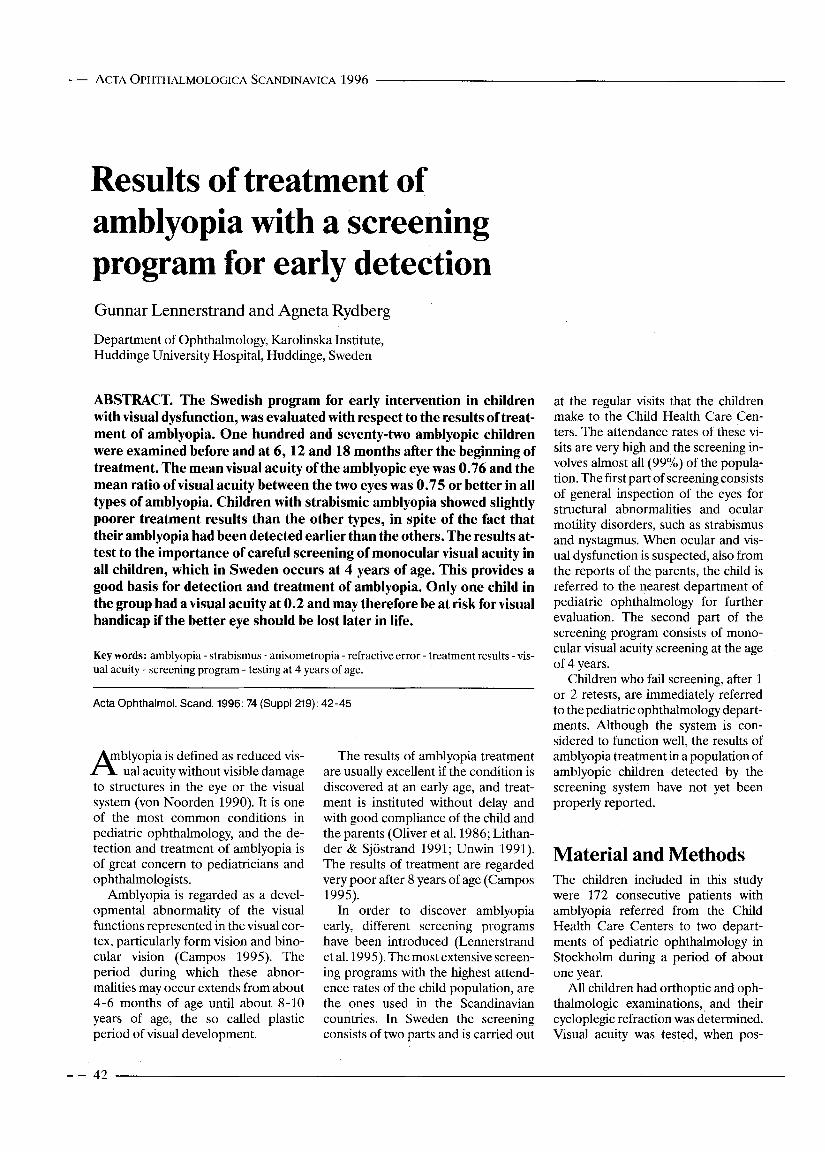
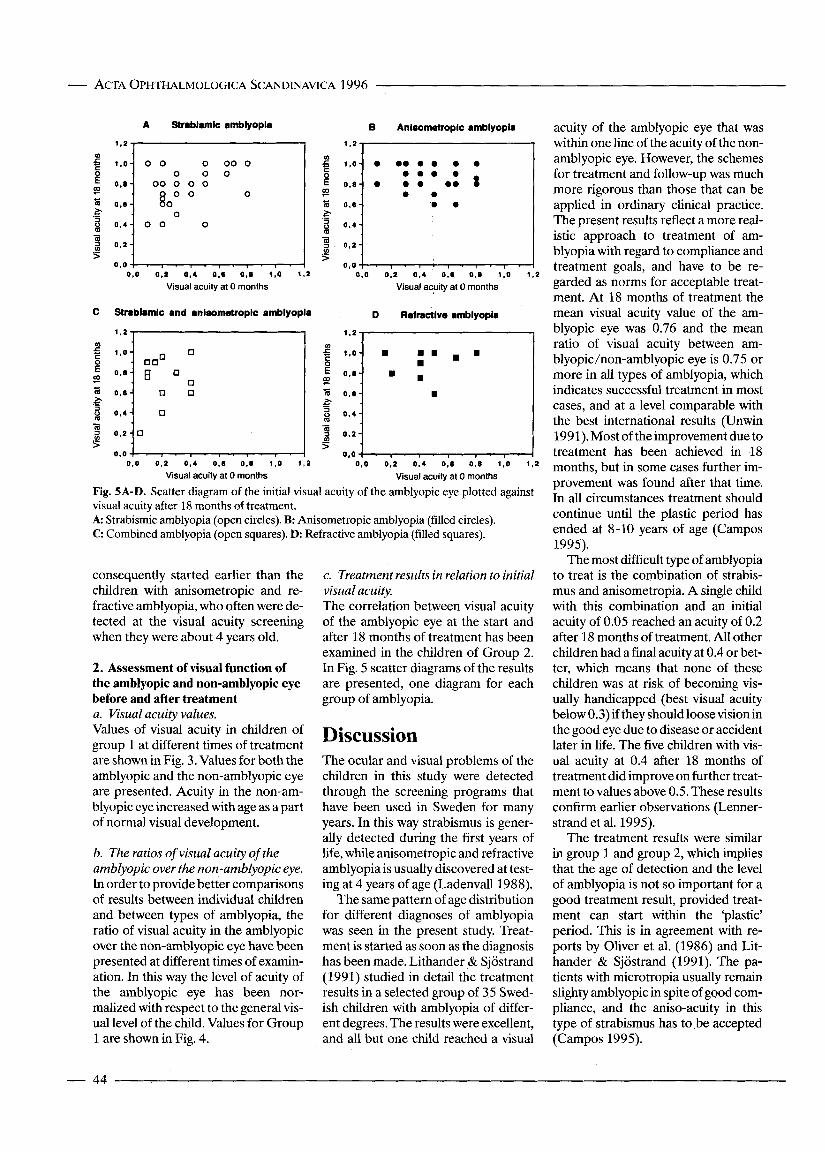
Fig. 5A-D. Scatter diagram of the initial visual acuity of the amblyopic eye plotted against visual acuity after 18 months of treatment. A: Strabismic amblyopia (open circles). B: Anisometropic amblyopia (filled circles). C: Combined amblyopia (open squares). D: Refractive amblyopia (filled squares).
consequently started earlier than the children with anisometropic and re- fractive amblyopia, who often were de- tected at the visual acuity screening when they were about 4 years old.
2. Assessment of visual function of the amblyopic and non-amblyopic eye before and after treatment a. Visual acuity values.
c. Treatment results in relation to initial visual acuity. The correlation between visual acuity of the amblyopic eye at the start and after 18 months of treatment has been examined in the children of Group 2. In Fig. 5 scatter diagrams of the results are presented, one diagram for each group of amblyopia.
Discussion Values of visual acuity in children of group 1 at different times of treatment are shown in Fig. 3. Values for both the amblyopic and the non-amblyopic eye are presented. Acuity in the non-am- blyopic eye increased with age as a part of normal visual development.
b. The ratios of visual acuity of the amblyopic over the non-amblyopic eye. In order to provide better comparisons of results between individual children and between types of amblyopia, the ratio of visual acuity in the amblyopic over the non-amblyopic eye have been presented at different times of examin- ation. In this way the level of acuity of the amblyopic eye has been nor- malized with respect to the general vis- ual level of the chdd. Values for Group 1 are shown in Fig. 4.
The ocular and visual problems of the children in this study were detected through the screening programs that have been used in Sweden for many years. In this way strabismus is gener- ally detected during the first years of life, while anisometropic and refractive amblyopia is usually discovered at test- ing at 4 years of age (Ladenvalll988).
The same pattern of age distribution for different diagnoses of amblyopia was seen in the present study. Treat- ment is started as soon as the diagnosis has been made. Lithander & Sjostrand (1991) studied in detail the treatment results in a selected group of 35 Swed- ish children with amblyopia of differ- ent degrees. The results were excellent, and all but one child reached a visual
acuity of the amblyopic eye that was within one line of the acuity of the non- amblyopic eye. However, the schemes for treatment and follow-up was much more rigorous than those that can be applied in ordinary clinical practice. The present results reflect a more real- istic approach to treatment of am- blyopia with regard to compliance and treatment goals, and have to be re- garded as norms for acceptable treat- ment. At 18 months of treatment the mean visual acuity value of the am- blyopic eye was 0.76 and the mean ratio of visual acuity between am- blyopichon-amblyopic eye is 0.75 or more in all types of amblyopia, whch indicates successful treatment in most cases, and at a level comparable with the best international results (Unwin 1991). Most of the improvement due to treatment has been achieved in 18 months, but in some cases further im- provement was found after that time. In all circumstances treatment should continue until the plastic period has ended at 8-10 years of age (Campos 1995).
The most difficult type of amblyopia to treat is the combination of strabis- mus and anisometropia. A single child with this combination and an initial acuity of 0.05 reached an acuity of 0.2 after 18 months of treatment. All other children had a final acuity at 0.4 or bet- ter, which means that none of these children was at risk of becoming vis- ually handicapped (best visual acuity below 0.3) if they should loose vision in the good eye due to disease or accident later in life. The five children with vis- ual acuity at 0.4 after 18 months of treatment did improve on further treat- ment to values above 0.5. These results confirm earlier observations (Lenner- strand et al. 1995).
The treatment results were similar in group 1 and group 2, which implies that the age of detection and the level of amblyopia is not so important for a good treatment result, provided treat- ment can start within the 'plastic' period. This is in agreement with re- ports by Oliver et al. (1986) and Lit- hander & Sjostrand (1991). The pa- tients with microtropia usually remain slighty amblyopic in spite of good com- pliance, and the aniso-acuity in this type of strabismus has to be accepted (Campos 1995).
- 44
ACTA OPHTHALMOLOGICA SCANDINAVICA 1996 -
Acknowledgments This study was supported by grants from the Swedish Medical Research Council (no 4751), the Karolinska Institute and the Sig- vard & Marianne Bernadotte Research Foundation for Children Eye Care. We thank colleagues at the departments of pedi- atric ophthalmology in Stockholm for pro- viding information about their patients.
References Campos C (1995): Amblyopia. Surv Oph-
Hedin A, Nyman KG & Derouet B (1980): thalmol40: 23-39.
A modified letter matching chart for test- ing young childrens visual acuity. J Pediatr Ophthalrnol Strabismus 1 7 114-118.
Ladenvall G (1988): Visual assessment of school children seven years old. Findings at screening analysis of treated children. Acta Ophthalmol (Copenh) 70: 412.
Lennerstrand G, Jakobsson P & Kvarn- strom G (1995): Screening for ocular dys- function in children: approaching a com- mon program. Acta Ophthalmol Scand
Lithander J & Sjostrand J (1991): Anisome- tropic and strabismic amblyopia in the age group 2 years and above: a prospective study of the results of treatment. Brit J Ophthalmol75: 111-116.
73 (Suppl214), pp 26-38.
von Noorden G (1990): Binocular Vision and Ocular Motility. The CV Mosby & Co, St. Louis.
Oliver M, Neumann R, Chiamovitch Y, Go- tesman N & Shimshoni L (1986): Com- pliance and results of treatment for am- blyopia in children more than 8 years old. Am J OphthalmollO2: 340-345.
Unwin B (1991): The treatment of am- blyopia - a historical review. Br Orthoptic J 48: 28-31.
Corresponding author: Professor Gunnar Lennerstrand Department of Ophthalmology Huddinge University Hospital S-141 86 Huddinge, Sweden.
The cause of death in Laurence-Moon-Bardet-Biedl syndrome Ruth E k e
Department of Ophthalmology, Central Hospital of Hedmark, Hamar, Norway
ABSTRACT. The certificates of death of 14 deceased patients with Laurence-Moon-Bardet-Biedl (LMBB) syndrome, in which retinal dys- trophy is a dominant feature, were reviewed. Death occurred at a con- siderably younger age than in the general population. Renal disease was noted as primary or contributing cause of death in 7 cases with the diag- noses: cyst of the kidney, renal sclerosis, renal failure, proteinuria, renal disease unspecified and malignant hypertension with renal involvement. It is concluded that renal involvement is characteristic of individuals with LMBB syndrome and seems to reduce life expectancy considerably.
Key words: Laurence-Moon-Bardet-Biedl syndrome - Bardet-Biedl syndrome - cause of death - renal disease - life expectancy.
Acta Ophthalmol. Scand. 1996: 74 (Suppl219): 45-47
aurence-Moon-Bardet-Biedl L (LMBB) syndrome is an autoso- ma1 recessive inherited disorder where tapetoretinal degeneration is a domi- nant feature. The LMBB syndrome is traditionally described with the cardi- nal symptoms: retinal dystrophy, obesity, polydactyly, hypogenitalism and mental retardation (McKusick
1992). Additional features are renal disease (Harnett et al. 1988), spastic paraplegia (Hutchinson 1900), diabetes mellitus and nerve deafness (Alstrom et al. 1959), cardiac anom- alies (Elbedour 1994), liver disease (Pagon et al. 1982; Nakamura et al. 1990) and dental anomalies (Kobrin et al. 1990; Loftererd et al. 1990; Borg-
strom et al. 1995). The LMBB syn- drome has been classified into the sep- arate clinical entities: Laurence-Moon, Bardet-Biedl and Alstrom syndromes (Schachat & Maumenee 1982) (Table 1). It has not been possible, however, to define the limits precisely (Rizzo et al. 1986; Escallon et al. 1989; Hauser et al. 1990; Nyska et al. 1991) and intra- familial variation of expression of the phenotype has been demonstrated (Green et al. 1989). A broadly based phenotype concept, LMBB syndrome, has therefore been proposed (RIZZO et al. 1986; Kobrin et al. 1990).
Renal involvement has been de- scribed as a sixth cardinal feature (Churchill et al. 198l), and it has been stated that the renal disease involved a considerable risk of progression to ter- minal renal failure (Linne et al. 1986). Renal histopathological changes have been identified in early childhood (Falkner et al. 1977) and hypertension has been noted in 10 of 20 patients with structural or functional abnor-
45 -