Embed Size (px)
Citation preview

Respectable
Addicts?
Identity and
Over-the-
Counter
Medicine Abuse
Richard CooperLecturer in Public Health
ScHARR, University of Sheffield

Brief background to OTC medicines Review of OTC abuse
literature/evidence Describe a qualitative study involving
those affected Describe findings Argue the respectable addict represents a
tension in three rival areas Identify emergent issues/problems Conclusions
OverviewOverview

Backgrou
nd and
evidence

OTC medicine OTC medicine backgroundbackground

Typology based on agency/predicament Typology based on agency/predicament apparent but confusion over terminology – apparent but confusion over terminology – addiction/dependency rare:addiction/dependency rare: Misuse (wrong dose or indication, unintentional)Misuse (wrong dose or indication, unintentional) Abuse (deliberately exploiting side effects, Abuse (deliberately exploiting side effects,
experimentation)experimentation) Substitution (to replace illicit drug use)Substitution (to replace illicit drug use)11
OTC Abuse LiteratureOTC Abuse Literature

Typology based on agency/predicament Typology based on agency/predicament apparent but confusion over terminology – apparent but confusion over terminology – addiction/dependency rare:addiction/dependency rare: Misuse (wrong dose or indication, unintentional)Misuse (wrong dose or indication, unintentional) Abuse (deliberately exploiting side effects, Abuse (deliberately exploiting side effects,
experimentation)experimentation) Substitution (to replace illicit drug use)Substitution (to replace illicit drug use)11
Variation in OTC medicines implicated in Variation in OTC medicines implicated in abuse internationally by availability and abuse internationally by availability and customer preferences.customer preferences.
OTC Abuse LiteratureOTC Abuse Literature
5 key groups of medicines implicated:Codeine containing compound analgesics – Solpadeine, Nurofen Plus
Cough products (dextromethorphan)
Laxatives
Decongestants – Sudafed
Antihistamines (sedative)– Nytol, Actifed, Night Nurse, Phenergan,

Relatively little empirical research into OTC abuse.Relatively little empirical research into OTC abuse. No evaluation of treatment. No evaluation of treatment. No clear patterns as to those affected.No clear patterns as to those affected.
OTC Abuse LiteratureOTC Abuse Literature
Scale of Issue/DemographicsTwo thirds of UK pharmacists have reported abuse/misuse.2,3,4
Third of NI general public reported encountering OTC Third of NI general public reported encountering OTC abuse.abuse.55
4% of US teenagers abusing OTC products.
21.4 million packs of codeine-containing OTC meds sold 2008.
A problem associated with middle-aged females? 6
Just over 200 clients with OTC opiate problems in formal treatment (~0.25% of all clients). Over half exit treatment drug-free. 6
15,000 web support users. 7

OTC Abuse LiteratureOTC Abuse Literature
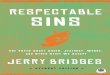
Primary Medicine of abuse
Additional Ingredient
•Addiction (codeine)•Euphoria (dextromethorphan)•Risk of other abuse (e.g. alcohol, illicit drugs)•Electrolyte imbalance (laxatives)•Convulsions/acidosis (chlorphenamine)•Gastro-intestinal irritation, haemorrhage , death (ibuprofen)•Rebound headaches (paracetamol and ibuprofen)•Hypokalaemia/acidosis (ibuprofen)
•Economic cost
•Accidents
• Adverse effect on jobs and relationships
PHYSIOLOGICALSOCIAL OTHER

OTC Abuse ResponsesOTC Abuse ResponsesSome evidence of attempts to Some evidence of attempts to manage/reduce abuse:manage/reduce abuse: Pharmacy-based (hide products, refuse sales, Pharmacy-based (hide products, refuse sales,
record sales)record sales) Harm-reduction intervention pilot – GP referralHarm-reduction intervention pilot – GP referral Proposed contract/reduction scheme in Proposed contract/reduction scheme in
pharmacies?pharmacies?

OTC Abuse ResponsesOTC Abuse Responses
Revised advice on OTC codeine sales 2009:
100 packs of co-codamol soluble now POM
Indications only for pain (not cold, flu) Front box warning: ‘Can cause
addiction. For three days use only.’
Similar changes in Australia
Some evidence of attempts to Some evidence of attempts to manage/reduce abuse:manage/reduce abuse: Pharmacy-based (hide products, refuse sales, Pharmacy-based (hide products, refuse sales,
record sales,)record sales,) Harm-reduction intervention pilot – GP referralHarm-reduction intervention pilot – GP referral Proposed contract/reduction scheme in Proposed contract/reduction scheme in
pharmacies?pharmacies?

OTC Abuse ResponsesOTC Abuse Responses
Year long APPDMGYear long APPDMG88 reported in 2009: reported in 2009: Training for doctors, nurses and AHPsTraining for doctors, nurses and AHPs Increased awareness of problemIncreased awareness of problem Recognition/support for on-line helpRecognition/support for on-line help Information for patients about risksInformation for patients about risks
Revised advice on OTC codeine sales 2009:
100 packs of co-codamol soluble now POM
Indications only for pain (not cold, flu) Front box warning: ‘Can cause
addiction. For three days use only.’
Similar changes in Australia
Some evidence of attempts to Some evidence of attempts to manage/reduce abuse:manage/reduce abuse: Pharmacy-based (hide products, refuse sales, Pharmacy-based (hide products, refuse sales,
record sales,)record sales,) Harm-reduction intervention pilot – GP referralHarm-reduction intervention pilot – GP referral Proposed contract/reduction scheme in Proposed contract/reduction scheme in
pharmacies?pharmacies?

Qualitativ
e Study

MethodsMethods
Semi-structured, qualitative telephone interviews with 16 key stakeholders of organisations with interests in OTC medicines
Semi-structured, qualitative face to face/phone Semi-structured, qualitative face to face/phone interviews with quota sample of interviews with quota sample of 1010 pharmacists and pharmacists and 77 MCAs from community MCAs from community pharmacies in UK pharmacies in UK
Semi-structured, qualitative telephone Semi-structured, qualitative telephone interviews with interviews with 25 25 individuals who have/had individuals who have/had experience of OTC medicine abuse/misuse. experience of OTC medicine abuse/misuse. Recorded/transcribed, ~1hr. Recruitment via Recorded/transcribed, ~1hr. Recruitment via postings on 2 internet forums helping those postings on 2 internet forums helping those with OTC medicine problems – CodeineFree with OTC medicine problems – CodeineFree and Overcountand Overcount
Stage 1
Stage 2
Stage 3

Semi-structured, qualitative telephone Semi-structured, qualitative telephone interviews with interviews with 25 25 individuals who have/had individuals who have/had experience of OTC medicine abuse/misuse. experience of OTC medicine abuse/misuse. Recorded/transcribed, ~1hr. Recruitment via Recorded/transcribed, ~1hr. Recruitment via postings on 2 internet forums helping those postings on 2 internet forums helping those with OTC medicine problems – CodeineFree with OTC medicine problems – CodeineFree and Overcountand Overcount
Stage 3

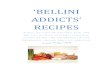
age Employment status Medicine(s) involved Doses Current use?
Treatment/support
M 40s Unemployed Paramol+Sudafed+alcohol
Up to 36/day either 16+16 or 12+12+12 III
No GP, DAT, (methadone), Overcount
M DND Professional Co-codamol, then Syndol Up to 8 per day I Yes GP, CFMM 30s Professional Co-codamol 12-14/day III Yes CFMM 30s Professional self-
employedNurofen Plus + prev. non-opiate illicit
Max of 60 tablets/ dayIII
No GP, DAT (Buprenorphine)CFM
F Former health prfn Solpadeine Up to 8/day I No CFMF Co-codamol sol +Rx co-codamol Up to 16/day (max 4/dose) III No CFM
F Healthcare profnl Nurofen Plus 32/day (max 64/day) III No CFM + buprenorphineF 30s Uni student Feminax then Cuprofen Plus prev.
alcohol36/day III Yes CFM
F 40s professional Nurofen Plus 24/day III No CFMF 20s Professional Co-codamol + prescribed Up to 8/day I No CFMF Professional Co-codamol + prescribed up to 16/day occ. prescribed II Yes GP,
M 50s Retired Professional Nurofen Plus + prescribed codeine 10/day Nurofen plus + MDD codeine III
No Overcount
M 60s Professional Solpadeine soluble Up to 10/day II No Private treatmentM Professional Phensedyl 90 bottles/week III No GP, DATM Professional Panadol Ultra then Nurofen Plus 15-20 of each III No GPM Solpadeine 4/day I No OvercountM Self-employed Nurofen Plus 10/day II Yes CFM, DAT, GPF Solpadeine Up to 8/day I Yes OvercountF Syndol Up to 8/day I Yes CFM, GPM Former health care
professionalCodiene linctus, Gees linctus,stolen DHC
Varied but much above max daily dose. III
No CFM + DAT (methadone)
M 60s Retired professional Phensedyl, Actifed, Codeine linc, diverted Rx codeine
200ml codeine linctus/day III no CFM+GP+DAT-methadone
F 30s Professional Syndol + nytol Syndol: 12/day II Yes Overcount
F 50s Professional Feminax, then Veganin 6-10/day. Max=12/day II Yes Overcount + GP + Drug Action


Initial useInitial use
All but two described initially using a product for a medical All but two described initially using a product for a medical condition (migraine, periods, ME, injury, gynae’)condition (migraine, periods, ME, injury, gynae’)
Use continued to avoid ‘withdrawal’ (headache, tremor, Use continued to avoid ‘withdrawal’ (headache, tremor, palpitations) or for other effect (buzz, calming, sedative).palpitations) or for other effect (buzz, calming, sedative).
Medicines were all codeine/DHC (Nurofen Plus, Co-codamol, Medicines were all codeine/DHC (Nurofen Plus, Co-codamol, linctus) but some pseudoephedrine, and sedative linctus) but some pseudoephedrine, and sedative antihistaminesantihistamines
“Physical pain doesn’t really bother me that much unless it interferes with something I am doing. So I was much more interested in the psychological effects [...] My ongoing anxiety.” Jack
“There was a medical condition involved. I was in hospital, came out of hospital and was given co-codomol or something at the time for the pain. That ended and the next thing I am downing Nurofen Plus.” Karen

Link between Rx and Link between Rx and OTCOTC

3 Types of Abuse3 Types of Abuse Words ‘addict’ or ‘addiction’ specifically used by participants.Words ‘addict’ or ‘addiction’ specifically used by participants. Drug seeking behaviours: Drug seeking behaviours: loss of control over self/consumption, ‘rituals’ of loss of control over self/consumption, ‘rituals’ of
specific brands, planned pharmacy routes, covert ( hidden to work, but not some specific brands, planned pharmacy routes, covert ( hidden to work, but not some friends/family)friends/family)
Harms varied: perceived withdrawal/anxiety at lower doses, GI Harms varied: perceived withdrawal/anxiety at lower doses, GI problems dependency/withdrawal, criminal acts, job/relationship problems dependency/withdrawal, criminal acts, job/relationship issues at higherissues at higher
“[...]I’ve never taken more than six a day, never gone over that […] Never escalated because I think I was too scared of going beyond that […] I don’t think I realised there was codeine in it at all” Aylsa (Nurofen Plus)
‘[…] the next thing I am downing Nurofen Plus. It started off probably taking the normal doses and the next thing [...] I am taking twenty four tablets a day.” Karen
“Well, I mean I suppose on a really bad day and this hasn’t happened recently, but on a really bad day, I suppose I could take sixteen […] So I would just knock back four at a time. Because that would give me that, as I say, it’s not a high. Literally, I zone out”. Rachel (co-codamol 8/500 tablets)
I would take eight in one day. But then of course in increasing amounts. Till the point came that I was taking thirty two a day. Even on really bad days, I would take a second lot of thirty two.” Theresa

Treatment and supportTreatment and support
Range of support identified with varying success and perceptions.Range of support identified with varying success and perceptions. Formal GP/DAAT help resisted by some for fear of recording problem.Formal GP/DAAT help resisted by some for fear of recording problem. Pharmacy involvement neutral – easy to bypass questions.Pharmacy involvement neutral – easy to bypass questions. On-line support offered confirmation/self-treatment but engagement low On-line support offered confirmation/self-treatment but engagement low
“As soon as I walked in there [DAAT] , you could see the other people who come there have got serious drug and alcohol problems and I stick out like a sore thumb.” Theresa
“I went to my doctors and I would either try my best, you know, with the prescribed dihydrocodeine but it er came to a point where it was beyond, you know, it needed a specialist to help.” Malcolm
[…] I have mentioned it to the doctor and he sort of said, ‘well it’s something you handle yourself’. At this sort of level, if you know what I mean?”Dwain
“[…] my own private GP […] he just laughed and said, ‘don’t be so stupid, stop taking them’. On the other hand, what is he supposed to say? ” Richard

Identity ClaimsIdentity Claims
All opioids Alcohol?
Managing appearances HiddenFamily

Addict IdentityAddict Identity ‘‘Addict’ or ‘addiction’ Addict’ or ‘addiction’
mentioned by all participants.mentioned by all participants. Variety of drug seeking Variety of drug seeking
behaviours described:behaviours described: Withdrawal experiencedWithdrawal experienced Loss of control over Loss of control over
self/consumptionself/consumption ‘‘Rituals’ of specific brandsRituals’ of specific brands Elaborate and methodical routes Elaborate and methodical routes
to visit pharmacies to avoid to visit pharmacies to avoid detectiondetection
Covert, hidden activity – (work, Covert, hidden activity – (work, public but some used friends, public but some used friends, family).family).
Shame identified by some – in Shame identified by some – in deceiving, hiding addiction.deceiving, hiding addiction.
On-line forums used to confirm On-line forums used to confirm (validate?) addict status.(validate?) addict status.
“Yeah I am an addict, no doubt about it. As much as a heroin addict, yeah. Shameful and it makes you feel dirty and guilty, but I was an
addict, yeah.” Yvette
“[...] my wife is, in fact in many ways, keeping an eye on me in that sense. She’ll say, ‘ooh, you having that again, are you?’ [...] actually at one point I started writing on when I bought the packet.” Graham
“[The web site] gives me the ability to anonymise myself. To experience and participate without it actually being physically me. I think where I am at right now is I need to own up who I am which probably wouldn’t mean I’d take part online, but it would I think part of my process.” John
“I also never hoarded it. It was part of the ritual for me to go out and have to find it every day.” Theresa
I do think we are all stupid quite honestly. I think I am stupid. I can’t believe that I have done this to myself. You know I find it really hard to understand.” Karen

Not like other addicts Not like other addicts but…but… Frequent attempts to Frequent attempts to
distinguish themselves distinguish themselves from other types of from other types of ‘addicts’, esp. those ‘addicts’, esp. those more chaotic/socially more chaotic/socially unacceptable.unacceptable.
However, recognition However, recognition that there were common that there were common features, either in the:features, either in the: Pharmacology of substance Pharmacology of substance
– e.g. codeine as opioid– e.g. codeine as opioid Dependency symptoms – Dependency symptoms –
withdrawal, dose withdrawal, dose
Some participants had Some participants had co-dependencies and co-dependencies and viewed OTC abuse in viewed OTC abuse in same way as same way as previous/current alcohol previous/current alcohol use, illicit substance use, illicit substance use.use.
DAAT services re-DAAT services re-enforced difference. enforced difference.
“I think in society it’s a negative stereotype, because you think of addicts and you think of drink, drugs, heroin, cocaine, you know needles and all those sorts of things […] But my understanding of an addict is somebody who cannot get through the day without what it is they are addicted to. I can’t get through the day without taking codeine.” Rachel
“I could not function without codeine & just because you can buy it legally in the
chemists, does not mean that it is any different from heroin. That’s just a social concept isn’t it, you know, no difference.” Yvette“As soon as I walked in there, you could see the other people who come there have got serious drug and alcohol problems and I stick out like a sore thumb. It’s painfully obvious people look at me and think ‘what on earth is somebody like her doing in a place like this’. Because I don’t have a can of Heineken in my hand or tram marks up my arm or stand outside smoking” Theresa
“If I went to any other pharmacies in town, nobody would even bat an eyelid [...] And I think as well if I was to go in and look like their stereotypical addict, they may go, ‘Oh well, you know’ and call the pharmacist over. But I don’t. I look like your normal middle aged woman.” Rachel

Professional identityProfessional identity Frequent discourse of claims Frequent discourse of claims
relating to occupational or relating to occupational or social status.social status.
Used to distinguish them and Used to distinguish them and their situation from other their situation from other forms of addiction.forms of addiction.
Attempts to assert Attempts to assert knowledge:knowledge: About pharmacologyAbout pharmacology Medicine doses/active Medicine doses/active
ingredientsingredients
Addiction is atypical for Addiction is atypical for some, as a loss of control set some, as a loss of control set against dominant control against dominant control over their (successful) lives.over their (successful) lives.
For some, NHS/GP For some, NHS/GP involvement actively resisted involvement actively resisted to avoid addiction being to avoid addiction being recorded & a career threat. recorded & a career threat.
“You know, should something different arise later that I need to get back to the doctor for but I have this mark from previous on my record, it affects what I need later on.” Jack
“[…]there are lots of people out there like me, that are intelligent professionals [...] I don’t know where we can go for support without putting ourselves at risk.” Theresa“I am a nurse so know what damage I was doing and still couldn’t stop and even when I got ill and had this huge gastric bleed, I still can’t believe that as an intelligent woman.”
“Oh my god, I hated it if I went away - and I go to America quite a bit, you know. Well you are not going to get them in America and that’s when you have got to go around thirteen pharmacies and find twenty packets to take with you.” Yvette
“Addicts are people on the street who haven’t got a job & I am sat here in a suit in an office, my own office with a very good career, senior manager within a very large organisation & I can’t be an addict. I am.” John

Discussio
n

Discussion questionsDiscussion questions Is the ‘respectable addict’ a viable category? Is the ‘respectable addict’ a viable category?
Linked to Reith’sLinked to Reith’s99 claim that addiction originated claim that addiction originated as a ‘middle class’ concern about control (cf as a ‘middle class’ concern about control (cf productivity in working classes)?productivity in working classes)?
Or is there a danger, after HackingOr is there a danger, after Hacking10, 10, of ‘making up of ‘making up people’ and spreading even further the web of people’ and spreading even further the web of addictive types?addictive types?
A moral concern about legitimate use and deviant A moral concern about legitimate use and deviant abuse?abuse?
Is a lesser category of pseudoaddictionIs a lesser category of pseudoaddiction1111 needed needed for some, to reflect inadequate pain relief?for some, to reflect inadequate pain relief?
What influence do on-line support groups have? What influence do on-line support groups have? For some (McIntosh & McKeganey)For some (McIntosh & McKeganey)1212, recovery , recovery narratives/identity are constructed by treatment.narratives/identity are constructed by treatment.
But...self-help group identity absent for many But...self-help group identity absent for many (passive).(passive).

ConclusionsConclusions
OTC medicine abuse occurs, often with links OTC medicine abuse occurs, often with links to medical treatment and range of medicine to medical treatment and range of medicine use and associated harms.use and associated harms.
Emergence of ‘Respectable addict’ identity Emergence of ‘Respectable addict’ identity reflects hidden nature of problem and with reflects hidden nature of problem and with implications for treatment.implications for treatment.
Variable engagement with, and benefit from, Variable engagement with, and benefit from, formal services (GP, DAAT, pharmacy).formal services (GP, DAAT, pharmacy).
Qualitative study limitations – recruitment Qualitative study limitations – recruitment through websites, self-selecting participants, through websites, self-selecting participants, not able to capture.not able to capture.

ReferencesReferences1. Temple DJ ‘Misuse of over the counter medicines in the UK’ In: Sheridan J & Strang
J (eds) Drug Misuse & Community Pharmacy London: Taylor and Francis 2003 2. Paxton R and Chapple P. Misuse of over-the-counter medicines: a survey in one
English county. Pharmaceutical Journal 1996;256:313-3153. Matheson C, Bond C & Pitcairn J. Misuse of OTC medicines from community
pharmacies: a population survey of Scottish pharmacies.Pharmaceutical Journal 2002;269:66-68
4. Pates R, McBride A, Li S & Ramadan R. Misuse of OTC medicines: a survey of community pharmacies in the South Wales health authority. Pharmaceutical Journal 2002;268:179-182
5. Wazaify M, Shields E, Hughes CM and McElnay JC. Societal perspectives on over-the -counter (OTC) medicines Family Practice 2005;22:170-176
6.6. National Treatment Agency. National Treatment Agency. Addiction to medicine: an investigation into the Addiction to medicine: an investigation into the configuration and commissioning of treatment services to support those who develop configuration and commissioning of treatment services to support those who develop problems with prescription-only or over-the-counter medicine.problems with prescription-only or over-the-counter medicine. London 2010 London 2010
7. Ford C and Good B. Over the Counter drugs can be highly addictive. British Medical Journal 2007;334;917
8.8. Reay, G. (2009). All-Party Parliamentary Drugs Misuse Group. An Inquiry into Reay, G. (2009). All-Party Parliamentary Drugs Misuse Group. An Inquiry into Physical Dependence and Addiction to Prescription and Over-the-Counter Physical Dependence and Addiction to Prescription and Over-the-Counter Medication. London.Medication. London.
9. Reith G. Consumption & its discontents: addiction, identity & the problem of freedom. The British Journal of Sociology 2004;55(2);283-300
10. Hacking I ‘Making up people. In Heller M et al Reconstructing Individualism Stanford Uni Press 1986
11. Bell K & Salmon A. Pain, physical dependence and pseudoaddiction: redefining addiction for ‘nice’ people. Int Journal of Drug Policy 2009;20:170-178
12. McIntosh J & McKeganey N. Addicts’ narratives of recovery from drug use: constructing a non-addict identity. Social Science and Medicine 2000;50:1501-1510

Funded by the
Pharmacy
Practice
Research
Trust
Richard CooperLecturer in Public Health
ScHARR, University of [email protected]













![Doctor X.ep01.480p.x264 [D Addicts]](https://img.pdfslide.us/doc/110x75/55320ec555034607098b4cd4/doctor-xep01480px264-d-addicts.jpg)