Embed Size (px)
Citation preview

Vol. 11, No.2 - July - Dec. 2008 J. 8aqai Med. Univ.
Rehabilitation of Fracture-Dislocation of Hip Joint
* FARHAN ISHAQUE
ABSTRACT: Fracture-dislocation of hip joint is one of the serious remedial conditions and often associated with neurological involment. Its rehabilitation requires a prolonged commitment of around 3-4 months. A case of a successful rehabilitation of a 32 year old male patient (nursing staff Fatima Hospital, BMU) is reported here, who underwent fracture-dislocation of right hip joint. The typical presentation of patient was internal rotation, flexion and adduction of the hip joint, as hip joint was dislocated posteriorly. This report describes the rehabilitation program that resulted in maximum outcome during the period of immobilization. The long term goals of hip fracture rehabilitation were to re-establish the normal anatomy of the hip joint and secondly to restore the functional status of the limb. Different therapeutic techniques and exercises around hip joint helped to maintain the muscular power and range of motion. After removal of skeletal traction, numerous physical therapy sessions improved muscle grading especially hip abductors and quadriceps muscles that resulted in maximum attainment of functional status. Subsequently advanced functional training made the patient to revert to its normal daily life.
KEYWORDS: Isometric Exercises, DTR, Traction, Heterotopic Ossification, Pelvic Tilt.
INTRODUCTION: Injuries around hip joint are one of the common musculoskeletal conditions2. It is very rare in adolescent and young populations but most commonly associated with old age19. Posterior dislocation of hip joint is one of them .. A hip dislocation occurs when the head of femur comes out of its articular surface i.e. acetabular cavity. Around 90% of patients, with posterior dislocation of hip joint, present with flexion, adduction and internal rotation of hip joint, along with leg shortening1,7. Whereas anterior dislocation is presented with flexion, abduction and external rotation of hip joint. Physical therapy management is essential after hip fracture 14. The satisfactory improvement of the patient after closed reduction requires the restoration of normal pelvic biomechanics in the early phase of the rehabilitation programlO
. One of the most crucial conditions which might turn into a serious complication is recurrent dislocation. As acetabulam is the weight bearing portion of hip joint; an early weight bearing might result in recurrent dislocationl 8.
Extra care should be taken for weight bearing activities, to achieve the normal lumbo-pelvic rhythm.
Case Summary: A 32 year old male patient was admitted to surgical ICU of Fatima Hospital of Baqai Medical University, with a history of road traffic accident. The patient was suffering from a fracture-dislocation of hip joint and was shifted to the Surgical I. C. U of Fatima Hospital, after getting emergency treatment from another private hospital. These types of fractures are seen in old age due to osteoporosis but in young age it is rare and often associated with a high energy trauma3
, as in this case. Clinically patient was suffering from posterior dislocation of hip joint along with the crack fracture of the acetabulum. On physical examination it was noted that the posterior dislocation presents with flexion, internal rotation and adduction1,7.
Patient experienced severe hip joint pain, radiating to the groin and leg. After closed reduction, patient was treated with skeletal traction (distal femur) lasting for six weeks. During this period of immobilization he was given therapeutic exercises to prevent future complication, like joint stiffness, muscle wasting, DVT or contracture formation.

Vol. 11, No.2 - July - Dec. 2008
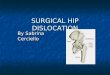
RADIOLOGICAL STUDIES: Radiological study revealed posterior dislocation and acetabular fracture of hip joint,(fig. 1. 1). The patient with hip dislocation can easily be diagnosed by looking at the position of the dislocated leg. At each follow up x- rays were repeated till the fracture got healed up.
Fig. 1.1: Fracture-Dislocation (posterior) of Right Hip Joint, Fatima Hospital (BMU)
NEUROLOGICAL EXAMINATION: Around 30-40 % of acetabular fractures are associated with sciatic nerve injury due to which patients are unable to move the leg7
. However this patient did not suffer from this complication and had no abnormal neurological or vascular involvement like AVN.
Sensory Examination: Patient did not suffer from any myotomal or dermatomal alteration and all reflexes were also intact.
Deep Tendon Reflexes:
• Pate!lar: L3-4 } Normal • AchIlles: SI-2
Motor Assessment (MMT): Manual muscle testing (MMT) was performed to assess the muscle strength of lower extremities 7• As the patient did not suffer from any nerve injury, he had enough strength in his lower extremities. Muscle charting indicated mild-moderate weakness in the following muscle groups that might be due to severe pain and muscle tightness.
... Iliopsoas (hip flexors) = 3/5 Right
... Gluteus medius and minimus (hip abductors) = 3/5 Right
... Gluteus maximus (hip extensors) = 3/5 Right
... Quadriceps femoris (knee extensors) = 4/5 Right
... Tibialis anterior (ankle dorsiflexors)= 4/5 Right
J. Baqai Med. Univ.
Biomechanical Analysis: The biomechanical study of the normal and dislocated hip joint is of great importance17 , because lumbopelvic rhythm is mandatory for a normal gait pattern. Due to the fracture of acetabulum, patient presented with Trendlenburg's gait (drooping of the pelvis on unaffected side) due to the weak hip abductors on effected side, to hold the pelvis during walking. A hip joint is a multiaxial ball and socket synovial joint which permits a large range of motions. Beside muscles, extra stability is provided by the strong ligaments and capsule, specifically the pubofemoral ligaments, iliofemoral and ischiofemoral ligaments. These ligaments control various range of motion at hip joint19 .
Movements at the Hip Joint: • Flexion(1l0*-120*) / Extension (10*-15*) = takes
place in sagittal plane and transverse axis • Adduction (30*)/ Abduction30*- 50*= takes place
in frontal plane and sagital axis (Anterio-posterior). • Internal (30-50*)/ External Rotation(50-60*) =
takes place in transverse plane and vertical axis. • Biomechanical alteration is one of the causes of
hip osteoarthritis, which causes sharing forces on articular cartilage leading to degeneration.
• Biomechanical investigations focusing on, the effect of fractures of the acetabulum on the alteration of hip joint mechanics,is a recent development.
ORTHOPAEDIC MANAGEMENT: A hip dislocation is a case of orthopaedic emergency and should be addressed as soon as possible to avoid future complications. The reduction of dislocated hip joint was done within 4 hours. Patient was treated conservatively by closed manipulative reduction of the dislocation8 and Orthopaedic surgeon recommended skeletal traction (distal femur) for a period of six weeks t6 heal the fracture of acetabular cavity fig, 1.2, 1.3. The aim of management was to reconstitute the hip joint to provide a stable, painless functional level and to avoid osteoarthritis of hip joint1. After six weeks skeletal traction was removed and patient did not show any leg length shortening. Bed rest of further 2 weeks was recommended to avoid recurrent dislocation and degenerative changes of hip joint15 • A hip dislocation can have long-term consequences, particularly if they are associated with fracture, as in this case.

Vol. 11, No.2 - July - Dec. 2008
Fig. 1.2
Fig. 1.3
X-Ray Showing Reduction after skeletal Traction
PHYSICAL THERAPY MANAGEMENT: The case report describes the rehabilitation plan of patient after fracture-dislocation of hip joint. Initially physical therapy was started to maintain the range of motion and muscular power around hip joint. During the period of skeletal traction , patellar mobilization and isometric exercises· of glutei, quadriceps and hamstring muscles were put into practice. The program further progressed with non-weight bearing, ·resistance training and stretching exercises, followed by partial weightbearing activities and full weight bearing after series of radiological study. That resulted in maximum attainment of joint stability.
J. 8aqai Med. Univ.
MOBILITY & STRENGTHENING EXERCISES: Strengthening and mobility exercises were given at hip and knee joint to prevent post fracture muscle . weakness and joint stiffness respectively. Precisely strengthening of the hip abductors, has been correlated well with the final functional outcome20
• In a literature review it was concluded that muscular strength significantly manipulates muscle physiology and enhances joint stability during movements and offers more ambulatory protection22
• Consequently strengthening exercises resulted in improvement of balance and proprioception22
• Strengthening exercises therefore played an important role in accomplishing our ultimate goal i.e. , gait training. Strengthening of quadriceps muscle also facilitates functional status of the patienrt.
Passive Mobility Exercise
Patient Performing SLR

Vol. 11, No.2 - July - Dec. 2008
Patella Mobilization
Patient Performing Isometric Gluteal Contraction (BMU)
WEIGHT BEARING: As standing causes compression forces on acetabular cavity 18 , the restriction of full weight bearing was maintained for 2 more weeks, after removal of skeletal traction. Patient was advised for partial weight bearing and step through gait using walking frame .
J. Baqai Med. Univ.
Patient Bearing Weight First Time After 8 Weeks of skeletal traction (BMU)
Patient was allowed partial weight bearing on efected leg after a period of eight weeks
with the help of walking frame.
After a period of 8 weeks, the fracture was perfectly healed, therefore patient was allowed for full weight bearing after 2 weeks of bed rest. Initially patient practiced sit to stand (STS) so that he can develop trunkle stability and neuro-muscular coordinationll .
According to a study which was conducted to investigate the effects of weight bearing and non weight bearing exercises after hip fracture, similar effects were seen in both groups. The combination of both types of exercise resulted in additional benefits on strength, balance, gait and functional performance21. It is suggested that early weight bearing should be avoided in cases of acetabular fracture, as standing causes compression forces on acetabular cavity18 and should concentrate on non-weight bearing exercises, until the fracture gets perfectly healed.
GAIT TRAINING: Ambulation is one of the most important components of physical therapy treatment4·7. Initially an antalgic gait pattern was observed as the patient suffered from a fracture-dislocation, which is a very painful condition23. By the end of 2nd month patient was ambulated with a walking frame, with partial weight bearing for two weeks and after two weeks he was encouraged to walk with a cane, until the limp was

Vol. 11, No.2 - July - Dec. 2008
disappeared. Patient usually shows scarcity and lack of confidence during balance and stance phase (weight bearing) due to the reduced muscle power around hip joint especially abductor group22. These are some of the factors which make rehabilitation a significant strategy, especially in terms of restoring the mess up functions22
.
Gait training using a walker and on parallel bar
In general, gait trallllllg helps in improving proprioception, muscular strength and balance22 .
FUNCTIONAL TRAINING: The physical performance and mobility is the key
J. 8aqai Med. Univ.
factor for functional recovery. The functional training started after a series of radiography and removal of skeletal traction, focusing the recovery of pre-fracture functional status, as soon as possible. Early weight bearing after acetebular fracture risks recurrent dislocation of joint, but at the end of the 3rd month rehabilitation programme the patient was able to perform certain challenging task like treadmill training, stairing up and down and wall sliding (eccentric muscle strengthening of quadriceps).
Treadmill Training
Stairing Activities

, .
Vol. 11. No.2 - July - Dec. 2008
Wall Sliding
DISCUSSION: Hip dislocations are often caused by any trauma or automobile accidents, usually accompanied by other injuries, like fracture of acetabulam that can complicate the process of Rehabilitation. This case was associated with acetabular fracture which is recognised as highly variable, in terms of age, gender, sex and fracture type3
. That is why successful consequences rely on extremely individualized management principles by experienced and skilled team3 . Some of the complications which are more prone to such conditions are recurrent dislocation, muscle atrophy (wasting of muscle) , heterotopic ossification (excess bone )2.13 , blood clots that can occur in the veins (DVT common complication)6 and secondary hip arthritis etc12.16. Identification and initiation of therapeutic treatment is very important in order to avoid these complications. Many patients experience long term disability after an orthopaedic management, but physical therapy is the key to restore a patient to its maximum functional status9. In Baqai Institute of Physical Therapy and Rehabilitation medicine we have successfully rehabilitated certain patients with this condition. Appropriate preliminary management options are significant for the desired outcome.
A comprehensive literature review suggests that an early failure in subsequent recovery manures can be accompanied by significant morbidity. Rehabilitation is a multidisciplinary effort of a skilful and capable team which includes health professionals such as
J. 8aqai Med. Univ.
Orthopaedic surgeon, Physical therapist, Nursing staff, social workers etc21. The main objective of this case report is to recognize the effectiveness and validity of physical therapy treatment. Physical therapy helped not only in restoring the functional status of the patient but it is also helpful in avoiding other secondary complications mentioned above. At the same time certain measures like prevention from falls, treatment of osteoporosis, regular exercise training are compulsory for a healthy physical life style22 .
CONCLUSION: The successful rehabilitation of patient constituents many early measures like on time emergency and orthopedic management, on time physical therapy commencement etc. In general, hip fractures are associated with poor outcomes due to prolong bed rest but this case report will provide a detail explanation of the appropriate and successful plan of care of post fractured-dislocation of hip joint. As there is no development of traumatic rehabilitation services in our society, therefore it is necessary to look into a new dimension of rehabilitation service which is more successful than the long-established traditional service. The long term goals of physical therapy treatment were not only to resume the functional independence of the patient but also to bring the patient back into the practical life.
REFERENCES: l. John Ebnezazr, essentials of orthopaedics for
physiotherapists, volume 1,2003.
2. Steven J. Schafer, Laura Ottaviani Schafer, Jeffrey O. Anglen, Martin Childers , Heterotopic ossification in rehabilitation patients who have had internal fixation of an acetabular fracture, Journal of rehabilitation Research and Development, vol. 37 No.4, July/August 2000.
3. Eric Pagenkopf, Andrew Grose, George Partal and David L. Helfet, Acetabular Fractures in the Elderly, Treatment Recommendations, journal of Hospital for Special Surgery(HSS) , 2006 September; 2(2): 161-17l.
4. Handoll, H H G (HH); Sherrington, Mobilisation strategies after hip fracture surgery in adults. Journal of Cochrane database of systematic

Vol. 11, No.2 - July - Dec. 2008
reviews (Online) 2007, vol (issue 1): pp CD001704, revised 2009/11103.
5. Thacker M, Post-operative management of acetabular fractures. Indian Journal of Orthopaedics, 2002, 36:29-30.
6. James P. Stannard, Renee S. Riley, et aI, Mechanical Prophylaxis Against Deep-Vein Thrombosis After Pelvic and Acetabular Fractures, The Journal of Bone and Joint Surgery (American) 83:1047-1051 (2001),2001.
7. Charlotte Yates, William D Bandy and R Dale Blasier, Traumatic pislocation of the Hip in a High School Football Player, journal of physical therapy, Vol. 88, No.6, June 2008, pp. 780-788, DOl: 10.25221200702.
8. Singh, Roop, Sharma, Sansar Chand, Goel, Tarun, Traumatic inferior hip dislocation in an adult with ipsilateral trochanteric fracture, Journal of orthopaedic trauma, 2006-Mar; vol 20 (issue 3): pp 220-2.
9. Bruyere, Brandi, M-L, Burlet, N, Harvey, Lyritis, G, Minne, H , Boonen, S, Reginster, J-Y, Rizzoli, R, Akesson, Post-fracture management of patients with hip fracture, Journal of Current medical research and opinion, 2008-0ct; vol 24 (issue 10): pp 2841-51.
10. Rumiana Tasheva, Restore the pelvis' tilt after surgically treated complex acetabular fractures in athletes, medicina spotrivia, Journal of Romanian sports medicine society, vol no 16, 2008 .
11. Shinsuke Yoshioka, Akinori Nagano, Dean C Hay, and Senshi Fukashiro, Biomechanical analysis of the relation between movement time and joint moment development during a sit-to-stand task, Journal of Biomed Eng Online.2009; 8: 27. [Pub Med]
12. Benjamin Gilles, Frank Kolo Christophe, Nadia Magnenat-Thalmann, ChristophD. Becker, SylvainR.Duc, Jacques.Menetrey, Pierre Hoffmeyer, MRI-based assessment of hip joint translations, Elsevier journal of biomechanics, vol. 42 (2009) 1201-1205.
J. 8aqai Med. Univ.
13. Jonathan Agner Forsberg, MD 1, Joseph M. Pepek, MD.et.al, Heterotopic Ossification in High-Energy Wartime Extremity Injuries, the Journal of Bone and Joint Surgery, 2009; 91: 1084-1091.
14. Lauridsen UB, de la Cour BB, Gottschalck L, Svensson BH Intensive physical therapy after hip fracture. A randomised clinical trial, 2002; 49: 70-2 [Medline]
15. Neil D Patel, Ravi K Trehan, Acute isolated acetabular fracture following a game of squash: a case report, Journal of Medical Case Reports, 28 November, 2007.
16. A. A . Faraj, K. So, Traumatic hip fracture subluxation, European Journal of Orthopaedic Surgery and Traumatology, Vol. 15, 2005.
17. Tanino Yoshitsugu, Biomechanics of A Lower Extremity-Functional Anatomy of Muscle And Joint Movement, Journal Of Kansai Physical Therapy, Vo1.5; No.; Page.37-40 (2005) .
18. Springer Berlin, Heidelberg, Weight bearing area during gait in normal and dysplastic hips, European
. Journal of Physiology, Vol. 439., January 2000.
19. Naveenpal S Bhatti, Hip Fracture, journal of eMedicine & sports medicine Jan 30, 2009 .
20. F Gottschalk, S Kourosh, and B Leveau, The functional anatomy of tensor fasciae latae and gluteus medius and minimus, journal of anatomy, 1989 October; Vol. 166: 179-189.
21. Sherrington C, Lord SR and Herbert RD,A randomised trial of weight-bearing versus nonweightbearing exercise for improving physical ability in inpatients after hip fracture. Australian Journal of Physiotherapy, (2003) 49 : 15-22.
22. Ana Luiza Cabrera Martimbianco, et.al, effects of proprioception in the rehabilitation process of hip fractures review article, journal of Acta ortopaedic .bras. vol. 16, 2008.
23. N. B. Foss, M. T. Kristensen, et.al, Postoperative pain after hip fracture, British Journal of Anaesthesia, 102 (1) . 2009.

Vol. 11, No.2 - July - Dec. 2008 J. Baqai Med. Univ.
INSTRUCTIONS TO AUTHORS
The Journal of Baqai Medical University is a biannual journal of medical and related sciences published by the Baqai Medical University. The journal is intended as a vehicle for the young medical scientist, research workers as well as senior scholars, for the exchange of information and publication of their research findings.
The manuscript prepared, according to specifications, given below, should be submitted to the Editor, Journal of Baqai Medical University. The Journal will be published twice a year (January and July) and the following categories will be included:
a. Original scientific articles. b. Review articles on important medical topics. c. Case report of educational value. d. Short communication for quick dissemination
of information. e. Letters to Editor. f. Book review. g. Announcement regarding important meetings,
workshops, seminars and other events relating to Health Sciences at national and International level.
(b) Written consent of all the authors on a prescribed proforma is essential.
(c) Copyright of the paper should be transferred to the Journal.
5. Manuscript with language deficiencies, error in syntax and typing mistakes may be returned back or may cause unnecessary delay in publication and therefore requires a thorough examination before submission.
6. The title page should contain, in addition to the article, Title, Author(s) Name(s) and Address, Key word and Abstract of the paper of up to 200 words. The name of the corresponding author should be properly indicated.
7. Tables, Photographs (on glossy paper) and illustrations to be submitted in duplicate, separately. Legends of the illustration, tables etc. should be typed on separate sheet. Formulae to be written by hand. Photograph(s) should be submitted only when extremely necessary and data can not be expressed in any other form.
1. Two complete copies of the manuscript, typed 8. The manuscript should be divided into the following sections for uniformity's sake.
2.
in double space on one side of the paper, with clear margin of atleast one inch on both sides, are to be submitted for consideration. All words that are meant to be italicized should be underlined.
The manuscript should be based on an original work, which has not been submitted or published elsewhere. 9.
3. All papers submitted for publication are subject to review by experts in the area of specialization.
4. (a) The responsibility for the scientific contents and statement made by the author(s) of the accepted paper, lies solely on the author(s).
Abstract, Introduction Materials and Methods, Results Discussion Observation (if applicable) Conclusion References
References to be numbered as they appear in the text and listed serially at the end .
i) Jones J, Fletter B. Complications after cardiopulmonary resuscitation, Am.J Public Health 1994; 12:687-8.
ii) Cox DR, Oake J. Analysis of survival date. London, Chapman Hall, 1984; 2-5.