-
7/28/2019 17 Fracture and Dislocation
1/11
FRACTURE AND DISLOCATION
SKELETAL TRAUMA
one of the most important aspects of orthopaedic radiology
commonest problem presented to the musculoskeletal
radiologist
FRACTURE occurs when there is a break in the continuity of
bone
either complete or incomplete
When a loading force is applied to bone, it initially deforms
elastically, and as the load isremoved, the deformity of the bone
is reversed and the bone returns to normal.
As the loading force is increased, however, the elasticity of
the bone is overcome, and aplastic fiture' occurs, with the bone
remaining deformed after cessation of the load.
Finally, complete failure of the bone will occur, giving rise to
a true fracture.
Repetitive loading of a bone at `subfracture' levels may lead to
the development ofstress fracture
TERMINOLOGIESOpen fracture
Bone fragments penetrate the skin
A comminuted fracture of the tibia, with medialdisplacement and
overriding of the distal fragment. Because ofthe Proximity of the
skin surface to the anteromedial aspect ofthe tibia, penetration of
the skin is likely, and in fact, air is seenin the soft tissues,
indicating that penetration is medialdisplacement, but lateral has
occurred. There angulation of thedistal fragment. A segmental
fibula fracture is noted.
Radiographic signs of open fracture Obvious prorusion of bone
fragments beyond the soft tissue margins
Absence of portions of the bone
Gross soft tissue disruption extending to the bone surface
Subcutaneous gas
Foreign material within the fracture
Closed fracture
fracture remains covered with intact skin
Nature of the fracture lines three major types
o transverseo oblique oro spiralo combination
Comminuted fracture
the injury produces more than one fracture line willoften
produce a minor triangular fragment of bone,known as a ` butterfly'
fragment
RADIOLOGY FRACTURE AND DISLOCATION Page 1
-
7/28/2019 17 Fracture and Dislocation
2/11
Segmental fracture
o one in which a segment of bone isisolated by fractures at each
end
Segmental fracture of thefemur: by definition acomminuted
fracture. In this
case the isolated segment isclearly malaligned
Incomplete fractures
occur most commonly in children, when bone resilience is
greater, and are of
three typeso plastic fractures
occur when there is bending of the bone without cortical
disruption, oracute angulation
o `torus' or ` buckle' fracture
fracture of the cortex on the compressive side of the bone with
anintact cortex on the tension side (Fig. 43.4):
Torus fracture of the radius. The cortex isbuckled on the dorsal
surface. Apart fromminor plastic deformity, the volar surfaceis
intact.
o greenstick fracture converse of the torus fracture, occurring
only on the tension side, with
cortical interception
Fractures should also be evaluated for continuity and proximity
of the fracture fragments apposition position of the major
fragments with respect to each other
distracted fragments which are not apposed are described as
being displacementalong the long axis of the bone, or displaced,
away from the long axis
o fracture should be described according to the direction of
displacement of thedistal fragment relative to the proximal
bone
Alignment
refers to the relationship along the axis of major fragments
described in two wayso most logical description refers to the
alignment of the distal fragment with
respect to the proximal
additional advantage of following the same rules' as apply
todisplacement
o describe the angulation as the direction of the apex of the
angle at thefracture site
Alternative method, commonly used by orthopaedic surgeons
RADIOLOGY FRACTURE AND DISLOCATION Page 2
-
7/28/2019 17 Fracture and Dislocation
3/11
Varus and valgus angulation are terms that are commonly
used,particularly by orthopaedic surgeons
refer to the alignment of the distal fragment with respect to
themidline of the body, with
o varus angulation of the distal fragment towards the
midlineo valgus reverse
Impaction
descriptive term for fractures in which the bone fragments are
driven into each other
ASSOCIATED SOFT TISSUE ABNORMALITIESJoint effusion or
hamarthrosis
fractures around a joint providing the joint capsule remains
intact
useful at the elbow, where elevation of the pads, either
anterior or posterior, is goodevidence of injury
Elbow effusion: elevation of the anterior fat pad
(arrow).Although not pathognomonic for fracture, anterior fat pad
elevationindicates significant effusion, and is frequently
associated with afracture. Careful Inspection of the unfused radial
head shows a minorcortical stepoff of the metaphysis, indicating a
fracture
lipohamarthrosis
RADIOLOGY FRACTURE AND DISLOCATION Page 3
-
7/28/2019 17 Fracture and Dislocation
4/11
fat fluid level within a joint
most commonly seen in the knee with radiograph made with a
horizontal beam
firm presumptive evidence of an intra articular fracture
Fat fluid level is seen in the knee joint on this cross table
view.This indicates intra-articular bone injury.
Soft-tissue swelling in the retropharyngcal space
being a reliable sign of cervical spine trauma
Compression fractures of the vertebral bodies of T7, T8and T9
with large paraspinal haematoma, which took
many months to absorb, still being visible after thefracture had
consolidated.
FRACTURE HEALING
After a fracture has occurred, the process of healing
begins.
RADIOLOGY FRACTURE AND DISLOCATION Page 4
-
7/28/2019 17 Fracture and Dislocation
5/11
RADIOLOGY FRACTURE AND DISLOCATION Page 5
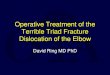
Stages of healing after a fracture
Considerable bleeding occursat the fracture. The blood
liesbetween the bone ends andunder the periosteum.
In a few days a blood clot
forms. Soon the clot isinvaded by osteoblasts fromthe nearby
bone and from theperiosteum.
The osteoblasts lay downnew bone which fills the gapbetween the
fragments andbulges out at the sides. Thisis the callus.
Over a period of manymonths the callus is absorbedby the
osteoblasts, and theymake more new bone exactlylike the original
one.
-
7/28/2019 17 Fracture and Dislocation
6/11
early stages of bone formation are not visible
radiographically
healthy person, new bone formation is visible within 4-6 wks,
with the healing processcomplete in 4-6 mos for a single fracture
in a large tubular bone
delay in union may be evident by a delay in the appearance of
new bone, and can occurfrom a variety of causes
EVALUATION OF SKELETAL TRAUMA
RADIOLOGY FRACTURE AND DISLOCATION Page 6
-
7/28/2019 17 Fracture and Dislocation
7/11
-
7/28/2019 17 Fracture and Dislocation
8/11
well defined lesion of mixed signal intensity occupies the
regionof the iliopsoas. The Mixed signal pattern is common
inhaematoma, indicating the complexity of the haematoma,
andvariations in haemoglobin, deoxyhaemoglobin, methaemoglobinand
haemosiderin levels
COMPLICATION OF FRACTURE most uncomplicated fractures heal
readily, in
open fractures have an increased potential for infection at the
fracture site and carefulscrutiny of the healing process is
warranted
tibia has long been singled out as a bone liable to delayed
union or non-uniono reasons
obscure, but poor vascular supply and lack of immobilisation
due to the large number of 'high-energy' Injuries seen in the
tibia,particularly from pedestrian bumper' injuries, with a large
amount ofresulting necrosis of soft tissue and bone at and around
the fracturesite
Causes of delayed union
Mechanical poor appositionInadequate stabilization
Pathological age-decreased osteoblastic activityDietary-vitamin
deficiency (C and D)Pathological fracture (underlying
abnormality:infection)
Non-uniono absence of bony union over a prolonged periodo
radiographic appearance is usually of a persistent fracture line,
usually with
sclerotic margins, and marked surrounding sclerosiso MRI may
have a role to play in the assessment of non-union with its ability
to
detect infective causes
Causes of non union1. Idiopathic (particularly tibia)2. Poor
stabilization3. Infection4. Pathological fracture5. Massive initial
trauma
Non-union of the tibia despite interosseousbone grafting and
surgical wiring. There issclerosis around the fracture line,
withoutfirm evidence of bone bridging, 1 yearafter the fracture
Maluniono fracture which heals in an unsatisfactory
anatomical
position, either with excessive overlap of fragments,giving rise
to shortening of the bone, or unsatisfactoryangulation or
displacement of the distal fragment
Malunion of the tibial fracture, which has healed well,but shows
lateral angulation of the distal fragment.
RADIOLOGY FRACTURE AND DISLOCATION Page 8
-
7/28/2019 17 Fracture and Dislocation
9/11
SPECIAL TYPES OF TRAUMAStress (fatigue) fractures
result from chronic repetitive forces which by themselves are
insufficient to causefracture, but over the course of time lead to
the classical changes of a stress fracture
occur in many bones, and usually at characteristic sites, often
as the result of athleticactivity
example: `march' fracture of the second and third metatarsal
head, the stress fractureof the mid and distal tibia and fibula in
long-distance runners and ballet dancers, andfractures of the
proximal fibula in paratroopers
earliest diagnosis can be made by nuclear medicine scanning or
MRIo show increased activity before radiographic signs appear. When
radiographic
signs appear, they may take several forms, depending upon the
stage of
healing or the chronicity of the stresso hairlike lucency may be
seen traversing the hone. New Bone formation around
the fracture may be the only radiographic sign, or may accompany
thecortical fracture
Multiple stress fractures are seen, some with obvious
horizontallucencies running perpendicular to the bone cortex. The
Patient was a joggerwho refused to give up jogging despite the
pain
TypesSpondylolysis pars inter- articularis defects
underlying causeso congenital hypoplasia of the articular
processeso degenerative change within the posterior joints
Mild degrees of spondylolisthesiso occur when there is loss of
articular cartilage at the posterior intervertebral
joints as in degenerative disease More severe
spondylolisthesis
o results from pars interarticularis defectso graded according
to severity
Grade I up to 25% displacement of the vertebral body Grade II up
to 50%
Grade III up to 75% Grade IV 100% displacement
Avulsion fractures
RADIOLOGY FRACTURE AND DISLOCATION Page 9
-
7/28/2019 17 Fracture and Dislocation
10/11
occur from avulsion of bone fragments at the site of ligamentous
or tendinousattachments throughout the skeleton
osteochondritis which represent avulsion fractures from chronic
or repeated traumao Osgood-Schlatter disease
diagnosis is made clinically, although it can he
suggestedradiographically when there is clear elevation of
fragments of the tibial
tubercle separated from the underlying boneo Sindig-Larsen
disease of the tibial tubercle and inferior patella
respectively
Common avulsion injuries at the origin of muscle tendon
insertions arc seen at theo inferior border of the ischium
(hamstrings)o Anterior inferior iliac crest (rectus lemons)o lesser
trochanter (iliopsoas)
Sites of avulsion fractures with muscle origin
Site of avulsion fracture Muscle originAnterior superior iliac
crest SartoriusAnterior inferior iliac crest Rectus femorisIschial
tuberosity HamstringsGreater trochanter GlutealsLesser trochanter
IliopsoasPosterior calcaneus Achilles tendonOlecranon process
TricepsSuperior patella QuadricepsInferior patella (Sinding-Larsen)
Patella ligament
Tibial tuberosity (Osgood-Schlatter) Patella ligament
Pathological fractures
occur through bone that has been weakened by an underlying
disease
occur through bone that is weakened by such conditions as
osteoporosis orosteomalacia, bone tumours (whether benign or
malignant) or even tumour-like lesions
of bone In elderly patients underlying malignancy should be
considered, especially if the
fracture occurs in a site other than those usually seen in
osteoporosis such as thefemoral neck, or in cases in which the
severity of the injury is inappropriate to thefracture created
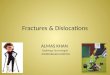
DISLOCATION
When a joint, instead of a bone, suffers a severe strain
No bones are broken, but one bone is pushed out of its proper
place
Dislocated joints are very painful
Usually look deformed because the bones are in wrong
positionFrom left to right, dislocation of theelbow,knee, and
little finger.
RADIOLOGY FRACTURE AND DISLOCATION Page 10From left to right,
dislocation of the elbow,knee, and little finger.
http://www.daviddarling.info/encyclopedia/E/elbow.htmlhttp://www.daviddarling.info/encyclopedia/E/elbow.htmlhttp://www.daviddarling.info/encyclopedia/K/knee.htmlhttp://www.daviddarling.info/encyclopedia/K/knee.htmlhttp://www.daviddarling.info/encyclopedia/F/finger_anatomy.htmlhttp://www.daviddarling.info/encyclopedia/E/elbow.htmlhttp://www.daviddarling.info/encyclopedia/K/knee.htmlhttp://www.daviddarling.info/encyclopedia/K/knee.htmlhttp://www.daviddarling.info/encyclopedia/F/finger_anatomy.htmlhttp://www.daviddarling.info/encyclopedia/K/knee.htmlhttp://www.daviddarling.info/encyclopedia/F/finger_anatomy.htmlhttp://www.daviddarling.info/encyclopedia/E/elbow.htmlhttp://www.daviddarling.info/encyclopedia/K/knee.htmlhttp://www.daviddarling.info/encyclopedia/F/finger_anatomy.htmlhttp://www.daviddarling.info/encyclopedia/E/elbow.html
-
7/28/2019 17 Fracture and Dislocation
11/11
Management
Reduction of dislocationo Process of putting the bones back into
their normal positions
Anethetic is given to relax the muscles
RADIOLOGY FRACTURE AND DISLOCATION Page 11