Embed Size (px)
Citation preview

international journal of athletic therapy & training january 2013 7
A hip dislocation that is combined with an acetabular fracture is typically caused by high-energy forces associated with a motor vehicle accident.1 Hip dislocation or acetabular fracture resulting from participa-tion in sports are typically less severe and
rarely occur together.2-5 Stilger et al.4 reported an acetabular fracture in a football player, after which the athlete was able to walk off the field. Regardless of mechanism, hip disloca-tions and displaced ace-tabular fractures have favorable outcomes if addressed quickly.6,7 Delayed initiation of
proper care can negatively affect prognosis, due to avascular necrosis or degenerative arthritis.8 Even though hip dislocation and acetabular fracture are very rare in athlet-ics, athletic trainers and therapists must still possess the necessary knowledge for the evaluation, treatment, and rehabilitation of such hip injuries.
Case ReportA 19 year-old college football quarterback (height = 184.15 cm, weight = 81.36 kg)
CASE REVIEW
Brent I. Smith, MS, ATC, LAT • ATI Physical Therapy and Steven S. Louis, MD • Hinsdale Orthopaedic Associates
was attempting to evade opposing players when he was tackled from behind during a game. He landed on his hands and knees while the opponent landed directly on his posterior pelvis. Following the tackle, the athlete remained on his left side, with his left hip flexed to almost 90 degrees, slightly internally rotated and adducted. He was examined in that position on the field by an athletic trainer. The athlete reported intense pain on the anterior, lateral, and posterior aspects of the left hip, and he was unable to move the hip. A shortened appearance of the left leg was noted. Distal sensation to light touch was normal and a dorsal pedal pulse was evident. Palpation of the posterior hip joint revealed a gross bony deformity. The athlete was stabilized by securing his left thigh against his right leg and emergency medical technicians were summoned. The athlete was transported to a local hospital where plain radiographs of the pelvis in Judet-oblique and anterior-posterior views were ordered (Figure 1). The radiographs indicated a left posterior wall acetabular fracture with a 4 × 2.6 cm fracture fragment, which included a portion of the weight bearing dome (WBD). The acetabular fragment was displaced poste-riorly and superiorly, and the dislocated femoral head was displaced superiorly and posteriorly. No fracture of the femur was
© 2013 Human Kinetics - IJATT 18(1), pp. 7-11
Hip Dislocation and Acetabular Fracture in a Collegiate Football Player
Combined hip dislocation and acetabular fracture is extremely unlikely to result from sport participation.
Expedient surgical management produces the best outcome.
Accelerated rehabilitation is not appropri-ate for a severe hip injury.
Key PointsKey Points

8 january 2013 international journal of athletic therapy & training
noted. The athlete was then transferred to a level-1 trauma center for further care.
Upon arrival at the second medical care facil-ity, the athlete continued to deny any neurological symptoms and additional radiographs were acquired. Closed hip reduction was achieved by manipulation, which was maintained by placement of a distal femo-ral Steinmann pin for longitudinal traction. Following reduction, additional radiographs and a computed tomography (CT) scan of the hip were obtained to determine the extent of acetabular displacement and to rule out defects of the femoral head (Figure 2). Open reduction and internal fixation (ORIF) of the acetabulum was determined to be the best treatment. Two days after the injury, the athlete underwent the procedure through a Kochner-Langenbeck (posterior) approach. Postoperative care included maintenance of longitudinal traction for approximately 24 hours, which was followed by continuous passive motion and physical therapy to facilitate ambulation. The patient began a 6-week course of daily dalteparin sodium injections for blood clot prophylaxis, and a compression stocking was worn. Indomethacin was prescribed to prevent heterotopic ossification. The patient was discharged 4 days following surgery. Axillary crutches were used for touch-down weight bearing (TDWB), with instruction to place up to 30
pounds of weight on the involved extremity. He was also instructed to avoid excessive hip flexion (e.g., squatting) and crossing the legs.
Following hospital discharge, coordination of the athlete’s care was assumed by the team orthopedic physician. Follow-up radiographs demonstrated that the ORIF procedure was successful, with no apparent loss of fixation. Four weeks of TDWB was recom-mended while the patient recovered from the surgical procedure at home. At 5 weeks following discharge from the hospital, the athlete began the formal reha-bilitation process. An evaluation at the initiation of the rehabilitation program revealed that the athlete’s primary complaints were left hip and knee pain and lack of active and passive range of motion (ROM) of the left knee. The patient reported no pain at rest, but he indicated that the knee was more uncomfortable than the hip during activity. Significant scar tissue formation over the medial distal femur and lateral hip was evident. Short-term goals for the first 4–6 weeks of rehabilitation were pain reduction, increased knee and hip ROM, and improved ambulation. Long-term goals included normalized gait, return to full strength, ability to perform running and cutting activities, and return to football participation. Gait training and scar mobilization were initiated during the first rehabilita-tion session.
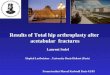
Figure 1 ap radiograph of pelvis showing left hip dislocation (arrow a) and posterior acetabular wall fracture (arrow B).
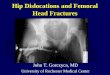
Figure 2 ct of left acetabular posterior wall fracture (arrow)

international journal of athletic therapy & training january 2013 9
The initial phase of rehabilitation was focused on improvement in strength and ROM during supervised sessions that were scheduled at a frequency of three times per week. Patellar mobilizations were performed, along with gentle passive stretching of the hip and knee joints. Therapeutic exercises included isometric contractions of the quadriceps and the hip adductors and abductors. Active exercises included heel slides, side-lying hip external rotation, standing hip flexion, side-lying hip abduction, and straight-leg raises. The open-chain exercises were progressed to include the resistance of two-pound weights and elastic tubing. Proprioception activities were initiated, and a station-ary bike was utilized to assist with restoration of ROM and both muscular and cardiovascular endurance. Exer-cises utilized during the ensuing weeks were selected to further restore strength and ROM, and gait training was performed on a treadmill. After 4 weeks, the athlete had achieved dramatic improvements in passive ROM and strength. He was capable of full weight bearing, but lack of full ROM and strength restoration contributed to an antalgic gait. Improvement in scar mobility was evident at both the lateral hip and medial knee.
At 9 weeks postsurgery, the patient began perform-ing closed-chain exercises that included mini-squats, calf raises, and leg presses. Dynamic activities were initiated, which included lateral step-ups and stool scoots. A home exercise program was developed for self-guided rehabilitation during a 3-week winter break. Upon return, the athlete exhibited a normalized gait, and strength at the hip and knee was normal, but neither hip nor knee ROM had improved. The athlete reported pain-free activity, but he still complained about tenderness at the hip incision site. He responded well to low-intensity plyometrics and treadmill jog-ging, and full ROM at the hip and knee was attained. At 5 months postsurgery, the athlete was cleared for sport-specific training that included aggressive cutting maneuvers and agility training but no contact for an additional 6 weeks. The athlete eventually returned to his previous level of function. He reported occasional hip discomfort during participation in a final season football, after which he graduated.
DiscussionCombined hip joint dislocation and acetabular fracture has been documented in the literature.9-11 The hip is a
very stable joint, but high-energy forces can produce disruption of its articulating surfaces.1 Motor vehicle accidents are the cause of up to 93% of hip fractures and dislocations;12 however, a severe hip joint injury can sometimes result from the lower energy forces associated with sports.3,4,13
Dislocation of the hip represents a small percent-age of all traumatic joint dislocations. Ninety percent of hip dislocations occur in a posterior direction,14 which may be attributed to the typical mechanism of injury. When the knee hits the dashboard of a car during a motor vehicle accident, a posteriorly-directed axial force is transmitted through the femur to the acetabulum.12 Sixty-six percent of posterior disloca-tions result in displaced fractures of the acetabulum or proximal femur.14
Judet et al.15 created a classification system for fractures of the acetabulum. The type of fracture was found to be the direct result of the position of the femur relative to the pelvis and the amount of force (i.e., greater force producing greater damage and displace-ment). Acetabular fracture associated with a posterior dislocation can range from nondisplaced, stable, pos-terior lip fractures to grossly displaced fractures that encompass a large portion of the WBD. Classification of an acetabular fracture is best established with antero-posterior and two Judet-oblique (i.e., obturator and iliac) radiographic views.16 The use of CT helps to identify loose bodies and impaction damage to the articular surfaces. Proper classification of an acetabular fracture is a key consideration for development of an appropriate treatment plan.
The long-term outcome of a hip fracture disloca-tion is affected by time-to-reduction. The prognosis is best when reduction of the dislocation is achieved within 6 hours of the traumatic event.6 Reduction of hip dislocation is routinely achieved by closed manipu-lation, but a case that is resistant to closed reduction (i.e., a “locked” or “fixed” dislocation) is considered an emergency that dictates immediate surgical interven-tion.17 Delayed reduction increases risk for avascular necrosis of the femoral head, degenerative arthritis,8 and prolonged nerve palsy.18 An acetabular fracture that includes a portion of the WBD complicates the reduction process.19
After reduction of a hip dislocation has been achieved, an acetabular fracture must be addressed. Conservative versus surgical treatment of acetabular

10 january 2013 international journal of athletic therapy & training
fractures continues to be a topic of debate. Nonopera-tive treatment is often employed if (a) the fracture is non-displaced20 or (b) congruency between the femo-ral head and WBD of the acetabulum demonstrates no more than 5 mm of displacement.21 Conservative management includes bed rest and traction for 6–12 weeks, which requires insertion of a Steinmann pin through the distal femur (longitudinal traction) and may require insertion of a Schanz pin in the proximal femur (lateral traction).22
One of three surgical approaches is used to access the displaced fragments for ORIF with screws and plates (i.e., Kocher-Langenbeck, extended iliofemoral, or ilioinguinal).7 ORIF has been reported to produce “good to excellent” results in 74–86% of patients.23-25 Postoperative complications include avascular necrosis, heterotopic ossification, infection, osteoarthrosis, deep vein thrombosis, and nerve palsy,26,27 some of which can be life-threatening issues.
Ambulation following hip surgery must limit stress on the articular surfaces of the hip joint. When prop-erly performed, TDWB has been reported to produce an appropriate level of joint pressure for avoidance of complications.28 Restoration of strength early in the rehabilitation process has been shown to maxi-mize postoperative prognosis,29 and its contribution to improvement of gait improves overall functional outcome.30
Summary The pathology associated with traumatic hip injuries largely depends on the magnitude of forces that are involved. Fractures and dislocations of the hip joint are most commonly caused by motor vehicle acci-dents and are rarely the result of sport participation. Prognosis largely depends on injury severity, and man-agement of severe injuries typically involves surgery. Although severe injury to the hip joint is infrequently encountered by athletic trainers and therapists, proper immediate management and postsurgical rehabilita-tion are both important factors that can influence the patient’s outcome.
References 1. Matta JM, Merritt PO. Displaced acetabular fractures. Clin Orthop.
1988;230:83-97.
2. Lambert BM. Nakajima MA. Acetabular fracture in a 19-year-old foot-ball player. Int J Athl Ther Train. 2011;16(2):4-7
3. Moorman CT, Warren RF, Hershman EB, et al. Traumatic posterior hip subluxation in American football. J Bone Joint Surg. 2003;85-A(7):1190-1196.
4. Stilger VG, Alt JM, Hubbard DF. Traumatic acetabular fracture in an intercollegiate football player: a case report. J Athl Train. 2000;35(1):103-107.
5. Yates C, Bandy WD, Blasier RD. Traumatic dislocation of the hip in a high school football player. Phys Ther. 2008;88(6):780-788.
6. Hugaard K, Thomsen PB. Traumatic posterior fracture-dislocation of the hip with fracture of the femoral head or neck, or both. J Bone Joint Surg. 1988;70-A(2):233-239.
7. Matta JM. Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg. 1996;78-A(11):1632-1645.
8. Jaskuka RA, Fischer G. Dislocation and fracture-dislocation of the hip. J Bone Joint Surg. 1991;73-A(3):465-469.
9. Borrelli J, Goldfarb C, Ricci W, Wagner JM, Engsberg JR. Func-tional outcome after isolated acetabular fractures. J Orthop Trauma.2002;16(2):73-81.
10. Liebergall M, Mosheiff R, Low J, Goldvirt M, Matan Y, Segal D. Acetabu-lar fractures: clinical outcomes of surgical treatment. Clin Orthop Relat R. 1999;366:205-216.
11. Sahin V, Karakas ES, Aksu S, Atlihan D, Turk CY, Halici M. Traumatic dislocation and fracture-dislocation of the hip: a long term follow-up study. J Trauma. 2003;54(3):520-529.
12. Rosenthal RE, Coker WL. Posterior fracture-dislocation of the hip: an epidemiologic review. J Traum. 1979;19(8):572-581.
13. Bass A, Lovell ME. Two cases of acetabular fractures sustained during competitive cycling. Brit J Sport Med. 1995;29(3):205-206.
14. Epstein HC. Traumatic dislocations of the hip. Clin Orthop.1973;92;116-142.
15. Judet R, Judet J, Letournel E. Fractures of the acetabulum: classifica-tion and surgical approaches for open reduction. J Bone Joint Surg. 1964;46-A(8):1615-1646.
16. Beaulé PE, Dorey FJ, Matta JM. Letournel classification for acetabular fractures: assessment of interobserver and intraobserver reliability. J Bone Joint Surg.2003;85-A(9):1704-1709.
17. Mehta S, Routt ML. Irreducible fracture-dislocations of the femoral head without posterior wall acetabular fracture. J Orthop Trauma. 2008;22(10):686-692.
18. Roffi RP, Matta JM. Unrecognized posterior dislocation of the hip associated with transverse and t-type fractures of the acetabulum. J Orthop Trauma. 1993;7(1):23-27.
19. Pape HC, Rice J, Wolfram K, Gänsslen A, Pohlemann T, Krettek C. Hip dislocation in patients with multiple injuries. Clin Orthop. 2000;377:99-105.
20. Matta JM, Anderson LM, Epstein HC, Hendricks P. Fractures of the acetabulum: a retrospective analysis. Clin Orthop. 1986;205:230-240.
21. Mears DC, Velyvis JH, Chang CP. Displaced acetabular fractures man-aged operatively: indicators of outcome. Clin Orthop. 2003;407:173-186.
22. Sen RK, Veerappa LA. Long-term outcome of conservatively managed displaced acetabular fractures. J Traum. 2009;67(1):155-159.
23. Kebaish AS, Roy A, Rennie, W. Displaced acetabular fractures: long-term follow-up. J Trauma. 1991;31(11):1539-1542.
24. Matta JM. Operative treatment of acetabular fractures through the ilioinguinal approach. Clin Orthop. 1996;305:10-19.
25. Oransky M, Sanguinetts C. Surgical treatment of displaced acetabu-lar fractures: results of 50 consecutive cases. J Orthop Trauma. 1993;7(1):28-32.

international journal of athletic therapy & training january 2013 11
26. Kaempffe FA, Bone LB, Border JR. Open reduction and internal fixation of acetabular fractures: heterotopic ossification and other complica-tions of treatment. J Orthop Trauma. 1991;5(4):439-445.
27. Wright R, Barrett K, Christie MJ, Johnson KD. Acetabular fractures: long-term follow-up of open reduction and internal fixation. J Orthop Trauma. 1994;8(5):397-403.
28. Givens-Heiss DL, Kreabs DE, Riley PO, et al. In vivo acetabular contact pressure during rehabilitation, part II: postacute phase. Phys Ther. 1992;72(10):700-705.
29. Borrelli J, Ricci WM, Anglen JO, Gregush R, Engsberg J. Muscle strength recovery and its effects on outcome after open reduction and internal fixation of acetabular fractures. J Orthop Trauma. 2006;20(6):388-395.
30. Ensberg JR, Steger-May K, Anglen JO, Borrelli J. An analysis of gait changes and functional outcome in patients surgically treated for displaced acetabular fractures. J Orthop Trauma. 2009;23(5):346-353.
Brent I. Smith is pursuing a Doctor of Health Sciences degree from A.T. Still University in Mesa, AZ and is with ATI Physical Therapy in Bolingbrook, IL.
Steven S. Louis is an orthopaedic surgeon with the Hinsdale Ortho-paedic Associates in Hinsdale, IL.
Joe J. Piccininni, EdD, CAT(C), The University of Toronto, is the report editor for this article.