Embed Size (px)
Citation preview

Refuse to Fuse!The development of a nucleus pulposus replacement
Biomimetic hydrogels in load-bearing applications
Gavin Braithwaite
CambridgePolymer Group, Inc.
Testing, Consultation, and Instrumentation for Polymeric Materials
Cambridge Polymer Group, 56 Roland Street, Suite 310
Boston, MA 02129

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 2
Refuse to Fuse!†
• The development of nucleus replacement as a case history for thedevelopment of naturally inspired solutions to surgical problems
• General Outline– The spine and sources of pain– Treatment options– PVA injectable hydrogels - “Thetagels”
• Spine treatment is at a turning-point analogous to the transition from fusion to total hip replacements in the 60’s
Image: http://marbella.to/humour/jun00/evolution.jpg† apologies to the unknown source of the title of the talk

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 3
Bad backs - perspective
• Predominantly a middle-aged issue– 50% of population have degenerative changes in the cervical spine by 50
• Back pain a major impact on the economy– The number one reason for healthcare expenditure– In 1998 $90 billion was spent on back pain– Causes 100 million days of lost work per year– $26 billion in direct back pain costs in 1998
• A serious source of problems for patients– Disables 1.2 million Americans per year– Over 80% of all Americans suffer from back-pain during their life– The second most common reason for visiting the doctor– The most common cause of disability in the US for under 45’s– Are the most significant cause of absenteeism in the US
Sources:Bare Bones. 2004 Weinstein, J.N., et al., United States' Trends and Regional Variations in Lumbar Spine Surgery: 1992-2003. . Spine 2006. 31(23): p. 2707-2714Windsor, R.E. and K.P. Sullivan. Lumbosacral Discogenic Pain Syndrome. 2004 Becker, C., Spine-tingling prospects. Modern Healthcare, 2003. 33(45): p. 30-32.Neckreference.com:- Causes. 2004 .
Image: http://www.holistix-treatments.co.uk

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 4
General spine structure
L5
L1
T12
T1
C7
C1
Cer
vica
lTh
orac
icLu
mba
rSa
crum
Spinal Nerve
Anterior Longitudinal Ligament
Posterior Longitudinal Ligament Vertebral Body
IntervertebralDisc
Lamina
SpinousProcess
Facet
Spinal Chord
Nucleus Pulposus
• The complex structure (hard & soft tissue) of the spine imparts high load bearing properties whilst still allowing motion and cushioning
Annulus Fibrosus
End Plate
Cancellous Bone
Neural Arch
Images: http://www.backpain-guide.comhttp://www.eorthopod.com
NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 5
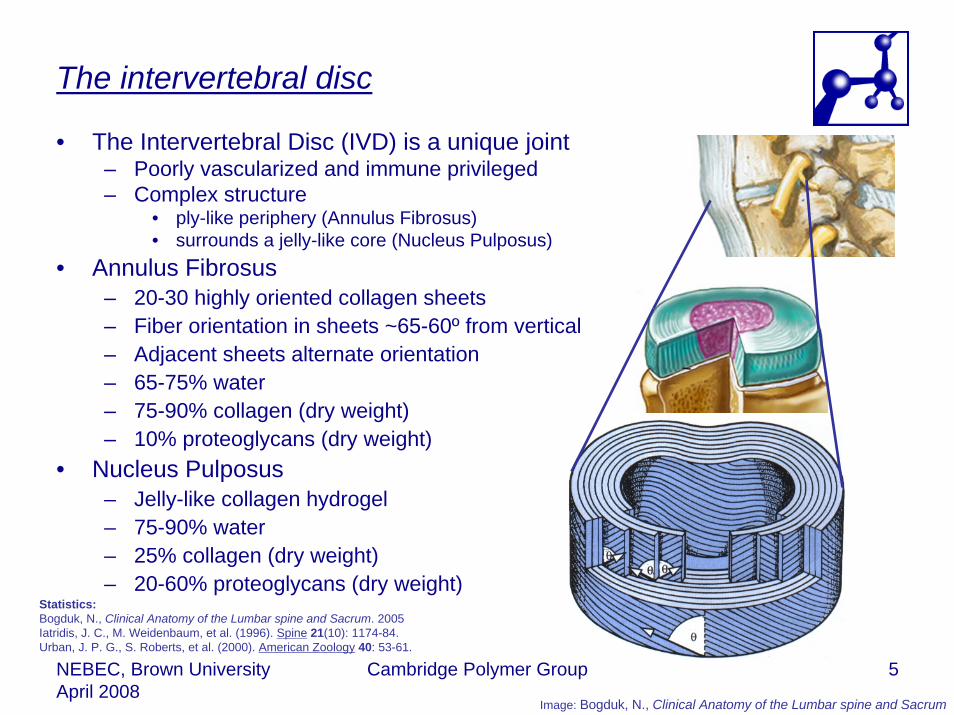
The intervertebral disc
• The Intervertebral Disc (IVD) is a unique joint– Poorly vascularized and immune privileged– Complex structure
• ply-like periphery (Annulus Fibrosus) • surrounds a jelly-like core (Nucleus Pulposus)
• Annulus Fibrosus– 20-30 highly oriented collagen sheets– Fiber orientation in sheets ~65-60º from vertical– Adjacent sheets alternate orientation– 65-75% water– 75-90% collagen (dry weight)– 10% proteoglycans (dry weight)
• Nucleus Pulposus– Jelly-like collagen hydrogel– 75-90% water– 25% collagen (dry weight)– 20-60% proteoglycans (dry weight)
Statistics:Bogduk, N., Clinical Anatomy of the Lumbar spine and Sacrum. 2005Iatridis, J. C., M. Weidenbaum, et al. (1996). Spine 21(10): 1174-84.Urban, J. P. G., S. Roberts, et al. (2000). American Zoology 40: 53-61.
Image: Bogduk, N., Clinical Anatomy of the Lumbar spine and Sacrum
NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 6
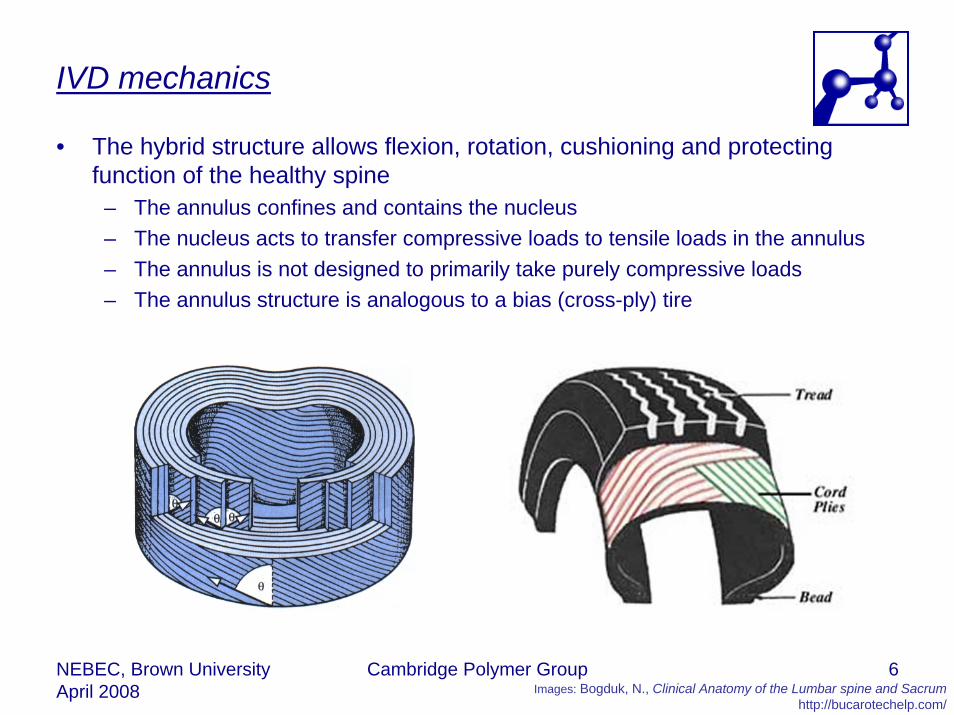
IVD mechanics
• The hybrid structure allows flexion, rotation, cushioning and protecting function of the healthy spine
– The annulus confines and contains the nucleus– The nucleus acts to transfer compressive loads to tensile loads in the annulus– The annulus is not designed to primarily take purely compressive loads– The annulus structure is analogous to a bias (cross-ply) tire
Images: Bogduk, N., Clinical Anatomy of the Lumbar spine and Sacrumhttp://bucarotechelp.com/

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 7
What happens when you have a puncture?
• When the IVD is intact, the loads are transferred from the nucleus to the annular walls
• When the nucleus is removed, or compromised, the loads are purely compressive on the annulus walls.
• This results in annular buckling, facet loading and degeneration
Images: www.savingadvice.com

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 8
The degenerative cascade
• The IVD starts deteriorating from youth– A healthy IVD supports and articulates the spine– IVD is poorly vascularized– Poor nutrition results in cell death– Cells responsible for maintenance of
proteoglycans– Lower hydration results in changed biomechanics– Changed loading damages annulus and
increases risk of herniations– Changed loads reduce disc height – Joint becomes lax and facet joints abnormally
loaded– Changed biomechanics result in bone
remodelling, osteophyte formation and arthrosis– Deterioration also influenced by
• Lifestyle, trauma, genetics, surgery…
Images: www.spineuniverse.com
NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 9
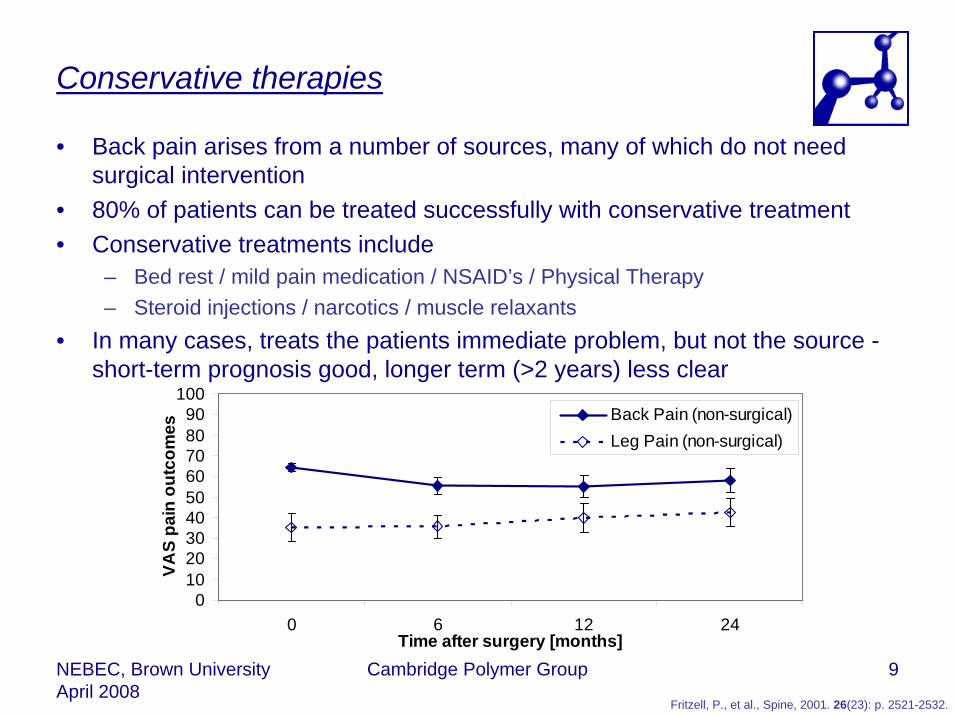
Conservative therapies
• Back pain arises from a number of sources, many of which do not need surgical intervention
• 80% of patients can be treated successfully with conservative treatment• Conservative treatments include
– Bed rest / mild pain medication / NSAID’s / Physical Therapy– Steroid injections / narcotics / muscle relaxants
• In many cases, treats the patients immediate problem, but not the source -short-term prognosis good, longer term (>2 years) less clear
0102030405060708090
100
0 6 12 24Time after surgery [months]
VAS
pain
out
com
es
Back Pain (non-surgical)Leg Pain (non-surgical)
Fritzell, P., et al., Spine, 2001. 26(23): p. 2521-2532.

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 10
Treat the symptom
• Large proportion of disc-related pain results from interaction with nerve root• Most surgical interventions are decompression of the nerve root
– 700,000 annually– Removal of herniated disc tissue (discectomy)– Removal of confining bone (laminectomy)
• Success rates high 50-90% initially– 50%-60% suffer recurring back pain, 20-30% re-suffer sciatica– After 10 years 75% suffer residual back pain, 13% severe
• Treats the symptom, not the cause• Removes material – compromise the disc and joint
Traynelis, V.C., Neurosurgical Focus, 2002. 13(2): p. Article 10.Errico, T.J., Letters to the editor New York Times 2004.
Resnick, D.K., et al., Journal of Neurosurgery: Spine, 2005. 2(6): p. 673-678. Images: http://www.eorthopod.com

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 11
Stop all movement
• Hypothesis: In more degenerated discs, pain comes from the motion – stop that and you have cured the symptom
• Fusion involves permanently fixing two vertebrae together– 320,000 fusions in the US in 2002, 90-95% operative success rates– 70-75% clinical success rates but “major” or “complete” relief from pain in only
50% of patients – “end of the road” for surgical intervention– Long-term, fusion is often no better than discectomy, or conservative therapy
0102030405060708090
100
0 6 12 24Time after surgery
VAS
pain
out
com
esBack Pain (non-surgical)Back Pain (surgical)Leg Pain (non-surgical)Leg Pain (surgical)
Image: healthlibrary.epnet.comFritzell, P., et al., Spine, 2001. 26(23): p. 2521-2532.

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 12
Restore – “Refuse to fuse”
• Spine interventional surgery at the same point as hip-surgery in the 60’s– Gold-standard is fusion – complete prevention of motion to prevent pain– New technologies will allow transition to “motion preservation”
• Total Disc Replacement (TDR)• Equivalent of the step to Total Hip Replacement
– Remove the painful region and replace with a motion segment
• Aggressive surgery• Too much motion?
DePuy Spine Charite
Images: www.spine-health.com

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 13
The treatment “gap”
• There is a set of patients currently poorly addressed by existing treatments• Aging but more active and wealthier demographics encouraging more “life-
enhancing” approaches (less invasive, more mobility, reduced pain)
Mild Moderate Severe
% o
f chr
onic
bac
k pa
in p
opul
atio
n
FusionArtificial disc
Dynamic stabilization
Conservative, non-surgical
DecompressionNucleus replacement
Annulus repair
Severity of disc degeneration
NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 14
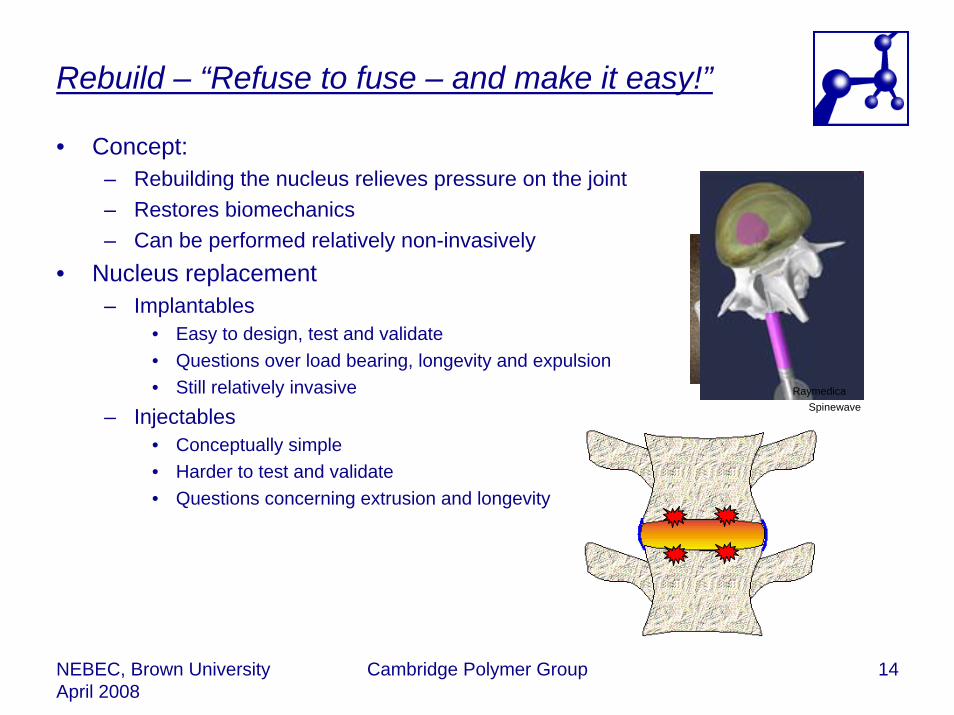
Rebuild – “Refuse to fuse – and make it easy!”
• Concept:– Rebuilding the nucleus relieves pressure on the joint– Restores biomechanics– Can be performed relatively non-invasively
• Nucleus replacement– Implantables
• Easy to design, test and validate• Questions over load bearing, longevity and expulsion• Still relatively invasive
– Injectables• Conceptually simple• Harder to test and validate• Questions concerning extrusion and longevity
RaymedicaSpinewave
NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 15
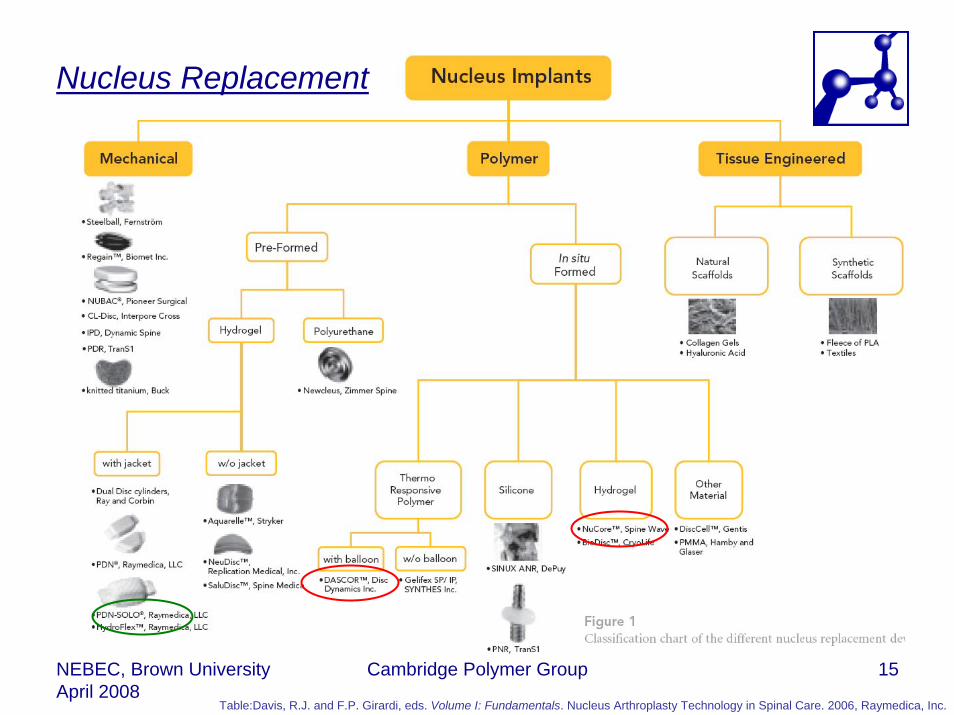
Nucleus Replacement
Table:Davis, R.J. and F.P. Girardi, eds. Volume I: Fundamentals. Nucleus Arthroplasty Technology in Spinal Care. 2006, Raymedica, Inc.

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 16
The ideal candidate
• The ideal candidate nucleus replacement should be– Properties similar to the natural nucleus
• Highly hydrated• Viscoelastic• Inert• Space-filling (even end-plate load distribution)
– Surgically it should also be• Injectable• Radiopaque and/or NMR visible• Revisable• Resist Extrusion/Expulsion• Minimally invasive (as little damage to the annulus as possible)
– An injectable hydrogel

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 17
Concept
NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 18
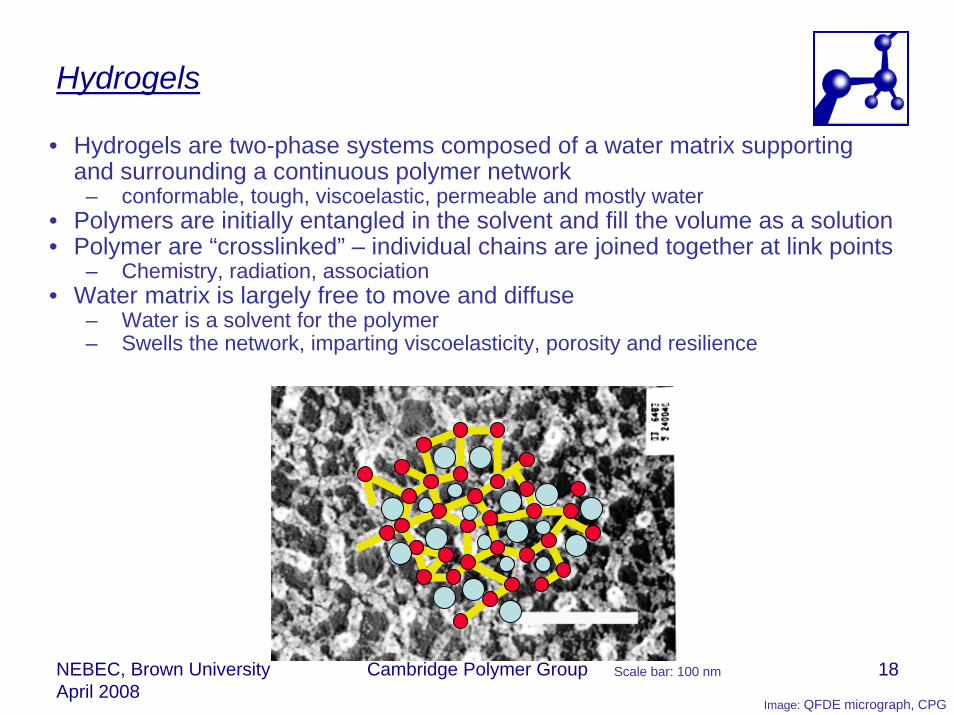
Hydrogels
• Hydrogels are two-phase systems composed of a water matrix supporting and surrounding a continuous polymer network
– conformable, tough, viscoelastic, permeable and mostly water• Polymers are initially entangled in the solvent and fill the volume as a solution• Polymer are “crosslinked” – individual chains are joined together at link points
– Chemistry, radiation, association• Water matrix is largely free to move and diffuse
– Water is a solvent for the polymer– Swells the network, imparting viscoelasticity, porosity and resilience
Scale bar: 100 nm
Image: QFDE micrograph, CPG

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 19
What material?
• Poly(vinyl alcohol) - PVA– Prepared by hydrolysis of poly(vinyl acetate)– Used industrially
• sizing in the textile industry • base gel component for cosmetics industry • as an adherent for the paper industry
– Increasing biomedical applications• opthalmic lubricant • artificial sponges • cartilage and meniscus replacement • nerve guides
– Generally considered non-toxic, blood compatible and non-degradeable
– Hydrophilic– Crystal structure similar to poly(ethylene)
• CHOH group fits into CH2 structure • Unit cell monoclinic with a=7.81 Å, b=2.52
Å (chain axis), c=5.51 Å and b=91°42’• Chains can link through hydrogen bonds
into sheets
Images: Billmeyer, F.W., Textbook of Polymer Science

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 20
Solvent driven gelation of PVA
Single Polymer Chain in solution
Cha
in E
xclu
ded
Volu
me
Solution Temperature
Tθ
Flory Interaction Parameter, 1/χ
χ θ(T, P,..)=1/2
Single Polymer Chain in solution
Cha
in E
xclu
ded
Volu
me
Gaussian distribution
Collapsed chainSwollen, distorted chain
Pol
ymer
Loc
al D
ensi
ty
Solvent “Quality”
“Bad” “Good”“Theta”
Solvent Rich
Polymer Rich
Polymer solution
20 µm
• Polymer solubility is controlled by the chemical potential• Expressed in terms of the solvent “quality”, described by the “Flory
Interaction Parameter”, χ– χ < 0.5 (good solvent) the polymer swells and dissolves– χ > 0.5 (bad solvent) the chain segments prefer to be next to each rather than
to a solvent molecule• Thus manipulation of the solvent can drive a controlled phase separation• And temperature can be used to control the crystallization
Image: ESEM CPG
NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 21
Injectable PVA hydrogels
-80
-60
-40
-20
0
20
40
60
80
100
0% 2% 4% 6% 8% 10% 12% 14% 16% 18% 20% 22% 24%
Mass percentage of ingredient [%]
Swel
l Rat
io (r
elat
ive
tohy
drat
ed) [
%]
Glycine Serine PEG 200Chondroitin NaCl Proline20K PEG PEG 400 Bovine Serum
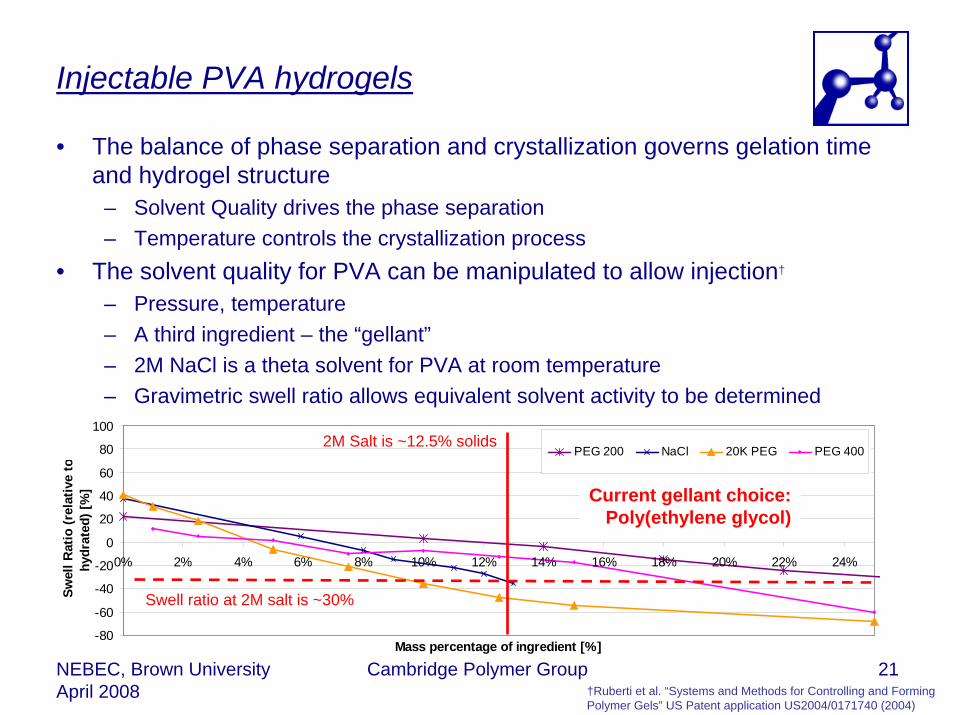
• The balance of phase separation and crystallization governs gelation time and hydrogel structure
– Solvent Quality drives the phase separation– Temperature controls the crystallization process
• The solvent quality for PVA can be manipulated to allow injection†
– Pressure, temperature– A third ingredient – the “gellant”– 2M NaCl is a theta solvent for PVA at room temperature– Gravimetric swell ratio allows equivalent solvent activity to be determined
-80
-60
-40
-20
0
20
40
60
80
100
0% 2% 4% 6% 8% 10% 12% 14% 16% 18% 20% 22% 24%
Mass percentage of ingredient [%]
Swel
l Rat
io (r
elat
ive
tohy
drat
ed) [
%]
PEG 200 NaCl 20K PEG PEG 4002M Salt is ~12.5% solids
Swell ratio at 2M salt is ~30%
Current gellant choice:Poly(ethylene glycol)
†Ruberti et al. “Systems and Methods for Controlling and Forming Polymer Gels” US Patent application US2004/0171740 (2004)
NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 22
• Validation of injectable material as permanent device not straight forward• Biocompatibility/Toxicity
– Industry standards e.g. ISO 10993– All ingredients pharmaceutical excipients
• Mechanical properties – use is unusual for the permanent device industry– Injected
• Must gel “fast” – rheology• Must gel in vivo – no existing tests
– Confined • Need not bear loads on its own – draft standards in development• Space fill and conform• Must not extrude/expulse – no existing tests
– Viscoelastic • Modulus - unconfined compression (stress-strain)• Fatigue testing rate sensitive – draft standards in development
– Hydrated• Must recognize impact of gelation environment – no existing tests• Must measure water contents (“Equilibrium Water Content”)
• Validation of injectable material as permanent device not straight forward• Biocompatibility/Toxicity
– Industry standards e.g. ISO 10993– All ingredients pharmaceutical excipients
• Mechanical properties – use is unusual for the permanent device industry– Injected
• Must gel “fast”• Must gel in vivo
– Confined • Need not bear loads on its own• Space fill and conform• Must not extrude/expulse
– Viscoelastic • Modulus - unconfined compression (stress-strain)• Fatigue testing rate sensitive
– Hydrated• Must recognize impact of gelation environment • Must measure water contents (“Equilibrium Water Content”)
Validation as a medical device
NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 23
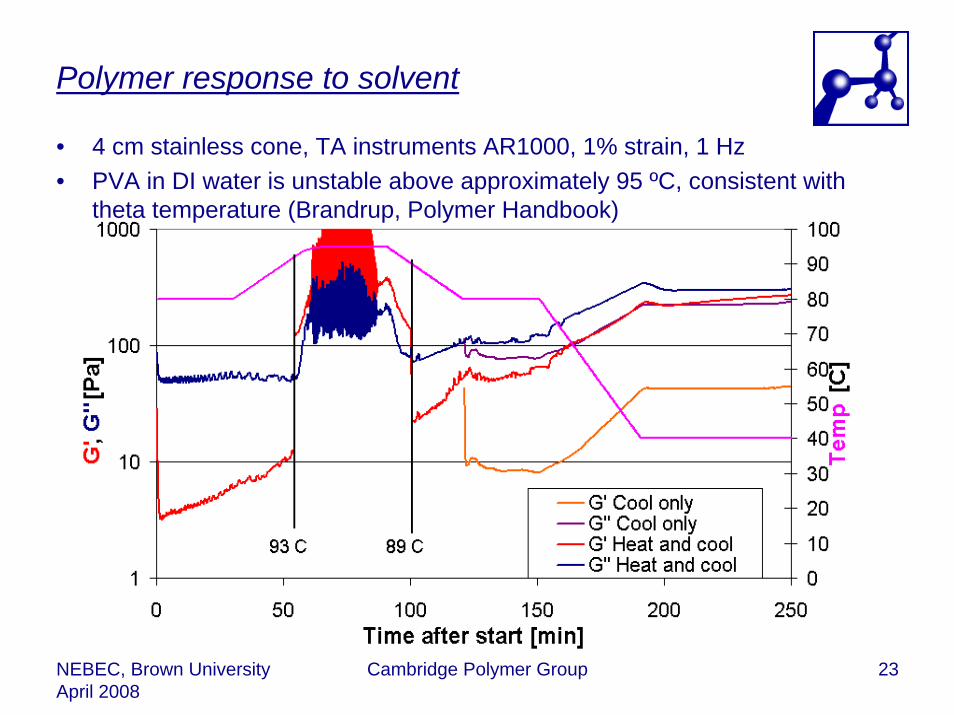
Polymer response to solvent
• 4 cm stainless cone, TA instruments AR1000, 1% strain, 1 Hz• PVA in DI water is unstable above approximately 95 ºC, consistent with
theta temperature (Brandrup, Polymer Handbook)
NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 24
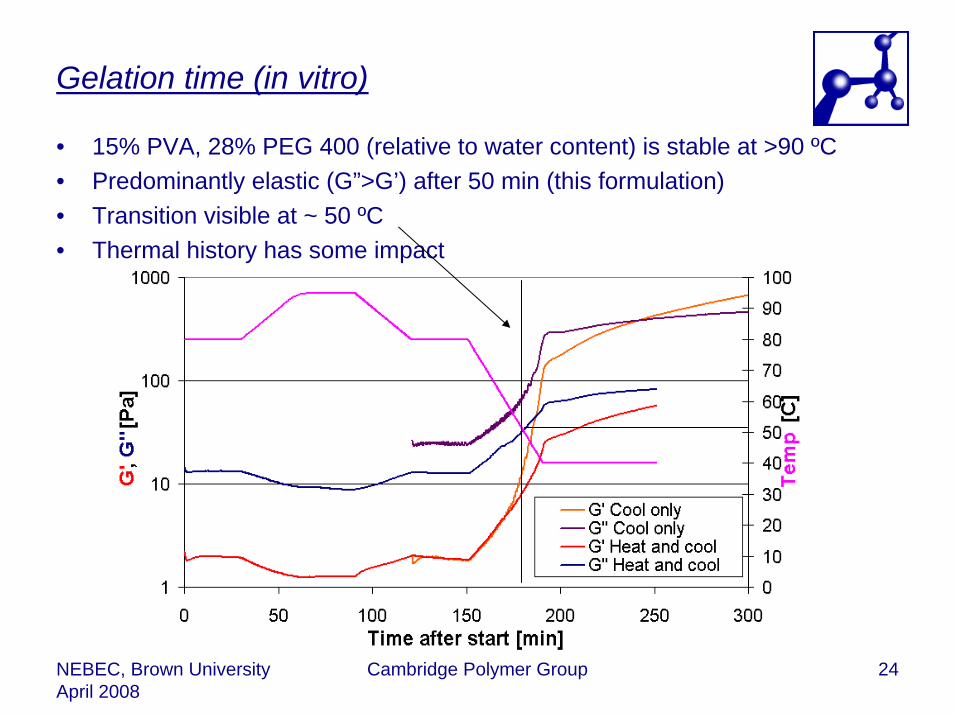
Gelation time (in vitro)
• 15% PVA, 28% PEG 400 (relative to water content) is stable at >90 ºC• Predominantly elastic (G”>G’) after 50 min (this formulation)• Transition visible at ~ 50 ºC• Thermal history has some impact

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 25
Impact of environment (in vitro)
• The hydrated environment in vivo must impact an injectable hydrogel formulation through
– Diffusion out of active ingredients (polymer, gellant, crosslinker)– Diffusion in of water and bodily fluids (dilution)
• 5% Agar hydrogel at 40 ºC used as model for in vivo environment
FailLittle opacity
Diffuse interface
PassCompletely opaque
Sharp interface

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 26
Impact of environment (ex vivo)
• Porcine vertebral column with excess tissue removed• Denucleated using commercial tool (Hydrocision)• Bleed needle used to relieve pressure• Entire column immersed in DI water for 4 hours at 40 ºC• Hydrogel injected at 40 ºC and submerged for one day
Bleed needle
Hydrogel in 5 ml syringe
Gelled hydrogel after 1 day
Gelled hydrogel after 1 day
Dissected IVD

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 27
Injectability
• Critical for a surgical application that the material is injectable• Empirically a surgeon can exert a force of up to ~150 N• The complex gelling polymer solution is not a simple Newtonian solution,
therefore injection forces difficult to predict a priori• Injection force measurement
– Custom fixture– Standard load-frame– 16G needle and 5 ml syringe
Polyethylene standoff
500 N load cell Linear
actuator
Acrylic tube
5 mL syringe
16 gauge needle0
50
100
150
200
0 5 10 15 20Time (s)
Forc
e (N
)
PassFail
NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 28
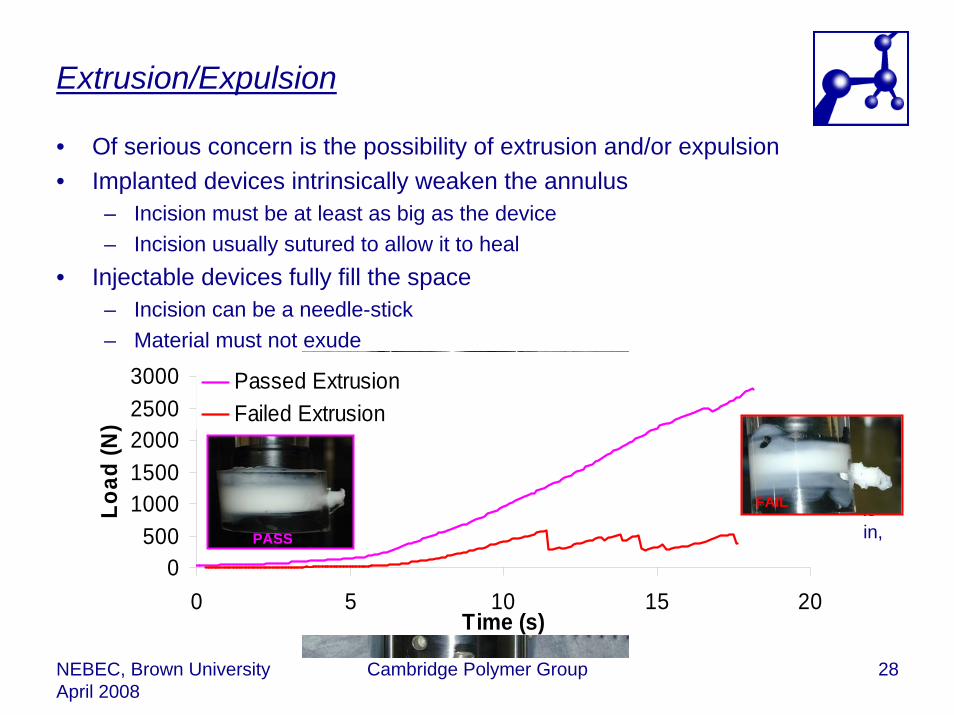
Extrusion/Expulsion
• Of serious concern is the possibility of extrusion and/or expulsion• Implanted devices intrinsically weaken the annulus
– Incision must be at least as big as the device– Incision usually sutured to allow it to heal
• Injectable devices fully fill the space– Incision can be a needle-stick– Material must not exude
Rigid container with plunger connected to load-frame. Load to 3000 N at 5 mm/min, 5 mm hole.
Orifice
Piston within acrylic sheath
0500
10001500200025003000
0 5 10 15 20Time (s)
Load
(N)
Passed ExtrusionFailed Extrusion
PASS
FAIL

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 29
Fatigue
• Fatigue testing is critical for biomedical materials– Conventional materials (PE, SS etc) have well developed techniques– Soft-solids do not– For an injectable nucleus replacement there are further problems
• Works in tandem with an “intact” annulus• (May) require hydration and fluid access• Must resist expulsion through pin-holes and orifices• Deformation is extremely complex (flexion/extension/rotation/compression/tension)
– Propose simpler model initially
Inst
ron

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 30
Confined compression fatigue
• Complete testing system and protocol under development in-house• RTV annulus based on ASTM guidance document• Porous end-plates (membrane supported by porous frit) to allow water
access• 40 ºC, 2750N ± 250N, 1Hz • Hydrogel gelled in situ,
injected through hole• Strain determined from
average displacement• Modulus determined from
displacement amplitude5 mm hole
Nucleus cavityRTV Annulus
Porous end-platesMembrane
NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 31
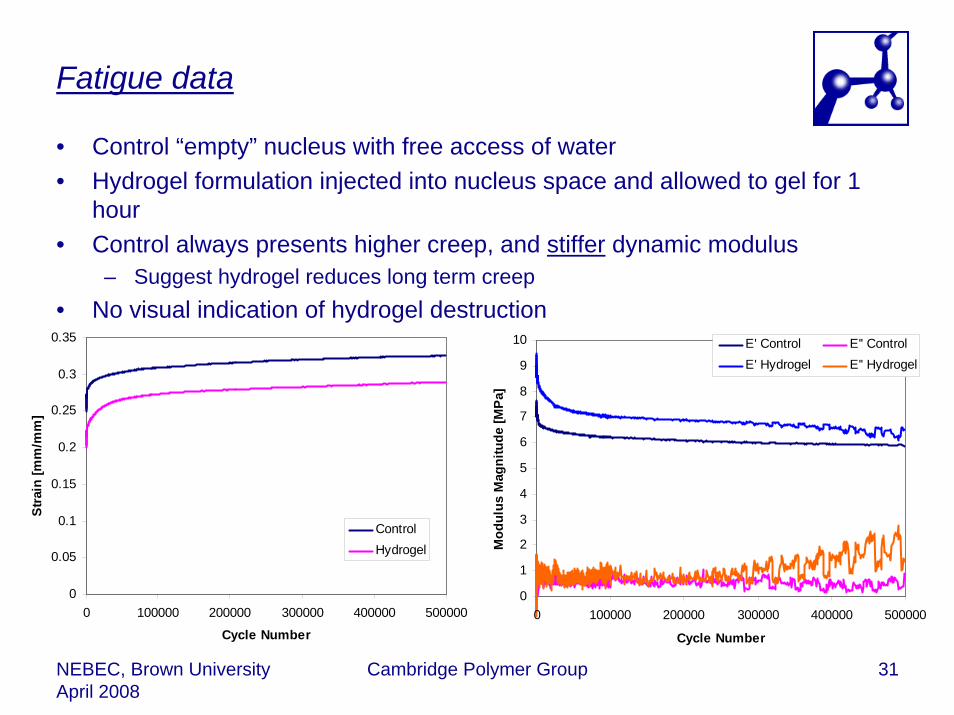
Fatigue data
• Control “empty” nucleus with free access of water• Hydrogel formulation injected into nucleus space and allowed to gel for 1
hour• Control always presents higher creep, and stiffer dynamic modulus
– Suggest hydrogel reduces long term creep• No visual indication of hydrogel destruction
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0 100000 200000 300000 400000 500000
Cycle Number
Stra
in [m
m/m
m]
ControlHydrogel
0
1
2
3
4
5
6
7
8
9
10
0 100000 200000 300000 400000 500000
Cycle Number
Mod
ulus
Mag
nitu
de [M
Pa]
E' Control E'' ControlE' Hydrogel E'' Hydrogel
NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 32
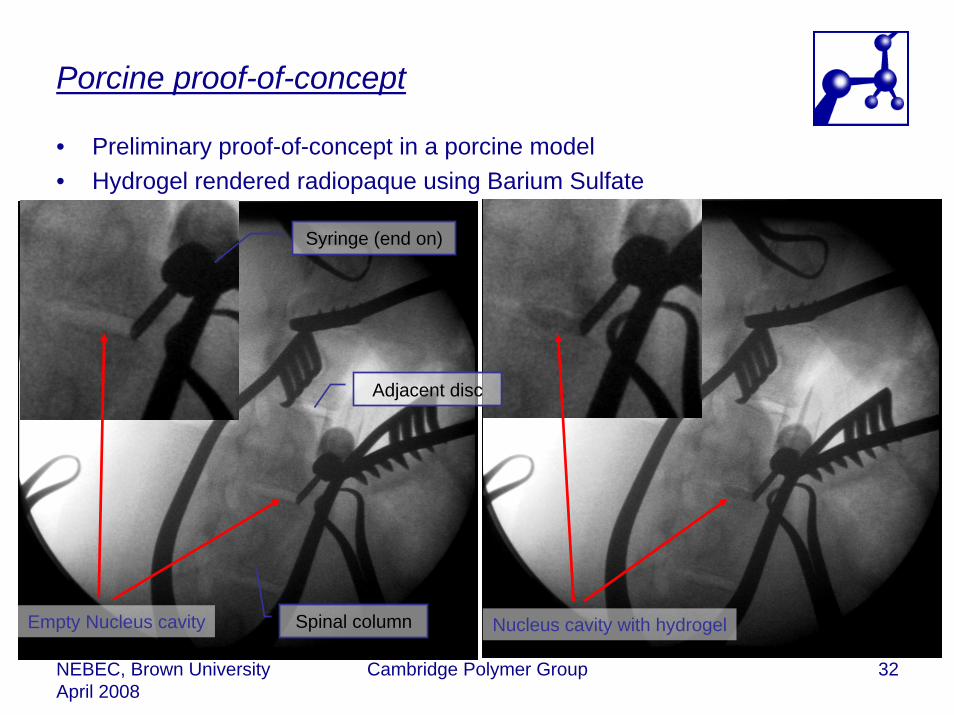
Porcine proof-of-concept
• Preliminary proof-of-concept in a porcine model• Hydrogel rendered radiopaque using Barium Sulfate
Empty Nucleus cavity Nucleus cavity with hydrogelSpinal column
Syringe (end on)
Adjacent disc

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 33
Where next…
• Injectable hydrogels hold great promise for nucleus replacement strategies– Hydrated, permeable, viscoelastic– Minimally invasive, easily revised
• PVA hydrogels have a proven biomedical track record– Inert and biocompatible– Good mechanical properties– Highly hydrated
• The techniques developed by CPG yield an exceptional opportunity to use an existing material in a expanding medical indication
• But…– Developing suitable tests is non-trivial– Challenge is to find a suite of tests that are relevant to the application
• Confined deformation• Hydrated environment and material
• Next…– Long term fatigue and quantitative determination of hydrogel aging– Further in vivo safety and longevity studies

NEBEC, Brown UniversityApril 2008
Cambridge Polymer Group 34
Acknowledgements
• Everyone at Cambridge Polymer Group– In particular Jason Berlin (bulk of experimental work)
• Lou Jenis at the Boston Spine Group• Questions:
– Gavin Braithwaite ([email protected])– Cambridge Polymer Group– 56 Roland Street, Suite 310– Boston. MA 02129


















![Puerarin Relieved Compression-Induced Apoptosis and ...downloads.hindawi.com/journals/sci/2020/7126914.pdfimpaired nucleus pulposus cell (NPC) proliferation [4]. Nucleus pulposus mesenchymal](https://img.pdfslide.us/doc/110x75/5f7fa24ee6184370f175b23e/puerarin-relieved-compression-induced-apoptosis-and-impaired-nucleus-pulposus.jpg)


![The protective effects of PI3K/Akt pathway on human nucleus pulposus … · 2020. 1. 28. · nucleus pulposus cells and nucleus pulposus progenitor cells [14]. Previous studies have](https://img.pdfslide.us/doc/110x75/60b265dd0d8b8040e758b496/the-protective-effects-of-pi3kakt-pathway-on-human-nucleus-pulposus-2020-1-28.jpg)






