Embed Size (px)
Citation preview

Int J Clin Exp Pathol 2014;7(12):8520-8531www.ijcep.com /ISSN:1936-2625/IJCEP0003306
Original ArticleNucleus pulposus cells derived IGF-1 and MCP-1 enhance osteoclastogenesis and vertebrae disruption in lumbar disc herniation
Zhongjiao Zhu1,6*, Peng Huang2*, Yanxue Chong1, Suraj K George3, Bingtao Wen1, Na Han4, Zhiqiang Liu5, Lixin Kang1, Nie Lin6
1Department of Orthopedics, Tenzhou Central People’s Hosipital, Tenzhou 277500, Shandong, China; 2Department of Emergency, Tengzhou Hospital of Traditional Chinese Medicine, Tengzhou 277500, Shandong, China; 3Department of Hematopathology, The University of Texas MD Anderson Cancer Center, Houston 77054, Texas, USA; 4Department of Orthopedics, Peking University People’s Hospital, Beijing 100029, China; 5Division of Medicine, Center for Cancer Immunology Research, The University of Texas M D Anderson Cancer Center, Houston 77054, Texas USA; 6Department of Orthopedics, Shandong University Qilu Hospital, Jinan, Shandong, 250012, China. *Equal contributors.
Received October 21, 2014; Accepted December 1, 2014; Epub December 1, 2014; Published December 15, 2014
Abstract: Study design: Chronic strained lumbar disc herniation (LDH) cases were classified into bulging LDH, her-niated LDH and prolapse LDH types according to imaging examination, and vertebrae disruptions were evaluated. Cytokines derived from the nucleus pulposus cells were detected, and their effects on osteoclastogenesis, as well as the mechanisms involved, were studied via an in vitro osteoclast differentiation system. Objective: To clarify the mechanisms of lumbar vertebrae resorption induced by lumbar herniation. Summary and background data: Chronic strained lumbar disc herniation induced vertebrae erosion exacerbates quality of patients’ life and clinical outcome. Although nucleus pulposus cells derived cytokines were reported to play an important role in this pathogenesis, the fundamental mechanisms underlying this process are still unclear. Methods: Chronic strained lumbar disc hernia-tion patients were diagnosed with CT scan and T2-weighted magnetic resonance imaging. RNA was extracted from 192 surgical specimens of the herniated lumbar disc and 29 surgical excisions of the lumbar disc from spinal injury patients. The expressions of osteoclastogenesis related cytokines and chemokines were examined using real time PCR. Monocytes were induced into osteoclast with M-CSF and RANKL in vitro, while the IGF-1 and MCP-1 were added into the differentiation procedure in order to evaluate the effects and explore the molecular mechanisms. Results: Vertebrae erosion had a positive relationship with lumbar disc herniation severity types. In all of the os-teoclastogenesis related cytokines, the IGF-1 and MCP-1 were the most highly expressed in the nucleus pulposus cells. IGF-1 enhances activation of NF-kB signaling directly, but MCP-1 upregulated the expression of RANK, so that enhanced cellular sensitivity to RANKL resulted in increasing osteoclastogenesis and activity. Conclusion: Lumbar herniation induced overexpression of IGF-1 and MCP-1 in nucleus pulposus cells aggravated vertebral erosions. Hence, this study suggests that targeting osteoclastogenesis related cytokines has potential clinical significance in the treatment of lumbar disc herniation patients.
Keywords: Lumbar disc herniation, vertebra disruption, IGF-1, MCP-1, osteoclast
Introduction
Spine-related disorders are among the most frequently encountered clinical condition in medicine. In western countries, low back pain (LBP) alone affects up to 80% of the population in their lifetime, with an annual prevalence of about 15% to 20%. The estimated annual expenditure for the care of low back problems
was more than $85 billion in the United States [1, 2]. In China, the LBP prevalence annually is about 8%, however, the overall cost of low back pains may amount to $100 billion due to the huge population base [3]. Low back pain and sciatica caused by lumbar disc herniation (LDH) are the most common causes of activity limita-tion and visits to physicians [4, 5]. LDH occurs when the nucleus in the center of the disc
Nucleus pulposus cells and osteoclastogenesis
8521 Int J Clin Exp Pathol 2014;7(12):8520-8531
presses against the annulus, causing the disc to bulge outward; the most common site is toward the bottom of the spine at L4-L5 or L5-S1 [6]. With further progress, the nucleus herniates completely through the annulus and squeezes out of the disc, placing pressure on the spinal canal or nerve roots [7]. In addition, the nucleus releases chemicals that can irritate the surrounding nerves, causing inflammation and pain [8].
Degeneration of the lumbar disc nucleus and chronic strain are the fundamental and domi-nant reasons for LDH, although the etiology is multifactorial, which includes environmental, nutritional, lifestyle, and occupational factors [9]. Degenerative changes in the fibrocartilagi-nous intervertebral disc (IVD) lead to a loss of structural integrity in the surrounding annulus fibrosus (AF), which can lead to herniation of the nucleus pulposus (NP). Biologically, disc cells in the AF and NP actively regulate IVD homeostasis, maintaining balance between anabolic and catabolic processes. This involves modulating their activity through a variety of substances, including enzymes, cytokines, enzyme inhibitors, and growth factors [10]. Anabolic regulators include polypeptide growth factors, such as insulin-like growth factor (IGF), transforming growth factor-β (TGF-β) and the bone morphogenetic proteins (BMPs), while catabolic mediators include various cytokines, enzymes, and aggrecanases [11]. LDH may result from an imbalance between these bio-
sand rat lumbar spine, vertebral endplate archi-tecture, and the utility of this model for autolo-gous disc cell implantation. Radiographic and histologic changes in the aging sand rat are very similar to those seen in human disc degen-eration [14]. It is hypothesized that experimen-tal discus lesion would initiate not only local-ized bone remodeling but also increase osteo-clast formation in a location remote to the injury site, due to altered spinal biomechanics. It is speculated that these changes in vertebral bone remodeling could be reflected by an increased RANKL expression [15]. The mecha-nism of vertebral destruction appears to be more complex than what is known, but remains unclear. We studied the effects of NP cells-derived cytokines on osteoclastogenesis and the mechanisms of bone resorption via in vitro osteoclast differentiation system.
Material and methods
Patients
192 patients were recruited between December 2010 to September 2012 from the Peking University People’s Hospital, Dalian University Zhongshan Hospital, Dalian Medical University Second Affiliated Hospital and Tengzhou People’s Central Hospital. All patients under-went a standardized history and physical exam-ination. Inclusion criteria were: recent low back pain (within 3 months), and available magnetic resonance imaging (MRI) demonstrating LDH corresponding to the neurological level and side suggested at the clinical presentation.
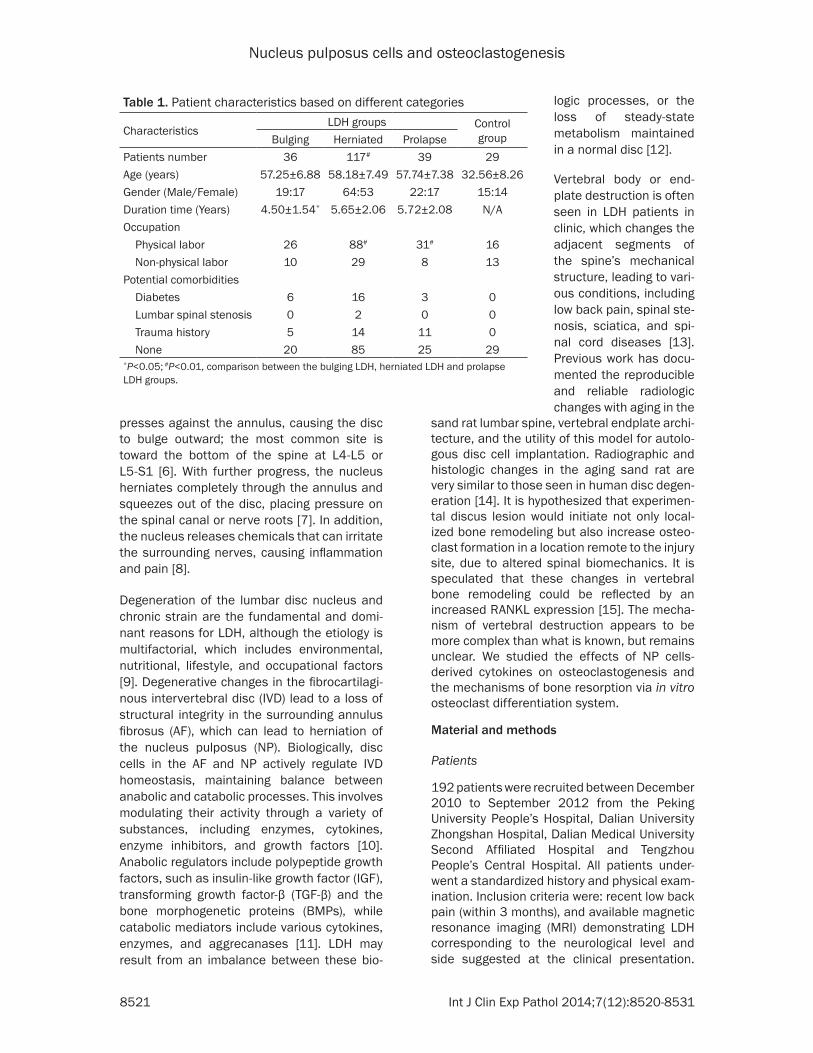
Table 1. Patient characteristics based on different categories
CharacteristicsLDH groups Control
groupBulging Herniated ProlapsePatients number 36 117# 39 29Age (years) 57.25±6.88 58.18±7.49 57.74±7.38 32.56±8.26Gender (Male/Female) 19:17 64:53 22:17 15:14Duration time (Years) 4.50±1.54* 5.65±2.06 5.72±2.08 N/AOccupation Physical labor 26 88# 31# 16 Non-physical labor 10 29 8 13Potential comorbidities Diabetes 6 16 3 0 Lumbar spinal stenosis 0 2 0 0 Trauma history 5 14 11 0 None 20 85 25 29*P<0.05; #P<0.01, comparison between the bulging LDH, herniated LDH and prolapse LDH groups.
logic processes, or the loss of steady-state metabolism maintained in a normal disc [12].
Vertebral body or end-plate destruction is often seen in LDH patients in clinic, which changes the adjacent segments of the spine’s mechanical structure, leading to vari-ous conditions, including low back pain, spinal ste-nosis, sciatica, and spi-nal cord diseases [13]. Previous work has docu-mented the reproducible and reliable radiologic changes with aging in the
Nucleus pulposus cells and osteoclastogenesis
8522 Int J Clin Exp Pathol 2014;7(12):8520-8531
Exclusion criteria were: known pregnancy; severe active medical or psychiatric comorbidi-ties that would limit study participation; infec-tious, inflammatory, or neoplastic cause of radiculopathy; significant degenerative or isth-mic spondylolisthesis suspected of contribut-ing to symptoms; and prior lumbar spine sur-gery at the affected level. The normal control group comprised of 29 patients, who suffered from acute vertebral burst fractures caused by violence. There was no history of back pain and lumbar spine MRI showed no pathology or signs of lumbar disc degeneration. All subjects signed the informed consent. The characteristics of the patients involved were summarized in the Table 1.
These patients were divided into three groups based on Computed Tomography, T1- and T2-weighted MRI imaging: the bulging lumbar disc herniation group (Bulging LDH), the herni-ated lumbar disc herniation group (Herniated LDH) and the prolapse lumbar disc herniation group (Prolapse LDH). The study was approved by the Medical Research Ethics Committee of Dalian Medical University and Peking University.
Quantitative real-time PCR
Nucleus pulposus samples from the patients were procured and rinsed thoroughly by icy 1×PBS immediately after biopsy, removed of annulus fibrosus, cut into the size of 1×1×1
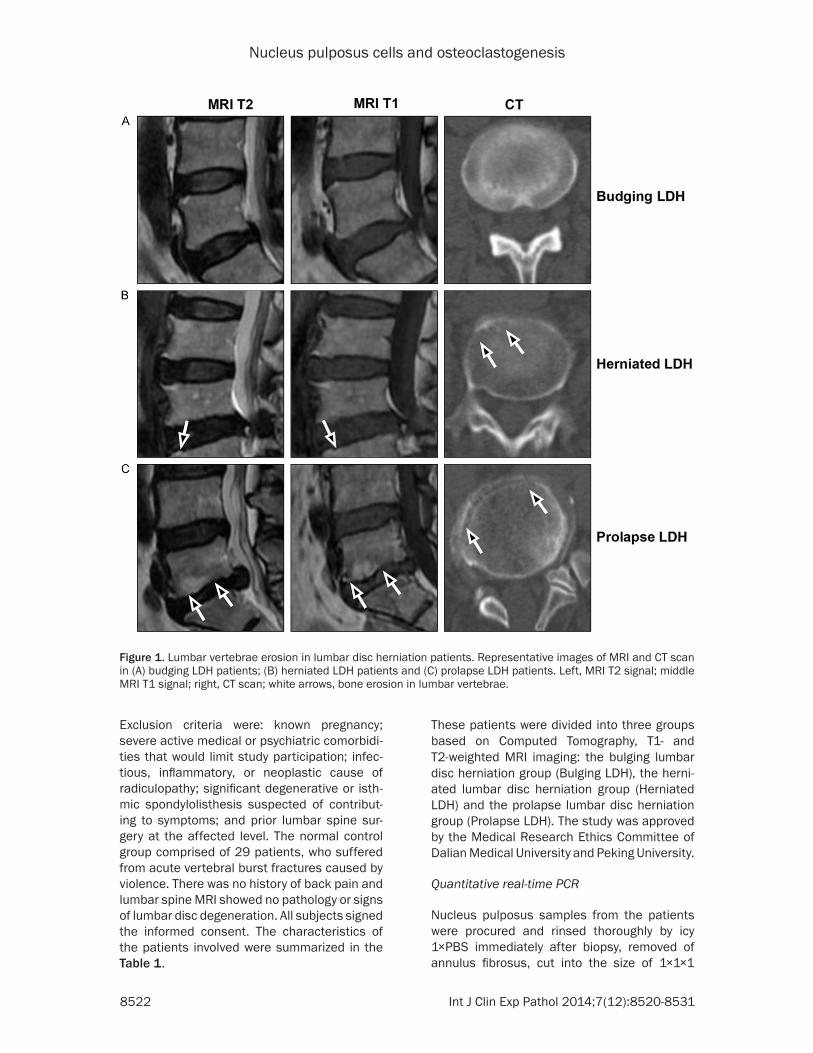
Figure 1. Lumbar vertebrae erosion in lumbar disc herniation patients. Representative images of MRI and CT scan in (A) budging LDH patients; (B) herniated LDH patients and (C) prolapse LDH patients. Left, MRI T2 signal; middle MRI T1 signal; right, CT scan; white arrows, bone erosion in lumbar vertebrae.

Nucleus pulposus cells and osteoclastogenesis
8523 Int J Clin Exp Pathol 2014;7(12):8520-8531
mm, quickly placed in liquid nitrogen and then stored at -80°C until RNA extraction. Total RNA was isolated with the TRIzol reagent (Invitrogen, CA). An aliquot of 1 μg of total RNA was sub-jected to reverse transcription with SuperScript II RT PCR kit (Invitrogen, CA). 1 μL of the final cDNA was applied to real-time PCR amplifica-tion with SYBR Green using the StepOnePlus real-time PCR system (Invitrogen, ABI, CA) abnd the listed primers (Supplemental Table 1).
Western blotting
Cells were harvested and lysed with lysis buffer (Cell Signaling Technology, MA). Cell lysates were subjected to SDS-PAGE, transferred to a polyvinylidene difluoride membrane and immu-noblotted with antibodies against phosphory-lated or nonphosphorylated NF-ĸB, p38, ERK, JNK, and AKT. The membrane was stripped and reprobed with anti-β-actin antibody (Sigma-Aldrich, MO) to ensure equal protein loading. Secondary antibodies conjugated to horserad-ish peroxidase were used for detection, fol-lowed by enhanced chemiluminescence (Pierce Biotechnology, IL) and autoradiography.
Flow cytometry
After treatment, cultured cells were washed twice with 1×PBS, blocked with human FcR binding inhibitor, then stained with 2 µg of phy-coerythrin-conjugated RANK antibody (eBiosci-ence, CA) at RT for 30 minutes, avoiding light, and finally analyzed with a FACS Calibur flow cytometer.
Differentiation
Peripheral blood mononuclear cells (PBMCs) were isolated using Ficoll-Paque (GE Healthcare) density gradient centrifugation. 1×106 PBMCs per well were seeded in 24-well plates and allowed to adhere for two hours in RPMI-1640 (Mediatech Cellgro). Cells were washed three
times with fresh medium to remove the non-adherent cells. The adherent PBMC cells were cultured in α-MEM (Gibco) supplemented with 10% fetal bovine serum (Hyclone), 100 units/ml penicillin, 100 μg/ml streptomycin, 50 ng/mL human RANKL (R&D Systems), and 25 ng/mL human M-CSF (R&D Systems) (Osteoclast conditioned medium, OCM). OCM was changed every three days. After twelve days of culture, TRAP staining of OCs was performed with Leukocyte Acid Phosphatase kit (Sigma-Aldrich) according to the manufacturer’s instructions.
TRAP staining and TRACP activity
The enzymatic marker of osteoclasts, TRAP was stained using a leukocyte acid phospha-tase kit (Sigma-Aldrich) following the manufac-turer’s instructions. Briefly, differentiated osteoclast cells were fixed with citrate/acetone solution and stained with acetate/naphthol/tartrate solution at 37°C for one hour, and final-ly the nuclei were stained with hematoxylin at room temperature for 5 minutes. Differentiated cells with characteristics of TRAP staining posi-tive, three or more nuclei and a cell body larger than 100 mm were considered to be osteo-clasts. The osteoclast enzyme marker, tartrate-resistant acid phosphatase (TRACP), was detected using a TRACP and ALP Assay kit (Takara, Clontech).
Statistical analysis
Experimental values are expressed as mean ± standard error of the mean unless otherwise indicated. The chi-square test was used for cat-egorical variables and the Student’s t-test or One-way ANOVA was used to compare the dif-ferences between groups. Statistical signifi-cance was analyzed using SPSS 10.0 software and a P value <0.05 was considered statisti-cally significant. All results obtained were from at least three independent experiments.
Table 2. Patient characteristics based on types of LDH
LDH type Total casesBone Disruption Total
positive Ratio (%) P- + ++ +++
LDH groups Bulging 36 35 1 0 0 1 2.8%Herniated 117 19 35 43 20 98 84% 0.001#
Prolapse 39 2 8 12 17 37 95% 0.001#, 0.01*
#, P<0.001, Herniated/Prolapse group vs. Bulging group; *, P<0.01, Prolapse group vs. Herniated group.

Nucleus pulposus cells and osteoclastogenesis
8524 Int J Clin Exp Pathol 2014;7(12):8520-8531
Results
Patient characteristics
192 patients were eligible to participate in this study. In patients enrolled in the current study, the mean age was 57.83±7.25 years (range
47-82 years). The male to female ratio was 105:87. The mean duration of low back pain was 5.29±1.89 years (range 1-10 years). The distribution of type of herniation: bulging LDH in 36 patients; herniated LDH in 117 patients; and prolapse LDH in 39 patients. These patients were divided into three groups accord-
Figure 2. Expression profile of osteoclastogenesis-associated cytokines in the herniated disc. Real-time PCR show-ing relative expressions of OC differentiation-associated cytokines (A) IGF-1 and (B) MCP-1 in lumbar disc nucleus pulposus cells.
Figure 3. Effects of IGF-1 on osteoclast (OC) differentiation from monocytes. A. TRAP staining for mature OCs in monocytes cultured in medium with M-CSF (25 ng/ml) and RANKL (50 ng/mL), in presence or in absence of IGF-1. B. Quantitative analysis of mature OCs generated from cocultures of monocytes with different dosage of IGF-1. Rep-resentative results from five independent experiments are shown. C. Real-time PCR showing enhanced expression of OC differentiation-associated proteins CTSK, TRAP, CALCA, and CALCR in monocytes cultured with the addition of RANKL and different dosage of IGF-1, compared with those in monocytes cultured with medium or RANKL only. *P≤0.05; **P≤0.01.
Nucleus pulposus cells and osteoclastogenesis
8525 Int J Clin Exp Pathol 2014;7(12):8520-8531
ing to different CT, MRI and pathology represen-tation as the bulging, herniated, and prolapse LDH groups. The percentages were 18.7%, 60.9%, and 20.3% respectively, in which the herniated LDH serves as the dominant type of LDH compared to the other types (P<0.01). The mean age of the bulging, herniated, and pro-lapse LDH groups were 57.25±6.88, 58.18±7.49, and 57.74±7.38 years respective-ly, and there was no significant difference between these groups (P>0.05). The male to female ratio was 19:17, 64:53, and 22:17 respectively, and no significance was found between groups. The average duration of low back pain from the onset of symptoms to sur-gery was 4.50±1.54 years in the bulging LDH group, 5.65±2.06 years in the herniated LDH group and 5.72±2.08 years in the prolapse group. There were significant differences between the bulging LDH and other two groups (P<0.05), however, there was no significant dif-ference between the herniated and prolapse LDH groups (P>0.05). With respect to employ-
ment status, the ratio of patients who are undertaking physical labor, was significantly higher in the herniated and prolapse groups compared to the bulging LDH group (P<001). In total twenty seven patients (14.06%) had potentially contributing comorbidities such as lumbar spinal stenosis and diabetes. Thirty patients (15.6%) had a history of trauma before the onset of their symptoms. Twenty nine patients of the control group, who all survived severe vehicle accidents and had undergone lumbar disc surgical removal, were not ana-lyzed in the characteristics categories because they only served as the source of specimen RNA extraction in the later experiments (Table 1).
MRI and CT appearance
To classify the clinical appearance and pathol-ogy type and find the relationship between lum-bar herniation and bone resorption in lumbar vertebrae, all patients enrolled in this study underwent T1- and T2-weighted magnetic reso-
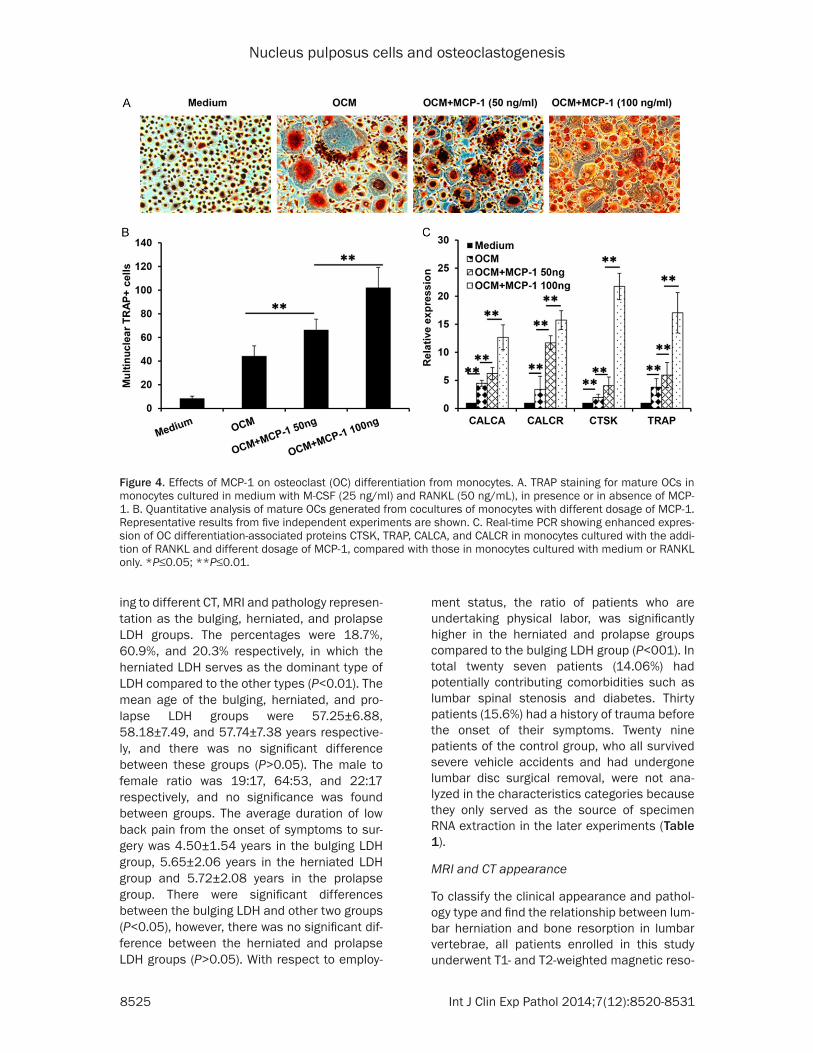
Figure 4. Effects of MCP-1 on osteoclast (OC) differentiation from monocytes. A. TRAP staining for mature OCs in monocytes cultured in medium with M-CSF (25 ng/ml) and RANKL (50 ng/mL), in presence or in absence of MCP-1. B. Quantitative analysis of mature OCs generated from cocultures of monocytes with different dosage of MCP-1. Representative results from five independent experiments are shown. C. Real-time PCR showing enhanced expres-sion of OC differentiation-associated proteins CTSK, TRAP, CALCA, and CALCR in monocytes cultured with the addi-tion of RANKL and different dosage of MCP-1, compared with those in monocytes cultured with medium or RANKL only. *P≤0.05; **P≤0.01.

Nucleus pulposus cells and osteoclastogenesis
8526 Int J Clin Exp Pathol 2014;7(12):8520-8531
nance imaging (MRI) examination and comput-ed tomography (CT) scan. As shown in the Figure 1, the representative images of patients with lumbar disc herniation demonstrated a mass in the posterior epidural space, at the L2-L3 level. The lesion exhibited low intensity on T1-weighted MRI and high and low intensi-ties on T2-weighted MRI. Different types showed different characteristics; for the bulg-ing LDH, both the T1- and T2-weighted MRI images showed the backward shift of the nucle-us, but all behind the posterior longitudinal liga-ment; signals for the disc inferior endplate were all even, and intervertebral disc boundaries were clear; on the MRI T2-weighted images, disc intensity signal decreased slightly. In the herniated LDH, the backward shifts of the nuclei were prominent and broke through the
posterior longitudinal ligament; disc intensity signal decreased significantly on the MRI T2-weighted images; signals for the disc inferi-or endplate were heterogeneous, intervertebral disc boundaries were rough, and the vertebra body also became lower. In the prolapse LDH, the backward shift of the nucleus broke through the posterior longitudinal ligament and discon-nected with discs, the signals for both side end-plates of discs were extremely rough, disc intensity signal decreased to black on the MRI T2-weighted images, and intervertebral spaces became narrow (Figure 1).
With regard to vertebra disruption, CT scans showed that in the bulging LDH groups no obvi-ous disruptions were found in most of the cases. Of all the 36 patients recruited in this
Figure 5. Mechanistic studies of the enhancing effects of IGF-1 and MCP-1 on osteoclastogenesis. A. Western blot showing upregulated levels of phosphorylated PI3K, STAT5, AKT and NK-kB in monocytes cultured with the OCM in addition of IGF-1, β-actin served as a protein loading control. B. Western blot showing upregulated levels of phos-phorylated PLCg1, ERK1/2, P38, and CREB, as well as the protein level of RANK in OCM with or without MCP-1, β-actin served as a protein loading control. C. Real-time PCR showed the dose dependent enhanced expression of RANK in monocytes cultured with different dosages of MCP-1. D. Flow cytometry showed the protein level of RANK due to MCP-1 treatment. Representative results from five independent experiments are shown. *P≤0.05; **P≤0.01.

Nucleus pulposus cells and osteoclastogenesis
8527 Int J Clin Exp Pathol 2014;7(12):8520-8531
study, only one disc showed slight disruption extending into the inner annulus (Grade 1), and the total positive rate was only 2.8%; in the her-niated LDH group. Of all 117 cases, 98 of them showed obvious endplate disruption; 35 of them were Grade 1, 43 of them were Grade 2, 20 of them were Grade 3, and the total positive rate was 84%, demonstrating a huge difference with that of the bulging group (P<0.001). In the prolapse group, of 39 total cases there were 37 cases where vertebra disruption was found, and the total positive rate was 95%, which was apparently higher than both the bulging (P<0.001) and herniated groups (P<0.01) (Table 2).
Elevated expression of cytokines in the herni-ated disc nucleus pulposus cells
Since a positive relationship was found between the bone resorption in vertebrae and herniated lumbar disc, we hypothesized that osteoclast (OC) differentiation or activity may be enhanced during the lumbar disc herniation. In order to analyze various cytokines involved in osteo-clastogenesis, we used the real time PCR to detect the mRNA expression profile of cyto-kines involved in osteoclastogenesis and activ-ity in the nucleus pulposus cells isolated from the surgical samples. According to the previous reports, we examined the mRNA levels of IL-1α, IL-6, RANKL, M-CSF, MCP-1, TGF-β, IGF-1, TNF-α, and PTHrP [16, 17]. Of all these cytokines, there were no significant changes in the mRNA levels of RANKL, M-CSF, or PTHrP, but the IL-1α, IL-6, TGF-β, and TNF-α levels were slightly increased. However, the changes had no signifi-cance between groups (data not shown). It is interesting to note that IGF-1 expression increased proportionally with the increasing severity of the lumbar disc herniation, as shown in the Figure 2A. Elevated IGF-1 expression in the bulging group was almost 10 fold higher, the herniated group was 12 fold higher, and the prolapse group was 16 fold higher than the healthy control group, respectively (P<0.01). Although there was no significant difference between the bulging and herniated groups (P>0.05), differences were all significant when compared with the prolapse group, respectively (P>0.05) (Figure 2A). Another cytokine with elevated mRNA expression is MCP-1, which also plays a stimulating role in osteoclastogen-esis and activity [18]. We found that MCP-1 mRNA increased over 5 fold in the bulging
group, more than 7 fold in the herniated group, and almost 14 fold in the prolapse group com-pared with the control group, respectively (P<0.001 for all LDH groups vs. control group). Moreover, the differences between groups were all very obvious, particularly the prolapse group (bulging vs. herniated, P<0.05; bulging vs. prolapse, P<0.001; herniated vs. prolapse, P<0.001) (Figure 2B).
IGF-1 and MCP-1 enhanced osteoclastogen-esis in vitro
Elevated cytokines from the disc nucleus pulp-osus cells may enhance osteoclast differentia-tion and activity around the vertebra bodies. To test the effects of IGF-1 and MCP-1 on osteo-clast differentiation, we performed an osteo-clast differentiation model using monocytes from the peripheral blood mononuclear cells (PBMC) with 25 ng/ml of RANKL and 50 ng/ml of M-CSF. In line with previous results, with RANKL, monocytes could differentiate into mature OCs (Figure 3A) [19]. In the presence of RANKL, CD14+ monocytes first developed into preOCs in a 7-day culture, and then developed into mature OCs with RANKL after an additional 7 days of culturing. TRAP staining, a specific method to identify the differentiated OCs by showing multinuclear (>3 nucleus per cell) and TRAP+ in the cell cytoplasm for mature OCs, showed enhanced osteoclastogenesis in the presence of IGF-1 at different doses (5 ng/ml and 10 ng/ml) compared to those cultured in a medium without IGF-1 (Figure 3A), because the multinuclear TRAP+ cells are significantly increased with the presence of IGF-1 (P<0.01). Quantitative analysis supported this observa-tion, which showed growing numbers of OCs generated from co-cultures of increasing doses of IGF-1 (Figure 3B). Real-time qPCR revealed enhanced expression of OC differentiation-associated marker genes CALCA, CALCR, CTSK, and TRAP in monocytes cultured with RANKL, and different dosages of IGF-1 compared to those in monocytes cultured with medium or RANKL only (Figure 3C).
Similarly, the enhancing effect of MCP-1 on OC differentiation was also induced in our experi-ment. TRAP staining for mature OCs showed increased density of multinucleated cells in the presence of MCP-1 at different doses (50 ng/ml and 100 ng/ml) compared to those cultured in medium without MCP-1 (Figure 4A).

Nucleus pulposus cells and osteoclastogenesis
8528 Int J Clin Exp Pathol 2014;7(12):8520-8531
Quantitative analysis of the mature OC cells and real-time PCR for the OC specific marker genes likewise supported this finding, which showed an increased number of OCs generated and enhanced expression of OC differentiation-associated proteins CALCA, CALCR, CTSK, and TRAP genes in monocytes cultured with RANKL and different dosages of MCP-1, compared to those in monocytes cultured with medium or RANKL only (Figure 4B and 4C).
IGF-1 and MCP-1 promotes osteoclast differen-tiation via different signaling pathways
In addition, we examined signaling pathways involved in the IGF-1 and MCP-1 enhanced OC differentiation respectively. We focused on NF-κB, PI3K/Akt, ERK, JNK, CREB, STAT, and p38 MAPK, because these signaling pathways are important for RANKL-induced OC differenti-ation [20-22]. When the monocytes were cul-tured with OCM in presence of M-CSF and RANKL, these signaling pathways were all acti-vated as detected by western blotting (Figure 5A). However, concerning the effects of IGF-1 and MCP-1 on these signaling pathways, mech-anistic studies showed quite different results. As shown in Figure 5A, the addition of IGF-1 enhanced the phosphorylation status of PI3K, STAT5, Akt, and NF-κB in a dose dependent manner; however, addition of MCP-1 enhanced the activation of PLCg, ERK, P38, and CREB (Figure 5B). Obviously, IGF-1 enhanced the acti-vation of NF-κB initiated by RANKL, and MCP-1 promoted the activation of CREB to transcript the downstream target genes.
Since RANKL binds to its receptor RANK on the progenitors of OCs and activates OC differenti-ation-associated signaling pathways, we won-dered whether the expression of RANK in monocytes is regulated by the nucleus pulpo-sus cells derived MCP-1, so that the sensitivity of the RANKL should be increased. We treated the monocytes with a different concentration of MCP-1 from 50 ng/ml to 200 ng/ml, and the mRNA and protein levels of RANK were deter-mined by quantitative real-time PCR and flow cytometry, respectively. Our qPCR data showed that the addition of recombinant MCP-1 signifi-cantly upregulated mRNA expression of MCP-1 in a dose dependent manner, and with 200 ng/ml of MCP-1 could increase the mRNA level to more than 10 folds (Figure 5C). Moreover, the addition of recombinant MCP-1 significantly
upregulated surface protein levels of RANK in monocytes in a dose-dependent manner as detected by flow cytometry (Figure 5D). These results clearly indicate that regulation of RANK by MCP-1 affects RANKL-induced OC differentiation.
Discussion
Our study revealed a new mechanism of verte-bra disruption induced by the osteoclastogen-esis enhanced cytokines, such as IGF-1 and MCP-1, in the lumbar disc herniation patients. LDH occurs as a result of abnormal pressure on the nucleus of the disc and injures the annulus through abnormal activities, such as repetitive bending, twisting, and lifting [23]. Long-term poor posture when working, or incorrect life-style, can place additional stress on the lumbar spine [24]. With aging, discs gradually dry out, lose their strength and resiliency, and easily induce the occurrence of herniation [25]. However, in the current study, we did not find statistically significant differences in the mean age, sex ratio, whether participants were smok-ers or diabetic, and history of trauma between the early and late groups. The average duration of low back pain from the onset of symptoms to surgery has a close relationship with the sever-ity of LDH; the longer the duration, the worse the LDH. Another contributing factor is employ-ment status. Our analysis shows that physical labor plays an important role in the severity of LDH, because the herniated and prolapsed LDH groups have a higher ratio of patients who are undertaking physical labor than the bulging LDH group, in which the severity of LDH group is much lighter.
Accordingly, we hypothesized that the herniat-ed lumbar disc induced inflammatory cytokines contribute to the vertebra disruption process. The nucleus pulposus cells have been reported to secrete cytokines for LDH induced inflamma-tion [26, 27]. Moreover, some inflammatory cytokines also contribute to OC differentiation and activity, as well as to promote recruitment of OC to bone surface [28]. The maturation of osteoclasts and their participation in bone resorption is regulated in part by hormones and cytokines, such as interleukin (IL-1) [29]. In our study, we examined the mRNA levels of IL-1α, L-6, RANKL, M-CSF, MCP-1, TGF-β, IGF-1, TNF-α and PTHrP that have been reported to improve osteoclast differentiation and activity [16, 17].

Nucleus pulposus cells and osteoclastogenesis
8529 Int J Clin Exp Pathol 2014;7(12):8520-8531
We found that most mRNA levels of these inflammatory cytokines, except RANKL, M-CSF, and PTHrP are elevated in LDH patients, and all three groups have higher expression than the healthy control group. Among them, the IGF-1 and MCP-1 showed the highest elevation, and both have a positive relationship with the sever-ity of LDH, because their mRNA expression increase proportionally with increasing severity of the LDH. High levels of IGF-1 and MCP-1 con-tribute to the recruitment of OC precursor cells to the vertebra surface and activate the OC differentiation.
Insulin-like growth factor (IGF-1) is a major regu-lator of skeletal growth and remodeling [30]. The role of IGF-1 in regulating osteoclastogen-esis is through its promotion of OC differentia-tion. It is required for maintaining the normal interaction between osteoblasts and osteo-clasts, to support osteoclastogenesis through its regulation of RANKL and RANK expression [31]. Studies have shown that IGF-1 acts on bone via both endocrine and autocrine/para-crine pathways [32]. Autocrine/paracrine regu-lation depends on skeletal IGF-1 produced by osteoblasts and by stromal cells of bone mar-row [33]. Recent studies have also shown that MCP-1, a chemokine that plays a critical role in the recruitment and activation of leukocytes during acute inflammation, promotes osteo-clast fusion into multinuclear cells. Multinuclear osteoclast formation has been seen to be sig-nificantly inhibited, as well as decreased bone resorption and elevated bone mass in MCP-1-deficient mice [34]. Other evidence shows that MCP-1 is related to various pathological condi-tions such as rheumatoid arthritic bone degra-dation, or is expressed at the site of tooth erup-tion and bacterially induced bone loss. It has also been found that increased MCP-1 serum levels in patients with breast, prostate and ovarian cancers correlated with advanced tumor stage and bone resorption. Our results support the observation that the relative expressions of OC differentiation-associated IGF-1 and MCP-1 in lumbar disc nucleus pulpo-sus cells increased with the severity of disc her-niation. Quantitative analysis likewise demon-strated that increasing doses of IGF-1 and MCP-1 added to medium significantly enhanced the expression of proteins associated with OC differentiation (CALCA, CALCR, CTSK, and TRAP). While IGF-1 enhanced the activation of NF-kB signaling directly, MCP-1 upregulated the
expression of RANK so that enhanced cellular sensitivity to RANKL led to increased osteo-clastogenesis and activity. We therefore con-clude that lumbar herniation induced overex-pression of IGF-1 and MCP-1 in nucleus pulpo-sus cells, which aggravated vertebral erosions. Our results suggest that targeting osteoclasto-genesis-related cytokines has potential clinical significance in treatment of lumbar disc hernia-tion patients.
Acknowledgements
This work was supported by the funds from Beijing Natural Science Foundation (#7113170).
Disclosure of conflict of interest
None.
Address correspondence to: Dr. Lixin Kang, Department of Orthopedics, Tengzhou Central People’s Hospital, 181 Xintan Road, Tengzhou 277500, Shandong, People’s Republic of China. Tel: 086-536-52548587; E-mail: [email protected]; Dr. Nie Lin, Department of Orthopedics, Shandong University Qilu Hospital, 107 W Wenhua Rd, Jinan, Shandong, 250012, China. Tel: 086-531-82169114; Email: [email protected]
References
[1] Friedly J, Standaert C and Chan L. Epidemiology of spine care: the back pain dilemma. Phys Med Rehabil Clin N Am 2010; 21: 659-677.
[2] Atlas SJ and Deyo RA. Evaluating and manag-ing acute low back pain in the primary care set-ting. J Gen Intern Med 2001; 16: 120-131.
[3] Liao ZT, Pan YF, Huang JL, Huang F, Chi WJ, Zhang KX, Lin ZM, Wu YQ, He WZ, Wu J, Xie XJ, Huang JX, Wei QJ, Li TW, Wu Z, Yu BY and Gu JR. An epidemiological survey of low back pain and axial spondyloarthritis in a Chinese Han population. Scand J Rheumatol 2009; 38: 455-459.
[4] Manchikanti L, Singh V, Falco FJ, Cash KA and Pampati V. Evaluation of the effectiveness of lumbar interlaminar epidural injections in managing chronic pain of lumbar disc hernia-tion or radiculitis: a randomized, double-blind, controlled trial. Pain Physician 2010; 13: 343-355.
[5] Orief T, Orz Y, Attia W and Almusrea K. Spontaneous resorption of sequestrated inter-vertebral disc herniation. World Neurosurg 2012; 77: 146-152.
Nucleus pulposus cells and osteoclastogenesis
8530 Int J Clin Exp Pathol 2014;7(12):8520-8531
[6] Pouriesa M, Fouladi RF and Mesbahi S. Disproportion of end plates and the lumbar in-tervertebral disc herniation. Spine J 2013; 13: 402-407.
[7] Strange DG, Fisher ST, Boughton PC, Kishen TJ and Diwan AD. Restoration of compressive loading properties of lumbar discs with a nu-cleus implant-a finite element analysis study. Spine J 2010; 10: 602-609.
[8] Hou SX, Tang JG, Chen HS and Chen J. Chronic inflammation and compression of the dorsal root contribute to sciatica induced by the inter-vertebral disc herniation in rats. Pain 2003; 105: 255-264.
[9] Manchikanti L, Glaser SE, Wolfer L, Derby R and Cohen SP. Systematic review of lumbar discography as a diagnostic test for chronic low back pain. Pain Physician 2009; 12: 541-559.
[10] Kepler CK, Ponnappan RK, Tannoury CA, Risbud MV and Anderson DG. The molecular basis of intervertebral disc degeneration. Spine J 2013; 13: 318-330.
[11] Specchia N, Pagnotta A, Toesca A and Greco F. Cytokines and growth factors in the protruded intervertebral disc of the lumbar spine. Eur Spine J 2002; 11: 145-151.
[12] Le Maitre CL, Richardson SM, Baird P, Freemont AJ and Hoyland JA. Expression of re-ceptors for putative anabolic growth factors in human intervertebral disc: implications for re-pair and regeneration of the disc. J Pathol 2005; 207: 445-452.
[13] Ito M, Abumi K, Takeda N, Satoh S, Hasegawa K and Kaneda K. Pathologic features of spinal disorders in patients treated with long-term he-modialysis. Spine (Phila Pa 1976) 1998; 23: 2127-2133.
[14] Gruber HE, Ashraf N, Kilburn J, Williams C, Norton HJ, Gordon BE and Hanley EN Jr. Vertebral endplate architecture and vascular-ization: application of micro-computerized to-mography, a vascular tracer, and immunocyto-chemistry in analyses of disc degeneration in the aging sand rat. Spine (Phila Pa 1976) 2005; 30: 2593-2600.
[15] Mackiewicz Z, Salo J, Konttinen YT, Kaigle Holm A, Indahl A, Pajarinen J and Holm S. Receptor activator of nuclear factor kappa B ligand in an experimental intervertebral disc degeneration. Clin Exp Rheumatol 2009; 27: 299-306.
[16] Lee SK and Lorenzo J. Cytokines regulating os-teoclast formation and function. Curr Opin Rheumatol 2006; 18: 411-418.
[17] Pacifici R. Cytokines and osteoclast activity. Calcif Tissue Int 1995; 56 Suppl 1: S27-28.
[18] Kim MS, Day CJ, Selinger CI, Magno CL, Stephens SR and Morrison NA. MCP-1-induced human osteoclast-like cells are tartrate-resis-
tant acid phosphatase, NFATc1, and calcitonin receptor-positive but require receptor activator of NFkappaB ligand for bone resorption. J Biol Chem 2006; 281: 1274-1285.
[19] Leibbrandt A and Penninger JM. RANKL/RANK as key factors for osteoclast development and bone loss in arthropathies. Adv Exp Med Biol 2009; 649: 100-113.
[20] Kajiya H. Calcium signaling in osteoclast differ-entiation and bone resorption. Adv Exp Med Biol 2012; 740: 917-932.
[21] Del Fattore A, Teti A and Rucci N. Osteoclast receptors and signaling. Arch Biochem Biophys 2008; 473: 147-160.
[22] Shinohara M and Takayanagi H. Novel osteo-clast signaling mechanisms. Curr Osteoporos Rep 2007; 5: 67-72.
[23] Postacchini F and Postacchini R. Operative management of lumbar disc herniation: the evolution of knowledge and surgical tech-niques in the last century. Acta Neurochir Suppl 2011; 108: 17-21.
[24] Kim SJ, Kim WR, Kim HS, Park HW, Cho YW, Jang SH, Hwang SJ and Ahn SH. Abnormal spontaneous activities on needle electromyog-raphy and their relation with pain behavior and nerve fiber pathology in a rat model of lumbar disc herniation. Spine (Phila Pa 1976) 2011; 36: E1562-1567.
[25] Lebkowski WJ and Dzieciol J. Degenerated lumbar intervertebral disc. A morphological study. Pol J Pathol 2002; 53: 83-86.
[26] Tian Y, Yuan W, Fujita N, Wang J, Wang H, Shapiro IM and Risbud MV. Inflammatory cyto-kines associated with degenerative disc dis-ease control aggrecanase-1 (ADAMTS-4) ex-pression in nucleus pulposus cells through MAPK and NF-kappaB. Am J Pathol 2013; 182: 2310-2321.
[27] Yamamoto J, Maeno K, Takada T, Kakutani K, Yurube T, Zhang Z, Hirata H, Kurakawa T, Sakai D, Mochida J, Doita M, Kurosaka M and Nishida K. Fas ligand plays an important role for the production of pro-inflammatory cyto-kines in intervertebral disc nucleus pulposus cells. J Orthop Res 2013; 31: 608-615.
[28] Souza PP and Lerner UH. The role of cytokines in inflammatory bone loss. Immunol Invest 2013; 42: 555-622.
[29] Kim JH, Jin HM, Kim K, Song I, Youn BU, Matsuo K and Kim N. The mechanism of osteoclast dif-ferentiation induced by IL-1. J Immunol 2009; 183: 1862-1870.
[30] Niu T and Rosen CJ. The insulin-like growth factor-I gene and osteoporosis: a critical ap-praisal. Gene 2005; 361: 38-56.
[31] Ochiai H, Okada S, Saito A, Hoshi K, Yamashita H, Takato T and Azuma T. Inhibition of insulin-like growth factor-1 (IGF-1) expression by pro-

Nucleus pulposus cells and osteoclastogenesis
8531 Int J Clin Exp Pathol 2014;7(12):8520-8531
longed transforming growth factor-beta1 (TGF-beta1) administration suppresses osteoblast differentiation. J Biol Chem 2012; 287: 22654-22661.
[32] Yakar S and Rosen CJ. From mouse to man: redefining the role of insulin-like growth factor-I in the acquisition of bone mass. Exp Biol Med (Maywood) 2003; 228: 245-252.
[33] Jiang J, Lichtler AC, Gronowicz GA, Adams DJ, Clark SH, Rosen CJ and Kream BE. Transgenic mice with osteoblast-targeted insulin-like growth factor-I show increased bone remodel-ing. Bone 2006; 39: 494-504.
[34] Morrison NA, Day CJ and Nicholson GC. Dominant negative MCP-1 blocks human os-teoclast differentiation. J Cell Biochem 2014; 115: 303-312.

Nucleus pulposus cells and osteoclastogenesis
1
Supplemental Table 1. Primers used for real-time PCRGene Forward ReverseIGF-1 CTTCAGTTCGTGTGTGGAGACAG CGCCCTCCGACTGCTGMCP-1 TTCCTCTTGAACCACAGT CTTGCAAAGACCCTCAAACALCA TTCATCAGGAAATGGAGCTG CATTCATCCACTGGCTGTTCCALCR GGGAATCCAGTTTGTCGTCT ACAAAGAAGCCCTGGAAATGCTSK GAACTGGCTATGAACCACCTG TTACTGCGGGAATGAGACAGTRAP AGATCCTGGGTGCAGACTTC AAGGGAGCGGTCAGAGAATARANK GAAGAAGAAGCCAGCAGGAC CCAGTCACATTTCCAGATGCGAPDH ATGGGTGTGAACCATGAGAA GTGCTAAGCAGTTGGTGGTG























![The protective effects of PI3K/Akt pathway on human nucleus pulposus … · 2020. 1. 28. · nucleus pulposus cells and nucleus pulposus progenitor cells [14]. Previous studies have](https://img.pdfslide.us/doc/110x75/60b265dd0d8b8040e758b496/the-protective-effects-of-pi3kakt-pathway-on-human-nucleus-pulposus-2020-1-28.jpg)




![Puerarin Relieved Compression-Induced Apoptosis and ...downloads.hindawi.com/journals/sci/2020/7126914.pdfimpaired nucleus pulposus cell (NPC) proliferation [4]. Nucleus pulposus mesenchymal](https://img.pdfslide.us/doc/110x75/5f7fa24ee6184370f175b23e/puerarin-relieved-compression-induced-apoptosis-and-impaired-nucleus-pulposus.jpg)