Embed Size (px)
Citation preview

RESEARCH ARTICLE
Reduction in Length of Stay and Morphine Use forNAS With the “Eat, Sleep, Console” MethodThomas Blount, MD,a Alana Painter, MD,a Emily Freeman, MSN, CPNP,a Matthew Grossman, MD,b Ashley G. Sutton, MDa
A B S T R A C T OBJECTIVES: To reduce average length of stay (ALOS) in infants with neonatal abstinencesyndrome (NAS) transferred to the inpatient floor from the mother-infant unit. Secondarily, weaimed to reduce morphine exposure in these infants.
METHODS: Using quality improvement methodology, we redesigned our approach to NAS on theinpatient floor. Key interventions included transitioning from a modified Finnegan NeonatalAbstinence Scoring System to the “Eat, Sleep, Console” method for withdrawal assessment,reeducation on nonpharmacologic interventions, and adding as-needed morphine as initialpharmacotherapy. Data for infants $35 weeks’ gestation with confirmed in utero opioid exposureand worsening symptoms of NAS requiring transfer to the inpatient floor were obtained, includingALOS, number of morphine doses, and total morphine amount administered. Infants withconditions requiring nothing by mouth for .12 hours or morphine initiation in the ICU wereexcluded.
RESULTS: ALOS for infants (baseline n 5 40; intervention n 5 36) with NAS transferred to theinpatient floor decreased from 10.3 to 4.9 days. Average morphine administered decreased from38 to 0.3 doses per infant. No infant in the intervention period required scheduled morphine. Thepercent of all infants transferred to the floor for NAS requiring any morphine decreased from 92%at baseline to 19% postimplementation. There were no observed adverse events or NAS-relatedreadmissions in the intervention period.
CONCLUSIONS: Transitioning to the Eat, Sleep, Console assessment with re-enforcement ofnonpharmacologic care and use of as-needed morphine as initial pharmacotherapy resulted in anotably decreased ALOS and near elimination of postnatal opioid treatment of infants with NASmanaged on our inpatient floor.
aDivision of GeneralPediatrics and AdolescentMedicine, Department of
Pediatrics, School ofMedicine, University of
North Carolina at ChapelHill, Chapel Hill, North
Carolina; and bSchool ofMedicine, Yale University,New Haven, Connecticut
www.hospitalpediatrics.orgDOI:https://doi.org/10.1542/hpeds.2018-0238Copyright © 2019 by the American Academy of Pediatrics
Address correspondence to Ashley G. Sutton, MD, Department of Pediatrics, University of North Carolina at Chapel Hill School ofMedicine, Campus Box 7225, 101 Manning Dr, Chapel Hill, NC 27514. E-mail: [email protected]
HOSPITAL PEDIATRICS (ISSN Numbers: Print, 2154-1663; Online, 2154-1671).
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Dr Blount was the primary investigator and conceptualized and designed the project, collected and analyzed data, and drafted the initialmanuscript; Dr Painter and Ms Freeman assisted with creation of the project protocol and assisted with project management, dataanalysis, and manuscript drafting and revision; Dr Grossman conceptualized and provided the protocol for the key intervention andassisted with manuscript drafting and revision; Dr Sutton assisted with conceptualization and project design, performed data collectionand analysis, and reviewed and revised the manuscript; and all authors approved the final manuscript as submitted and agree to beaccountable for all aspects of the work.
HOSPITAL PEDIATRICS Volume 9, Issue 8, August 2019 615
by guest on February 19, 2021www.aappublications.org/newsDownloaded from

Neonatal abstinence syndrome (NAS) is aclinical diagnosis made when an infantexperiences withdrawal symptoms afterbirth because of in utero opioid exposure.Increased opioid use and abuse hasresulted in a rising incidence of NASnationally, recently estimated to affect6.0 infants per 1000 hospital births.1,2
Historically, approaches to management ofinfants with NAS have been focused on acombination of nonpharmacologic andpharmacologic treatment, typically in theNICU.3 A growing body of research supportsa collaborative approach to care thatincludes maintaining the maternal-infantdyad (“rooming in”) and increasednonpharmacologic interventions includingskin-to-skin placement, swaddling, andlimiting stimulation.2,4–6 Additionally, aprotocol-driven approach to infants withNAS can be used to minimize variability incare, shorten average length of stay (ALOS),and improve patient outcomes.7–11 The mostcommonly used tool in evaluation of infantswith NAS is the modified Finnegan NeonatalAbstinence Scoring System (FNASS).12
However, FNASS has notable limitations asan assessment tool, including challengeswith internal consistency and lack ofrigorous validation.13 As a result, manygroups have recently departed from strictFNASS-based approaches to NASevaluation.4,7,14 One novel method forwithdrawal assessment, known as the “Eat,Sleep, Console” (ESC) method, relies on astructured assessment of newborn feeding,sleep duration between feedings, and abilityto be consoled to inform management ofwithdrawal rather than FNASS scoring.7,14,15
Previous improvement efforts at ourinstitution resulted in a protocol-basedapproach to infants with NAS that usedFNASS scores for assessment, emphasizedmaintaining the maternal-infant dyad duringtreatment, and incorporatednonpharmacologic treatments forwithdrawal. The ALOS for infants with NAS atour institution decreased over a 4-yearperiod from 22 to 10 days by 2017 after theimplementation of these measures. Theseimprovements successfully reduced ourALOS to below the national average of16 days16 and resulted in a reduction in thepercentage of all infants with confirmed in
utero opioid exposure treated withpharmacotherapy at our institution to 30%.
However, our team felt that furtheropportunities for improvements existed.Infants with elevated FNASS scores in themother-infant unit (MIU) were transferredto the inpatient floor for initiation ofmorphine therapy including methodicalweans that continued even when FNASSscores were consistently low. FNASS scoringitself was a source of frustration forproviders given the perception of poorinterrater reliability and that performingthe assessment involves disturbing theinfant and potentially exacerbatingwithdrawal. In this setting, with the recentpublication of alternative methods forassessment,4,7,14 we began to note apreference among our provider group awayfrom strict adherence to FNASS-basedmanagement. Additionally, we treat a largematernal population managed withmedication-assisted treatment (MAT), whichwe do not administer after maternaldischarge. Infants requiring prolongedhospitalization thus resulted in mother-infantdyad separation because mothers left thebedside to continue their own treatment.
To further improve care for infants with NASon the inpatient floor, we undertook aquality improvement initiative. We primarilyaimed to reduce the ALOS for infants withNAS transferred to the inpatient floor by50% in a 6-month period. We additionallyaimed to reduce the percent of infants withNAS receiving treatment with morphine by50% and the total amount of morphinereceived by those infants treated withmorphine by 50%.
METHODSSetting
Our institution is a tertiary-care academicmedical center with multiple subhospitals.Our MIU admits 3700 infants annually,including ∼100 infants per year with knownin utero opioid exposure. Newborn infantsadmitted to our MIU room in with mothersto minimize dyad separation. Our institutionis a regional referral center for womenincarcerated at the time of delivery and alsocollaborates with a large residentialtreatment facility for women with substanceuse disorder. As a result, the majority of our
infants with NAS are born to mothersreceiving MAT, most commonly withbuprenorphine.
Healthy, inborn infants who are $35 weeks’gestation and $1.8 kg are admitted tocouplet care on the MIU. Infants born tomothers with previous substance use orimprisonment at time of delivery as well asthose with known opioid exposure undergourine and meconium toxicology screening.Infants in the MIU are managed withnonpharmacologic interventions and aremonitored for withdrawal by using theFNASS every 2 to 4 hours (determined byscore) beginning at 12 hours of life. Infantswith 2 consecutive scores $12 or3 consecutive scores $8 are transferredfrom the MIU to the inpatient floor in theadjoined children’s hospital for initiation ofmorphine therapy with cardiorespiratorymonitoring because our MIU does not havelicensing for monitored infant beds. Forinfants with tobacco and long-acting opioidexposure, we generally do not transferbefore 36 hours of life and attribute earliersymptoms to tobacco withdrawal. Mothersaccompany infants after transfer whenmedically possible. If the mother is unableto discharge, the infant is transferred aloneand the mother visits as medically ablebecause no nursing care is provided for themother on the pediatric floor. If conditionsaside from NAS require NICU transfer in anopioid-exposed infant, the infant ismonitored and treated for NAS in theNICU with an approach that differs fromthat used in the MIU and on the inpatientfloor.
In our baseline period, once an infant wastransferred to the inpatient floor, morphinewas initiated at 0.03 mg/kg every 4 hourswith FNASS scores every 2 to 4 hours asabove. If necessary, morphine wasincreased by 10% to 20% increments until2 consecutive FNASS scores were #8.Morphine dosage was decreased daily by10% of the peak dose until at roughly0.02 mg/kg per dose, then dose frequencywas spaced consecutively to every 6, 8, or12 hours and then finally to every 24 hoursbefore discontinuation. Care teamsconvened on daily rounds to review theFNASS scores and clinical status. Infants
616 BLOUNT et al
by guest on February 19, 2021www.aappublications.org/newsDownloaded from

were maintained on cardiorespiratorymonitoring during morphine treatment andhad vital signs monitored every 2 to 4 hoursdepending on the FNASS score that wasdictated. Infants were typically dischargedwithin 24 hours of the last morphine dose.
Intervention
We developed a 5-member multidisciplinarytask force including physicians (hospitalistand residents), a newborn nursery provider,and a pediatric pharmacist to review thecare of infants with NAS on the inpatientfloor in June 2017. We obtained baselinedata, completed a key driver diagram(Supplemental Fig 5), and implemented2 key interventions that were approved bystakeholders on the inpatient floor. First, weimplemented as-needed (PRN) dosing ofmorphine at our previous startingtreatment dose (0.03 mg/kg) for infants withNAS symptoms not controlled bynonpharmacologic interventions. Dosingwas repeated if the infant continued to meetthe pharmacotherapy threshold at the 4-hour mark or at any point moving forward.If scheduled morphine was needed on the
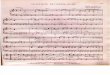
basis of multiple PRN doses, we allowedweaning by 10% of the peak dose up to3 times per day when appropriate. Wediscontinued scheduled morphine at dosingof 0.02 mg/kg every 4 hours with no changein dosing interval and transitioned back toPRN dosing after discontinuation ofscheduled morphine. Second, we replacedthe use of FNASS scores for monitoringinfants with NAS for withdrawal with theESC method as described by Grossmanet al.7,14 Specifically, nurses assessed if theinfant fed 1 oz or had an adequatebreastfeeding session, slept at least 1 hourbetween feedings, and consoled within10 minutes when crying. The interventionswere included in a new protocol thatreemphasized nonpharmacologicinterventions as the standard treatment ofNAS (including reducing environmentalstimulation, pacifier use, swaddling, andincreasing caloric density of formula)(Fig 1). Infants not receiving morphine werenot placed on cardiorespiratory monitorsand had vital signs obtained once per shiftwith blood pressure measurements once
per day. We created a guideline forproviders with specific instructions on howto enter orders for ESC and the need for theprovider to assess, at the bedside, anyinfant not meeting ESC criteria for potentialintervention.
Planning the Intervention andImplementation
As we approached implementation, wehosted a session for nurses and hospitalistscovering recent articles describing newapproaches to the management of infantswith NAS. Two weeks before implementation,we presented the new ESC approach to thefloor nurses for feedback and discussion.One week before implementation, the newprotocol and treatment guidelines wereposted on the resident and hospitalist Webrepository and introduced at residentmorning report. The protocol was also sentto residents leading the ward teams at thestart of each new resident rotation block.We did not change our approach for infantsin the MIU or the NICU; therefore, infantscontinued to receive FNASS scores in thesesettings. The threshold for transfer to the
FIGURE 1 New provider protocol and floor management for patients with NAS on the inpatient floor. a The medical doctor may choose to weanmore rapidly if clinically indicated. NBN, newborn nursery; NG, nasogastric; q4, every 4 hours.
HOSPITAL PEDIATRICS Volume 9, Issue 8, August 2019 617
by guest on February 19, 2021www.aappublications.org/newsDownloaded from

inpatient floor from the MIU was also notchanged.
Studying the Intervention
Baseline (June 2016–October 2017) andintervention and sustainment (November2017–December 2018) data were obtainedvia weekly automated reports from theelectronic medical record (EMR), whichidentified infants who were $35 weeks’gestation, $1.8 kg, and had at least 1 FNASSscore documented. Manual chart reviewwas then performed to confirm inclusion ofonly those infants with documented third-trimester opioid exposure either by positivematernal or infant drug screening ormaternal prescription. Included infants inthe analysis were confirmed to havedocumented scores in the MIU of 2 FNASSscores $12 or 3 scores $8 before transfer,signaling worsening withdrawal. Weexcluded infants transferred for ongoing
observation without elevated FNASS scores,infants with NAS initiated on morphine whileadmitted to the NICU for another condition(hypoglycemia, respiratory insufficiency),and infants who had risk for NAS but wereunable to have enteral feedings for.12 hours related to respiratory status,given the potential impact of nonfeedingstatus on withdrawal symptoms.
Data extracted from the EMR reportsincluded length of stay (hours), totalnumber of morphine doses duringhospitalization (count), total amount ofmorphine received during hospitalization(milligrams per kilogram), and percent ofinfants with NAS treated with morphine.Additionally, patient characteristics,including birth weight, discharge weight,gestational age, maternal race, and payer,were extracted. During the manual chartreview to confirm inclusion criteria, otherpatient factors were manually extracted,
including documentation of breastfeedingattempt, primary opioid exposure, andmaternal polypharmacy use, includingtobacco. Infant charts, including care teamnotes, were manually reviewed forbalancing and safety measures as below.
Measures and Data Analysis
Our primary outcome measure was ALOS forinfants with NAS transferred to the inpatientfloor. We identified infants by anydocumented FNASS score to ensure that allinfants known to have opioid exposure wereincluded in the initial data set for potentialinclusion. This method reduced thelikelihood of missing data that can occurwhen relying on provider coding. ALOS wasdefined as the time from birth to either thetime of discharge or the time ofdiscontinuation of the ESC protocol forinfants with resolved NAS who weremedically cleared but awaiting placementdetermination. As secondary outcomes, wemeasured the number of morphine dosesand the cumulative dose of morphinereceived per infant with NAS on theinpatient floor. Balancing measuresincluded adverse events (ie, desaturation,apnea, seizure, or need for NICU transferfrom the floor), percent weight change frombirth to discharge, and 30-day readmissionor emergency department presentation toour network of hospitals. Data weremonitored by using statistical processcontrol charts appropriate for eachmeasure to assess improvement over timein key aims. Standard Shewhart rules wereused for the interpretation anddetermination of special cause variation(primarily 8 consecutive points on the sameside of the centerline).
Ethical Considerations and HumanSubjects Protection
Our institutional review board reviewed thisinternal improvement project anddetermined that it did not meet theregulatory criteria for research involvinghuman subjects and that ongoing oversightwas not required. No interventions involvedcomparison of therapies, and subjects werenot randomly assigned. No personal healthdata were shared outside of the investigatorteam.
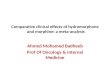
FIGURE 2 Flowchart for inclusion or exclusion of infants. NPO, no enteral feedings.
618 BLOUNT et al
by guest on February 19, 2021www.aappublications.org/newsDownloaded from

RESULTS
A total of 389 infants (baseline n 5 203;intervention n 5 186) were identified by theautomated EMR report as having at least1 FNASS score during newbornhospitalization. After manual chart review,76 infants (baseline n 5 40; interventionn 5 36) with escalating NAS symptomsrequiring transfer to the inpatient floor metcriteria for inclusion in the final analysis(Fig 2). Characteristics of included infantswith NAS during baseline and interventionperiods are summarized in Table 1. Of note,.80% of included infants were born tomothers on MAT, with buprenorphine being themost common medication. The only measureddifference noted between the groups wasincreased rate of maternal tobacco use inthe intervention cohort (P 5 .03).
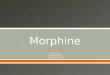
The ALOS for infants with NAS transferred tothe inpatient floor decreased from abaseline of 10.3 days to 4.9 days during theintervention period (Fig 3). The percent ofinfants treated with morphine on the floordecreased from 92% at baseline to 19%
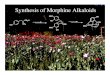
postintervention. Overall, only 9% of allinfants with in utero opioid exposure at ourinstitution (including those discharged fromthe MIU) received any pharmacotherapypostintervention. There was a substantialdecrease in the average number ofmorphine doses from 38 doses per infant to0.3 doses per infant (Fig 4). The averagetotal morphine dosage per infant treatedwith morphine decreased from 1.1 to0.03 mg/kg per infant. In the interventionperiod, 0 infants received scheduledmorphine dosing and only 1 infant receivedmultiple doses (3) of PRN morphine.
Special cause variation was achieved withreduction in mean in November 2017,essentially at the outset of implementation,for each outcome measure. Of note, therewere many points of special cause variationin the number of doses per infant notedboth above and below the upper and lowercontrol limits at baseline in Fig 3. Thisvariation improved postintervention.
There were no NAS-attributable 30-dayreadmissions or emergency department
visits in the baseline or interventionperiods. One infant in the baseline grouphad a desaturation attributed to a dosingerror in oral morphine. There were noadverse events documented in theintervention period. Percent change frombirth weight at discharge did reveal specialcause variation from an average of 3% belowbirth weight at baseline (average age∼10 days old) to 5% below birth weight in theintervention period (average age ∼5 days old).
DISCUSSION
Changing our approach to the managementof infants with NAS on the inpatient floorreduced ALOS and decreased morphine use.Implementation of the ESC method and PRNdosing of morphine with re-enforcement ofnonpharmacologic therapies, includingformula fortification, led to near eliminationof pharmacotherapy use and resulted in.50% further reduction in ALOS for infantswith NAS managed on our floor. Importantly,we did not observe an increase inreadmission rate or in adverse events,although these events were rare at baseline.Infants at discharge had a further 2%decrease in weight relative to birth weight.Given that infants were discharged anaverage of 5 days earlier and typicallybefore 1 week of life, this change in weightis likely not clinically significant but isinstead a reflection of discharge occurringat a younger postnatal age. Of note, we didobserve an increase in tobacco use amongmothers in the intervention period (Table 1),although if anything, this difference would beexpected to be more likely to exacerbate NASrather than improve outcomes. Overall,demographics and characteristics are providedto offer some guidance on the populations,but small numbers limit interpretability ofcomparative statistics, and this study wascompleted as a quality improvementintervention and not a controlled trial.
The number of morphine doses per infant atbaseline had a wide range (0–106 doses)and significant variability, including multiplepoints outside of the control limits (Fig 4).This variation was markedly improvedpostimplementation. We suspect variation isrelated to differences in provider decisionsto escalate or wean morphine dosing on thebasis of the previous protocol. Additionally,
TABLE 1 Characteristics of Included Infants With NAS
Preintervention(n 5 40)
Postintervention(n 5 36)
P
Gest age, wk 39 2/7 39 0/7 .540
Birth wt, kg 3.21 3.04 .142
Any breastfeeding, n (%) 21 (53) 24 (67) .203
Maternal race, n (%)
White 33 (83) 31 (86) .664
African American 4 (10) 3 (8) .801
Other 3 (7) 2 (6) .731
Sex, n (%)
Male 21 (53) 16 (44) .481
Insurance, n (%)
Medicaid 38 (95) 34 (94) .914
Maternal opioid, n (%)
Buprenorphine 26 (65) 18 (50) .182
Methadone 8 (20) 13 (36) .114
Othera 6 (15) 5 (14) .890
Otherb exposures, n (%)
Tobacco 25 (63) 30 (83) .035c
Polypharmacy 32 (80) 33 (91) .136
a Any other opioid besides buprenorphine or methadone.b Additional relevant exposure history.c Statistically significant.
HOSPITAL PEDIATRICS Volume 9, Issue 8, August 2019 619
by guest on February 19, 2021www.aappublications.org/newsDownloaded from

after the publication of the ESC method7 wenoted multiple patients who received lesspharmacotherapy despite having FNASSscores meeting criteria for treatment perbaseline protocol. We suspect that thepublication of ESC may have resulted inindividual providers to deviate from astrictly FNASS-based treatment approachbefore a change of the treatment protocol,although we cannot be certain.
We initially aimed for a 50% reduction in thetotal cumulative dose of morphine in infantswith NAS transferred to the inpatient floorand were able to exceed this goal because oflow use of pharmacotherapy overall in theintervention period. Infants treated (n 5 7)with morphine during the intervention periodrequired only PRN morphine to meet ESCparameters. The 1 infant who receivedmultiple PRN doses of morphine wasreceiving phototherapy, and thusnonpharmacologic interventions were limited.
We acknowledge that the degree of reduction inmorphine use was unexpected. This markedchange could elicit criticism that our objectivewas explicitly to avoid pharmacotherapy,potentially at the expense of infants experiencingwithdrawal. However, the new protocol offeredPRN dosing and had specific instructions forinitiation and weaning of scheduled morphinewhen required. Treatment decisions were madeby the clinical team, supervised by.15 differentattending physicians during the interventionperiod. Chart review of infants during theintervention period supported that infants wereconsistently meeting ESC protocol criteria orresponding to enhanced nonpharmacologicinterventions when not meeting parameters andnot that providers or staff were avoiding opioiduse in infants who were otherwise notfunctioning well.
By adopting a new ESC-based protocol forevaluating infants with NAS, we were able toachieve a paradigm shift at our institution. This
approach incorporates the strengths ofpreviously published approaches in that it isprotocol driven, standardized, and allows forcontinued rooming in while using a morestraightforward evaluation of how an infant istolerating the transition to extrauterine life andmanaging withdrawal symptoms.2,4,7,15 Ourresults support the original publication byusing this approach in a different populationand location.7,15 The majority of our infants wereexposed to buprenorphine and/or naloxone inutero, rather than methadone, and ourstandard of care was already to transferinfants with NAS to the inpatient floor, likelycontributing to a lower baseline ALOS thanreported by Grossman and colleagues.15 Wehad previously implemented manyimprovements, including nonpharmacologicinterventions and not admitting otherwise wellinfants with NAS to the NICU.
This model has worked well at ourinstitution in which transfer from the MIU
FIGURE 3 Statistical process control chart for length of stay (LOS) for infants with NAS transferred to the inpatient floor. The LOS for consecutiveneonates with NAS transferred to the inpatient floor from June 2016 to December 2018. The data source is from a business objectsreport in Epic by documented FNASS score in newborn hospitalization. LCL, lower control limit; UCL, upper control limit.
620 BLOUNT et al
by guest on February 19, 2021www.aappublications.org/newsDownloaded from

to the inpatient floor allows for rooming inand fostering a quieter, dark environmentfor infants. Although continued opioid usefor infants with NAS experiencingwithdrawal remains an option formanagement, the potential long-term effectsof prolonged hospitalization and furtheropioid exposure in a critical period oftransition for this at-risk population are notknown. Additionally, by minimizingpharmacologic treatment, we were able todecrease vital sign frequency andcardiorespiratory monitoring, therebypromoting a calmer environment in theroom for the infant and family. In addition,although not measured directly in our study,the potential impacts on dyad bondingresulting from a shorter hospital stay andreduced opioid exposure are important
considerations when weighing the risks andbenefits of prolonged, scheduledpharmacotherapy to manage infants whoare meeting the basic requirements ofpostnatal transition.
Our study has several limitations that areworth noting. We report a relatively smallsample size, which particularly limits theinterpretability of comparative statistics(Table 1). Regarding outcomes, the smallsample size, in part, is mitigated by the useof process control charts over time and theextent of the change in outcomes in thepopulation. Given that the implementedinterventions occurred in essentially thesame time period (2 weeks apart), it isdifficult to pinpoint the exact component ofthis intervention that led to the dramaticchange. However, because
nonpharmacologic care was alreadystandard, ESC and an option for PRNmorphine seem to be the largest drivers ofthe change.
There were some unique features of ourpopulation that may impact the results of asimilar approach in different settings. Wedid not have any baseline readmissions forNAS-related causes, which limitsinterpretability of having no readmissions,despite halving the ALOS, in thepostintervention group given that this is arare event in our population. We attributeour low rate of readmissions in part to ourpopulation of mothers because many arereceiving stable MAT perinatally in asupportive residential care environment.Others are incarcerated at the time ofdelivery, resulting in the infant being placed
FIGURE 4 Statistical process control chart for number of morphine doses given per neonate with NAS transferred to the inpatient floor. The datasource is from a business objects report in Epic by documented FNASS score in newborn hospitalization. LCL, lower control limit; UCL,upper control limit.
HOSPITAL PEDIATRICS Volume 9, Issue 8, August 2019 621
by guest on February 19, 2021www.aappublications.org/newsDownloaded from

in alternative care at discharge. Additionally,buprenorphine was the most common inutero opioid exposure in our infant cohort,which likely improved our outcomesthroughout the study given thatbuprenorphine has been shown to favorablyimpact NAS severity.17,18 Although relevant toapplication elsewhere, there were nodetected differences in primary opioidexposure in baseline and interventiongroups, and this exposure would not haveresulted in the dramatic changesdemonstrated.
Importantly, outcomes outside of the initialhospitalization and 30-day postdischargeperiod (both positive and negative) with theESC assessment approach compared toFNASS assessments remain largelyunknown. An understanding of the impact ofvarious treatment approaches on maternal-infant bonding, neurodevelopment, andadverse events is lacking with this approach(and others) in this population. Theindependent impacts on infant outcomes ofneonatal withdrawal and use of opioids forits treatment are not well understood givena population with heterogenous in uteroexposures to substances at baseline.Medium- and long-term postdischargeoutcomes including growth anddevelopmental trajectories for infantsassessed with FNASS scores versus the ESCmethod or treated for NAS withoutpharmacotherapy compared with those thatreceive pharmacotherapy are alsounknown. However, many centers, includingours, use the FNASS for assessment in theMIU and discharge a large percentage ofinfants with in utero opioid exposurewithout using pharmacotherapy. Thus, anypotential impacts on infant outcomes arenot necessarily unique to the ESC approach,although they should be further explored.
Unlike other studies,4,7,14 we did not collectFNASS data for patients after transfer to theinpatient floor because we felt it sent amixed message to continue collecting FNASSscores that would not be acted on. We alsohad concerns about the vigilant andstimulatory environment promoted byFNASS scoring itself. As such, our resultsare limited only to the historicalcomparison of the baseline management of
similar infants rather than comparison ofhow the infants during the interventionperiod would have been managed under ourprevious approach.
CONCLUSIONS
Our new approach for infants with NASincorporating the ESC assessment methodand PRN morphine improved themanagement of infants with NAS on ourinpatient floor by decreasing ALOS andreducing postnatal opioid exposure withoutshort-term adverse consequences to theinfant. Results were achieved in the initial 6-month improvement period and have beensustained without further intervention. Ourimplemented approach, including the ESCmethod and further emphasis onnonpharmacologic interventions as equallyimportant to pharmacologic interventions,is simple and can be easily applied at otherinstitutions without rigorous training orvalidation of competency as required ofmore detailed scoring systems. Oneparticularly important implication of ourstudy is use of PRN morphine as initialpharmacotherapy. Infants in our populationwho required morphine needed minimalPRN doses, and under our previousapproach, they would have automaticallybeen initiated on scheduled morphine.Because of the success on the inpatientfloor, our next steps include expansion ofthe ESC approach to the MIU to allow for ahomogenous assessment tool betweenunits.
REFERENCES
1. Patrick SW, Davis MM, Lehmann CU,Lehman CU, Cooper WO. Increasingincidence and geographic distribution ofneonatal abstinence syndrome: UnitedStates 2009 to 2012. J Perinatol. 2015;35(8):650–655
2. Patrick SW, Schumacher RE, Horbar JD,et al. Improving care for neonatalabstinence syndrome. Pediatrics. 2016;137(5):e20153835
3. Bogen DL, Whalen BL, Kair LR, Vining M,King BA. Wide variation found in care ofopioid-exposed newborns. Acad Pediatr.2017;17(4):374–380
4. Holmes AV, Atwood EC, Whalen B, et al.Rooming-in to treat neonatal abstinencesyndrome: improved family-centeredcare at lower cost. Pediatrics. 2016;137(6):e20152929
5. MacMillan KDL, Rendon CP, Verma K,Riblet N, Washer DB, Volpe Holmes A.Association of rooming-in with outcomesfor neonatal abstinence syndrome: asystematic review and meta-analysis.JAMA Pediatr. 2018;172(4):345–351
6. Atwood EC, Sollender G, Hsu E, et al. Aqualitative study of family experiencewith hospitalization for neonatalabstinence syndrome. Hosp Pediatr.2016;6(10):626–632
7. Grossman MR, Berkwitt AK, Osborn RR,et al. An initiative to improve the qualityof care of infants with neonatalabstinence syndrome. Pediatrics. 2017;139(6):e20163360
8. Asti L, Magers JS, Keels E, Wispe J,McClead RE Jr. A quality improvementproject to reduce length of stay forneonatal abstinence syndrome.Pediatrics. 2015;135(6). Available at:www.pediatrics.org/cgi/content/full/135/6/e149425941308
9. Burnette T, Chernicky L, Towers CV. Theeffect of standardizing treatment whenmanaging neonatal abstinencesyndrome [published online ahead ofprint May 14, 2018]. J Matern FetalNeonatal Med. doi:10.1080/14767058.2018.1465038
10. Saunders C, King T, Smith S, et al.Neonatal abstinence syndrome:evaluating the effectiveness of anevidence-based multidisciplinary careapproach. J Perinat Neonatal Nurs. 2014;28(3):232–240
11. Hall ES, Wexelblatt SL, Crowley M, et al.Implementation of a neonatal abstinencesyndrome weaning protocol: amulticenter cohort study. Pediatrics.2015;136(4). Available at:www.pediatrics.org/cgi/content/full/136/4/e80326371196
12. Mehta A, Forbes KD, Kuppala VS.Neonatal abstinence syndromemanagement from prenatal counseling
622 BLOUNT et al
by guest on February 19, 2021www.aappublications.org/newsDownloaded from

to postdischarge follow-up care: resultsof a national survey. Hosp Pediatr. 2013;3(4):317–323
13. Jones HE, Seashore C, Johnson E, et al.Psychometric assessment of theneonatal abstinence scoring system andthe MOTHER NAS Scale. Am J Addict.2016;25(5):370–373
14. Grossman MR, Lipshaw MJ, Osborn RR,Berkwitt AK. A novel approach toassessing infants with neonatal
abstinence syndrome. Hosp Pediatr.2018;8(1):1–6
15. Wachman EM, Grossman M, Schiff DM,et al. Quality improvement initiative toimprove inpatient outcomes for neonatalabstinence syndrome. J Perinatol. 2018;38(8):1114–1122
16. Patrick SW, Schumacher RE,Benneyworth BD, Krans EE, McAllisterJM, Davis MM. Neonatal abstinencesyndrome and associated health care
expenditures: United States, 2000-2009.JAMA. 2012;307(18):1934–1940
17. Jones HE, Kaltenbach K, Heil SH, et al.Neonatal abstinence syndrome aftermethadone or buprenorphine exposure.N Engl J Med. 2010;363(24):2320–2331
18. Brogly SB, Hernández-Diaz S, Regan E,Fadli E, Hahn KA, Werler MM. Neonataloutcomes in a Medicaid population withopioid dependence. Am J Epidemiol.2018;187(6):1153–1161
HOSPITAL PEDIATRICS Volume 9, Issue 8, August 2019 623
by guest on February 19, 2021www.aappublications.org/newsDownloaded from

DOI: 10.1542/hpeds.2018-0238 originally published online July 8, 2019; 2019;9;615Hospital Pediatrics
SuttonThomas Blount, Alana Painter, Emily Freeman, Matthew Grossman and Ashley G.
Console'' MethodReduction in Length of Stay and Morphine Use for NAS With the ''Eat, Sleep,
ServicesUpdated Information &
http://hosppeds.aappublications.org/content/9/8/615including high resolution figures, can be found at:
Supplementary Material
2018-0238.DCSupplementalhttp://hosppeds.aappublications.org/content/suppl/2019/07/05/hpeds.Supplementary material can be found at:
Referenceshttp://hosppeds.aappublications.org/content/9/8/615#BIBLThis article cites 15 articles, 6 of which you can access for free at:
Subspecialty Collections
rovement_subhttp://www.hosppeds.aappublications.org/cgi/collection/quality_impQuality Improvementon:practice_management_subhttp://www.hosppeds.aappublications.org/cgi/collection/administratiAdministration/Practice Managementfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
mlhttp://www.hosppeds.aappublications.org/site/misc/Permissions.xhtin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.hosppeds.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on February 19, 2021www.aappublications.org/newsDownloaded from

DOI: 10.1542/hpeds.2018-0238 originally published online July 8, 2019; 2019;9;615Hospital Pediatrics
SuttonThomas Blount, Alana Painter, Emily Freeman, Matthew Grossman and Ashley G.
Console'' MethodReduction in Length of Stay and Morphine Use for NAS With the ''Eat, Sleep,
http://hosppeds.aappublications.org/content/9/8/615located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://hosppeds.aappublications.org/content/suppl/2019/07/05/hpeds.2018-0238.DCSupplementalData Supplement at:
Print ISSN: 1073-0397. Illinois, 60143. Copyright © 2019 by the American Academy of Pediatrics. All rights reserved. published, and trademarked by the American Academy of Pediatrics, 345 Park Avenue, Itasca,publication, it has been published continuously since 1948. Hospital Pediatrics is owned, Hospital Pediatrics is the official journal of the American Academy of Pediatrics. A monthly
by guest on February 19, 2021www.aappublications.org/newsDownloaded from