Embed Size (px)
Citation preview
MORPHINE MILLIGRAM
EQUIVALENTS (MMEs)
Elisabeth Fowlie Mock, MD, MPH, FAAFPMaine Quality Counts
Caring For ME Webinar
11/8/2016

Objectives
By the conclusion of this webinar, the learner will
have:
�Identified & be prepared to use a MME
calculator
�Understood how PMP can assist in improving
quality and safety of patient care
�Strategized to create patient registries for
opioid use
Acknowledgements
� Lisa Letourneau, Quality Counts
� Noah Nesin, PCHC
� Eric Haram, MidCoast Hospital ARC
� Faculty & Participants, QC Chronic Pain
Collaboratives
� Bangor Area Controlled Substance
Workgroup
� Karyn Wheeler & Chris Beaudette, QC
Disclosure
� EFM was a paid Peer Consultant for Maine Quality
Counts’ Chronic Pain Collaboratives 1&2, funded by
an unrestricted grant from Pfizer Independent
Grants for Learning and Change (IGL&C) group.
� MICIS does not receive any direct pharmaceutical
support.
Big Questions
�Which MME calculator to use?
�How will MMEs be handled by Maine’s
Prescription Monitoring Program?
�How can providers keep track of changes in
patients’ daily MME dosage?
�How can practices use EMRs to record
providers’ opioid prescribing by MME?
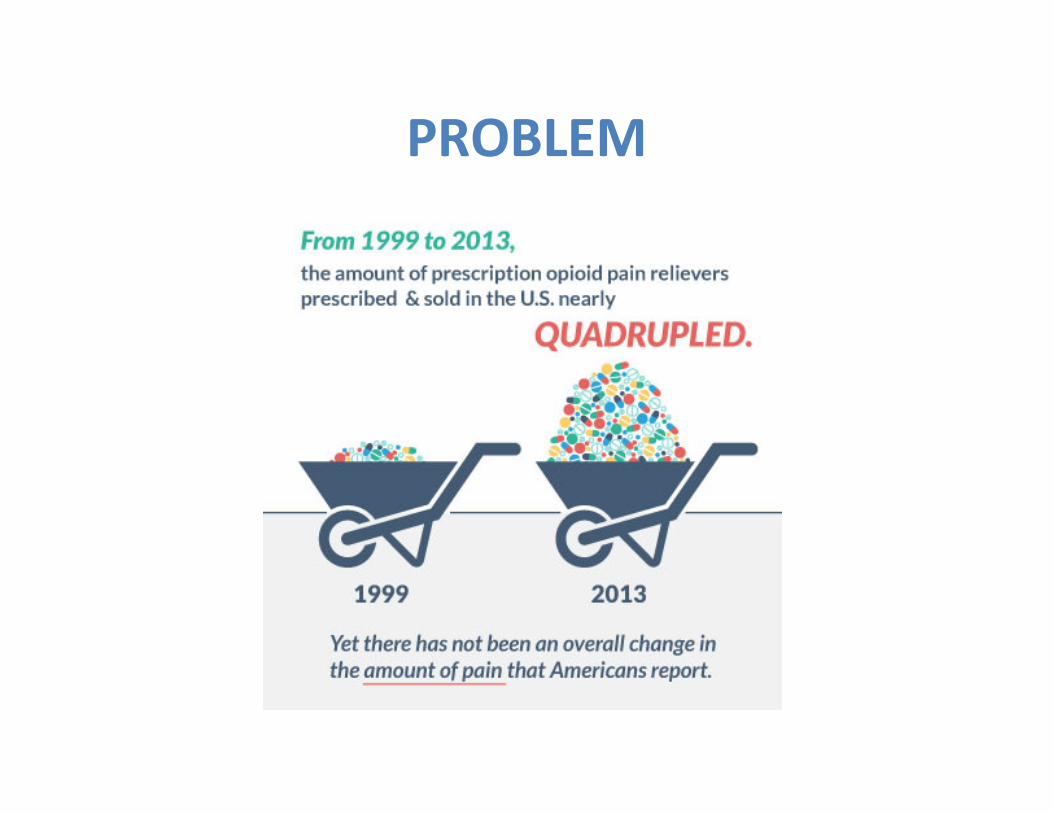
PROBLEM
National Response—March 2016
� Reversing the epidemic
requires changing the
way opioids are
prescribed
� CDC’s Injury Center
developed evidence-
based guidelines for
opioid prescribing
THE HEALTHCARE FORCE AWAKENS
if you only read 1 thing on opioids,
read these 3 pages!
THE TRUTH ABOUT OPIOIDS
“We know of no other
medication routinely used
for a nonfatal condition that
kills patients so frequently.”
Freiden. NEJM: 374;16:1501-4.
Opioids go beyond NNT & NNH:
NUMBER NEEDED TO KILL
�All comers on opioids: NNK=550
�Doses >200 MME: NNK=32
Median time from first opioid rx to death: 2.6 years
Freiden. NEJM: 374;16:1501-4
Maine Chapter 488 (LD 1646)
July 2016
� Limits on script duration (7/30d)
� Mandatory PMP check (opioids/BZDP)
� 100 MME daily limit
� Required CME
� E-prescribing (Schedule II)
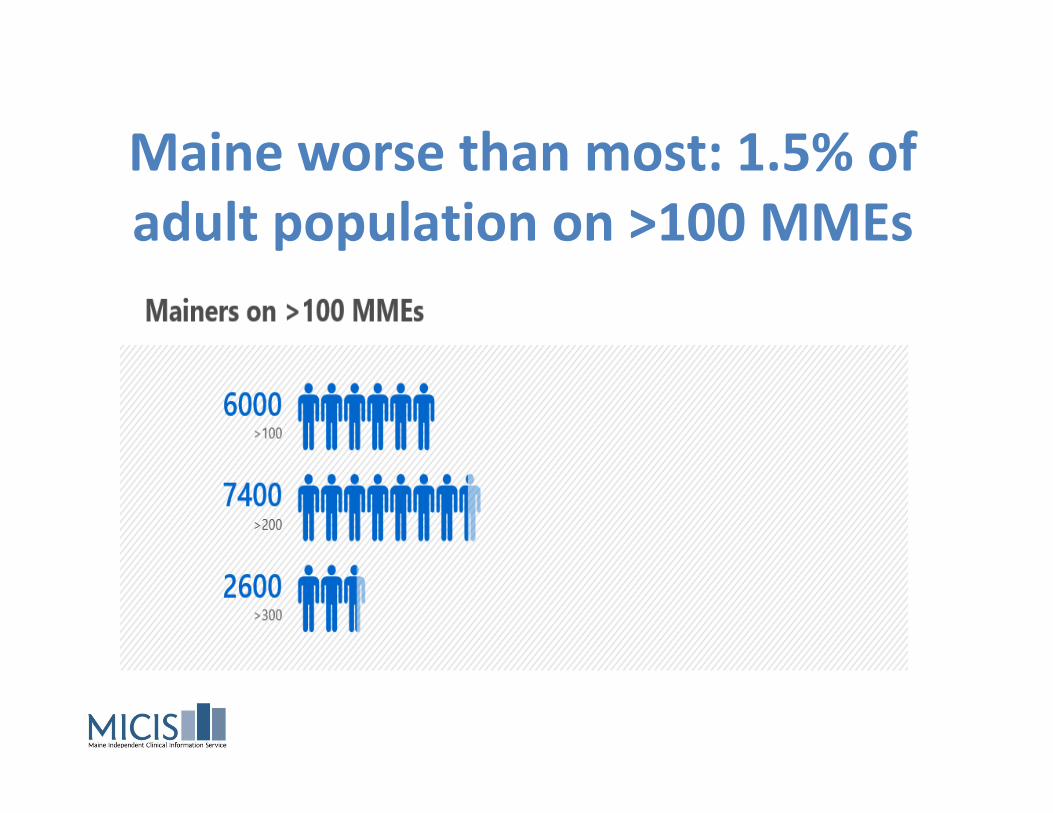
Maine worse than most: 1.5% of
adult population on >100 MMEs
DIFFERENT NAMES FOR THE SAME THING
� MME=morphine milligram equivalent
� MED=morphine equivalent dose
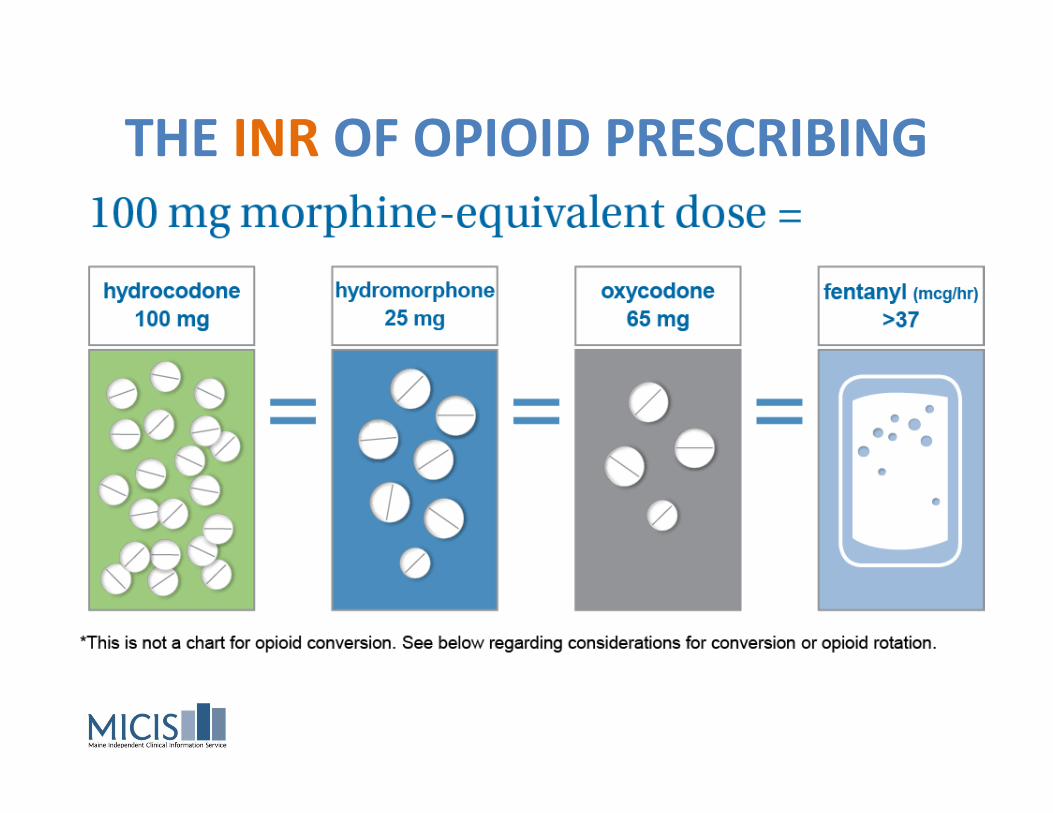
THE INR OF OPIOID PRESCRIBING
Calculating MMEs
Recommended calculator:
http://agencymeddirectors.wa.gov/Calculato
r/DoseCalculator.htm
�BEWARE METHADONE
�PMP will include an calculator “soon”
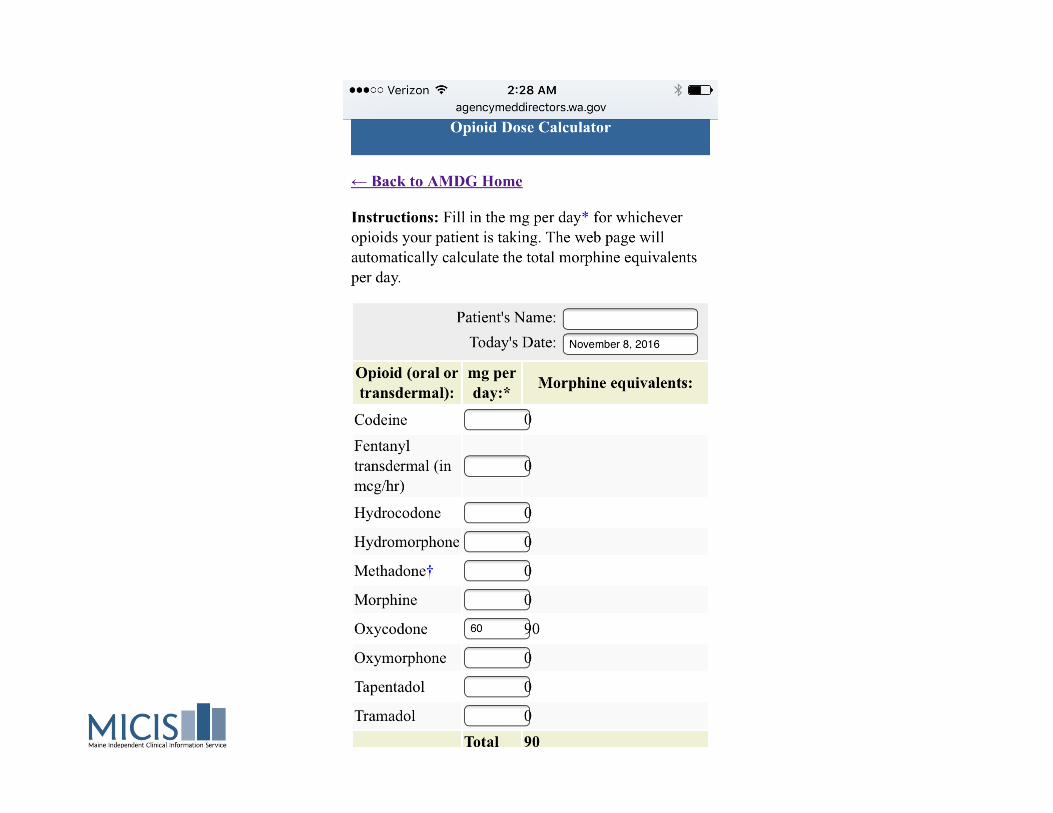
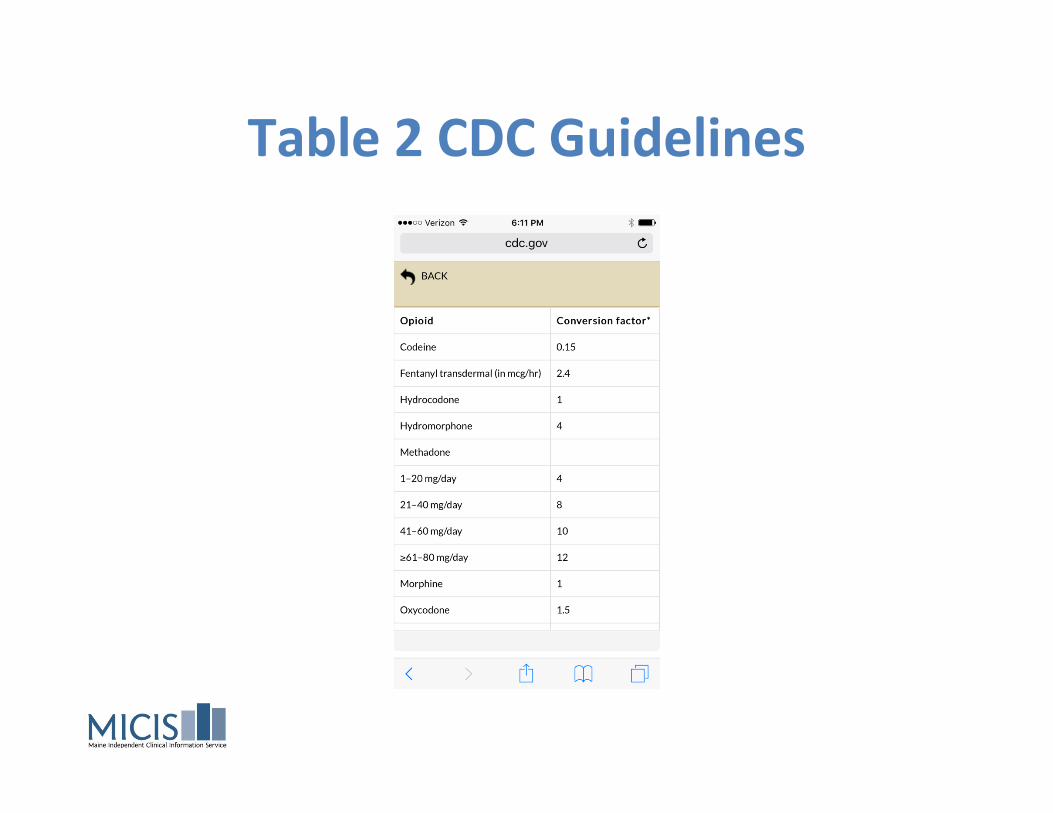
Table 2 CDC Guidelines
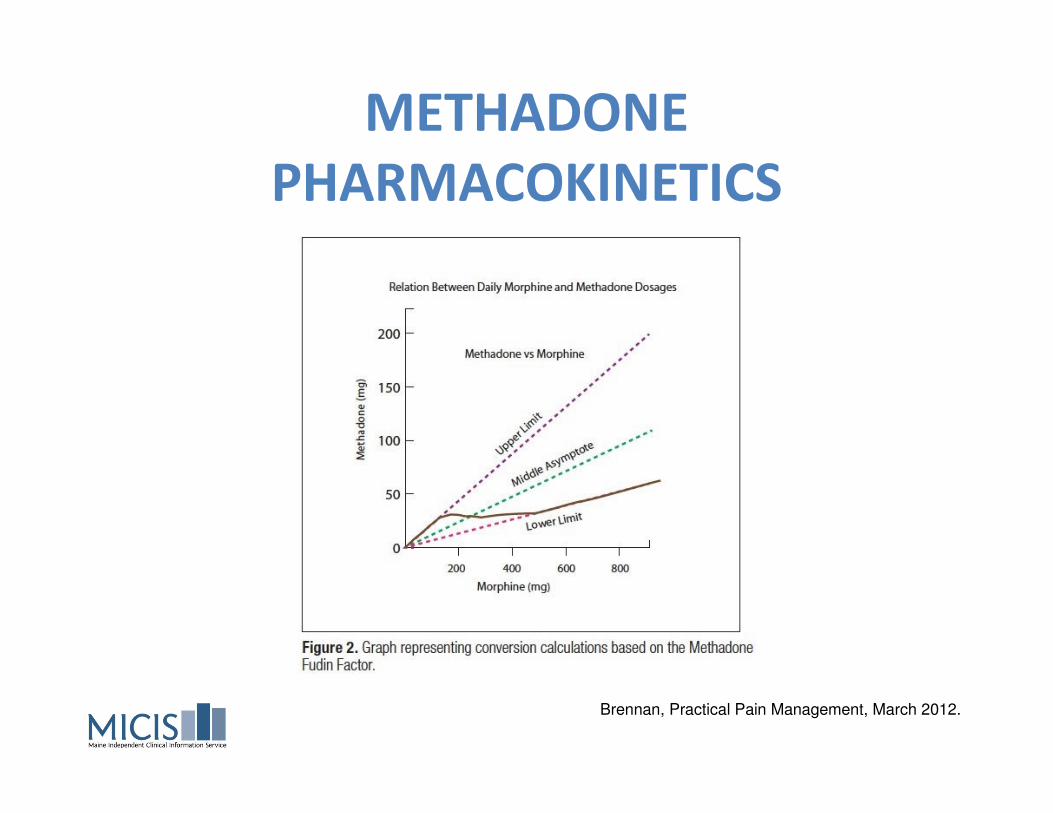
METHADONE
PHARMACOKINETICS
Brennan, Practical Pain Management, March 2012.
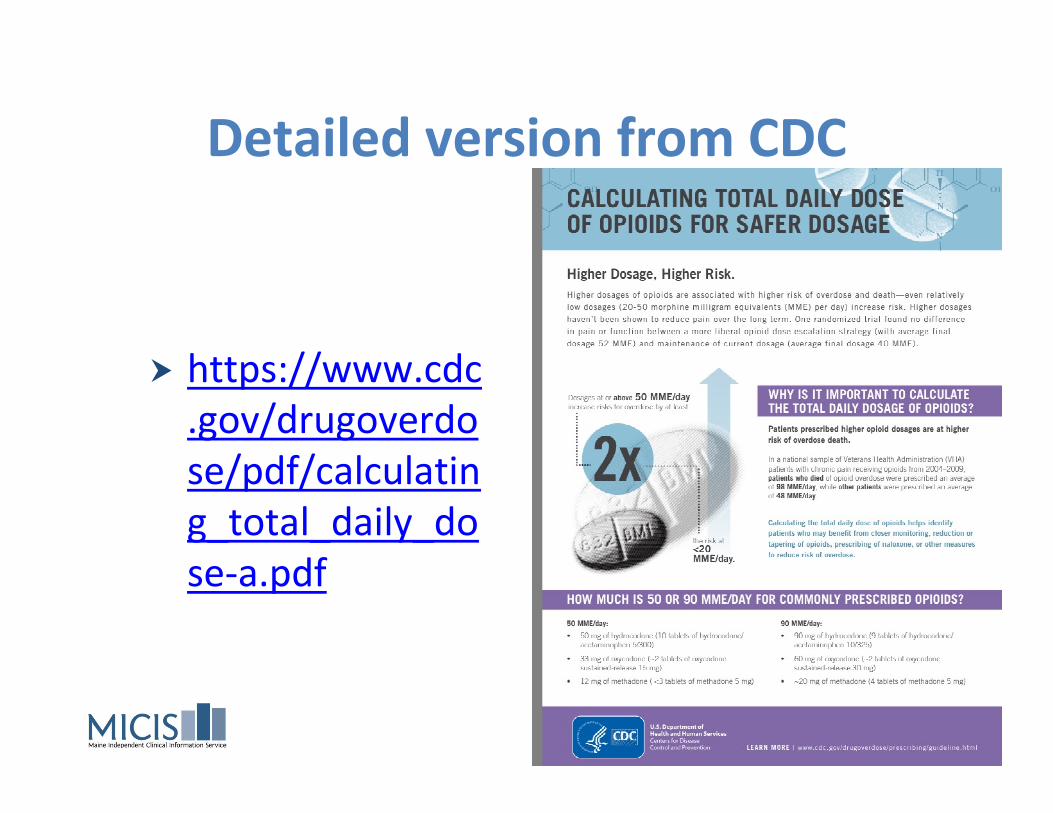
Detailed version from CDC
� https://www.cdc
.gov/drugoverdo
se/pdf/calculatin
g_total_daily_do
se-a.pdf
Calculator Options
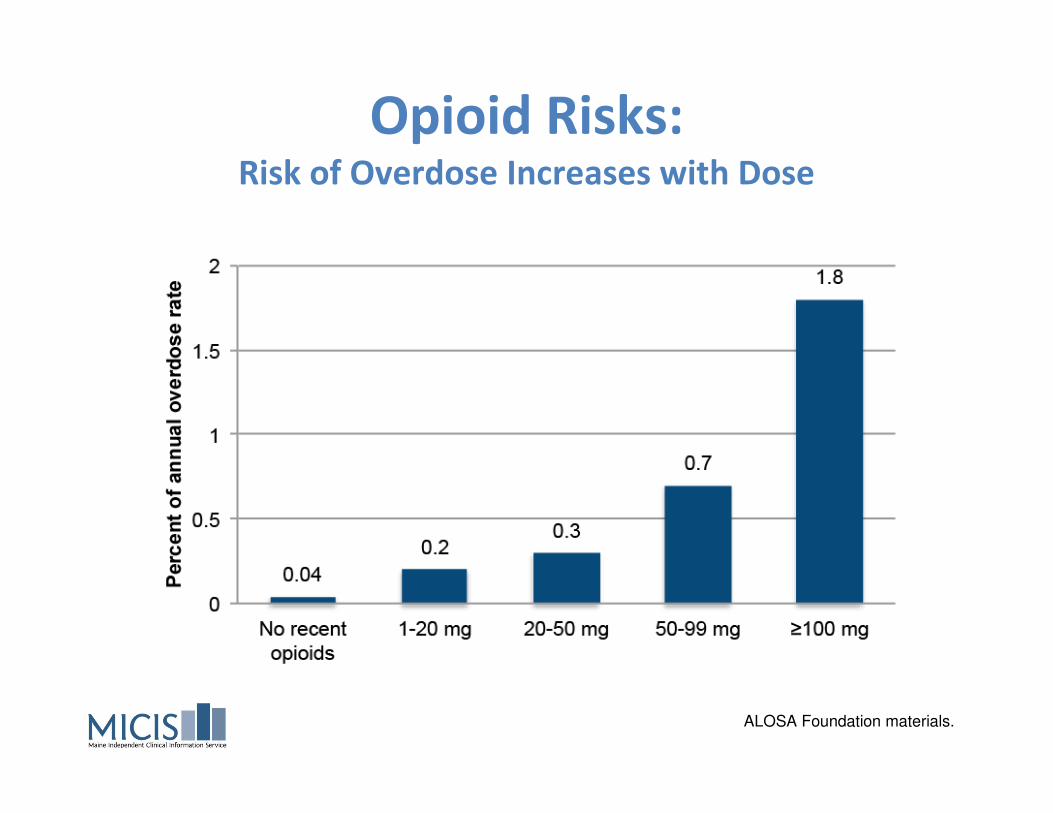
Opioid Risks: Risk of Overdose Increases with Dose
ALOSA Foundation materials.
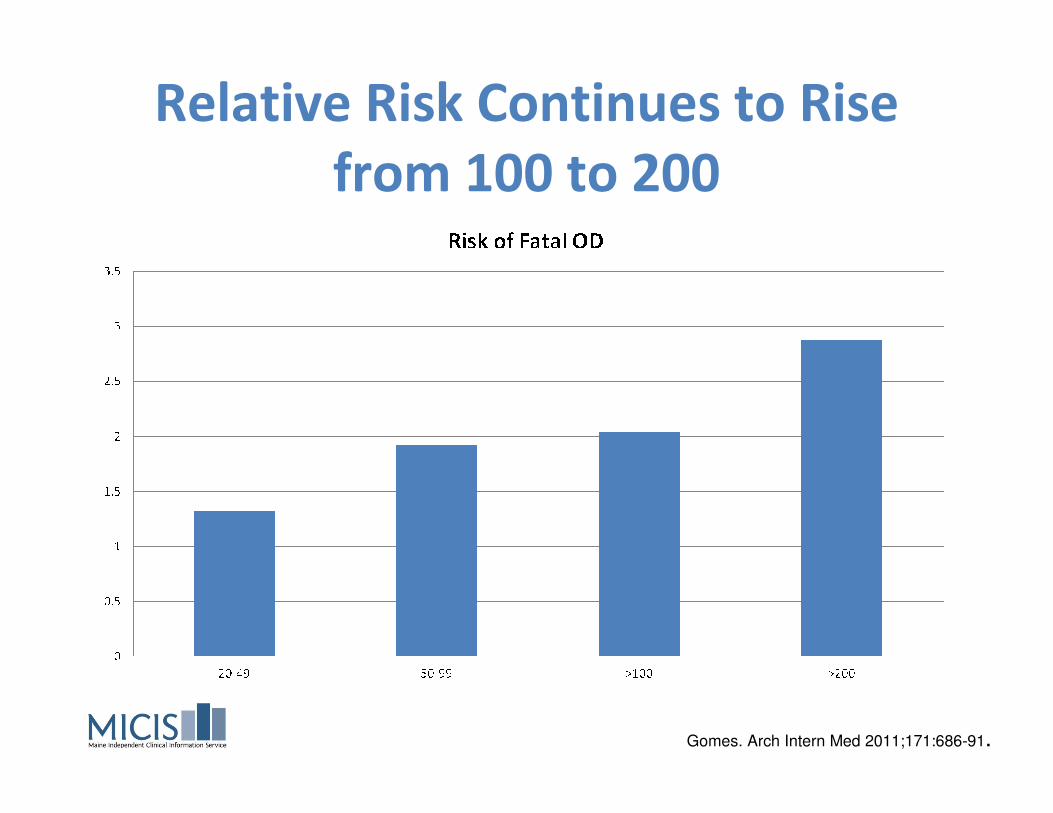
Relative Risk Continues to Rise
from 100 to 200
Gomes. Arch Intern Med 2011;171:686-91.
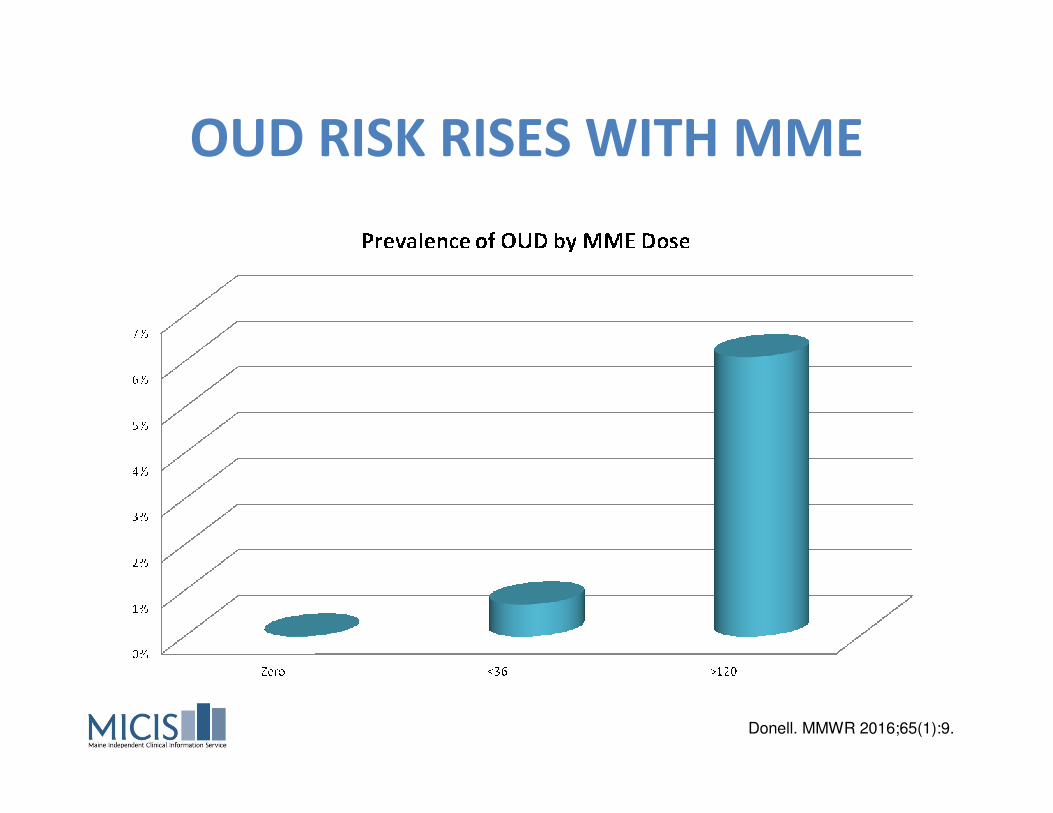
OUD RISK RISES WITH MME
Donell. MMWR 2016;65(1):9.
“There is no completely
safe opioid dose”http://www.agencymeddirectors.wa.gov/Files/2015AMDGOpioidGuideline.pdf
“UNDERAPPRECIATED
CONTRIBUTION”
Benzodiazepines thought to be associated
with nearly 80% of opioid overdose deaths
Gudin. Postgrad Med 2013; 125(4):115-130.
“High-risk Regimens”
� Clinicians should use caution when
prescribing opioids at any dosage, should
carefully reassess evidence of individual
benefits and risks when increasing dosage to
≥50 morphine milligram equivalents
(MME)/day, and should avoid increasing
dosage to ≥90 MME/day or carefully justify a
decision to titrate dosage to ≥90 MME/day.
CDC Guidelines, April 2016.

Monitoring Frequency
� Published guidelines recommend re-
evaluation (face-to-face appointment) by
prescriber
– every 90d for patients receiving >50 MMEs
– every 30d for patients receiving >120 MMEs
CDC 2016 Guidelines; WA State Medical Directors
Bangor Area Controlled Substance
Workgroup (BACSG)
� Collaborative effort among EMHS, St.
Joseph’s, PCHC, Acadia, CHCS and multiple
other entities
� Developed standard INFORMED CONSENT
and Prescribing Guidelines for OPIOIDS,
BENZOS, STIMULANTS
Chronic Pain
Playbook
� Mainequalitycounts.org/
controlledmedication
playbook
Harm reduction
� Hardwire naloxone
protocols into your
practice
� Ideally rx to all patients on
opioids
� Highest risk: co-rx’d BZDP,
EtOH use, respiratory
compromise, MME>50https://www.mainemed.com/MICIS
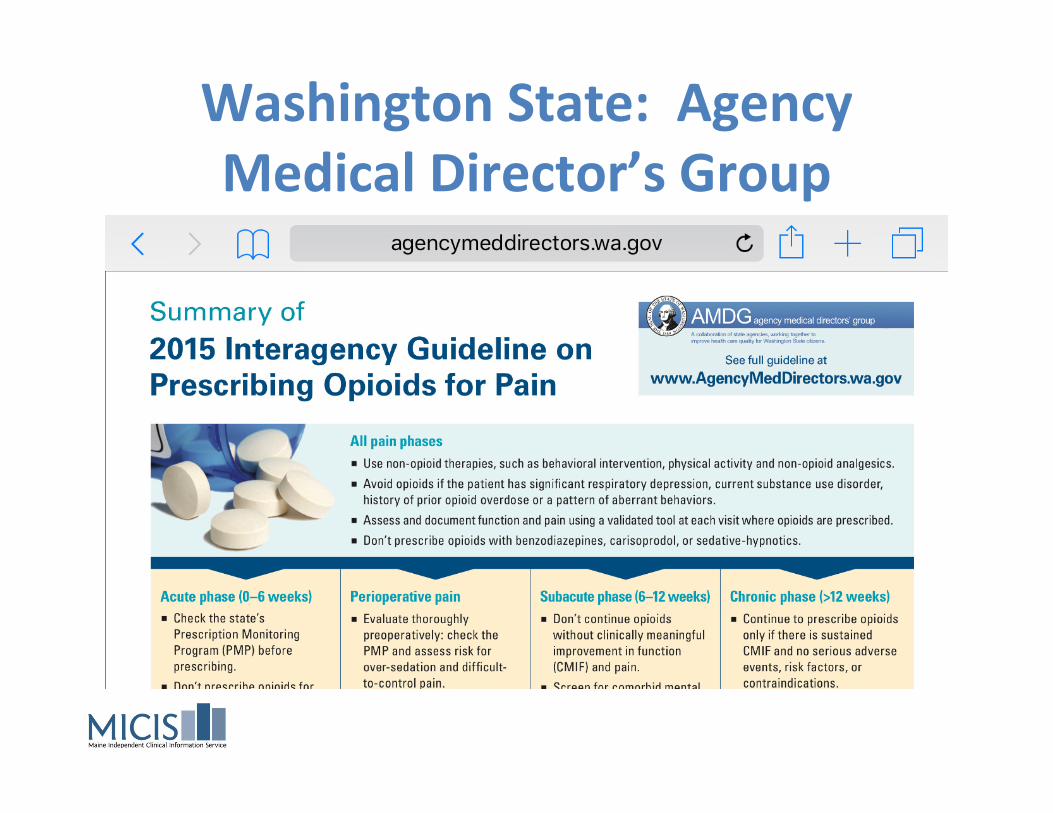
Washington State: Agency
Medical Director’s Group
Creating a Registry
� Methods:
� EMR generated list triggered by ICD codes,
problem list or prescriptions
� Manually compiled list from individual provider’s
PMP lists (suggest 3 month window)
� Prospectively generated list from refill requests
Using the registry
� Some practices are able to actively engage a
list through the EMR
� Many others end up creating a spreadsheet
and managing manually (time/labor intensive
but decreases as weanings progress)
PATIENT X, early 2016
PROBLEM LIST
� HYPERTENSION
� OBSTRUCTIVE SLEEP APNEA, INTOLERANT
OF CPAP
� CHRONIC BACK PAIN ON CHRONIC OPIOIDS,
MME=220
� CHRONIC KIDNEY DISEASE STAGE 3
� DEPRESSION
� PTSD
PATIENT X, late 2016
PROBLEM LIST
� HYPERTENSION
� OBSTRUCTIVE SLEEP APNEA, INTOLERANT
OF CPAP
� CHRONIC BACK PAIN ON CHRONIC OPIOIDS,
MME=120, actively tapering
� CHRONIC KIDNEY DISEASE STAGE 3
� DEPRESSION
� PTSD
PATIENT X, 2017 PROBLEM LIST
� HYPERTENSION
� OBSTRUCTIVE SLEEP APNEA, INTOLERANT
OF CPAP
� CHRONIC BACK PAIN, OPIOIDS
DISCONTINUED
� CHRONIC KIDNEY DISEASE STAGE 3
� DEPRESSION
� PTSD
THINK LOCAL
� For local resources regarding utilizing EMRs
for chronic pain and opioid management,
contact these Maine practices who
participated in 12-18 month learning
collaboratives:
– Local experts
– Early adopters
– Ready to spread best practices
CPC1 Participants
� Bucksport Regional Health Center
� CMMC Family Medicine Residency, Lewiston
� DFD Russell Medical Center, Leeds
� EMMC Center for Family Medicine (Residency), Bangor
� Harrington Family Health Center
� Sacopee Valley Health Center (ECHO only), Porter
� Scarborough Family Medicine
� St. Joseph Internal Medicine, Bangor
CPC2 Participants� Brewer Medical Center (PCHC)
� CMMC Family Medicine Residency, Lewiston
� EMMC Husson Family Medicine, Bangor
� Dover Foxcroft Family Medicine
� Inland Family Care, Unity
� Maliseet Health and Wellness Center, Littleton
� Mark Braun, MD, Scarborough
� MMP Family Medicine Portland/Falmouth
� St. Joseph Internal Medicine, Bangor
� Sheepscot Valley Health Center, Coopers Mills
� Swift River Family Medicine, Rumford
� Westbrook Primary Care
� Winterport Community Health Center
Under CPC1 section
on QC website
Big Questions
�Which MME calculator to use?
�How will MMEs be handled by Maine’s
Prescription Monitoring Program?
�How can providers keep track of changes in
patients’ daily MME dosage?
�How can practices use EMRs to record
providers’ opioid prescribing by MME?









![Abstracts of the 10th Annual Meeting of the Lumbar Spine ... · risk [RR]=1.66, p=0.015) and narcotic consumption greater than 85 oral morphine equivalents on postoperative day 0](https://img.pdfslide.us/doc/110x75/605294e4171017610e21c9c2/abstracts-of-the-10th-annual-meeting-of-the-lumbar-spine-risk-rr166-p0015.jpg)