Embed Size (px)
Citation preview

Heroin,Fentanyl and other
Opioids
Steve Hanson

Heroin/Opioids
142Americans
192


Neurotransmitter Action
ReuptakeRelease of NT
Receptor

Brain Changes

This is Your Brain on Drugs
6

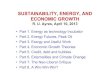
Opiates Increase DA Release

0
100
150
200
250
0 1 2 3 4 5hr
Time After Morphine
% o
f B
asal R
ele
ase
MORPHINE
Source: Di Chiara and Imperato
HEROIN

What Drugs Do
Agonists
• Increase NT activity
• Produce more NT
• Block Reuptake
• Mimic NT’s
Antagonists
• Decrease NT activity
• Block NT’s
• Decrease NT’s
Mixed• Ceiling effect

Opiates
• Dates to 4,000 BC
• Mimics endorphin activity
• Natural - Opium, morphine, codeine
• Semi-synthetic- Heroin, Dilaudid
• Synthetics - Darvon, Demerol, Fentanyl

Modern History• Off and on use through until the 60’s
• “Man with the Golden Arm”
• Vietnam war – soldiers using heroin
• 1970’s – increased prevalence – urban areas
• Treatment programs – Methadone Maintenance / Therapeutic Communities
• 1980’s Hard to find – substitutes
• 1990’s – resurgence
• 2010’s – “epidemic”

Opiates
•Heroin more potent -60-80% - <10% in ‘70’s
•Younger age group - High School
•Users start with snorting - IV within 12 months
•Withdrawal painful - not deadly

NATURAL OPIATES
MorphineCodeineThebaine
OPIUM

Semi-synthetics
Heroin Dilaudid
Morphine


Synthetics
• Demerol
• Fentanyl
• Methadone
• Darvon

Opiates
• Fat solubility – Heroin – high – rush
• Morphine – lower – longer onset
• Heroin metabolized into morphine
• Morphine metabolized by the liver
• Metabolite is 10-20X more powerful
• Detectable in urine for 2-4 days

The Action ofHeroin(Morphine)

Tolerance
• Rapid tolerance with continued use
• Initial dose of 50mg/day can go to 500mg/day in as little as 10 days
• Cell sensitivity thought to be the tolerance mechanism.

Opiates & Reward Pathway

Opiates Increase DA Release

Agonists, Mixed and Antagonists

Heroin
Effects
• Analgesia - change in pain perception
• Euphoria - intense• Sedation - “on the nod”• Respiratory depression• Cough suppression• Nausea/vomiting• Constipation
Withdrawal
• Pain• Depression• Alert• Rapid breathing• Coughing• Nausea/vomiting• Diarrhea• 3-5 days

Addiction/Dependency Cycle
•Opioids trigger reward system – euphoria – leads to continued use – addiction
•Withdrawal symptoms are significant – regular use to avoid withdrawal - dependence

Addiction vs. Dependency

Natural History of Opioid Dependence

Potency Factors by Weight
• Morphine 1
• Heroin 3
• Codeine 0.1
• Dilaudid 8
• Demerol 0.05
• Fentanyl 300 - 1000

Heroin usage patterns
•Highly addictive and dependence producing
•Significant tolerance up to 35X
• Increased cost
•Tolerance management (Tx, jail, etc.)
•Mixing with other opiates and other drugs (speedballing/cocaine)

OxyContin
• Oxycodone – synthesized from thebaine (part of opium)
• OxyContin – 1995• Crush the tablet for quicker high
• Oral, snort, inject
• Percocet – oxycodone & acetaminophen
• Percodan – oxycodone & aspirin

Vicodin
•Hydrocodone and acetaminophen
• Lorcet, Lortab
•Schedule III – high psychological/medium physical
•Pain and post-surgical use (pain)

Fentanyl
• Synthetic Opiate
• Very powerful formulas
• Extensive Medical Use
• Sold as heroin
• High overdose risk

Potency
NIDA

Overdose amount

Treatment
• Traditional Recovery Based/NA
• Naltrexone - Antagonist/Blocker
• Opiate Maintenance Tx – withdrawal management• Methadone- daily
• Buprenorphine/Suboxone
• Methadone to abstinence models

PharmacotherapyMethadone
Buprenorphine
Naltrexone
Psychosocial Interventions
CBT, MI, CM
Recovery SupportAA, NA, SMART Recovery
Recovery Coaches
What is effective treatment?

Detox
• Detox: Medical risk with opioid withdrawal is low, while discomfort is very high • Inpatient • Outpatient
• Only recommended during 2nd trimester of pregnancy if mother is invested
• Otherwise methadone stabilization is in best interest of mother and fetus

Levels of Care
• Inpatient rehabilitation• 5-21 days length of stay• Focus on medical/psychiatric stabilization• May initiate Suboxone for opiates
• Community residence (halfway houses)• Supportive living environment• 3-12 months

Levels of Care
• Intensive Residential
▪ Supportive environment – therapeutic community
▪ Longer term stays 6-24 months
▪ Focus on rehabilitation/sober living skills
• Outpatient
▪ Intensive outpatient

Does Treatment Work?
• Medications +psychosocial therapy bothbenefit brain function and recovery.
• Each affects different partsof brain and inopposite ways.
PET scans adapted and retouched from Goldapple et al. 2004

Pharmacological Approaches
Goals – Provide:• relief from withdrawal symptoms,
• prevent drugs from working,
• reduce craving,
• aversive reactions
These actions are helpful in
reducing relapse and increasing
retention in programs

Pharmacological Approaches
Methadone – Opiate addiction – reduces craving, mediates withdrawal symptoms, helps restore normal functioning
Buprenorphine (Suboxone) – similar to methadone, may be prescribed by an MD with special training)
Naltrexone (Vivitrol) – stops opiates from working, changes alcohol action for some – reduction in relapse – 30 day dose.

Pharmacology of Treatments

Patient Needs
Diabetes
• Some can control with diet
• Some can control with medication
• Some are insulin dependent
• Without adequate treatment -many will die
Opiod Addicts
• Some can quit on own
• Some can remain abstinent with “regular” treatment
• Some need ORT
• Without adequate treatment -many will die

Buprenorphine Maintenance75% retained in treatment75% abstinent by toxicology
Detoxification0% retained in treatment20% died
Kakko et al. Lancet. 2003 Feb 22;361(9358):662-8
Buprenorphine is Effective at Retaining Patients in Treatment & Preventing Relapse

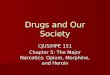
Methadone EffectivenessGunne & Gronbladh, 1984
H H HH
H H HH
H H HH
H H HH
H
H H HH
H H HH
H H HH
H H HH
H
Methadone Regular Outpatient Rx.
Baseline

Methadone EffectivenessGunne & Gronbladh, 1984
After 2 Years
1- Sepsis & endocarditis
2- Leg amputation
3- Sepsis
P H HH
H
P HP
H H HH
H H HH
H H H
Methadone No Methadone1
32
D
D

Methadone EffectivenessGunne & Gronbladh, 1984
P H H
H
P
Methadone No Methadone
After 5 Years
P P D
D
D
D
D

Centers for Disease Control (2011)
Retention in treatmentHeilig, Lancet 2003

BuprenorphineA tragic appendix: Mortality
Heilig, Lancet 2003
Placebo BPN
Dead 4/20 (20%) 0/20 (0%)

Vivitrol•Long Acting
Injectable
•Helps with compliance
•Non-Addicting

Is Vivitrol “THE ANSWER”?
2015 Vermont Review
• Research is limited. FDA approval based on a single 6 month trial in Russia.
• Health Risk – Liver toxicity, Death (51 from 2006-2010)
• Overdose Risk upon termination
• Effective for Some – still to be defined

NARCAN - Overdose Reversal Kits
7/9/2019 52

Alive is Good!