Embed Size (px)
Citation preview
Chris Parry
Wellcome Trust Major Overseas Programme in Tropical Medicine Mahidol-Oxford Tropical Medicine Research Unit
Bangkok, Thailand
Chittagong Medical College Hospital, Bangladesh Angkor Hospital for Children, Cambodia
Rational use of Microbiology
What are the problems?
Individual patient microbiology
Public health microbiology and disease surveillance
Does it matter?
Rational use of Microbiology
What are the problems?
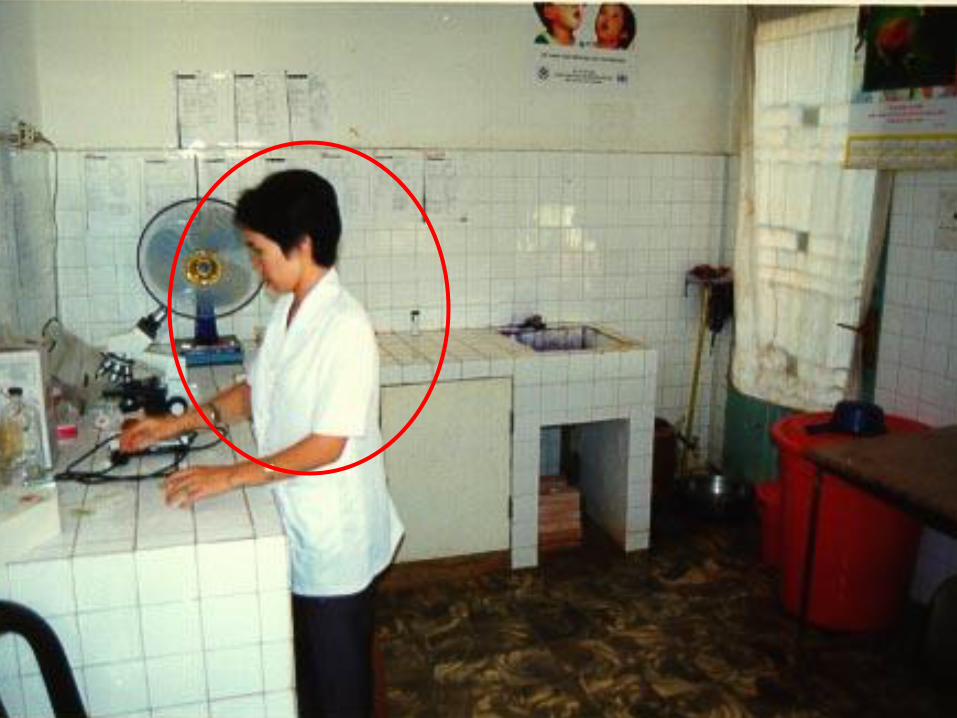
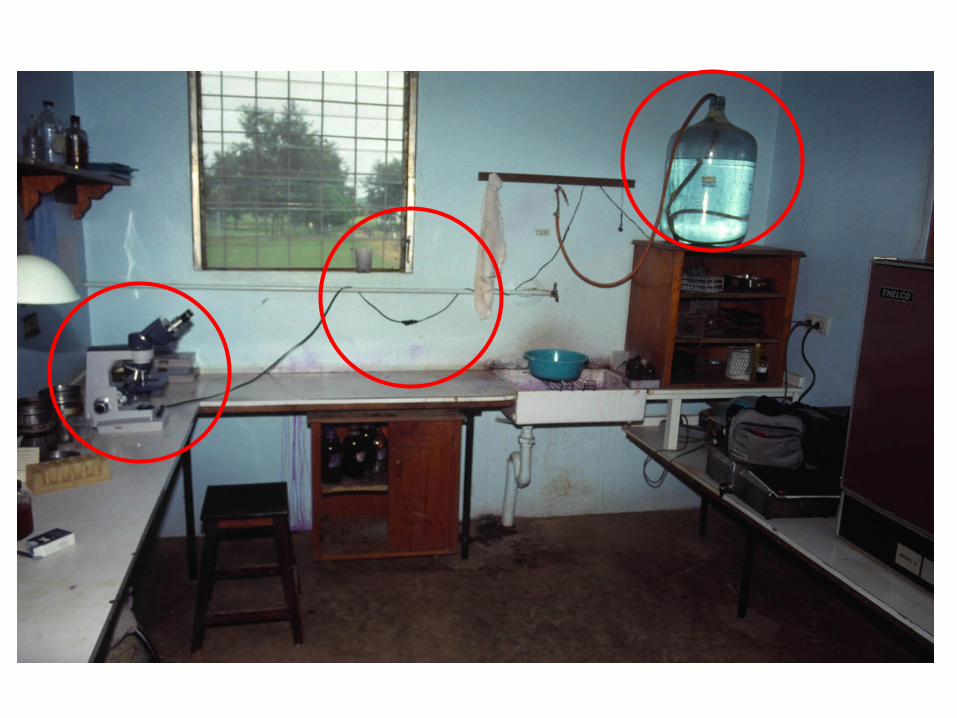


Private laboratories
Sample Result Cost?
Private laboratories
Sample Result Quality?
Outside the government network
• Individual patient management
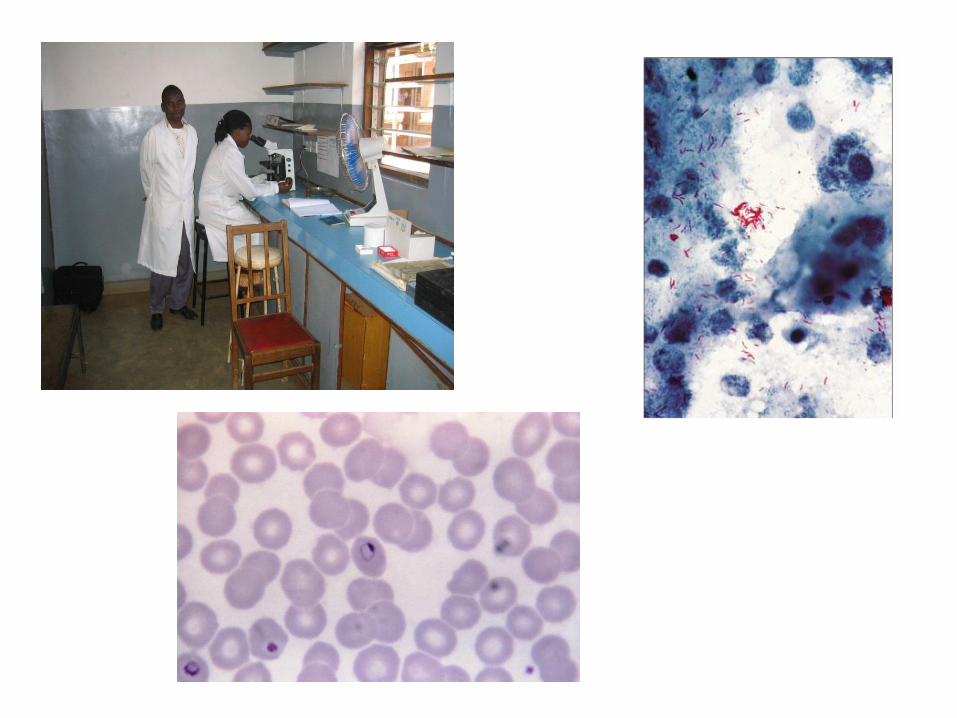
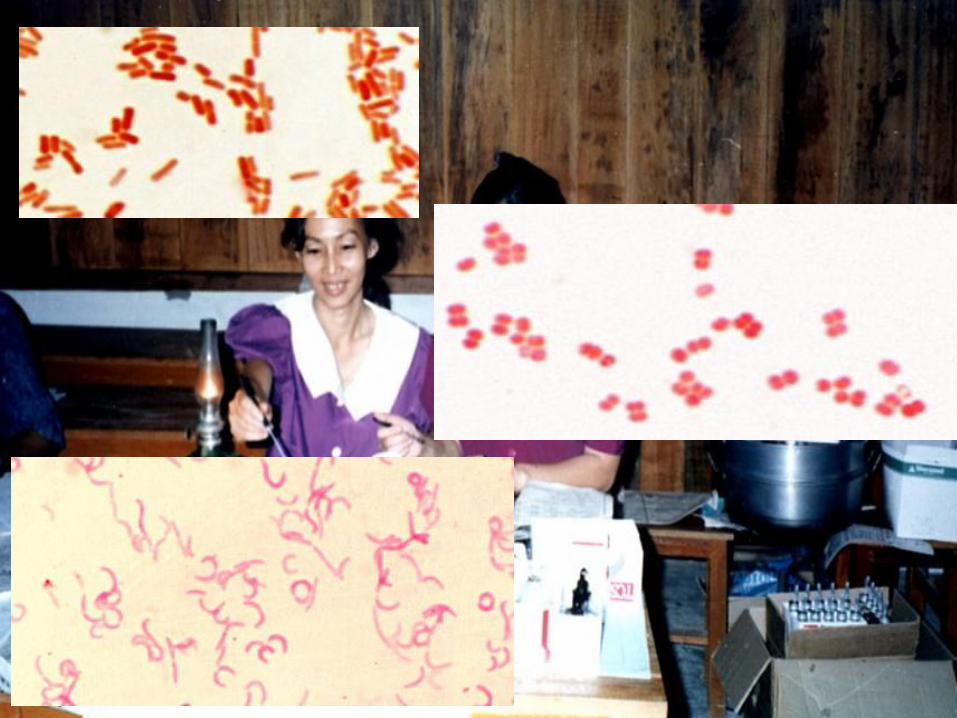
• Microscopy
• Bacterial culture
• Serology
• Molecular methods management
What is the laboratory service for?
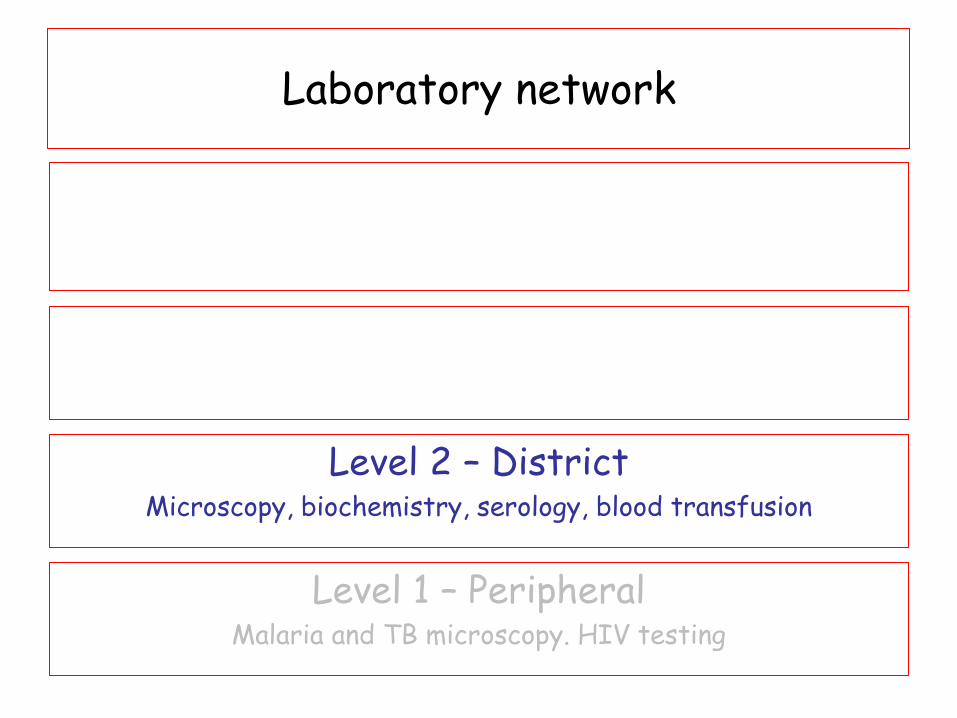
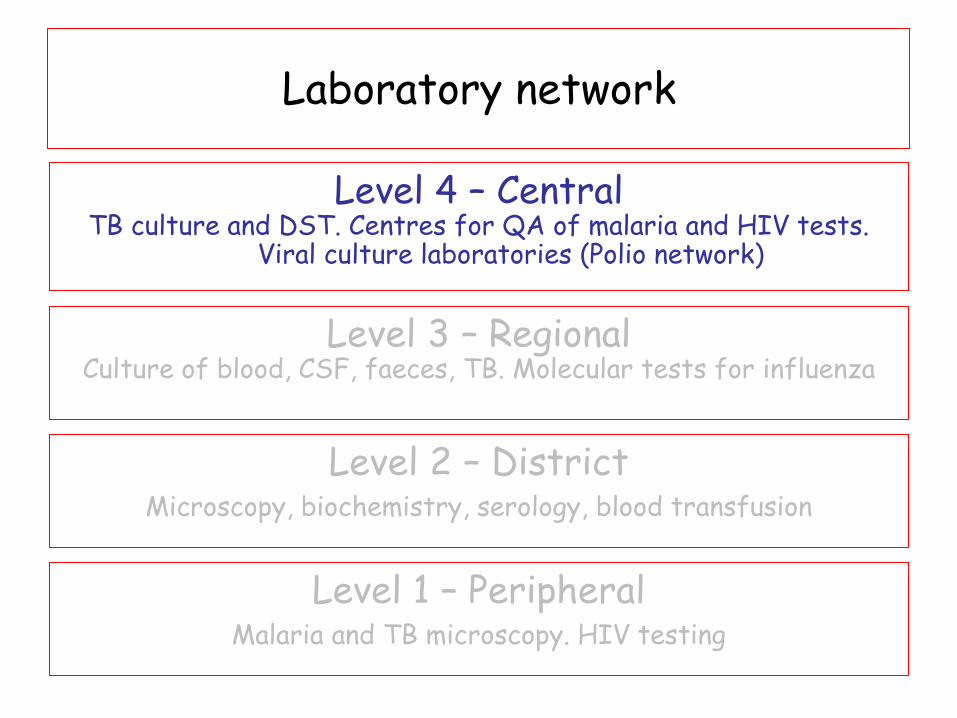
Laboratory network
Level 1 – Peripheral Malaria and TB microscopy. HIV testing
Level 2 – District Microscopy, biochemistry, serology, blood transfusion
Level 3 – Regional Culture of blood, CSF, faeces, TB. Molecular tests for influenza
Level 4 – Central TB culture and DST. Centres for QA of malaria and HIV tests.
Viral culture laboratories (Polio network)
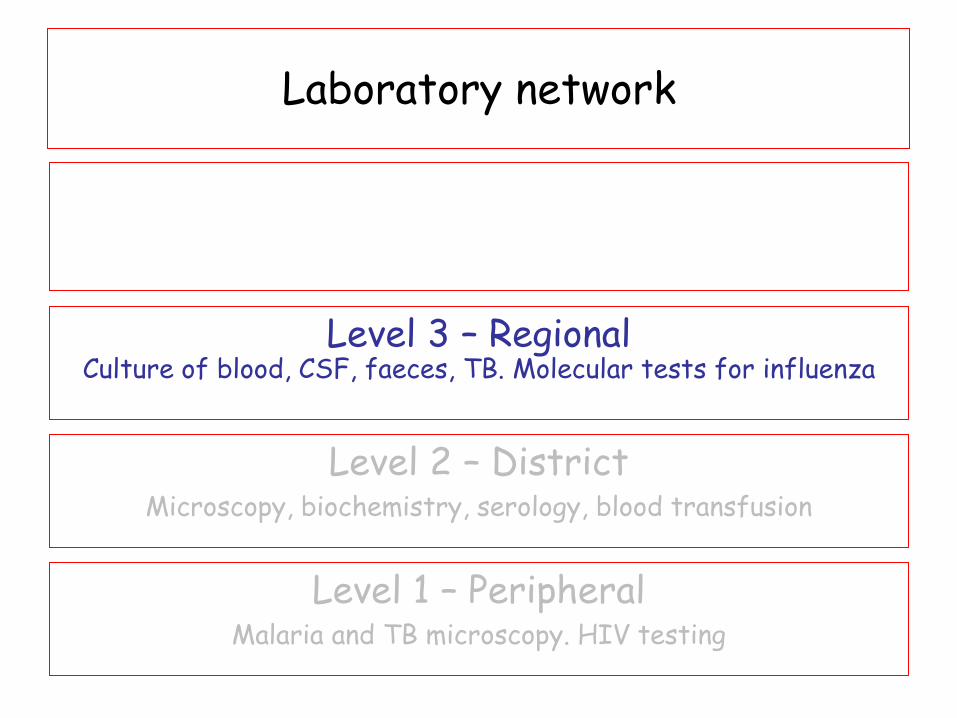
Laboratory network
Level 1 – Peripheral Malaria and TB microscopy. HIV testing
Level 2 – District Microscopy, biochemistry, serology, blood transfusion
Level 3 – Regional Culture of blood, CSF, faeces, TB. Molecular tests for influenza
Level 4 – Central TB culture and DST. Centres for QA of malaria and HIV tests.
Viral culture laboratories (Polio network)
Laboratory network
Level 1 – Peripheral Malaria and TB microscopy. HIV testing
Level 2 – District Microscopy, biochemistry, serology, blood transfusion
Level 3 – Regional Culture of blood, CSF, faeces, TB. Molecular tests for influenza
Level 4 – Central TB culture and DST. Centres for QA of malaria and HIV tests.
Viral culture laboratories (Polio network)
• 25/M, teacher
• Previously well
• Fever, cough and nausea for 5 days
• Cefuroxime 500 mg po bid for 4 days
• Temperature 1030F
• Slight hepatomegaly
• WBC 6200 (N 78, L 20)
• AST 138; ALT 127
Patient 1
• Cefixime 200 mg IV bd -1 day
• Co-amoxyclav 1.2 g IV tds – 4 days
• No improvement
• Still high fever
Patient 1
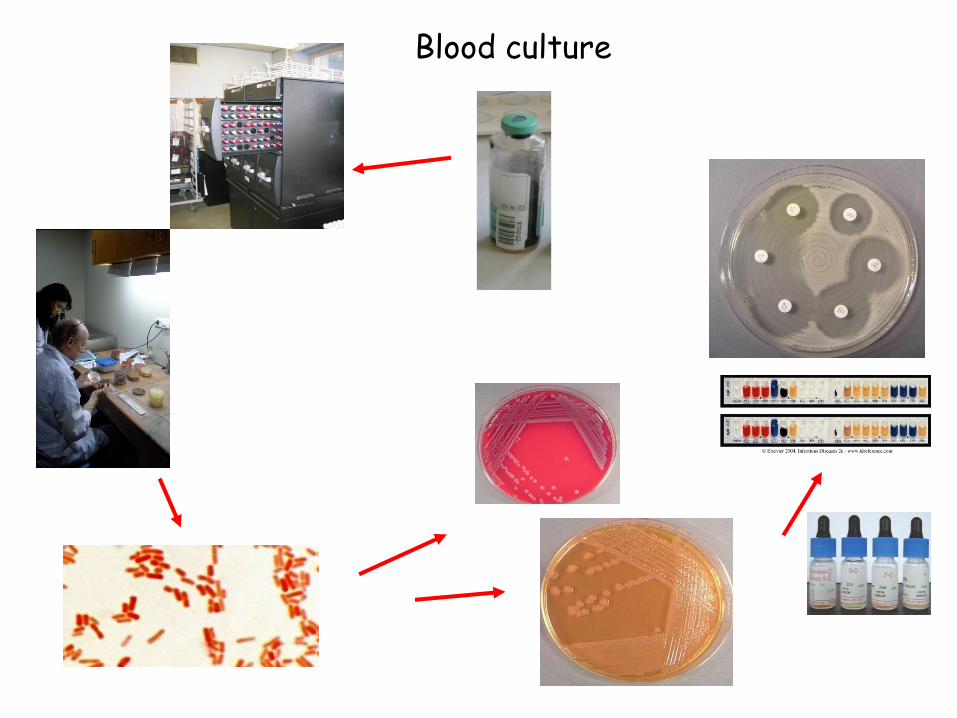
Blood culture
Blood culture:
Salmonella enterica serovar Typhi
Resistant to
Chloramphenicol , Ampicillin and Co-trimoxazole
Nalidixic acid
Decreased susceptibility to
Ciprofloxacin
Susceptible to
Ceftriaxone, Azithromycin
Patient 1
• Diagnosis: Typhoid fever
• Ceftriaxone 2 g IV od – 5 days
• Clinical condition was improved
• Discharged home
• Azithromycin 500mg oral od - 7 more days
Patient 1
Patient 2
• 30/M, farmer
• Fever; Abdominal pain; Nausea and vomiting 5 days
• Co-amoxyclav – no improvement
• Unwell; Temp 101.40C;
• Tender L side abdomen
• WBC 14000 (N 90, L 10)
• Urine: Pus cells ++
• Blood culture:
• Enterobacter cloacae
• Resistant:
• Ampicillin, chloramphenicol, co-trimoxazole,
co-amoxyclav, ceftriaxone
Patient 2
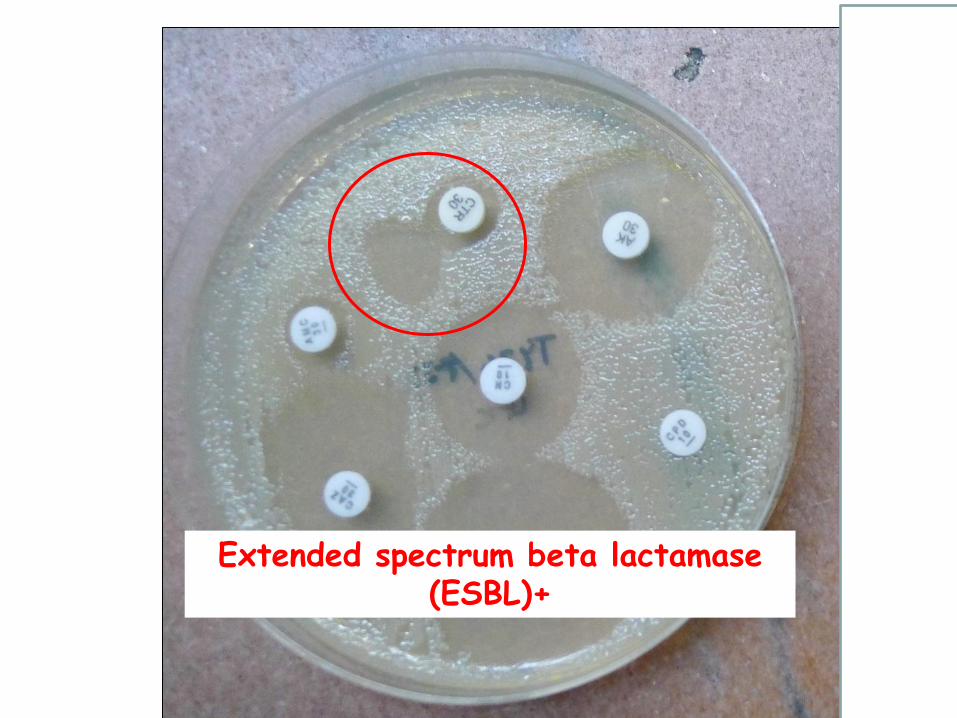
Extended spectrum beta lactamase (ESBL)+
• Blood culture:
• Enterobacter cloacae
• Resistant:
• Ampicillin, chloramphenicol, co-trimoxazole,
co-amoxyclav, ceftriaxone
• Suscseptible:
• Imipenem, ciprofloxacin, gentamicin
Patient 2
• Diagnosis:
Enterobacter UTI with bacteraemia
ESBL + strain
• Treatment changed to ciprofloxacin
• Good recovery
Patient 2
Bacterial Culture - Advantages
– Establish the microbiological diagnosis
– Sensitivity/resistance result to guide antimicrobial
choice
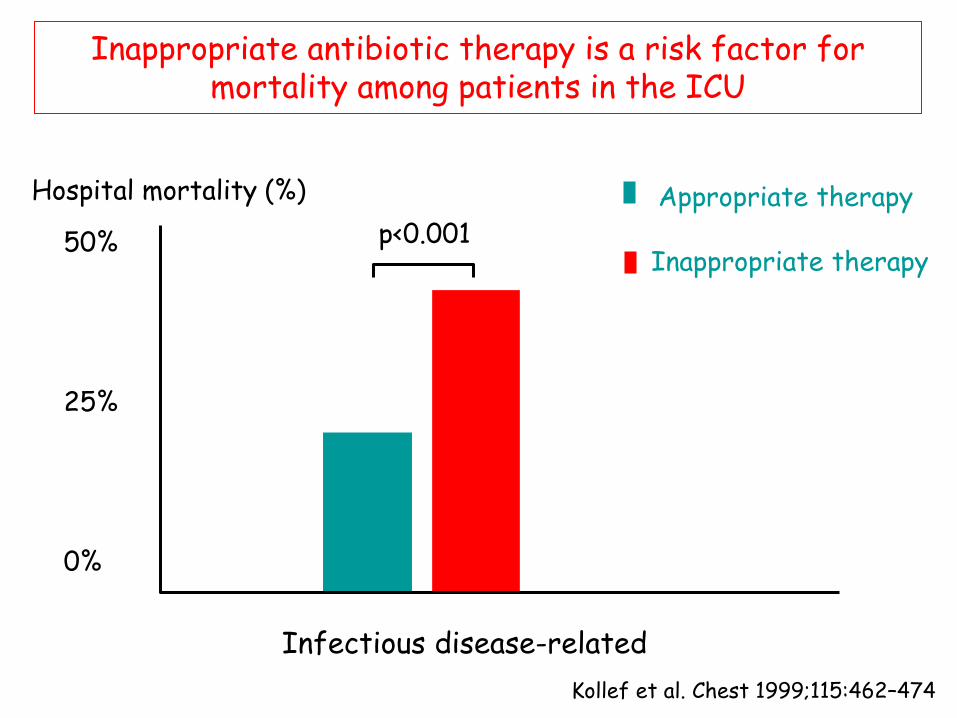
Inappropriate antibiotic therapy is a risk factor for mortality among patients in the ICU
Kollef et al. Chest 1999;115:462–474
Hospital mortality (%)
0
20
50
Appropriate therapy
Inappropriate therapy
40
30
10
Infectious disease-related
p<0.001 50% 25% 0%
Bacterial Culture – Further advantages
– Establish the common bacteria causing sepsis in
your location
– Define the resistance patterns of these common infections
– Helps with empiric antimicrobial choices
– Lead to development of an antimicrobial guideline
Bacterial Culture - Disadvantages
– Slow
– Expensive
– Skin contamination
– May be negative because of:
• Prior antibiotic treatment • Volume of blood too small
– Negative blood culture does not exclude infection
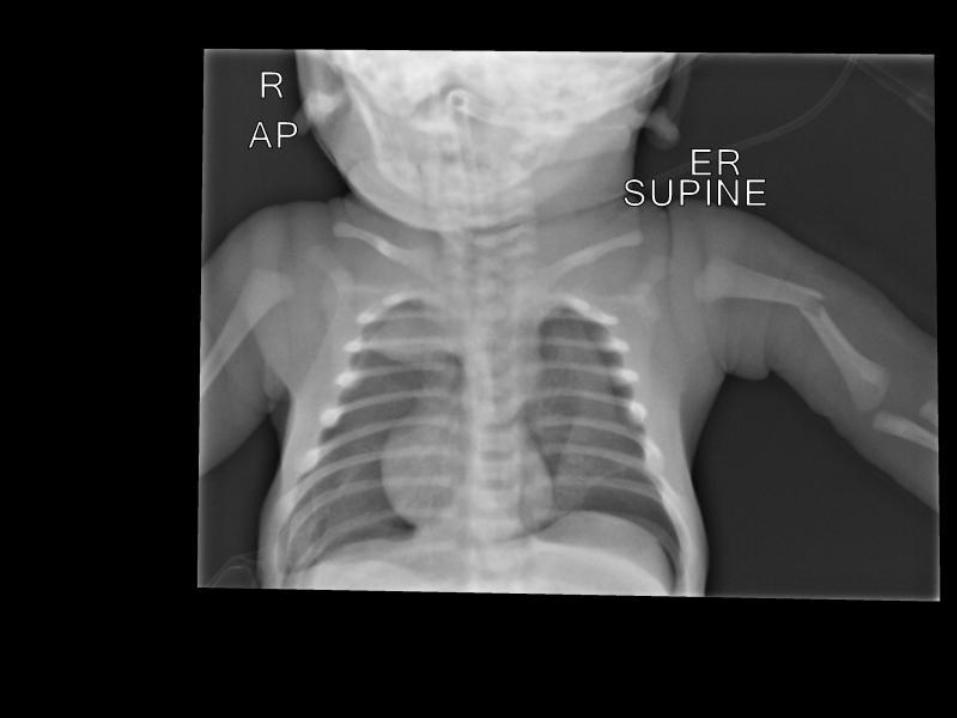
• Newborn -Boy
• Full term - prolonged delivery
• Birth trauma - fracture left humerus • Inflamed umbilicus with pus
• Intubated and ventilated • Arm splinted • Ampicillin and gentamicin
Patient 3
• Blood culture: No growth • Umbilical swab: Coagulase negative Staphylococcus
• Persistent umbilical infection • Change to cloxacillin
Patient 3
• Day 8 • Improving • No fever for 3 days
• Extubated • ET aspirate sent for culture
Patient 3
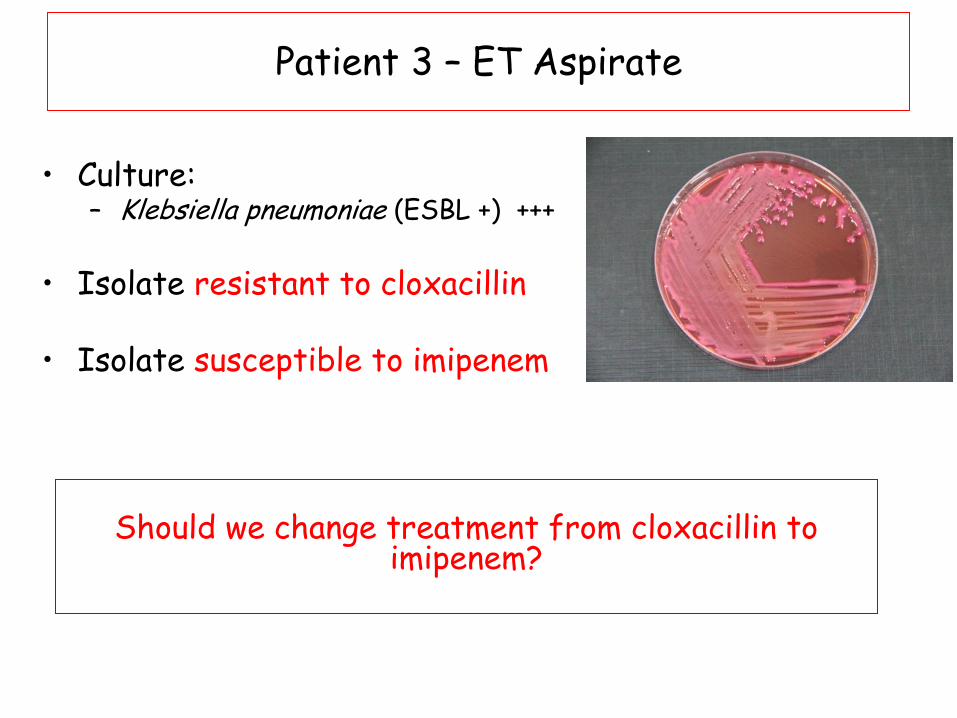
• Culture:
– Klebsiella pneumoniae (ESBL +) +++
• Isolate resistant to cloxacillin
• Isolate susceptible to imipenem
Patient 3 – ET Aspirate
Should we change treatment from cloxacillin to
imipenem?
• Clinically improving • Extubated • No fever • No clinical signs of pneumonia • WCC: 10.8 • CRP: 1.0
• Conclusion: • Oropharyngeal colonisation not infection • No change in treatment
Patient 3
• Remained well until…
• Day 20 • Worse again • Lung crackles and fever
• WCC: 17.0 (Neutrophils 8.4) • CRP: 2.3
Patient 3
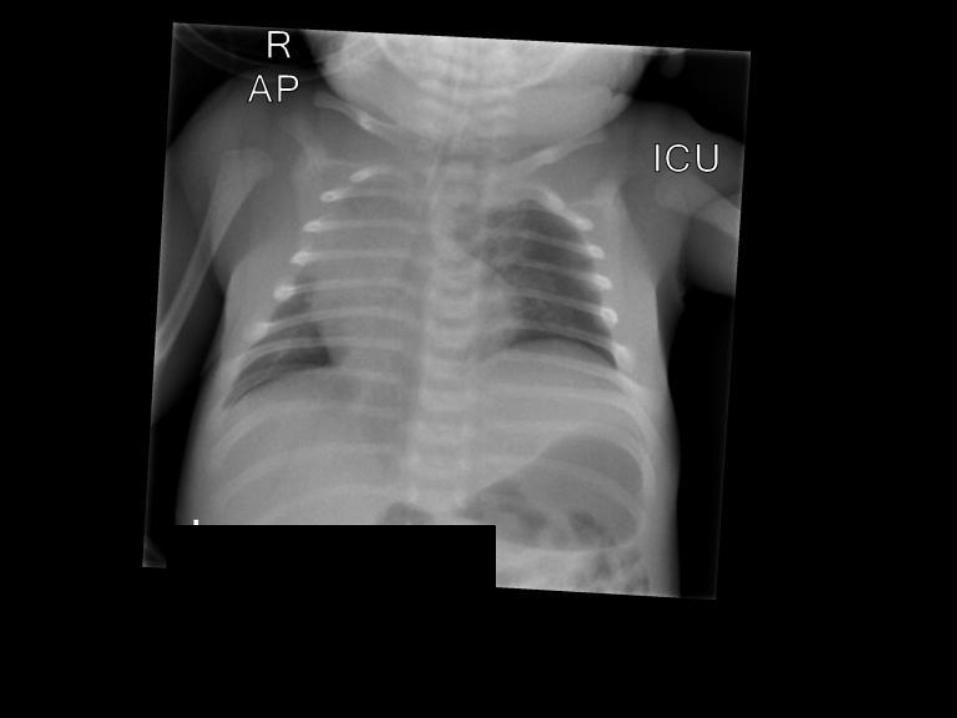
• Clinical diagnosis of pneumonia • CXR new L sided density
• Health care associated
• Empiric treatment?
• Imipenem
Patient 3
• Blood culture and ET Aspirate • Pseudomonas aeruginosa
• Isolates sensitive to imipenem
• Recovered
Patient 3
• Diagnosis of infection is clinical
• The microbiology result does not tell you whether
there is infection
• Particularly with cultures from sites with a normal bacterial flora
How can the microbiology laboratory help you?
• Diagnosis of infection is clinical
• The microbiology result does not tell you whether
there is infection
• Particularly with cultures from sites with a normal bacterial flora
• If there is evidence of clinical infection
• The microbiology result tells you what is the likely infecting pathogen
How can the microbiology laboratory help you?
• Malaria • HIV • Leishmaniasis • Dengue • Hepatitis • Syphilis
Why don’t we use rapid diagnostic tests (RDT)?
• Advantages
• ‘Point of care’ • Kit based • Easy to perform
• Disadvantages
• Expense • User variability • Poor sensitivity and specificity
Why don’t we use rapid diagnostic tests (RDT)?
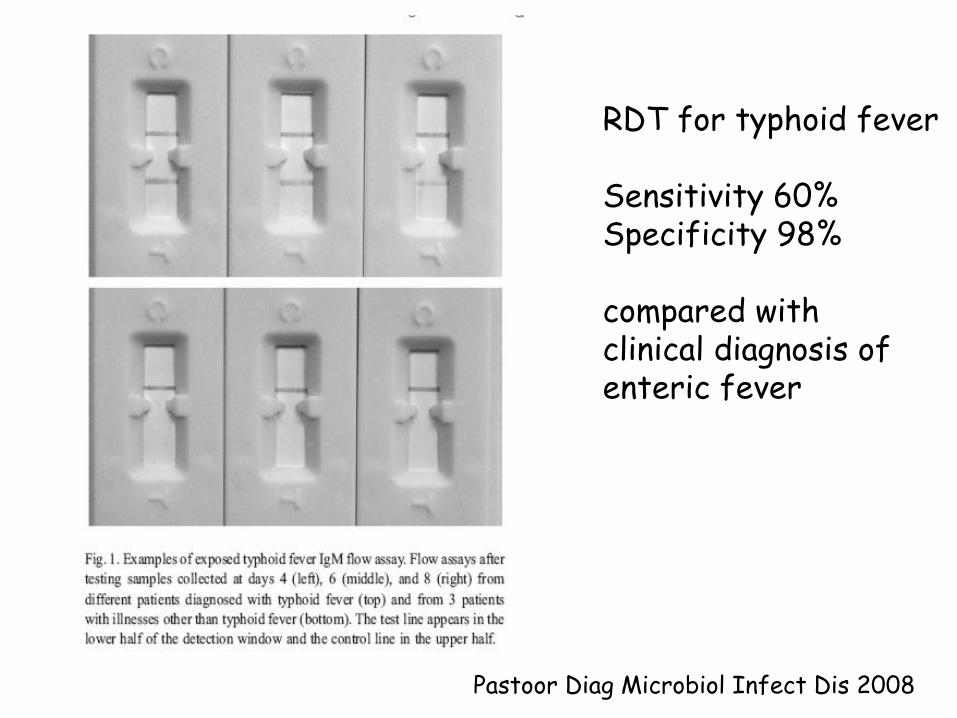
Pastoor Diag Microbiol Infect Dis 2008
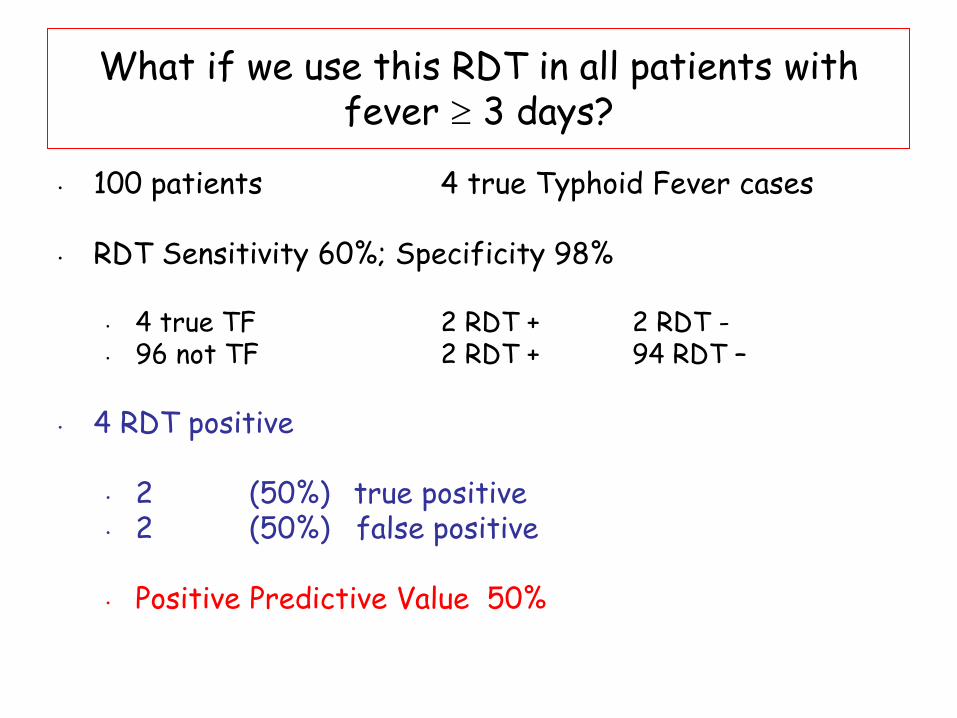
RDT for typhoid fever Sensitivity 60% Specificity 98% compared with clinical diagnosis of enteric fever
What if we use this RDT in all patients with fever 3 days?
• 100 patients 4 true Typhoid Fever cases
• RDT Sensitivity 60%; Specificity 98%
• 4 true TF 2 RDT + 2 RDT - • 96 not TF 2 RDT + 94 RDT –
What if we use this RDT in all patients with fever 3 days?
• 100 patients 4 true Typhoid Fever cases
• RDT Sensitivity 60%; Specificity 98%
• 4 true TF 2 RDT + 2 RDT - • 96 not TF 2 RDT + 94 RDT –
• 4 RDT positive
• 2 (50%) true positive • 2 (50%) false positive
• Positive Predictive Value 50%
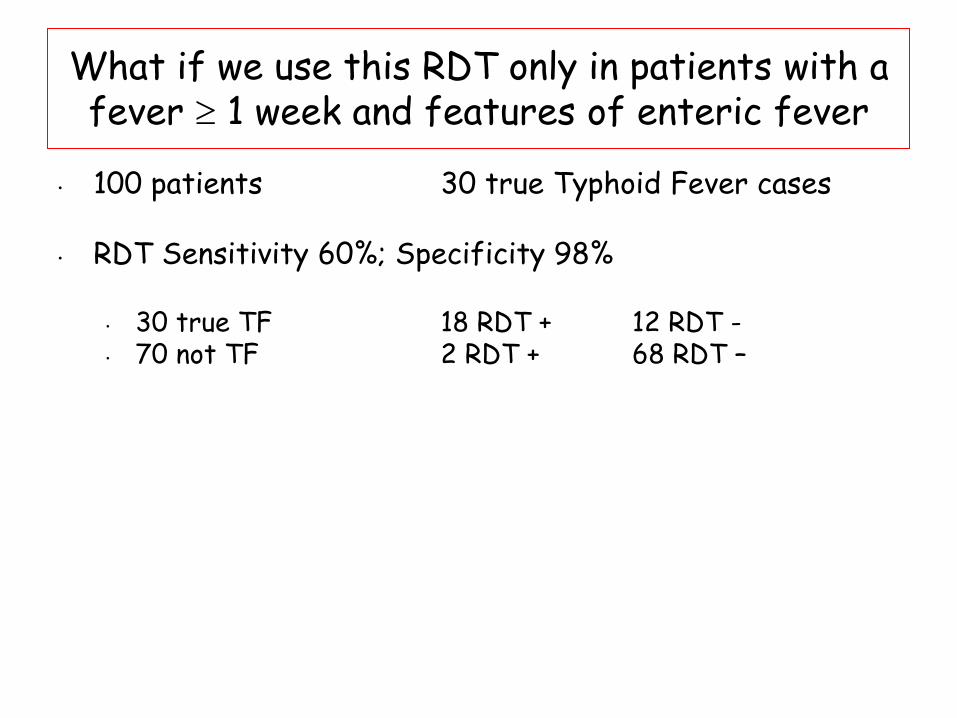
What if we use this RDT only in patients with a fever 1 week and features of enteric fever
• 100 patients 30 true Typhoid Fever cases
• RDT Sensitivity 60%; Specificity 98%
• 30 true TF 18 RDT + 12 RDT - • 70 not TF 2 RDT + 68 RDT –
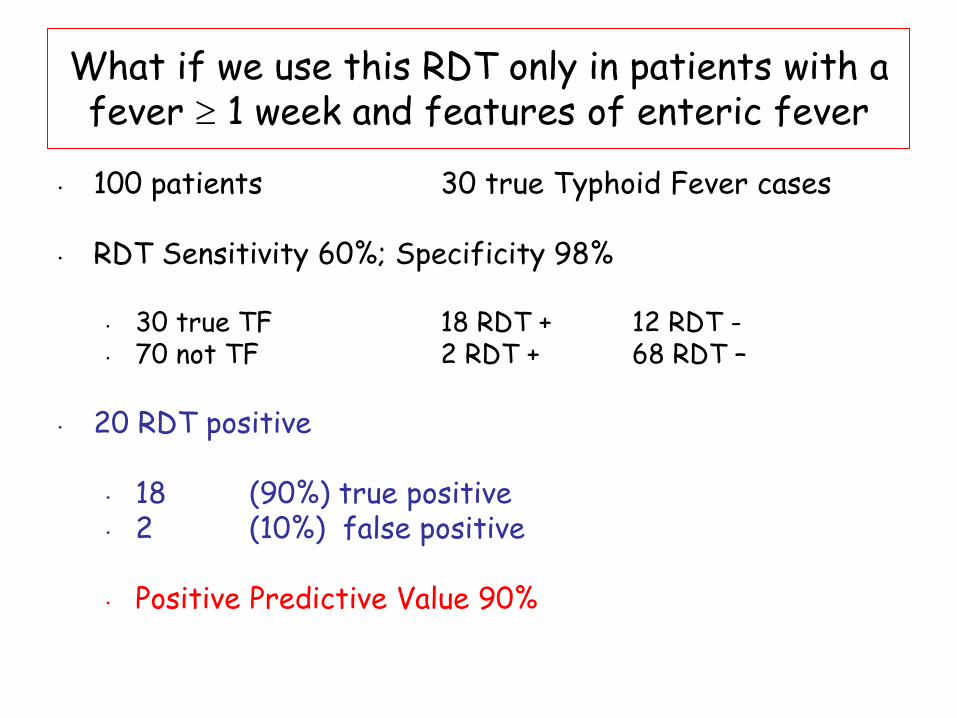
What if we use this RDT only in patients with a fever 1 week and features of enteric fever
• 100 patients 30 true Typhoid Fever cases
• RDT Sensitivity 60%; Specificity 98%
• 30 true TF 18 RDT + 12 RDT - • 70 not TF 2 RDT + 68 RDT –
• 20 RDT positive
• 18 (90%) true positive • 2 (10%) false positive
• Positive Predictive Value 90%
Molecular methods
GeneXpert MTB/Rif Cost
Easy Quick Sensitive Specific
Laboratory network
Level 1 – Peripheral Malaria and TB microscopy. HIV testing
Level 2 – District Microscopy, biochemistry, serology, blood transfusion
Level 3 – Regional Culture of blood, CSF, faeces, TB. Molecular tests for influenza
Level 4 – Central TB culture and DST. Centres for QA of malaria and HIV tests.
Viral culture laboratories (Polio network)
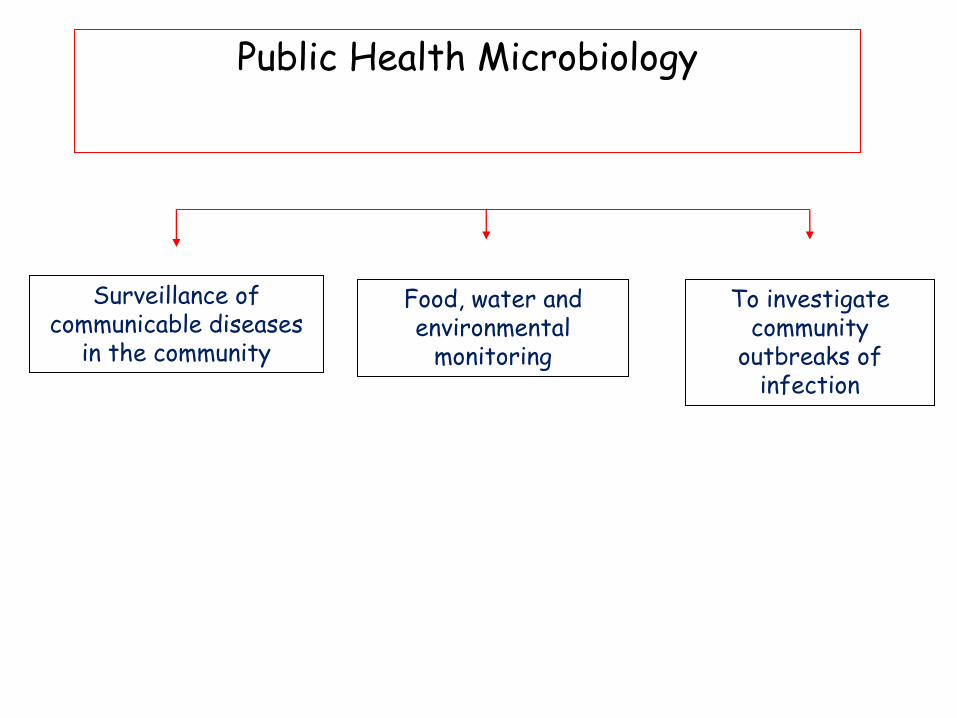
Public Health Microbiology
To investigate community
outbreaks of infection
Food, water and environmental
monitoring
Surveillance of communicable diseases
in the community
Surveillance of new and emerging pathogens
Avian influenza Nipah virus MDR and XDR TB NDM carbapenameses in Enterobacteriacae
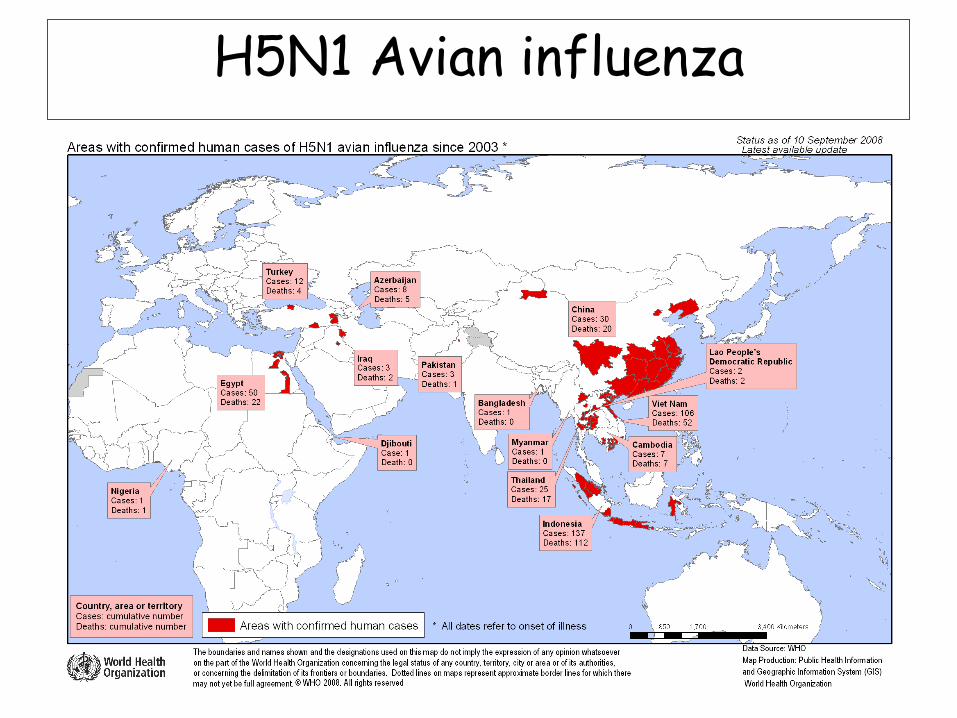
H5N1 Avian influenza
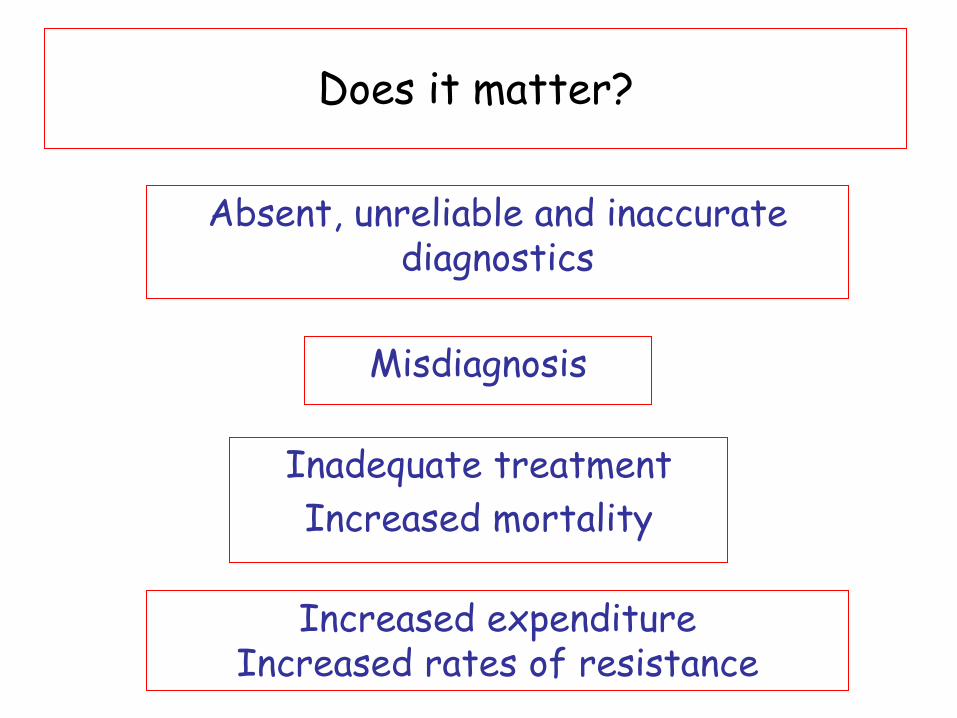
Misdiagnosis
Inadequate treatment
Increased mortality
Increased expenditure Increased rates of resistance
Absent, unreliable and inaccurate diagnostics
Does it matter?
Learning points
• Microbiology can be helpful for clinicians
– For individual patient management
– To provide local epidemiological data
– Inform antimicrobial guidelines
Learning points
• Careful clinical interpretation of results
– Isolates from sterile sites
– Isolates from sites with a normal flora
– Serology result interpretation
– Be aware of the limitations of microbiology
Learning points
• Public health microbiology
• Important function distinct from routine diagnostic microbiology
• Linked to disease epidemiology and surveillance
Learning points
• Countries need a laboratory network
• Trained staff
• Relevant panel of standardised investigations at each level
• Quality Assurance of results !!
• Public - private collaboration ?
Thank you
![WELCOME [bsmedicine.org]bsmedicine.org/congress/2017/Prof._Dr._Prabir_Mohan... · 2018-12-15 · Non-alcoholic fatty liver disease (NAFLD) and metabolic syndrome have become a public](https://img.pdfslide.us/doc/110x75/5f21c1c950d8652777135131/welcome-2018-12-15-non-alcoholic-fatty-liver-disease-nafld-and-metabolic.jpg)