Embed Size (px)
Citation preview

Vol. 115 No. 3 March 2013
Rare diagnosis of IgG4-related systemic disease by lip biopsy in aninternational Sjögren syndrome registryAlan N. Baer, MD,a Christine G. Gourin, MD,b William H. Westra, MD,c Darren P. Cox, DDS, MBA,d
John S. Greenspan, BDS, PhD,e and Troy E. Daniels, DDS, MS,e for the Sjögren’s International CollaborativeAlliance, Baltimore, Maryland; and San Francisco, CaliforniaJohns Hopkins University School of Medicine, University of the Pacific, and University of California, San Francisco
IgG4-related disease has been recently defined as a distinct clinic-pathologic entity, characterized by dense IgG-4plasmacytic infiltration of diverse organs, fibrosis, and tumefactive lesions. Salivary and lacrimal glands are a target of thisdisease and, when affected, may clinically resemble Küttner tumor, Mikulicz disease, or orbital inflammatory pseudotumor. Insome patients, the disease is systemic, with metachronous involvement of multiple organs, including the pancreas, aorta,kidneys, and biliary tract. We report a 66-year-old man who presented with salivary gland enlargement and severe salivaryhypofunction and was diagnosed with IgG4-related disease on the basis of a labial salivary gland biopsy. Additional featuresof his illness included a marked peripheral eosinophilia, obstructive pulmonary disease, and lymphoplasmacytic aortitis. Hewas evaluated in the context of a research registry for Sjögren syndrome and was the only 1 of 2594 registrants with minorsalivary gland histopathologic findings supportive of this diagnosis. (Oral Surg Oral Med Oral Pathol Oral Radiol 2013;115:
e34-e39)Chronic bilateral enlargement of the lacrimal and/orsalivary glands can have an inflammatory, infectious, orneoplastic etiology. In 1892, Mikulicz provided a de-tailed description of the acinar atrophy and massivesmall cell infiltration of the glandular interstitium in aman with this clinical presentation.1 “Mikulicz syn-drome” was subsequently found to have a variety ofetiologies, including lymphoma, Sjögren syndrome(SS), and the newly described group of immunoglobu-lin (Ig)G4-related diseases.2-4 In SS, persistent swellingof the salivary glands occurs in a minority of patientsand raises concern for lymphomatous transformation.5
Within the past decade, IgG4 plasmacytic infiltrationhas been recognized as a pathologic feature of severalforms of salivary and lacrimal gland disease, includingchronic sclerosing sialadenitis (Küttner tumor), orbitalinflammatory pseudotumor, and “Mikulicz disease.”6-8
Supported by contract N01-DE-32636 from the National Institutes ofHealth, Bethesda, MD.The authors report no relevant conflicts of interest.aAssociate Professor, Department of Medicine (Rheumatology),Johns Hopkins University School of Medicine.bAssociate Professor, Department of Otolaryngology and Head andNeck Surgery, Johns Hopkins University School of Medicine.cAssociate Professor, Departments of Pathology and Otolaryngologyand Head and Neck Surgery, Johns Hopkins University School ofMedicine.dAssistant Professor, Department of Pathology, University of thePacific School of Dentistry.eProfessor, Departments of Orofacial Sciences and Pathology,Schools of Dentistry and Medicine, University of California.© 2013 Elsevier Inc. All rights reserved.2212-4403/$ - see front matter
http://dx.doi.org/10.1016/j.oooo.2012.07.485e34
Patients with these forms of IgG4-related plasmacyticsalivary and lacrimal gland disease may have systemicdisease (known variably as IgG4-related systemic dis-ease, IgG4-related sclerosing disease, and IgG4-posi-tive multiorgan lymphoproliferative syndrome), mani-fested by contemporaneous or past involvement ofother organs with a pathologic process marked by IgG4plasmacytic infiltration, extensive fibrosis, and obliter-ative phlebitis.9-11 Elevated serum IgG4 levels and eo-sinophilia are often present. The most common is scle-rosing pancreatitis; others include lymphoplasmacyticaortitis, retroperitoneal fibrosis, sclerosing cholangitis,and inflammatory pseudotumors of the lung, breast, orliver.
Kitagawa et al.6 were the first to identify IgG4-plasmacytic infiltration as a pathologic feature ofchronic sclerosing sialadenitis (Küttner tumor), a tu-morlike condition affecting most often the submandib-ular glands. Their study was based on a retrospectivereview of pathologic material. Following their report in2005, other Japanese investigators reported patientswith severe and persistent swelling of the lacrimal andsalivary glands in whom IgG4 plasmacytic infiltrationof the affected glands and/or elevation of serum IgG4levels was present.12,13 In some of these patients, thediagnosis was established or supported by minor labialsalivary gland biopsy.6,14-16 These patients were differ-ent from those affected by SS, having a more equalgender ratio, normal sialography, and excellent re-sponse to corticosteroids.16,17 Reports of IgG4-relatedsialadenitis are rare in the United States, although arecent retrospective case series from the Massachusetts
General Hospital has confirmed the frequent presence
OOOO CASE REPORTVolume 115, Number 3 Baer et al. e35
of IgG4 plasmacytic infiltration in cases of Küttnertumor.18
We report herein a patient with IgG4-related systemicdisease who presented with salivary gland swelling andsevere xerostomia. His diagnosis was established withinthe context of the Sjögren’s International CollaborativeClinical Alliance (SICCA) research registry.19
MATERIAL AND METHODSSICCA is an ongoing longitudinal multisite observa-tional study that is developing and studying a large andgrowing cohort of uniformly evaluated individualsfrom ethnically diverse populations.19 Enrollment cri-teria are broad to create a cohort reflecting a wide rangeof symptoms and signs, from possible early SS towell-established disease. SICCA participants must be atleast 21 years of age and have at least one of thefollowing: a complaint of dry eyes or dry mouth; aprevious diagnosis of SS; elevated titers of antinuclearantibodies (ANA), rheumatoid factor, and/or anti-SS-Aor SS–B antibodies; bilateral parotid enlargement; arecent increase in dental caries; or a possible diagnosisof secondary SS. Enrollment began in fall 2004 at 6international SICCA Research Groups that recruit, en-roll, and examine participants, and collect and shipbiospecimens to the central repository in San Francisco,CA. The groups are located at University of BuenosAires and German Hospitals, Buenos Aires, Argentina;Peking Union Medical College Hospital, Beijing, Chi-na; Copenhagen University Hospital, Glostrup, Den-mark; Kanazawa Medical University, Japan; King’sCollege London, UK (added in 2007); and Universityof California, San Francisco, CA. In 2009, additionalresearch groups were established at the Johns HopkinsUniversity and the University of Pennsylvania, and inAravind, India.
All SICCA groups use the same protocol-directedmethods to provide uniform evaluations; data recordsfrom ocular, oral, and rheumatologic examinations; andbiospecimen collections. Labial salivary gland biopsysamples are obtained at the time of the SICCA baselineevaluation on all participants, or a previous biopsyspecimen is accepted if it was obtained no more than 3years previously and the microscopic slides are avail-able for examination. Labial salivary gland biopsies areperformed, after local anesthetic infiltration, to harvest5 to 10 glands, some of which are fixed in neutralbuffered formalin whereas others are quickly frozen inliquid nitrogen. Three to 5 formalin-fixed labial sali-vary glands are processed by the local pathology de-partments (paraffin embedding, sectioning, and hema-toxylin and eosin [H&E] staining) and remainingglands are frozen and stored in liquid nitrogen. H&E-
stained sections of each specimen are evaluated inde-pendently by 2 of 3 pathologists calibrated in thisassessment (T.E.D., D.C., and J.G.), who are blindedwith regard to the participants’ demographic, clinical,and serologic characteristics and who assign 1 of 6possible diagnoses: focal lymphocytic sialadenitis, non-specific chronic sialadenitis, sclerosing chronic sialad-enitis, granulomatous inflammation, marginal-zone(mucosa-associated lymphoid tissue [MALT]) lym-phoma, or within normal limits.20
Informed consent was obtained from all participantsin the SICCA research registry in compliance with theHelsinki Declaration, and the study was approved bythe University of California, San Francisco, Committeeon Human Research; the Johns Hopkins UniversitySchool of Medicine Institutional Review Board; and thelocal institutional review boards at the other participat-ing institutions.
CASE REPORTA 66-year-old man presented with a 6-month history of
parotid and submandibular gland enlargement, severe xero-stomia, dry eyes, 25-pound weight loss, and night sweats. Hiscurrent illness began 9 months earlier with 2 episodes ofpneumonia, followed by a productive cough and dyspnea. Oncomputed tomography (CT) imaging, there was enlargementof the left parotid and right submandibular glands (Fig. 1). Aneedle biopsy of the left parotid gland 1 month earlier hadshown a polymorphous lymphocytic infiltrate, but no evi-dence of neoplasm. On his initial evaluation at our institution,he had diffuse enlargement and induration of his parotid (left
Fig. 1. CT scan of the neck. There is enlargement of the leftparotid gland relative to the right, without a discrete mass orsurrounding soft tissue stranding.
greater than right) and submandibular glands. The oral cavity
lasma
ORAL MEDICINE OOOOe36 Baer et al. March 2013
was dry and minimal saliva could be expressed throughWharton or Stensen ducts. There was no palpable lymphade-nopathy. He underwent an evaluation for possible SS as aparticipant of SICCA. On an unanesthetized Schirmer test,there was 5 mm of wetting over 5 minutes in both eyes.Ocular surface staining with lissamine green and fluoresceinwas abnormal, with scores of 8 in both eyes, using a quanti-tative scoring method devised by the SICCA investigators.21
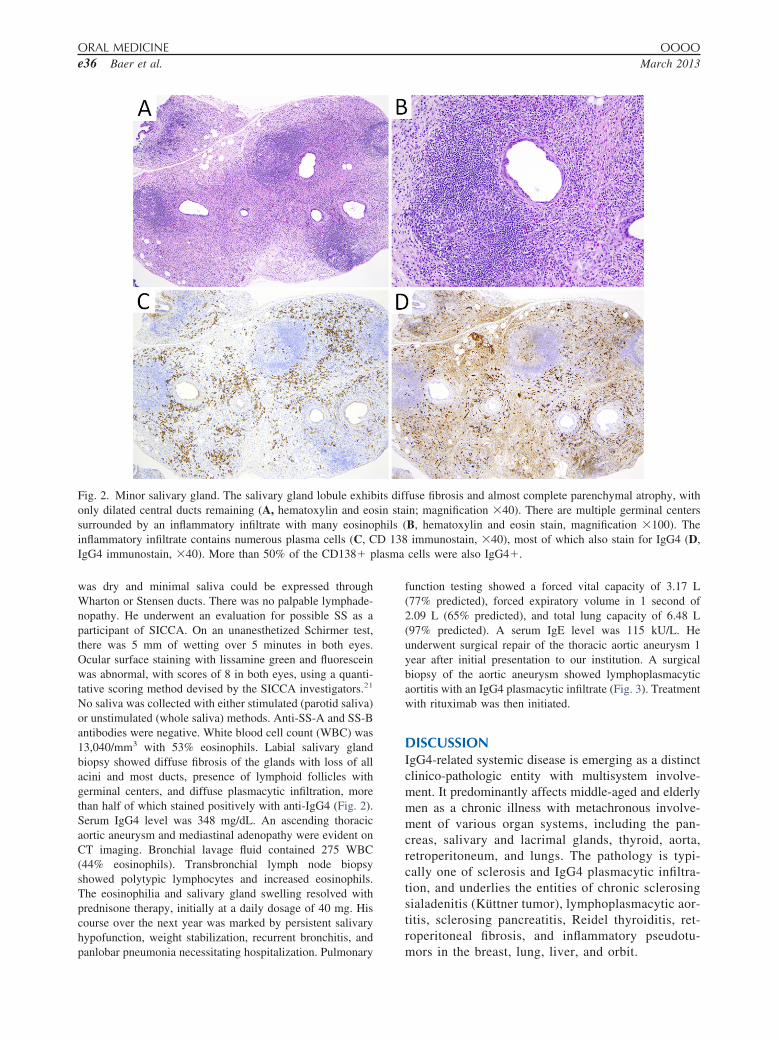
No saliva was collected with either stimulated (parotid saliva)or unstimulated (whole saliva) methods. Anti-SS-A and SS-Bantibodies were negative. White blood cell count (WBC) was13,040/mm3 with 53% eosinophils. Labial salivary glandbiopsy showed diffuse fibrosis of the glands with loss of allacini and most ducts, presence of lymphoid follicles withgerminal centers, and diffuse plasmacytic infiltration, morethan half of which stained positively with anti-IgG4 (Fig. 2).Serum IgG4 level was 348 mg/dL. An ascending thoracicaortic aneurysm and mediastinal adenopathy were evident onCT imaging. Bronchial lavage fluid contained 275 WBC(44% eosinophils). Transbronchial lymph node biopsyshowed polytypic lymphocytes and increased eosinophils.The eosinophilia and salivary gland swelling resolved withprednisone therapy, initially at a daily dosage of 40 mg. Hiscourse over the next year was marked by persistent salivaryhypofunction, weight stabilization, recurrent bronchitis, and
Fig. 2. Minor salivary gland. The salivary gland lobule exhibonly dilated central ducts remaining (A, hematoxylin and eosurrounded by an inflammatory infiltrate with many eosinoinflammatory infiltrate contains numerous plasma cells (C, CIgG4 immunostain, �40). More than 50% of the CD138� p
panlobar pneumonia necessitating hospitalization. Pulmonary
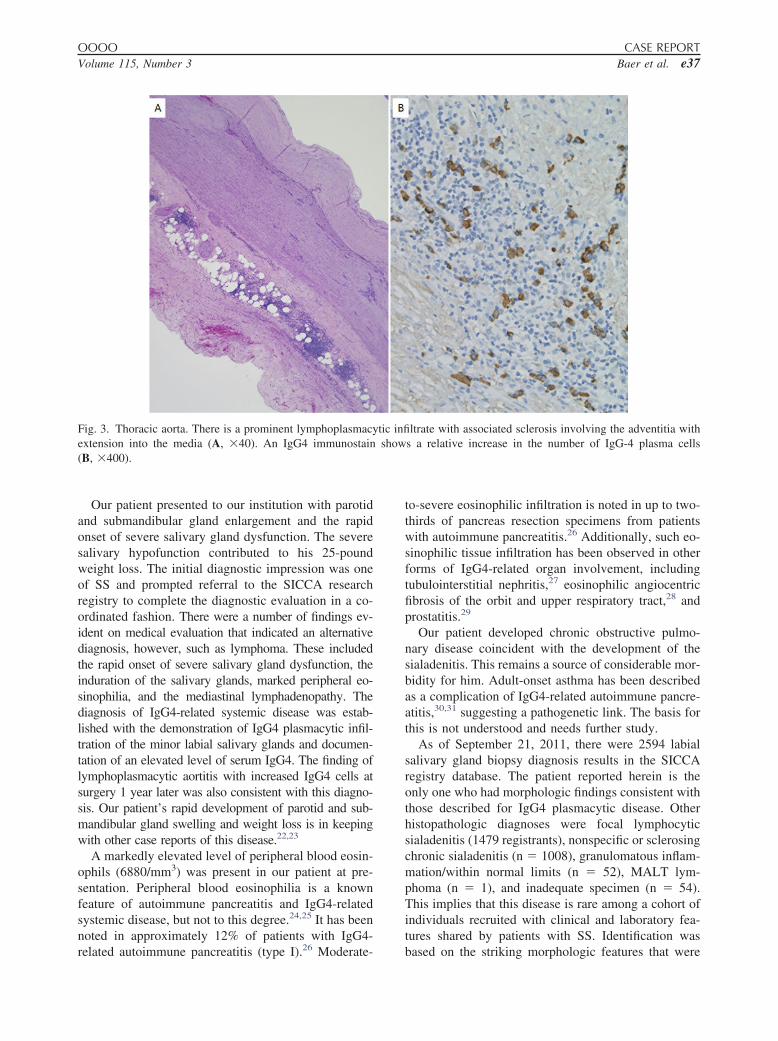
function testing showed a forced vital capacity of 3.17 L(77% predicted), forced expiratory volume in 1 second of2.09 L (65% predicted), and total lung capacity of 6.48 L(97% predicted). A serum IgE level was 115 kU/L. Heunderwent surgical repair of the thoracic aortic aneurysm 1year after initial presentation to our institution. A surgicalbiopsy of the aortic aneurysm showed lymphoplasmacyticaortitis with an IgG4 plasmacytic infiltrate (Fig. 3). Treatmentwith rituximab was then initiated.
DISCUSSIONIgG4-related systemic disease is emerging as a distinctclinico-pathologic entity with multisystem involve-ment. It predominantly affects middle-aged and elderlymen as a chronic illness with metachronous involve-ment of various organ systems, including the pan-creas, salivary and lacrimal glands, thyroid, aorta,retroperitoneum, and lungs. The pathology is typi-cally one of sclerosis and IgG4 plasmacytic infiltra-tion, and underlies the entities of chronic sclerosingsialadenitis (Küttner tumor), lymphoplasmacytic aor-titis, sclerosing pancreatitis, Reidel thyroiditis, ret-roperitoneal fibrosis, and inflammatory pseudotu-
fuse fibrosis and almost complete parenchymal atrophy, within; magnification �40). There are multiple germinal centersB, hematoxylin and eosin stain, magnification �100). Theimmunostain, �40), most of which also stain for IgG4 (D,
cells were also IgG4�.
its difsin staphils (D 138
mors in the breast, lung, liver, and orbit.
OOOO CASE REPORTVolume 115, Number 3 Baer et al. e37
Our patient presented to our institution with parotidand submandibular gland enlargement and the rapidonset of severe salivary gland dysfunction. The severesalivary hypofunction contributed to his 25-poundweight loss. The initial diagnostic impression was oneof SS and prompted referral to the SICCA researchregistry to complete the diagnostic evaluation in a co-ordinated fashion. There were a number of findings ev-ident on medical evaluation that indicated an alternativediagnosis, however, such as lymphoma. These includedthe rapid onset of severe salivary gland dysfunction, theinduration of the salivary glands, marked peripheral eo-sinophilia, and the mediastinal lymphadenopathy. Thediagnosis of IgG4-related systemic disease was estab-lished with the demonstration of IgG4 plasmacytic infil-tration of the minor labial salivary glands and documen-tation of an elevated level of serum IgG4. The finding oflymphoplasmacytic aortitis with increased IgG4 cells atsurgery 1 year later was also consistent with this diagno-sis. Our patient’s rapid development of parotid and sub-mandibular gland swelling and weight loss is in keepingwith other case reports of this disease.22,23
A markedly elevated level of peripheral blood eosin-ophils (6880/mm3) was present in our patient at pre-sentation. Peripheral blood eosinophilia is a knownfeature of autoimmune pancreatitis and IgG4-relatedsystemic disease, but not to this degree.24,25 It has beennoted in approximately 12% of patients with IgG4-
Fig. 3. Thoracic aorta. There is a prominent lymphoplasmacextension into the media (A, �40). An IgG4 immunostain(B, �400).
related autoimmune pancreatitis (type I).26 Moderate-
to-severe eosinophilic infiltration is noted in up to two-thirds of pancreas resection specimens from patientswith autoimmune pancreatitis.26 Additionally, such eo-sinophilic tissue infiltration has been observed in otherforms of IgG4-related organ involvement, includingtubulointerstitial nephritis,27 eosinophilic angiocentricfibrosis of the orbit and upper respiratory tract,28 andprostatitis.29
Our patient developed chronic obstructive pulmo-nary disease coincident with the development of thesialadenitis. This remains a source of considerable mor-bidity for him. Adult-onset asthma has been describedas a complication of IgG4-related autoimmune pancre-atitis,30,31 suggesting a pathogenetic link. The basis forthis is not understood and needs further study.
As of September 21, 2011, there were 2594 labialsalivary gland biopsy diagnosis results in the SICCAregistry database. The patient reported herein is theonly one who had morphologic findings consistent withthose described for IgG4 plasmacytic disease. Otherhistopathologic diagnoses were focal lymphocyticsialadenitis (1479 registrants), nonspecific or sclerosingchronic sialadenitis (n � 1008), granulomatous inflam-mation/within normal limits (n � 52), MALT lym-phoma (n � 1), and inadequate specimen (n � 54).This implies that this disease is rare among a cohort ofindividuals recruited with clinical and laboratory fea-tures shared by patients with SS. Identification was
ltrate with associated sclerosis involving the adventitia withs a relative increase in the number of IgG-4 plasma cells
ytic infishow
based on the striking morphologic features that were

ORAL MEDICINE OOOOe38 Baer et al. March 2013
distinct from other histopathologic patterns of sialad-enitis. These findings include the complete fibrosis ofthe salivary glands with total loss of acini in concertwith a lymphoplasmacytic infiltrate. IgG4-relatedsialadenitis must be distinguished from sclerosingchronic sialadenitis. In the latter, involvement is oftennot uniform from gland to gland in the specimen (sug-gesting ductal obstruction as a potential etiology) andductal dilatation is a prominent feature. The fibrosis ofIgG4-related sialadenitis is characterized by highly cel-lular proliferation with plump fibroblasts admixed withinflammatory cells as opposed to the more extensivecollagenous deposition seen in sclerosing chronicsialadenitis. It is not known whether this differencereflects the relative chronicity of the disease processesbefore the diagnostic biopsies are performed. Immuno-histochemical staining for IgG4-positive plasma cellswas not performed as a part of the routine histopatho-logic assessment of labial salivary glands in the SICCAstudy. Thus, we cannot exclude the possibility thatearlier or less severe forms of IgG4-related sialadenitismight have been overlooked with the routine histologictechniques used in the SICCA study.
In summary, IgG4-related sialadenitis is a rare entitydespite a number of recent case series of IgG4-relatedsialadenitis from Japan. Its recognition is important,however, because it may be associated with clinicallyimportant lesions of other organs, such as lymphoplas-macytic aortitis. Our case highlights the utility of the lipbiopsy in establishing the diagnosis of diverse systemicdiseases with oral manifestations, including IgG4-re-lated systemic disease.
REFERENCES1. Mikulicz J. Uber eine eigenartige symmetrische Ekrankung der
Thränen-und Mundspeicheldrüsen. Beitr Chir 1892; festschriftfür Billroth:610-630.
2. Schaffer AJ, Jacobsen AW. Mikulicz’s syndrome: a report of tencases. Am J Dis Child 1927;34:327-46.
3. Stone JH, Zen Y, Deshpande V. IgG4-related disease. N EnglJ Med 2012;366:539-51.
4. Ihrler S, Harrison JD. Mikulicz’s disease and Mikulicz’s syn-drome: analysis of the original case report of 1892 in the light ofcurrent knowledge identifies a MALT lymphoma. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2005;100:334-9.
5. Anaya JM, McGuff HS, Banks PM, Talal N. Clinicopathologicalfactors relating malignant lymphoma with Sjogren’s syndrome.Semin Arthritis Rheum 1996;25:337-46.
6. Kitagawa S, Zen Y, Harada K, Sasaki M, Sato Y, Minato H, etal. Abundant IgG4-positive plasma cell infiltration characterizeschronic sclerosing sialadenitis (Kuttner’s tumor). Am J SurgPathol 2005;29:783-91.
7. Cheuk W, Yuen HK, Chan JK. Chronic sclerosing dacryoadeni-tis: part of the spectrum of IgG4-related sclerosing disease? Am JSurg Pathol 2007;31:643-5.
8. Yamamoto M, Takahashi H, Ohara M, Suzuki C, Naishiro Y,
Yamamoto H, et al. A new conceptualization for Mikulicz’sdisease as an IgG4-related plasmacytic disease. Mod Rheumatol2006;16:335-40.
9. Stone JH, Khosroshahi A, Hilgenberg A, Spooner A, IsselbacherEM, Stone JR. IgG4-related systemic disease and lymphoplas-macytic aortitis. Arthritis Rheum 2009;60:3139-45.
10. Cheuk W, Chan JK. IgG4-related sclerosing disease: a criticalappraisal of an evolving clinicopathologic entity. Adv AnatPathol 2010;17:303-32.
11. Masaki Y, Dong L, Kurose N, Kitagawa K, Morikawa Y,Yamamoto M, et al. Proposal for a new clinical entity, IgG4-positive multiorgan lymphoproliferative syndrome: analysis of64 cases of IgG4-related disorders. Ann Rheum Dis2009;68:1310-5.
12. Yamamoto M, Harada S, Ohara M, Suzuki C, Naishiro Y,Yamamoto H, et al. Clinical and pathological differences be-tween Mikulicz’s disease and Sjogren’s syndrome. RheumatolOxf Engl 2005;44:227-34.
13. Masaki Y, Sugai S, Umehara H. IgG4-related diseases includingMikulicz’s disease and sclerosing pancreatitis: diagnostic in-sights. J Rheumatol 2010;37:1380-5.
14. Doe K, Hohtatsu K, Lee S, Nozawa K, Amano H, Tamura N,Takasaki Y. [Case report: usefulness of lip biopsy for the diag-nosis of IgG4-related diseases with retroperitoneal fibrosis: re-port of a case.] Nihon Naika Gakkai Zasshi 2011;100:1645-7.Japanese.
15. Nakada H, Shibasaki O, Nakashima M, Yoshinami H, Kase Y.[IgG4-related Mikulicz’s disease: a report of 3 cases.] NihonJibiinkoka Gakkai Kaiho 2010;113:798-804. Japanese.
16. Yamamoto M, Takahashi H, Sugai S, Imai K. Clinical andpathological characteristics of Mikulicz’s disease (IgG4-relatedplasmacytic exocrinopathy). Autoimmun Rev 2005;4:195-200.
17. Takahashi H, Yamamoto M, Suzuki C, Naishiro Y, ShinomuraY, Imai K. The birthday of a new syndrome: IgG4-relateddiseases constitute a clinical entity. Autoimmun Rev2010;9:591-4.
18. Geyer JT, Ferry JA, Harris NL, Stone JH, Zukerberg LR, Lau-wers GY, et al. Chronic sclerosing sialadenitis (Kuttner tumor) isan IgG4-associated disease. Am J Surg Pathol 2010;34:202-10.
19. Daniels TE, Criswell LA, Shiboski C, Shiboski S, Lanfranchi H,Dong Y, et al. Sjogren’s international collaborative clinical alli-ance research groups. An early view of the internationalSjogren’s syndrome registry. Arthritis Rheum 2009;61:711-4.
20. Daniels TE, Cox D, Shiboski CH, Schiødt M, Wu A, LanfranchiH, et al. Sjogren’s International Collaborative Clinical AllianceResearch Groups. Associations between salivary gland histo-pathologic diagnoses and phenotypic features of Sjogren’s syn-drome among 1,726 registry participants. Arthritis Rheum2011;63:2021-30.
21. Whitcher JP, Shiboski CH, Shiboski SC, Heidenreich AM,Kitagawa K, Zhang S, et al. Sjogren’s international collaborativeclinical alliance research groups. A simplified quantitativemethod for assessing keratoconjunctivitis sicca from theSjogren’s syndrome International registry. Am J Ophthalmol2010;149:405-15.
22. Stone JH, Caruso PA, Deshpande V. Case records of the Mas-sachusetts General Hospital. Case 24-2009. A 26-year-oldwoman with painful swelling of the neck. N Engl J Med2009;361:511-8.
23. Abe T, Sato T, Tomaru Y, Sakata Y, Kokabu S, Hori N, et al.Immunoglobulin G4-related sclerosing sialadenitis: report of twocases and review of the literature. Oral Surg Oral Med OralPathol Oral Radiol Endod 2009;108:544-50.
24. Kamisawa T, Anjiki H, Egawa N, Kubota N. Allergic manifes-tations in autoimmune pancreatitis. Eur J Gastroenterol Hepatol
2009;21:1136-9.
OOOO CASE REPORTVolume 115, Number 3 Baer et al. e39
25. Wang Q, Lu CM, Guo T, Qian JM. Eosinophilia associated withchronic pancreatitis. Pancreas 2009;38:149-53.
26. Sah RP, Pannala R, Zhang L, Graham RP, Sugumar A, Chari ST.Eosinophilia and allergic disorders in autoimmune pancreatitis.Am J Gastroenterol 2010;105:2485-91.
27. Cornell LD, Chicano SL, Deshpande V, Collins AB, SeligMK, Lauwers GY, et al. Pseudotumors due to IgG4 immune-complex tubulointerstitial nephritis associated with autoim-mune pancreatocentric disease. Am J Surg Pathol 2007;31:1586-97.
28. Deshpande V, Khosroshahi A, Nielsen GP, Hamilos DL, StoneJH. Eosinophilic angiocentric fibrosis is a form of IgG4-relatedsystemic disease. Am J Surg Pathol 2011;35:701-6.
29. Uehara T, Hamano H, Kawakami M, Koyama M, Kawa S, SanoK, et al. Autoimmune pancreatitis-associated prostatitis: distinct
clinicopathological entity. Pathol Int 2008;58:118-25.30. Roggin KK, Rudloff U, Klimstra DS, Russell LA, Blumgart LH.Adult-onset asthma and periocular xanthogranulomas in a patientwith lymphoplasmacytic sclerosing pancreatitis. Pancreas 2007;34:157-60.
31. Ito S, Ko SB, Morioka M, Imaizumi K, Kondo M, Mizuno N,Hasegawa Y. Three cases of bronchial asthma preceding IgG4-related autoimmune pancreatitis. Allergol Int 2012;61:171-4.
Reprint requests:
Alan N. Baer, MDJohns Hopkins University School of Medicine5200 Eastern AvenueSuite 4000, Mason Lord Building, Center TowerBaltimore, MD 21224
[email protected]




























