Embed Size (px)
Citation preview
IgG4 – Related Disease
Suda Sibunruang, M.D.
Outline
• Introduction
• Historical context
• Pathogenesis
• Epidemiology
• Clinical manifestations and laboratory findings
• Treatment and prognosis
Outline
• Introduction
• Historical context
• Pathogenesis
• Epidemiology
• Clinical manifestations and laboratory findings
• Treatment and prognosis
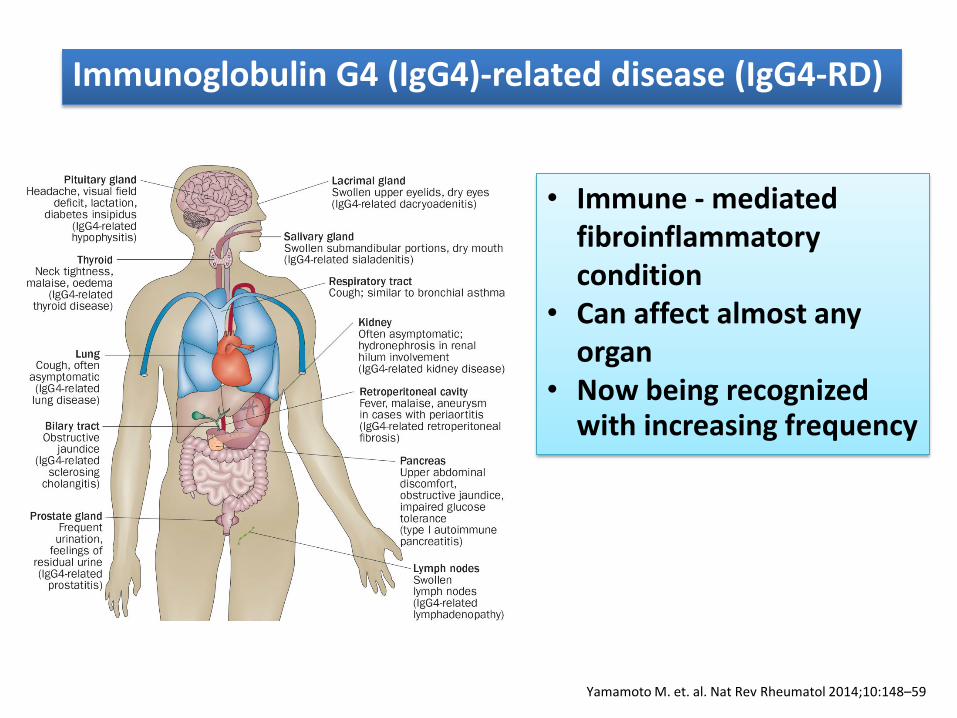
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Immunoglobulin G4 (IgG4)-related disease (IgG4-RD)
• Immune - mediated fibroinflammatory condition
• Can affect almost any organ
• Now being recognized with increasing frequency
www.rheumatologynetwork.com ,access May 25, 2015
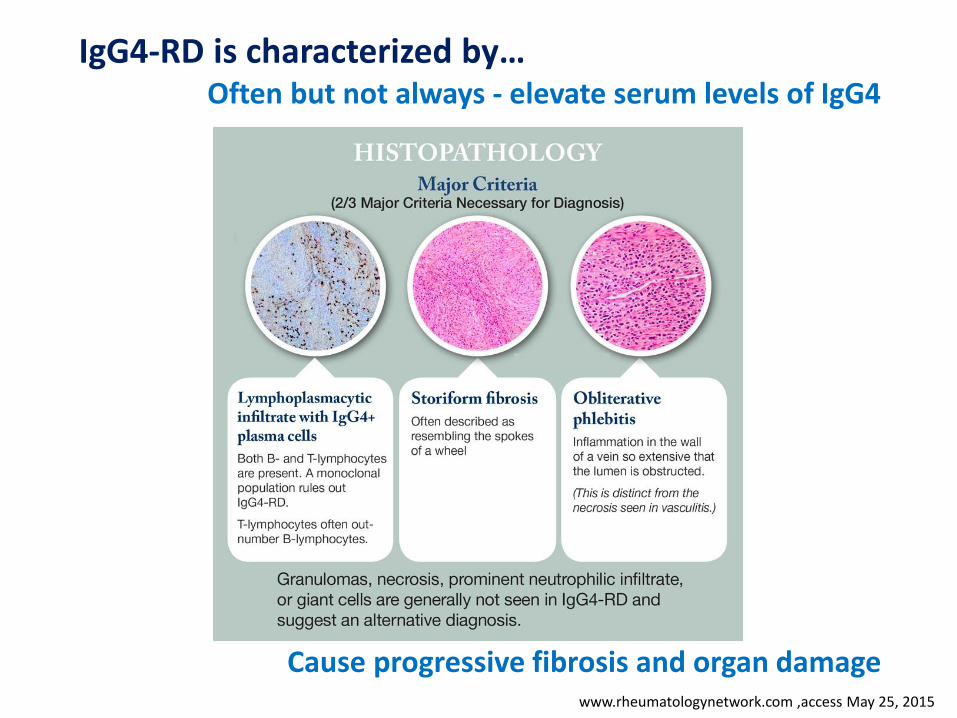
IgG4-RD is characterized by… Often but not always - elevate serum levels of IgG4
Cause progressive fibrosis and organ damage
Picture from www.mbl.co.jp , access May 25, 2015
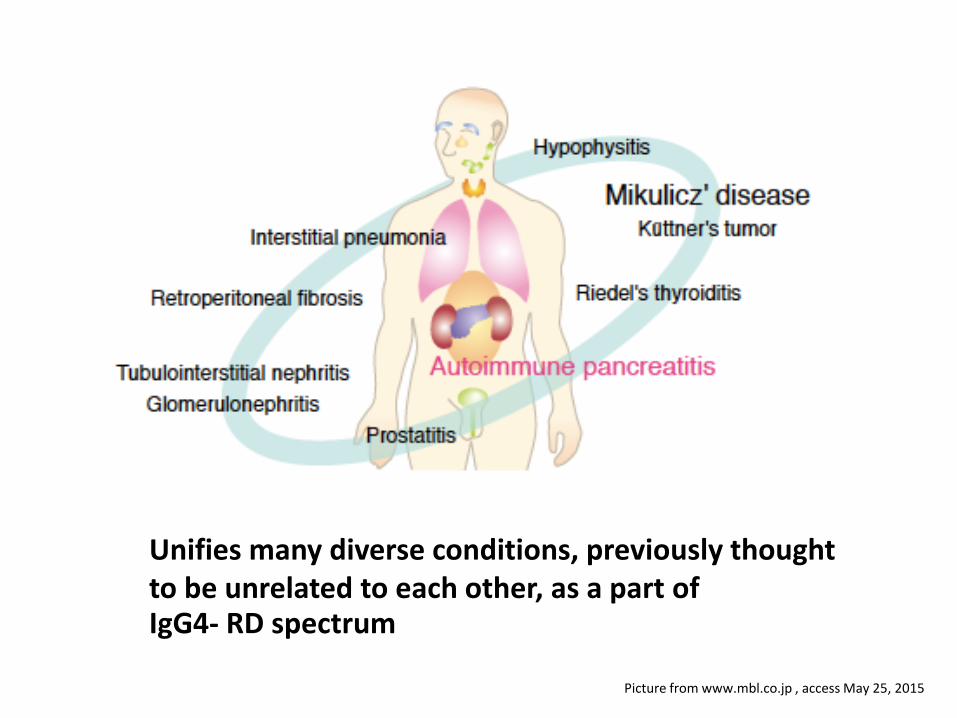
Unifies many diverse conditions, previously thought to be unrelated to each other, as a part of IgG4- RD spectrum
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
• Early intervention using glucocorticoids can improve IgG4-related organ dysfunction • However, patients often relapse when doses of these agents are tapered • Disease has also been associated with an increased incidence of certain malignancies
Outline
• Introduction
• Historical context
• Pathogenesis
• Epidemiology
• Clinical manifestations and laboratory findings
• Treatment and prognosis
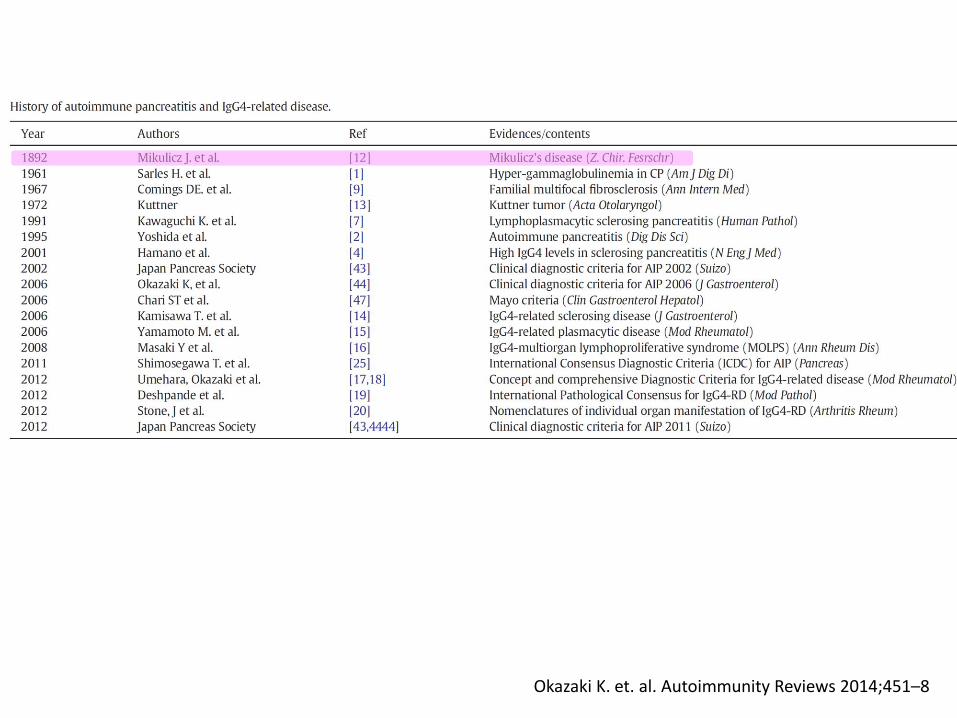
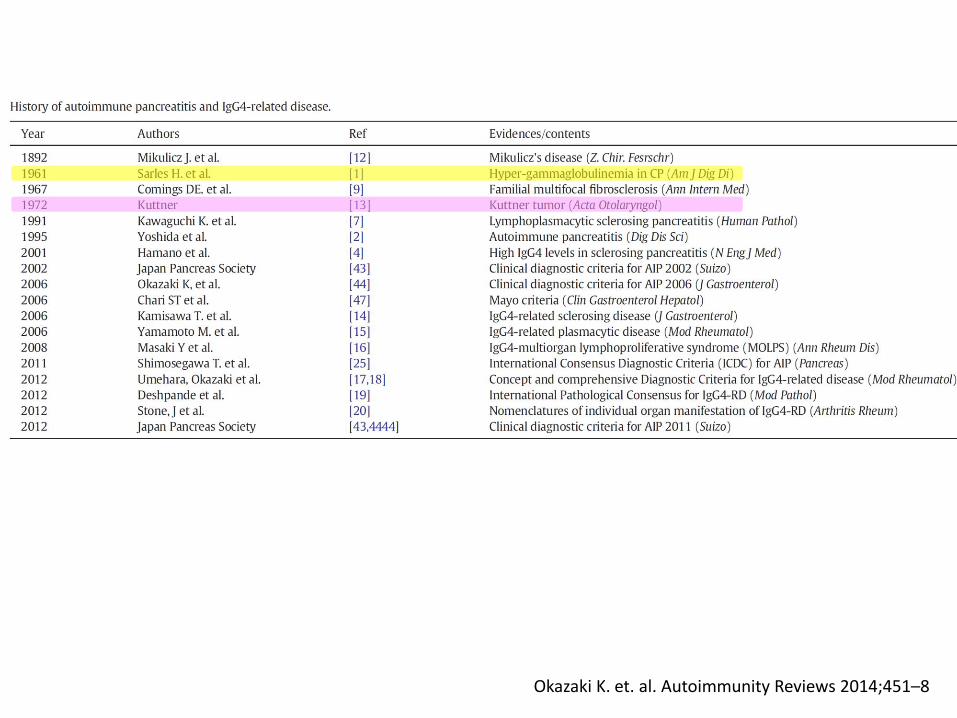
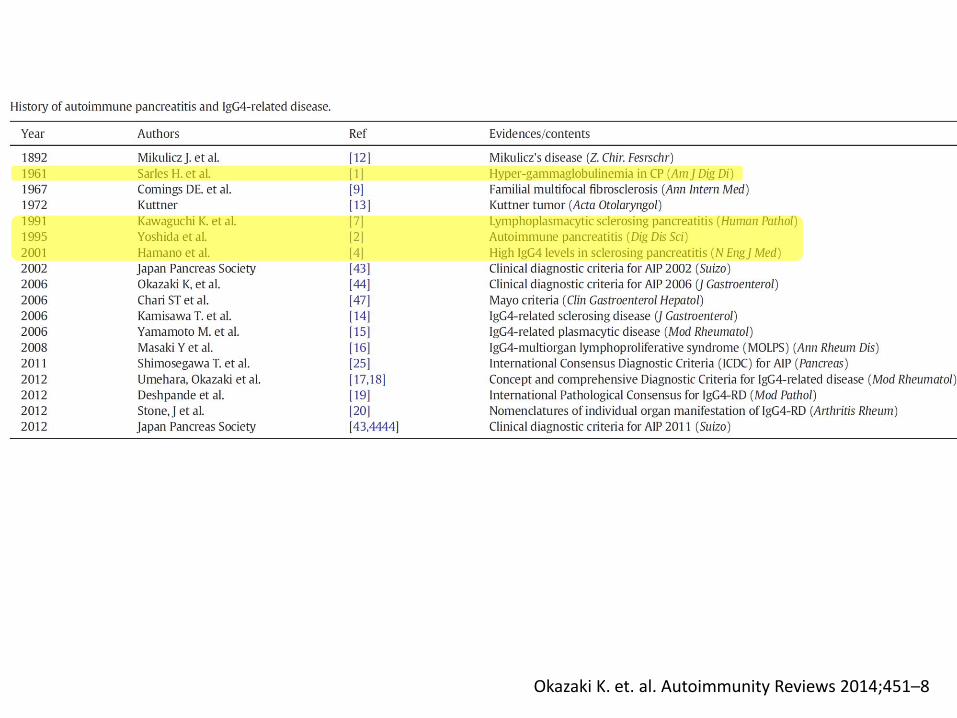
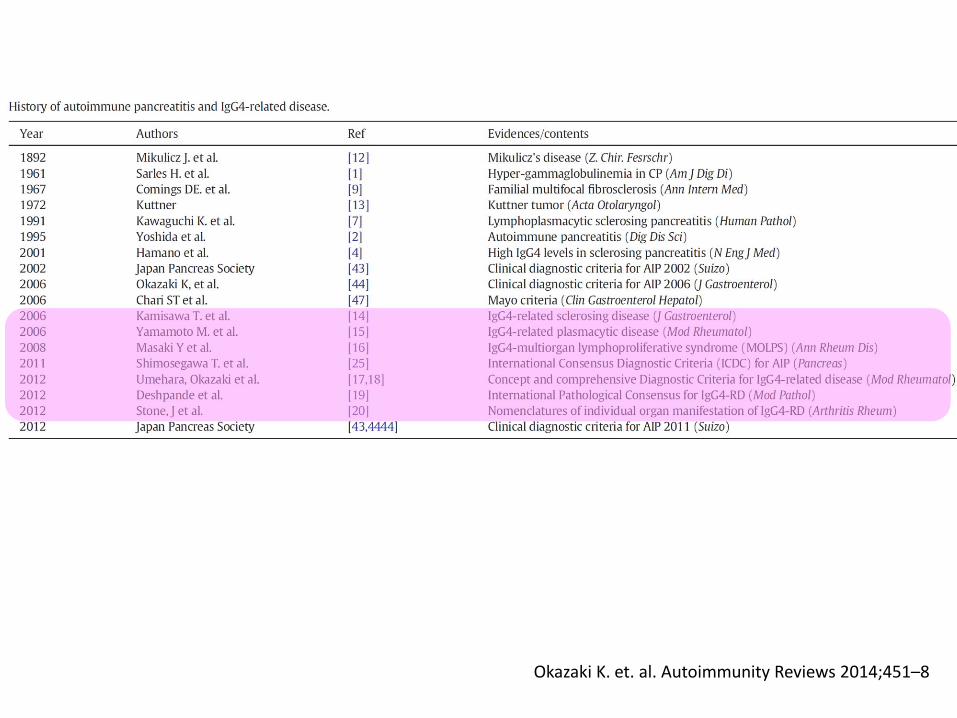
Okazaki K. et. al. Autoimmunity Reviews 2014;451–8
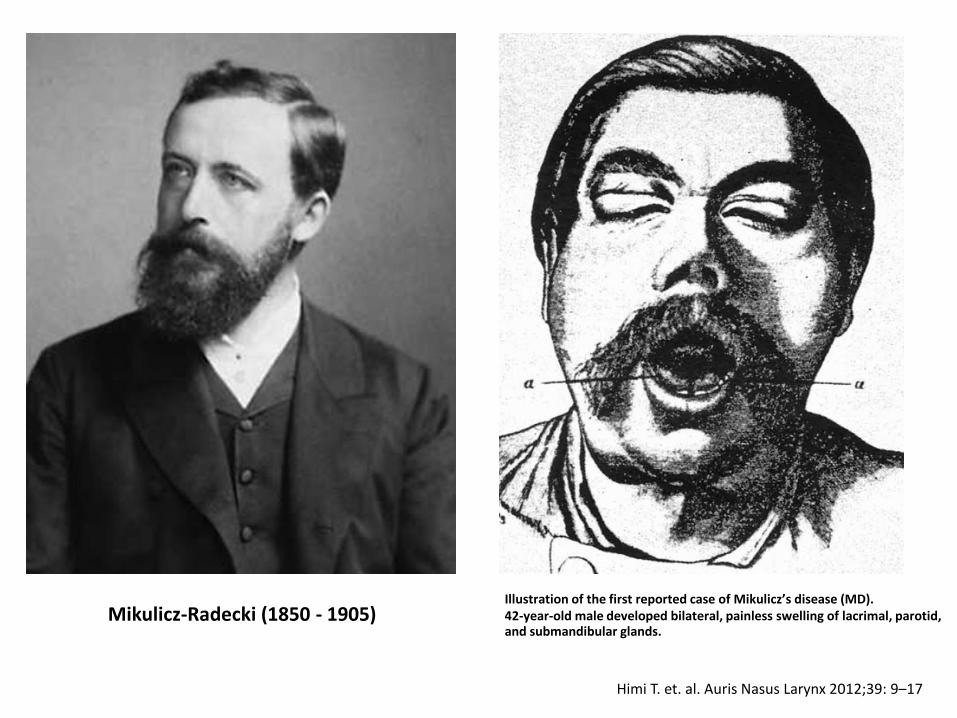
Himi T. et. al. Auris Nasus Larynx 2012;39: 9–17
Mikulicz-Radecki (1850 - 1905) Illustration of the first reported case of Mikulicz’s disease (MD). 42-year-old male developed bilateral, painless swelling of lacrimal, parotid, and submandibular glands.
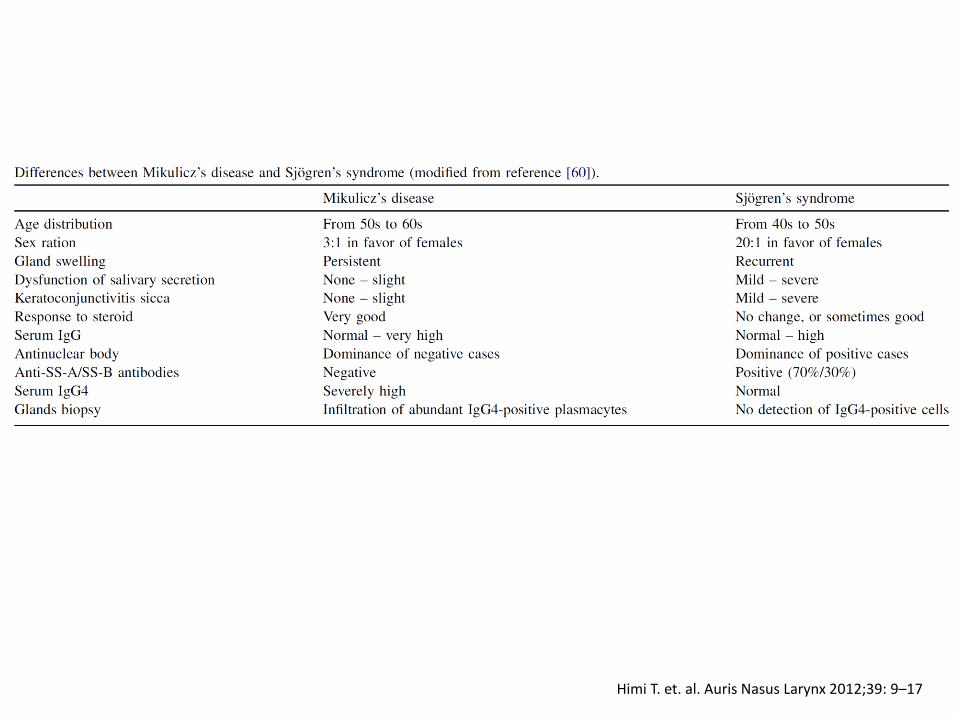
Himi T. et. al. Auris Nasus Larynx 2012;39: 9–17
Himi T. et. al. Auris Nasus Larynx 2012;39: 9–17
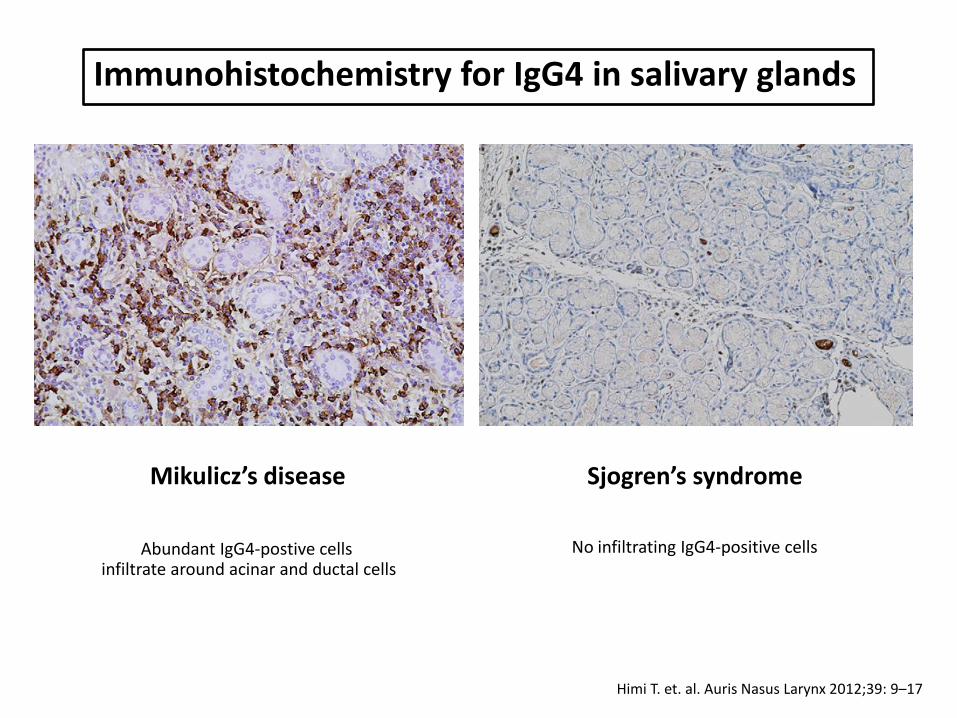
Immunohistochemistry for IgG4 in salivary glands
Abundant IgG4-postive cells infiltrate around acinar and ductal cells
No infiltrating IgG4-positive cells
Mikulicz’s disease Sjogren’s syndrome
Okazaki K. et. al. Autoimmunity Reviews 2014;451–8
Okazaki K. et. al. Autoimmunity Reviews 2014;451–8
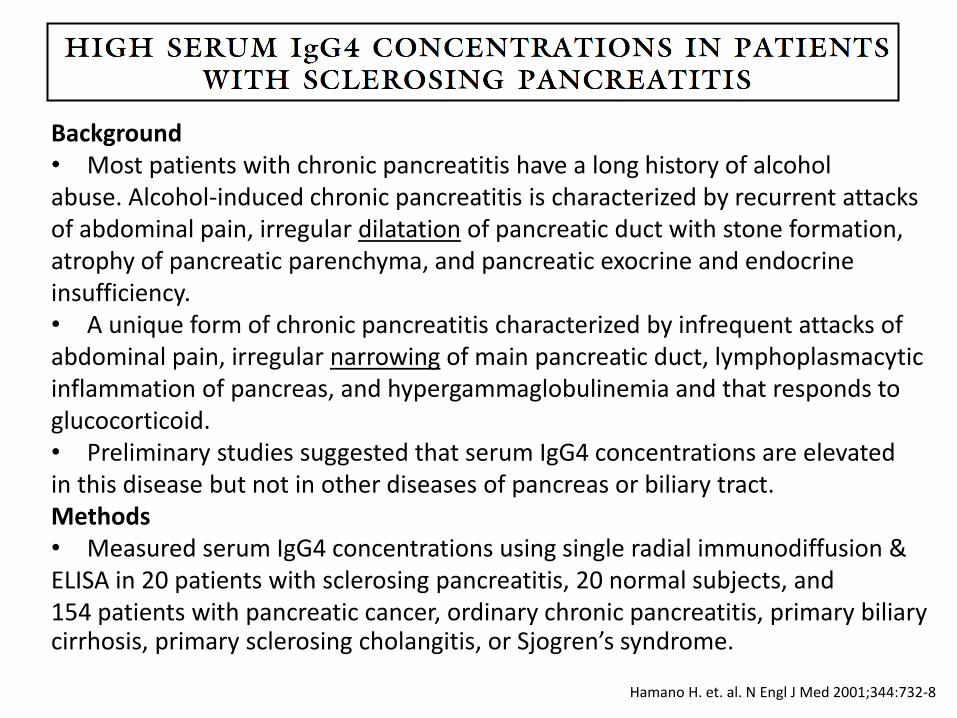
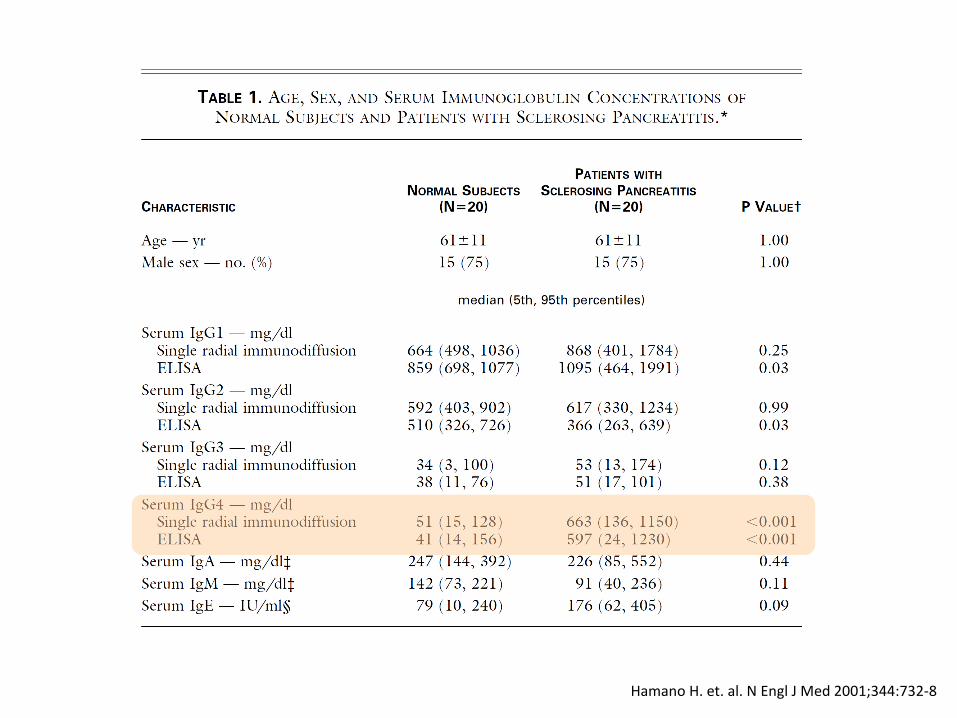
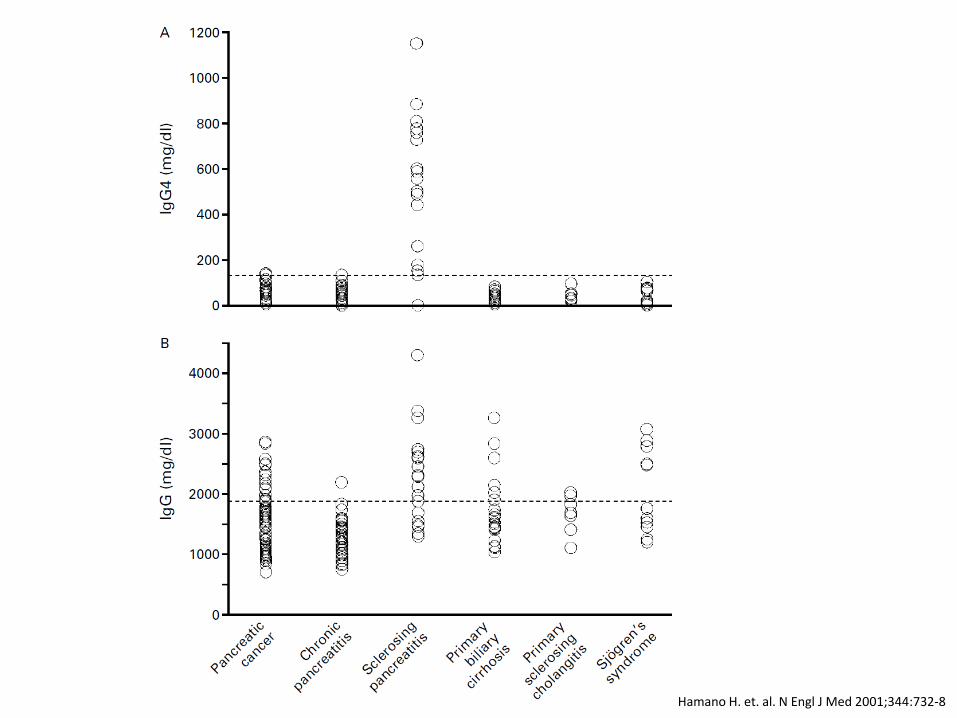
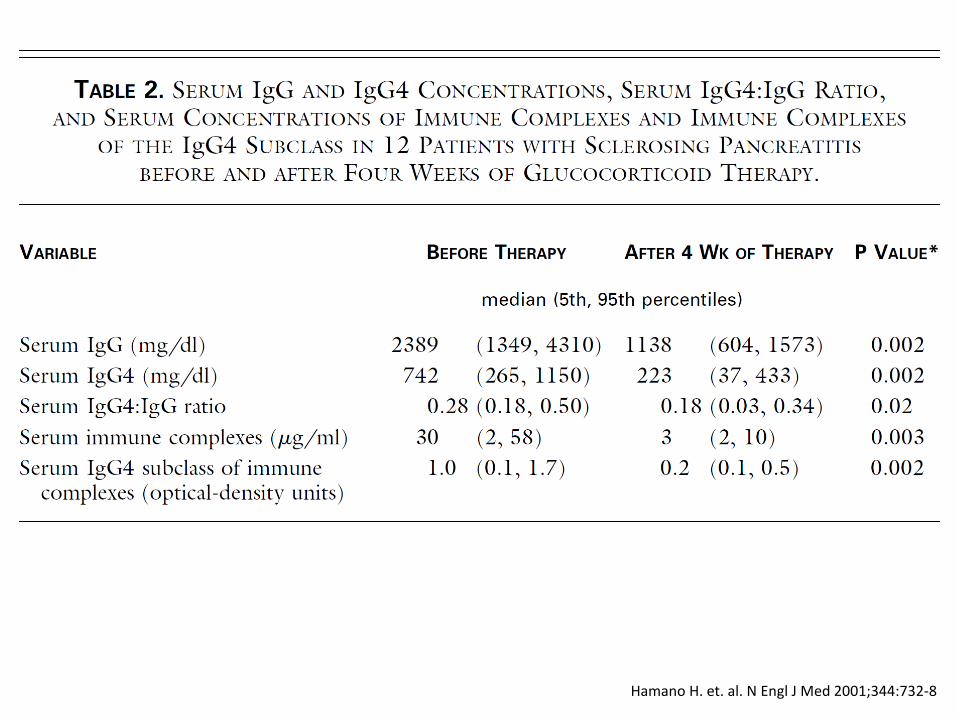
Hamano H. et. al. N Engl J Med 2001;344:732-8
Background • Most patients with chronic pancreatitis have a long history of alcohol abuse. Alcohol-induced chronic pancreatitis is characterized by recurrent attacks of abdominal pain, irregular dilatation of pancreatic duct with stone formation, atrophy of pancreatic parenchyma, and pancreatic exocrine and endocrine insufficiency. • A unique form of chronic pancreatitis characterized by infrequent attacks of abdominal pain, irregular narrowing of main pancreatic duct, lymphoplasmacytic inflammation of pancreas, and hypergammaglobulinemia and that responds to glucocorticoid. • Preliminary studies suggested that serum IgG4 concentrations are elevated in this disease but not in other diseases of pancreas or biliary tract. Methods • Measured serum IgG4 concentrations using single radial immunodiffusion & ELISA in 20 patients with sclerosing pancreatitis, 20 normal subjects, and 154 patients with pancreatic cancer, ordinary chronic pancreatitis, primary biliary cirrhosis, primary sclerosing cholangitis, or Sjogren’s syndrome.
Okazaki K. et. al. Autoimmunity Reviews 2014;451–8
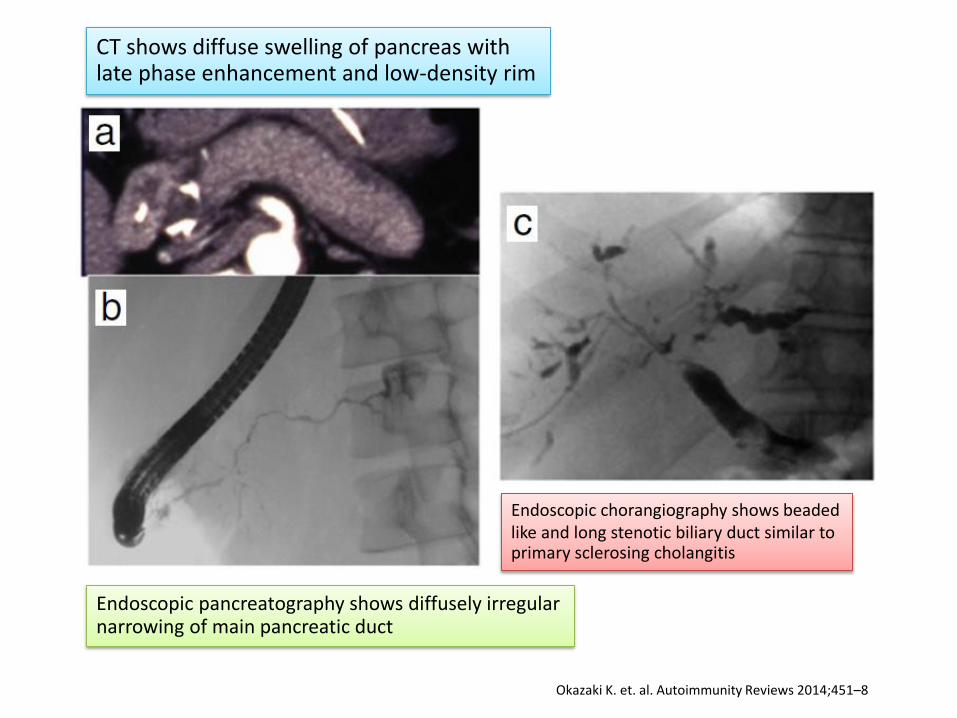
CT shows diffuse swelling of pancreas with late phase enhancement and low-density rim
Endoscopic pancreatography shows diffusely irregular narrowing of main pancreatic duct
Endoscopic chorangiography shows beaded like and long stenotic biliary duct similar to primary sclerosing cholangitis
Hamano H. et. al. N Engl J Med 2001;344:732-8
Hamano H. et. al. N Engl J Med 2001;344:732-8
Hamano H. et. al. N Engl J Med 2001;344:732-8
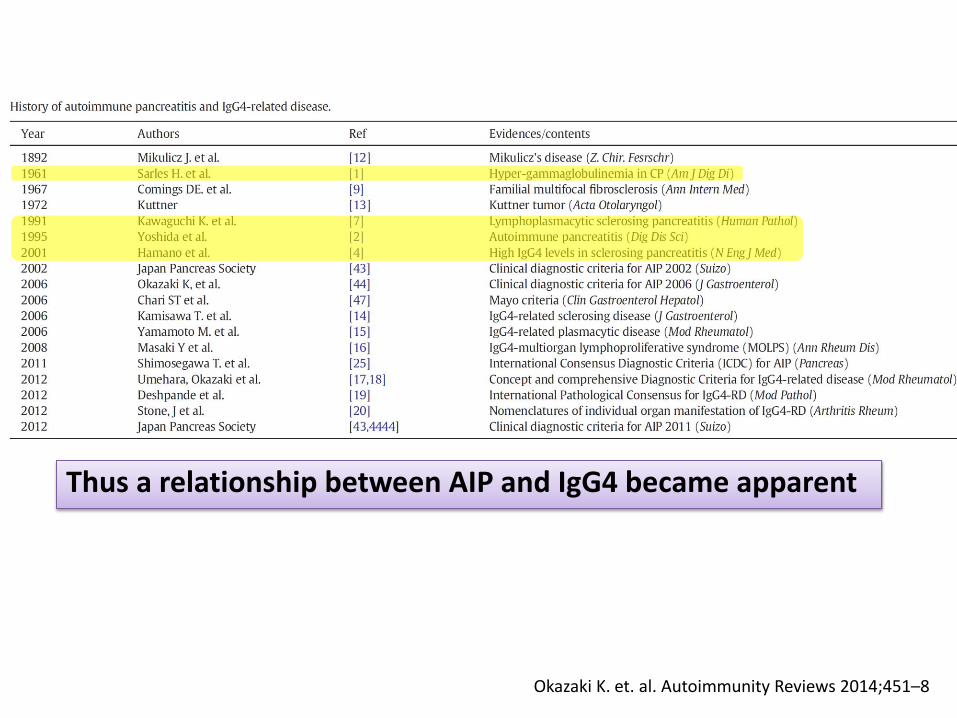
Okazaki K. et. al. Autoimmunity Reviews 2014;451–8
Thus a relationship between AIP and IgG4 became apparent
Okazaki K. et. al. Autoimmunity Reviews 2014;451–8
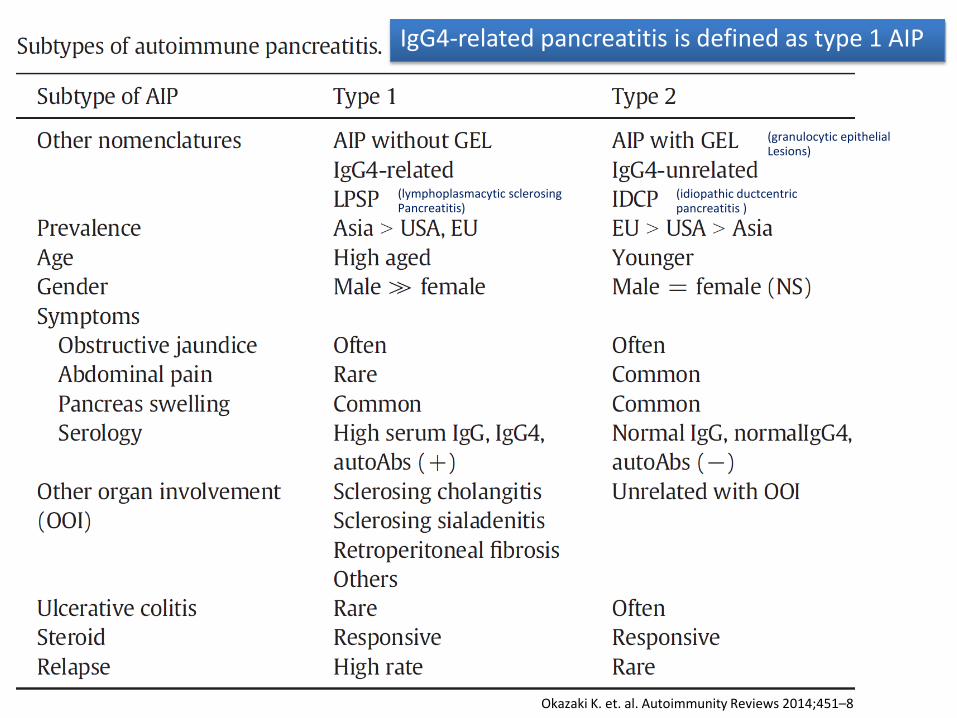
IgG4-related pancreatitis is defined as type 1 AIP
(lymphoplasmacytic sclerosing Pancreatitis)
(idiopathic ductcentric pancreatitis )
(granulocytic epithelial Lesions)
Okazaki K. et. al. Autoimmunity Reviews 2014;451–8
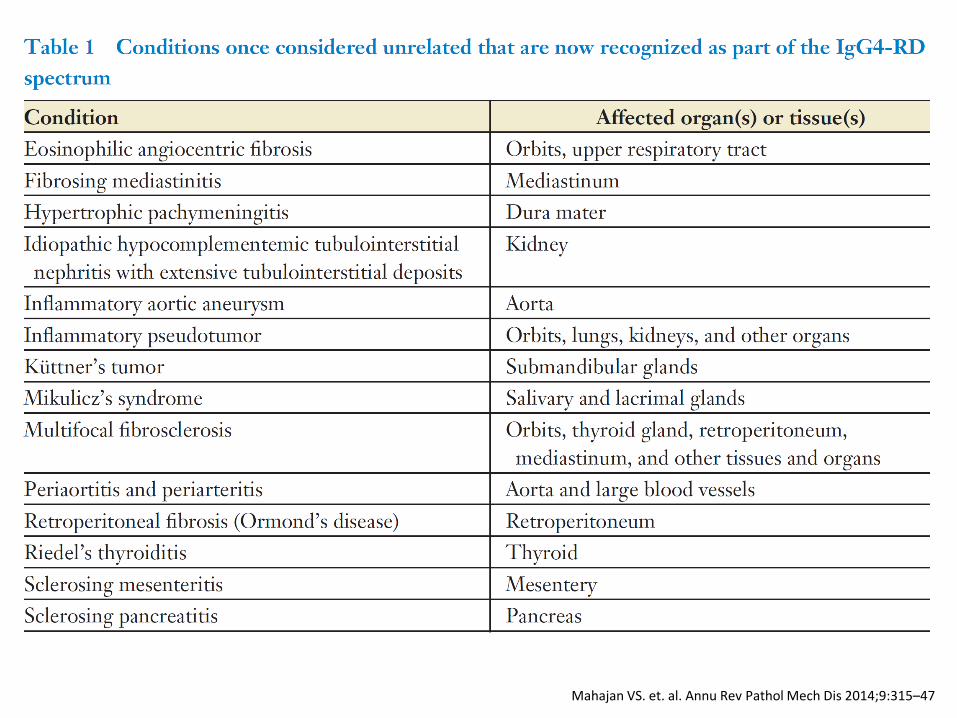
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47
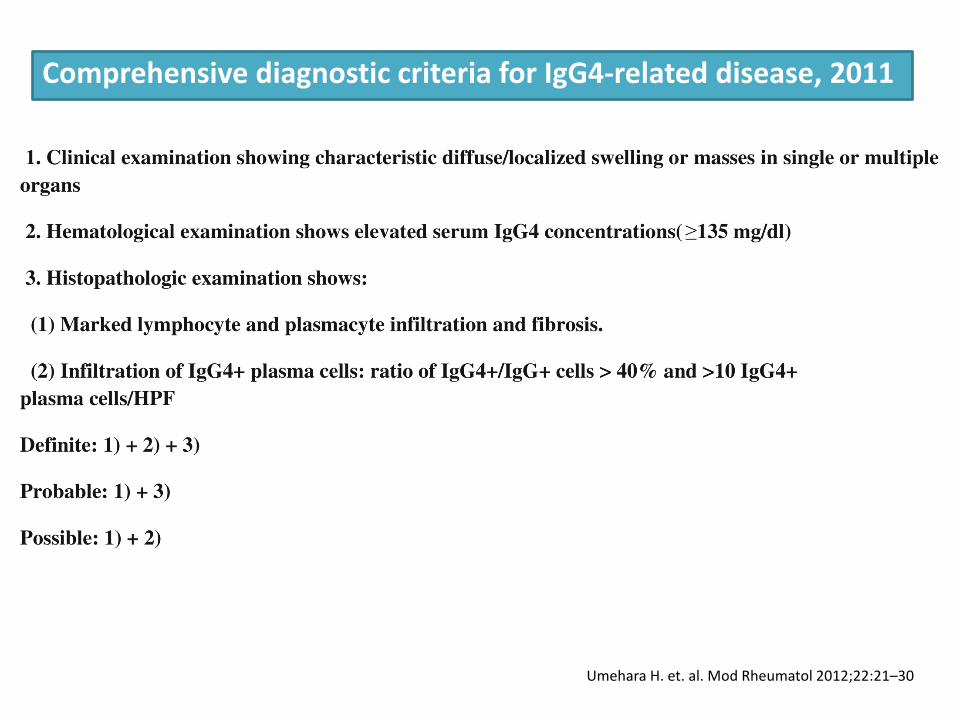
Umehara H. et. al. Mod Rheumatol 2012;22:21–30
Comprehensive diagnostic criteria for IgG4-related disease, 2011
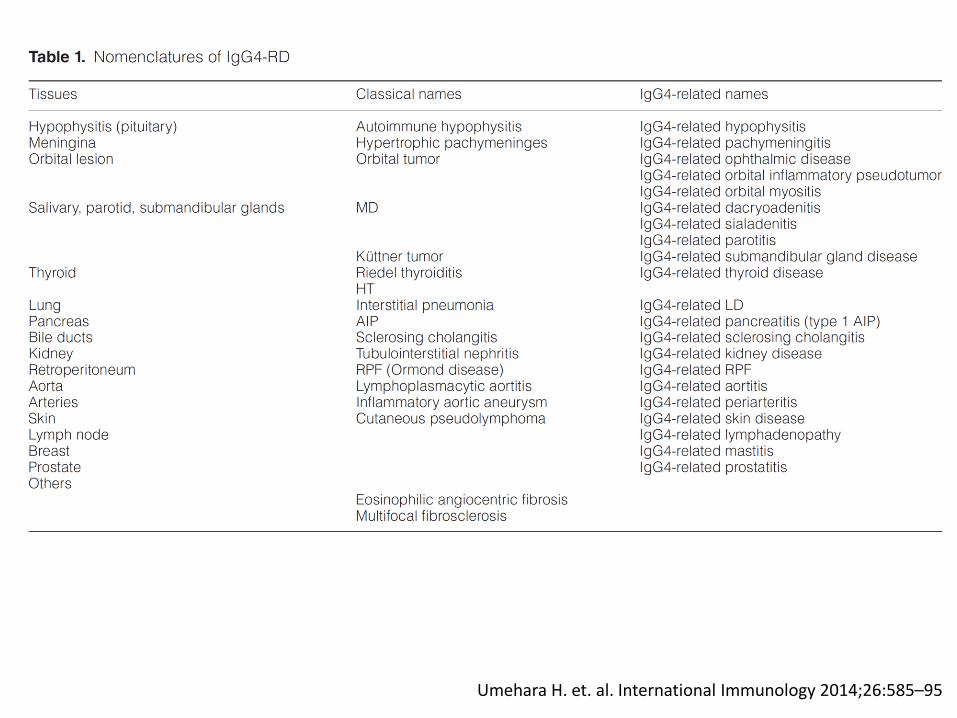
Umehara H. et. al. International Immunology 2014;26:585–95
Outline
• Introduction
• Historical context
• Pathogenesis
• Epidemiology
• Clinical manifestations and laboratory findings
• Treatment and prognosis
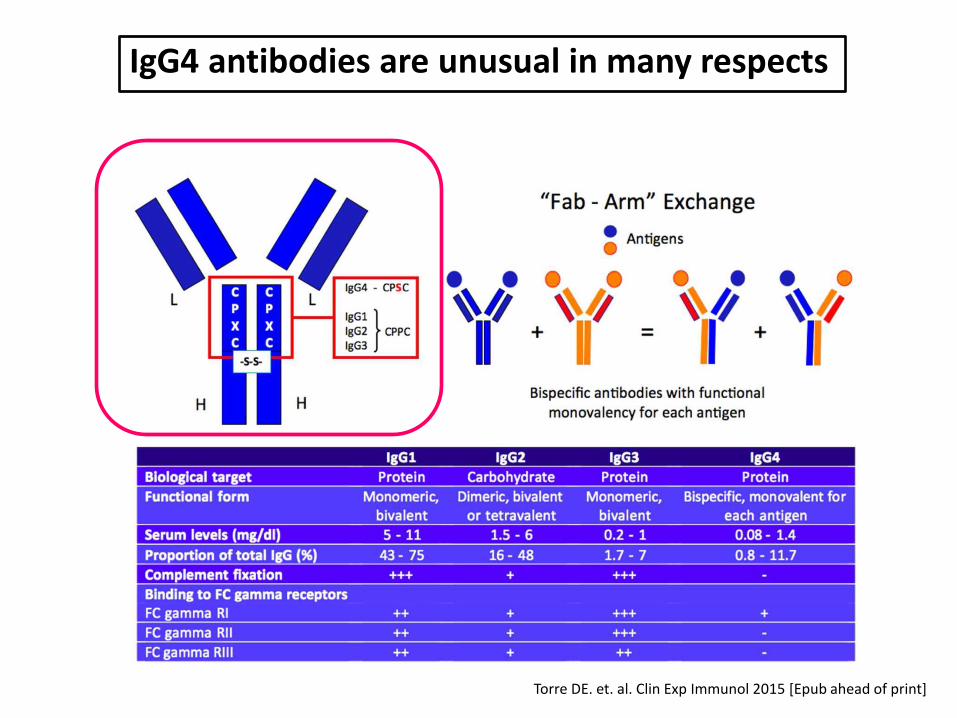
IgG4 antibodies are unusual in many respects
Torre DE. et. al. Clin Exp Immunol 2015 [Epub ahead of print]
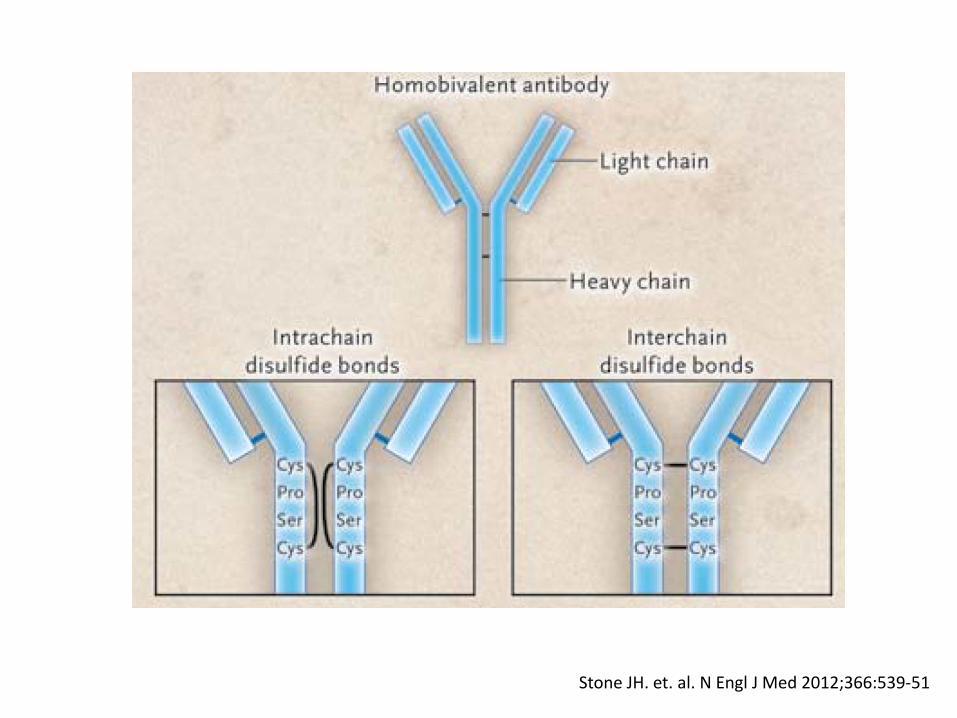
Stone JH. et. al. N Engl J Med 2012;366:539-51
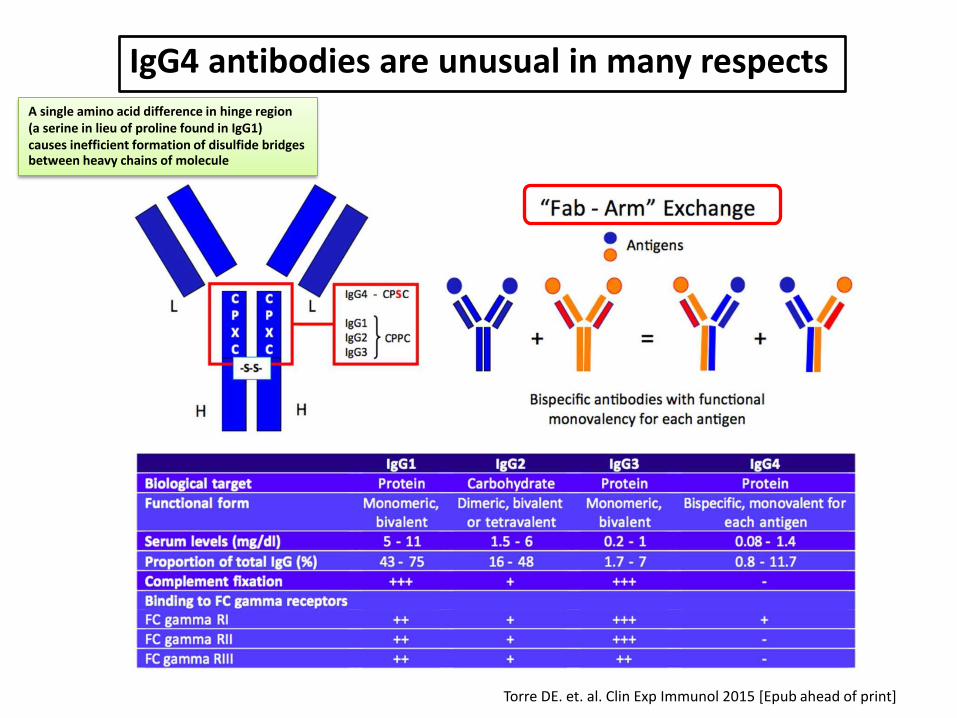
IgG4 antibodies are unusual in many respects
Torre DE. et. al. Clin Exp Immunol 2015 [Epub ahead of print]
A single amino acid difference in hinge region (a serine in lieu of proline found in IgG1) causes inefficient formation of disulfide bridges between heavy chains of molecule
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
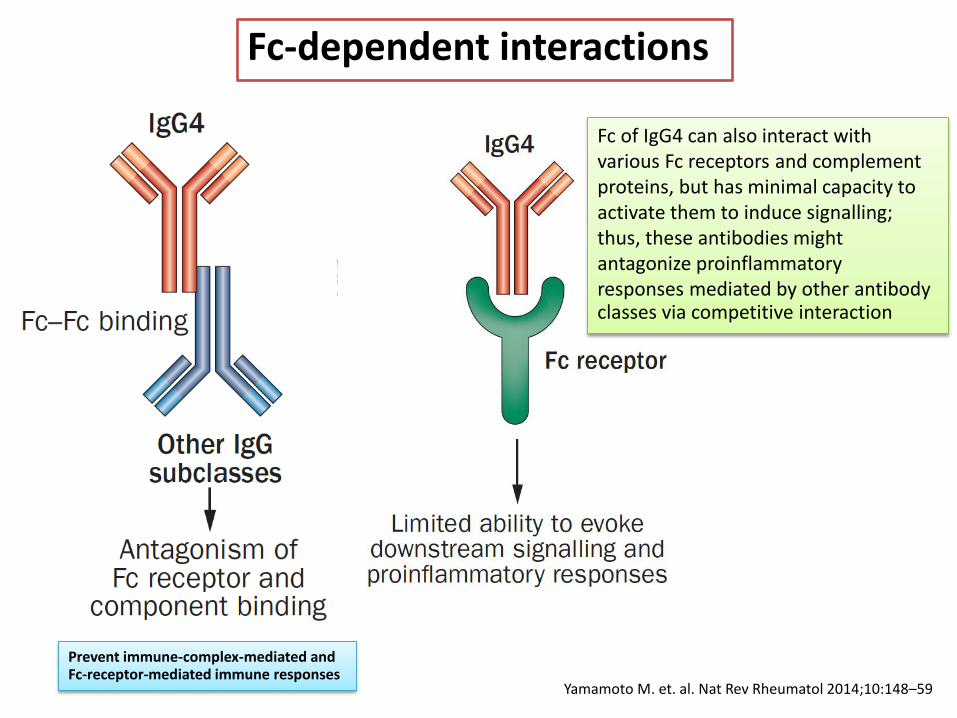
Fc-dependent interactions
Prevent immune-complex-mediated and Fc-receptor-mediated immune responses
Fc of IgG4 can also interact with various Fc receptors and complement proteins, but has minimal capacity to activate them to induce signalling; thus, these antibodies might antagonize proinflammatory responses mediated by other antibody classes via competitive interaction
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47
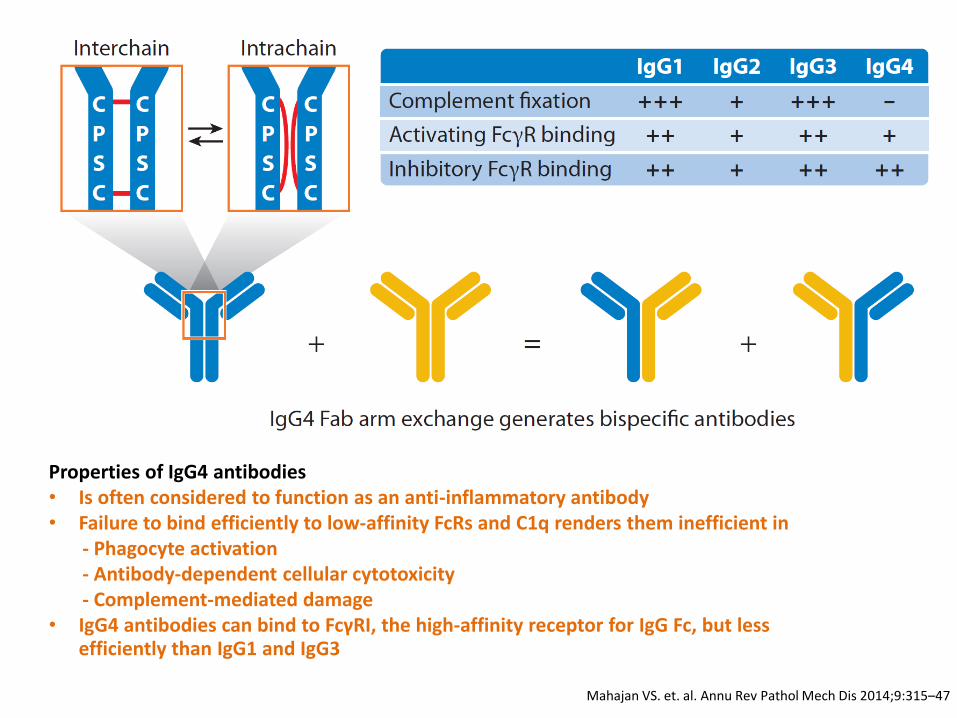
Properties of IgG4 antibodies • Is often considered to function as an anti-inflammatory antibody • Failure to bind efficiently to low-affinity FcRs and C1q renders them inefficient in - Phagocyte activation - Antibody-dependent cellular cytotoxicity - Complement-mediated damage • IgG4 antibodies can bind to FcγRI, the high-affinity receptor for IgG Fc, but less
efficiently than IgG1 and IgG3
Pathogenesis
• Remains unclear
• Whether IgG4 antibodies are pathogenic in IgG4-RD or are produced in excess in response to inflammatory stimuli due to their anti-inflammatory properties, remains unclear
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
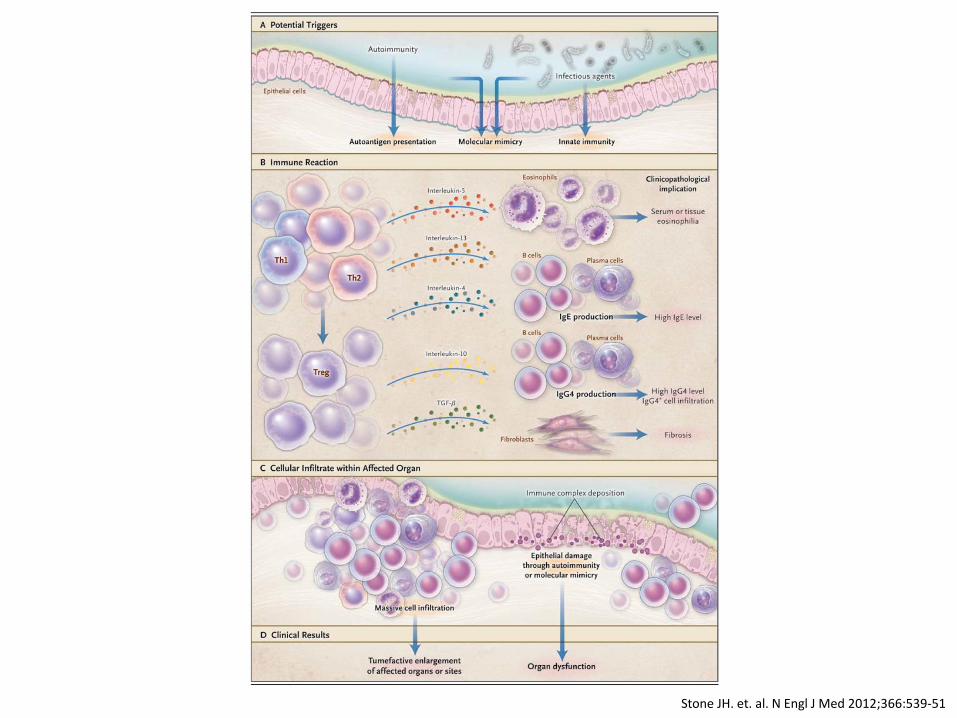
Stone JH. et. al. N Engl J Med 2012;366:539-51
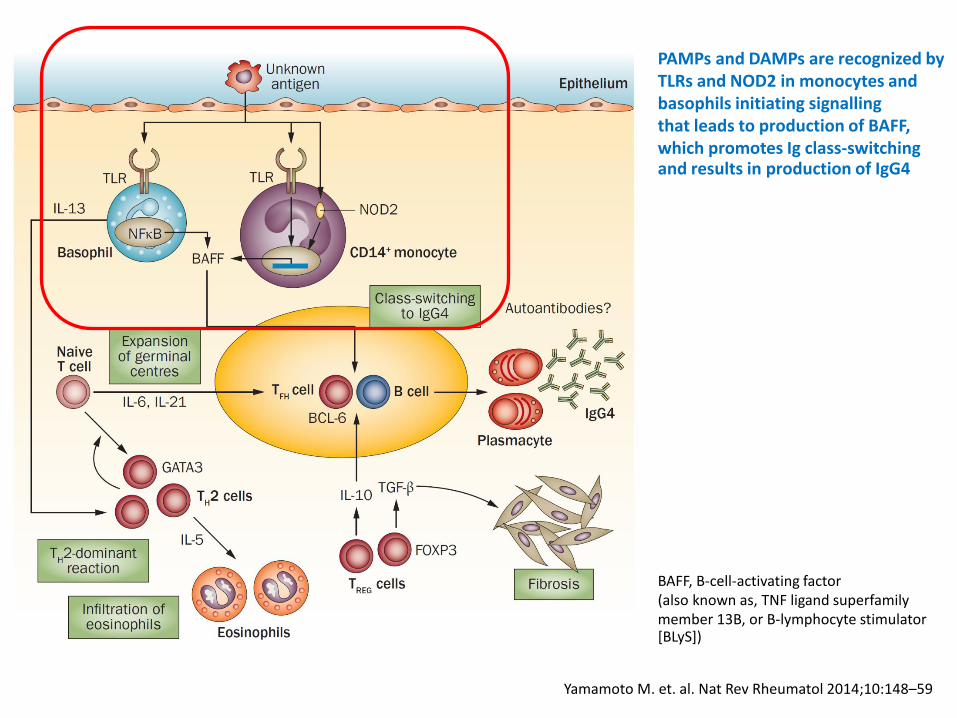
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
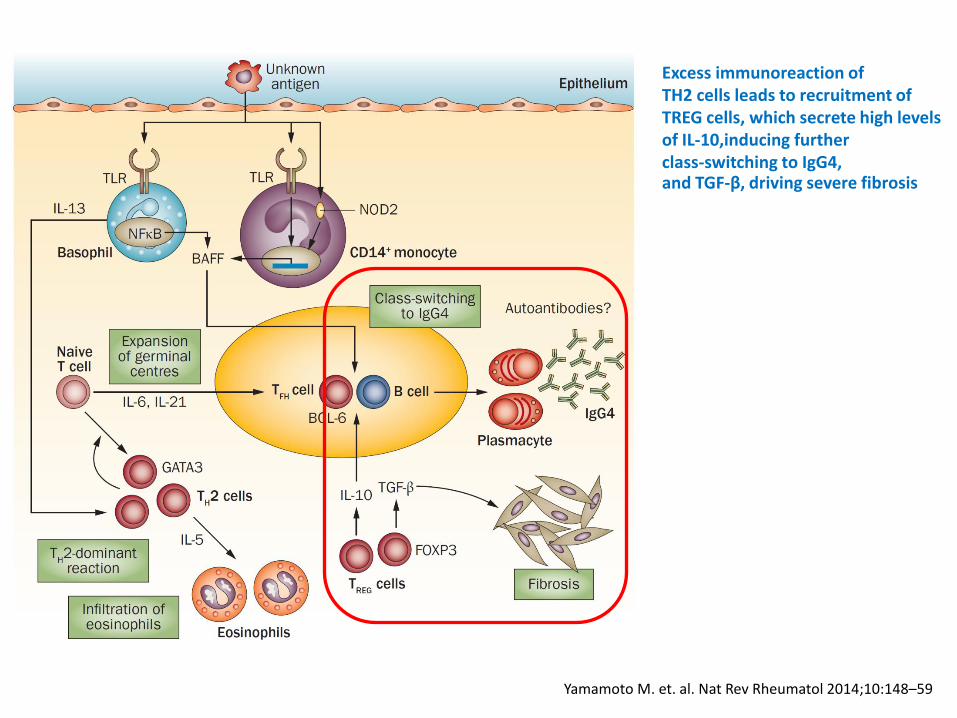
PAMPs and DAMPs are recognized by TLRs and NOD2 in monocytes and basophils initiating signalling that leads to production of BAFF, which promotes Ig class-switching and results in production of IgG4
BAFF, B-cell-activating factor (also known as, TNF ligand superfamily member 13B, or B-lymphocyte stimulator [BLyS])
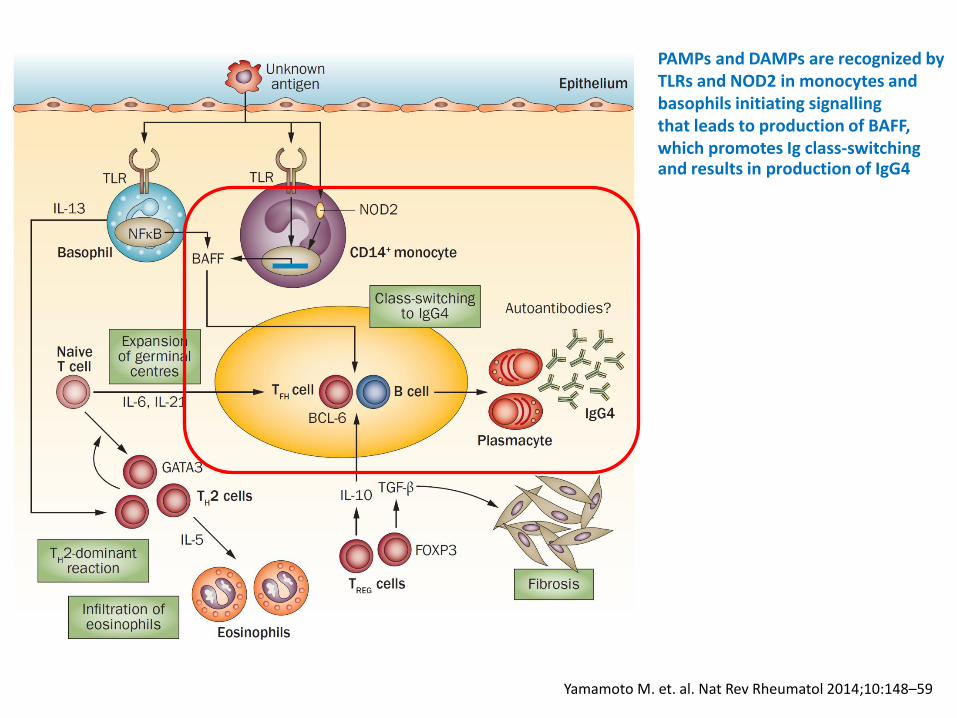
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
PAMPs and DAMPs are recognized by TLRs and NOD2 in monocytes and basophils initiating signalling that leads to production of BAFF, which promotes Ig class-switching and results in production of IgG4
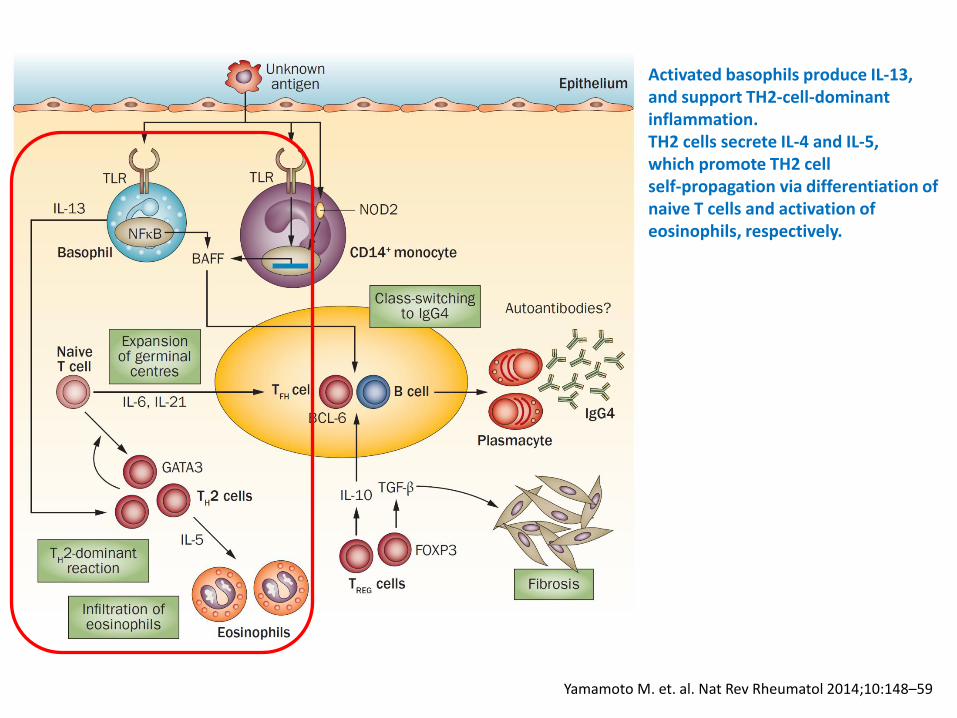
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Activated basophils produce IL-13, and support TH2-cell-dominant inflammation. TH2 cells secrete IL-4 and IL-5, which promote TH2 cell self-propagation via differentiation of naive T cells and activation of eosinophils, respectively.
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Excess immunoreaction of TH2 cells leads to recruitment of TREG cells, which secrete high levels of IL-10,inducing further class-switching to IgG4, and TGF-β, driving severe fibrosis
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
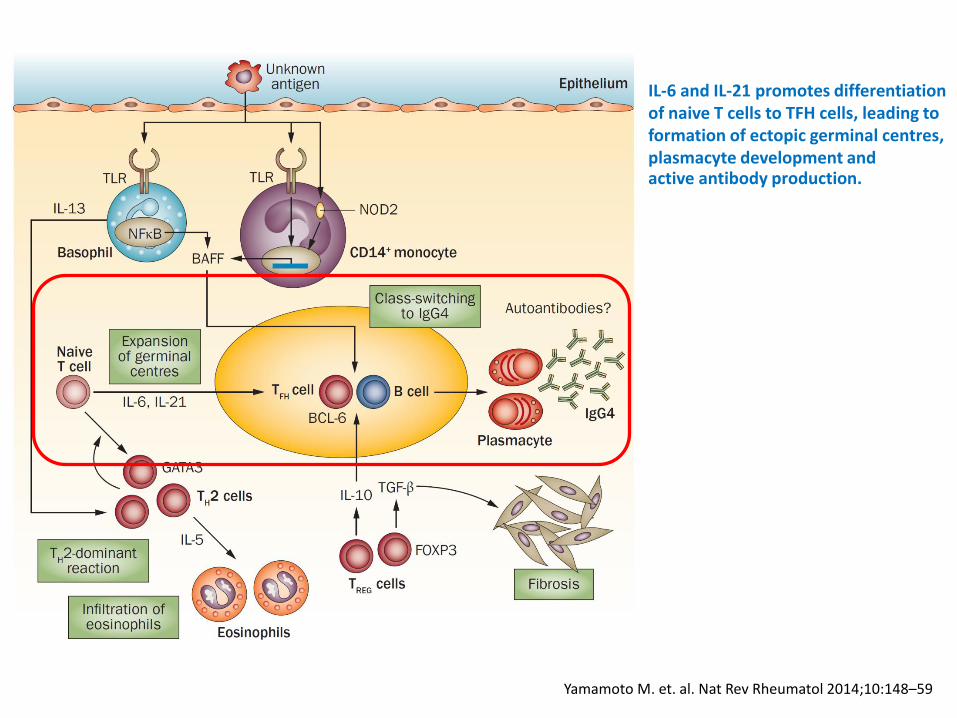
IL-6 and IL-21 promotes differentiation of naive T cells to TFH cells, leading to formation of ectopic germinal centres, plasmacyte development and active antibody production.
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47
Potential triggers
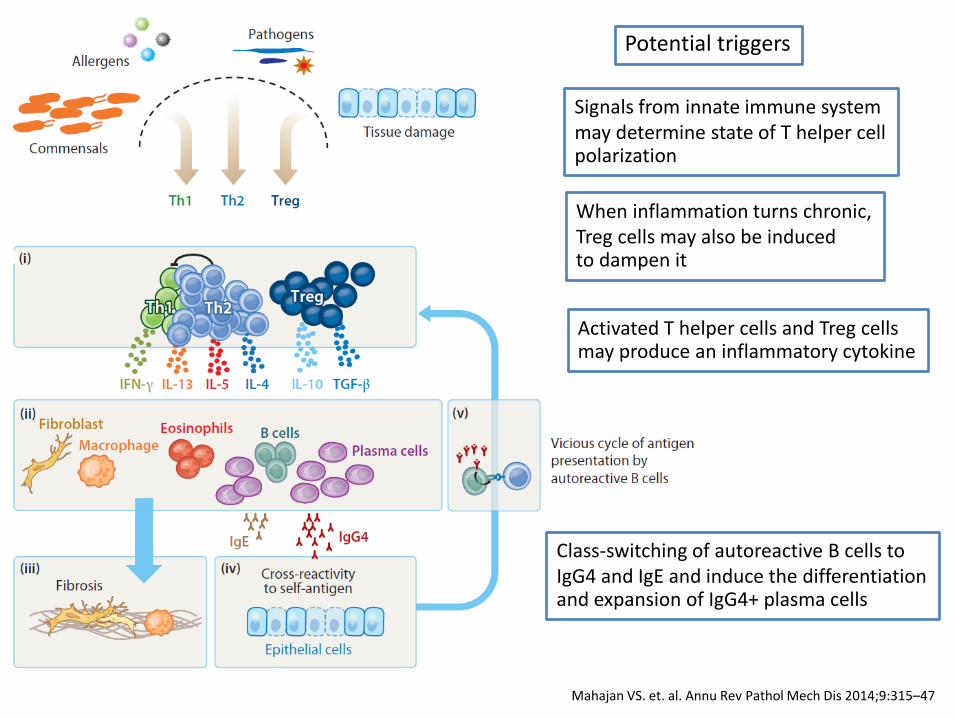
Signals from innate immune system may determine state of T helper cell polarization
When inflammation turns chronic, Treg cells may also be induced to dampen it
Activated T helper cells and Treg cells may produce an inflammatory cytokine
Class-switching of autoreactive B cells to IgG4 and IgE and induce the differentiation and expansion of IgG4+ plasma cells
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47
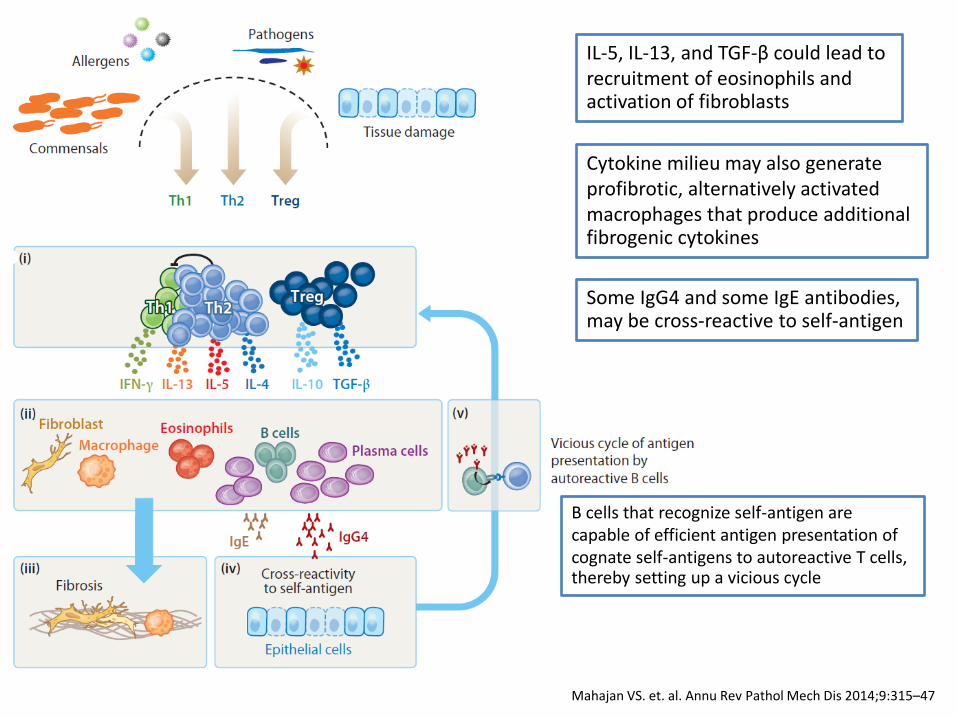
IL-5, IL-13, and TGF-β could lead to recruitment of eosinophils and activation of fibroblasts
Cytokine milieu may also generate profibrotic, alternatively activated macrophages that produce additional fibrogenic cytokines
Some IgG4 and some IgE antibodies, may be cross-reactive to self-antigen
B cells that recognize self-antigen are capable of efficient antigen presentation of cognate self-antigens to autoreactive T cells, thereby setting up a vicious cycle
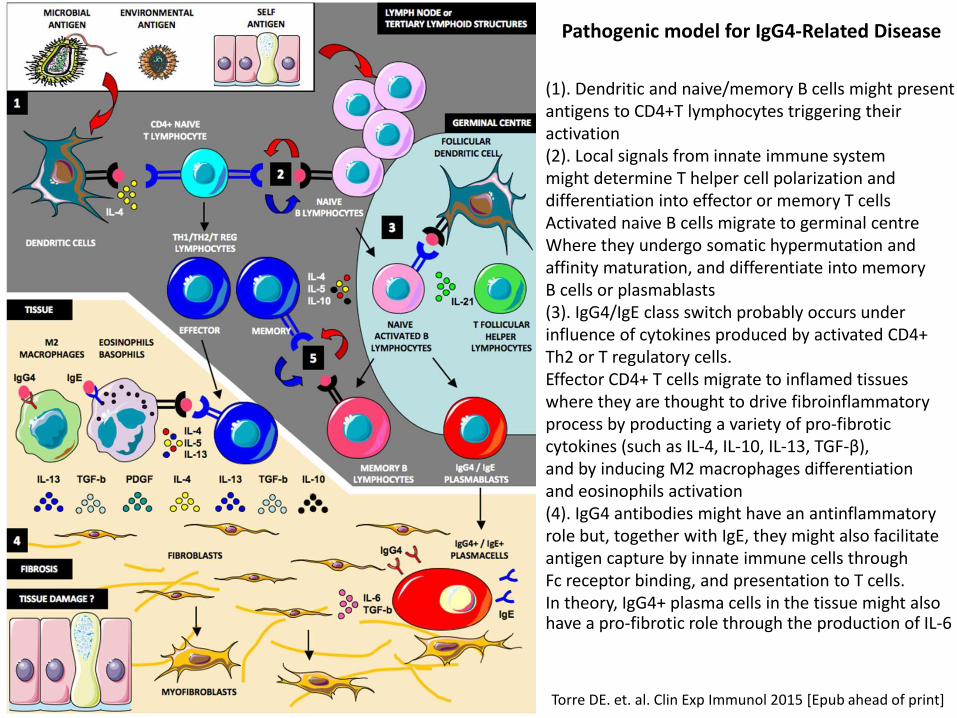
Pathogenic model for IgG4-Related Disease
Torre DE. et. al. Clin Exp Immunol 2015 [Epub ahead of print]
(1). Dendritic and naive/memory B cells might present antigens to CD4+T lymphocytes triggering their activation (2). Local signals from innate immune system might determine T helper cell polarization and differentiation into effector or memory T cells Activated naive B cells migrate to germinal centre Where they undergo somatic hypermutation and affinity maturation, and differentiate into memory B cells or plasmablasts (3). IgG4/IgE class switch probably occurs under influence of cytokines produced by activated CD4+ Th2 or T regulatory cells. Effector CD4+ T cells migrate to inflamed tissues where they are thought to drive fibroinflammatory process by producting a variety of pro-fibrotic cytokines (such as IL-4, IL-10, IL-13, TGF-β), and by inducing M2 macrophages differentiation and eosinophils activation (4). IgG4 antibodies might have an antinflammatory role but, together with IgE, they might also facilitate antigen capture by innate immune cells through Fc receptor binding, and presentation to T cells. In theory, IgG4+ plasma cells in the tissue might also have a pro-fibrotic role through the production of IL-6
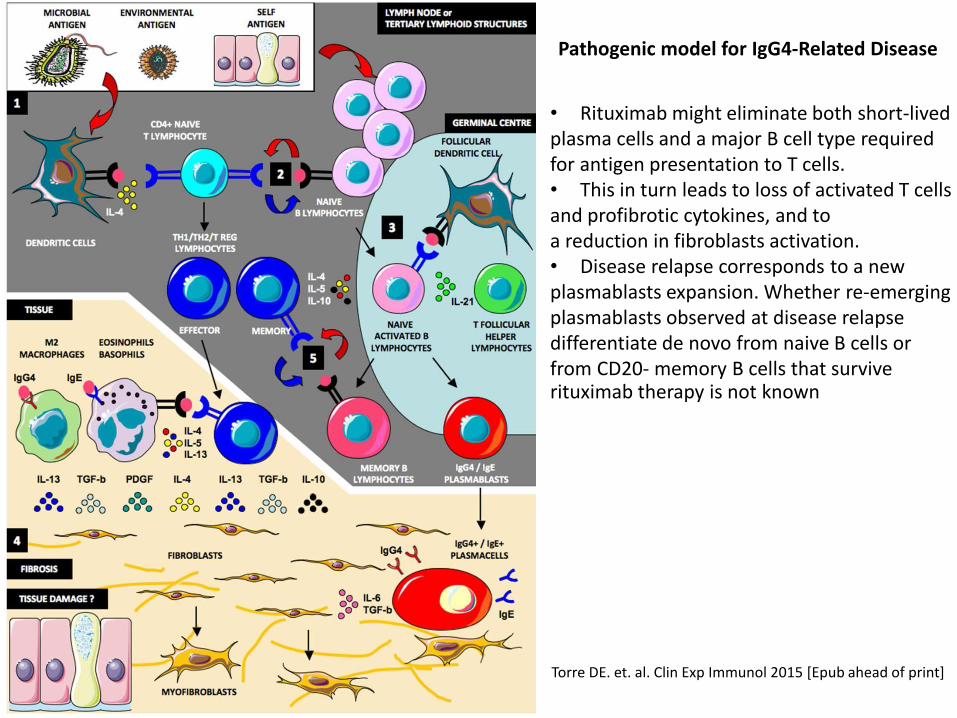
Pathogenic model for IgG4-Related Disease
Torre DE. et. al. Clin Exp Immunol 2015 [Epub ahead of print]
• Rituximab might eliminate both short-lived plasma cells and a major B cell type required for antigen presentation to T cells. • This in turn leads to loss of activated T cells and profibrotic cytokines, and to a reduction in fibroblasts activation. • Disease relapse corresponds to a new plasmablasts expansion. Whether re-emerging plasmablasts observed at disease relapse differentiate de novo from naive B cells or from CD20- memory B cells that survive rituximab therapy is not known
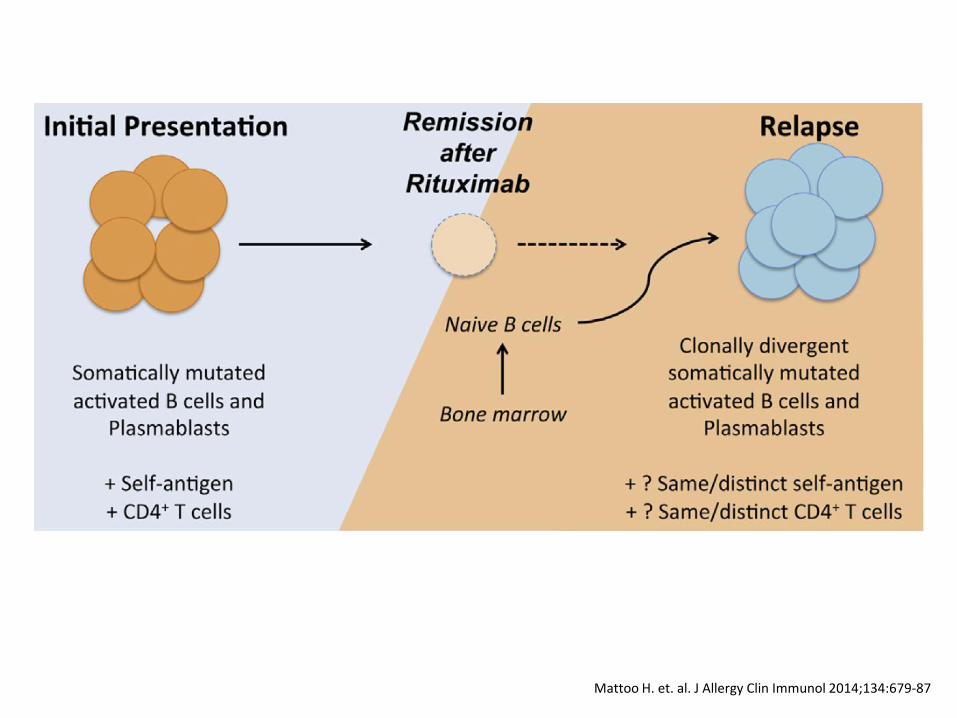
Mattoo H. et. al. J Allergy Clin Immunol 2014;134:679-87
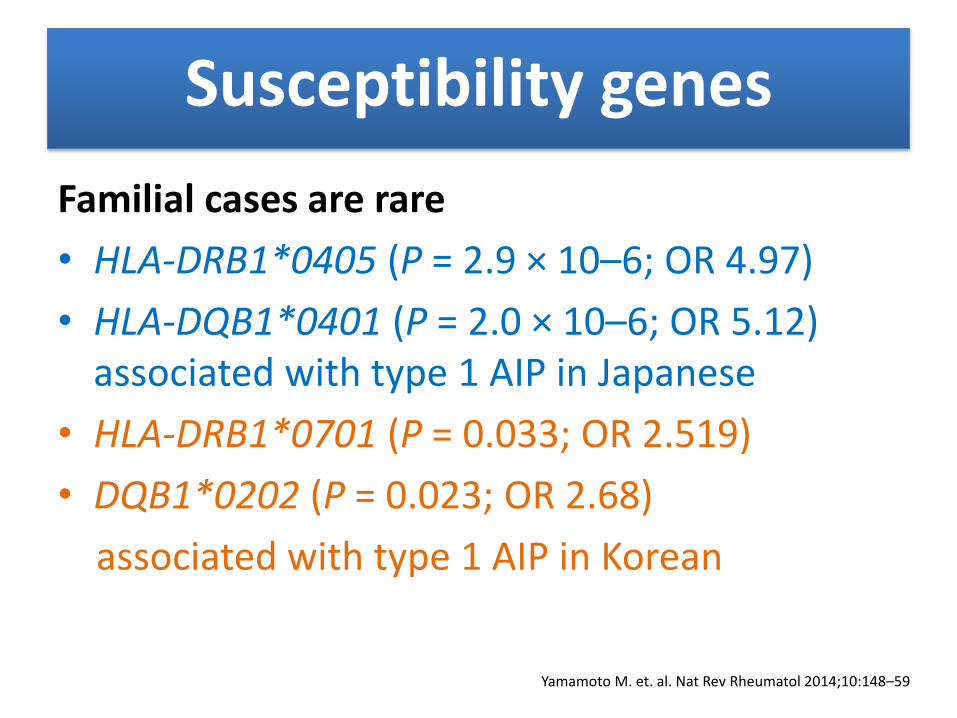
Susceptibility genes
Familial cases are rare
• HLA-DRB1*0405 (P = 2.9 × 10–6; OR 4.97)
• HLA-DQB1*0401 (P = 2.0 × 10–6; OR 5.12) associated with type 1 AIP in Japanese
• HLA-DRB1*0701 (P = 0.033; OR 2.519)
• DQB1*0202 (P = 0.023; OR 2.68)
associated with type 1 AIP in Korean
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Micro-organisms (1)
• Might be a triggering factor for the immune, and potentially autoimmune responses
• Helicobacter pylori plasminogen-binding protein (PBP) has been a focus of attention because antibodies targeting this protein were detected in patients with AIP
• PBP shares amino acid sequence homology with human E3 ubiquitin-protein ligase UBR2, which is expressed in pancreatic acini
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Micro-organisms (2)
• However, PBP is not specific to H. pylori, and is expressed by other enterobacteria
• Furthermore, study that identified anti- PBP antibodies in AIP only included patients with type 2 AIP
• Therefore, whether a relationship exists between PBP and IgG4-RD remains to be determined
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Autoantibodies • Hypergammaglobulinaemia and certain autoantibodies
are often detected
• In patients with IgG4-related dacryoadenitis and sialadenitis, ANA (titres ≥160:1) were detected in 15.7%, whereas RF was detected in 20.0%
• Anti-carbonic anhydrase II antibodies, anti-lactoferrin antibodies, and anti-pancreatic secretory trypsin inhibitor antibodies have been reported in patients with type 1 AIP
• However, these autoantibodies are neither associated with disease activity nor related to clinical features
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Outline
• Introduction
• Historical context
• Pathogenesis
• Epidemiology
• Clinical manifestations and laboratory findings
• Treatment and prognosis
Epidemiology (1)
• Remains poorly described, partly because of substantial challenges in recognition and diagnosis
• Most cases have been reported in Asia, but case reports from Europe and USA are now increasing
• Incidence throughout Japan was estimated to be 0.28–1.08/100,000, with 336–1,300 patients newly diagnosed per year
• Approximately 6,700–26,000 patients who developed IgG4-RD over the past 20 years
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47 Umehara H. et. al. Mod Rheumatol 2012;22:21–30
Epidemiology (2)
• Incidence of IgG4-RD through a network of Japanese researchers in an AIP study; they reported that 8,000 patients throughout Japan had IgG4-RD, including around 4,300 patients with IgG4-related dacryoadenitis and sialadenitis and 2,700 patients with type 1 AIP
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47 Umehara H. et. al. Mod Rheumatol 2012;22:21–30
Outline
• Introduction
• Historical context
• Pathogenesis
• Epidemiology
• Clinical manifestations and laboratory findings
• Treatment and prognosis
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
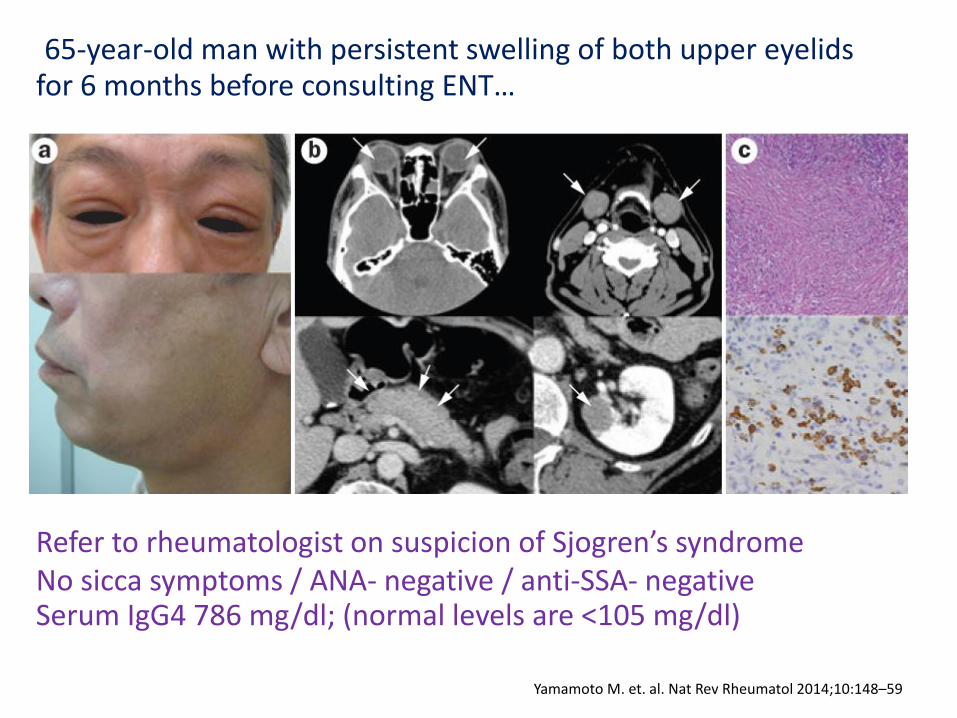
65-year-old man with persistent swelling of both upper eyelids for 6 months before consulting ENT…
Refer to rheumatologist on suspicion of Sjogren’s syndrome No sicca symptoms / ANA- negative / anti-SSA- negative Serum IgG4 786 mg/dl; (normal levels are <105 mg/dl)
Clinical signs & Lab finding (1)
• Typical patient is a middle aged to
elderly male
• Overall male-to-female ratio in most organ systems is 3.5 : 1
• Some variability exists in sex distribution
from organ to organ
• Head and neck, male to- female ratio is closer to 1 : 1
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47
Clinical signs & Lab finding (2)
• Swollen but painless organs
• Rarely present with general symptoms such as fever and malaise
• Almost all cases present with elevated serum levels of IgG4 (≥135 mg/dl)
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Clinical signs & Lab finding (3)
• Hypocomplementaemia and elevated levels of circulating immune complexes are often detected in patients with multiple organ dysfunction, particularly with renal involvement
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Organ involvement
Involvement of nearly every anatomic site has been reported, but most commonly affected;
• Pancreas
• Biliary tract
• Major salivary glands (submandibular, parotid)
• Lacrimal glands
• Retroperitoneum
• Lymph nodes
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
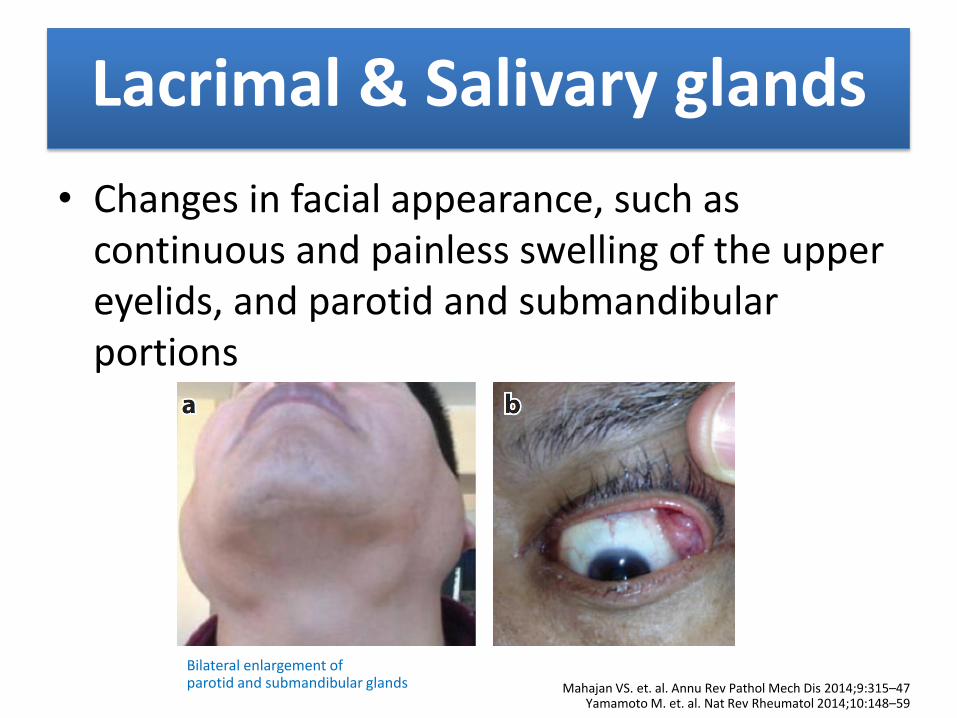
Lacrimal & Salivary glands
• Changes in facial appearance, such as continuous and painless swelling of the upper eyelids, and parotid and submandibular portions
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Bilateral enlargement of parotid and submandibular glands
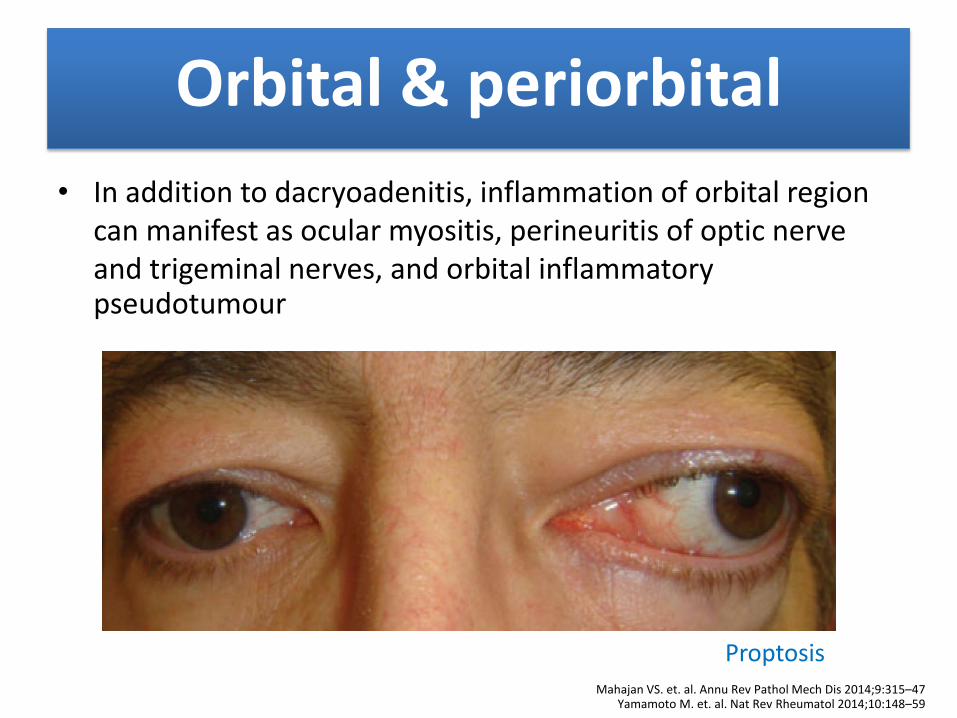
Orbital & periorbital • In addition to dacryoadenitis, inflammation of orbital region
can manifest as ocular myositis, perineuritis of optic nerve and trigeminal nerves, and orbital inflammatory pseudotumour
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Proptosis
Sogabe, Y. et al. Jpn J Ophthalmol 2012;56:511–4
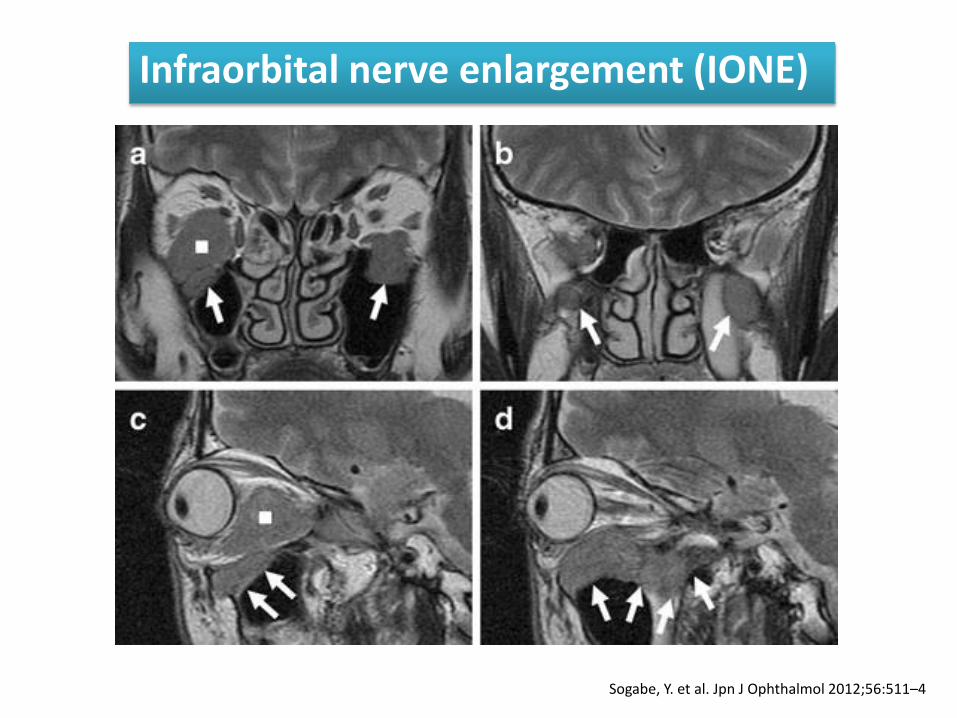
Infraorbital nerve enlargement (IONE)
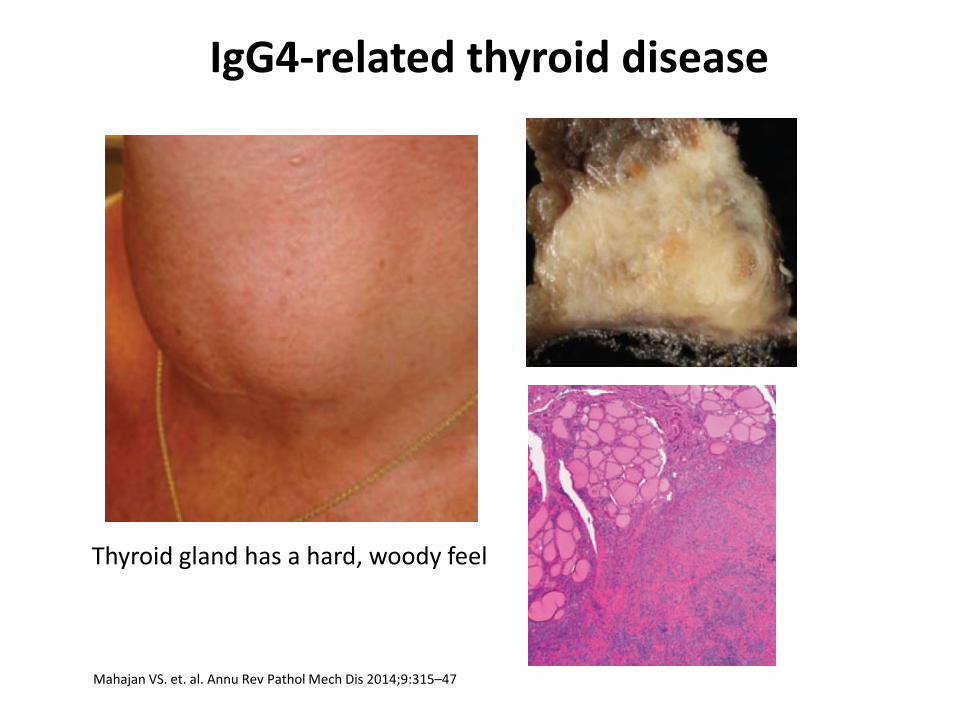
Thyroid gland
Certain forms of thyroiditis are on spectrum of IgG4-RD
• A substantial portion of cases of Riedel thyroiditis
• Fibrous variant of Hashimoto thyroiditis
IgG4-related thyroiditis is often associated with massive enlargement of thyroid due to lymphocytic infiltration
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47
IgG4-related thyroid disease
Thyroid gland has a hard, woody feel
Pituitary gland & dura mater
CNS involvement; generally does not affect brain parenchyma
• Hypophysitis (pituitary gland) Anterior hypophysitis; headache, visual field deficit
and lactation, etc.
Posterior hypophysitis is often associated with
diabetes insipidus Clinical manifestations depend on which hormonal axis is interrupted
• Pachymeningitis (dura mater) Involve either intracranial meninges or intraspinal meninges
Chronic headache and cranial neuropathy
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Lung and respiratory tract
Pulmonary involvement:
Bronchial
• asthma-like symptoms, with CT imaging revealing thickened bronchial and bronchiolar walls
Alveolar
• asymptomatic, but CT imaging detects various patterns of inflammation suggestive of interstitial or organizing pneumonia
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59

Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47
IgG4-RD has a predilection for bronchovascular bundle regions
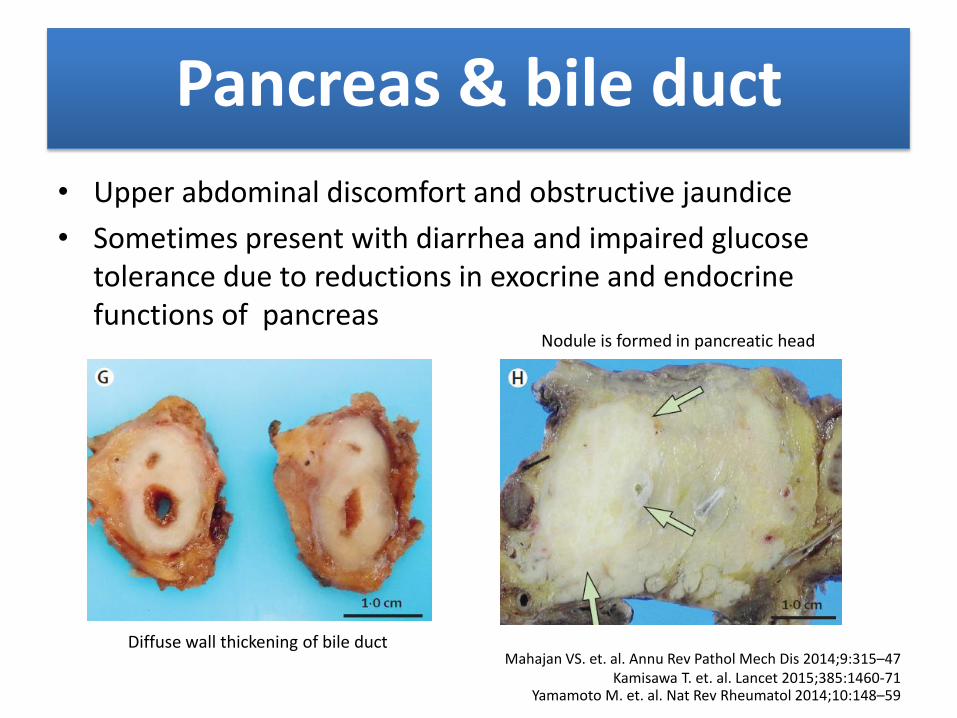
Pancreas & bile duct • Upper abdominal discomfort and obstructive jaundice
• Sometimes present with diarrhea and impaired glucose tolerance due to reductions in exocrine and endocrine functions of pancreas
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47 Kamisawa T. et. al. Lancet 2015;385:1460-71
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Diffuse wall thickening of bile duct
Nodule is formed in pancreatic head
Kidney
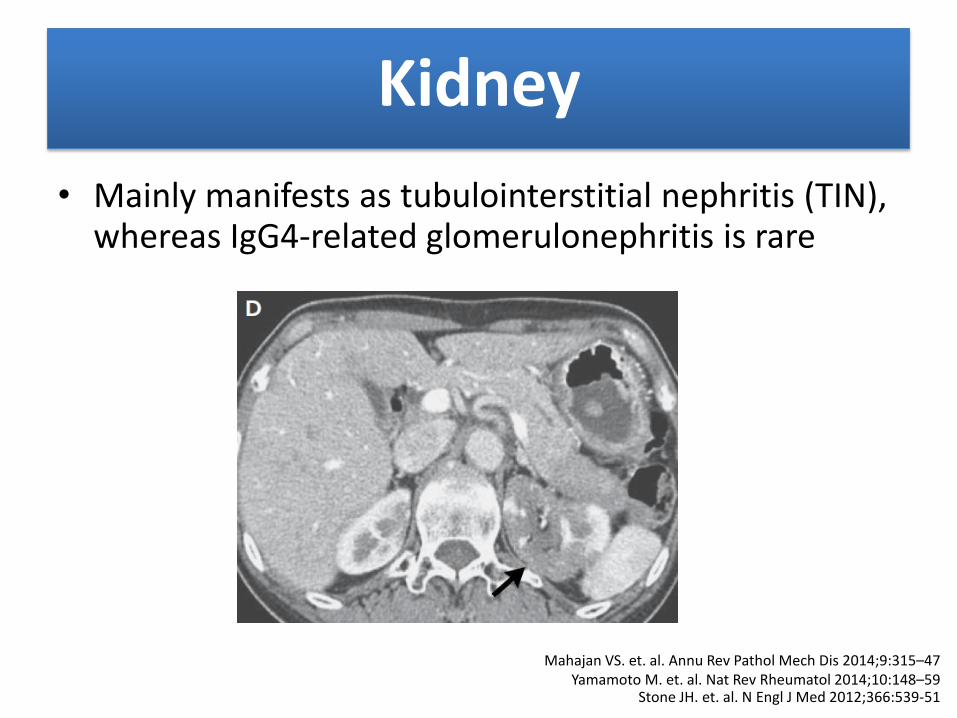
• Mainly manifests as tubulointerstitial nephritis (TIN), whereas IgG4-related glomerulonephritis is rare
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Stone JH. et. al. N Engl J Med 2012;366:539-51
Retroperitoneal cavity
• Retroperitoneal fibrosis can be drug-induced, malignancy-related or idiopathic
• A proportion of cases of idiopathic retroperitoneal fibrosis (Ormond’s disease) are considered to represent IgG4-RD
• Main affected sites are regions around thoracic and lumbar spine, abdominal aorta and branching arteries, and ureters
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
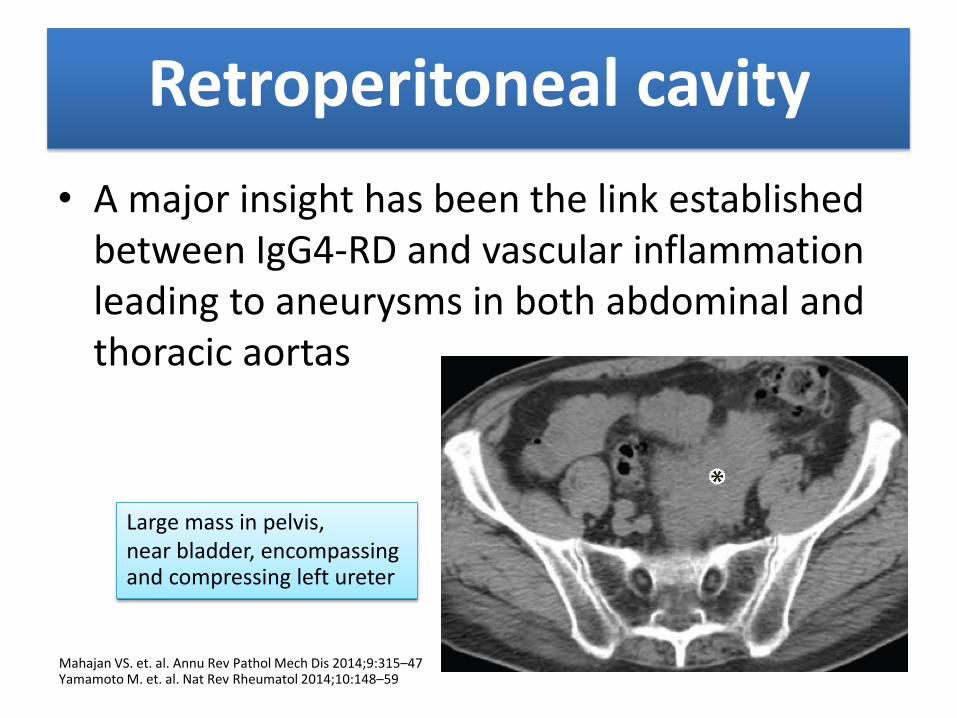
Retroperitoneal cavity
• A major insight has been the link established between IgG4-RD and vascular inflammation leading to aneurysms in both abdominal and thoracic aortas
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Large mass in pelvis, near bladder, encompassing and compressing left ureter
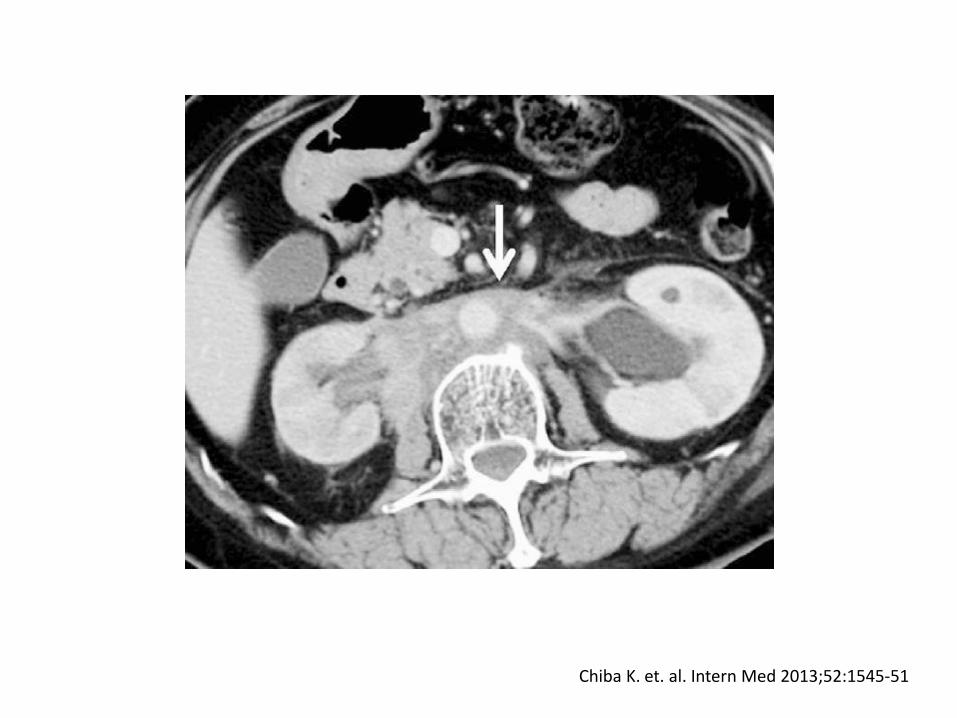
Chiba K. et. al. Intern Med 2013;52:1545-51
Prostate gland
• Symptoms of benign prostatic hyperplasia
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Lymph nodes
• Either generalized or localized adjacent to a specific affected organ
• Generally 1–3 cm in diameter and are non tender
• Although lymphadenopathy is often a prominent clinical feature, establishing diagnosis through lymph node biopsy is generally difficult because it is unusual for lymph nodes to undergo degree of fibrosis observed in other organs
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Skin
• Small number of patients with cutaneous disease associated with IgG4-RD
• Typical lesions are erythematous, flesh-colored papules with a predilection for head and cheeks
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59

Lowe GC. et. al. International Journal of Dermatology 2015;54:377–82
Bilateral lymphadenopathy and an erythematous eruption on chest, and a papular lichenoid eruption on lower extremity
Investigations
• Radiologic studies
• Serum IgG4 level
• Histopathology
Radiologic studies
• Indeed, diagnosis is often suggested by incidental radiologic findings on studies performed for reasons related or unrelated to IgG4-RD
• Selection of imaging modality appropriate to assessment of IgG4-RD is based on organ under evaluation, local radiology expertise, and availability, as well as considerations such as radiation exposure and cost
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Radiologic studies
• Enhanced CT and F-fluorodeoxyglucose positron emission tomography (FDG-PET) are useful tools for diagnosis and examination of complications
• CT images reveal organ enlargement
• FDG-PET detects severe inflammation
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Serum IgG4
• Remain important in evaluation and longitudinal assessments, but elevated levels are neither necessary nor sufficient for diagnosis of IgG4-RD
• 3 - 30% of patients have normal serum IgG4 level
• Elevated IgG4 concentrations have been observed in a variety of other conditions
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
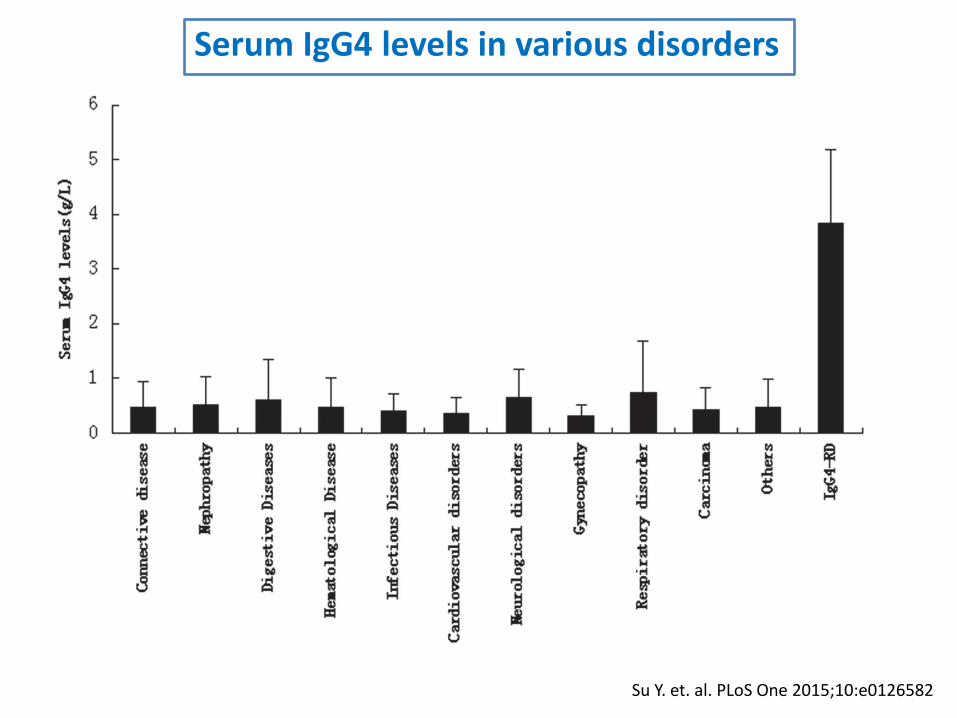
Su Y. et. al. PLoS One 2015;10:e0126582
Serum IgG4 levels in various disorders
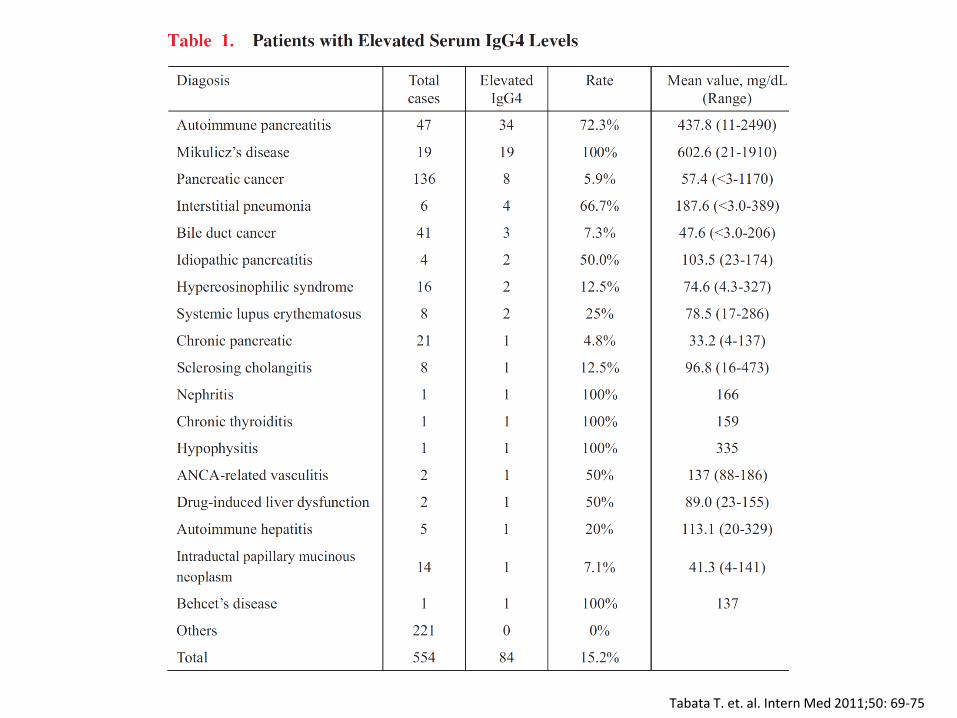
Tabata T. et. al. Intern Med 2011;50: 69-75
Serum IgG4
• However, degree of serum IgG4 elevation correlates with number of organs involved: the greater the extent of disease,
the higher the likelihood of an elevated
serum IgG4
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
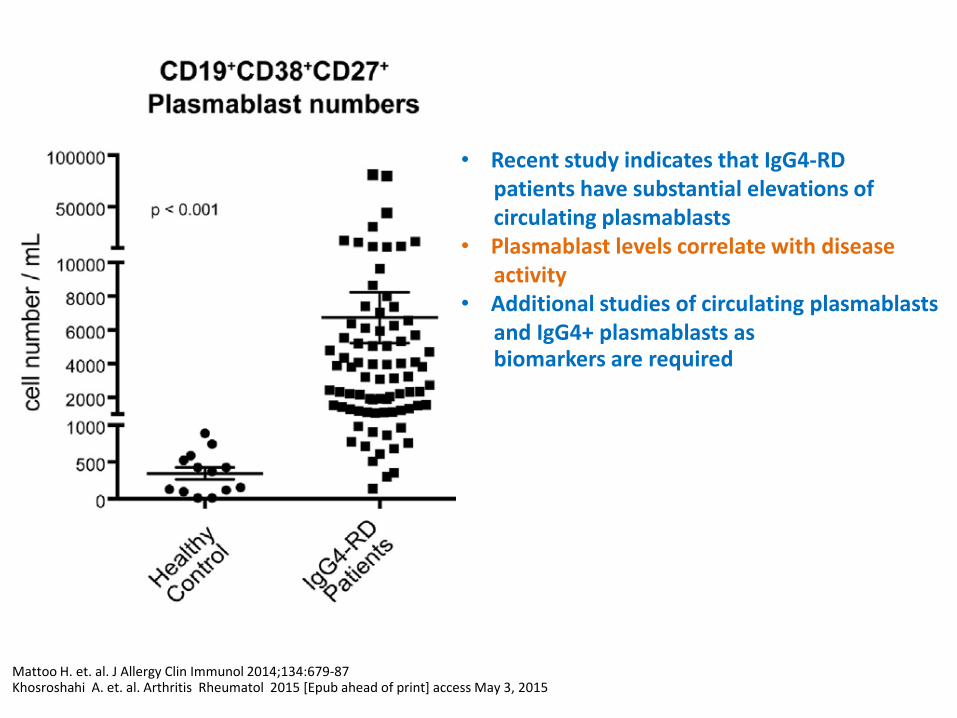
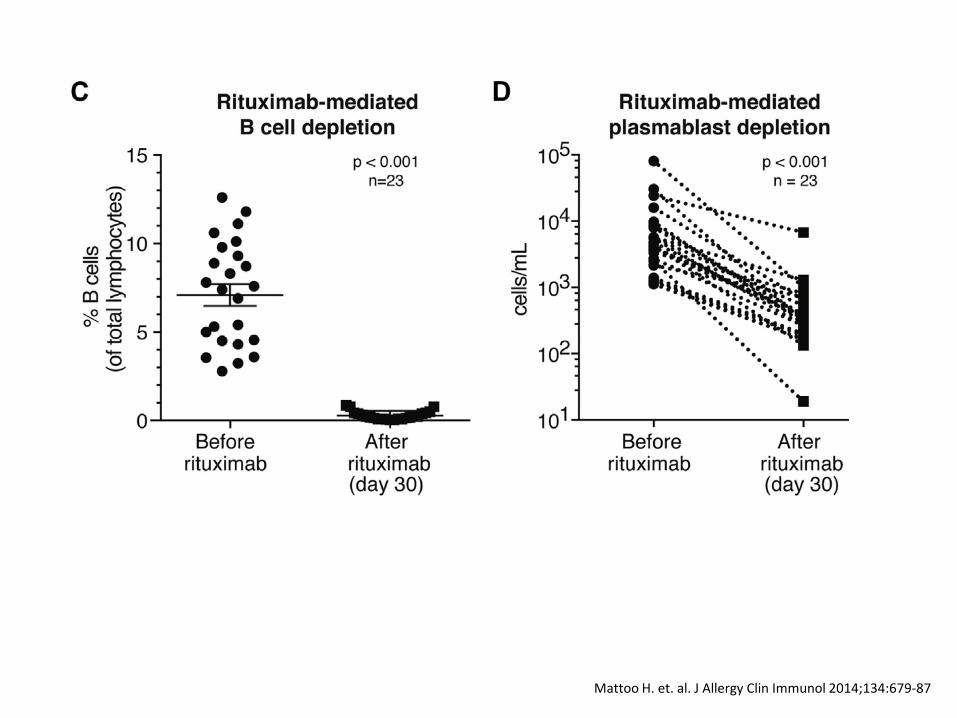
Mattoo H. et. al. J Allergy Clin Immunol 2014;134:679-87 Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
• Recent study indicates that IgG4-RD patients have substantial elevations of circulating plasmablasts • Plasmablast levels correlate with disease activity • Additional studies of circulating plasmablasts and IgG4+ plasmablasts as biomarkers are required
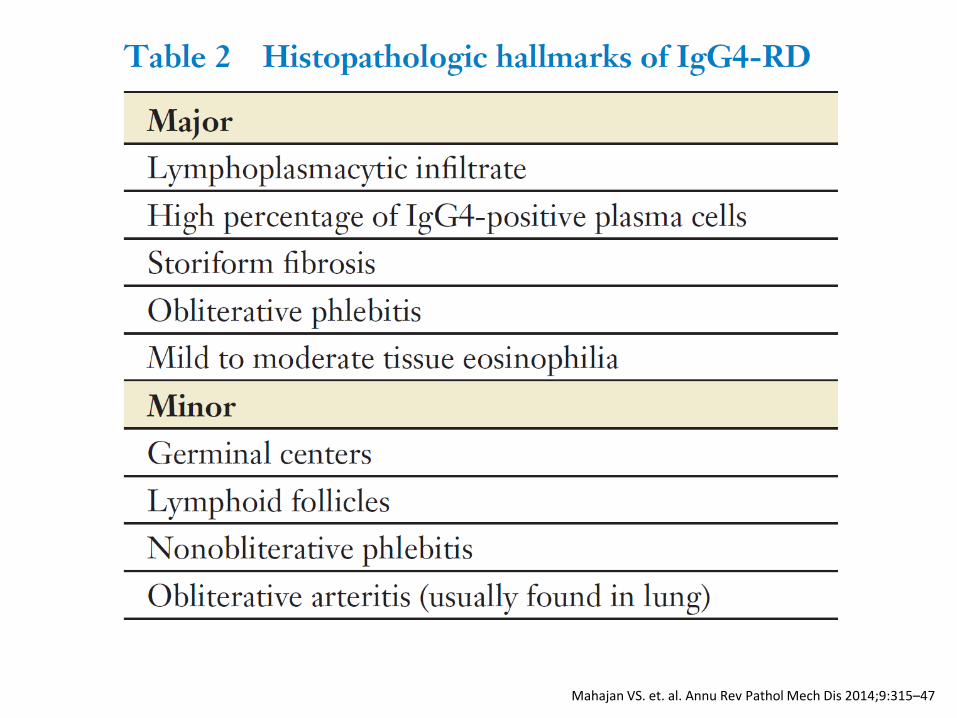
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47
Stone JH. et. al. N Engl J Med 2012;366:539-51
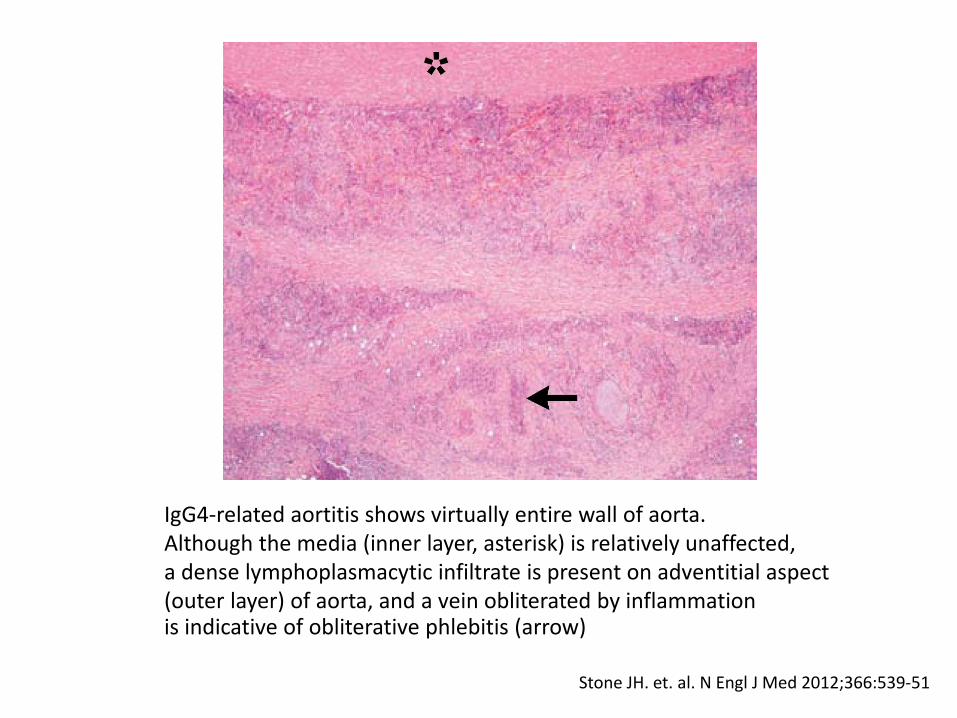
IgG4-related aortitis shows virtually entire wall of aorta. Although the media (inner layer, asterisk) is relatively unaffected, a dense lymphoplasmacytic infiltrate is present on adventitial aspect (outer layer) of aorta, and a vein obliterated by inflammation is indicative of obliterative phlebitis (arrow)
Kamisawa T. et. al. Lancet 2015;385:1460-71 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
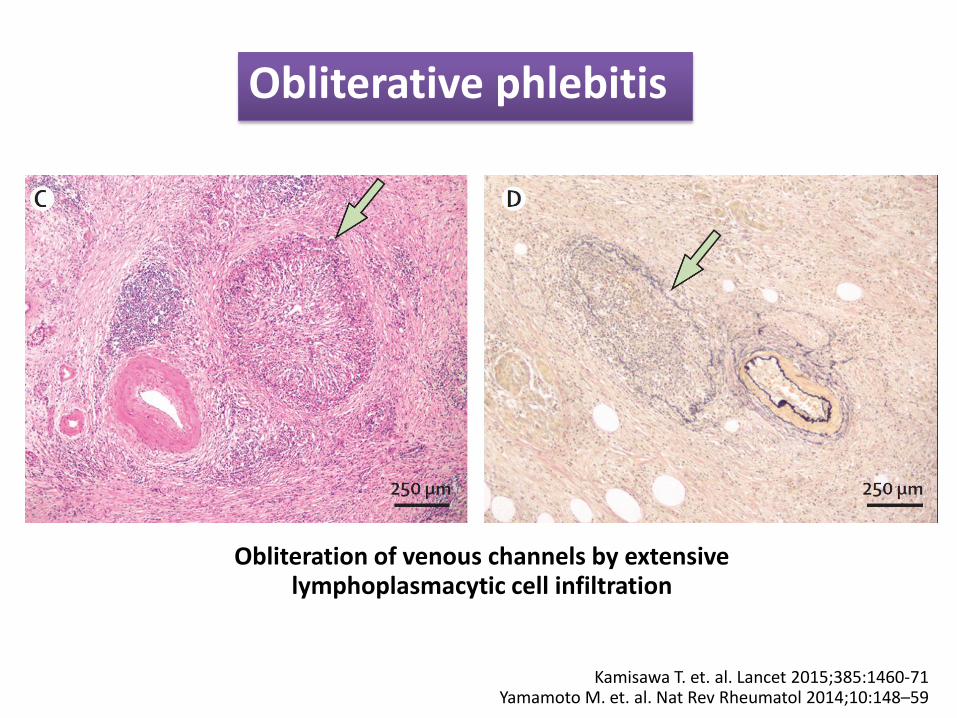
Obliterative phlebitis
Obliteration of venous channels by extensive lymphoplasmacytic cell infiltration
Kamisawa T. et. al. Lancet 2015;385:1460-71
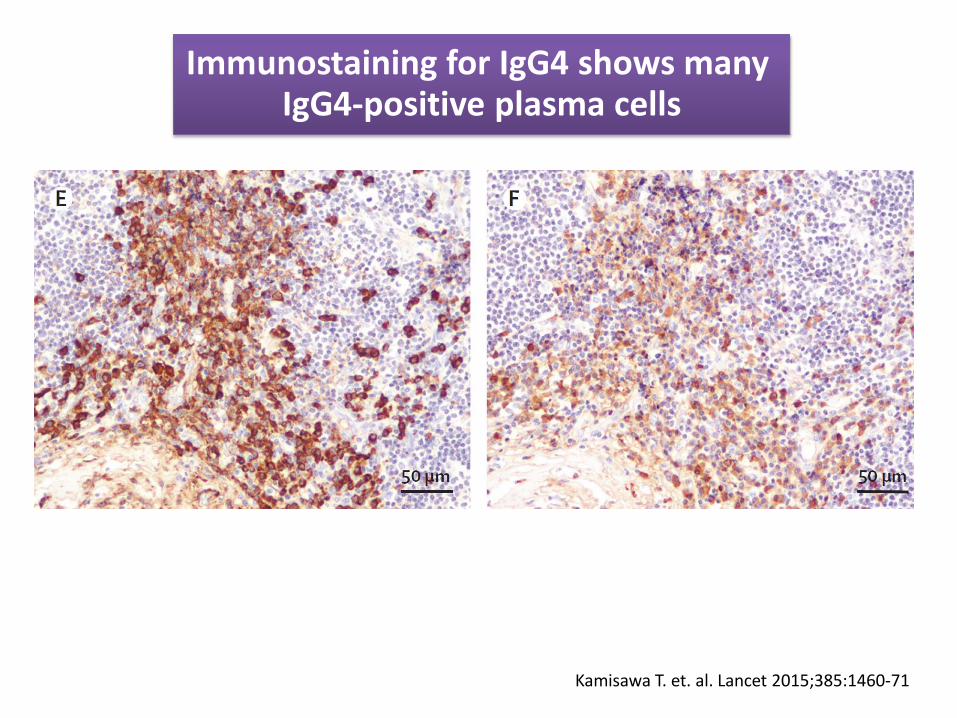
Immunostaining for IgG4 shows many IgG4-positive plasma cells
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47
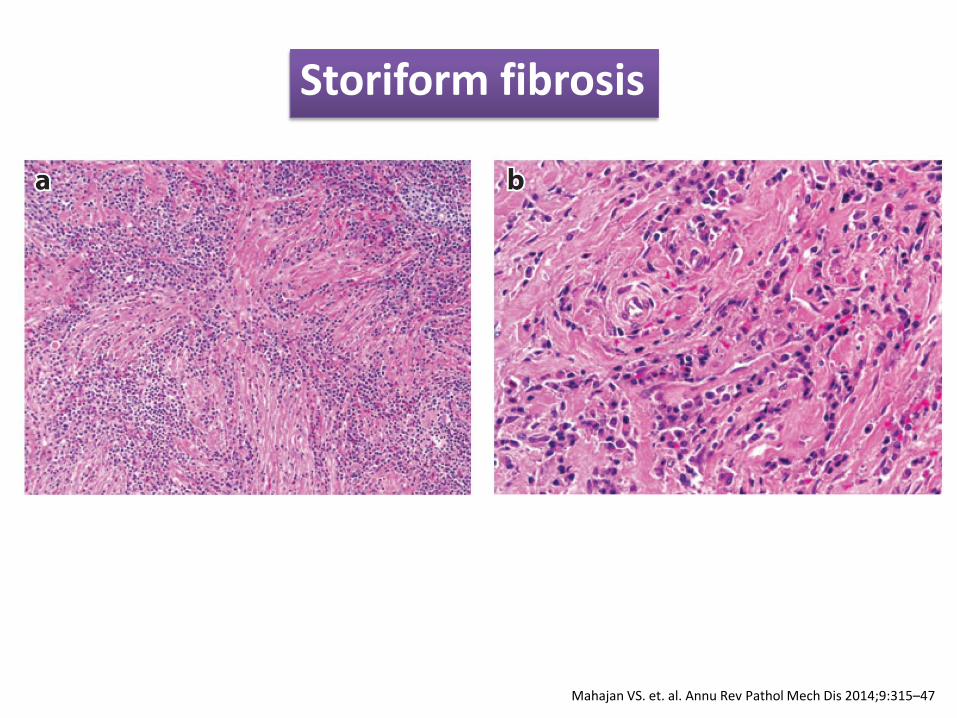
Storiform fibrosis
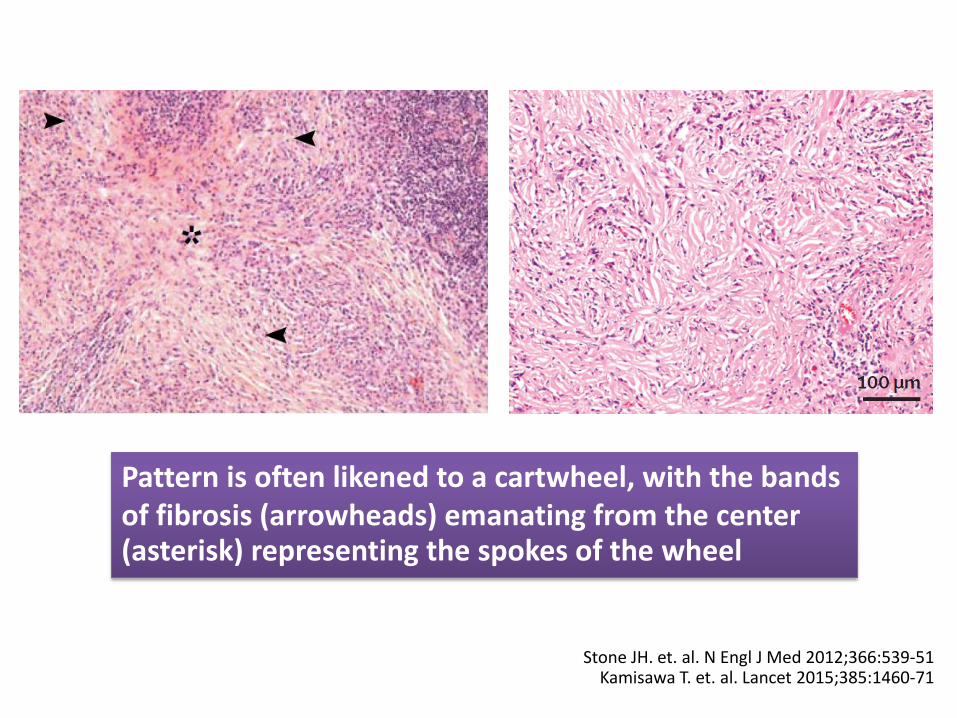
Stone JH. et. al. N Engl J Med 2012;366:539-51 Kamisawa T. et. al. Lancet 2015;385:1460-71
Pattern is often likened to a cartwheel, with the bands of fibrosis (arrowheads) emanating from the center (asterisk) representing the spokes of the wheel
Histopathology
• Presence of significant IgG4+ plasma cell infiltrates in biopsy specimens is not specific for IgG4-RD
• Common mimickers of IgG4-RD, including malignancy, granulomatosis with polyangiitis, eosinophilic granulomatosis with polyangiitis, and multicentric Castleman’s disease
• Findings of storiform fibrosis and obliterative phlebitis heighten diagnostic specificity, but clinicopathologic correlation is always essential
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Histopathology
• Needle biopsies are usually insufficient for diagnosis of IgG4-RD
• Storiform fibrosis might not be detected; hence, use of en-bloc biopsy is recommended
• However, needle biopsy generally use to exclude malignancy with some confidence
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
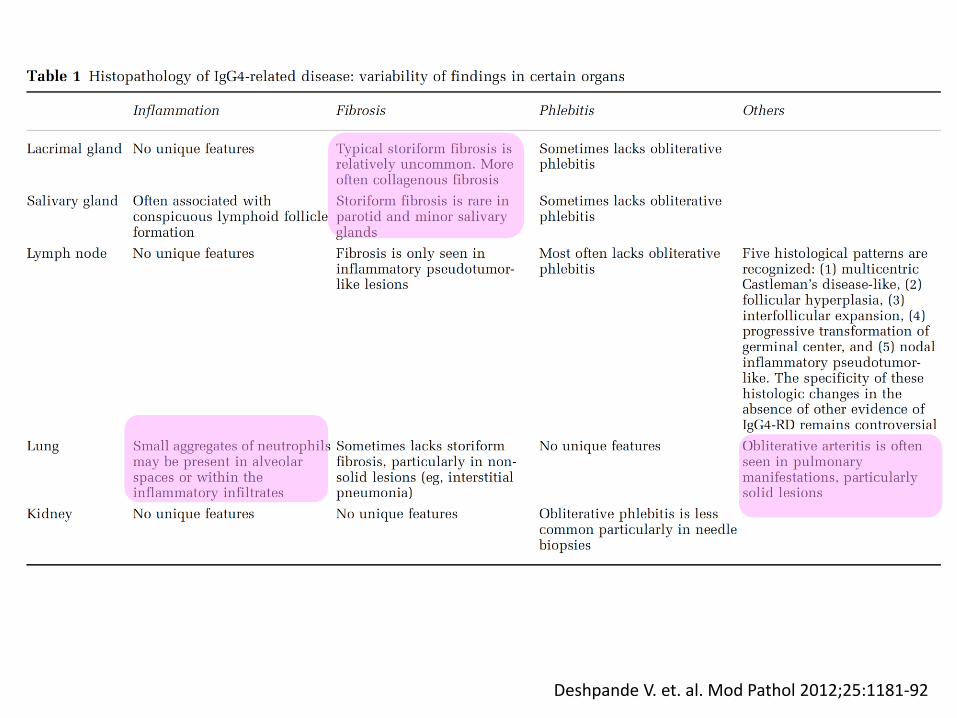
Deshpande V. et. al. Mod Pathol 2012;25:1181-92
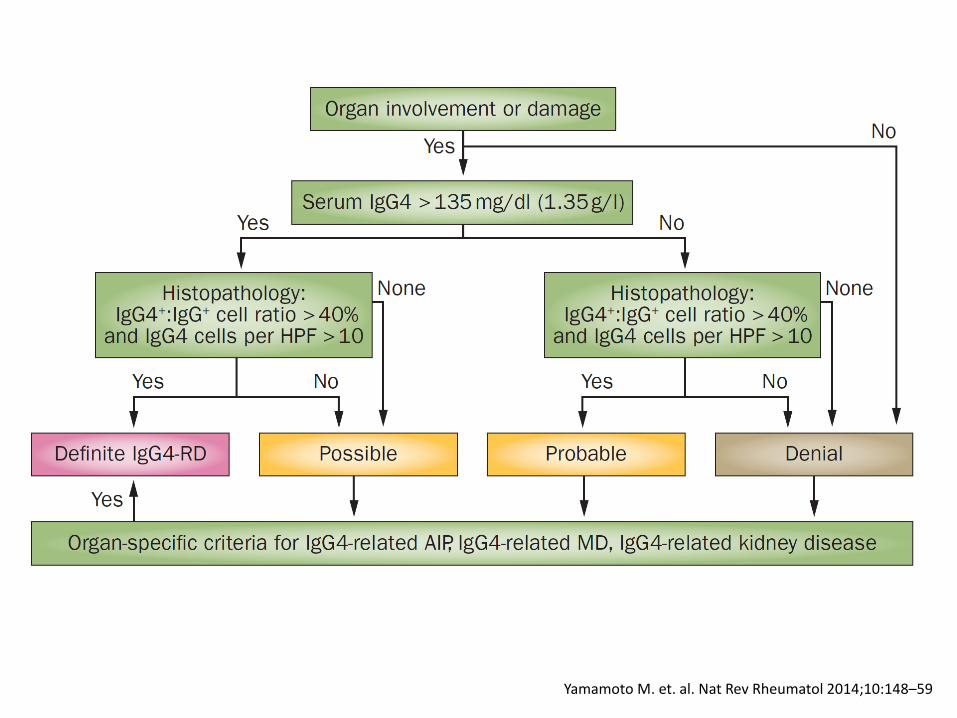
Diagnosis
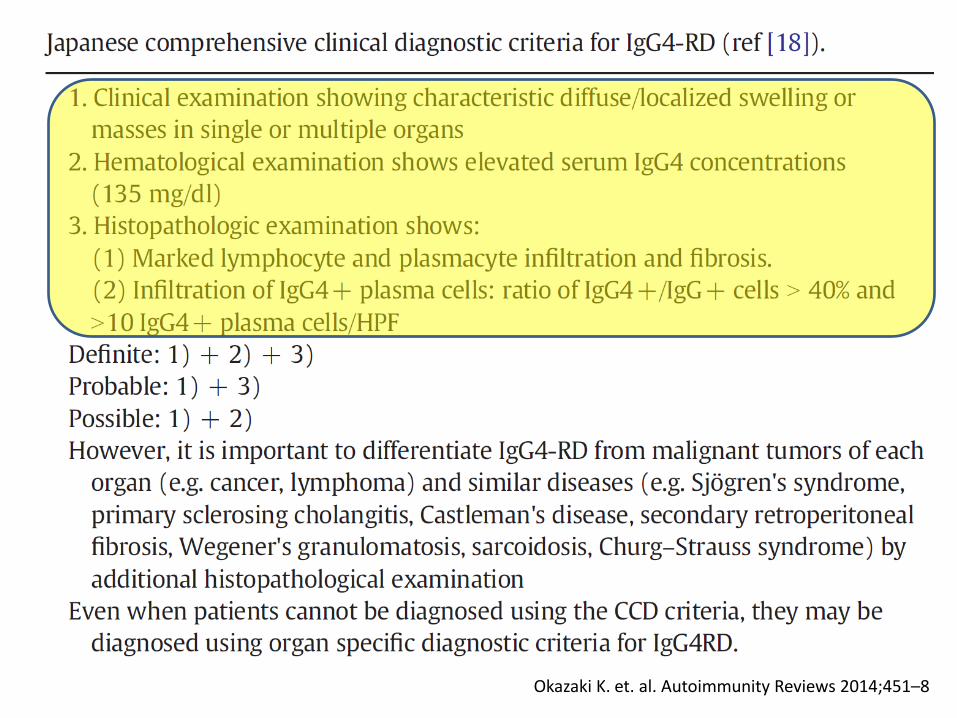
Okazaki K. et. al. Autoimmunity Reviews 2014;451–8
Umehara H. et. al. Mod Rheumatol 2012;22:21–30 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
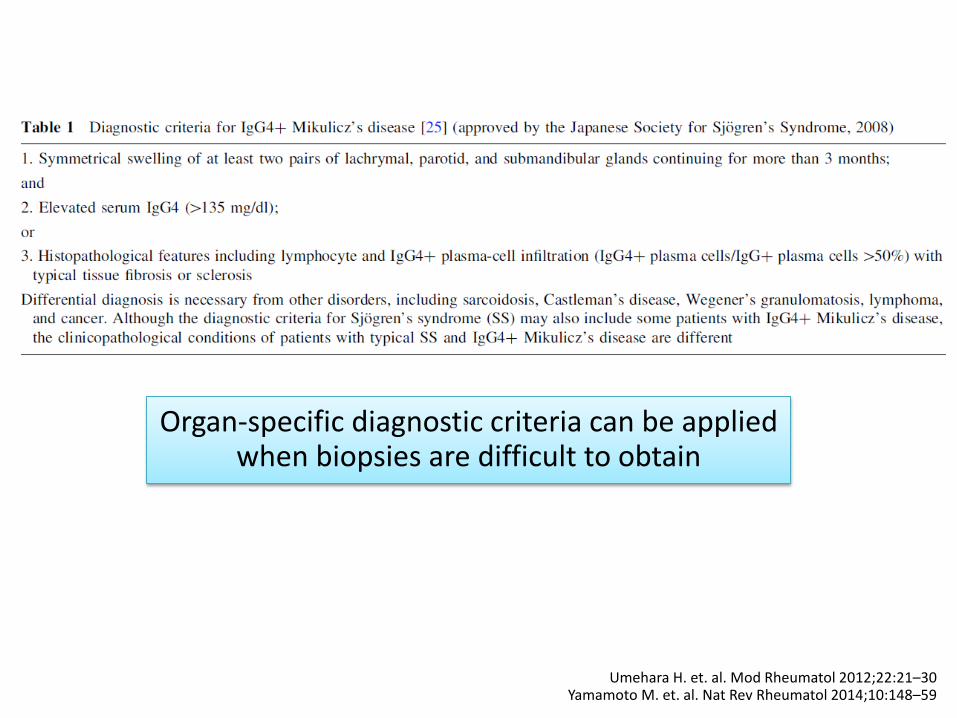
Organ-specific diagnostic criteria can be applied when biopsies are difficult to obtain
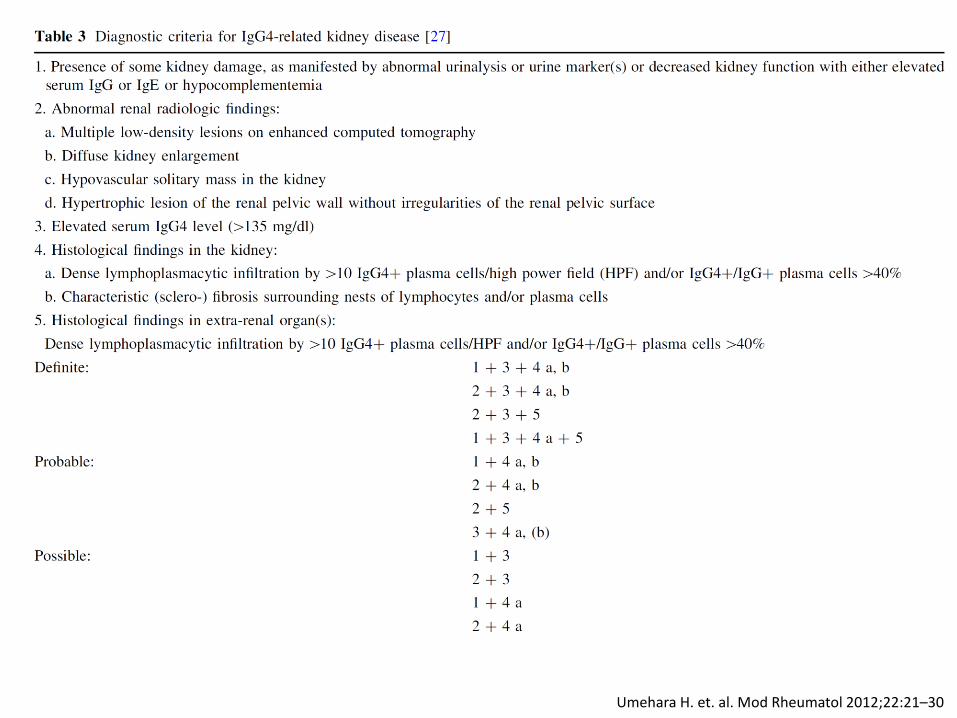
Umehara H. et. al. Mod Rheumatol 2012;22:21–30
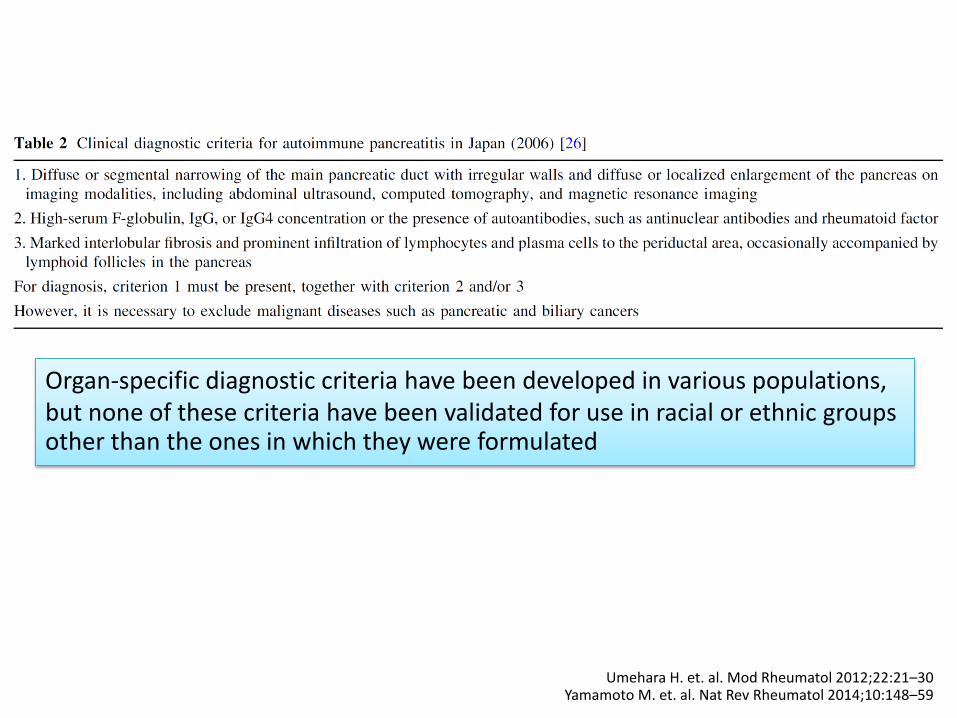
Umehara H. et. al. Mod Rheumatol 2012;22:21–30 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Organ-specific diagnostic criteria have been developed in various populations, but none of these criteria have been validated for use in racial or ethnic groups other than the ones in which they were formulated
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Outline
• Introduction
• Historical context
• Pathogenesis
• Epidemiology
• Clinical manifestations and laboratory findings
• Treatment and prognosis
Major aim of treatment
• Prevention of fibrosis and its potentially destructive impact on organs
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Treatment
• Not all manifestations of IgG4-RD require immediate treatment
• “Watchful waiting” may be appropriate, for example, in patients with asymptomatic lymphadenopathy or mild submandibular gland enlargement
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Treatment
• Spontaneous remissions or temporary remissions without treatment have been reported, but follow-up in such cases was short and a relapsing-remitting pattern with progressive organ injury has been well-described
• Further, metachronous nature of IgG4-RD suggests that although disease may appear to improve at least temporarily in one organ, it may re-emerge months or years later at a different site
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Treatment
• Treatment leads to faster and more complete remission with fewer long-term complications of IgG4-RD than does waiting to treat
• Treatment is therefore justified in most cases in which laboratory evidence or radiology studies suggest organ dysfunction
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Treatment
Multiple approaches have been reported,
• Systemic glucocorticoid
• “Steroid-sparing” immunosuppressive drugs
• Biologic agents
• Surgical resection of affected tissues
But no randomized clinical trials or formal treatment guidelines exist
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Kamisawa T. et. al. J Gastroenterol 2014;49:961–70 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
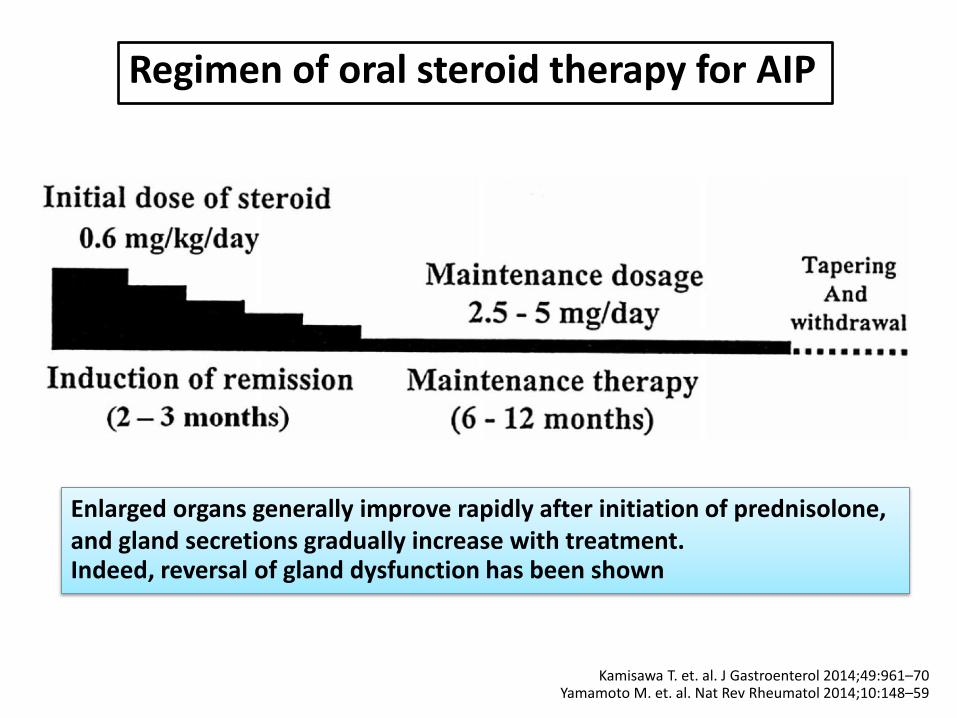
Regimen of oral steroid therapy for AIP
Enlarged organs generally improve rapidly after initiation of prednisolone, and gland secretions gradually increase with treatment. Indeed, reversal of gland dysfunction has been shown
Maintenance therapy In an effort to minimize morbidity, those with organ-threatening IgG4-RD manifestations and patients at elevated risk of relapse likely benefit from maintenance therapy Higher risk for recurrence following remission induction • Multi-organ disease • Significantly elevated serum IgG4 concentrations • Involvement of proximal bile ducts • History of disease relapse Optimal duration of maintenance therapy has not been studied
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Maintenance therapy
• Relapses in IgG4-RD patients are common, even with the use of glucocorticoid maintenance therapy
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Hart PA, et al. Gut 2013;62:1607–15 Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
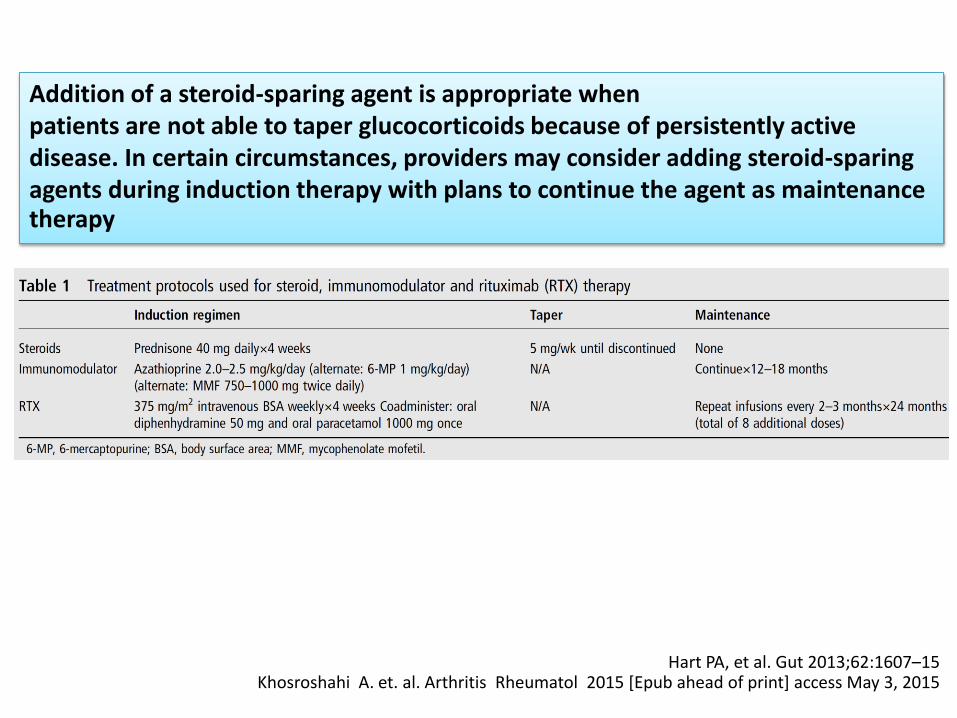
Addition of a steroid-sparing agent is appropriate when patients are not able to taper glucocorticoids because of persistently active disease. In certain circumstances, providers may consider adding steroid-sparing agents during induction therapy with plans to continue the agent as maintenance therapy
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47
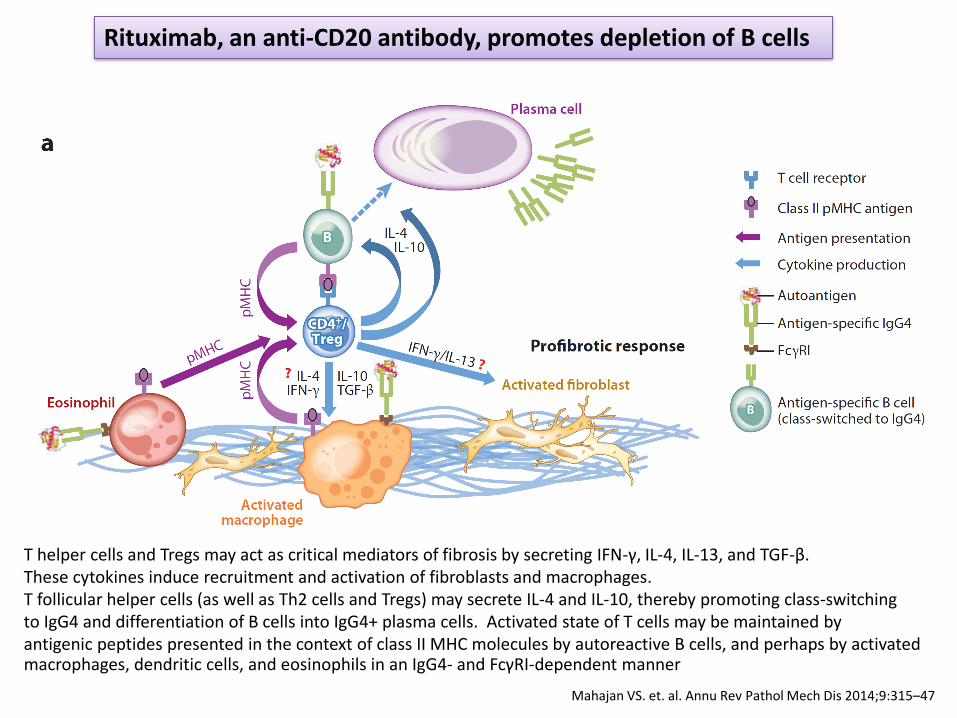
Rituximab, an anti-CD20 antibody, promotes depletion of B cells
T helper cells and Tregs may act as critical mediators of fibrosis by secreting IFN-γ, IL-4, IL-13, and TGF-β. These cytokines induce recruitment and activation of fibroblasts and macrophages. T follicular helper cells (as well as Th2 cells and Tregs) may secrete IL-4 and IL-10, thereby promoting class-switching to IgG4 and differentiation of B cells into IgG4+ plasma cells. Activated state of T cells may be maintained by antigenic peptides presented in the context of class II MHC molecules by autoreactive B cells, and perhaps by activated macrophages, dendritic cells, and eosinophils in an IgG4- and FcγRI-dependent manner
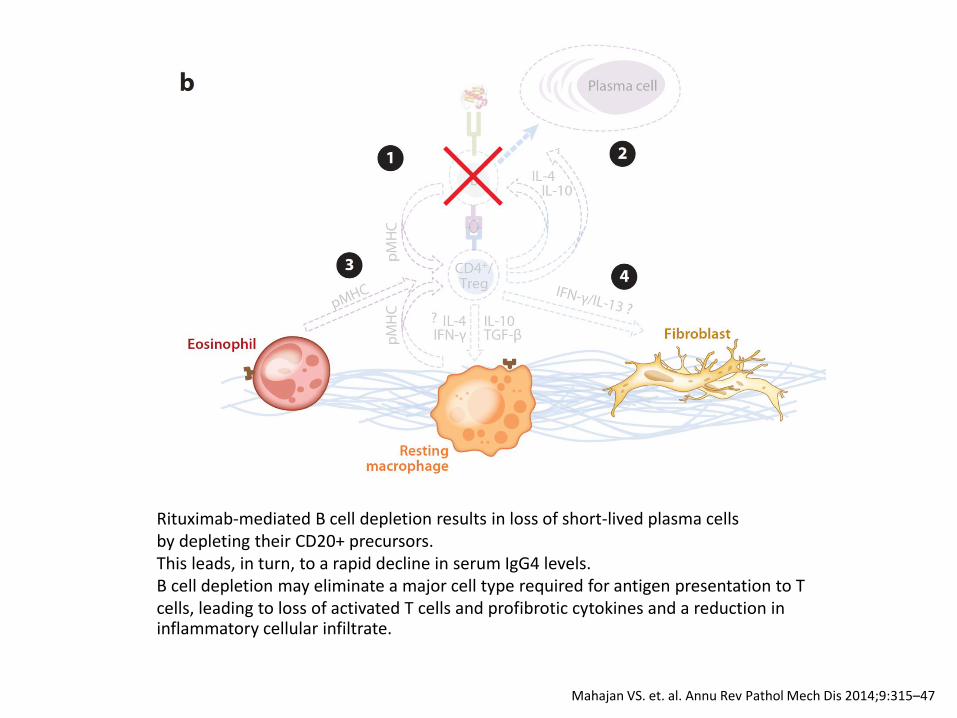
Mahajan VS. et. al. Annu Rev Pathol Mech Dis 2014;9:315–47
Rituximab-mediated B cell depletion results in loss of short-lived plasma cells by depleting their CD20+ precursors. This leads, in turn, to a rapid decline in serum IgG4 levels. B cell depletion may eliminate a major cell type required for antigen presentation to T cells, leading to loss of activated T cells and profibrotic cytokines and a reduction in inflammatory cellular infiltrate.
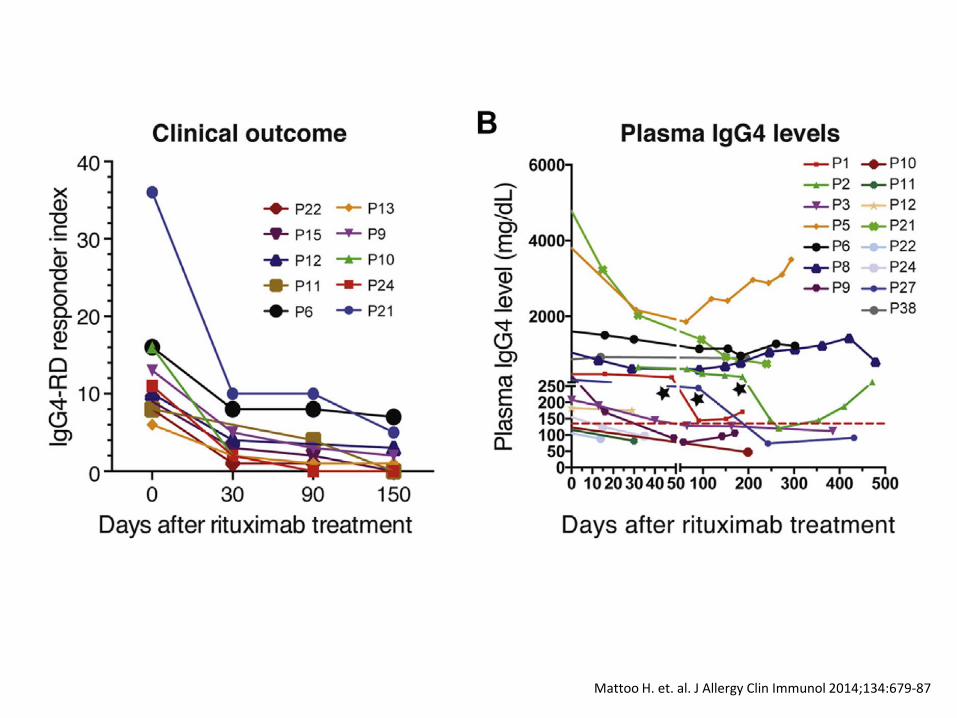
Mattoo H. et. al. J Allergy Clin Immunol 2014;134:679-87
Mattoo H. et. al. J Allergy Clin Immunol 2014;134:679-87
IgG4-RD Responder Index (RI)
• Quantitative means of assessing overall disease response to treatment
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
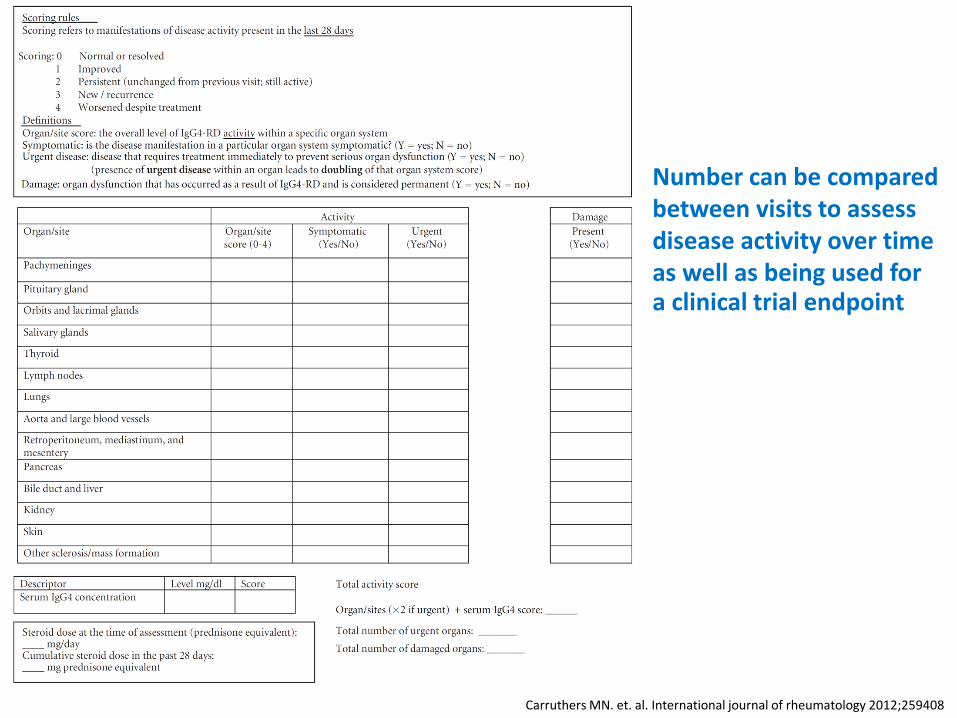
Carruthers MN. et. al. International journal of rheumatology 2012;259408
Number can be compared between visits to assess disease activity over time as well as being used for a clinical trial endpoint
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Highly Fibrotic Lesions
• Long-standing, highly fibrotic lesions may respond poorly if at all to currently available pharmacologic agents
• In such patients, risk-benefit balance may not favor repeated courses of treatment
• Surgical debulking is an option, but suitability of surgical interventions is governed by anatomic regions and adjacent structures involved
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Prognosis
• Although initial prognosis of patients with IgG4-RD is generally good, relapse ratio after tapering or discontinuing steroids is very high
• Around half of patients treated for IgG4-related dacryoadenitis and sialadenitis who relapse present with new lesions in different organs during both short-term and long-term (>10 years) follow-up
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Inoue D. et. al. Medicine (Baltimore) 2015;94:e680 Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
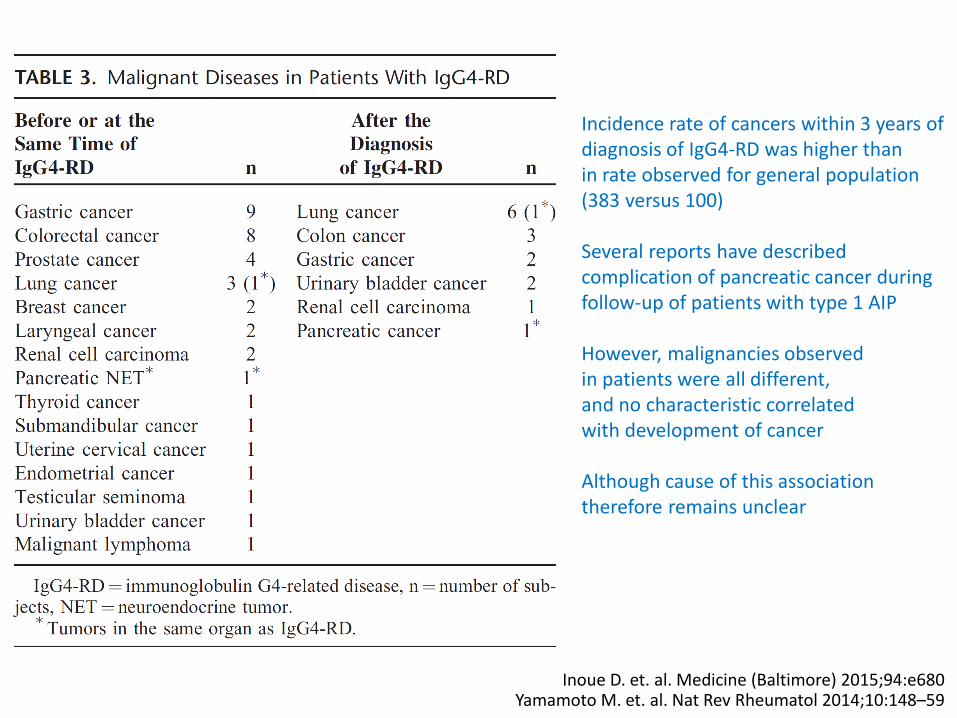
Incidence rate of cancers within 3 years of diagnosis of IgG4-RD was higher than in rate observed for general population (383 versus 100) Several reports have described complication of pancreatic cancer during follow-up of patients with type 1 AIP However, malignancies observed in patients were all different, and no characteristic correlated with development of cancer Although cause of this association therefore remains unclear
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
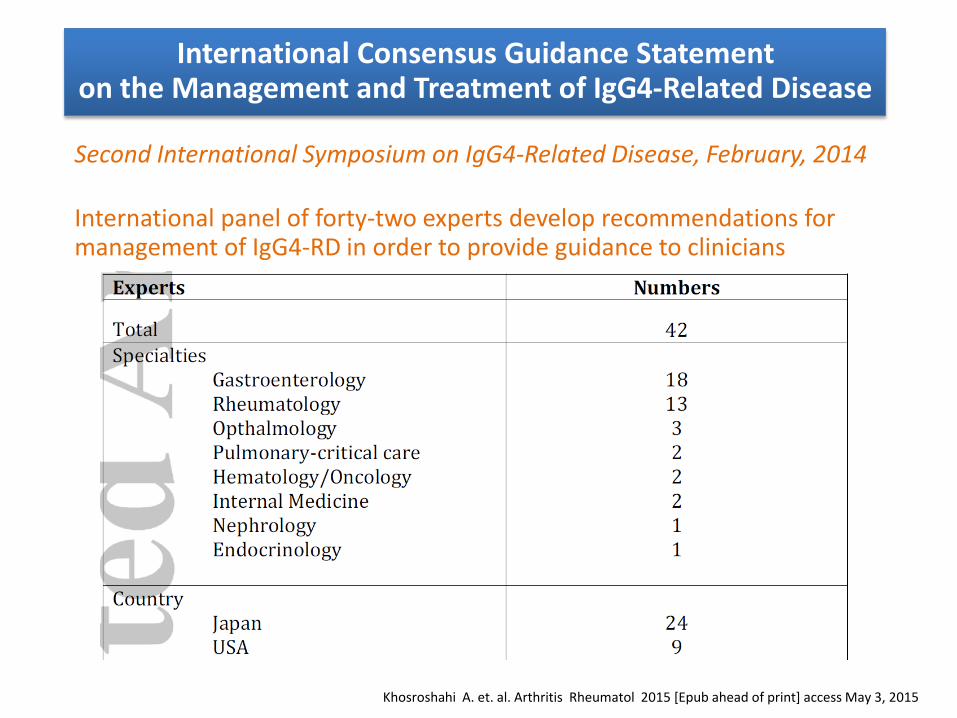
International Consensus Guidance Statement on the Management and Treatment of IgG4-Related Disease
Second International Symposium on IgG4-Related Disease, February, 2014 International panel of forty-two experts develop recommendations for management of IgG4-RD in order to provide guidance to clinicians
Patient Evaluation
• Most accurate assessment of IgG4-RD is based on a full clinical history, physical examination, selected laboratory investigations, and appropriate radiology studies (96% agreement)
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Clinicopathologic correlation is required to make correct diagnosis
Tissue Confirmation Prior to Treatment
• Diagnostic confirmation by biopsy is strongly recommended for exclusion of malignancies and other IgG4-RD mimics
(94% agreement)
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Indications for Therapy
• All patients with symptomatic, active IgG4-RD require treatment, some urgently.
A subset of patients with asymptomatic
IgG4-RD also requires treatment
(87% agreement)
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Remission Induction With Glucocorticoids
• Glucocorticoids are the first-line agent for remission induction in all patients with active, untreated IgG4-RD unless contraindications to such treatment are present
(94% agreement)
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Use of Steroid-Sparing Agents
• Some but not all patients require combination of glucocorticoids and a steroid-sparing immunosuppressive agent from the start of treatment
• This is because glucocorticoid monotherapy will ultimately fail to control disease and long-term glucocorticoid toxicities pose a high risk to patients
(46% agreement)
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Use of Maintenance Therapy Following Remission Induction
• Following a successful course of induction therapy, certain patients benefit from maintenance therapy
(94% agreement)
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Managing Disease Relapse
• Re-treatment with glucocorticoids is indicated in patients who relapse off of treatment following successful remission induction
• Following relapse, introduction of a steroid-sparing agent for continuation in remission maintenance period should be considered (81% agreement)
Khosroshahi A. et. al. Arthritis Rheumatol 2015 [Epub ahead of print] access May 3, 2015
Take home message (1)
• IgG4-RD represents a chronic inflammatory disorder characterized by various systemic organ dysfunctions
• Disease is associated with elevated serum levels of IgG4 and specific histopathological features, including abundant IgG4+ plasmacyte infiltration, storiform fibrosis and obliterative phlebitis
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Take home message (2)
• Associated with a predominantly type 2 T-helper-cell cytokine profile, and infiltration of regulatory T cells
• Examination for systemic organ failure and screening for underlying malignancies is important during the diagnosis and follow-up of IgG4-related disease
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Take home message (3)
• Glucocorticoids are effective in the treatment of IgG4-related disease, but the rate of relapse after tapering or discontinuing glucocorticosteroids is high
Yamamoto M. et. al. Nat Rev Rheumatol 2014;10:148–59
Thank you for your attention





























