Embed Size (px)
Citation preview
Document of
The World Bank
Report No: ICR2610
IMPLEMENTATION COMPLETION AND RESULTS REPORT(TF-090182)
ON A
TRUST FUND
IN THE AMOUNT OF EURO 13.45 MILLION(US$ 17.5 MILLION EQUIVALENT)
TO THE
REPUBLIC OF THE PHILIPPINES
FOR A
EC-TF FOR HEALH SECTOR REFORM
April 26, 2013
Human Development DepartmentEast Asia and the Pacific Region
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
CURRENCY EQUIVALENTS
(Exchange Rate Effective October 10, 2012)
Currency Unit = Philippine Peso (PhP)US$ 1.00 = 42.64 PhP
FISCAL YEARJanuary 1 - December 31
ABBREVIATIONS AND ACRONYMS
AOP Annual Operations PlanARMM Autonomous Region in Muslim MindanaoBEmONC Basic Emergency Obstetric and Newborn CareBnB Botika ng BarangaysCAS Country Assistance StrategyCBMS Community-Based Monitoring SystemCEmONC Comprehensive Emergency Obstetric and Newborn CareCHD Center for Health DevelopmentCOA Commission on AuditCPR Contraceptive Prevalence RateDBM Department of Budget and ManagementDENR Department Environment and Natural ResourcesDLI Disbursement Linked IndicatorsDOH Department of HealthDPT3 Diphteria, Pertussis, and TetanusDSWD Department of Social Welfare and DevelopmentEC European CommissioneNGAS Electronic National Government Accounting SystemEPI Expanded Program on ImmunizationFl Fourmula One for HealthFDA Food and Drug AdministrationFHSIS Field Health Services Information SystemHSEF Health Sector Expenditure FrameworkHSRA Health Sector Reform AgendaHSRP Fl for Health Program - Health Sector Reform ProgramILHZ Inter-Local Health ZonesIP Indigent ProgramIPs Indigenous PeoplesIPPF Indigenous People's Policy FrameworkISR Implementation Status ReportJAC Joint Appraisal CommitteeJAPI Joint Assessment and Planning InitiativeLGUs Local Government Units
M&E Monitoring and EvaluationMDGs Millennium Development GoalsNDHS National Demographic and Health SurveyNHIP National Health Insurance ProgramNHTS National Household Targeting SystemNHTS-PR National Household Targeting System - Poverty ReductionNOH National Objectives for HealthNPS National Program SupportNSSHRP National Sector Support for Health Sector Reform ProjectOOP Out-of-PocketPDO Project Development ObjectivesPEFA Public Expenditure and Financial AccountabilityPFM Public Financial ManagementPHIC Philippine Health Insurance CorporationPhP Philippine PesoPIPH Province-wide Investment Plans for HealthRHU Rural Health UnitsSDAH Sector Development Approach for HealthSLA Service Level AgreementsTB TuberculosisTHE Total Health ExpendituresUHC Universal Health Care
Vice President: Axel van Trotsenburg
Country Director: Motoo Konishi
Sector Manager: Toomas Palu
Project Team Leader: Roberto Rosadia
ICR Team Leader: Eileen Brainne Sullivan

PHILIPPINESEC-TF FOR HEALH SECTOR REFORM
CONTENTS
Data SheetA. Basic InformationB. Key DatesC. Ratings SummaryD. Sector and Theme CodesE. Bank StaffF. Results Framework AnalysisG. Ratings of Project Performance in ISRsH. RestructuringI. Disbursement Graph
1. Project Context, Development Objectives and Design...................... 12. Key Factors Affecting Implementation and Outcomes .......... 5.......53. Assessment of Outcomes ........................................... 114. Assessment of Risk to Development Outcome. .................... ..... 185. Assessment of Bank and Recipient Performance ........................... 186. Lessons Learned ..................................... ......... 227. Comments on Issues Raised by Recipient/Implementing Agencies/Partners ..... 24Annex 1. Project Costs and Financing ................................. 26Annex 2. Outputs by Component ............................... ..... 27Annex 3. Economic and Financial Analysis ............................. 31Annex 4. Bank Lending and Implementation Support/Supervision Processes ...... 32Annex 5. Beneficiary Survey Results................................. 33Annex 6. Stakeholder Workshop Report and Results......................... 34Annex 7. Summary of Recipient's ICR and/or Comments on Draft ICR .... ..... 35Annex 8. Comments of Cofinanciers and Other Partners/Stakeholders . .......... 36Annex 9. List of Supporting Documents .......................... ..... 37MAP
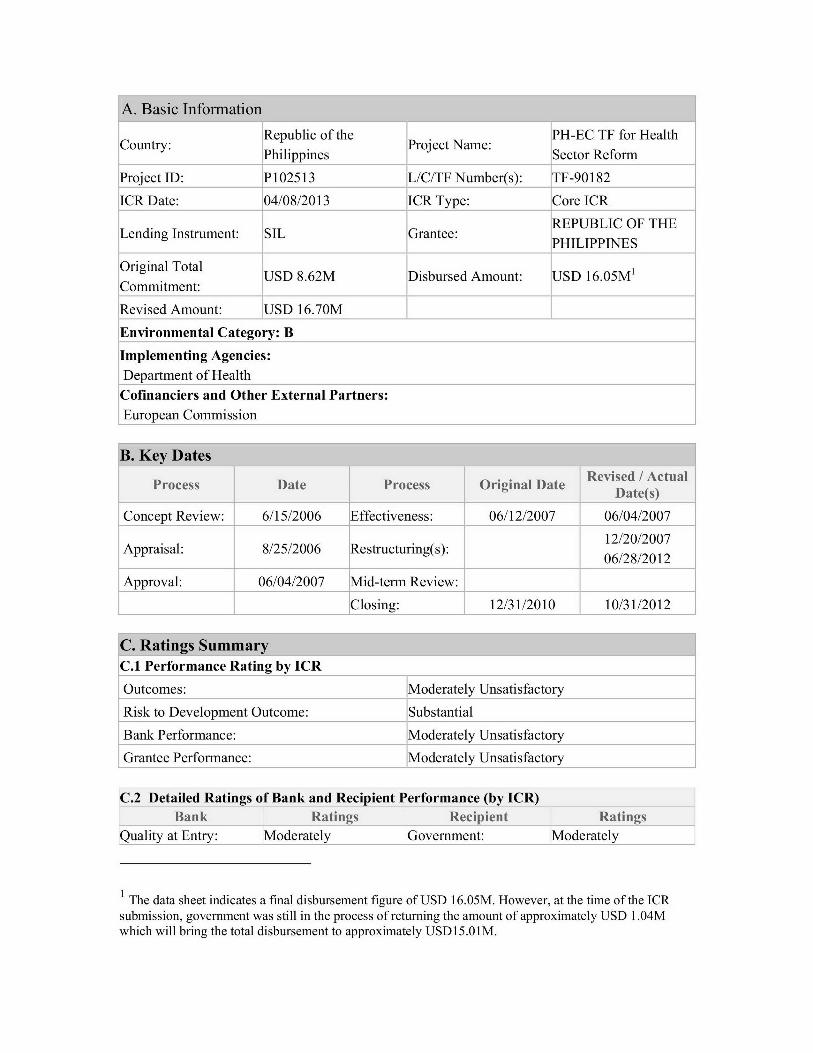
A. Basic Information
Republic of the PH-EC TF for HealthPhilippines Sector Reform
Project ID: P102513 L/C/TF Number(s): TF-90182
ICR Date: 04/08/2013 ICR Type: Core ICR
REPUBLIC OF THELending Instrument: SIL Grantee: PHILIPPNES
Original Total USD 8.62M Disbursed Amount: USD 16.05M'Commitment:
Revised Amount: USD 16.70M
Environmental Category: B
Implementing Agencies:Department of Health
Cofinanciers and Other External Partners:European Commission
JB. Key DatesRevised / ActualProcess Date Process Original DateDaes
Concept Review: 6/15/2006 Effectiveness: 06/12/2007 06/04/2007
12/20/2007Appraisal: 8/25/2006 Restructuring(s): 12/202
06/28/2012
Approval: 06/04/2007 Mid-term Review:
Closing: 12/31/2010 10/31/2012
C. Ratings SummaryC.1 Performance Rating by ICR
Outcomes: Moderately Unsatisfactory
Risk to Development Outcome: Substantial
Bank Performance: Moderately Unsatisfactory
Grantee Performance: Moderately Unsatisfactory
C.2 Detailed Ratings of Bank and Recipient Performance (by ICR)Bank Ratings Recipient Ratings
uality at Entry: Moderately overnment: Moderately
The data sheet indicates a final disbursement figure of USD 16.05M. However, at the time of the ICRsubmission, government was still in the process of returning the amount of approximately USD 1.04Mwhich will bring the total disbursement to approximately USD15.01 M.
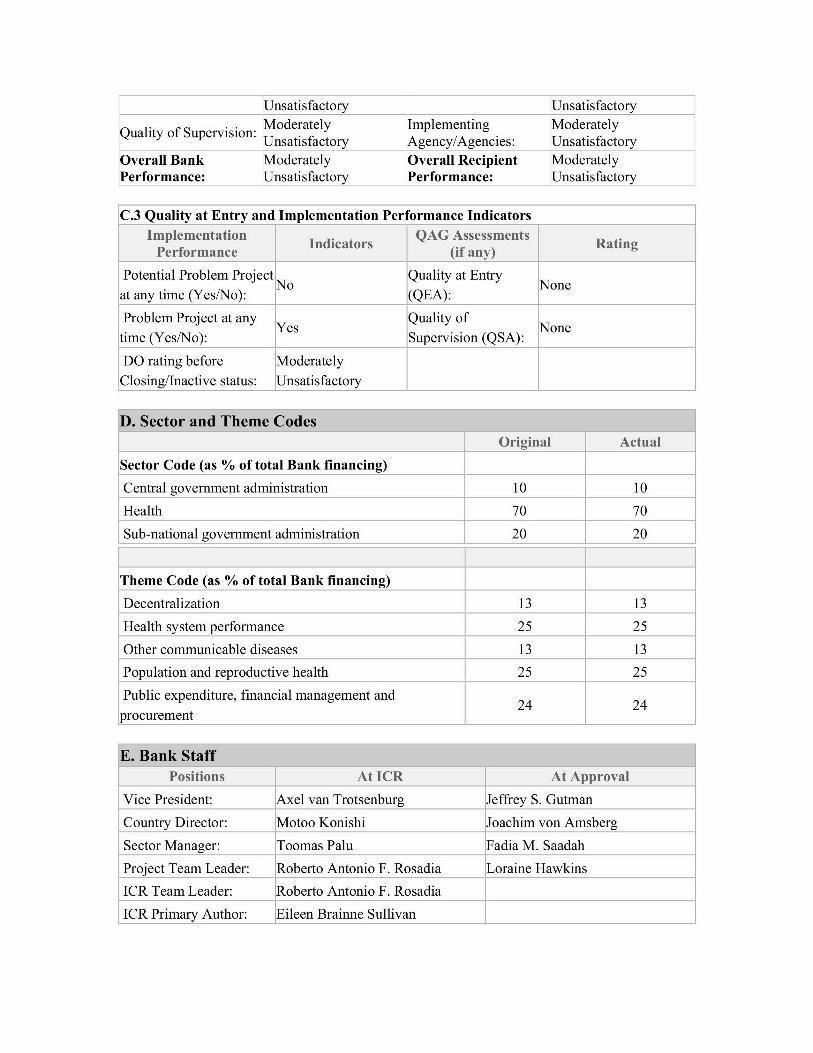
Unsatisfactory Unsatisfactory
i . Moderately Implementing ModeratelyUnsatisfactory Agency/Agencies: Unsatisfactory
Overall Bank Moderately Overall Recipient ModeratelyPerformance: Unsatisfactory Performance: Unsatisfactory
C.3 Quality at Entry and Implementation Performance Indicators
Implementation Indicators QAG Assessments RatingPerformance (if any)
Potential Problem Project Quality at EntryNo Noneat any time (Yes/No): (QEA):
Problem Project at any Yes Quality of Nonetime (Yes/No): Supervision (QSA):
DO rating before Moderately
Closing/Inactive status: Unsatisfactory
D. Sector and Theme CodesOriginal Actual
Sector Code (as % of total Bank financing)
Central government administration 10 10
Health 70 70
Sub-national government administration 20 20
Theme Code (as % of total Bank financing)
Decentralization 13 13
Health system performance 25 25
Other communicable diseases 13 13
Population and reproductive health 25 25
Public expenditure, financial management and 24 24procurement
E. Bank StaffPositions At ICR At Approval
Vice President: Axel van Trotsenburg Jeffrey S. Gutman
Country Director: Motoo Konishi Joachim von Amsberg
Sector Manager: Toomas Palu Fadia M. Saadah
Project Team Leader: Roberto Antonio F. Rosadia Loraine Hawkins
ICR Team Leader: Roberto Antonio F. Rosadia
ICR Primary Author: Eileen Brainne Sullivan
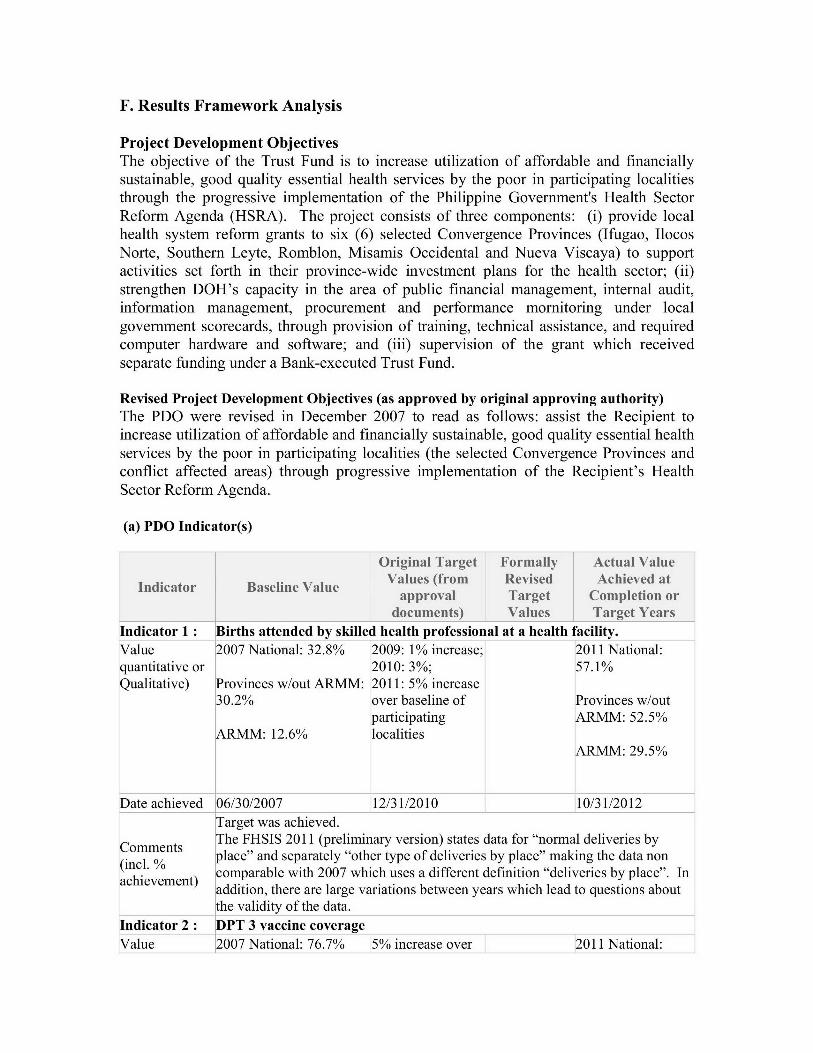
F. Results Framework Analysis
Project Development ObjectivesThe objective of the Trust Fund is to increase utilization of affordable and financiallysustainable, good quality essential health services by the poor in participating localitiesthrough the progressive implementation of the Philippine Government's Health SectorReform Agenda (HSRA). The project consists of three components: (i) provide localhealth system reform grants to six (6) selected Convergence Provinces (Ifugao, IlocosNorte, Southern Leyte, Romblon, Misamis Occidental and Nueva Viscaya) to supportactivities set forth in their province-wide investment plans for the health sector; (ii)strengthen DOH's capacity in the area of public financial management, internal audit,information management, procurement and performance mornitoring under localgovernment scorecards, through provision of training, technical assistance, and requiredcomputer hardware and software; and (iii) supervision of the grant which receivedseparate funding under a Bank-executed Trust Fund.
Revised Project Development Objectives (as approved by original approving authority)The PDO were revised in December 2007 to read as follows: assist the Recipient toincrease utilization of affordable and financially sustainable, good quality essential healthservices by the poor in participating localities (the selected Convergence Provinces andconflict affected areas) through progressive implementation of the Recipient's HealthSector Reform Agenda.
(a) PDO Indicator(s)
Original Target Formally Actual ValueValues (from Revised Achieved at
approval Target Completion ordocuments) Values Target Years
Indicator 1 : Births attended by skilled health professional at a health facility.Value 2007 National: 32.8% 2009: 1% increase; 2011 National:quantitative or 2010: 3%; 57.1%Qualitative) Provinces w/out ARMM: 2011: 5% increase
30.2% over baseline of Provinces w/outparticipating ARMM: 52.5%
ARMM: 12.6% localitiesARMM: 29.5%
[Date achieved 106/30/2007 12/31/2010 10/31/2012Target was achieved.The FHSIS 2011 (preliminary version) states data for "normal deliveries by
Cmn ts. % place" and separately "other type of deliveries by place" making the data nonav. e comparable with 2007 which uses a different definition "deliveries by place". In
addition, there are large variations between years which lead to questions aboutthe validity of the data.
Indicator 2 : ]DPT 3 vaccine coverageValue 2007 National: 76.7% 5% increase over 2011 National:
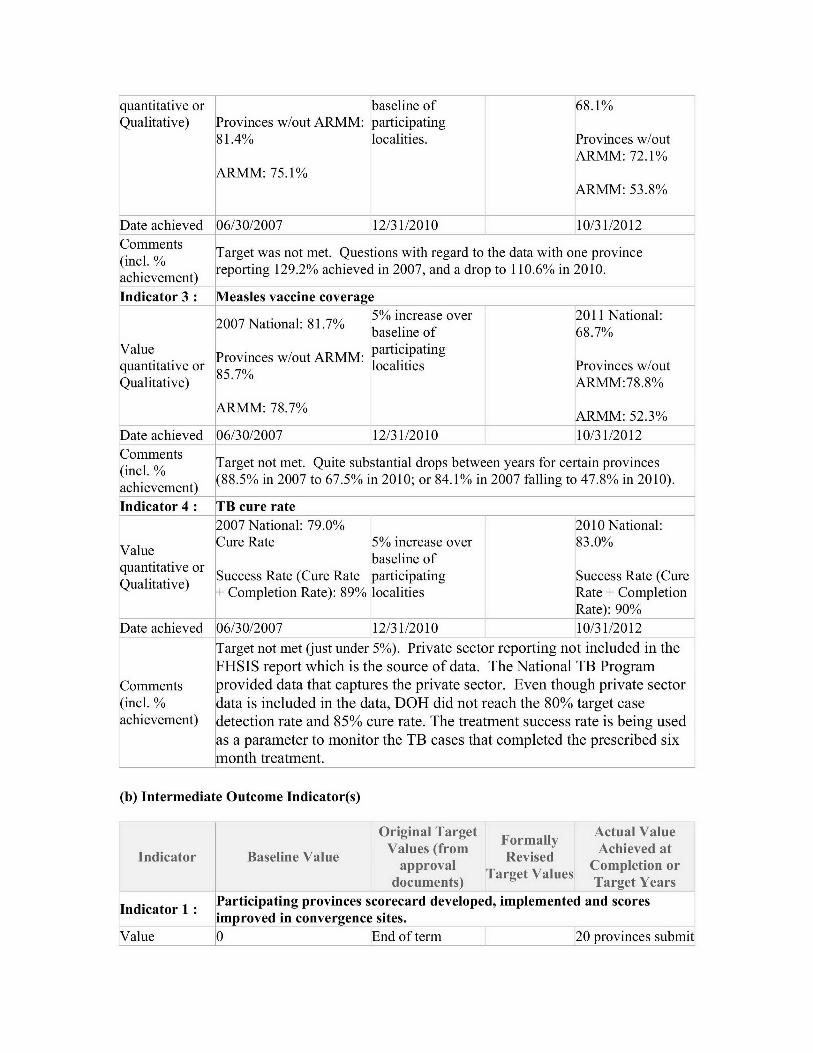
quantitative or baseline of 68.1%Qualitative) Provinces w/out ARMM: participating
81.4% localities. Provinces w/outARMM: 72.1%
ARMM: 75.1%ARMM: 53.8%
Date achieved 06/30/2007 12/31/2010 10/31/2012Comments Target was not met. Questions with regard to the data with one province(incl. %Iac. reporting 129.2% achieved in 2007, and a drop to 110.6% in 2010.achievement)
Indicator 3 : Measles vaccine coverage5% increase over 2011 National:
2007 National: 81.7% baeieo.87baseline of 68.7%Value . participatingquantitative or 85v7% localities Provinces w/outQualitative) ARMM:78.8%
ARMM: 78.7% ARMM: 52.3%
[Date achieved 106/30/2007 12/31/2010 10/31/2012Comments Target not met. Quite substantial drops between years for certain provinces
ac. t (88.5% in 2007 to 67.5% in 2010; or 84.1% in 2007 falling to 47.8% in 2010).achievement)Indicator 4 : ITB cure rate
2007 National: 79.0% 2010 National:
Value Cure Rate 5% increase over 83.0%. baseline of
quantitative orbaeieoQuanitativer Success Rate (Cure Rate participating Success Rate (Cure
+ Completion Rate): 89% localities Rate + CompletionRate): 90%
Date achieved 06/30/2007 12/31/2010 10/31/2012
Target not met (just under 5%). Private sector reporting not included in the
FHSIS report which is the source of data. The National TB ProgramComments provided data that captures the private sector. Even though private sector(incl. % data is included in the data, DOH did not reach the 80% target caseachievement) detection rate and 85% cure rate. The treatment success rate is being used
as a parameter to monitor the TB cases that completed the prescribed sixmonth treatment.
(b) Intermediate Outcome Indicator(s)
Original Target Actual ValueFormallyromAchieved at
Indicator Baseline Value Values (from Revised cmpletapproval Completion or
documents) Target YearsParticipating provinces scorecard developed, implemented and scoresImproved in convergence sites.
Value 0 End of term 20 provinces submit
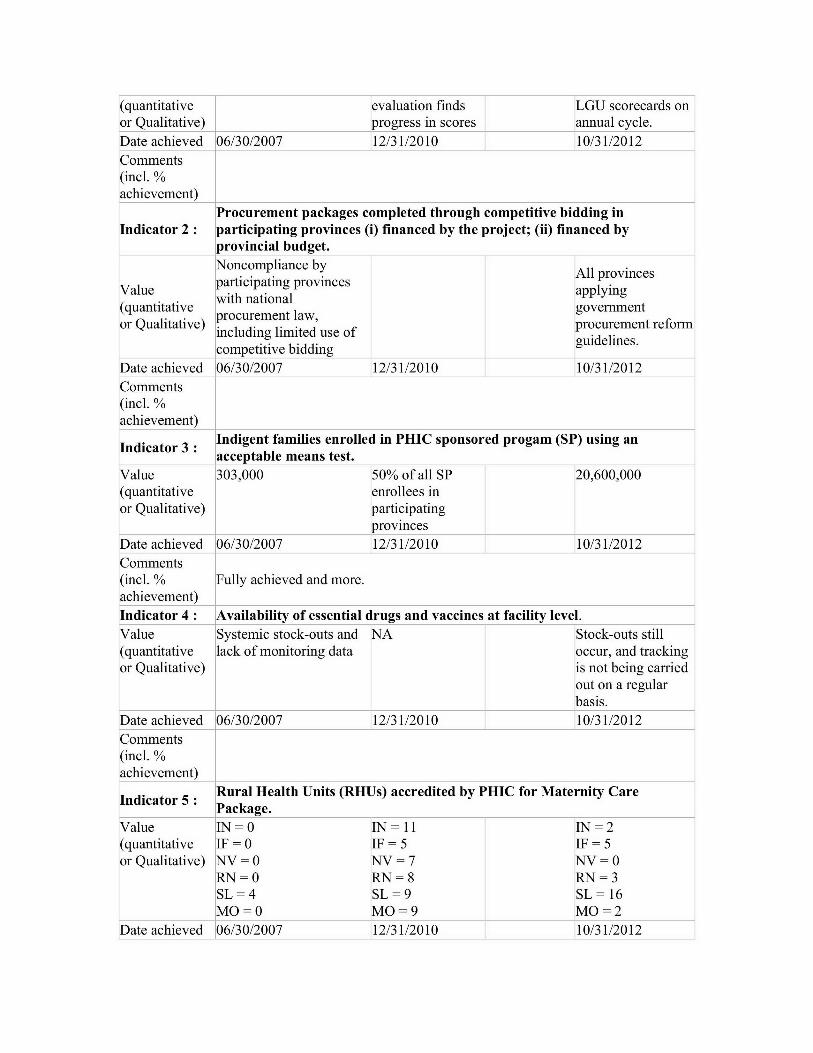
(quantitative evaluation finds LGU scorecards onor Qualitative) progress in scores annual cycle.Date achieved 06/30/2007 12/31/2010 10/31/2012Comments(incl. %achievement)
Procurement packages completed through competitive bidding inIndicator 2: participating provinces (i) financed by the project; (ii) financed by
provincial budget.Noncompliance by All provinces
Value participating provinces applyingwith national
(quantitative government.procurement law,
or Qualitative) . .a.,'procurement reformincluding limited use of guidelines.competitive bidding
Date achieved 06/30/2007 12/31/2010 10/31/2012Comments(incl. %achievement)
Indicator 3 : Indigent families enrolled in PHIC sponsored progam (SP) using anacceptable means test.
Value 303,000 50% of all SP 20,600,000(quantitative enrollees inor Qualitative) participating
provinces
Date achieved 06/30/2007 12/31/2010 10/31/2012Comments(incl. % Fully achieved and more.achievement)Indicator 4 : lAvailability of essential drugs and vaccines at facility level.Value Systemic stock-outs and NA Stock-outs still(quantitative lack of monitoring data occur, and trackingor Qualitative) is not being carried
out on a regularbasis.
Date achieved 06/30/2007 12/31/2010 10/31/2012Comments(incl. %achievement)
Indicator 5: Rural Health Units (RHUs) accredited by PHIC for Maternity CarePackage.
Value IN =0 IN =11 IN= 2(quantitative IF = 0 IF = 5 IF = 5or Qualitative) NV=0 NV = 7 NV=0
RN = 0 RN = 8 RN = 3SL=4 SL=9 SL=16MO = 0 MO=9 MO = 2
Date achieved 06/30/2007 12/31/2010 10/31/2012
Comments(incl. % 28/49 achieved. Target not met.achievement)
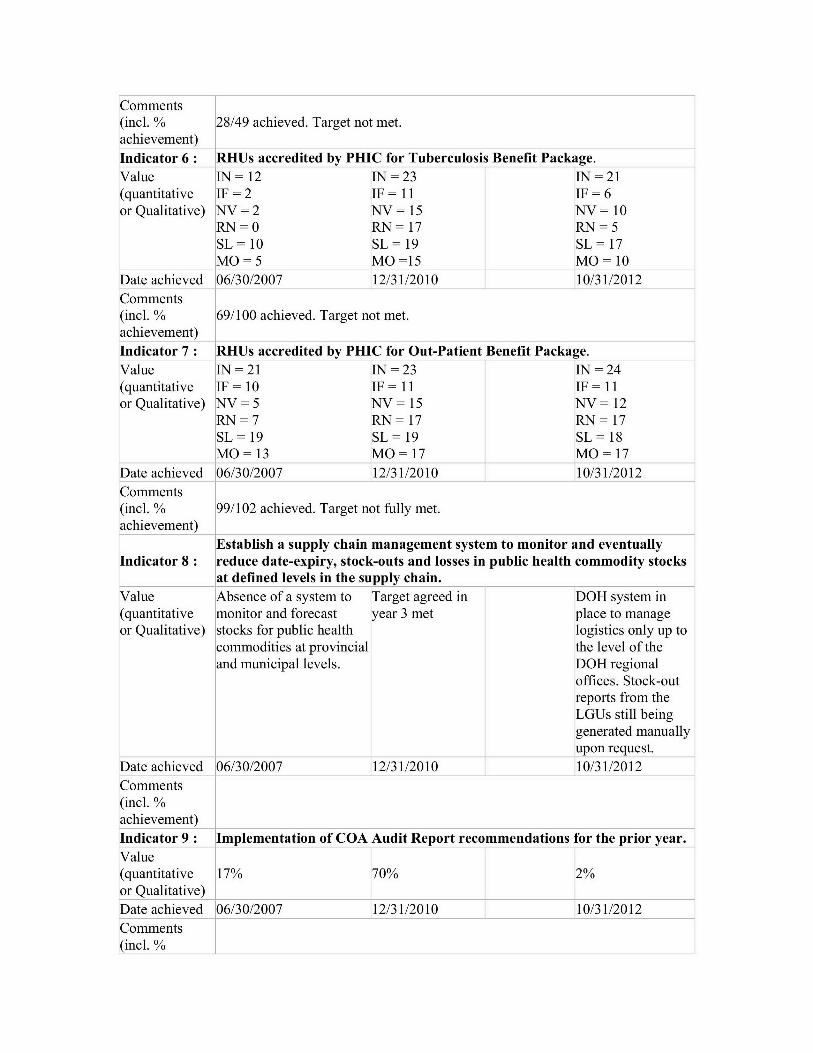
Indicator 6 : RHUs accredited by PHIC for Tuberculosis Benefit Package.Value IN= 12 IN =23 IN =21(quantitative IF = 2 IF = 11 IF = 6or Qualitative) NV=2 NV = 15 NV= 10
RN = 0 RN = 17 RN = 5SL=10 SL=19 SL=17MO = 5 MO =15 MO = 10
Date achieved 06/30/2007 12/31/2010 10/31/2012Comments(incl. % 69/100 achieved. Target not met.achievement)
Indicator 7 : IRHUs accredited by PHIC for Out-Patient Benefit Package.Value IN = 21 IN =23 IN =24(quantitative IF = 10 IF = 11 IF = 11or Qualitative) NV = 5 NV = 15 NV = 12
RN = 7 RN = 17 RN = 17SL=19 SL=19 SL=18MO = 13 MO = 17 MO = 17
[Date achieved 106/30/2007 12/31/2010 10/31/2012Comments(incl. % 99/102 achieved. Target not fully met.achievement)
Establish a supply chain management system to monitor and eventuallyIndicator 8: reduce date-expiry, stock-outs and losses in public health commodity stocks
at defined levels in the supply chain.Value Absence of a system to Target agreed in DOH system in(quantitative monitor and forecast year 3 met place to manageor Qualitative) stocks for public health logistics only up to
commodities at provincial the level of theand municipal levels. DOH regional
offices. Stock-outreports from theLGUs still beinggenerated manuallyupon request.
[Date achieved 106/30/2007 12/31/2010 10/31/2012Comments(incl. %achievement)
Indicator 9: Implementation of COA Audit Report recommendations for the prior year.Value(quantitative 17% 70% 2%or Qualitative)[Date achieved 106/30/2007 12/31/2010 10/31/2012
Comments
(incl. %
achievement)Internal Audit (IA) staff trained; annual IA plan of scheduled audits
Indicator 10 : implemented; updating and improvement in agency IA benchmarkindicators.
Value None At least 80% of IA 100% staff trained.(quantitative staff trained 2010 2010 IA Planor Qualitative) IA plan implemented with
implemented. annual schedule ofaudits.
[Date achieved 106/30/2007 12/31/2010 10/31/2012Comments(incl. %achievement)
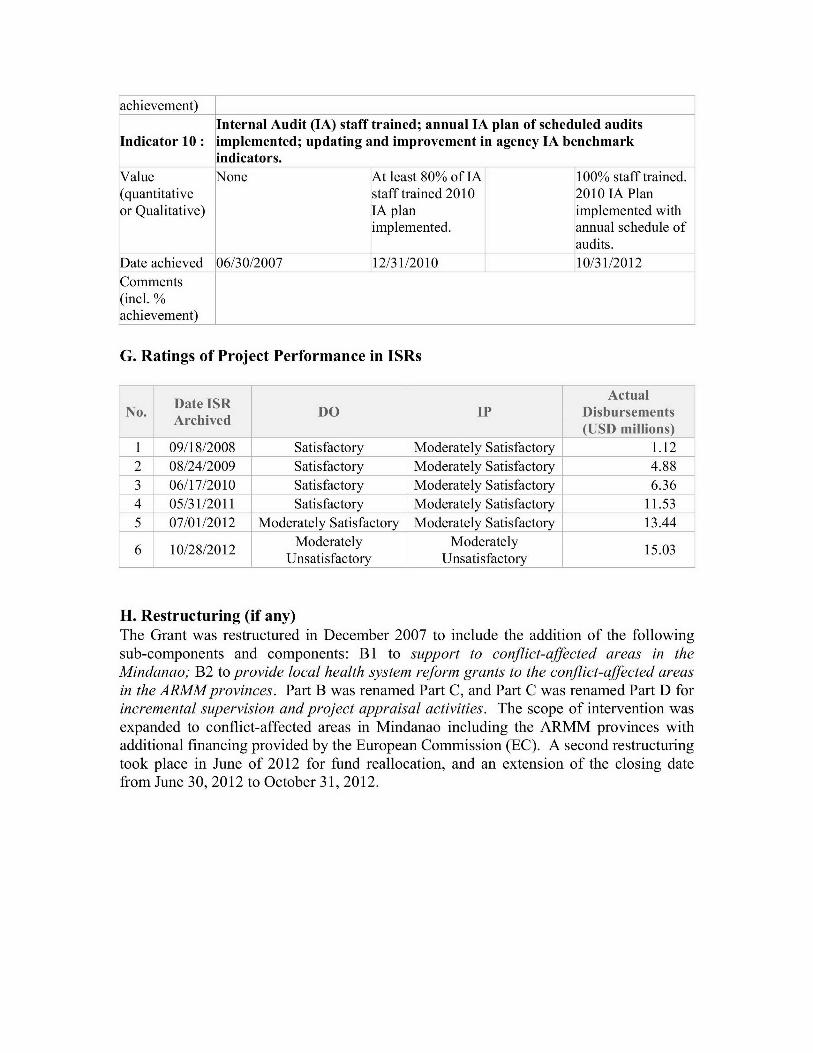
G. Ratings of Project Performance in ISRs
ActualDate ISR Ata
No. Ate DO IP Disbursements(USD millions)
1 09/18/2008 Satisfactory Moderately Satisfactory 1.122 08/24/2009 Satisfactory Moderately Satisfactory 4.883 06/17/2010 Satisfactory Moderately Satisfactory 6.364 05/31/2011 Satisfactory Moderately Satisfactory 11.535 07/01/2012 Moderately Satisfactory Moderately Satisfactory 13.446 1Moderately Moderately
Unsatisfactory Unsatisfactory
H. Restructuring (if any)The Grant was restructured in December 2007 to include the addition of the followingsub-components and components: B1 to support to conflict-affected areas in theMindanao; B2 to provide local health system reform grants to the conflict-affected areasin the ARMM provinces. Part B was renamed Part C, and Part C was renamed Part D forincremental supervision and project appraisal activities. The scope of intervention wasexpanded to conflict-affected areas in Mindanao including the ARMM provinces withadditional financing provided by the European Commission (EC). A second restructuringtook place in June of 2012 for fund reallocation, and an extension of the closing datefrom June 30, 2012 to October 31, 2012.
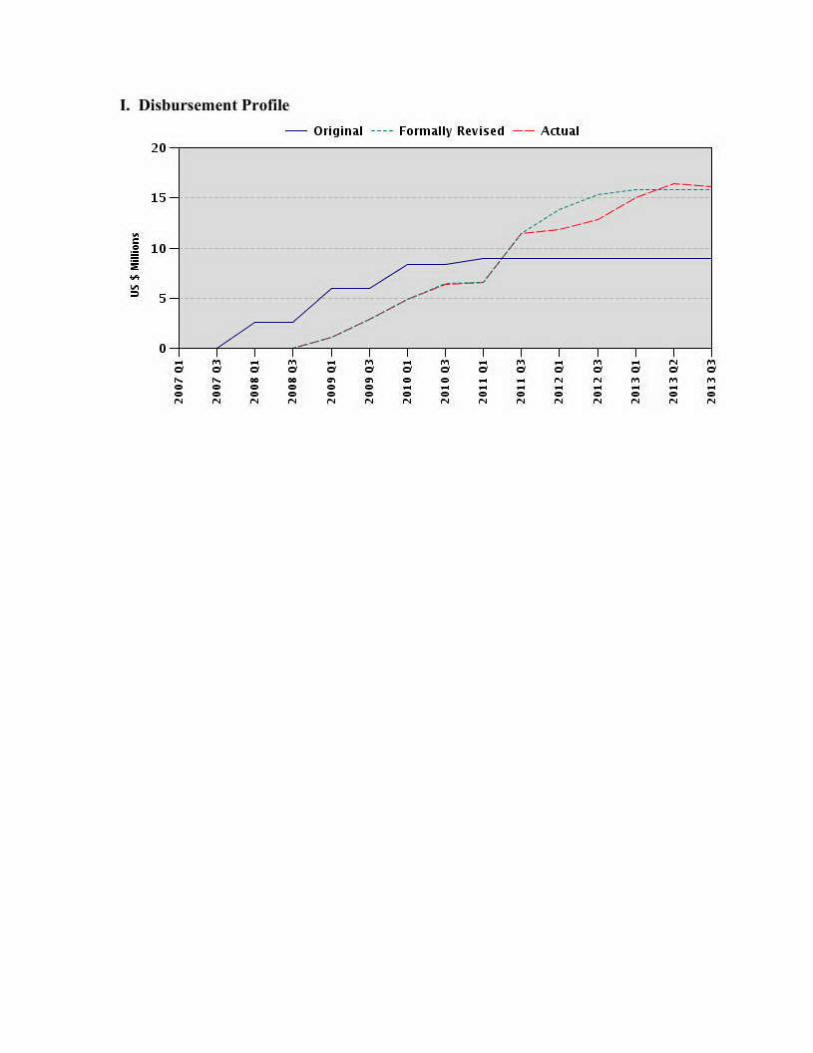
. Disbursement Profile
Original Formally Revised -- Atual20-
|| |
o-
1. Project Context, Development Objectives and Design
1.1 Context at Appraisal
1. At the time of grant preparation, and the associated project to which this Grantwas linked to -- the National Sector Support for Health Reform Project - NSSHRP -(P075464) -- the Philippines had embarked on a number of reforms to deal with majordisparities in health outcomes (across provinces, and across income quintiles). Overallhealth expenditures, as well as public expenditures on health were lower than the averagefor other middle income countries. Out-of-pocket (OOP) payments as a percentage oftotal health expenditures (THE), was high at 54 percent, leading households intounsustainable expenditures (catastrophic payments). The country was grappling with theimpacts of two previous reform programs - the 1991 decentralization of health servicesto Local Government Units (LGUs) and the 1995 enactment of the National HealthInsurance Program (NHIP), scaling up health insurance for the population and theestablishment of the Philippines Health Insurance Corporation (PHIC) or PhilHealth. Thedecentralization reforms led to fragmentation in health financing and the delivery of care.Health services provided by the public sector are shared between the Department ofHealth (DOH) and the local government units (LGUs). While the 1995 national healthinsurance reforms addressed some of this fragmentation, as well as providing fundsthrough PhilHealth, progress in providing healthcare for the poor was limited.
2. The Health Sector Reform Agenda (HSRA) of 1998-2004, had begun to addressthe problems described above. But progress was slower than expected. In 2005, theHSRA reinvigorated its focus on the reform framework: FOURmula One for Health (Fl)which had four pillars:
* Pillar I: Health Financing through increased financial protection for the poor andsick;
* Pillar II: Health Service Delivery through supply-side measures to upgradepublic health facilities in all communities to meet PhilHealth's accreditationstandards;
* Pillar III: Health Regulation for more effective regulation of the health sector andof drugs and commodities; and
* Pillar IV: Good Governance for a stronger results focus and coordinationbetween DOH and LGUs in delivering public health programs.
3. As implementation of the HSRA's recommendations was deemed to be too slow,the DOH adopted a phased implementation strategy in 2002, beginning with select''convergence" provinces (designated as priority provinces for the implementation of theHealth Sector Reform Agenda by DOH Administrative Order No. 12005-0023), andsought development partner assistance to support the HSRA in these sites. Fl wasexpected to focus on results through the National Objectives of Health (NOH) of 2005-2010 and in line with the Millennium Development Goals (MDGs) as well as with theMedium Term Philippine Development Plan (MTPDP) of 2004-2010. The goals of Fl
1
are to improve health outcomes, health system, equity in health care financing, especiallyfor the poor and vulnerable populations. Using the medium-term Health SectorExpenditure Framework (HSEF), the annual budgeting process, and a performancemonitoring framework for DOH, PhilHealth and convergence provinces should be able tolink budgeting and resource allocation to outputs and intermediate results. These linkswere intended to reduce obstacles to reform. With regard to fragmentation in financing,Sector Development Approach for Health (SDAH) was adopted under Fl to aligndevelopment partners-supported reform activities across the entire health sector under asingle national implementation plan and under harmonized local health investment plansin each convergence province.
4. It was recognized that the HSRA had partial success due to: (1) limitations inprioritizing a complex reform agenda and translating it into do-able, fiscally realisticaction plans, (2) limited coordination between DOH and PhilHealth over reform strategy,(3) limited capacity in results-based management, (4) excessively cautious behaviour byPhilHealth in scaling up the NHIP, (5) fragmented donor support, and (6) constrainedfiscal space.
5. In addition, the Country Assistance Strategy (CAS) 2006-2008 focused onsupporting public expenditure management reform, improved governance, and bettertargeting of public expenditure at a time when the country's fiscal situation was fragile.The approach of the new CAS was well suited to supporting the F 1 strategy of linking thehealth budget with reforms to health expenditure management.
6. The context outlined above led to the design of the Bank project NSSHRP(National Sector Support for Health Reform), and a budget support Grant of Euro 48.5million from the European Commission (EC) for the Health Sector Policy SupportProgrammes to assist the government in areas of good governance, health financing,health service delivery, and regulation, specifically of drugs and medicines. The EC TFGrant under review was but a small slice of the total support provided by the Bank andthe EC, and targeted six convergent provinces. These provinces did not meet thestandard fiduciary requirements, and therefore required oversight, for which the ECrequested Bank management of the Grant. It was also agreed at the time of Grantdevelopment, that the project's outcome measures were to be based on the overall sectoroutcomes, rather than outcomes specific to the Grant.
1.2 Original Project Development Objectives (PDO) and Key Indicators
7. The objective of the Trust Fund was to increase utilization of affordable andfinancially sustainable, good quality essential health services by the poor in participatinglocalities through the progressive implementation of the Philippine Government's HealthSector Reform Agenda (HSRA). The project consisted of two operational components,to: (i) provide local health system reform grants to six (6) selected ConvergenceProvinces (Ifugao, Ilocos Norte, Southern Leyte, Romblon, Misamis Occidental andNueva Viscaya) to support activities set forth in their province-wide investment plans forthe health sector, and (ii) strengthen DOH's capacity in the area of public financialmanagement, internal audit, information management, procurement and performance
2
monitoring under local government scorecards, through provision of training, technicalassistance, and required computer hardware and software. The third component was themanagement of the Grant which received separate funding.
8. Key indicators were:(a) Births attended by skilled health professional at a health facility increased by 5percent of baseline;(b) DPT 3 vaccine coverage increased by 5 percent from baseline;(c) Measles vaccine coverage increased by 5 percent from baseline;(d) TB cure rate increased by 5 percent from baseline;(e) TB case detection rate increased by 5 percent from baseline.
9. The intermediate results indicators can be found in Annex 2.
1.3 Revised PDO (as approved by original approving authority) and Key Indicators,and reasons/justification
The PDO were revised in December 2007 to read as follows: assist the Recipient toincrease utilization of affordable and financially sustainable, good quality essential healthservices by the poor in participating localities (the selected Convergence Provinces andconflict affected areas) through progressive implementation of the Recipient's HealthSector Reform Agenda.
1.4 Main Beneficiaries
10. The primary beneficiaries of the project were poor households in the ConvergenceProvinces, starting with the first six: 1) Ilocos Norte, 2) Nueva Vizcaya, 3) Ifugao, 4)Romblon, 5) South Leyte, and 6) Misamis Occidental. In early October 2007, the EUDelegation requested the Bank to amend the existing Trust Fund AdministrationAgreement to include additional provinces in conflict affected areas of Mindanao and theAutonomous Region of Muslim Mindanao (ARMM) in support of the upscaling of theimplementation of the health sector reforms under the Fl for Health. These additionalMindanao provinces were: 7) Isabela City, 8) Zamboanga del Sur, 9) Zamboanga delNorte, 10) Zamboanga Sibugay, 11) Compostela Valley, 12) Davao Oriental, 13) Lanaodel Norte, 14) Sarangani, 15) Sultan Kudarat, 16) ARMM (Maguindanao, Lanao del Sur,Basilan, Sulu, Tawi-Tawi)
1.5 Original Components
11. Part A: Recipient-Executed activities: Support to selected provinces/Local systemreform grants. The component would provide local health system reform grants to six (6)selected Convergence Provinces (Ifugao, Ilocos Norte, Southern Leyte, Romblon,Misamis Occidental and Nueva Viscaya) to support activities set forth in their province-wide investment plans for the health sector. These plans would aim at developing andimplementing the four goals of the government's health sector reform agenda, namely:financing, regulation, health services delivery and good governance.
3
12. Part B: Recipient-Executed activities: Support to DOH/Strengthening DOH'scapacity. This component would strengthen DOH's capacity in the area of publicfinancial management, internal audit, information management, procurement andperformance monitoring under local government scorecards, through provision oftraining, technical assistance, and required computer hardware and software.
13. Part C: Bank-Executed activities: Incremental supervision activities. Thecomponent would finance direct incremental costs incurred by the Bank in supervisingthe Recipient-executed activities under the grant.
1.6 Revised Components
14. The components were restructured in December 2007 to include theimplementation of the EU's Mindanao Health Sector Policy Support Programme(MHSPSP) through an amendment to the Administration Agreement as follows: a newPart B was added: B1 would support to conflict-affected areas in the Mindanao; B2would provide local health system reform grants to the conflict-affected areas in theARMM provinces. Part B was renamed Part C, and Part C was renamed Part D forincremental supervision and project appraisal activities. The scope of intervention wasexpanded to conflict-affected areas in Mindanao including the ARMM provinces withadditional financing provided by the European Commission (EC), and an amendment tothe existing Grant Agreement (TF070600). A second restructuring took place in June of2012 that was approved for fund reallocation, and an extension of the closing date fromJune 30, 2012 to October 31, 2012 to allow certain key activities to be completed.
1.7 Other significant changes
15. The original EC Grant was for EUR 6.75 million, signed in April 2007 (EUR 5.75million for the convergence provinces and EUR 1.0 million for DOH). The EC providedadditional funding of EUR 6.7 million, bringing total EC grant to EUR 13.45 million, toinclude the ARMM and select Mindanao provinces which expanded the scope of theproject, and put a heavier burden on the DOH to manage the project. Each province hadto put in place Province-wide Investment Plans for Health (PIPH) followed by annualoperational and procurement plans, together with Service Level Agreements (SLAs).These would be reviewed by the Joint Appraisal Committee (JAC). The implementationset-up and the need for rigorous control were appreciated, but with Local GovernmentUnits (LGUs) at differing levels of capacity, this required substantial capacity building.
16. The supervision missions were carried out through the Joint Assessment andPlanning Initiative (JAPI), which is a forum of partners in health. The JAPI met twotimes a year to carry out the implementation of the Grant and made recommendations onimplementation issues. However, the JAPI supervisions may have been insufficientgiven some of the issues that emerged during implementation, and closer and more fieldvisits may have been warranted.
4
2. Key Factors Affecting Implementation and Outcomes
2.1 Project Preparation, Design and Quality at Entry
17. The Grant was provided by the EC to support the government's health reformsthrough the Fl for health strategy, on areas such as service delivery (e.g. healthfacilities/infrastructures), governance (e.g. improvement of the public financialmanagement), information system (including the monitoring system) with the aim ofbringing quality improvement of health services in the convergence provinces. TheGrant under review is but a small slice of a larger grant financed by the EC throughbudget support to the government. The Grant itself focused on six provinces which hadweaker fiduciary systems and required more intensive capacity building and oversight,leading to the subsequent agreement with the World Bank to manage this Grant. Theactivities were subsequently expanded to include the Mindanao and ARMM provinces.The focus was to improve service delivery for the poor and develop and/or improvemanagement tools of the DOH. The DOH, responsible for overall policy and regulation,devolved oversight for implementation of the policies and strategies to the decentralizedlevel, which in turn devolved the tasks to the regional offices - from the Centers forHealth Development (CHDs) to the Local Government Units (LGUs) responsible forservice delivery. Capacity among the CHDs varied and was uneven. The capacity ofLGUs also varied and some required much more capacity building than others. The Grantplaced emphasis on capacity building with the development and use of standardized toolsto ensure consistency among the CHDs and the LGUs. The Grant relied on the samestructure as the NSSHRP to facilitate implementation. However, the ProjectDevelopment Objectives (PDO) and the monitoring indicators were not appropriate forthis Grant, since the activities under the Grant were much smaller in scale and much morelocalized. For example, the Grant indicators do not fully measure the "increasedutilization of affordable and financially sustainable, good quality essential health servicesby the poor in participating localities". Usage was measured by skilled attendants andvaccine coverage, however, affordability was not measured, nor were measures availableto evaluate financial sustainability. Quality was measured through the availability ofessential drugs and vaccines and accreditation of health facilities. Both the Grant PDOand indicators were over ambitious and reflected national level data, but not for theconvergent provinces.
18. Unforeseen during the design phase, was the active role required by the DOH toprovide more intensive guidance to the CHDs and to the LGUs in implementing thereform. The devolution of the health sector was not as robust as was expected, andcertain LGUs had difficulty in fulfilling the requirements under the Grant andimplementing the reform. With regard to the identification of the poor, the LGUs werenot willing to use the government's proxy means testing tool, and did not agree tofinancially support the payment of premium of the poor identified by the government'sNHTS, which, for all intents and purposes, was a far more improved tool to the systemused by the LGUs. The LGU system had a roster of households which did not fall underthe NHTS definition of the poor. These refer to LGU-sponsored "poor" before theimplementation of NHTS, whereby the LGU social worker filled out a checklist/intake
5
form and ascertained whether a family qualified as poor or not. Other LGUs implementeda Community-Based Monitoring System (CBMS) or some other proxy means testmethodology.
19. Oversight of the Grant and review/approvals of the PHIPs and AOPs wasprovided by the JAC, which ensured that these were aligned with the national reforms.The JAC also served as an advisory body to the DOH and Fl provinces. The JACreviewed and approved the Province-wide Investment Plan for Health (PIPHs). TheOperational Manual for Local Health Systems Reform Grants described the method bywhich the grants provided to the LGUs would be dispensed, the purpose of improvingperformance, and the Project Operation Manual governed the grants provided to the DOHto improve the financial and procurement management of the reform and the Grant.Standard operational and procurement plans were developed with the Annual ServiceLevel Agreements (SLAs), and training was provided to the LGUs.
20. The model of using PIPHs and Annual Operation Plans (AOP) for ensuringimplementation of the reform at LGU level was deemed effective on focusing theattention of the total 16 convergence provinces on healthcare delivery, prioritizingprogram activities, and funding (such as the provision of birthing facilities to ensurecoverage and outreach). The municipalities were involved in the development of thePIPH with Memorandum of Understandings established between municipalities andprovinces.
21. In establishing the above, the design could have been reinforced to better managethe capacity issues which emerged at multiple levels of the Grant structure, and which ledto serious delays in the launch of activities. The learning curve was steep in (a) preparingoperational and procurement plans on a realistic and manageable basis (PIPHdevelopment took almost two years to prepare for the 16 provinces); (b) the time neededfor reviews by the JAC, which became quite lengthy; (c) the need for extended exchangesbetween the field and the central level in finalizing the documentation; (d) the timeneeded to prepare the PIPHs, followed by the AOPs; and finally (e) the preparation of theSLAs which were contracts that needed to be abided to in order to receive funds. TheDOH and the LGUs adhered to the Government Procurement Reform Act and which theBank likewise subscribed to -- thus there was no conflict on the procurement system andmethodologies to be used under the Grant. Both the LGUs and the DOH procured goodsand equipment. However, the DOH had the responsibility for procuring consultantservices, and which they were not as familiar with procedures and guidelines. In the caseof ARMM, the agreement was that the DOH Central Office would undertake theprocurement process with inputs from ARMM DOH with regard to the preparation of thebidding documents and inputs to the technical specifications
22. The other aspect that led to delays was the process of accreditation of LGUs bywhich LGUs could avail of PhilHealth reimbursements, and setting up a scorecard systemwhich rated LGU performance and ability to receive the variable tranches (disbursementsbased on meeting targets). In addition, the CHDs needed to be trained in the PhilHealth
6
Benchbook Standards for Out-Patient Services, for which DOH had oversightresponsibility.
23. The Grant could have strengthened the Monitoring and Evaluation (M&E)framework in how data was to be collected, the responsible entity in charge of that data,frequency of data collection, and how the outcomes related to funding or funds expended(an example is TB coverage--amount expended), as well as regular reporting. The Grantcould have improved the M&E system by identifying indicators which better matched theactivities being undertaken under the Grant and ensure that the PDOs were better alignedwith the objectives of the Grant rather than the overall reform program.
24. The above issues could have benefitted from a quality at entry process so that theproblems noted above could have been resolved early on. For example, it is noted belowthat the annual SLAs took quite some time to be processed which delayed Grant activities.
2.2 Implementation
25. Originally, the EC Grant was to fund six provinces. This was expanded to selectMindanao and ARMM provinces, in which the Fl would be implemented. The DOH wasresponsible for overall implementation. The mechanisms described above were put inplace to that effect.
26. The first annual SLAs between the LGUs and DOH were not signed until May2007, and the Annual Operation Plans for CY2007 were approved only in March 2008.The Operational Manual for Local Health Systems Reform Grants (which became the FlOperations Manual for Convergence Provinces: Implementation of the Province-wideInvestment Plan for Health) was finalized in November 2007, and the Project OperationManual was not approved till May 2009.
27. Procurement orientation workshops were held in March 2007, however not tilllate in 2007 did the first six provinces have their bidding documents ready. There wereengineering and architectural design issues which proved contentious for the sixprovinces. In addition, clarity of roles could have been better managed to avoidmisunderstanding within DOH as to the responsibility it held with regard to theprocurement process under the Grant, which then led to delays in procurement processingand approval of procurement packages. This was also compounded by an insufficientnumber of human resources to undertake the procurement activities at the DOH level,given that DOH was managing a multitude of activities in parallel. Funding wasavailable under the Grant to strengthen DOH capacity, which was not fully used duringthe Grant period. The financial management review of October 2007 found that financialmanagement capacity could have been strengthened, systems improved to adequatelyimplement the project, and increases in human resources to manage the Grant overall. Inaddition, during a critical time, the DOH was unable to focus on the task at hand due tothe rationalization plan being carried out in parallel by the Department of Budget andManagement (DBM) which required DOH staff time and which took their attention awayfrom project implementation. It is worth mentioning that the rationalization plan has notyet been adopted by the DBM. It was also noted that the process of clearing the LGU
7
work plans and SLAs was negatively impacted by the above, which led to further delaysin the final submission and approvals of the provincial Annual Operation Plans andProvincial Procurement Plans. A more proactive approach from DOH might haveresolved some of the above. Nevertheless, once the learning curve was overcome, theSLAs became institutionalized and are now being implemented nationwide.
28. Up to September 2008 it was noted that the DOH had not yet finalized the M&Eof the sector reform. Data collection mechanisms had not been defined, nor qualitycontrol of data, data analysis, and use of the data for improved decision-making.Baseline data was collected, but given the validity question of the data it is unclearwhether real progress has been made.
29. A rather more serious impact was the inconsistent reporting on progress and thesubmission to the Bank (and the EC) on both progress and procurement reports. Delaysin submission of the audit report were also regular occurrences.
30. Overall, the Grant would have benefitted from increased oversight, focus onresults, reduced bureaucracy, and clearer flow of decision making, to ensure that fundswere timely disbursed and indicators better monitored.
2.3 Monitoring and Evaluation (M&E) Design, Implementation and Utilization
31. The ME3 is the M&E system which the DOH used, and within the ME3 was thescorecard system that was being used under the Grant. The scorecard was to align LGUactivities among all LGUs and compare LGU performance. The ME3 included data onthe Millennium Development Goals (MDGs), which was part of the design, and the dataselected was in response to the four pillars of the HSRP. However, the design of theM&E and indicators selected were for a more national high-level approach, which did nottake into account the local context and whether the indicators identified and selected werecurrently being collected, or could be collected. The SLAs were a framework to assistthe LGUs in collecting standardized national data which would feed into the process ofdetermining the effects of the reform. However, the "standardized" tool did not respondto the reality on the ground as certain LGUs could not collect the data, not having amechanism to do so. Some of the SLA indicators were subsequently modified to allowthe LGUs to collect and report on data that they could collect. However, that meant thatcomparability between the LGUs could not take place, and LGUs could not be evaluatedon the same basis. SLAs were later improved for uniformity and comparability. Thismodification benefitted the LGUs, as they received variable tranche awards for goodperformance (which was on the basis of what they could collect and analyze), but withlittle effort in putting in place a mechanism to collect more useful data that could informdecision makers on the key health issues of the province, or on required national data.
32. The M&E framework was subsequently revised to include standard indicators forall LGUs. Data in the last Implementation Status Report (ISR) does not reflect accuratedata. Therefore, this review corrects that data based on the Field Health ServiceInformation System (FHSIS) reports received for 2007, 2010, and 2011. A review of thedata shows a wide variation, bringing into question the validity of the data and the
8
verification process of the data. For example, under the rubric "Births attended by skilledhealth professional at a health facility", Ilocos Norte shows a jump from 35.0 percent in2007 to 74.6 percent in 2010; Misamis Occidental shows a jump of 17.0 percent in 2007to 50.5 percent in 2010, and Sulu a drop from 7.9 percent in 2007 to 2.8 percent in 2010.It is unclear whether there is an issue with the definition of the indicator (the FHSISreports for Normal Type Deliveries and Other Type Deliveries in Health facilities. Thequestion is whether both types of deliveries are being reported or only one. In addition,there may be an issue of the denominator, period of reporting, self-reports, and potentialdisconnect of data flow from the provinces to DOH. Data on delivery attendant does notspecify the locale, only the health professional providing the service. The 2010 FieldHealth Services Information System also changed the reporting format which makes itdifficult to compare data between different years. Determining LGU performancethrough the SLAs does not lead to clarity on what was achieved as far as makinghealthcare delivery accessible to the most vulnerable. Attribution is therefore difficultto ascertain given the above, and there is disconnect between the high-level indicatorsand local implementation.
2.4 Safeguard and Fiduciary Compliance
33. The safeguards were rated Category B. There were a number of caveats whichthe team was to ensure compliance:
34. Civil Works. It was agreed that the Country Systems Approach, using theenvironmental regulations and procedures already in place in the Philippines, wassatisfactory to address the issues under the project. There was no new constructionplanned; and assurances were provided that issues such as noise, dust, worker safety, andisolation of work area would be addressed for the rehabilitation of existing buildings.
35. The environmental and healthcare waste management guidelines developed forthe 2nd Women's Health and Safe Motherhood Project in the Philippines would be used tosatisfactorily address the healthcare waste issues in this Grant. It was noted that anAdministrative Order which covers medical waste, and the guidelines and manual wereendorsed by the safeguards team. The DOH reported general compliance with agreedenvironmental management plans. The DOH enforced the proper management of HealthCare Waste through its technical guidelines. The Department of Environment andNatural Resources also monitors compliance with these guidelines. There were nosignificant environmental safeguards issues in the project.
36. Indigenous People: Most of the target provinces had indigenous minoritypopulations, thereby triggering the policy. An Indigenous People's Policy Framework(IPPF) was prepared for the NSSHRP, and was found to be satisfactory. The project hasinvested in goods, equipment, and systems to make a contribution to healthcare access toindigenous people, but there is no concrete data that can provide a more substantialassessment.
37. Per a Bank mission report of February 2011, the DOH documented and assessedthe implementation of the Indigenous Peoples' (IP) Plan in Surigao del Sur, the results of
9
which were to inform the development of a broader policy for enhancing delivery ofhealth services in indigenous communities. The DOH stated that there were variousinitiatives by different DOH Field Offices related to IP-focused health delivery, and thefindings were to be synthesized for lessons learned and toward the development of apolicy framework or guidelines to be disseminated. The government has prepared withthe EC a targeted IP project which is under implementation.
38. Financial and procurement management were issues under the Grant as the DOHand the LGUs were unfamiliar with procurement procedures and processes. Despitetraining provided, there needed close follow-up of the full process, in light of inadequateor appropriate reporting of financial and procurement processes, recurrent delays in thereceipt of Financial Monitoring Reports, overdue audit reports, tracking of expendituresat both the DOH and decentralized levels, and the inability to obtain progress andprocurement reports as requested by the World Bank. There were also problems withreconciliation of accounts, separate book keeping, inaccurate use of forms, etc. Therelease of funds by the DOH to the provinces, and usage of funds for DOH's owncapacity building program, was also problematic due to bureaucratic processes bothwithin and outside of the DOH, staff turnover, adequate knowledge of internalprocedures, and the need for a more proactive approach by relevant budgetary agencies toresolve problems.
39. In addition, the delays in procurement were due to the difficulty that LGUs had infollowing the procedures required (World Bank and government had harmonized thebidding procedures), and the LGUs found themselves overwhelmed by the large programthey had to implement. The learning curve was steep for all parties concerned in gettingthe activities off the ground. In addition, there were issues surrounding shoppingprocedures requiring at least three quotes; this was difficult to obtain in certainenvironments due to distance and lack of interest. Given the problems encountered inbeing able to garner more bidder interest and participation, and to improveimplementation, acceptance of a minimum of two quotes was approved for the DOH onan exceptional basis for specific procurement packages. Once the learning curve wasachieved, the LGUs appreciated the structure and organization they had to follow, andwere able to comply with procedures.
2.5 Post-completion Operation/Next Phase
40. The health reform will continue under the Government's commitment toUniversal Health Care. The government expects that membership of NHTS householdsinto NHIP will increase with enhanced NHIP benefits package being implemented, aswell as service delivery transformations to support a reformed NHIP. The DOH couldalso benefit from increased support, particularly in the field of monitoring and evaluation,to ensure that the programs being implemented result in outputs and outcomes thatinform policy. In addition, additional work on the validity and quality of data would bebeneficial to better inform trends, progress, and policies in the sector. SeveralDevelopment Partners are working on a number of fronts to strengthen health servicedelivery.
10
3. Assessment of Outcomes
3.1 Relevance of Objectives, Design and Implementation
41. The Project Development Objectives (PDO), though overly ambitious for thisGrant, remain highly relevant for the Philippines as the government strives to achieveUHC by 2016. The government continues to push ahead with the enrolment of thepoorest families in the Philippines into PhilHealth's Sponsored Program. Prior to theNSSHRP and the Grant, the different instruments used by the LGUs to target the poorwere not satisfactory, and instead resulted in the politicization of enrolment of the poor.The Grant achieved a certain measure of success, though direct attribution is difficult toascertain. Poor families are being enrolled in the national program, but the quality ofservices is not reflected in the indicators which remain unmet (vaccination coverage,accreditation of Rural Health Units), and the capacity of DOH requires furtherstrengthening. In addition, closer attention to absorptive capacity and government systemat the design stage might have identified some of the issues that were raised duringimplementation.
42. The design of the Grant was also relevant in providing much needed additionalequipment and technical assistance to solidify aspects of the reform, and provided neededtools to improve the efficiency of public financing in the health sector, toward a moreresults-oriented system. However, given the above, the design of the Grant should havebeen strengthened to take into account weaknesses encountered under implementation.The Grant tied in with the CAS on supporting public expenditure management reform,improved governance, and targeting of public expenditure. An outcome is that thecurrent CAS has adopted the National Program Support (NPS) model as one of the keyinstruments for support to social sectors.
43. The Grant tagged onto the same implementation arrangement as the NSSHRP.As it turned out, implementation was fraught with issues due to the fragmentation ofdecentralization, lack of firm oversight, bureaucratic delays and the need to apply rulesand procedures that implementers were not familiar with, including procedures forquality data collection and usage. Without a good tracking system, it was difficult to tiein expenditure with outcomes under the PIPHs, SLAs, and other contractualarrangements.
3.2 Achievement of Project Development ObjectivesRating: Moderately Unsatisfactory
44. The Project Development Objectives of increasing utilization of affordable andfinancially sustainable, good quality essential health services by the poor wasoverambitious for this Grant and therefore difficult to assess given the weak incrementalchanges in baseline to actual figures, or even in some cases regression in outcomes. Therating is therefore rated Moderately Unsatisfactory. Despite the government makinggreat efforts under the NSSHRP to purchase needed vaccines, vaccination coverageremained low for the 16 provinces. However, the findings of a 2008 review noted anumber of issues, such as a high volume of drugs and vaccines that had expired before
11
even being dispensed, poor inventory and consumption reports on distribution of vaccinesand drugs, and minimal use of inventory cards and inconsistent information.
* measles vaccination decreased;* small incremental changes in DPT3 vaccine coverage;* no improvement in TB case detection rates;* systemic stock-outs and lack of monitoring for the availability of essential drugs
and vaccines at facility level.
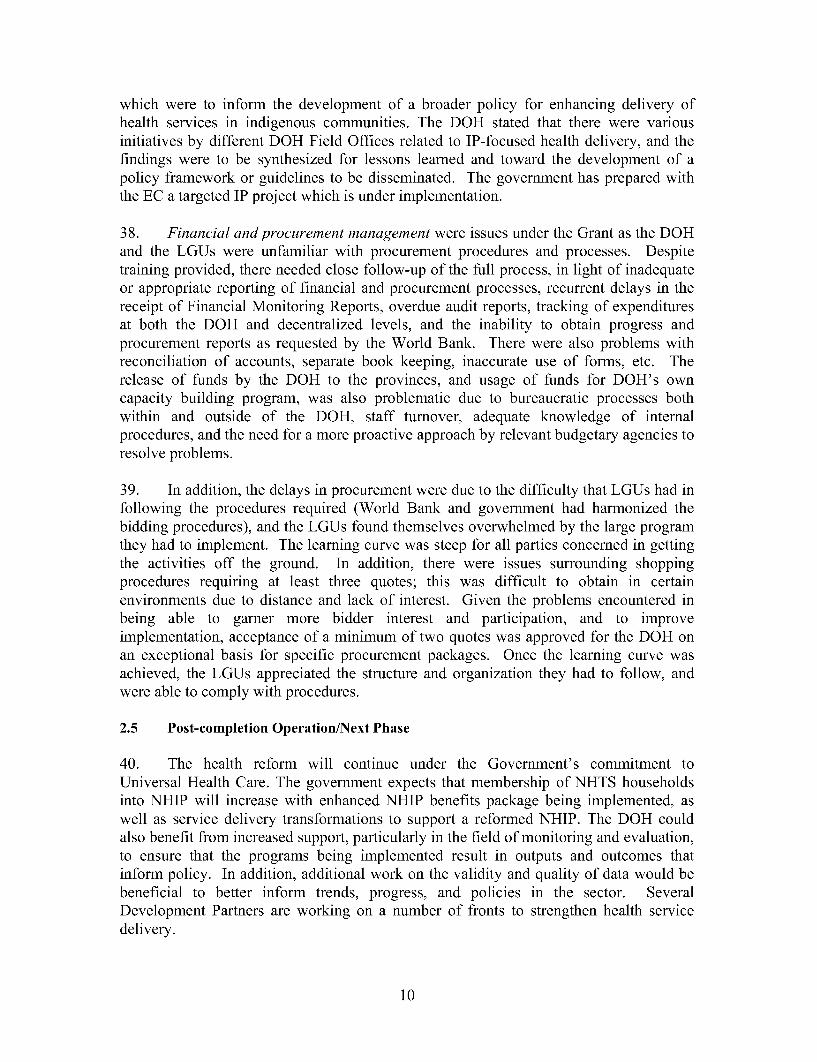
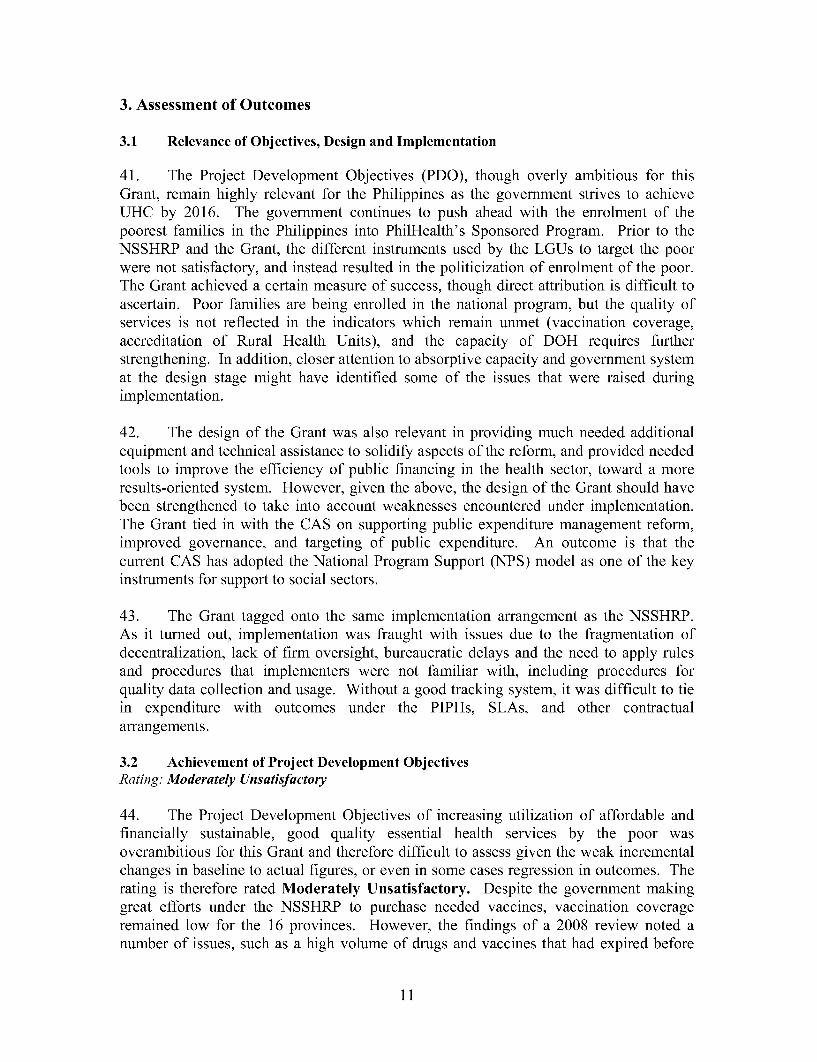
45. However, some data obtained suggests that there have been improvements overtime for other health issues, such as improvements to morbidity rates of acute lowerrespiratory tract infection and pneumonia, filariasis morbidity rates, and malariamorbidity rates.
Acute Lower Respiratory Tract Infection & Pneumoniamorbidity rate by year Philippines, 1997 - 2010
rigure 4B15
1200
1000
IO
600
400
1997 1998 1999 2000 2001 2002 2003 2DD4 2005 2006 2007 2008 2009 2010
Year
Filariasis morbidity rate by yearPhilippiFus,r199e-2010 g 4B.13 Malaria morbidity rate by year
Philippines, 1997 -2010
Figure 4019120
25
01900
20
1997 199 1999 2000 2001 2002 2U03 ZOM9 2005 2006 2007 2008 21D9 201
Ye
12
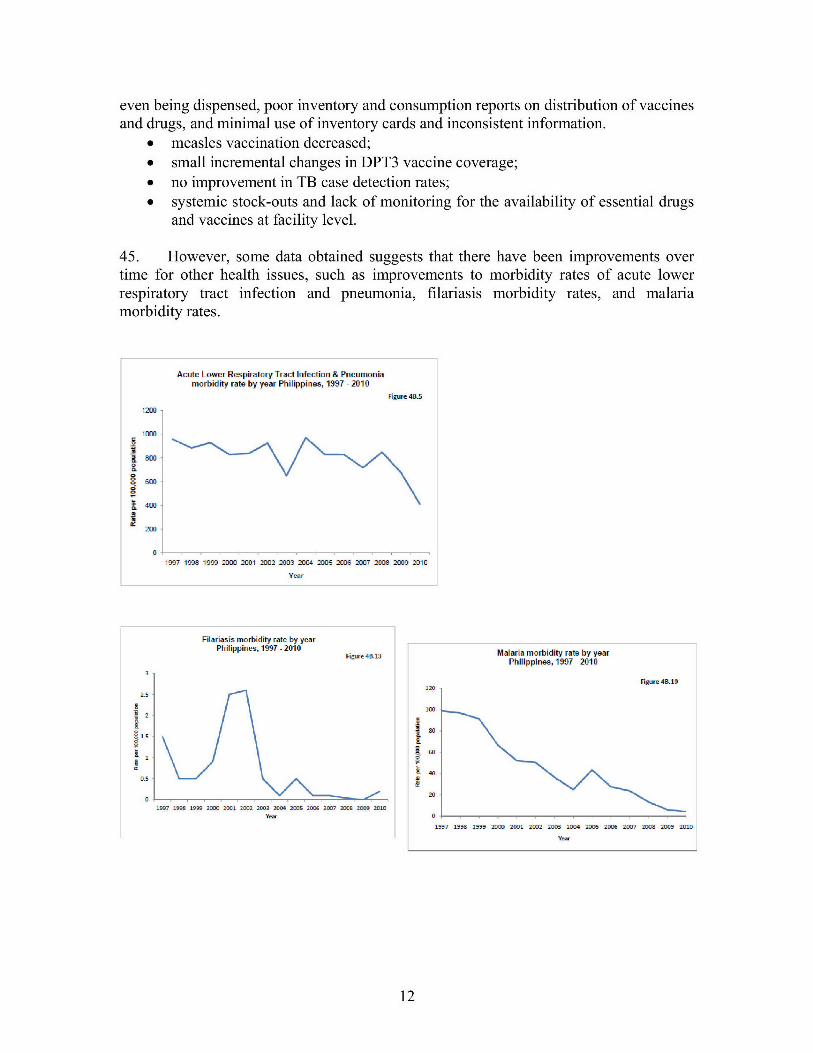
46. In addition, the Rural Health Units (RHUs) did not meet all their targets asreflected in the table below: 28/49 RHUs were accredited for Maternity Care Package;69/100 RHUs were accredited for Tuberculosis Package; and 99/102 RHUs wereaccredited for Out-Patient Package. Some of the key reasons of non-accreditation wereto do with issues of non-compliance with physical space requirements (TB-DOTs, MCP),necessary and needed equipment, and qualified trained personnel.
Target Activity Target/Outcome Actual OutcomeRHU accredited by PHIC for Ilocos Norte 11 Ilocos Norte 2Maternity Care Package Ifugao 5 Ifugao 5
Nueva Vizcaya 7 Nueva Vizcaya 0Romblon 8 Romblon 3South Leyte 9 South Leyte 16Misamis Occidental 9 Misamis Occidental 2
Total 49 28RHU accredited by PHIC for Ilocos Norte 23 Ilocos Norte 21Tuberculosis Benefit Package Ifugao 11 Ifugao 6
Nueva Vizcaya 15 Nueva Vizcaya 10Romblon 17 Romblon 5South Leyte 19 South Leyte 17Misamis Occidental 15 Misamis Occidental 10
Total 100 69RHU accredited by PHIC for Out- Ilocos Norte 23 Ilocos Norte 24Patient Benefit Package Ifugao 11 Ifugao 11
Nueva Vizcaya 15 Nueva Vizcaya 12Romblon 17 Romblon 17South Leyte 19 South Leyte 18Misamis Occidental 17 Misamis Occidental 17
Total 102 99
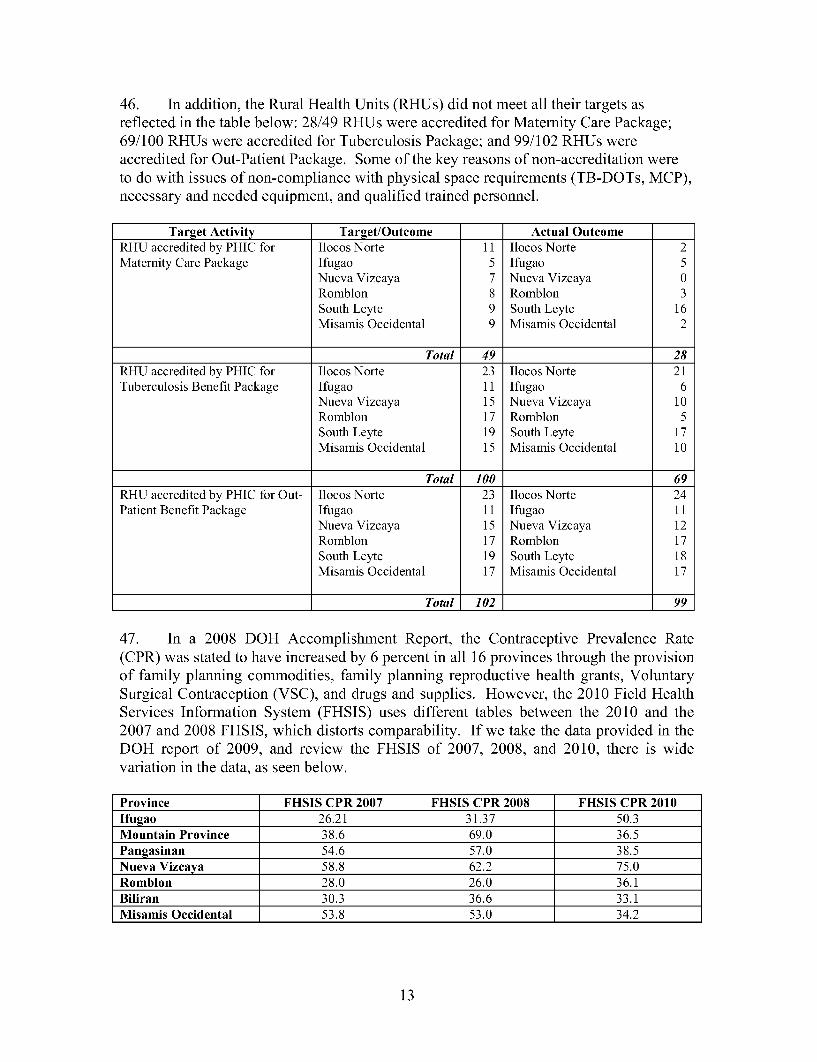
47. In a 2008 DOH Accomplishment Report, the Contraceptive Prevalence Rate(CPR) was stated to have increased by 6 percent in all 16 provinces through the provisionof family planning commodities, family planning reproductive health grants, VoluntarySurgical Contraception (VSC), and drugs and supplies. However, the 2010 Field HealthServices Information System (FHSIS) uses different tables between the 2010 and the2007 and 2008 FHSIS, which distorts comparability. If we take the data provided in theDOH report of 2009, and review the FHSIS of 2007, 2008, and 2010, there is widevariation in the data, as seen below.
Province FHSIS CPR 2007 FHSIS CPR 2008 FHSIS CPR 2010Ifugao 26.21 31.37 50.3Mountain Province 38.6 69.0 36.5Pangasinan 54.6 57.0 38.5Nueva Vizcaya 58.8 62.2 75.0Romblon 28.0 26.0 36.1Biliran 30.3 36.6 33.1Misamis Occidental 53.8 53.0 34.2
13
48. The 2011 Family Health Survey notes a 2011 national CPR rate accomplishmentof 48.9 percent, which was the same rate assessed under the National Demographic andHousehold Survey (NDHS) in 2003 (48.9 percent), whereas the 2008 NDHS noted 50.7percent.
49. Data for birth attendance by a skilled health professional at a health facility alsohighlights the need for data validation and improvements in data collection and reporting.For example, one non-ARMM province shows improvements in the indicator, but dataprovided from provincial reports differ from the data reported in the FHSIS. This may bedue to the definition of the indicator (only normal deliveries in hospitals or inclusion ofother deliveries in hospital), denominator, reporting period, etc.
2007 FHSIS 2007 Prov. 2010 FHSIS 2010 Prov. 2011 FHSIS 2011 Prov.Report Report Report
30.1% 31.1% 49.3% 54.8% 51.1% 60.2%
50. It is noted that coverage by PhilHealth for the poor increased substantially withthe introduction of the NHTS-Poverty Reduction method. This comprises the poorestfamilies who had not been enrolled under the original LGU targeted program. TheNHTS data covered 48.5 percent of the poor in the 16 provinces. However, what isdifficult to determine is the quality of coverage under UHC or the quality of healthservices received by that population group which could be strengthened throughqualitative and quantitative surveys.
51. Given the lack of progress reports, it is difficult to attribute progress under the ECTF Grant. A substantial amount of policy, regulation and legislation has been approvedover the intervening years, yet the applicability and implementation of these is not knownor fully assessed. Some of these are related to the Quality Medicine Act of 2008 (whereenforcement by the Food and Drug Administration (FDA) is of concern); the PhilippineNational Drug Formulary which was incorporated under the Generics Act (before theGrant implementation period) to promote rational drug use and which formed the basisfor claim reimbursement for drugs and medicines from PhilHealth; and many others. Ofnote is the recently signed Responsible Parenthood and Reproductive Health Act of 2012by the President of the Philippines.
52. In parallel, achievements are noted in use of generic drugs (47 percent in 2003 to60 percent in 2010); facility based deliveries, reduction of chronic disease medication,increased number of nurses for community health services, performance monitoringthrough scorecards and standardization, among others. The Grant financed neededequipment and training, established the Inter-Local Health Zones (ILHZ) to make servicedelivery access more efficient, and rehabilitated a number of health centers. The 2012EC evaluation states that the health mapping exercise (rationalization plans) was lesseffective as patients were assigned to health centers which proved to be farther afield thana health center next door.
14
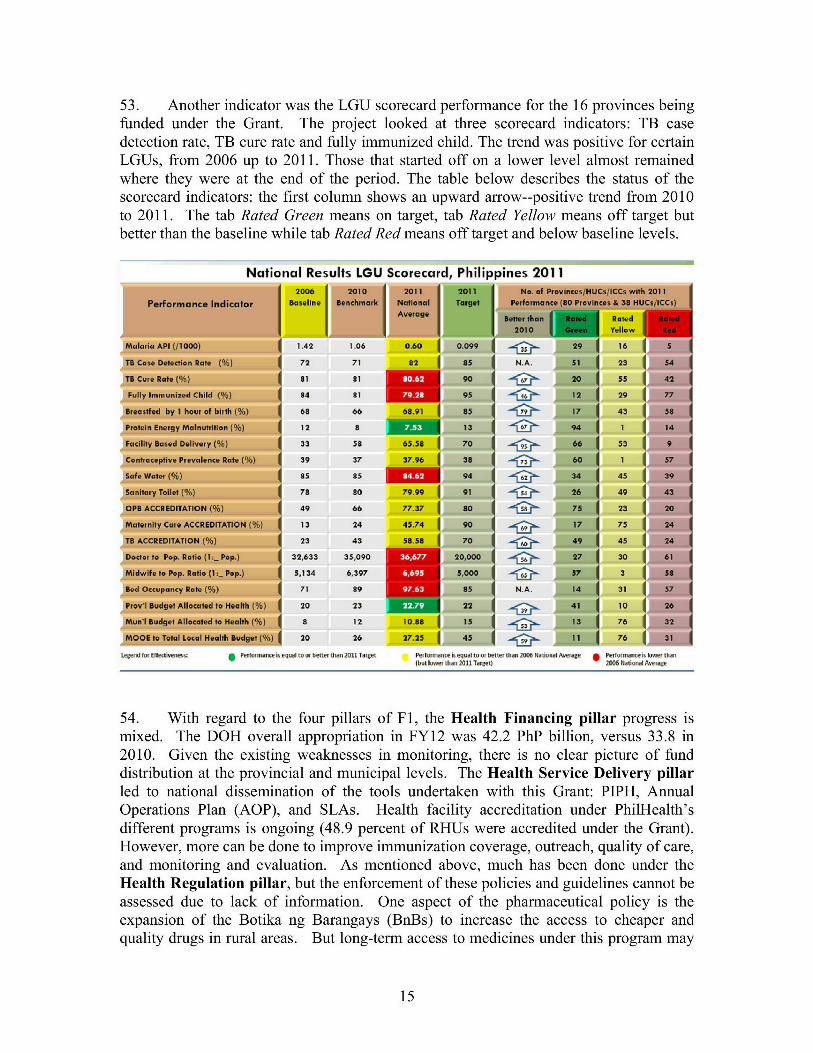
53. Another indicator was the LGU scorecard performance for the 16 provinces beingfunded under the Grant. The project looked at three scorecard indicators: TB casedetection rate, TB cure rate and fully immunized child. The trend was positive for certainLGUs, from 2006 up to 2011. Those that started off on a lower level almost remainedwhere they were at the end of the period. The table below describes the status of thescorecard indicators: the first column shows an upward arrow--positive trend from 2010to 2011. The tab Rated Green means on target, tab Rated Yellow means off target butbetter than the baseline while tab Rated Red means off target and below baseline levels.
National Results LGU Scorecard Phl ippines 20112006 The 20" 201 2b, verss 38 MI
PeroranlanPic )or aseline TyaccretatIMO
= J 100 I= Yellow
Malaria API (/1000) 1 42 1.06 0.60 0.099 2 9 16
TO Case Deection Roe %a 72 71 82 85 N A.uzi 23
T Cumo Rtorig 81 e1 90 m20 a3
Fully IRnummed Child ai4 o 95 12 29
aiseed dy I hue o lack ofA, i68 66 68.91 85 p17- A 43 i
ProtD Energy Mafutiotn (% n 12 a 13 c9t4 t c
Fadlity Bsrd Del inry (% ra33 ao 65.58 70 66 33
1Conbraceptive Prvalonce Rate (39 37 37.96 30 -60A 1
Safe Water (% 85 a5 94 34_ 45
i a d yTole ()78 80 79.99 91 26949
OPB ACCREDITATION (%A) 49 66 77.37 80 75 -A 231
MaternIty Care ACCREDITATION () 13 24 45.74 90 -17- 75
TB ACCREDITATION 1%) 23 43 58.58 70 49 45
Doc. o .... to Pop, Ratio (1.-_ Pop ) 32,633 35,090 3667 20,000 27 30
MIIdwi*e to Pop. Rail* [h: Pop.) 5,134 6,397 6,000 57oo 1
11.d Oc-parwY Rat(% 71 SQ 97685 N.A. 14 31
ProVI BWdget Allocated to Health {} 20 23 2241 1
Mun'l Bud"e Allocated to Health %) 8 12 10.88 15 -1 3 76 1
MOOE to Trtal Local Health BMdgt(% 20 26 V7.25 45 11 76
Legnd ar ffetivnes: g Pe"orm-Ncisqual towu bcttm1 hdn 2011 Taiget Perfonanc i, 1qu1 to- od bem, thn 2006 Natinal A-Verag Perfornianceh lao- than(but lOweF than 2011 Taret) 2006 National Averate
54. With regard to the four pillars of Fl, the Health Financing pillar progress ismixed. The DOH overall appropriation in FY12 was 42.2 PhP billion, versus 33.8 in2010. Given the existing weaknesses in monitoring, there is no clear picture of funddistribution at the provincial and municipal levels. The Health Service Delivery pillarled to national dissemination of the tools undertaken with this Grant: PIPH, AnnualOperations Plan (AOP), and SLAs. Health facility accreditation under PhilHealth'sdifferent programs is ongoing (48.9 percent of RHUs were accredited under the Grant).However, more can be done to improve immunization coverage, outreach, quality of care,and monitoring and evaluation. As mentioned above, much has been done under theHealth Regulation pillar, but the enforcement of these policies and guidelines cannot beassessed due to lack of information. One aspect of the pharmaceutical policy is theexpansion of the Botika ng Barangays (BnBs) to increase the access to cheaper andquality drugs in rural areas. But long-term access to medicines under this program may
15
only be sustainable with increased investments, routine supervision, monitoring andsupport systems. The Good Governance pillar was successful in standardizing andinstitutionalizing the PIPHs, the AOPs, and the rationalization process of the healthsystems. The Grant further developed on the Expenditure Tracking System (which stillremains at a more central level), and the Electronic National Government AccountingSystem (e-NGAS), was still being used at the decentralized level. Separately, the ECfunded additional work on public financial management at both the national and locallevels through separate funding. These included work with DBM on implementing PEFAat the sub-national levels and assisting Grant LGUs come with their own PFMdevelopment plans.
3.3 Efficiency
55. Net present value, economic and financial rate of return, or cost-effectiveness wasnot calculated a priori for the grant. Nevertheless, overall national health spendingprovides a mixed picture. Out-of-Pocket (OOP) spending continues to be the largestsource of health spending (54 percent). However, since the election of the newgovernment, there is a strong commitment to increasing health spending with a relatedincrease in the DOH's budget which has risen significantly- from PhP 31 billion in 2011,to PhP 42 billion in 2012, and PhP 53.8 billion in 2013. An increasingly larger share ofDOH's budget goes to financing premium for indigents - from PhP 3 billion in 2011 toPhP 12.6 billion in 2012. There is also an increase of financing share of public healthprogram out of total government health spending (33.7 percent in CY2007 to 44.7percent in CY2013). Prior to the grant, the share of public health program out of thegovernment health spending (excluding staff salary) was 25 percent, while 65 percentwent into hospital operations.
56. The efficiency of grant execution through the measurement of disbursement washigh, given the block grant nature of the disbursement tranches. However, efficiency wasdampened by the DOH's inability to disburse the amounts in a timely manner and thesevaried between the provinces (disbursement to the ARMM provinces was much delayed)given the processes impacting project supervision outlined earlier). In addition, the DOHwas not able to fully track expenditures with associated outcomes.
3.4 Justification of Overall Outcome RatingRating: Moderately Unsatisfactory (MU)
57. The overall outcome rating is moderately unsatisfactory based on substantialrelevance, modest efficacy, and modest efficiency. While the Grant supportedimprovements to health delivery and LGU performance through the use of scorecards,including capacity building efforts at the DOH, there is a lack of data that shows higherutilization of health services by the poor. Nor is there data to indicate that OOP paymentshave been reduced. Poor households were only enrolled in April 2011 and PhilHealth hasonly recently enhanced its benefits packages which would ensure better financialprotection. In addition, though the NSSHRP and the Grant made available needed publichealth goods, data for the priority public health targets were not fully met. Tools
16
developed under the Grant were semi-institutionalized, but more will be required,particularly in linking performance with outcome.
3.5 Overarching Themes, Other Outcomes and Impacts
(a) Poverty Impacts, Gender Aspects, and Social Development
58. The Grant focused on making healthcare accessible to the poor in convergenceprovinces. Despite the lack of progress reports from the Recipient's side, activities werecarried out for the most part: healthcare was strengthened through renovation ofhealthcare facilities; training; purchase of needed equipment was allocated at servicedelivery entry points; and Basic, and Comprehensive Emergency Obstetric and NewbornCare (BEmONC/CEmONC) services were reinforced. Equipment for blood banks wasprovided, dental services, and basic healthcare packages were provided throughPhilHealth allowing the most vulnerable to gain access to primary care. The ECevaluation report notes that IP were not sufficiently consulted on their needs, and datafrom a Catchment and Case Flow Analysis carried out by the EC TA team shows that theIPs have less access to primary health care, however the report does not state how manyprovinces this was carried out in.
(b) Institutional Change/Strengthening
59. The Grant contributed to strengthening the delivery of health services through therehabilitation of health care centers, and funded training and needed equipment andgoods. The Grant also provided variable tranche releases to award good performingLGUs, increasing competition to improve service delivery, and institutionalized the useof planning and implementation tools, which increased cooperation and collaborationbetween the LGUs and the DOH. However, several weaknesses remain. There areinsufficient funds for the maintenance of the health system overall, and more particularlyin infrastructure. The rationale behind the DOH implementing the Health FacilityEnhancement Program (HFEP) was as a one-time capital investment to complement theincreased financing provided by PhilHealth. There is a need to increase the focus andeffort on prioritizing activities, and providing a more robust rationale for investment inthe sector based on solid data. The DOH would need to make more efficient use ofresources, responding more to demand rather than supply. In addition, a focus on actualhealth delivery rather than on health infrastructure, and increased performance throughimpact evaluation so that the information can be used for sound policy and decision-making would be warranted. Funding was available under the Grant to strengthenDOH's capacity; however, there was a missed opportunity as funds were not used tostrengthen procurement capacity, or to strengthen the M&E system.
(c) Other Unintended Outcomes and Impacts (positive or negative)
60. The original design of the project incorporated a means test to identify the poor:Community-Based Monitoring System (CBMS). The Department of Social Welfare andDevelopment (DSWD) also had a means testing system. The LGUs defined who the poorwere using the systems they had. However, when PhilHealth scaled-up health insurance
17
for poor families, using the National Household Targeting System for Poverty Reduction(NHTS-PR), the LGUs resisted as the list of the poor did not match between the NHTS-PR and the list provided by each LGU. This has caused some deep seated sensitivity inhaving to remove the non-NHTS-PR beneficiaries from the LGU list. This was the firsttime in the Philippines that a refined targeting mechanism, based on well-accepted proxymeans test (PMT) methodology was available, and was disseminated to all socialassistance programs. PhilHealth had to cross-match the list generated through the NHTSwith the existing list of sponsored members. Other issues had to be resolved such as theLGU cost sharing arrangement under the NHIP.
61. This was a significant policy success as it led to enrolment of around 5.2 millionfamilies (approximately 20 percent of the population). Use of the NHTS also paved theway for the government's scale-up of universal health care (UHC).
3.6 Summary of Findings of Beneficiary Survey and/or Stakeholder WorkshopsN/A
4. Assessment of Risk to Development OutcomeRating: Substantial (S)
62. The government is committed to UHC, and the law No. 10351 "An ActRestructuring the Excise Tax on Alcohol and Tobacco Products", was signed in lateDecember 2012. The additional revenues from the Sin Tax Bill are expected to be usedto fund UHC enrolment and health expenditures for prevention and promotion. Inaddition, the DOH budget was increased by 44 percent from 2010 to 2011 to cover anenhanced premium of PhP 2400 (US$54) for all National Household Targeting System -Poverty Reduction (NHTS-PR) targeted poor households. The 2013 budget includes PhP13.8 billion (approximately US$305 million) to cover the remaining households under theNHTS-PR. The LGUs now need to be convinced that the NHTS-PR method willcorrectly identify the most vulnerable populations. The DOH needs to better organize itsrole and accountability in light of the experience under the Grant, and solidify the toolsdeveloped, and improve efficiency and effectiveness of services to the population.
5. Assessment of Bank and Recipient Performance
5.1 Bank Performance
(a) Bank Performance in Ensuring Quality at EntryRating: Moderately Unsatisfactory (MU)
63. The Grant was in supplement to the NSSHRP. Therefore a Quality at Entryassessment was not carried out as the Grant tagged onto the same institutional andimplementation arrangements that were in place under the NSSHRP, through a GrantAgreement. The Grant was targeted originally to six provinces to pilot the reform of F 1,and the Bank was contracted by the Donor to carry out the supervision as those provincesrequired closer financial and procurement management. The Administration Agreementwas signed between the EC and the World Bank in April 2007. There was no preparation
18
phase per se, as both the NSSHRP and the Grant were being prepared and implementedduring the same period (NSSHRP was under implementation since March of 2007 andthe Grant became effective in June 2007). The Grant applied the same implementationformat as the NSSHRP. Both the project and the Grant experienced serious delays. As inboth the project and the Grant, there was insufficient attention to how implementationwould be undertaken. The Grant relied on the existing governmental structure anddecentralization of service delivery, but there was insufficient attention to the existingcapacity of both the DOH and PhilHealth in implementing the reform program.
64. In addition, there was little assessment as to the participation of the LGUs, theircapacity and willingness to participate in the reform process, particularly in light of whatoccurred on the ground with the use of the CBMS and the national program using NHTS-PR.
65. The Bank carried out a financial and procurement assessment of the ARMMprovinces in 2008, which was delayed due to the resurgence of conflict, but wassubsequently completed in October 2009. These delays meant that the ARMM provinceswere unable to complete their 2011/12 SLAs in time as the closing date was not extendedand closed in October 2012.
(b) Quality of SupervisionRating: Moderately Unsatisfactory (MU)
66. There were shortcomings in the quality of the Bank's supervision. The teamcarried out detailed supervision reviews of the Grant in early 2008 and 2009, raisingsome of the more serious concerns and requesting government response. However, thisattention became less concentrated with the changes in Bank task management over thelifetime of the Grant. There was a notable shift from detailed supervision of activities toa focus on disbursement of Grant proceeds, with increased assistance in procurementsupport to the detriment of closer operational supervision. The team did not avail of thetools at its disposal when faced with non-compliance of fiduciary aspects, which mighthave triggered a respect for the legal clauses in the Grant Agreement (submission oftimely audits, and financial management reports, procurement reports, and progressreports). There are no government/Implementing Agency progress reports in the files.Based on an EC report of November 2010, the provincial Annual Operations Plans(AOP) approvals had improved substantially over time and the 2010 AOPs for the 16provinces were endorsed in December 2009. The EC delegation mission notedimprovements in results as outlined in the SLAs (TB detection rate partly achieved at 89percent for 6/10 provinces; TB cure rate of which 7 provinces had performed better thanthe national average; breastfeeding within one hour after birth was partly achieved with 7provinces outperforming from the national average).
67. The joint missions that took place could have been further strengthened withindividual missions and more in-depth reporting, particularly in the latter part of theimplementation period. The last progress report from the World Bank to the ECidentified in the files was dated September 30, 2011. The status primarily relies onfinancial information rather than a progress report on activities, outputs, and outcomes.
19

68. There was detailed follow-up by the fiduciary teams on financial and procurementmanagement and the files are populated with approved procurement plans, AOPs, IFRs,etc. However, procurement reports lack an in-depth description of what was achieved.The third party verification focused primarily on scorecard performance and assessmentof procurement and financial management systems. Workshops were held onprocurement orientation following the new and revised harmonized procurementdocuments (Resolution No. 06-2010). Nevertheless, it was noted that turn-around time ofprocurement undertaken by the LGUs was quite long and drawn out, requiring multiplelevels of review (LGU to CHD, submitted to DOH through the Bureau of InternationalHealth Center) and finally to the Bank for prior review, taking a total of 3-6 months orlonger to complete the cycle. The restructuring could have tried to mitigate some of theissues, particularly if a Mid-Term Review of the Grant had been held in mid-course.
(c) Justification of Rating for Overall Bank PerformanceRating: Moderately Unsatisfactory (MU)
69. UHC had not been a national policy at the time of the Grant, and therefore, theobjective of expanding the Fl reform to key provinces was justified, particularly withadditional assistance to DOH to put in standards and tools for prioritization andrationalization of services. Following the Mindanao peace process, it was logical toinclude ARMM provinces in the Grant activities. The assessment on feasibility of successrelied on the preparation and implementation arrangements of the NSSHRP. Both theproject and the Grant suffered from the same weaknesses with lack of reporting andfollow-up on outcomes, and more in-depth supervision.
5.2 Recipient Performance
(a) Government PerformanceRating: Moderately Unsatisfactory (MU)
70. The government made a decision to adopt NHTS and introduced it nationally.This had an impact on the ability to pilot and learn from implementation of the reform.In parallel, the LGUs argued to retain their own methods of identifying the poor, andwere paying for premiums out of public funds. PhilHealth attempted to convince theLGUs to adopt the NHTS with little success. There was an unsatisfactory compromisebetween the LGU and the government, and currently, two parallel systems exist to covertwo sets of populations. The premium of the poor identified by NHTS is paid for by thegovernment, while the premium of the "poor" identified by LGU method is paid for byLGUs, though the target population is not the most vulnerable. The decentralization didnot lend itself to successful achievement of health delivery services, and though 5.2million households have been reached by PhilHealth, there is no clear evidence howUHC is improving the health of the most vulnerable.
20

(b) Implementing Agency or Agencies PerformanceRating: Moderately Unsatisfactory (MU)
71. Decentralization brought its own challenges, and both the DOH and the LGUs,through the CHDs, were unable to tackle some of the more contentious issues. The DOHhad problems in its own organization to be effective, and human resource constraints andabsorptive capacity led to many delays in project implementation. The DOH ran intodifficulties with the DBM, due to lack of clarity of roles and responsibilities (the DOHdealt with two offices in the DBM: a bureau in charge of the DOH as a whole, and aseparate Project Management Office in charge of the EC Grant), which led to furtherconfusion on the interpretation of issuances, response to DOH requests, etc.. In addition,personnel changes within the DBM led to implementation difficulties. Several issueswere raised early in the project by both the EC and the World Bank. But due to lack ofreporting from DOH on progress on the ground, questionable data and evaluationmethods, it is not clear how problems were addressed and resolved. Audit reportrecommendations describe a wide array of issues. As an example, in a 2010 audit report,it was noted that for the 2008 AOP, 67 percent of activities had not been completed(enrollment of indigents, procurement of TB laboratory equipment, rabies vaccines,among others). On a number of levels, the audit report reiterated the need for DOH toreview its ability to manage a large influx of funds, and the need to timely release fundsso that the provinces could provide the benefits needed to their population and fulfill theirSLAs. One province received funds for the 2008 SLA which were budgeted under arequest for Supplemental Budget 2009, and only received in December 2009. One of theaudits found that there were also anomalies in dispensing funds at the provincial level,with Medical Officers acting as Special Disbursement Officers, which was contrary tosound practices.
72. In addition, it is difficult to determine the participatory approach that occurred aspolarization between the LGUs and government/PhilHealth methods led to a conflict ofscope and result which has not been resolved to date. It was noted that the DOH didinvolve the CHDs later on in the approval process of LGU plans, but not in the process ofthe initial PIPH development, which may have caused some confusion initially. TheDOH did not carry out sufficient overall supervision of the Grant activities in theprovinces and municipalities. In addition, the coverage and impact of services weredifficult to determine due to the weakness of the monitoring and evaluation system, andtracking of expenditures. Oversight and management of health sector delivery remainedweak due to the structural organization which was reactive, having to constantly adjust to
reform parameters.
73. Weak communication in imparting the requirements of the reform led to delays inLGUs fulfilling and accurately preparing their SLAs. This became clearer once scoresprovided on achievements of the SLA performance targets were provided with theircorresponding tranches. In 2008, LGUs were allowed by the DOH to select some of theSLA indicators. Several LGUs admitted that selected indicators were based on what wasmost doable and achievable. This led to a standardization of indicators to be monitoredstarting in 2009. A noted problem was the selection of indicators and inconsistency with
21
what was actually being collected in the field. In addition, and as noted above, therewere also delays in disbursement/tranche release which led to delays in implementationand achievements of SLA targets (particularly for large provinces like Pangasinan[not aproject site but part of the original 16 convergence provinces], with 44 municipalities and4 cities, placing them at a disadvantage since it took them longer to implement province-wide interventions).
74. The latter years have seen much work done with regard to procuring neededmedical equipment, commodities, training of staff, organization of services, andidentification and incorporation of the poor into PhilHealth. However, with no record ofprogress report on the Recipient's side, it is difficult to determine the extent theseactivities have had on service delivery.
(c) Justification of Rating for Overall Recipient PerformanceRating: Moderately Unsatisfactory (MU)
75. The Grant was seriously delayed in implementation. Once the bottlenecks werecleared, implementation started at full steam, though there were still some issuessurrounding the realism and achievability of the SLAs and PIPHs. The delays also meantthat provinces, particularly ARMM provinces, were urgently trying to complete allactivities before Grant closure. Overall governance could have been improved and toolsmore systematized in order to monitor and evaluate progress and quality of data.
6. Lessons Learned
76. Use of country systems in National Program Support Operations to ensureownership and continuity of reforms: The Grant under review was provided to the WorldBank as a fiduciary agent for a work program that required closer follow-up andmonitoring. The instruments used under the Grant required a steep learning curve,compounded by the complication of learning new systems (financial and procurementmanagement of an entity outside of governmental agencies), and lack of a coherentnational implementation framework. Due to the devolution of delivery of healthcareservices, and the reigning political and social contexts, the DOH could have used aportion of the Grant to ensure compliance with country systems through increasedtraining and supervision, while strengthening ownership of the reforms as well asaccountability. Ownership and accountability need to be served by robust systems ofmanagement, oversight, and monitoring and evaluation in order to benefit the continuityof services and reforms engaged under this Grant. The M&E framework needs to bedeveloped with full partnership of all agencies to make it a viable system, and which canbe further developed and strengthened over time.
77. Strengthening results and policy focus of National Program Support: Budgetsupport operations provide the opportunity to link policy dialogue with outcomes andresults when well managed. However, in the case of the Grant, variable tranche releaseswere used to promote results achieved, and putting agencies in competition to increaseperformance and apply, in this case, national policies to improve access to health for the
22
poorest populations. This was less successful under the Grant due to a weakenedgovernance structure. However, the framework and model introduced new behavioursand challenged implementing agencies to look toward a more goal oriented approach,rather than a short-term physical approach.
78. Increased capacity building to ensure that decentralized services respond tosupply and demand. The Grant was provided through the DOH which funneled the fundsto the LGUs at the decentralized level. A clearer capacity and institutional assessmentwould have highlighted the issues surrounding the absorptive and implementationcapacities of both the DOH and LGUs in implementing the Grant and the nationalreforms. The Grant allocation could have better served the institutions involved inbuilding up their capacity through managerial, implementation, and monitoring andevaluation training so that Grant proceeds could have had more of an impact.
79. Strenjtheninj M&E focus: As mentioned above, the M&E framework requires afull participatory approach so that indicators that are relevant to monitor results andoutcomes are owned by those who will use them. A lesson from this Grant is how todesign and build a robust M&E system in an environment of decentralization, autonomy,and devolution of service delivery, where reporting is required for national programssuch as Universal Health Coverage, and more particularly when baseline was notavailable at the start of the operation. The Grant did not fully explore the data feedbackloop which requires concerted consultations with health professionals, administrators,financiers, and civil society, to engage in a dialogue on the baseline of health status, theinputs required to positively increase health outcomes, and to monitor the compact ofreaching those outcomes. The Grant did not outline methods of collection and qualitycontrol of data.
80. The need for monitoring and sharing of information to make a useful contributionto mainstreaminZ improvements of healthcare delivery. The Grant was especially weakon reporting by governmental entities on implementation progress. Though reporting islikely done internally through the health sector, sharing of that information and thequality of that information with other agencies and partners has led to perceivedfragmentation of efforts and results. One aspect is the interpretation of indicators forimproved service delivery, when sights were focused on the physical aspects, and less onquality of care. Quality improvement models look at how services are being done, gapsin delivery of quality care, and remedial actions to improve service delivery. These neednot be purely physical, but more organizational, bottoms-up approach, participative, andowned by those directly involved in the delivery of care. On the other hand, agenciesinvolved in oversight/implementation are responsible for close monitoring andsupervision of technical and qualitative aspects of a project/grant, in order to gleanlessons and prompt feedback to improve delivery of services and exchanges to improvethe technical quality of supervision.
81. Strenthenin central-local relations, particularly in promoting the introductionof national programs: Any reform requires clear roles, rules and procedures so that alllevels of government agencies can work together within a clearly defined framework,
23
regardless of internal changes. Lack of clarity and accountability weakened the potentialof the Grant outcomes. Strong organization, management, and absorptive capacity willallow for better mainstreaming of activities as part of day-to-day business, particularly inthe context of major reforms. One innovation was LGU scorecards which provided theopportunity for healthy competition in service delivery; but without clear and transparentrules of business, this can be derailed, particularly if the incentives are not the right ones.
82. In the process of devolution for a country like the Philippines, third partyverification should also comprise performance and management audits to better informand resolve issues of implementation. The third party verification was a financial audit.This could have been supplemented with a performance and management audit todetermine where the bottlenecks were, issues to be resolved, and improvements made toimplementation. The number of governing bodies, and the autonomous set-up of LGUs,did not lend to full cooperation and collaboration. A performance and management auditcould have brought together the parties toward a more proactive solution toimplementation.
7. Comments on Issues Raised by Grantee/Implementing Agencies/Donors
(a) Grantee/Implementing agencies
83. Comments were not received from the DOH as of the date of this report.
(b) Cofinanciers/Donors
84. The mission met with EU representatives on October 18, 2012. The following arecomments made.
a) Validity of the data received is in question given differing numbers from varioussources. The trend is consistently poor on quality of data. An example is theMaternal Mortality Rate (MMR), though there has been little progress in the lastdecade. Provincial data does not collect for MMR. A proxy indicator would bebirths by skilled attendant. However, this may be underreported.
b) Government would need to do a yearly verification for quality of data.c) Surveys do not always disaggregate by province (only by regions).d) Improved scorecard for certain provinces. The efforts made had some positive
effects.e) Political commitment matters in order to ensure good capacity building for the
LGUs. LGU performance varies greatly.f) Little effort in a feedback loop to ensure that performance is discussed and
improved.g) Province-wide Investment Plans for Health were bottom-up. Needs assessments
could have been strengthened at the municipal level to ensure that the Province-wide Investment Plans responded to actual needs. Politics intrude in the goodfunctioning of this approach.
h) The PIPH process could have been improved with greater attention and focus onthe priorities, with full participation from all stakeholders.
24
i) Provinces that had access to the EC technical assistance fared better than thosethat did not due to proximity of expertise.
j) The EC technical assistance had a positive effect in being the communicationlinks between the LGUs and the DOH.
k) An absorption capacity at the level of DOH was noted. DOH has engaged intotoo many initiatives, without regard to the number of staff needed to carry outthose tasks. There has been a severe reduction of DOH staff in the last year.
1) DOH managers are far too preoccupied with other activities to be able to focus onthe core functions required by the DOH.
m) Despite the reorganization, the internal environment is not conducive for effectiveworking relationships or results, nor with donor coordination, but priorities lieelsewhere, which leads to ineffective use of funds or outcomes.
n) Donors need to engage in a broader spectrum of activities rather than focus oneach individual agenda, so as to be able to promote a more coordinated andcoherent approach. However, the DOH needs to be in the driver's seat for this toeffectively happen.
o) Infrastructure is poor which is why the Grant financed rehabilitation, but there isin parallel little maintenance of the infrastructure, differing designs, lack ofstandards, and lack of resources to maintain the infrastructure overall.
p) The health mapping exercise was not used by all provinces, with little follow-upto ensure consistency of use and application.
q) Despite good relations with the World Bank, there was little informationexchange (only two reports were received: 2009/20 10 and in 2011). Financialreports were received but with little substance. Province audits were not received.There was also lack of technical support to the DOH to facilitate implementationof program activities.
r) Operational meetings were held between the World Bank the EC, and the DOHfrom the start of the project. The technical coordination meeting minutes wereshared. There was an open dialogue. However, all of this could have beenfacilitated through better reporting.
s) A recommendation was to share aide-memoire with partner agencies.
(c) Other partners and stakeholdersN/A
25
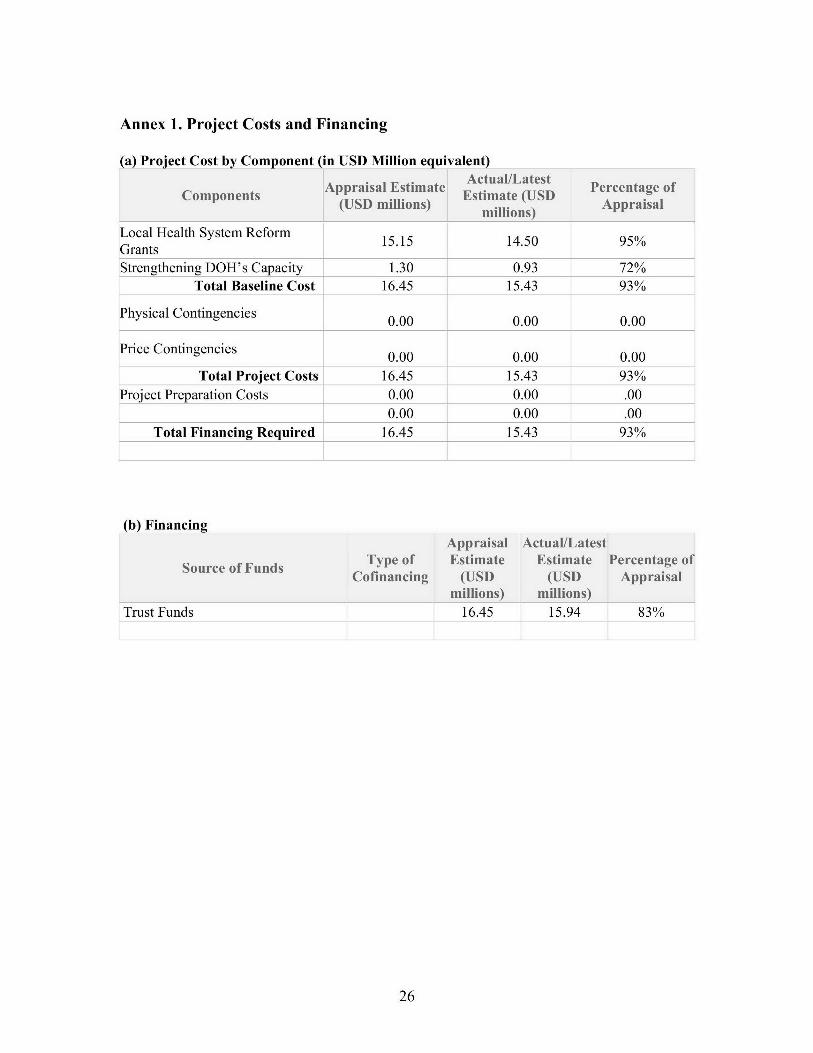
Annex 1. Project Costs and Financing
(a) Project Cost by Component (in USD Million equivalent)Actual/Latest
Appraisal Estimate Atulate Percentage ofComponents (UDmlin) Estimate (USD Apria
(USD millions) millions) Appraisal
Local Health System Reform 15.15 14.50 95%GrantsStrengthening DOH's Capacity 1.30 0.93 72%
Total Baseline Cost 16.45 15.43 93%
Physical Contingencies 0.00 0.00 0.00
Price Contingencies 0.00 0.00 0.00
Total Project Costs 16.45 15.43 93%lProject Preparation Costs 0.00 0.00 .00
0.00 0.00 .00Total Financing Required 16.45 15.43 93%
(b) FinancingAppraisal Actual/Latest
Type of Estimate Estimate Percentage ofCofinancing (USD (USD Appraisal
millions) millions)
Trust Funds 16.45 15.94 83%
26
Annex 2. Outputs by Component
Progress reports on the Recipient side have thus far been unavailable to complete thissection with detail
What this section can speak to is that Part A banked on the strength of Fl as a morecomprehensive approach to health reforms which were aligned with public expendituremanagement and governance reform. Using the medium-term Health Sector ExpenditureFramework (HSEF), and the annual budgeting process, a performance monitoringframework for DOH, PhilHealth and convergence provinces linked budgeting andresource allocation to outputs and intermediate results. These links were intended toreduce obstacles to reform. With regard to fragmentation in financing, SectorDevelopment Approach for Health (SDAH) was adopted under Fl to align developmentpartners-supported reform activities across the entire health sector under a single nationalimplementation plan and under harmonized local health investment plans in eachconvergence provision.
Investment plans took three years to develop (started 2006). Once these were completed,the SLAs were established in 2008. However, the LGU investment plans were by thenoutdated but the "approved" activities not amended, and these activities were funded(except for facility upgrades and equipment which underwent a re-review). The DOHconducted an analysis on the problems and issued guidelines on how best to preparePIPH for the future.
Procurement Plans (PP) were established for each region. As there are no progressreports from the Recipient side, one can review each provincial PP for what was intendedto be purchased and approved under the Grant. Without going into great detail for eachof the provincial PP as these are exhaustive and were prepared and approved on a yearlybasis, key items under the PPs were for information technology equipment, medicalequipment, dental equipment, obstetric medical equipment, civil works, maintenanceequipment, office equipment, general goods, community-based grants (workshops forskilled and birth attendants, course on community-IMCI, courses on child care andnutrition, workshop on adolescent reproductive health...), laboratory equipment, medicalsupplies, etc.
The government took the not-yet-implemented pilot and scaled it up to 23 provinces in2008 and then to 81 provinces in 2009. The JAC was overloaded. In 2007, the ECrequested the Bank to include additional provinces (ARMM). This led to a burden for theDOH to manage the Grant.
DOH was provided with funding under Part B to implement public financial management(PFM), and capacity building in fiduciary areas. DOH was responsible for tracking theperformance of LGUs through mechanisms established under the reform (investmentplans, annual operation plans, training plans, project procurement and management plans,and Service Level Agreements). However, this took a substantial amount of time todevelop, establish, approve, and institutionalize, which led to serious delays in
27
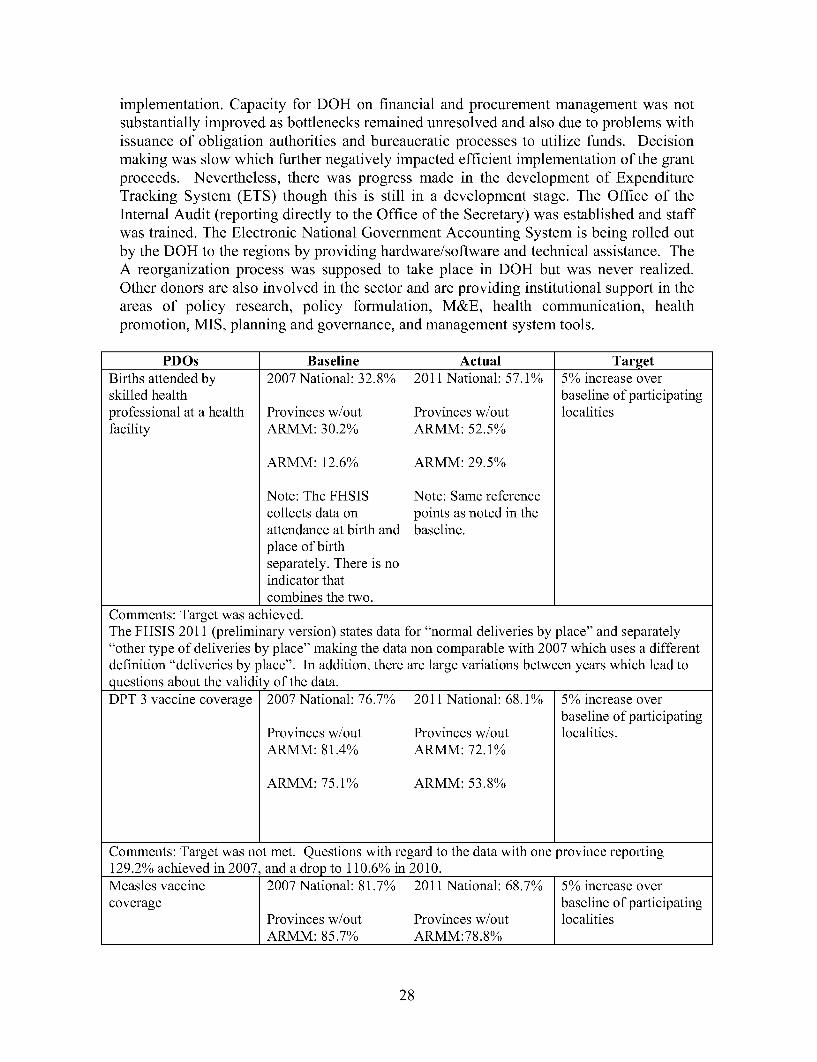
implementation. Capacity for DOH on financial and procurement management was notsubstantially improved as bottlenecks remained unresolved and also due to problems withissuance of obligation authorities and bureaucratic processes to utilize funds. Decisionmaking was slow which further negatively impacted efficient implementation of the grantproceeds. Nevertheless, there was progress made in the development of ExpenditureTracking System (ETS) though this is still in a development stage. The Office of theInternal Audit (reporting directly to the Office of the Secretary) was established and staffwas trained. The Electronic National Government Accounting System is being rolled outby the DOH to the regions by providing hardware/software and technical assistance. TheA reorganization process was supposed to take place in DOH but was never realized.Other donors are also involved in the sector and are providing institutional support in theareas of policy research, policy formulation, M&E, health communication, healthpromotion, MIS, planning and governance, and management system tools.
PDOs Baseline Actual TargetBirths attended by 2007 National: 32.8% 2011 National: 57.1% 5% increase overskilled health baseline of participatingprofessional at a health Provinces w/out Provinces w/out localitiesfacility ARMM: 30.2% ARMM: 52.5%
ARMM: 12.6% ARMM: 29.5%
Note: The FHSIS Note: Same referencecollects data on points as noted in theattendance at birth and baseline.place of birthseparately. There is noindicator thatcombines the two.
Comments: Target was achieved.The FHSIS 2011 (preliminary version) states data for "normal deliveries by place" and separately"other type of deliveries by place" making the data non comparable with 2007 which uses a differentdefinition "deliveries by place". In addition, there are large variations between years which lead toquestions about the validity of the data.DPT 3 vaccine coverage 2007 National: 76.7% 2011 National: 68.1% 5% increase over
baseline of participatingProvinces w/out Provinces w/out localities.ARMM: 81.4% ARMM: 72.10%
ARMM: 75.1% ARMM: 53.8%
Comments: Target was not met. Questions with regard to the data with one province reporting129.2% achieved in 2007, and a drop to 110.6% in 2010.Measles vaccine 2007 National: 81.7% 2011 National: 68.7% 5% increase overcoverage baseline of participating
Provinces w/out Provinces w/out localitiesARMM: 85.7% ARMM:78.8%
28
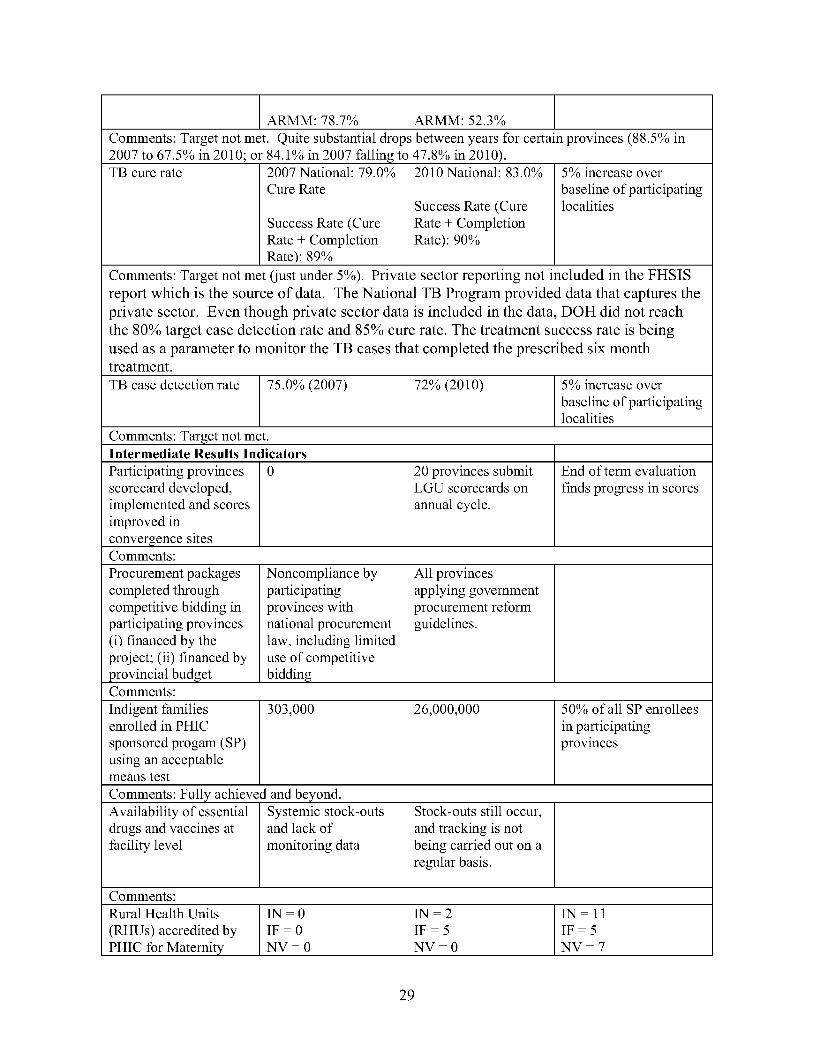
ARMM: 78.7%. ARMM: 52.3%]Comments: Target not met. Quite substantial drops between years for certain provinces (88.5% in2007 to 67.5% in 2010; or 84.l1% in 2007 falling to 47.8% in 2010).TB cure rate 2007 National: 79.0% 2010 National: 83.0% 5% increase over
Cure Rate baseline of participatingSuccess Rate (Cure localities
Success Rate (Cure Rate + CompletionRate + Completion Rate): 90%Rate): 89%
Comments: Target not met (just under 5%). Private sector reporting not included in the FHSISreport which is the source of data. The National TB Program provided data that captures theprivate sector. Even though private sector data is included in the data, DOH did not reachthe 80% target case detection rate and 85% cure rate. The treatment success rate is beingused as a parameter to monitor the TB cases that completed the prescribed six monthtreatment.TB case detection rate 75.0% (2007) 72% (2010) 5% increase over
baseline of participatinglocalities
Comments: Target not met.Intermediate Results IndicatorsParticipating provinces 0 20 provinces submit End of term evaluationscorecard developed, LGU scorecards on finds progress in scoresimplemented and scores annual cycle.improved inconvergence sitesComments:Procurement packages Noncompliance by All provincescompleted through participating applying governmentcompetitive bidding in provinces with procurement reformparticipating provinces national procurement guidelines.(i) financed by the law, including limitedproject; (ii) financed by use of competitiveprovincial budget biddingComments:Indigent families 303,000 26,000,000 150%o of all SP enrolleesenrolled in PHIC in participatingsponsored progam (SP) provincesusing an acceptablemeans test_______________ _______________j
Comments: Fully achievd and beyond. __________
Availability of essential Systemic stock-outs Stock-outs still occur,drugs and vaccines at and lack of and tracking is notfacility level monitoring data being carried out on a
regular basis.
Comments:Rural Health Units IN - 0 IN - 2 I 11(RHUs) accredited by IF l 0 IF t i notPHIC for Maternity NV = 0 NV =0 NV-= 7
29
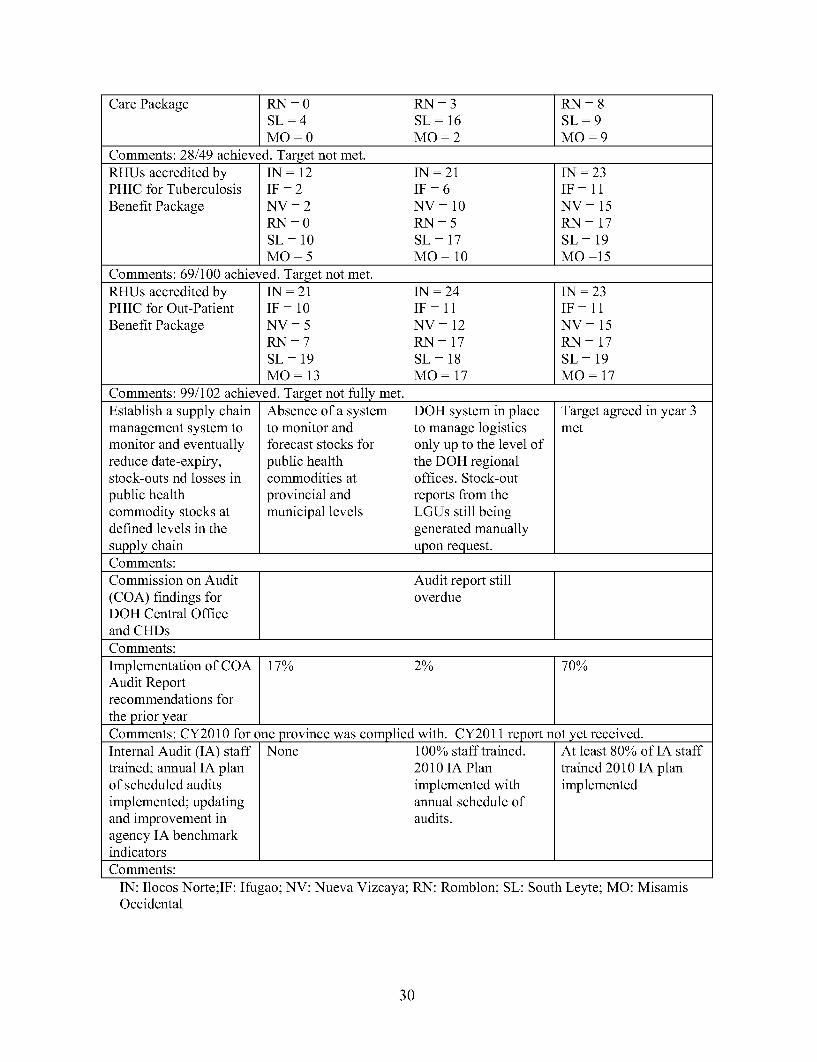
Care Package RN = 0 RN = 3 RN = 8SL=4 SL=16 SL=9MO=0 MO=2 MO=9
Comments: 28/49 achieved. Target not met.RHUs accredited by IN = 12 IN = 21 IN = 23PHIC for Tuberculosis IF = 2 IF = 6 IF = 11Benefit Package NV = 2 NV = 10 NV = 15
RN = 0 RN = 5 RN = 17SL=10 SL=17 SL=19MO=5 MO= 10 MO =15
Comments: 69/100 achieved. Target not met.RHUs accredited by IN = 21 IN = 24 IN = 23PHIC for Out-Patient IF = 10 IF = 11 IF = 11Benefit Package NV = 5 NV = 12 NV = 15
RN = 7 RN = 17 RN = 17SL=19 SL=18 SL=19MO = 13 MO = 17 MO = 17
Comments: 99/102 achieved. Target not fully met.Establish a supply chain Absence of a system DOH system in place Target agreed in year 3management system to to monitor and to manage logistics metmonitor and eventually forecast stocks for only up to the level ofreduce date-expiry, public health the DOH regionalstock-outs nd losses in commodities at offices. Stock-outpublic health provincial and reports from thecommodity stocks at municipal levels LGUs still beingdefined levels in the generated manuallysupply chain upon request.Comments:Commission on Audit Audit report still(COA) findings for overdueDOH Central Officeand CHDsComments:Implementation of COA 17% 2% 70%Audit Reportrecommendations forthe prior yearComments: CY2010 for one province was complied with. CY201 1 report not yet received.Internal Audit (IA) staff None 100% staff trained. At least 80% of IA stafftrained; annual IA plan 2010 IA Plan trained 2010 IA planof scheduled audits implemented with implementedimplemented; updating annual schedule ofand improvement in audits.agency IA benchmarkindicatorsComments:
IN: Ilocos Norte;IF: Ifugao; NV: Nueva Vizcaya; RN: Romblon; SL: South Leyte; MO: MisamisOccidental
30
Annex 3. Economic and Financial Analysis(including assumptions in the analysis)
This was a grant, and an economic and financial analysis was not included.
31
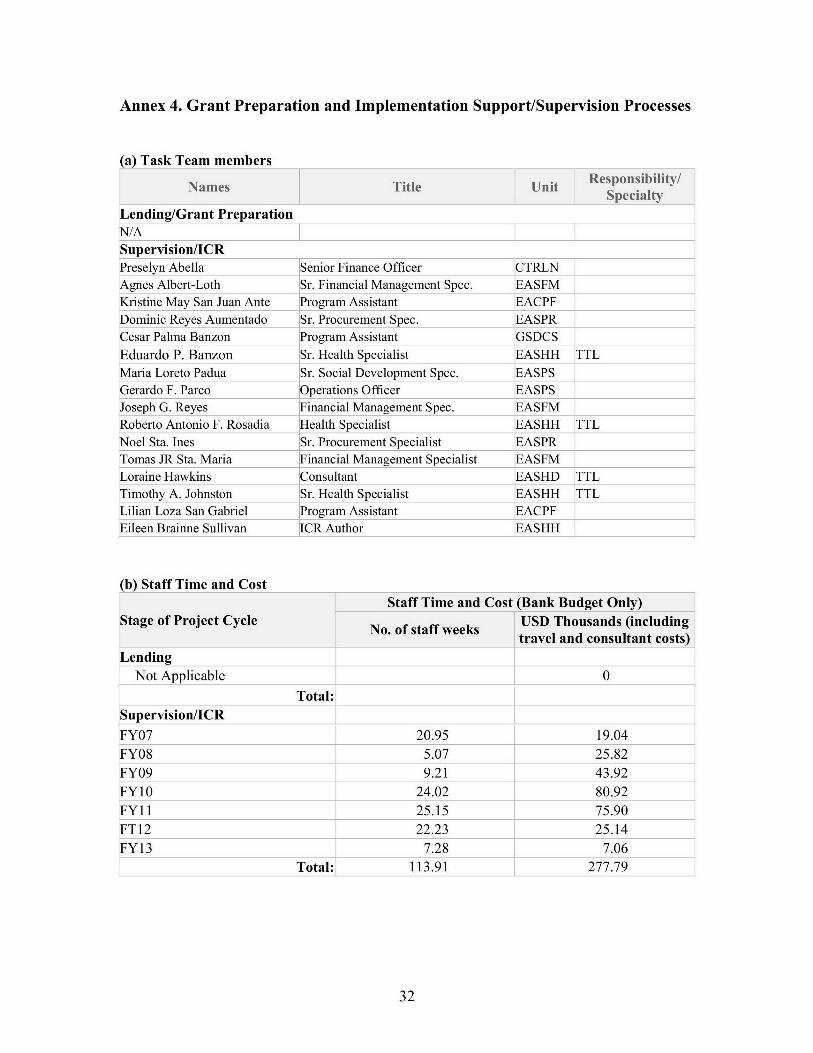
Annex 4. Grant Preparation and Implementation Support/Supervision Processes
(a) Task Team members
Names Title Unit RepniltySpecialty
Lending/Grant Preparation[N/ASupervision/ICRPreselyn Abella Senior Finance Officer CTRLN I
Agnes Albert-Loth Sr. Financial Management Spec. EASFM I
Kristine May San Juan Ante lProgram Assistant EACPF
Dominic Reyes Aumentado Sr. Procurement Spec. EASPRCesar Palma Banzon Program Assistant GSDCSEduardo P. Banzon [Sr. Health Specialist EASHH TTLMaria Loreto Padua [Sr. Social Development Spec. EASPS
[Gerardo F. Parco Operations Officer EASPS I
Joseph G. Reyes Financial Management Spec. EASFM I
Roberto Antonio F. Rosadia Health Specialist EASHH TTLNoel Sta. Ines Sr. Procurement Specialist EASPR
Tomas JR Sta. Maria Financial Management Specialist EASFM
Loraine Hawkins Consultant EASHD TTLTimothy A. Johnston Sr. Health Specialist EASHH [TTLLilian Loza San Gabriel Program Assistant EACPF I
lEileen Brainne Sullivan ICR Author EASHH
(b) Staff Time and CostStaff Time and Cost (Bank Budget Only)
Stage of Project Cycle USD Thousands (includingtravel and consultant costs)
[LendingNot Applicable 0
Total:Supervision/ICR
FY07 20.95 19.04
FY08 5.07 25.82FY09 9.21 43.92
FY10 24.02 80.92FY11 25.15 75.90FT12 22.23 25.14
_FY13 7.28 7.06Total: 113.91 277.79
32

Annex 5. Beneficiary Survey Results
(ifany)
NA
33

Annex 6. Stakeholder Workshop Report and Results
(ifany)
NA
34

Annex 7. Summary of Grantee's ICR and/or Comments on Draft ICR
Comments were not available at the time of the completion of this report.
35
Annex 8. Comments of Cofinanciers and Other Partners/Stakeholders
See section 7 (b).
36

Annex 9. List of Supporting Documents
1. World Bank Report of August 19, 2010: Project Annual Report for CY2007-2009.2. 2008 Accomplishment Report, Department of Health (2009).3. Mission Aide-memoires (various dates)4. Implementation Status and Result Reports (various dates)5. Consolidated Audit Reports (2009; 2010)6. Key Achievements and Challenges, European Union Delegation to the Philippines,
November 2010.7. Financing Agreement, June 2007.8. Field Health Services Information System (2007; 2008; 2010)9. COA Audit Reports (2009; 2010).10. Project Appraisal Document of the National Sector Support for Health Reform
Project (IBRD 73950)
37
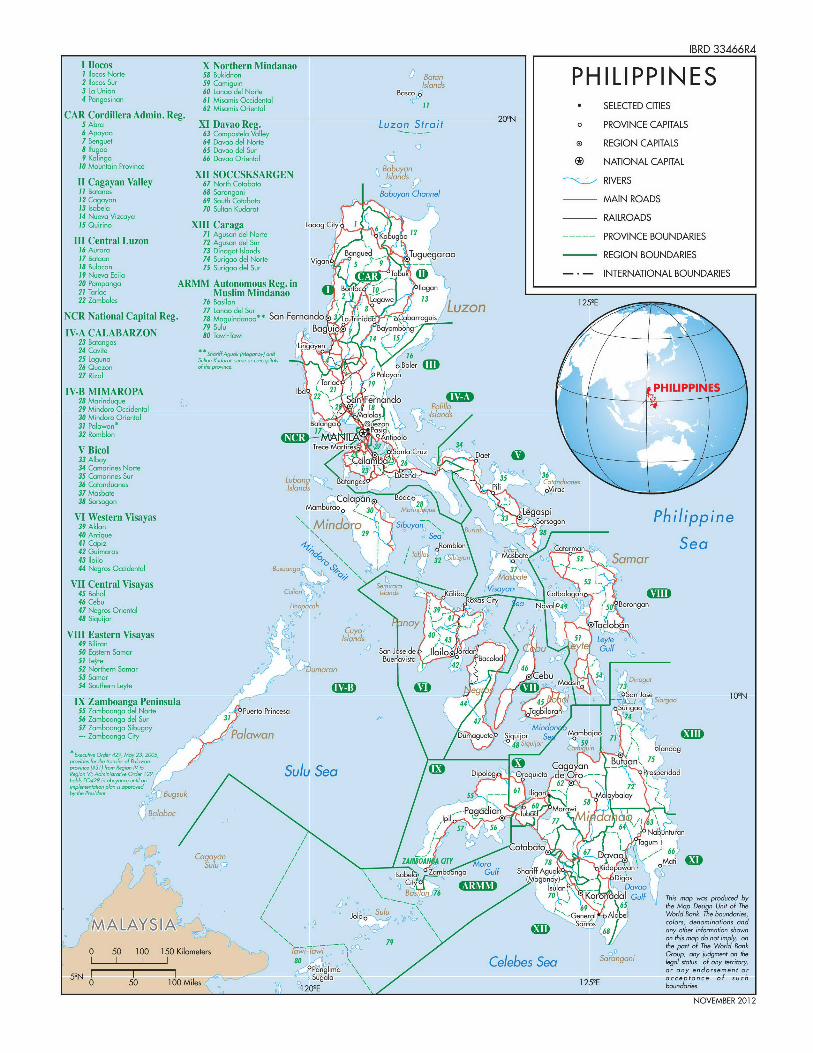
IBRD 33466RAI Ilocos X Northern Mindanao
I:ocos Norte 58 Bukidron Baton PH ILIPPIN ES2 locos Sur 59 Camiguin Islands3 La Union 60 Lanao del Norte BOscoa4 Pangasinan 61 Misamnis Occidentol Bso
62 Mis4ais Oriental I1 * SELECTED CITIESCAR Cordillera Admin. Reg. 20'N5 Abra XI Davao Reg. Luzon Strait o PROVINCE CAPITALS
6 Apayao 63 Compostela Valley7 Benguet 64 Davao del Norte e REGION CAPITALS8 Ifugo 65 Davao del Sur9 Kalingo 66 Davao Oriental B NATIONAL CAPITAL10 Mountain Province Babuyan
XII SOCCSKSARGEN IslandII Cagayan Valley 67 North Cotabato RIVERSII Batones 68 Sarangani Babuyan Channel12 Cagayan 69 South Cotabato a MAIN ROADS13 Isobelo 70 Sultan Kudarat14 Nueva Vizcaya - RAILROADSIS Quirino XIII Caraga Laoag City 6 1
71 Agunn ze Norte Kabugao ---- PROVINCE BOUNDARIESIII Central Luzon 72 Agusan dle Sur16 Acroro73 Dinagot Islcmcls
7 Bta 74 Srigo del Norte vgn Bnged Tuguegarao REGION BOUNDARIES18 Bulacon 75 Surigao del Sur Vign -19 Nuevo Ecija 7 S l u - - INTERNATIONAL BOUNDARIES20 Pampango ARMIM Autonomous Reg. in Banta- 1-' - Ilgan21 Tarlac Muslim Mindanao 2 - an22 Zambales 76 Basilan ag 1 zonI125E
NCR National Capital Reg. 78 M gind no ** San Fernando . L d d a78 agundaao* Sn Frnado3 L.,Tinidd-d bCaborroguis
IV-A CALABARZON 80 Tu,vi-Towi Baguio* 7 ong23 Batangas L a24 Cavite **Sh.,iffAguak (M.ganoynd Lin\I-yen25 Laguna SI-o Kat rvea cocaprca
26 Quezon o pc Baler27 Rizal Palayan
IV-B MIMAROPA 2ba ar lin FPHnlIPdPI28 Marinduque rS29 Mindoro Occidental ,2 8 t Pol11o30 Mindoro Oriental aloloJ slands
31 Palawan* Balonga e32 Romblon U*onpolo
V Bicol enta Cr Daet33 Al6cy 33Alalam a2 '26 ----- -34 Comarines Norte
3 e35 Comarines Sur La B uc 35 36
40 Aniu ny 29ana n unas .nc
36 Cotonccunes ludn 3 - l37 MMbste38 Sornogon Mo l and 2 , K
rooo LegaspiVI9 Eastern Visayas i Philippine
VI Wetenlisyam\ Mindoro SiyaN40 Antiqe2-;
41 C npi. J d o on c u Cetor Sea42 GuiNors oma Duma 4643 Saima * S a nar44 Negros Occidentol 1PN
VII Central VisayasCuinnlds - oo45 Bohol clel Norne PuroPicsqan I gao46 Ceboa del sea Nro9Boronga47 Negros Oriental MhNdon48 Siquijor n
VIII Eastern Visayas Ilands 43 P1 O t np49 Bilirpn Pan T d Ma . 6 I50 57tern Somor 6 Na,un5I LeyteBu sa 4 cod
52 Northern S\m Il bGrAp53 (Magonu no Di.g54 Southern Leyte 65 h D i
IX Zamboana Peninsula 1 - 8 - i a55 Zombongo 1eel Norte 150 KitotinceT56 Z I Iboang8 del Sur 3 r P a s nar"m1
57 ZoPgmoango Sibugoy anyaendorsurnagoegeCit Siquilor S a 71
Ns 0 1 Mles1 ugl \\0159Eac nceotsuch
R%-VI;mci,,0,k, 129 SuluSea Dipolog Oroquietaode ,N-O 201hulA, E04290 ih bcy.-O62
716 mP-"- 'd 3.gsuk 5
Ilign M layola/ ~ ~ ~ I Marc 703 * iMti4
3ao a Jobl, N gddi ull\- 77 enro A A' oe Wol 3\kyhbudei
on66 thin" mo o eipy,o
0a 50 100 Mie d 1\ Gulf Thi ndon proucenbr2~ N6 6 h a esg nto h
NOVMBE 2012





























