Embed Size (px)
Citation preview
Document o f The World Bank
Report No: 25461-PK
PROJECT APPRAISAL DOCUMENT
ON A
PROPOSED CREDIT
IN THE AMOUNT OF SDR 14.7 MILLION (US $20.0 MILLION EQUIVALENT)
TO THE
ISLAMIC REPUBLIC OF PAKISTAN
FOR A
PARTNERSHIP FOR POLIO ERADICATION
APRIL 21,2003
Human Development Unit South Asia Regional Office
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
CURRENCY E Q U I V A L E N T S
(Exchange Rate Ef fect ive December 1,2002)
Currency Unit = PK Rupees (Rs) Rupees 1 = US$0.0174
US$1 = Rupees 57.50
AFP CAS CDC DFID EPI EU FATA F M O H GDP GOP GF GPEI I C C IDA I-PRSP I P V JICA N G O NID NIH N P I N P V NWFP OPV PEI RI SAPP SIA SNID UNICEF UNF UNFPA USAID VVM W H O WPV
F I S C A L YEAR July 1 -- June 30
A B B R E V I A T I O N S AND A C R O N Y M S Acute flaccid paralysis Country Assistance Strategy Centers for Disease Control and Prevention (USA) Department o f International Development (UK) Expanded Program for Immunization European Union Federally Administered Tribal Areas Federal Ministry o f Health Gross Domestic Product Government o f Pakistan Bill & Melinda Gates Foundation Global Polio Eradication Initiative Inter-Agency Coordinating Committee International Development Agency Interim Poverty Reduction Strategy Paper Inactivated Polio Vaccine Japan International Cooperation Agency Non-governmental Organization National Immunization Day National Institute o f Health National Programme for Immunization Net Present Value Nor th Westem Frontier Province Oral Polio Vaccine Polio Eradication Initiative Rotary Intemational Social Action Program Project Supplemental Immunization Activities Sub-National Immunization Day United Nations Children’s Fund United Nations Foundation United Nations Population Fund United States Agency for Intemational Development Vaccine Via l Monitor Wor ld Health Organization Wild Polio Virus
V i c e President: M i e k o N i s h i m i z u
Sector Di rector : Charles Griffin Country ManagedDirector : John W. Wall
Task T e a m Leader: Jagmohan S. Kang
PAKISTAN PARTNERSHIP FOR POLIO ERADICATION
CONTENTS
A. Project Development Objective
1. Project development objective 2. Key performance indicators
B. Strategic Context
1. Sector-related Country Assistance Strategy (CAS) goal supported by the project 2. Ma in sector issues and Government strategy 3. Sector issues to be addressed by the project and strategic choices
C. Project Description Summary
1. Project components 2. Key policy and institutional reforms supported by the project 3. Benefits and target population 4. Institutional and implementation arrangements
D. Project Rationale
1. Project alternatives considered and reasons for rejection 2. Major related projects financed by the Bank and/or other development agencies 3. Lessons learned and reflected in the project design 4. Indications o f borrower commitment and ownership 5. Value added o f Bank support in this project
E. Summary Project Analysis
1. Economic 2. Financial 3. Technical 4. Institutional 5. Environmental 6. Social 7. Safeguard Policies
Page
2 2
2 3 3
11 12 13 13 14
14 15 16 16 17 18 19
F. Sustainability and Risks
1. Sustainability 2. Critical risks 3. Possible controversial aspects
G. Main Conditions
1. Effectiveness Condition 2. Other
H. Readiness for Implementation
I. Compliance with Bank Policies
Annexes
Annex 1: Annex 2: Annex 3: Annex 4: Annex 5 : Annex 6:
Annex 7: Annex 8: Annex 9:
Project Design Summary Detailed Project Description Estimated Project Costs Economic Analysis Financial Summary (A) Procurement Arrangements (B) Financial Management and Disbursement Arrangements Project Processing Schedule Documents in the Project File Statement o f Loans and Credits
Annex 10: Country at a Glance Annex 11: IDA Buy-Down Mechanism Annex 12: Supervision Plan, FY2004-2006
19 19 20
20 20
20
21
22 25 27 28 34 35 38 40 41 43 46 48 51
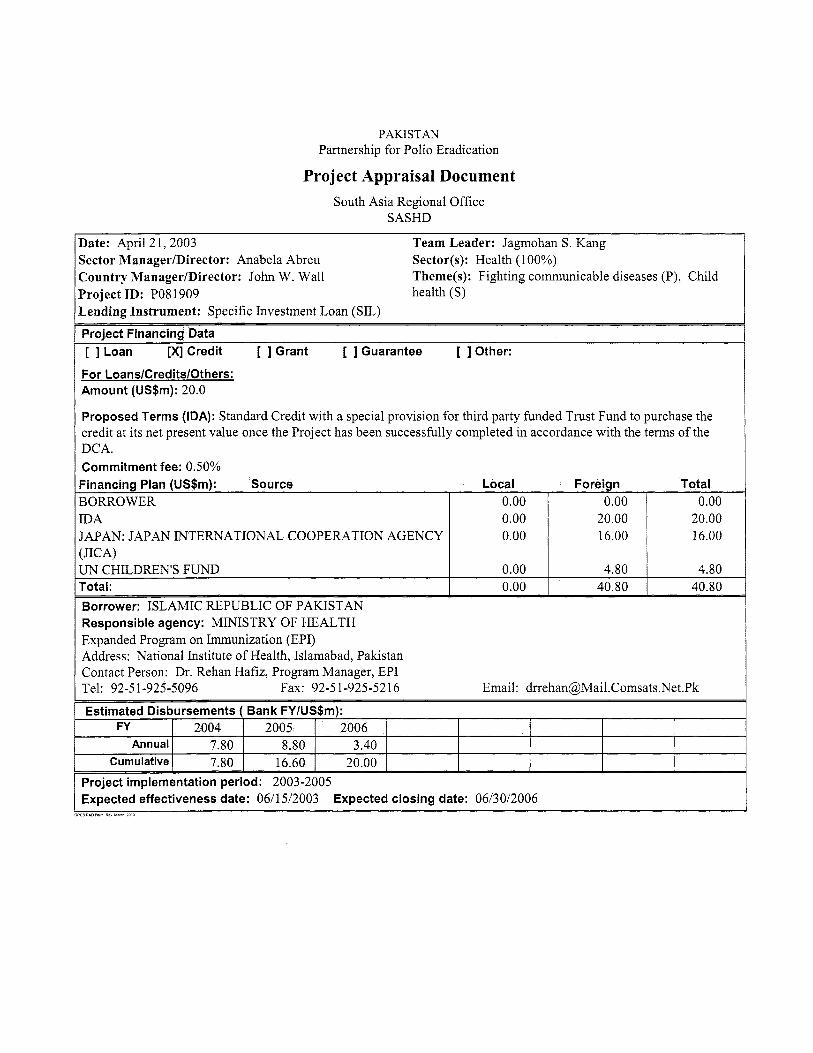
BORROWER [DA JAPAN: JAPAN INTERNATIONAL COOPERATION AGENCY [JICA)
0.00 1 0.00 I 0.00 0.00 0.00
LJN CHILDREN’S FUND
20.00 16.00
0.00 I 4.80 1 4.80
20.00 16.00
Total: 0.00 I 40.80 I 40.80 Borrower: ISLAMIC REPUBLIC OF PAKISTAN Responsible agency: MINISTRY OF HEALTH Expanded Program on Immunization (EPI) Address: National Institute o f Health, Islamabad, Pakistan Contact Person: Dr. Rehan Hafiz, Program Manager, EPI Tel: 92-51-925-5096 Fax: 92-51-925-5216 Email : drrehan@Mail .Comsats .Net.Pk
Estimated Disbursements ( Bank FYlUS$m): FY I 2004 [ 2005 I 2006 [
Annual I 7.80 1 8.80 I 3.40 I Cumulative 1 7.80 I 16.60 I 20.00 I
Project implementation period: 2003-2005 Expected effectiveness date: 0611 512003 Expected closing date: 06/30/2006
_PS*O/” Ra” Y M ZcCO
A. Project Development Objective
1. Project development objective: (see Annex 1)
The project purpose i s to assist the Government o f Pakistan (GOP) in eradicating Poliomyelitis from Pakistan. The project objective i s to support the supply o f the additional oral polio vaccine (OPV), needed during 2003-05, for the country’s supplementary immunization activities (SIAs), i.e., for conducting National Immunization Days (NIDs), Sub-National Immunization Days (SNIDs) and “mop-up operations”. The project i s part o f a World Health Organization (WHO) led, multi-country effort and w i l l contribute to a global public good, Le., the eradication o f Polio from the world by 2005.
2. K e y performance indicators: (see Annex 1)
The following two indicators will be used to measure project performance:
0
Timely arrival o f the OPV at the central stores o f GOP’s Expanded Program on Immunization (EPI), Islamabad, Le., at least five weeks before each o f the SIAs; and SIA coverage o f 80% achieved in the remaining endemic provinces during 2005.
The timely arrival o f the vaccine w i l l be measured through the EPI’s vaccine arrival reports. SIA coverage wil l be measured through a cluster sampling survey according to a W H O approved methodology. Achievement o f these indicators w i l l be a trigger for the IDA buy-down. (See section D.5). Also the number o f reported polio cases will be an outcome o f interest and wil l be reported through the Acute Flaccid Polio (AFP) Surveillance System. The details o f key indicators for measuring the achievement o f the development objectives are described in Annex 1.
B. Strategic Context 1. Sector-related Country Assistance Strategy (CAS) goal supported b y the project: (see Annex 1) Document number: 22219-PAK Date of latest CAS discussion: May 15, 2002
General CAS Goals and Health Sector Related Objectives: The CAS, in support o f GOP’s Interim Poverty Reduction Strategy (I-PRSP), seeks to focus on the reforms to (i) strengthen macroeconomic stability and government effectiveness; (ii) improve the business environment for growth; and (iii) improve equity through support for pro-poor and pro-gender equity policies.
In the social sectors, the CAS supports the core I-PRSP objectives o f empowering people by creating opportunities for increasing incomes, promoting education, improving access to health services, and implementing safety net programs. In health, it seeks to support the key program interventions o f immunization, communicable disease control, and maternal and child health programs. I t also supports achievement o f improved governance and increased efficiency o f public sector expenditures through devolution o f powers to local governments; strengthening o f district health systems; improvement o f monitoring and evaluation; and development o f partnerships wi th the private sector.
The proposed project supports the CAS objective o f improving equity through supporting pro-poor policies, and CAS’S health sector priorities. The poor are at greatest risk from polio due to their unsanitary and crowded living conditions, lower health status, and low immunization coverage. Polio creates both short and long te rm impoverishment, severely limits the children’s future potential and reduces capacity to benefit f rom education and employment opportunities. The project seeks to eradicate polio from Pakistan and contribute to i t s eradication from the world.
- 2 -
2. M a i n sector issues and Government strategy:
While Pakistan’s health indicators have improved in the nineties, they remain weak relative to i t s per capita income o f $440. The infant mortality rate o f 82/1000 live births in 2000101 (Pakistan Integrated Household Survey 2001/02) i s among the highest in South Asia. Total fertility rate o f 4.8 children per woman (Pakistan Reproductive Health and Family Planning Survey 2000/01) i s also highest except for Bhutan. One out o f 30 women dies in childbirth, and malnutrition among women and children continues to be a major cause o f morbidity. Much o f this mortality and morbidity i s caused by preventable or readily treatable diseases, with 40% o f total disease burden related to communicable disease. (Pakistan: Towards Health Sector Strategy, World Bank 1996). The health system, with an urban and curative bias, i s characterized by (i) low (0.7% o f the GDP) and inefficient public spending; (ii) uneven public and private service quality; (iii) lack of consumer protectiodeducation; (iv) lack o f risk-pooling mechanisms; and (v) a weak regulatory framework. People’s dissatisfaction with public services i s evident from their seeking 80% o f the outpatient care from the private sector.
The government tried to address several o f the above weaknesses though the multi-donor supported, 1992-2001, Social Action Program Project (SAPP), that focused on programmatic and management reforms, communicable disease control and maternal health. SAPP achieved limited success in improving the quality o f health services. However, health outcomes improved with increased resource allocation for preventive and promotive program, especially immunization coverage o f children which, for polio, i s s t i l l around 58% against the at-least 80% needed. Weakly implemented reforms, staff absenteeism, weak outputloutcome monitoring and deficient supervision impeded progress.
Government’s Current Health Agenda: GOP’s broader devolution initiative aims at addressing key health issues by improving staff accountability, efficiency, service quality and coordination wi th the private sector. The medium-term human development strategy, outlined in the I-PRSP and in the 2001 Health Policy, focuses on (i) strengthening preventive health services including immunization, communicable disease control, maternal and child health, and family planning; (ii) improving the quality o f hospital services at the tehsil (sub-district) and district headquarters hospitals; and (iii) strengthening management capacity at the district level. GOP has increased financing for immunization and the routine immunization program i s being strengthened.
3. Sector issues to be addressed by the project and strategic choices:
The WHO-launched 1988 Global Polio Eradication Initiative (GPEI), the largest public health effort in history, has been highly successful. By 2002, polio cases had decreased by 99%, from 350,000 in 125 countries to 480 in 9 countries. However, ridding the world o f this disease by immunizing the final 1% potential cases, involves reaching the remotest and most unreachable populations and convincing those who doubt the vaccine’s benefits. On the other hand, because the number o f polio cases i s presently small in any one country, national governments tend to see polio as a lesser priority relative to more pressing health issues, such as rapid population growth or high infant mortality. Also exhaustion has set in among the governments, donors and communities because o f the frequent, large-scale polio campaigns. However, polio eradication remains a global priority because a single infected child puts al l the world’s children at risk o f contracting the disease.
Pakistan is, after India and Nigeria, the world’s third largest poliovirus reservoir. The Global Polio Eradication Initiative (GPEI) has identified ten countries that would require intense and sustained efforts to interrupt polio transmission; Pakistan i s one o f these. Achieving polio eradication in Pakistan w i l l be a
- 3 -
major contribution to achieving eradication worldwide.
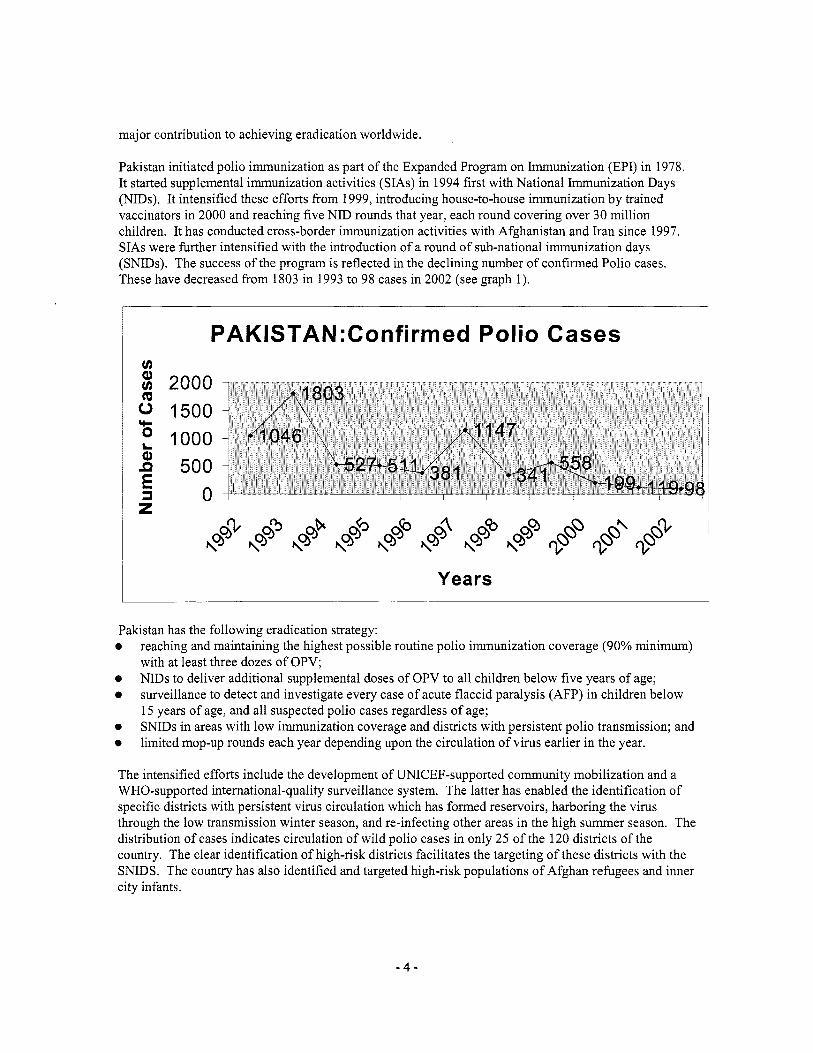
Pakistan initiated polio immunization as part o f the Expanded Program on Immunization (EPI) in 1978. I t started supplemental immunization activities (SIAs) in 1994 f i rs t wi th National Immunization Days (NIDs). I t intensified these efforts from 1999, introducing house-to-house immunization by trained vaccinators in 2000 and reaching five NID rounds that year, each round covering over 30 mil l ion children. I t has conducted cross-border immunization activities wi th Afghanistan and Iran since 1997. SIAs were further intensified with the introduction o f a round o f sub-national immunization days (SNIDs). The success o f the program i s reflected in the declining number o f confirmed Polio cases. These have decreased from 1803 in 1993 to 98 cases in 2002 (see graph 1).
I PAK1STAN:Confirmed Polio Cases
1 Years
Pakistan has the following eradication strategy: 0
0 0
0
0
reaching and maintaining the highest possible routine polio immunization coverage (90% minimum) with at least three dozes o f OPV; NIDs to deliver additional supplemental doses o f OPV to all children below five years o f age; surveillance to detect and investigate every case o f acute flaccid paralysis (AFP) in children below 15 years o f age, and al l suspected polio cases regardless o f age; SNIDs in areas wi th low immunization coverage and districts with persistent polio transmission; and limited mop-up rounds each year depending upon the circulation o f virus earlier in the year.
The intensified efforts include the development o f UNICEF-supported community mobilization and a WHO-supported international-quality surveillance system. The latter has enabled the identification o f specific districts with persistent virus circulation which has formed reservoirs, harboring the virus through the low transmission winter season, and re-infecting other areas in the high summer season. The distribution o f cases indicates circulation o f wild polio cases in only 25 o f the 120 districts o f the country. The clear identification o f high-risk districts facilitates the targeting o f these districts with the SNIDS. The country has also identified and targeted high-risk populations o f Afghan refugees and inner city infants.
- 4 -

Polio
An effective polio eradication program i s in place in Pakistan. The Technical Advisory Group (TAG), which consists o f reputed international and national experts and advises GOP on polio eradication, has noted (i) a sharp reduction o f transmission in the reservoir areas; (ii) improvement in surveillance quality; (iii) successful implementation o f S IAs ’ high-risk area approach; and (iv) continued improvement in the quality of NIDs and SNIDS. I t has also noted that high quality surveillance and laboratory data i s driving the program, and that a solid structure i s in place with the potential to provide broader benefits to immunization. Pakistan needs to make a final, strong push to achieve polio free status. I t has the capacity and clear plans in place to achieve this through intensified efforts during 2003-2005. The government i s maintaining strong commitment and support to polio eradication, but given the pressures on i t s economy, requires external assistance to maintain the momentum.
IDA would support the Pakistan Polio Eradication Initiative (PEI), and the global eradication efforts, in partnership with Bill and Melinda Gates Foundation, the Rotary International and the United Nations Foundation.
- 5 -

Strategic Choices:
Polio can be eradicated through effective routine immunization services or through well-executed vaccination campaigns. The routine services have not proved equal to the task, and strengthening these services i s a medium to long-term effort. So far, such efforts have met with mixed success in Pakistan. Routine coverage for OPV i s about 58% against the over 80% needed to achieve interruption o f transmission. At the present stage o f eradication efforts, routine services can control the disease, prevent outbreaks and facilitate eradication. But the only strategy to interrupt poliovirus transmission and achieve eradication i s the short-term, focused, high quality supplementary immunization activities (SIAs). During the last two years, S I A s have been effective in reaching out to the hard-to-reach and resistant populations. Accordingly, this project w i l l support the SIAs to achieve polio free status in Pakistan by 2005. The Government o f Pakistan, supported by GAVI and other development partners, best supports strengthening o f routine immunization through the on-going initiatives.
IDA can support polio eradication in Pakistan through a normal IDA credit or the special IDA buy-down arrangement adopted for this project, and other similar projects in polio-endemic countries. This arrangement, on satisfactory project implementation, wi l l reduce the IDA credit to grant terms. The buy-down arrangement i s preferred over normal IDA credit because the decision to eradicate polio i s a global decision and a global responsibility, and not only o f the last few polio-endemic countries. Investing in eradicating the last few cases i s less attractive than investing in programs with larger national pay-offs, such as reduced mortality or fertility. The additional support in grant funding w i l l provide the incentive needed to address a disease with greater cross-border or global benefits than national ones. Further, the eradication o f an infectious disease i s a global public good. Once a disease i s eradicated, every child born in the world i s protected. Also the IDA buy-down mechanism, which w i l l convert the credit into a grant only on satisfactory implementation, w i l l encourage the government to focus on implementation and results.
IDA can support OPV procurement or some or all components o f SIAs. I t will, however, finance only the OPV procurement and supply. A vaccination campaign, apart from the vaccines, has several components including social mobilization, logistics, monitoring and evaluation and program management. In Pakistan, these other components are financed by GOP and i t s other development partners including DFID, Government o f Japan, the Netherlands, USAID, Center for Disease Control, Atlanta (CDC) and Rotary International. For the additional OPV needed for the SIAs, however, only partial financing i s expected to be available from the Government o f Japan, and CDC through UNICEF. Also given the planned timeframe o f stopping transmission by the end o f 2003, i t wi l l be simpler and quicker to prepare, implement and monitor a single-component project, especially when other elements for successful SIAs are already in place.
C. Project Description Summary 1. Project components (see Annex 2 for a detailed description and Annex 3 for a detailed cost breakdown):
The project will support Pakistan's Polio Eradication Initiative (PEI) which has three components: (i) the procurement o f OPV; (ii) supplemental operations comprising three main areas: cold chain, social mobilization and training; and (iii) surveillance. It wi l l assist GOP to eradicate polio by the end o f 2005, with an IDA support o f $20.0 million.
This project w i l l provide financing for only one component i.e. the procurement o f OPV for immunizing all children up to five years o f age, under Pakistan's PEI. IDA support wi l l ensure timely procurement
- 6 -
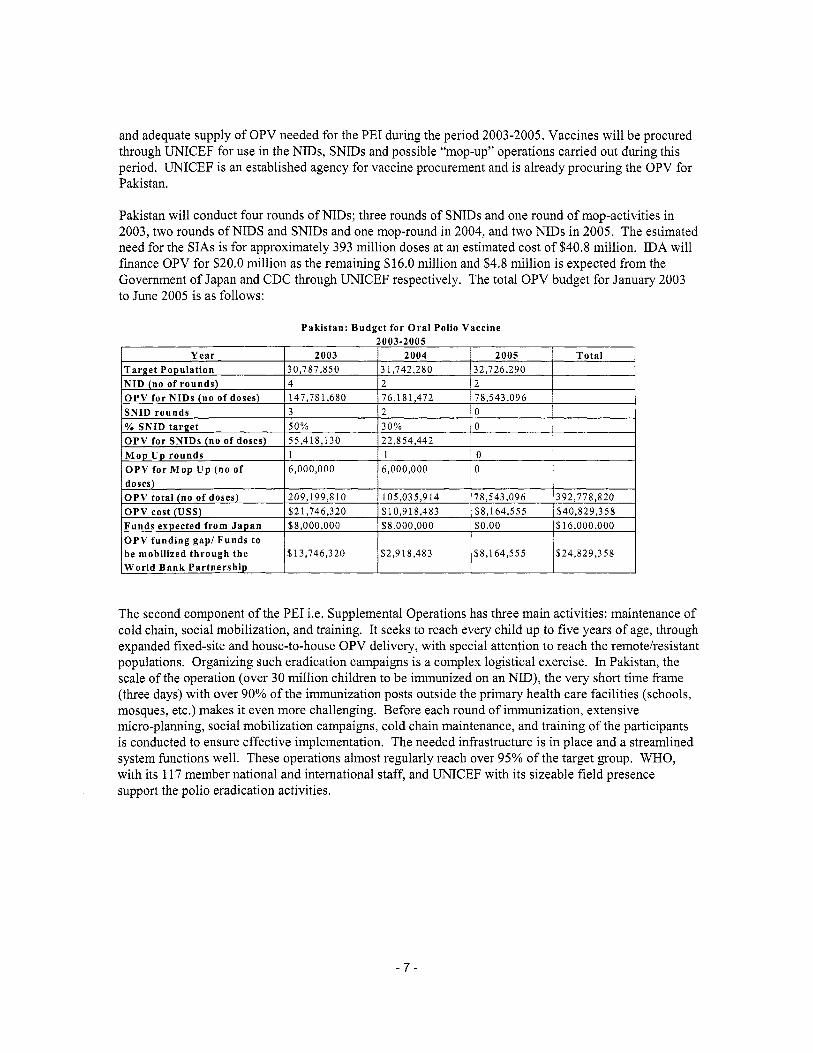
and adequate supply o f OPV needed for the PEI during the period 2003-2005. Vaccines w i l l be procured through UNICEF for use in the NIDs, SNIDs and possible “mop-up” operations carried out during this period. UNICEF i s an established agency for vaccine procurement and i s already procuring the OPV for Pakistan.
O P V cost (US$) Funds expected from Japan O P V funding gap/ Funds to be mobilized through the World Bank Partnership
Pakistan w i l l conduct four rounds o f NIDs; three rounds o f SNIDs and one round o f mop-activities in 2003, two rounds o f NIDS and SNIDs and one mop-round in 2004, and two NIDs in 2005. The estimated need for the SIAs i s for approximately 393 mi l l ion doses at an estimated cost o f $40.8 million. IDA will finance OPV for $20.0 mi l l ion as the remaining $16.0 mill ion and $4.8 mi l l ion i s expected from the Government o f Japan and CDC through UNICEF respectively. The total OPV budget for January 2003 to June 2005 i s as follows:
$21,746,320 $10,918,483 $8,164,555 $40,829,358 $8,000,000 $8,000,000 $0.00 $16,000,000
$13,746,320 $2,9 18,483 $8,164,555 $24,829,358
The second component o f the PEI i.e. Supplemental Operations has three main activities: maintenance o f cold chain, social mobilization, and training. I t seeks to reach every child up to five years o f age, through expanded fixed-site and house-to-house OPV delivery, with special attention to reach the remotelresistant populations. Organizing such eradication campaigns i s a complex logistical exercise. In Pakistan, the scale o f the operation (over 30 mi l l ion children to be immunized on an NID), the very short time frame (three days) wi th over 90% o f the immunization posts outside the primary health care facilities (schools, mosques, etc.) makes i t even more challenging. Before each round o f immunization, extensive micro-planning, social mobilization campaigns, cold chain maintenance, and training o f the participants i s conducted to ensure effective implementation. The needed infrastructure i s in place and a streamlined system functions well. These operations almost regularly reach over 95% o f the target group. WHO, with i t s 117 member national and international staff, and UNICEF with i t s sizeable field presence support the polio eradication activities.
- 7 -
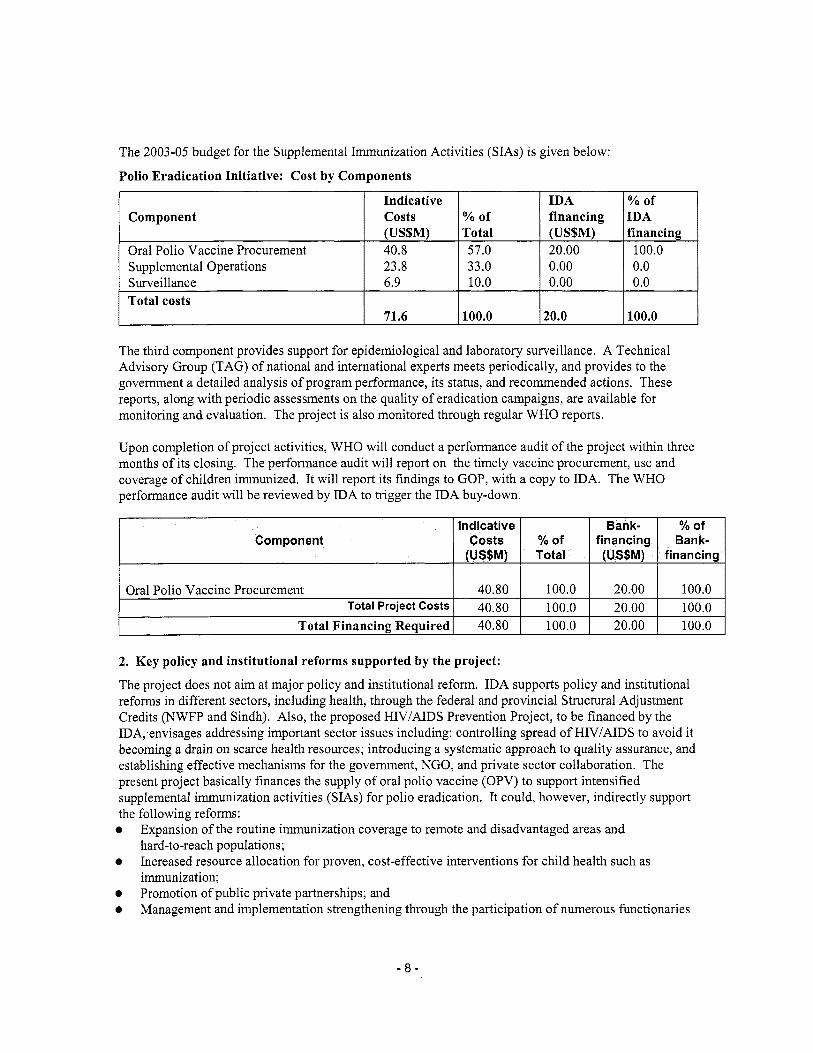
The 2003-05 budget for the Supplemental Immunization Activities (SIAs) i s given below:
Polio Eradication Initiative: Cost by Components
Oral Polio Vaccine Procurement
Component (US$M) Total (US$M) financing 40.8 57.0 20.00 100.0
Indicative Yo of I costs
Total costs 71.6 100.0 20.0 100.0
Supplemental Operations 1 23.8 1 33.0 I 1 0.0 Surveillance 6.9 10.0 0.0
Indicative
(US$M) Component costs
Bank- % of % of financing Bank- Total (US$M) financing
The third component provides support for epidemiological and laboratory surveillance. A Technical Advisory Group (TAG) o f national and international experts meets periodically, and provides to the govemment a detailed analysis o f program performance, i t s status, and recommended actions. These reports, along with periodic assessments on the quality o f eradication campaigns, are available for monitoring and evaluation. The project i s also monitored through regular W H O reports.
Oral Polio Vaccine Procurement Total Project Costs
Total Financing Required
Upon completion o f project activities, W H O will conduct a performance audit o f the project within three months o f i t s closing. The performance audit w i l l report on the timely vaccine procurement, use and coverage o f children immunized. I t w i l l report i t s findings to GOP, with a copy to IDA. The WHO performance audit w i l l be reviewed by IDA to trigger the IDA buy-down.
40.80 100.0 20.00 100.0 40.80 100.0 20.00 100.0 40.80 100.0 20.00 100.0
2. Key policy and institutional reforms supported by the project:
The project does not aim at major policy and institutional reform. IDA supports policy and institutional reforms in different sectors, including health, through the federal and provincial Structural Adjustment Credits (NWFP and Sindh). Also, the proposed H N I A I D S Prevention Project, to be financed by the IDA, envisages addressing important sector issues including: controlling spread o f HIV/AIDS to avoid i t becoming a drain on scarce health resources; introducing a systematic approach to quality assurance, and establishing effective mechanisms for the govemment, NGO, and private sector collaboration. The present project basically finances the supply o f oral polio vaccine (OPV) to support intensified supplemental immunization activities (SIAs) for polio eradication. I t could, however, indirectly support the following reforms: 0
0
0 0
Expansion o f the routine immunization coverage to remote and disadvantaged areas and hard-to-reach populations; Increased resource allocation for proven, cost-effective interventions for child health such as immunization; Promotion o f public private partnerships; and Management and implementation strengthening through the participation o f numerous functionaries
- 8 -
in large and technically well-supported eradication campaigns.
3. Benefits and target population:
The project w i l l benefit all Pakistani children below the age o f five. I t w i l l benefit especially poor and disadvantaged children, eventually al l the world’s children, and the Pakistani population at large. The project has a strong poverty focus because those living in poor and unsanitary conditions are particularly susceptible to polio, and immunization coverage i s lowest among these groups. The project, by supporting the NIDs and SNIDs, w i l l target poor, remote and underprivileged communities. I t will especially benefit children whose mothers are unable to take them to health facilities due to socio-cultural restrictions on female mobility. The participation o f Lady Health Workers in these campaigns w i l l ensure that the poorest and the most vulnerable, especially the girls, get immunized against polio. Even children who do not receive immunization during the SIAs wil l benefit f rom the “herd immunity” that results from the SIAs when a coverage of 80% i s achieved. The project w i l l assist Pakistan in eliminating polio as a public health problem and free scarce resources for use on addressing other important sector issues. The prevention o f disability would alleviate human suffering, and decrease economic loss and social burden caused by the disease. However all the above benefits can be achieved only if the S I A s are implemented effectively and, as planned, Pakistan achieves W H O poliofree certification.
The repeated S I A s campaigns in Pakistan have led to the development o f substantial capacity in planning and managing community based interventions, epidemiology, social mobilization, diagnostic services to support public health interventions and other technical areas. This capacity w i l l eventually strengthen the health system through more effective implementation o f other public health interventions and thereby benefit the general population.
Vitamin A i s distributed during the NIDs in Pakistan. Provision o f Vitamin A reduces the blindness incidence among children and reduces infant mortality generally. Combining Vitamin A with the N I D s increases their benefit to poor children who are most at-risk o f the Vitamin A deficiency.
The project i s part o f a global effort to eradicate polio world-wide. Such eradication i s a global public good. Therefore the benefits o f this project go far beyond the national target group, and will include the present and future world populations.
4. Institutional and implementation arrangements:
The project will be implemented and monitored through the existing government structures that implement the Pakistan Polio Eradication Initiative (PEI), i.e., through the Expanded Program on Immunization (EPI). To ensure timely procurement and supply o f the OPV to the EPI and to monitor i t s effective use, the following arrangements will be in place.
Procurement: OPV will be procured and supplied to the EPI by UNICEF under an agreement between the GOP and UNICEF. A draft agreement for the purpose has been finalized. UNICEF’s international procurement division, based in Copenhagen, will undertake the procurement following UNICEF’s procurement procedures. The National Program Manager, EPI wi l l be responsible for receiving the OPV in Islamabad and for i t s in-country storage, distribution, administration and use.
Vaccine requirements are forecast by the National Program Manager EPI based on the latest estimates o f the population o f children under five years, and the number o f doses to be given per child during a given year. The requirements are estimated with technical support from WHO, UNICEF and TAG and are endorsed by the Inter-Agency Coordination Committee (ICC). The program requirements o f OPV for the
- 9 -
years 2003-05 are 209 mi l l ion doses for 2003, 105 mi l l ion dozes for 2004, and 79 mi l l ion dozes for 2005.
Financial Management: Simplified financial management arrangements are appropriate for this project. The project does not envisage direct involvement o f the Borrower in the management and accounting o f funds. UNICEF w i l l be responsible for these functions under the agreement for OPV supply. The credit proceeds w i l l be disbursed directly to UNICEF on receipt o f withdrawal applications f rom the Borrower. Expenditure w i l l be incurred only on items laid down in the agreement including OPV costs, freight, and handling charges.
UNICEF w i l l submit semi-annual financial reports to GOP, with a copy to IDA, in an agreed format that tracks funds disbursed, vaccines purchased and number o f children immunized. IDA wil l use these reports to monitor the outstanding balance and the funds received and spent by UNICEF. Also, these reports w i l l enable IDA to verify the expenditures before subsequent disbursements. GOP w i l l be able to confirm to IDA the receipt o f the quantities o f OPV indicated in these reports. GOP w i l l also submit to IDA semiannual utilization o f the vaccines received.
GOP i s not required to appoint an independent external auditor or to submit an audit report o f the annual financial statements. However, the Association retains the option to request for an audit.
Supplemental Immunization Activities (SIAs): The OPV procured and supplied under the project w i l l be used for the S I A s which are organized and implemented as follows.
Polio eradication i s integrated within the Expanded Program on Immunization (EPI). The Federal Ministry o f Health implements the program at the national level through the Federal EP I Cell, and wi th technical support from W H O and UNICEF. The National Program Manager, EPI, i s responsible for implementing the Polio Eradication Initiative (PEI) and SIAs. A W H O team consisting o f a CDC seconded senior epidemiologist, a senior program administrator, an NID controller, an EPI expert, a statistician, a social mobilization expert and a logistician, assists the National Program Manager, EPI. The Provincial Program Manager, EPI provides the technical and managerial leadership under the guidance o f the Director-General, Health Services, and i s responsible for planning, implementing, monitoring and evaluating the S I A s at the provincial level. At the District level, the program i s implemented through the district health services under the supervision o f the Executive District Health Officer (EDHO). EDHO and the district EPI officers undertake detailed micro planning to ensure that volunteers, health and other department staff and transport are available on the day o f the vaccination campaign. They also verify that calculations on the logistics forms with regard to the target population, number and location o f NID posts, cold chain needs, and ice requirements are accurate. This process i s facilitated and supported by the Provincial and Federal Program Managers and by WHO and UNICEF local consultants. Coordination Committees at the federal, provincial and district levels include government officials o f related departments, local political and social leaders, and representatives o f the NGOs and donors.
The Federal M O H i s responsible for the procurement, storage and supply o f vaccines, cold chain equipment, syringes, needles, social mobilization (air time costs) and for transport. The Provincial Departments o f Health bear the cost o f staff, training, health education, stationary, POL (petrol, oil, lubricants), and contingencies.
A national level Inter-Agency Coordination Committee (ICC), chaired by the Secretary Health coordinates partner agency and national support to the EPI and polio eradication activities, mobilizes resources for polio eradication, advises the government on polio related policies and reviews progress towards polio er'adication. Similar committees function at the provincial level chaired by the provincial
- 1 0 -
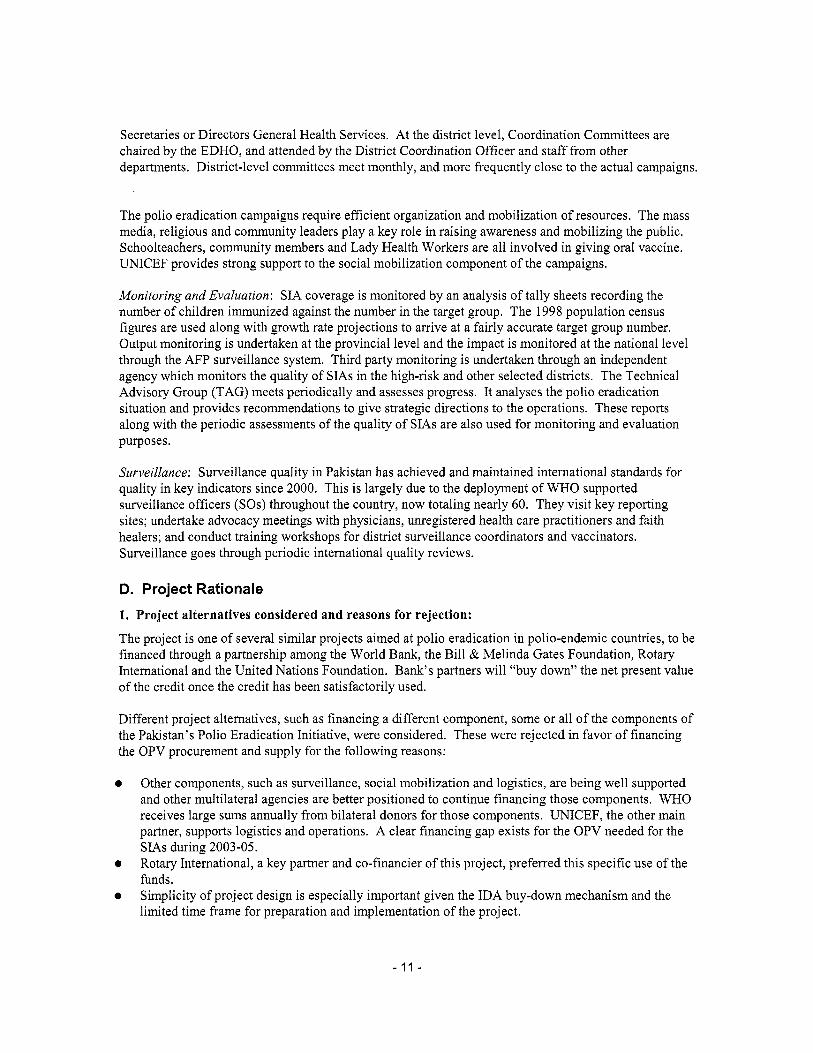
Secretaries or Directors General Health Services. At the district level, Coordination Committees are chaired by the EDHO, and attended by the District Coordination Officer and staff from other departments. District-level committees meet monthly, and more frequently close to the actual campaigns.
The polio eradication campaigns require efficient organization and mobilization o f resources. The mass media, religious and community leaders play a key role in raising awareness and mobilizing the public. Schoolteachers, community members and Lady Health Workers are all involved in giving oral vaccine. UNICEF provides strong support to the social mobilization component o f the campaigns.
Monitoring and Evaluation: SIA coverage i s monitored by an analysis o f tally sheets recording the number o f children immunized against the number in the target group. The 1998 population census figures are used along with growth rate projections to arrive at a fairly accurate target group number. Output monitoring i s undertaken at the provincial level and the impact i s monitored at the national level through the AFP surveillance system. Third party monitoring i s undertaken through an independent agency which monitors the quality o f S I A s in the high-risk and other selected districts. The Technical Advisory Group (TAG) meets periodically and assesses progress. It analyses the polio eradication situation and provides recommendations to give strategic directions to the operations. These reports along with the periodic assessments o f the quality o f S IAs are also used for monitoring and evaluation purposes.
Surveillance: Surveillance quality in Pakistan has achieved and maintained international standards for quality in key indicators since 2000. This i s largely due to the deployment o f W H O supported surveillance officers (SOs) throughout the country, now totaling nearly 60. They visit key reporting sites; undertake advocacy meetings with physicians, unregistered health care practitioners and faith healers; and conduct training workshops for district surveillance coordinators and vaccinators. Surveillance goes through periodic international quality reviews.
D. Project Rationale 1. Project alternatives considered and reasons for rejection:
The project i s one o f several similar projects aimed at polio eradication in polio-endemic countries, to be financed through a partnership among the World Bank, the Bill & Melinda Gates Foundation, Rotary International and the United Nations Foundation. Bank’s partners wi l l “buy down” the net present value of the credit once the credit has been satisfactorily used.
Different project alternatives, such as financing a different component, some or al l o f the components o f the Pakistan’s Polio Eradication Initiative, were considered. These were rejected in favor o f financing the OPV procurement and supply for the following reasons:
Other components, such as surveillance, social mobilization and logistics, are being wel l supported and other multilateral agencies are better positioned to continue financing those components. WHO receives large sums annually f rom bilateral donors for those components. UNICEF, the other main partner, supports logistics and operations. A clear financing gap exists for the OPV needed for the SIAs during 2003-05. Rotary International, a key partner and co-financier o f this project, preferred this specific use o f the funds. Simplicity o f project design i s especially important given the IDA buy-down mechanism and the limited time frame for preparation and implementation o f the project.
- 11 -
The alternative o f procuring the vaccines through the government was considered. Because this project i s one o f an international series, and because specific financing arrangements have been agreed among the partners, it was decided to organize procurement and supply through UNICEF, an agency well recognized for i t s expertise in vaccine procurement.
An alternative would be to invest in strengthening the routine program. Routine immunization coverage remains low in Pakistan and it i s known that the high and increasing coverage o f supplemental activities has contributed to the rapid decline in polio cases. The project builds on that strength. Also strengthening routine immunization i s a longer-term, program type intervention and not the most appropriate for polio eradication, where immediate results are sought. SAPP-2 i s a more suitable vehicle for that approach and i s already addressing the strengthening o f routine immunization.
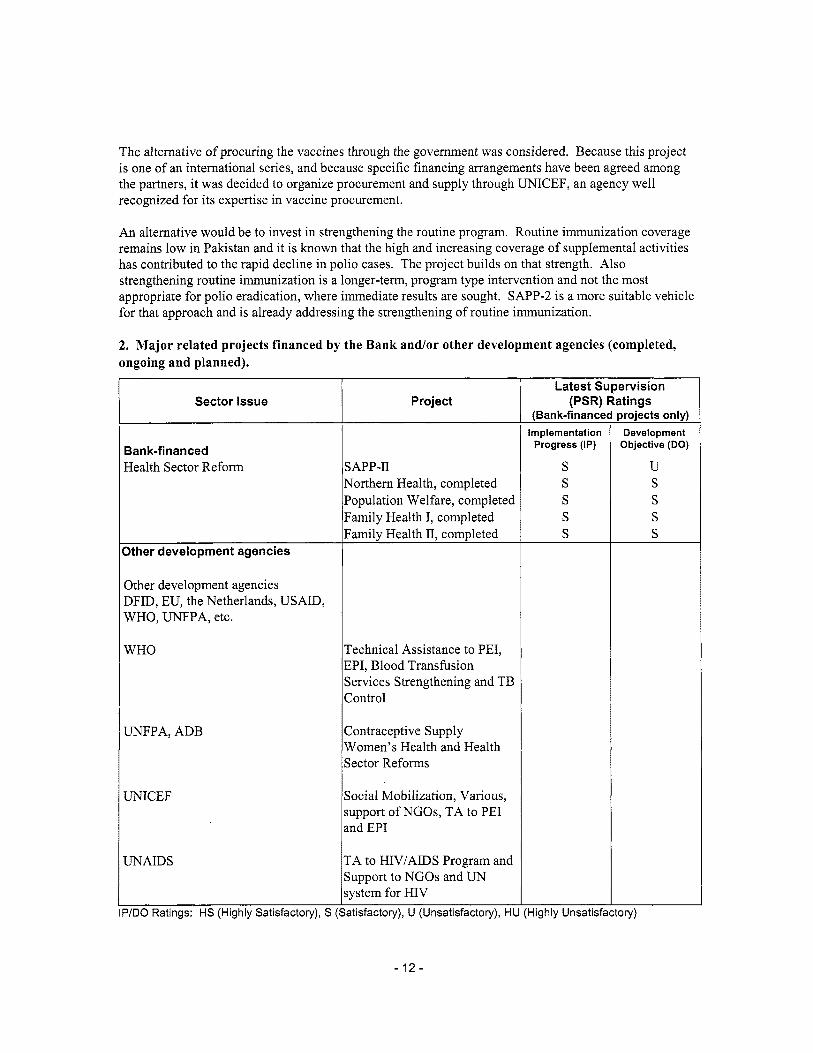
2. M a j o r related projects financed by the B a n k and/or other development agencies (completed, ongoing and planned).
Sector Issue
Bank-financed Health Sector Reform
Other development agencies
Other development agencies DFID, EU, the Netherlands, USAID, WHO, UNFPA, etc.
W H O
UNFPA, ADB
UNICEF
UNAIDS
Project
SAPP-I1 Northern Health, completed Population Welfare, completed Family Health I, completed Family Health 11, completed
Technical Assistance to PEI, EPI, Blood Transfusion Services Strengthening and TB Control
Contraceptive Supply Women's Health and Health Sector Reforms
Social Mobilization, Various, support o f NGOs, TA to PEI md EPI
TA to HIV/AIDS Program and Support to NGOs and UN system for HIV
Latest Supervision (PSR) Ratings
(Bank-f/nance Implementation
Progress (IP)
S S S S S
P/DO Ratings: HS (Highly Satisfactory), S (Satisfactory), U (Unsatisfactory), HU (Highly Unsatisk
- 12-
projects only) Development
Objective (DO)
U S S S S
ory)

3. Lessons learned and reflected in the project design:
Globally polio eradication i s benefiting from some o f the important lessons learnt f rom smallpox eradication. While the objective i s eradication, the program focus i s more on disease surveillance than on immunization coverage. Flexible eradication strategies are driven by regular and good quality surveillance data. For example, Pakistan i s employing SIAs flexibility, based on surveillance data indicating the main disease pockets. A similar approach i s planned for "mopping-up" the final cases as eradication nears.
The project design reflects the lessons from earlier IDA-supported HNP projects in the South Asia region: 0
0
Keep the project design simple and well-defined. IDA support w i l l focus on a single component o f the polio eradication program. Use o f a Project Coordination Unit may undermine the regular structures in a Ministry. The project w i l l be implemented using the existing structures and institutions in place for implementation o f routine immunization and PEI activities. Establish good coordination with the other partners. The Resident mission has a senior health specialist who w i l l provide technical support locally and participate in the Inter-Agency Coordination Committee meetings.
0
Other relevant lessons from the completed projects in Pakistan, especially f rom the SAPP, are: Focus on aualitv: SIAs provide house-to-house, convenient immunization services; the objective itself i s to achieve a coverage o f over 90% o f children in the targeted districts. Decentralize, streamline and shift to community control: The project involves repeated, large-scale efforts through full involvement o f the community. Without such community support, this project can not be successfully implemented. Improve monitorinp and evaluation and the value and timeliness of feedback: The project seeks to achieve polio eradication through focused, large-scale campaigns that utilize surveillance data as the basis o f planning. Strong monitoring and evaluation o f on-going campaigns using third party drives PEI activities. Address sustainabilitv: Sustainability w i l l not be an issue in this project aimed at eradication o f the disease, polio, which will also contribute to i t s eradication f rom the world. Build political will throughout the society: Repeated community participation in campaigns beside the government officials i s likely to be conducive to the promotion o f such political wi l l in the society.
4. Indications of borrower commitment and ownership:
The EPI program, established in 1985 in Pakistan, i s a high priority program o f the Federal Ministry o f Health and the Provincial Departments o f Health. EPI was one o f the seven federally-funded public health programs included in the Second Social Action Program Project (SAPP-2), supported by the Bank and other development partners. PEI i s implemented through the existing EPI program. The government i s fully committed to eradicating polio. Recent financial constraints that cut into public health expenditure largely spared the EPI program. President Musharraf personally participated in the 2002 spring round o f the National Immunization Day (NID). The Minister o f Health, participated in the ICC meeting and high-level advocacy meetings to champion the eradication initiative. Overall the PEI enjoys a high degree o f political and community support.
- 13-
5. Value added of Bank support in this project:
Pakistan’s Polio Eradication Initiative has been a major national effort since 1994, and has been supported by several donors. W H O and UNICEF are the lead technical partners for polio eradication globally and in Pakistan. Through them, the donors are providing grant funds for the operations, surveillance and vaccine costs. An additional $20.0 mi l l ion i s needed to meet the vaccine requirements for 2003-2005. IDA w i l l meet this gap through a normal credit that w i l l be reduced to grant funding through an innovative IDA Buy-down mechanism.
Following an appeal from the Global Polio Eradication Technical Advisory Committee, the Bank, in partnership with the Gates Foundation (GF), Rotary International (RI) and UN Foundation, has developed the IDA Buy-down financing mechanism to support intensified polio eradication activities in polio-endemic countries. These countries are: Afghanistan, Pakistan and India in South Asia and Nigeria and Angola in the Africa Region. A Polio Eradication Trust Fund, to be financed by GF and RI and managed by the World Bank, has been established. The Trust Fund w i l l pay the service fee for the Credit during the implementation and buy down the net present value o f the IDA Credit, reducing it to grant terms, when the projects are successfully completed. Thus IDA Credit to Pakistan wil l in effect be a grant for polio eradication. Since the partners will buy the credit at the N e t Present Value, it enables them to leverage their funds for financing polio eradication in Pakistan and elsewhere: they need about a third o f the funds they would otherwise need to finance the same goods and services. Through the partnership, they are also able to access the rigor o f Bank’s project preparation and supervision in support o f their efforts for polio eradication.
Bank w i l l pilot, through this project, a new financing approach to encourage urgent action on a global public good with significant externalities. This approach wil l enable the Bank to engage public and private partners in a common global cause.
E. Summary Project Analysis (Detailed assessments are in the project fi le, see Annex 8)
1. Economic (see Annex 4): 0 Cost benefit 0 Cost effectiveness 0 Other (specify) Justifzcation: Using standard public finance criteria, public involvement in and financing o f the Supplementary Immunization Activities to eradicate polio i s justified. Control o f an infectious disease i s a classic example o f a public good for health. Global eradication i s a global public good with high externalities.
NPV=US$ million; ERR = % (see Annex 4)
Because o f the diversity o f the communities, government administrative levels and partners that have contributed to the implementation o f the Global Polio Eradication Initiative (GPEI), i t i s not possible to accurately quantify the value o f the financial and in-kind expenditures within a country. After quantifying the number o f NIDs volunteer hours per country, wage rates f rom the year 2000 World Development Indicators statistical database were applied to establish a monetary value for the ‘volunteer’ effort. Based on these calculations, according to a forthcoming W H O study, between 1988 and 2005, world-wide polio endemic countries w i l l have contributed at least US$2.35 bi l l ion in volunteer time alone for polio eradication activities. These calculations do not account for the opportunity cost o f the volunteer time. They also do not reflect the substantial government resources used at the national, provincial, district and community levels to pay for petrol, social mobilization, training and other
- 1 4 -
activities.
Between 1988 and 2005, external sources w i l l have provided at least US$2.75 bi l l ion to polio endemic countries to support eradication strategy implementation cost. This included OPV procurement and operational costs for supplemental immunization activities including cold chain refurbishment, training and social mobilization. The strengthening o f surveillance has absorbed external resources for vehicles, computers, other equipment, supplies, training, personnel and related costs. External resources are also used for the certification and containment processes, advocacy and resource mobilization, documentation, meetings and administration. Different mechanisms are used to channel these resources to polio-endemic countries, primary ones being multilateral funding through W H O and UNICEF, and direct bilateral funding.
Normal cost-benefit analysis does not easily apply to disease eradication. While the costs o f eradicating the last case o f polio are very high in relation to the by then very low burden o f the disease, the benefits o f successful eradication are infinite. The disease will be extinct from the world for-ever, unless a man-made mistake or a disaster causes it to reappear. However, ceasing immunization seems no longer a straightforward option. The recent increase in terrorist threats has impacted the development o f post-eradication certification strategies.
WHO estimates that if eradication i s not achieved, even with improved routine immunization coverage, the burden o f disease due to polio would be significant. Between 2001 and 2040 there would be 10.6 mill ion new cases o f polio worldwide, representing the loss o f 60 mi l l ion DALYs (discounted at 3%), nearly al l o f which would occur in low-income developing countries. Eradication would result in cost savings in all countries in which OPV i s currently used, if polio vaccination were to stop in 2010. Even in the ‘worst case’ scenario, in which OPV may be replaced with a universal IPV strategy, the cost per DALY saved would be low, at approximately US$50 per discounted DALY saved in developing countries.
2. Financial (see Annex 4 and Annex 5): NPV=US$ million; FRR = % (see Annex 4) Present efforts to eradicate polio world-wide are financially supported by a large group o f bilateral and private donor agencies, mainly under the coordination o f W H O and UNICEF. These two agencies also provide technical support in the implementation o f the eradication efforts. The polio-endemic countries provide about 50 percent o f the financing, mainly through human resources and recurrent costs.
The project w i l l support the procurement o f the OPV. The quantity o f vaccine procured wil l depend on the needs identified by the polio surveillance. There remains a risk that eradication w i l l be delayed, requiring additional funds in the future. In that case, additional funds w i l l also be needed for the program support. Commitment to polio eradication i s high and continuous future support from the global community i s likely.
Fiscal Impact:
Financial sustainability i s not an issue since the supplementary activities o f the polio eradication program will end with the disease.
Improved surveillance systems set up for poliomyelitis wi l l need to be integrated in regular operations o f the health sector, in terms o f functioning and financing. There i s anecdotal evidence o f positive synergies between the polio eradication program and health systems, but these have not yet been fully exploited.
- 1 5 -
3. Technical: There are several reasons why polio can and should be eradicated: (i) there i s no animal reservoir to sustain the disease; (ii) the virus has a limited persistence in the environment; (iii) there i s no long-term camer state; (iv) permanent immunity i s provided following infection; and (v) a safe, highly effective, and easily administered vaccine i s available. Polio causes paralysis, most frequently in children, and between 5-10% o f cases die when the breathing muscles are paralyzed. Polio i s incurable and i t s effects are largely irreversible.
There has been a delay in meeting the global eradication target for the year 2000. This i s not unlike similar experiences in the Americas (9 months late, 1991) or the Western Pacific Regions (2 years late, 1997). Pakistan i s s t i l l on target to meet the Global Strategic Plan’s revised target o f 2005.
The eradication strategies are proving successful. At this point in the initiative, the most significant risks are: (1) weaknesses o f the routine immunization services; (2) the possibility that political support may decline; and (3) uncertainty about continued funding.
GOP’s three year strategic plan for the Polio Eradication Initiative, was reviewed during the appraisal together with WHO and other donors. The review clearly indicated that the government i s keen on improving routine EPI services, that political commitment to polio eradication both at the federal and provincial levels remains strong, and that donors are wil l ing to support the program, with the needed funds, through i t s final push to achieve eradication.
4. Institutional:
4.1 Executing agencies:
The project will be implemented through the existing federal, provincial, and district structures implementing the routine immunization and the Polio Eradication Initiative (PEI). No new structures w i l l be created.
The Federal EPI cell manages the national immunization program and wil l be responsible for project execution at the national level. I t i s a relatively strong unit with adequate technical support, from W H O and UNICEF, for program planning, surveillance, social mobilization and monitoring and evaluation. Other partners supporting the PEI, such as DFID, have carried out institutional reviews o f the federal, provincial and local structures involved in the execution. They support capacity building and overall program strengthening activities. The Bank will work closely wi th the partners and wil l keep informed o f the relevant institutional issues.
4.2 Project management:
N o new management structures w i l l be created for the project.
4.3 Procurement issues:
OPV w i l l be procured through UNICEF. The Bank has accepted that UNICEF w i l l use i t s own procedures for the procurement and delivery o f the OPV. Government o f Pakistan and UNICEF have finalized the text o f a draft agreement, to be entered into between them, for this purpose. There are no significant procurement issues.
4.4 Financial management issues:
- 16-
As this project does not require direct involvement o f the Borrower in the disbursement o f IDA credit, and IDA funds will be transferred directly to UNICEF, there are no significant financial management issues. Assurance that the Bank’s fiduciary requirements are met, especially that funds are used for the purpose intended with due regard to economy and efficiency, wi l l be obtained through the measures discussed in Annex 6 and addressed in the OPV Agreement to be entered into by the Borrower and UNICEF. Upon receipt o f a direct payment request from the GOP, IDA funds w i l l be transferred to UNICEF for the procurement o f OPV. UNICEF’s regular financial management system and auditing procedures wil l be used for this project. Although the Borrower i s not required to carry out annual audits, the Association retains the option to request for an audit.
WHO coordinates program support provided by a group o f bilateral donors and private foundations. These funds provide a large part o f the recurrent budget for the SIAs. It i s expected that W H O w i l l release funds speedily to facilitate project implementation. This aspect was assessed during the appraisal and i t was found that there have been no instances o f delayed release o f funds by W H O for project implementation o f SIAs. GOP i s fully satisfied with the way W H O i s handling the release o f funds for polio eradication activities in Pakistan.
5. Environmental: 5.1 Summarize the steps undertaken for environmental assessment and E M P preparation (including consultation and disclosure) and the significant issues and their treatment emerging from this analysis.
The project w i l l contribute in a significant way to the eradication o f wild poliovirus f rom the environment and will contribute to worldwide eradication o f poliomyelitis. The project’s methodology, stimulating oral vaccination with the attenuated virus, has no significant negative environmental impact. The appraisal mission observed supplemental immunization activities in action, as the January sub-national immunization days (SNIDs) coincided with the mission dates, and came to the conclusion that no significant negative environmental issues would need to be addressed under the project.
Environmental Category: C (Not Required)
The key stakeholders o f the project are children below 5 years o f age receiving the vaccines. Their parents, especially their mothers, have been the targets, for the last several years, o f IEC campaigns for the ongoing polio eradication efforts. Other stakeholders are the provincial and federal health authorities responsible for the implementation o f the campaign. The international community i s another important stakeholder, given that disease eradication i s a global public good. Therefore, the polio eradication campaigns have seen an extraordinary cooperation from many donors, governments and communities. The Bank‘s contribution, towards the end o f the campaign, i s coupled with that o f the Gates Foundation, Rotary International and the United Nations Foundation.
5.2 What are the main features o f the EMP and are they adequate?
NA
5.3 For Category A and B projects, timeline and status o f EA:
NA 5.4 How have stakeholders been consulted at the stage o f (a) environmental screening and (b) draft EA report on the environmental impacts and proposed environment management plan? Describe mechanisms o f consultation that were used and which groups were consulted?
NA
5.5 What mechanisms have been established to monitor and evaluate the impact o f the project on the environment? D o the indicators reflect the objectives and results o f the EMP?
NA
Date o f receipt o f final draft:
- 17-

6. Social: 6.1 Summarize key social issues relevant to the project objectives, and specify the project's social development outcomes.
The project specifically aims at benefiting vulnerable and previously neglected groups by providing polio immunization. Poor families, particularly their children, would be the primary beneficiaries o f the project. Quantitative studies have found low utilization rates at public health facilities catering to the poor. Qualitative assessments o f other health projects indicate that lack o f physical access to services i s a problem in some areas. A larger problem seems to be the poor quality o f health services. While wealthier groups can purchase health services from the private sector, the poor are unable to afford these services and continue to rely on traditional practitioners. The project would address these issues in respect o f polio eradication by developing specific strategies and by using surveillance data to reach the "hard-to-reach" populations.
6.2 Participatory Approach: How are key stakeholders participating in the project?
The Polio Eradication Initiative (PEI) has established a framework for broad, on-going participation largely through the Inter-Agency Coordination Committee. This mechanism includes representatives from: (i) key government ministrieddepartments; (ii) multilateral agencies (UNICEF and WHO); (iii) bilateral agencies including the Government o f Japan, the Netherlands, EU, DFID, USAID, CDC, etc.; (iv) NGOs; and (v) community mobilization and media experts. The ICC meets regularly to review needs and strategies o f the national polio eradication program, and to assess the performance o f supplemental immunization activities (SIAs).
The PEI has achieved a coverage o f over 90% during the last few years by placing high priority on mobilizing participation o f the beneficiaries as well as o f the key stakeholders. Traditional and religious leaders have been sensitized and are now very committed to the cause. Rejection o f polio vaccination now concerns only a very small percentage o f the population.
6.3 How does the project involve consultations or collaboration wi th NGOs or other c iv i l society organizations?
The Program holds consultations wi th partner NGOs and community groups which actively participate in social mobilization activities for SIAs. NGOs and community groups are represented in the ICC described above, and they participate wi th government representatives in joint training workshops for the micro planning o f polio activities.
6.4 What institutional arrangements have been provided to ensure the project achieves i t s social development outcomes?
The current institutional arrangements for the PEI have been effective in increasing the number o f Pakistani children immunized against polio, and in reaching certification-level acute flaccid polio (AFP) surveillance (one case o f AFP per 100,000 population under 15), and approaching the international standard for collection o f adequate diagnostic specimens from at least 80% o f AFP cases within 14 days o f onset o f paralysis. This project w i l l reinforce these arrangements to promote interaction and coordination between the government departments, international agencies, NGOs and community groups at the national, state and local levels.
6.5 How w i l l the project monitor performance in terms o f social development outcomes?
The project seeks to contribute to polio eradication in Pakistan and globally through the supply o f oral polio vaccine to the Expanded Program on Immunization in Pakistan. I t wi l l do so by providing the oral polio vaccine for use in the supplemental immunization activities (SIAs) which target al l children below
- 18-
the age o f five. Even if some children are le f t out, they benefit from the "herd" immunity once a coverage o f above 80% i s achieved. The project's monitoring indicator requires a SIA coverage o f 85% in each province in 2005. This w i l l be measured through a W H O performance audit to be conducted within three months o f the close o f the project.
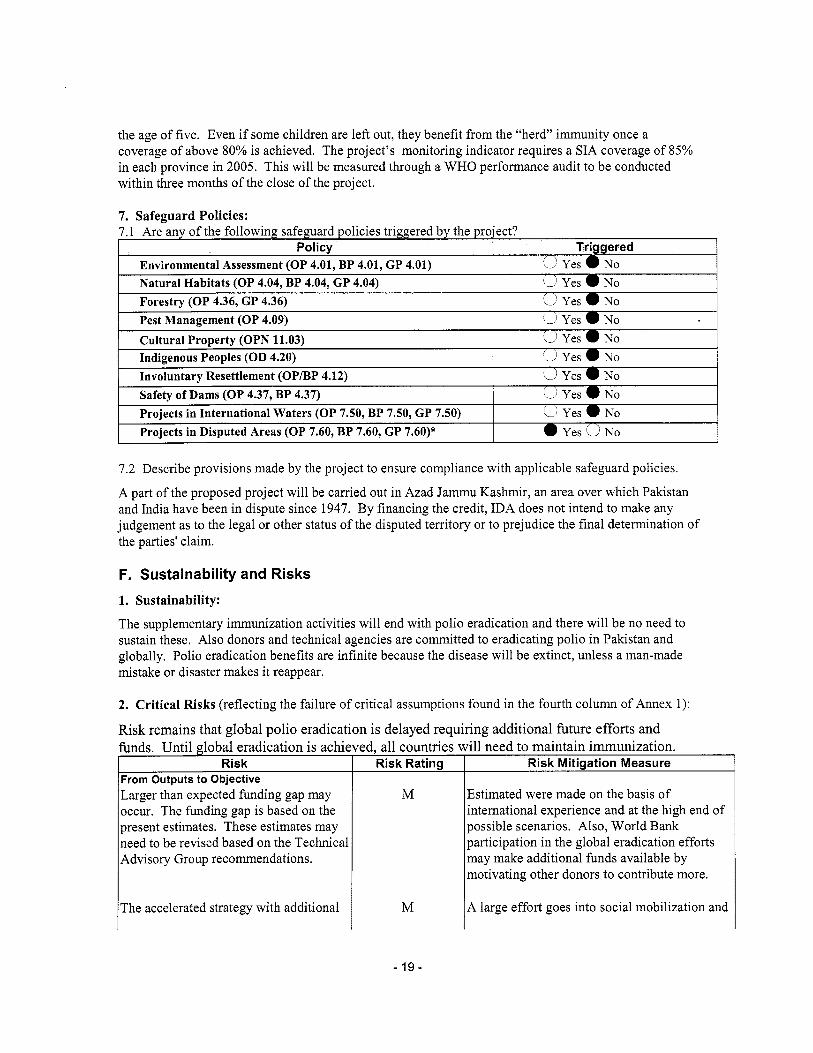
Risk From Outputs to Objective Larger than expected funding gap may occur. The funding gap i s based on the present estimates. These estimates may need to be revised based on the Technical Advisory Group recommendations.
7. Safeguard Policies:
Risk Rating Risk Mitigation Measure
Estimated were made on the basis o f international experience and at the high end o f possible scenarios. Also, Wor ld Bank participation in the global eradication efforts may make additional funds available by motivating other donors to contribute more.
M
7.2 Describe provisions made by the project to ensure compliance with applicable safeguard policies.
A part o f the proposed project w i l l be carried out in Azad Jammu Kashmir, an area over which Pakistan and India have been in dispute since 1947. By financing the credit, IDA does not intend to make any judgement as to the legal or other status o f the disputed territory or to prejudice the final determination o f the parties' claim.
F. Sustainability and Risks 1. Sustainability:
The supplementary immunization activities wi l l end with polio eradication and there w i l l be no need to sustain these. Also donors and technical agencies are committed to eradicating polio in Pakistan and globally. Polio eradication benefits are infinite because the disease will be extinct, unless a man-made mistake or disaster makes it reappear.
The accelerated strategy wi th additional M A large effort goes into social mobilization and
- 19-
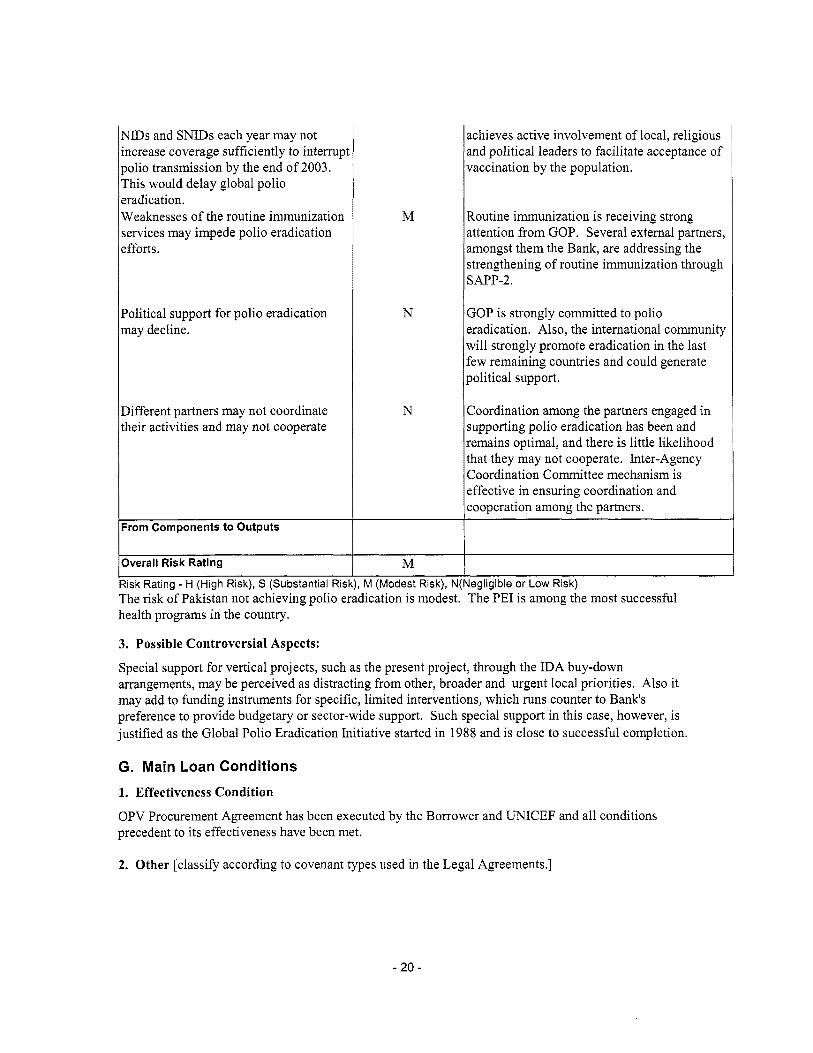
NIDs and SNIDs each year may not increase coverage sufficiently to interrupi polio transmission by the end o f 2003. This would delay global polio eradication. Weaknesses o f the routine immunization services may impede polio eradication efforts.
Political support for polio eradication may decline.
Different partners may not coordinate their activities and may not cooperate
h From Components to Outputs
Overall Risk Rating I Risk Rating - H (High Risk), S (Substantial Ris
M
N
N
M M (Modest Risk), Ni
The risk o f Pakistan not achieving polio eradication i s modest. health programs in the country.
3. Possible Controversial Aspects:
achieves active involvement o f local, religious and political leaders to facilitate acceptance o f vaccination by the population.
Routine immunization i s receiving strong attention f rom GOP. Several external partners, amongst them the Bank, are addressing the strengthening o f routine immunization through SAPP-2.
GOP i s strongly committed to polio eradication. Also, the international community wi l l strongly promote eradication in the last few remaining countries and could generate political support.
Coordination among the partners engaged in supporting polio eradication has been and remains optimal, and there i s l i t t le likelihood that they may not cooperate. Inter-Agency Coordination Committee mechanism i s effective in ensuring coordination and cooperation among the partners.
legligible or Low Risk) The PEI i s among the most successful
Special support for vertical projects, such as the present project, through the IDA buy-down arrangements, may be perceived as distracting from other, broader and urgent local priorities. Also i t may add to funding instruments for specific, limited interventions, which runs counter to Bank's preference to provide budgetary or sector-wide support. Such special support in this case, however, i s justified as the Global Polio Eradication Initiative started in 1988 and i s close to successful completion.
G. Main Loan Conditions 1. Effectiveness Condition
OPV Procurement Agreement has been executed by the Borrower and UNICEF and a l l conditions precedent to i t s effectiveness have been met.
2. Other [classify according to covenant types used in the Legal Agreements.]
- 20 -
H. Readiness for Implementation E 1. a) The engineering design documents for the f i rs t year's activities are complete and ready for the
start o f project implementation. 1. b) Not applicable.
2. The procurement documents for the first year's activities are complete and ready for the start o f project implementation.
quality. 3. The Project Implementation Plan has been appraised and found to be realistic and o f satisfactory
4. The following items are lacking and are discussed under loan conditions (Section G):
1. Compliance with Bank Policies x 1. This project complies wi th al l applicable Bank policies. E' 2. The following exceptions to Bank policies are recommended for approval. The project complies
with all other applicable Bank policies.
Sector ManagerlDirector ntry ManagerlDirector
-21 -
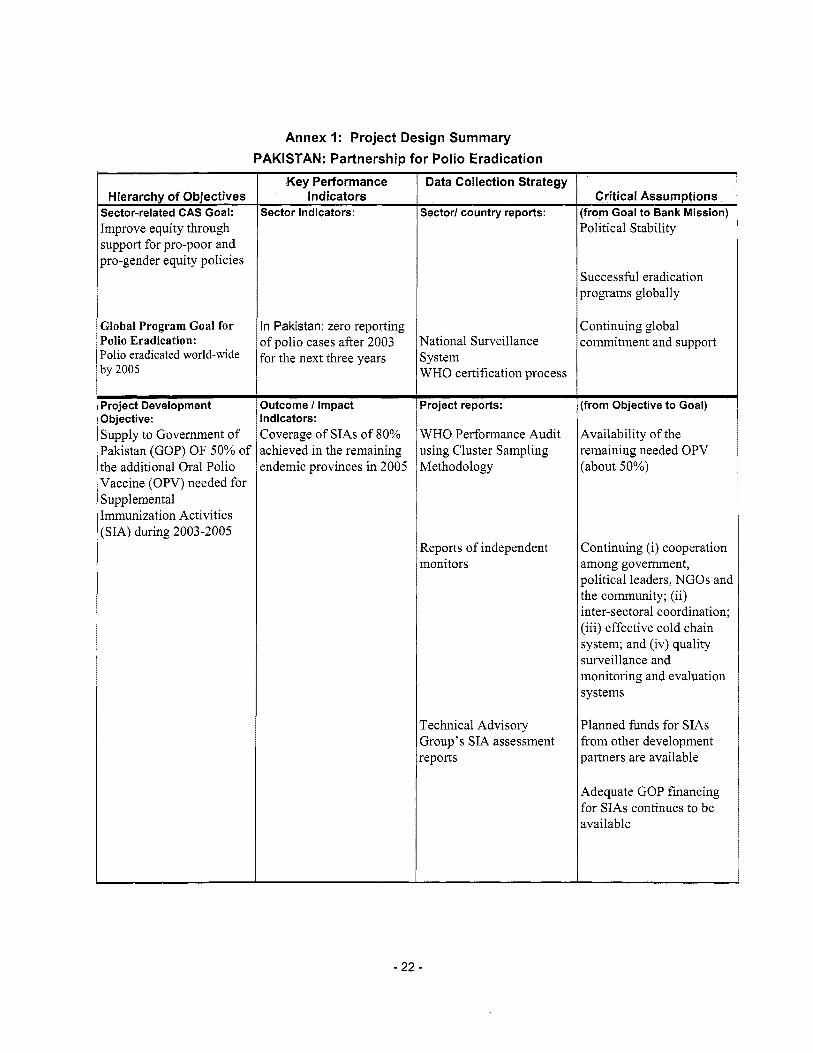
Annex 1: Project Design Summary PAKISTAN: Partnership for Polio Eradication
Hierarchy of Objectives jector-related CAS Goal:
Key Performance Indicators
Sector Indicators:
'olio Eradication: 'olio eradicated world-wide )y 2005
o f polio cases after 2003 for the next three years
Data Collection Strategy
Jroject Development lbjective: ;upply to Government o f 'akistan (GOP) OF 50% o f he additional Oral Polio
Sector1 country reports:
Outcome I Impact Indicators: Coverage o f S I A s o f 80% achieved in the remaining endemic provinces in 2005
Vational Surveillance system WHO certification process
Jroject reports:
VHO Performance Audit ising Cluster Sampling vlethodology
ieports o f independent nonitors
rechnical Advisory 3roup's S I A assessment ,eports
Critical Assumntions [from Goal to Bank Mission) Political Stability
Successful eradication programs globally
Continuing global commitment and support
(from Objective to Goal)
Availability o f the remaining needed OPV (about 50%)
Continuing (i) cooperation among government, political leaders, NGOs and the community; (ii) inter-sectoral coordination; (iii) effective cold chain system; and (iv) quality surveillance and monitoring and evaluation systems
Planned funds for SIAs from other development partners are available
Adequate GOP financing for SIAs continues to be available
- 22 -

htput from each :omponent: rimely provision o f OPV o GOP
Data Collection Strategy
Output indicators:
Procurement o f UNICEF certified OPV and delivery to GOP’s Expanded Program on Immunization (EPI) for use in the SIAs: five weeks o f before each round o f S IAs
Critical Assumptions (from Outputs to Objective) Project reports:
EPI’s Vaccination Arrival Reports
Continuing effective coordination between GOP, UNICEF and other Inter-Agency Coordination Committee partners
UNICEF’s quarterly financial reports
GOP’s quarterly financial reports
Technical Advisory
International vaccine market i s stable
Regional peace and political stability
Group’s assessment reports Bank’s bi-annual and other supervision reports
- 23 -
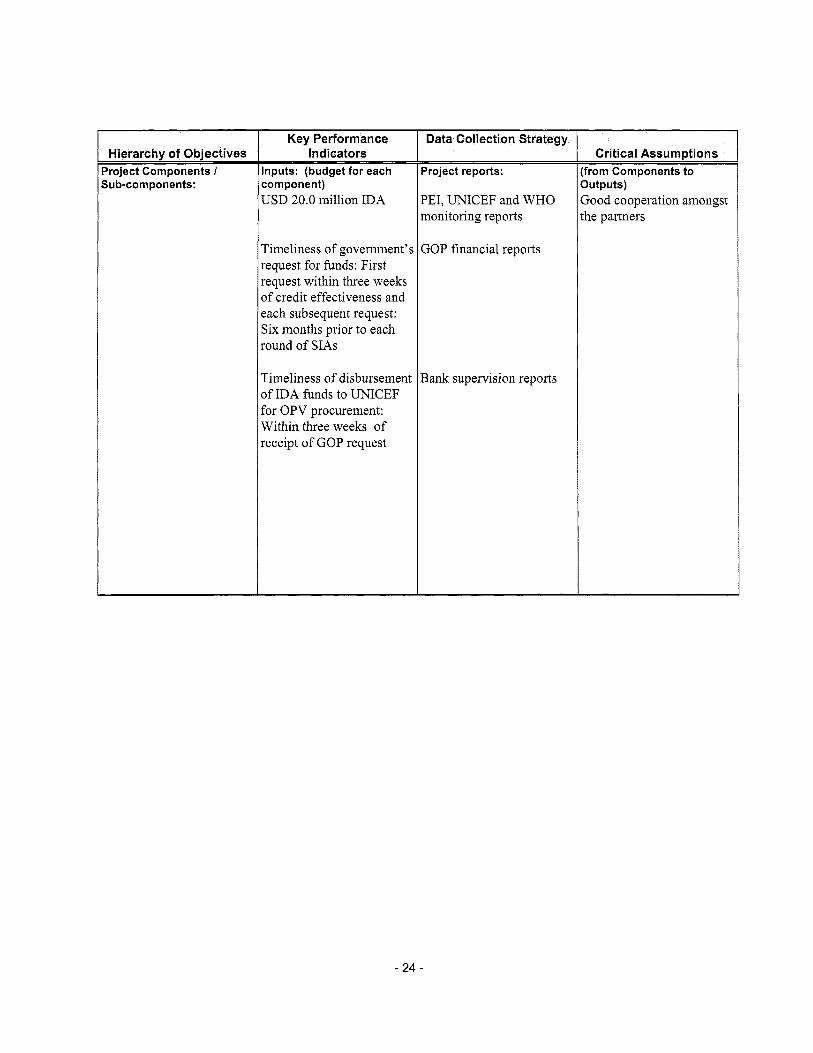
Hierarchy of Objectives Jroject Components I Sub-components:
Key Performance Indicators
Data Collection Strategy
Timeliness o f government’s request for funds: First request within three weeks o f credit effectiveness and each subsequent request: Six months pr ior to each round o f SIAs
Timeliness o f disbursement o f IDA funds to UNICEF for OPV procurement: Within three weeks o f receipt o f GOP request
GOP financial reports
Bank supervision reports
Critical Assumptions from Components to Iutputs) 3ood cooperation amongst he partners
- 24 -
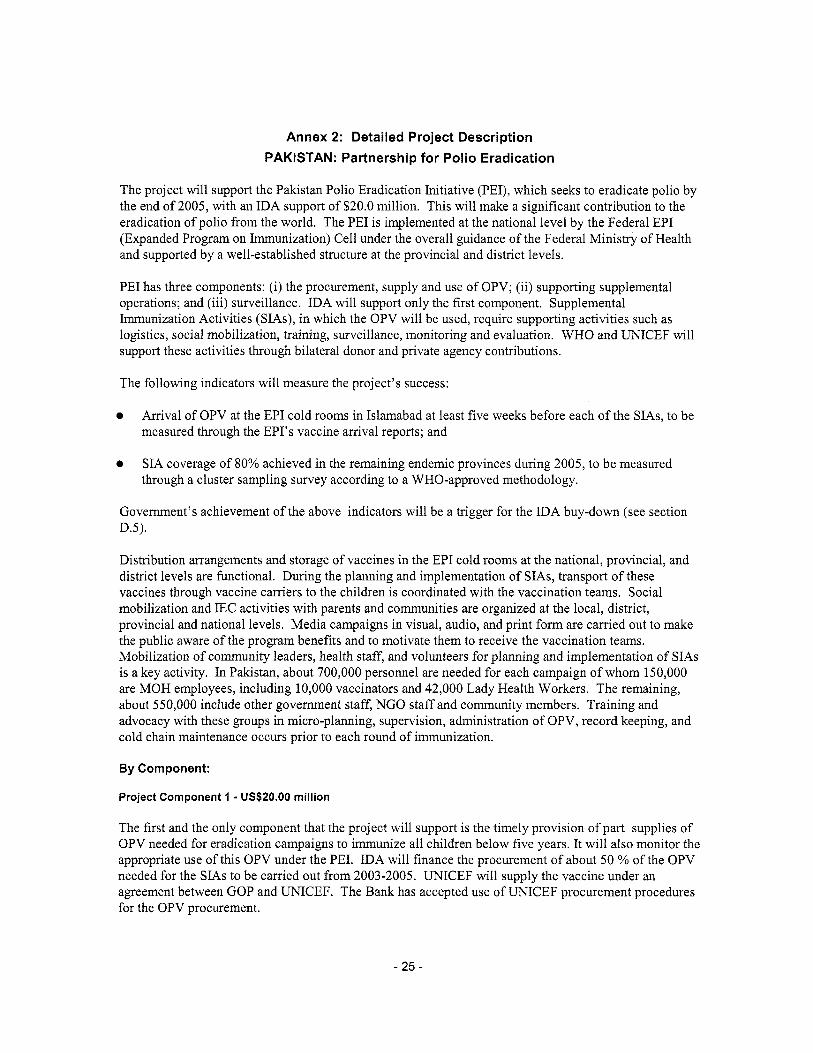
Annex 2: Detailed Project Description PAKISTAN: Partnership for Polio Eradication
The project wi l l support the Pakistan Polio Eradication Initiative (PEI), which seeks to eradicate polio by the end o f 2005, with an IDA support o f $20.0 million. This will make a significant contribution to the eradication o f polio from the world. The PEI i s implemented at the national level by the Federal EPI (Expanded Program on Immunization) Cell under the overall guidance o f the Federal Ministry o f Health and supported by a well-established structure at the provincial and district levels.
PEI has three components: (i) the procurement, supply and use o f OPV; (ii) supporting supplemental operations; and (iii) surveillance. IDA w i l l support only the f i rs t component. Supplemental Immunization Activities (SIAs), in which the OPV w i l l be used, require supporting activities such as logistics, social mobilization, training, surveillance, monitoring and evaluation. W H O and UNICEF w i l l support these activities through bilateral donor and private agency contributions.
The following indicators will measure the project’s success:
0 Arrival o f OPV at the EPI cold rooms in Islamabad at least five weeks before each o f the SIAs, to be measured through the EPI’s vaccine arrival reports; and
0 SIA coverage o f 80% achieved in the remaining endemic provinces during 2005, to be measured through a cluster sampling survey according to a WHO-approved methodology.
Government’s achievement o f the above indicators w i l l be a trigger for the IDA buy-down (see section D.5).
Distribution arrangements and storage o f vaccines in the EPI cold rooms at the national, provincial, and district levels are functional. During the planning and implementation o f SIAs, transport o f these vaccines through vaccine carriers to the children i s coordinated with the vaccination teams. Social mobilization and IEC activities with parents and communities are organized at the local, district, provincial and national levels. Media campaigns in visual, audio, and print form are carried out to make the public aware o f the program benefits and to motivate them to receive the vaccination teams. Mobilization o f community leaders, health staff, and volunteers for planning and implementation o f SIAs i s a key activity. In Pakistan, about 700,000 personnel are needed for each campaign o f whom 150,000 are M O H employees, including 10,000 vaccinators and 42,000 Lady Health Workers. The remaining, about 550,000 include other government staff, N G O staff and community members. Training and advocacy with these groups in micro-planning, supervision, administration o f OPV, record keeping, and cold chain maintenance occurs prior to each round o f immunization.
By Component:
Project Component 1 - US$20.00 million
The first and the only component that the project will support i s the timely provision o f part supplies o f OPV needed for eradication campaigns to immunize al l children below five years. I t wi l l also monitor the appropriate use o f this OPV under the PEI. IDA w i l l finance the procurement o f about 50 % o f the OPV needed for the S IAs to be carried out from 2003-2005. UNICEF will supply the vaccine under an agreement between GOP and UNICEF. The Bank has accepted use o f UNICEF procurement procedures for the OPV procurement.
- 25 -
The component’s success will be measured by the following indicators:
Timeliness o f GOP’s request for funds for procurement o f the OPV: GOP w i l l send, within three weeks o f project effectiveness, a withdrawal application to the Bank requesting payment to UNICEF.
0 Timeliness o f disbursement o f WB funds to UNICEF for OPV procurement: Bank wil l transfer funds to UNICEF within 30 business days o f the date on which the Withdrawal Application i s received by the Bank.
0 Timeliness o f procurement and supply by UNICEF; the OPV w i l l arrive at the EPI cold rooms in Islamabad at least 5 weeks before each round o f SIAs.
Funds w i l l not be handled by GOP and w i l l be transferred directly to UNICEF. Accordingly only UNICEF w i l l provide financial management and accounting for the funds and provide quarterly reports to the government with copies to IDA. IDA w i l l use these reports to monitor the outstanding balance and the funds received and spent by UNICEF.
S I A s coverage i s monitored by an analysis o f the tally sheets recording the number of children immunized against the number in the target group. Output monitoring i s undertaken at the provincial leve l through independent monitors, and impact monitoring at the national level through the AFP surveillance system. The Technical Advisory Group meets periodically and assesses progress. I t s reports, along with the periodic assessments o f the S I A s quality undertaken by W H O and other technical partners, are also used for monitoring and evaluation purposes.
W H O w i l l evaluate this component within three months o f the project closing, focusing on the timeliness of OPV procurement and supply, and vaccination coverage. W H O w i l l submit i t s report to GOP with copies to Bank.
- 26 -
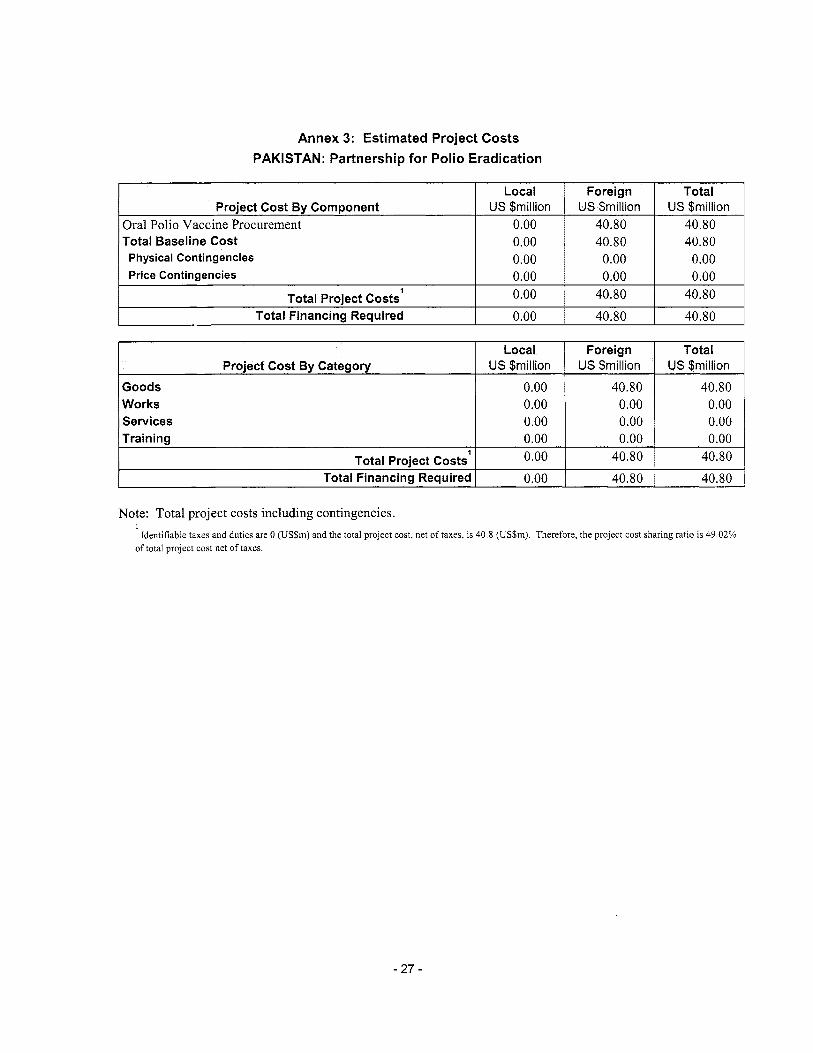
Annex 3: Estimated Project Costs PAKISTAN: Partnership for Polio Eradication
Local US $million
Oral Polio Vaccine Procurement 0.00 Total Baseline Cost 0.00 Physical Contingencies 0.00 Price Contingencies 0.00
Total Project Costs’ 0.00 Total Financing Required 0.00
Local US $million
Goods 0.00 Works 0.00 Services 0.00 Trainina 0.00
Project Cost By Component
Project Cost By Category
Foreign Total US $million US $million
40.80 40.80 40.80 40.80
0.00 0.00 0.00 0.00
40.80 40.80 40.80 40.80
Foreign Total US $million US $million
40.80 40.80 0.00 0.00 0.00 0.00 0.00 0.00
1 Total Project Costs
Total Financing Required
Note: Total project costs including contingencies. I
Identifiable taxes and duties are 0 (USSm) and the total project cost, net o f taxes, i s 40.8 (US$m), Therefore, the project cost sharing ratio i s 49.02% o f total project cost net o f taxes.
0.00 40.80 40.80 0.00 40.80 40.80
- 27 -

Annex 4: Cost Benefit Analysis Summary PAKISTAN: Partnership for Polio Eradication
GLOBAL HEALTH STRATEGEES VERSUS LOCAL PRIMARY HEALTH CARE PRIORITIES - A CASE STUDY OF NATIONAL IMMUNTSATION DAYS IN SOUTHERN AFRICA
B Schreudcr, C Kostermans
luildrng on thP succasful eradication of smallpox, the World Iealth Organisation, together with other agencies, is tiow ntiving quickly to the eradicatlon of poliomyelitis, originally imed for the year 2WO Plans for the subsequent global bradication of measles are in an advanced stage txadication jt both polio and measles incorporate ab LI fundamental tsatcgy high rouhne coverage, surveillancc and special iatronal immunisation days (NIUsf, which are supplemen- ary to routine vaccination services
There has been a Itvely debate o n whether punr countrieb, hi th many health prohtems that could be contmiled, should livert their l imited resources for a global goal of eradication hat may have low priori ty for their children From a cost- :ffectiveners pcrspective, NIDY are fully justifiable €-Towever, i c ld observations in s u b 4 ~ a r a n Afr ica show that KIDS Iivert resources and, to a certain extent, attenhon from the ievelopmcnt of comprehensive prunary health care (PHCI l’he routine immunisation coverage rates dropped o n JvPragc since the introductton of NIDs tn 1996, which is contrary to what was obser t td m the western Paafir and tither regions
The additional investment to be made when moving from disease control to cradication may exceed the financial capacity of an individual country Since the industrialwed countries benefit most from eradicahon, they shouid take responsihility for covering the needs of those countries that cannot afford the inveshnent. The W1IO’s trequcnt argument that NIDs $?re promotive to PHC 19 not contfrmed in the s i t i i th rm African region The authors think that the CVl 10 should, therefore, focus its attention on diminishing the negative side-effects of KID5 a n d on g e t t q the positive 5idr effects incorporated in the integrated health services in a siistdinablc way 5 i t r k i d * ?101 91 24.) 3 4
- 28 -

In disease control one can dishn@h between effective control, eliniinat~on, global erz~dication, and extinction A l l require deliherate eftorts
Effectii e wnt ro l i s the reduction of disease inadcnce, pre‘calence morbidity or mortality to a locally acceptable le\ el, while ehminahon of tiiscaw or infection 15 the wduclioii to Lero (if the Incidence in a defined geographical area Both mntrol and clinimahon require continued control measure6
iricillence o t infection caused hy a specihc agent, inter\ ention measure< are no loner needed. Extinction occiirs when the specific agent no longer exists in nature or the lauorator:,
From an economic point of blew, elimination 19 generdll) considered tu be I n s cost-effective than ciiseast, cctntm!, since the cost per case controlled usually follows tne iavi of diminishing returns E1 adicatlon L\ espccia11> attractwe, 6mce an) specific iiiterVeiitiOn can be stopped after global ~ert i f icat ion that transmission of infection has ceased
G lnhd eradication i s the reduchoii to t w o of the wor idwide
Huildmg on the sticcessf~il eradication u!’ smallpox in 1979, the World Health Organisat~on (WiO), United Nations Children’s Furid (UKICEF) and other agencies are no& mavin!: quickly touards the eradicahcm of poliomyel~tis, w h x h they hqw to achieve by the year 2000 Plans for the global
The cradicabon programme5 for polio and measles incorporate the folio% ing three fundamental strategies high routine coverage, supplenicntal vaccination (national ininiunisatioii dam (EvIDs)) and active sune i l lmce In particular the hIDs have occasioned In ely dchate, w i t h
posi tlnnb
to ha te 2 annual NKh 1 month apart in the cold beason,
a l l children below the age ot 5 >ears, regardless of their taccination status i’v’ith regard to measles, countries h a v e done campaigi5 among children aged between 9 monthr; and 14 1 ears Malawi rmp1cmcritt.d i t s campaign In September 1998 and Suazi land ant1 South Mrica did mathematical m i i d ~ l l i n g to show when the follow-up campaigns must be held
cannut he schiebed through routine sersiccs a h i e They demonstrate the enormou’r savings that can be* achieved alter cradiration, owing to the highly fakourablc c o ~ t - e f f e c t i ~ e n w
ale i n an advanced stage
i I proponents and opponent5 sometimes laking dogmatic
In the southern A f r i cm siib-region, the strategy for polio is
i 1 wnt inu ing for up to 3 years. The taiget group for vaccinahon is
I
On the line hand, proponents of NID. il.iim that eradication
(C/ El ratios Im On the other hand, opponents claim that the almost ni i l i tarv bertical approach of W I D 5 competes w i th and riegatit elv affect3 comytretiensivr primary health Cart’ (PI IC) de\clopment Some a l w feai thdt eiadicahon btrategies are bccoming thcl publ ic health strategies for the coming century, diserting fu dten t ion from the continuous care of x ulncinble ~ n d i v i d r i a l ~ In
M a r i h 2U01, \<>I i ) i \ c ! 3 5AMJ - 29 -
their vieti Strenpthenmg rovhnc immiinisatitxi wrviccb 14 mrorc. sustainable
l h i s article attempt< tit br ing both partis togetlier h\ considering puinh ot mutual agreement It has been r$ritten from personal partiapetion in the first rounds of Nllh as well as pa tk ipa t i on in the southem 4frican sub-regional planning and ctaluat ion meeting\ of n.iticinal Eqxnded Prngnmme fur Ininiunisaticm (EPI) managers, orfiani’ed bt the W!1014frica Acgianal Otfice (AFRO) Costs and operationaf aspects of Nflk in southern Africa are also analysed in thii study Finaliy, the study includes replies or subscriherc. to the Afro-h‘et discuszion group on X1Ds Replies were to thc foflowing questions ( 1 ) CVhat are the direct costs ibo t l i human and mcvictary)’ { r i i Can an indi%idual countq atford not tu participate in a glnbal init iatitc7 (iiii I-low docs an indiviriual poor cnuntr) benefit from M D s ’ ( iv) What are the negative effccts of KIDS on suztainability of PHC’ ( P ) Can the% effects he minimised’
THE DILEMMAS O F ERADICATION ln their article cntitlrd ‘Ethical dilemmas in current planning for polio eradicatiim’, Taylor cf ti! looked at the d i l e m m ~ s nf polio eradiration a t Slobal level Tlir authors expressed their concern at the intcnsi:ication of wor ldwide cradrcation ctfort. UI particular the organication ot h1Lh The authors also raise questions regarding the balance between g1obal goalls and Ioc pnorihe3 and the resulting ethical implicaiicinz.
Probabl) the most important qucstion raised b j the author 15 bvhethcr pmr countneb, M i th many cni?ttollahle health problems, shouid divert their lrntitcd reiourceb tctwards a global goal that ha3 low priorit); for theii r lu ld ren Cnfortunately the author5 do not pro.i.!de a clear-cut answer this yueshon T h s article attempts to provide cur t i dn answe for smithern At rica
What are the costs of NIDs? A cost study of \IDS in the sctulhem A f r i c m \ V I 10 sub-rep showed that thc aicragc direct cnst per saicinated chi ld of f \
round5 of pcilio vaccint wil i dio:rnd L‘SS0.92 Thrz iriduded cost of vaccines, training. logisticb, and social niobii isation V;iccines, a t 4 8 O 0 (if the total, ctsn&tuted the niajot cost 7hc cnst ~l a single mea4cs \nccin;ltion dnr ing a cantpaign, gi\ en with a disposahlc synizgc that is p roper l j destr close to US1 %me s a l ings can be m d e h) gi and pLio vacc.ncs at the 5 d m ~ bme, hut the dr operatima1 strategrez tnr polio acid 1 i i e a 4 ~ ‘ ~ twdicat ic in ma! not a’ways allow tor thi\
The total cwts of NIB in thc sub-region ha\ e been calculaled. For polici $\e ~ssirmr.d thc max imum ” x i o three annual ran ipa ips of t w ) rnunds for al l children a& under 5 >ears For mcaslcs \be aizuined three campaigns init ial campaign for a l l chi ld icn appd between 4 month% d
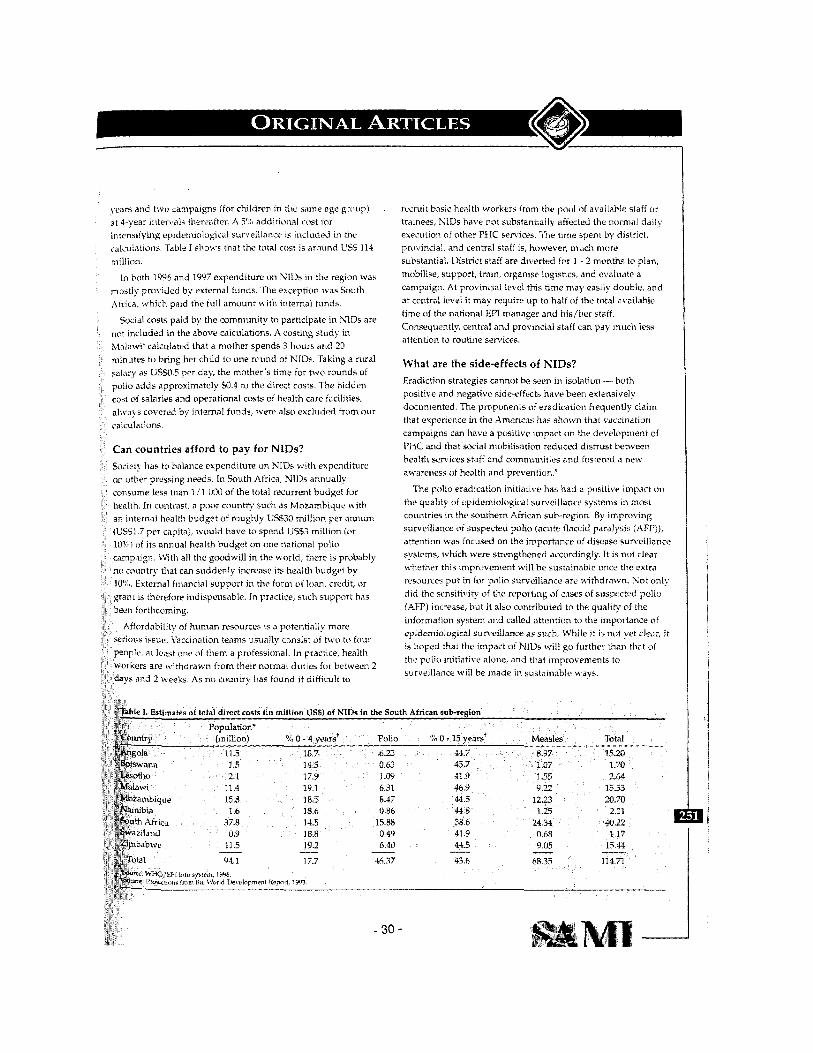
tear’ i ana t w o campaigns (for children in the m n e age group) a i 4-vear i r i tcnals thereafter A :‘I dddi:iotral r o y t for intenvrymg epidemialol;ical survcillance is included in the cLslcuiations Table J shows that the total cost 1% around US$ 114 imilllon
mostly prcivided bv external funds The exception l+as Eouth .\tr$ca, which paid the tu]! amount ~ i t h internal funds
In hith 1996 and 1997 expenditure on XIUS in the region \%a\
501-1J1 costs paid by the comniunity to parhcipatc in NIUs are not included in the above calculations. A cosnng stud) in Malawi ‘ calculated that a mother ~pends 3 hours a n d 20 minutes to bring her chi ld to one round of NIDs Tahng a rural salary a i L‘SW 5 per day, the mother’b hme for two rounds of polio adds approximatelv SO 3 to ;he direct costs The hidden cog of w1arie.i and operational costs uf health care facilities, ais\+ s covered by internal funda, \+ere also excluded from ~ t i r
Can countries afford to pay for NIDs? Suciet’i has to balance cxpendituro on NIDs w i t h expenditure on other p i e w n g needs In South i i t r ica, N I h annually comume les- than 1 ,’1 OMl of the totai r r cu r tm t budget fur
21th In wi i t iast , a poor country such a’i hlozainbiquc w i th in tcmal health budget ot rough11 L‘SS30 mi l l ion per annum
S51 7 per capita), would h a t e to spend L553 million (or %I of its annual health budget on one national polio mp’ugn tVith all the goodwi l l in the world, there 13 probabl) countr) that can suddcnlp increase i t s health budget by
<’% External financial support in the torn1 of loan, credit, or ant IS tireretore indispensable in practice, such support has
fordability o! hunian resources IS a potenhally more u c izwt’ kaccmatlon teams usuallv consist of tMo to four
<)pie a \ least m e of thenr a protessional In practiie, health rkers are wi thdrawn from their normal d u t m fnr between 2
ys and 2 weeks As no countr! has found it di t f icul t to
recruit basic health work trainees, KIDS have not substantially aifeckxl the norni‘il d,tily exemtion of other PHC services. The time spent by district. provincial, m d central staff is, however, much more substantial. District staff are diverted for I ~ 2 months to plan, mubilise, support, train, organise logisrics, and evaluate a campaign. At pruvincial level this t ime may easily double, and at central level i t may require up to hal f of the total asailnhlc time of the national EPI manager and his/l icr staff. Consequently, central aid provincial staff can pay much less attention to routine services.
What are the side-effects of NIDs? Eradiction strategies cannot be =en in isolation ”- both positive and ncgative s ide4fects have been extensively docuniented. The propunents of eradication frequently claim that experience in the Americas has shown that vaccination campaigns can have a positive impart cin the developmcnt of PZiC and thatkocial mnbilisntion reduced distrust between health wrvices staff and cwnni unities and hstercd a new awarelies of health and preventicin.‘
the quality of cpideinicilogical surveillance systems in niwt countries in the southern African suh-region. By imprnsing surveillance of suspected polio (acute Claccid paralysis (AFI ’ ) ) , attention was focused on the importance of disease surveillance syslrms. u#hich were strengthened accordingly. I t is nttt clear whether this improvement will be sustainablc m c c the extra rcwurces pu t in for pol io surveillance are withdrawn. S o t only d id the sensitisih; of the reporting of cases of suspcctcd pol io (Am) increase, bu t i t also contributed to the quality of the
,tern and called attenticin to the importance of 1 surwi l lance as such. While if is nu! y t clex, i t
is hoped that the impact of NlUs will go further than that of the pol io init iative alone, and that improvements to surveillance will be made in sustainable ways,
rorn the pot11 of availablc staff OT
The pol io eradication init iaiive has had a posi t ivr impart on
0.86 15 a3 0 49 6 40
46 77 -
- 30 -
3
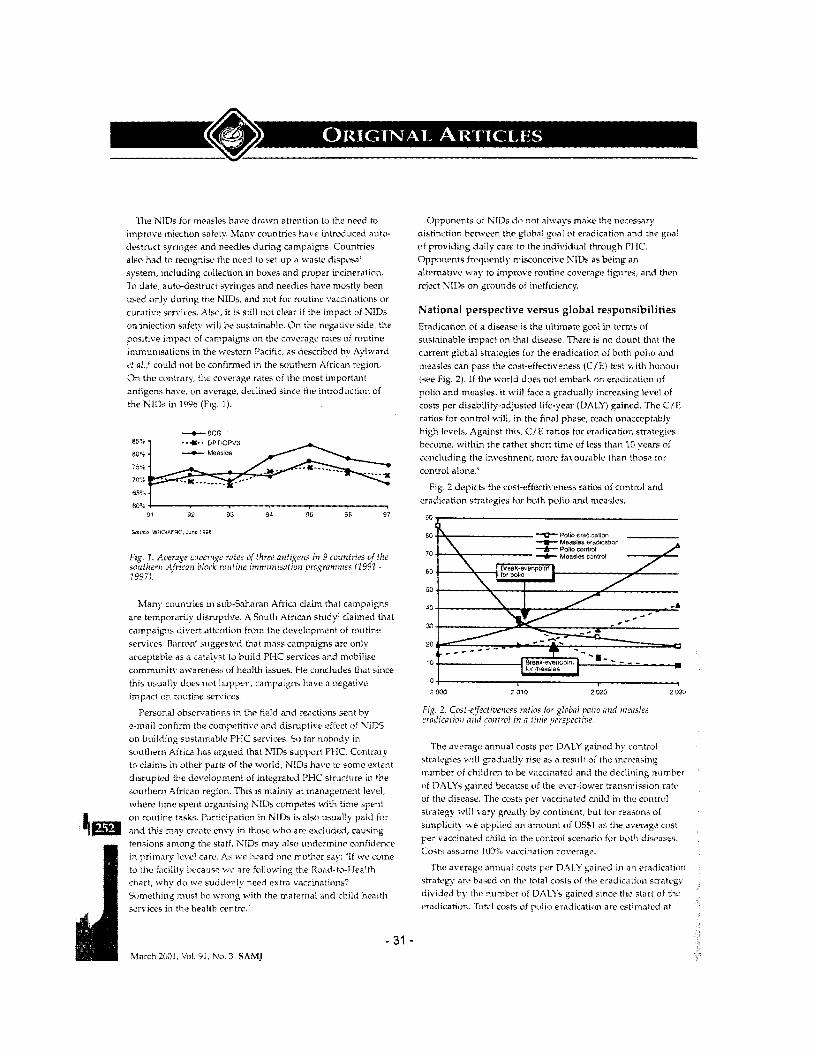
l l t e NlDs for measles have drawn attention to the need to improve injechon safety. destruct syringes and needles during campaihms. Countrit5 also had tc rec(igniw the need to set l ip a waste diymsa! system, including ctdiection in boxes and proper incineration. To date, auto-destruct syringes and needles have mostly been used only dur ing the NIDs, and not for routine vaccinations or curatise services. Also, i t i s sti l l not clear i f the impact of NIDs on injection safet! wilf be sustaindbie. On the negative side, the posihve impart of campaigns on the coverage rates of routine imii~unisaticins in the western Pacific, as described by Aylward ?! 01.: could no t be confirmed in the southem African region. On the cctntrary, t l ic coverage rates o i the most important antigens have, on average, declined since the introduction of the NlDj in 1496 (Fig. 1).
countries have introduced auto-
Many countries iii subSaharati Africa claim that campaigns are temporarily disritptire. A South African study' claimed that campaigns divert attention from the rierelclpinent of routinc services B;irrcm* suggr*sted that mass campaigns are only acceptable as a catalyst to build P I X services and mobilise community a ~ a r e n e s ~ of health issues. kle concludes that bitice this usually does not happen, campaigns have a negative impact on roctinc senices.
I'erscmal obsenrationr; in the fiold and reactions sent by e-mail c m f i r m the competitive anti disruptive effect of X'S on bui ld ing sustainable PfiC services. Si) far nobody in southern Africa has argued thd KIDS support P I K . Contrary to claims in other parts of the world, NlDs have to some extent disrupted thc development of integrated PHC structiire in the southern African region. This IS mainly at management level, tshcre time spent organking NtDs competes w i th tinie spent on routine tasks I'arricipation in NlDs is also usually paid for and t h i s may create envy in those w h o are excluded, causing tensions among the staff. h'Ib may iilso undermine corifidencr
lwe l care. As ICB heard oiic mother say: ' I f we come i t? becausc wc are fo l l im ing the R c m i
chart, why do we suddenly need extra vaccinatici S [mc lh ing must be wn ing w i th the matemdl and chiid health services in the health centre,'
Opponents u t NIDs do not al>*ash make the necessary distinctim hehvffn the ~ l o b a l goal ot eradication and thc goat of prosiding dails caw to the indrvidual through PHC Opponmts frequently t~ i i sco i i ce i~e XIUS as being an altcmativc w a y to improve rouhnc cmera rrlect \lI)s on grounds of ~nef i ic ienry
National perspective versus global responsibilities Eradication ot a disease is the ulti inate goa. in terms uf wstainablc impar t on that disease There i s no doubt that the current glcbal strateg~es fur the eradication of botb puiio and meazles can paw the cost-etfcrtivenes (CICI test with honour (see Fig 2) I f the \+torid does not embark on eradicatiun of polio and measles. i t will face a gradual11 tncreasmg IC\ e l of cost5 per disability-adjusted life-year (UALY) gained The f / F rahos for conwol will, in the hnal phase, reach unacceptahlv high lebels Against this, C I F iatios for eradication strategies become, withm the rather Short time of less than 10 vears of concluding the investment, more fasourablc than those tor control alone
Fig 2 d~p ic t s the cost-effectwenesz rahob of control and eradicativn strategies for both pol10 and measles
90
80 Polio e m salton
70
EO
20
Measles ersdL60oP
40
30
20 10
s 2 ma 2 010 2 020 2 050
Fig. 2. Cosi-eJrectiocrtm ratios,&or s / r~boi / i c h i i d I ~ : L * ~ I E I erodicatioir aiid co,tt.rd in ii f ! r w prrspect ix
The average annual costs per DALY gained hy control strategies will gra&Aally rise a5 a result of the inweasin$ number of children to be vaccinated and the declining number oi DALYs gained because o f the erer-lower transmission r a t r of the disease, l l i e COS& per vaccinatcd chi ld in thc control strategy will vary greatly by continent, bu t for rea3ons of simplicity we applied a n aniount of US51 as the average cost per vaccinated child in the control scenario for both diseases. Costs assume IUO?c vaccination coverag?.
The averagc annuc~l costs per I)hI.,Y g'iined in an cvx i i ca t ion strategy are based on the total rnsts c t l the eradication strategy div ided by the number of DALI's gained since the start of thc eradicaiivn. Total costs ot pcilio eradication arc estiinatcd at

l"+J hrllion, and that tor measle> at LES3 7 billion (L'NICEF I Y V ) The ,irerage ,iiinunl costa arc the result of the dirisioii ni the total u s t s b y tw number ot w a r s since tht, start of eradication A Y', annual dtscountinji has bcwt 'ipplied tO ~cirrect for ut i l i ty in the future
It 15 assumrd that tor both polit) and measles al l routine \ accinatiors 1.1 11; be 5wpended rf a w-odd free of polio or mea5 e\perted numbers of DALYs ga trend? presented in the tlihil Burden of Diseasffi sericb '
Bart e: o l demonstrated that enormous savings pa:ticuiarl> 1 the i i idurtriali ieci wcvld, would be ma& after the global tv t i i r ra t " ui a wor ld free ot polio The future savings matie
investirig nu\+ in erd ica t ion efforts are suh.t.mtia1 rhese vings sho t ld be used tt) Support the iur thcr development o f tegrated PHC, and to compensate for the d:wuphon to these n w e s that RlUs are currently provoking
Init iative5 for global eradication of disease are comparable t t )
thcr globdl a p e m e n t c between ctmntnei on i$sucs sitch ab an r gilt'. and the banning of land rnines anrl nuciear wTu Gibe11 its great impact, such an agreement should k e ared w i th the greatest poswhlccari and on11 c n d o r d i f xpcctcd contribution of each i n d i r i d m t couiitrj IC defined
e e radmt ion of polio wa5 endoiwd bc a 1Q6R global lution of dl member states of the WHO and was rmed at the Woild Summit for C hildren in 1090 On both i m s the endorsement of polio eradication wac bawd
> on technical fcasib~l t ty anti expected future benefits icatioiis itf hlU5 un health s?stcms and I ' I i C were not
nce eradication 13 J. global inltiati\e, coninutmcnth 4iould h a d according to c a p a a t ~ between the 'iid\cs' and 'has e-
A h long a& there 15 no consensus regding their rtance, eradicatwn inihatites mal not receive the sar) hroad support and funding I f the in i t ia l i te is no t h r ~ d bv denors i t becomes an empty statement, and the
e-rwts' can only adopt H pozturr nf ~ F I S S I V C re5istanct:
'1 i i o r i c tan p i n t oi \ iew the indu5tria 5 most trom rapid rradication J 1 t : ~ e v c v the heneiits in reduction dre greater in developing countries where the ce ut new cases of both polin and measles i s higher
or rt .I] raise the question i:1 wliethcr poor coiirtrie5 ant hcalth pr&iem? should divert their l imi ted 15 tohard$ d p,hhal giial that hd\ ]OM [~ri(irit> for their idii.ri Bc cieiinitiim, global eradication mitiati\-e- tiwd
-port of all counbies tit the 'oiintrv could lpopardi.-e tn
~ n d i i iduai countr> refu.es n t i m i i t w w i d not he iuirtthicni to cxcic iw w n i e re on t ia t coiintrr I i that c n u i ~ t r ~ , I i ~ ~ \ e t PI, wttcr5 froni lntc in implementation, thcn com:iiittcd c u i i ~ i t r i c ~ \ i o
- 32 -
greatw resiti~rces should he prcpared to a prnvidinp vaccines Cir covering recurrent
One can qucsticxi ivhether NlDs arc a n absoiiitc requirement for cradicating polio, lii fact, NIB have neve: been undertaken in the USA and Canada. Other countries w i th h igh routine ctrverage ratcs and R reliable sunseillance system in place (including %u:h Africa) decided not to complete the tiill set of *i years of two rctunds of NICs, relying rather on their surveillance y t e m as a prerequisite for the 'Free of polict' certification,
fioweuer, the a r r e n t coverage rates of the rtiutine El3 services in .some countries in the southern At r i ian sub-region 'Ihble 11) do not proside a solid basis for achieving tht: target or globdl eradication of polio in d reasonable time period.
Comider ing that upgrading the roiltitie EPI services implies a major efftrrt. in the short term i t i s much organisc NlUs. The impart of NIDs on d probably greatest in those coiintries whew routine coverage is lowest. As a resul t of their weak infrastructure, these are probably the very countries that will evperieiice r w s t disruption from NlD5. To minimise the negative side-effects in thest: countries, NiUs must be planned s e ~ carefully and well in advance. Instead of persisting in p m t i r i g out the positive i m p i t NlDb have on PllC, the bi 'J I0 would dtr better lo pay more attention to the negative side-effects of KIDS. I f PHC hits to be stren#hened, there are mom appropriate ways of doing $0.
Tne rrcation of vertical S IDs structure s h d d not he blunt ly
i reiected. I t scrves a conipleteiy different obj ind i \k lua i care pro\*ided hy the integrated P e r i d i c campa1gn5 can never repiace the ctmtjniious rare of I'T-JC
The discirssicin sht.iiiid, therefore. no t he about whc-ther nhtjons should be administered thrrrugh routine servicei
or through h'l l )s. Sucicty needs integrated I'tlC, and i t nt)ed;i 1% on a tcmpnr,iry I n s i s to eradiciitr di
Eradication initiative3 could contribute to sustaiirahle develnpmcnt of thc hcalth infrastructure by improving epidemiological s u n d i a n c e systems. This w i l l riot cinlj, hc beneficial to the health infrastructure as a rshole, but will also prevent too many vaccination,c being administered, a possibility in unreliable surveillance systems. Investinp in surveillanrt. will quickly pay off.
Since the Alma Ats conference in 1970, disciissions PI: the extent to which target-driven progrsmnies affect sustainable Pi IC have been polariseii. The limited health budget has to bc div ided betwren both rradicaticm yrogramines arid PHC, and in that respect they arc comp?ti:xve. Dur ing the past 20 years target-driven vertical progranmes have been scpirate from and have ccimpeted with integraird PHC. Each system contributes in i t s own way towards improving health. Both systems have a vertical targct dimension and a horizontal indiv idual care dimension, The vertical dimension i s stronger in target-driven programmes, the horizontal i s stronger in PIIC. Vertical programinei may have a rpecial placc in certain phases of the fight against disease% namely in the beginning to start up a t x q p " e and at thc end to finish the job. To date, the world is still d iv ided into horizontalists and wrticalists. Both groups would do better to si1 down togethcr and wease the horizcintal arid vertical i ibr ts into a sustainable wcb.
I'he views expressed in this nrtiilc 'ire those ui the authors and should not be attributed to their respective organisations.
\2ic thank the following people for providing ideas and ccimnli?nts [in thii article: Julie Cliff !Univrrsidade Cudardv Mondlane, Maputo!, Felicity Cutts il.,ondon Schml of Hygiene and 'Iropical Medicine), I lilbrarid t h a k (Consultant for i.fi.alth Devciopment, Leidcn), Robin Biellik (WHO, tla:.are!, I.ucy Giison (Centre for Health I'oiicy, Cnisersily ni the CYitwatersrand, johanneshurg).
RE-lWW,<eS
: M h IR'crMmp ,&mm
- 33 - \ . l . r ^ C ? , \ t 7 ~ ,'..I u, h,. 2 C h h l l

Annex 5: Financial Summary PAKISTAN: Partnership for Polio Eradication
Years Ending
I Year1 I Year2 I Year3 1 Year4 I Year5 I Year6 I Year 7 Total Financing Required
Project Costs Investment Costs 21.8 10.8 8.2 0.0 0.0 0.0 0.0 Recurrent Costs 0.0 0.0 0.0 0.0 0.0 0.0 0.0
Total Project Costs 21.8 10.8 8.2 0.0 0.0 0.0 0.0 Total Financing 21.8 10.8 8.2 0.0 0.0 0.0 0.0
IBRDllDA 7.8 8.8 3.4 0.0 0.0 0.0 0.0 Government 0.0 0.0 0.0 0.0 0.0 0.0 0.0
Central 0.0 0.0 0.0 0.0 0.0 0.0 0.0 Provincial 0.0 0.0 0.0 0.0 0.0 0.0 0.0
Co-financiersJapan 14.0 2.0 0.0 0.0 0.0 0.0 0.0 User FeeslBeneficiaries 0.0 0.0 0.0 0.0 0.0 0.0 0.0 U N IC EFKDC 0.0 0.0 4.8 0.0 0.0 0.0 0.0 Total Project Financing 21.8 10.8 8.2 0.0 0.0 0.0 0.0
Main assumptions:
Financing
- 34 -
Annex 6(A): Procurement Arrangements PAKISTAN: Partnership for Polio Eradication
Procurement
Procurement Capacity Assessment
As per the Director OPCPR’s Memorandum dated October 17,2002, a formal assessment o f the procurement capacity o f the Federal EPI Cell (Project Implementing Agency) i s not necessary according to Procurement Services Policy Group guidelines dated August 1 1, 1998. This i s because under the project, UNICEF, and not the implementing agency, will handle procurement.
Procurement Planning
The quantity o f vaccine required i s determined b y the needs identified by the Technical Advisory Group (TAG). These needs are regularly adjusted based on surveillance findings. If surveillance shows unexpectedly good results, and not al l project funds are needed for procurement o f OPV for during 2003-2005, through the f i rs t quarter 2005, IDA funds will be reprogrammed for the procurement o f OPV needed for in the second hal f o f 2005 and in 2006. If TAG determines that are no longer needed, the available funds wil l be used for procurement o f polio vaccines for the routine immunization program. A TAG recommendation to this effect wi l l be needed.
Procurement Implementation Arrangements
The Federal EPI Cell w i l l be responsible for project execution at the national level. While EPI i s a strong program, i t has limited capacity for procurement, especially for large scale international procurement o f the kind required under the project. The borrower will enter into an agreement with UNICEF for the supply o f the oral polio vaccine (OPV). UNICEF wil l ensure supply o f OPV to EPI. EPI will be responsible for the in-country storage, distribution and administration o f the vaccines. UNICEF w i l l report on a semiannual basis to the Government o f Pakistan with a copy to IDA on (a) purchase orders placed by UNICEF, (b) actual quantities o f OPV delivered to NIH, and (c) expenditure from the OPV Procurement Account during the reporting period. Payments to UNICEF w i l l include i t s standard handling charges for vaccine procurement, an amount not exceeding 6% o f the vaccine cost, and other non-freight costs, if any.
Procurement Methods
Goods (Vaccines)
All goods to be financed under the IDA credit shall be procured in accordance with the Guidelines for Procurement under IBRD Loans and IDA Credits, January 1995, revised in January 1999. Specifically, the goods w i l l comprise OPV only, which shall be procured from UNICEF in accordance with the provisions o f Para. 3.9 o f the Procurement Guidelines.
The Credit w i l l finance OPV for U S $20 mill ion under a single agreement with UNICEF for the supply o f OPV. IDA w i l l clear the draft agreement before signing.
IDA Prior Review
- 35 -
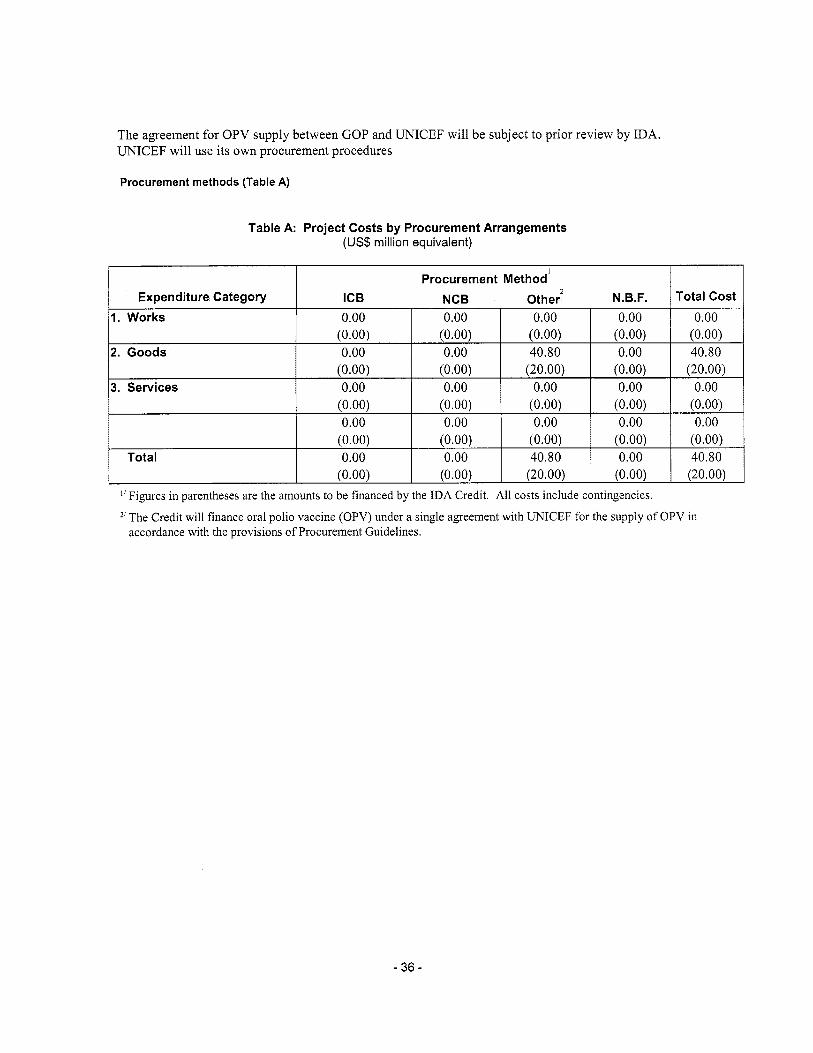
The agreement for OPV supply between GOP and UNICEF will be subject to prior review by IDA. UNICEF will use i t s own procurement procedures
(0.00)
Procurement methods (Table A)
(0.00) (20.00) I (0.00) I (20.00) I
- 36 -
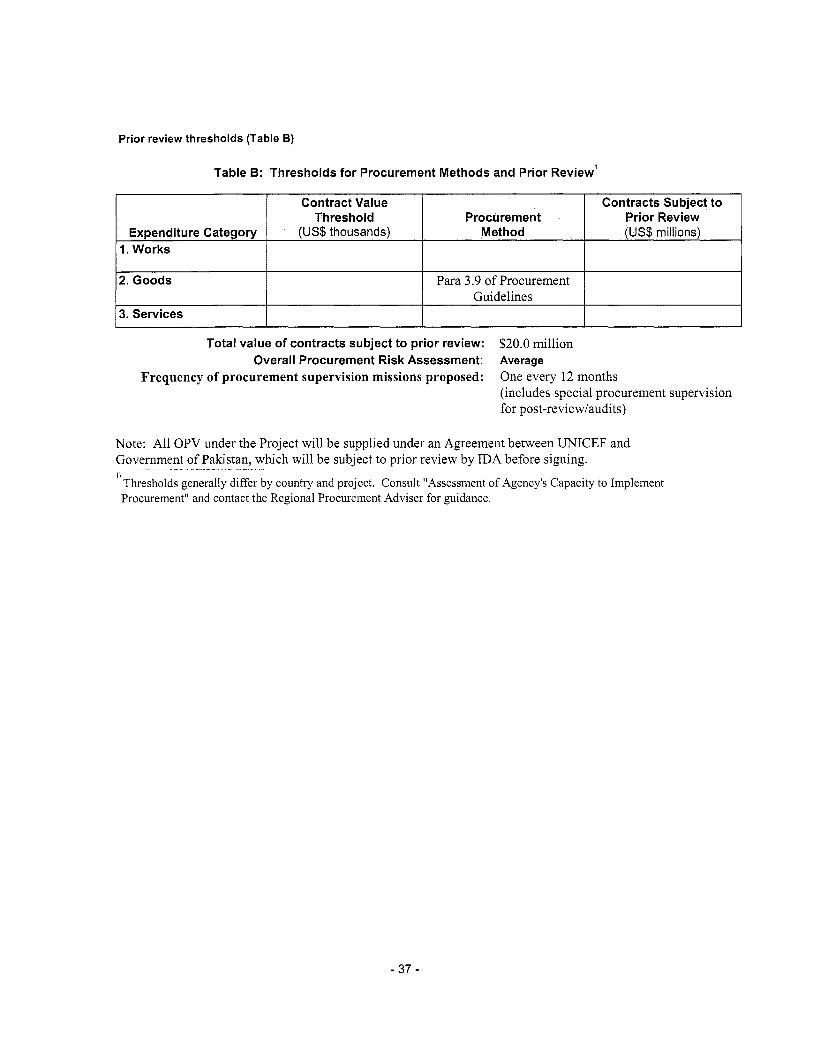
Prior review thresholds (Table B)
Expenditure Category 1. Works
2. Goods
3. Services
Table B: Thresholds for Procurement Methods and Prior Review'
Contract Value Contracts Subject to Threshold Procurement Prior Review
(US$ thousands) Method (US$ millions)
Para 3.9 o f Procurement Guidelines
Total value of contracts subject to prior review:
Frequency of procurement supervision missions proposed:
$20.0 million
One every 12 months (includes special procurement supervision for post-review/audits)
Overall Procurement Risk Assessment: Average
Note: A l l OPV under the Project will be supplied under an Agreement between UNICEF and Government o f Pakistan, which will be subject to prior review by IDA before signing.
' Thresholds generally differ by country and project. Consult "Assessment o f Agency's Capacity to Implement ~- ,
Procurement" and contact the Regional Procurement Adviser for guidance
- 37 -
Annex 6(B): Financial Management and Disbursement Arrangements PAKISTAN: Partnership for Polio Eradication
Financial ManaPement
1. Summary o f the Financial Management Assessment
NA
Overview o f Implementation Arrangement
IDA has entered into a partnership with funding agencies, Le., Bi l l and Melinda Gates Foundation, UN Foundation and Rotary International to support this project. The project will support a single component, Le., the provision o f oral polio vaccine (OPV). I t i s piloting an innovative financing mechanism: although IDA financial resources will be provided to the Government of Pakistan (GOP), third party funding from the above partners will "buy down" the service charge, the commitment fee and repayments by financing the net present value (NPV) o f the IDA credit. This would, in effect, mean grant funding for the program.
The IDA credit will finance a single agreement for the supply of OPV. An Agreement will be signed between the GOP and UNICEF for the supply of OPV with the arrangements below:
OPV will be procured by UNICEF for GOP following i t s own procurement procedures. The draft agreement between GOP and UNICEF will be subject to the Bank's prior review and no objection. GOP will send withdrawal applications to the Bank, authorizing the Bank to make direct payments to UNICEF of amounts requested by UNICEF under this Agreement, through an initial, and subsequently semiannual, withdrawal applications; UNICEF will maintain a separate ledger account, through which al l o f UNICEF's receipts and expenditures for the purposes of providing the services contemplated under this Agreement will be recorded; and UNICEF will report semiannually to GOP, with copy to the Bank, on the use of funds received including, (a) balance at the beginning and end o f the reporting period; (b) purchase orders placed by UNICEF during the reporting period; (c) actual quantities of OPV delivered and number of children immunized during the reporting period; and (d) expenditures from the OPV Procurement Account during the reporting period.
The above arrangements are based on the proposed agreement for supply o f OPV to be entered into between UNICEF and GOP.
Financial Management Arrangements
This project does not require direct involvement o f the Borrower in the management and accounting of funds, which will be the responsibility o f UNICEF.
The credit proceeds will be disbursed by the Bank directly to UNICEF as stipulated in the agreement between the GOP and UNICEF.
The needed quantities o f vaccines will be agreed in advance and the price i s relatively stable.
The Bank will accept semiannual reports from UNICEF as meeting the financial information requirements for Financial Monitoring Reports. The assurance that the Bank's fiduciary requirements
- 38 -
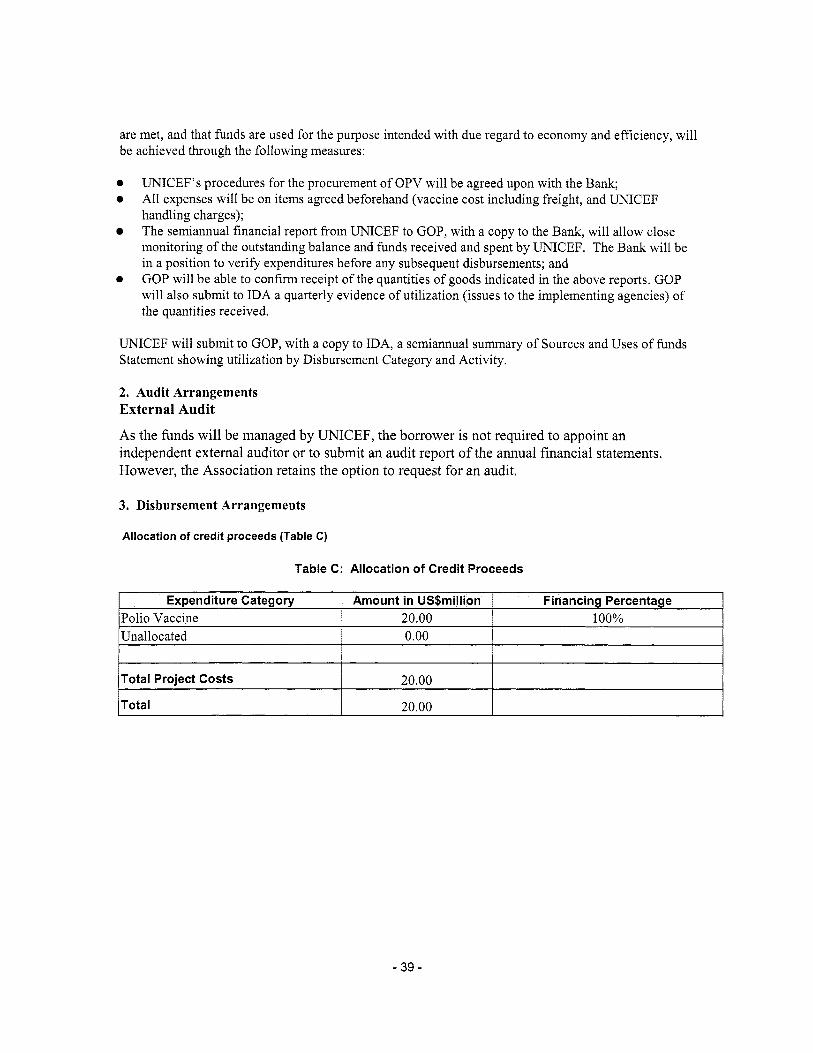
are met, and that funds are used for the purpose intended with due regard to economy and efficiency, w i l l be achieved through the following measures:
Expenditure Category Polio Vaccine Unallocated
a e
UNICEF’s procedures for the procurement o f OPV w i l l be agreed upon with the Bank; All expenses will be on items agreed beforehand (vaccine cost including freight, and UNICEF handling charges); The semiannual financial report from UNICEF to GOP, wi th a copy to the Bank, w i l l allow close monitoring o f the outstanding balance and funds received and spent by UNICEF. The Bank will be in a position to verify expenditures before any subsequent disbursements; and GOP w i l l be able to confirm receipt o f the quantities o f goods indicated in the above reports. GOP will also submit to IDA a quarterly evidence o f utilization (issues to the implementing agencies) o f the quantities received.
0
Amount in US$million Financing Percentage 20.00 100% 0.00
UNICEF w i l l submit to GOP, wi th a copy to IDA, a semiannual summary o f Sources and Uses o f funds Statement showing utilization by Disbursement Category and Activity.
Total Project Costs
2. Audit Arrangements External Audit
As the hnds wil l be managed by UNICEF, the borrower i s not required to appoint an independent external auditor or to submit an audit report o f the annual financial statements. However, the Association retains the option to request for an audit.
20.00
3. Disbursement Arrangements
Total
Allocation of credit proceeds (Table C)
20.00
Table C: Allocation of Credit Proceeds
- 39 -
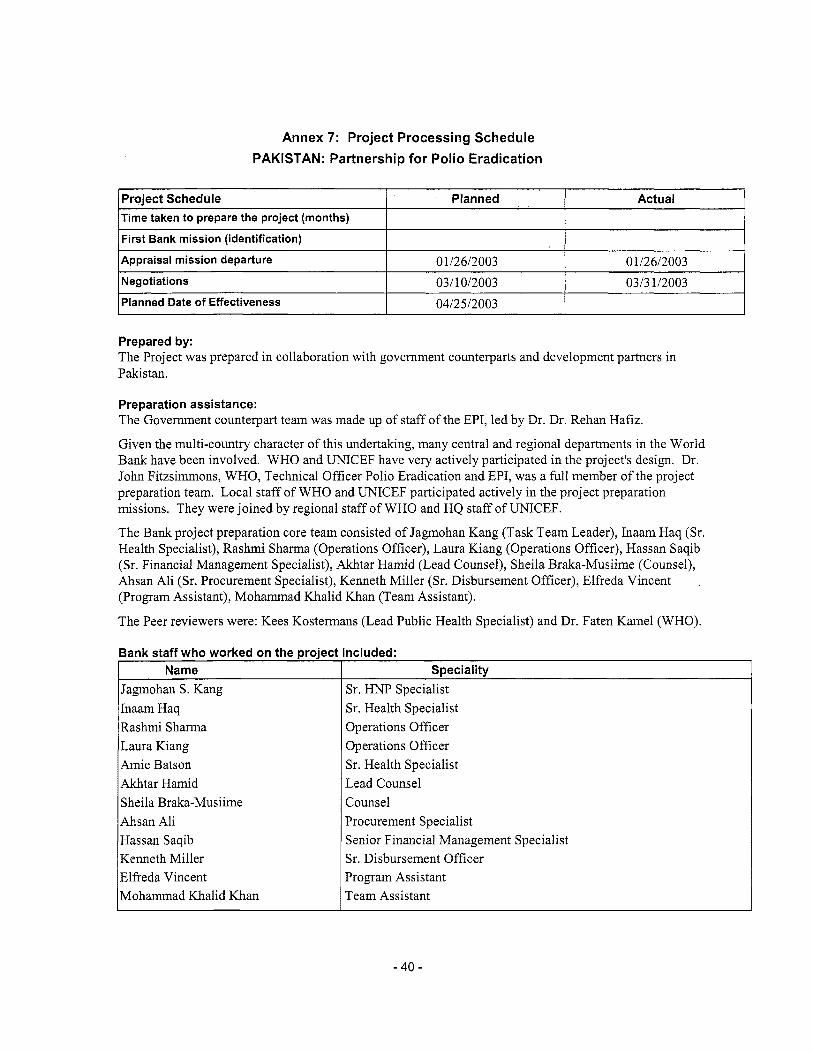
Annex 7: Project Processing Schedule PAKISTAN: Partnership for Polio Eradication
Project Schedule Time taken to prepare the project (months)
Planned Actual
I First Bank mission (identification) I I I Appraisal mission departure
Negotiations 0 112612003 Oll2612003 03/10/2003 0313 112003
I Planned Date of Effectiveness I 0412512003 I I
Name
Prepared by: The Project was prepared in collaboration with government counterparts and development partners in Pakistan.
Speciality
Preparation assistance: The Government counterpart team was made up o f staff o f the EPI, led by Dr. Dr. Rehan Hafiz.
Given the multi-country character o f this undertaking, many central and regional departments in the World Bank have been involved. W H O and UNICEF have very actively participated in the project's design. Dr. John Fitzsimmons, WHO, Technical Officer Polio Eradication and EPI, was a full member o f the project preparation team. Local staff o f W H O and UNICEF participated actively in the project preparation missions. They were joined by regional staff o f W H O and H Q staff o f UNICEF.
The Bank project preparation core team consisted o f Jagmohan Kang (Task Team Leader), Inaam Haq (Sr. Health Specialist), Rashmi Sharma (Operations Officer), Laura Kiang (Operations Officer), Hassan Saqib (Sr. Financial Management Specialist), Akhtar Hamid (Lead Counsel), Sheila Braka-Musiime (Counsel), Ahsan Ali (Sr. Procurement Specialist), Kenneth M i l l e r (Sr. Disbursement Officer), Elfreda Vincent ,
(Program Assistant), Mohammad Khal id Khan (Team Assistant).
The Peer reviewers were: Kees Kostermans (Lead Public Health Specialist) and Dr. Faten Kame1 (WHO).
Hassan Saqib Kenneth Miller Elfreda Vincent Mohammad Khalid Khan
Senior Financial Management Specialist Sr. Disbursement Officer Program Assistant Team Assistant
I Jagmohan S. Kang I Sr. HNP Specialist Inaam Haq Rashmi Sharma Laura Kiang h i e Batson Akhtar Hamid Sheila Braka-Musiime Ahsan Ali
Sr. Health Specialist Operations Officer Operations Officer Sr. Health Specialist Lead Counsel Counsel Procurement Specialist
- 40 -
Annex 8: Documents in the Project File* PAKISTAN: Partnership for Polio Eradication
A. Project Implementation Plan
Polio Eradication Project Through IDA Buy Down - Project Implementation Plan, Expanded Program on Immunization (EPI), Ministry o f Health (MoH), Government o f Pakistan, April 2, 2003.
8. Bank Staff Assessments
Proposal for The Government o f Japan, Polio Eradication Activities in Pakistan - 2003, Revised September 2002 - UNICEF.
Pakistan Integrated Household Survey (PIHS) - Round 4: 2001-02 - Federal Bureau o f Statistics, Statistics Division, Government o f Pakistan, Islamabad July 2002.
Summative Assessment o f Polio NID-October 22-24,2002 - submitted to UNICEF Islamabad by Gallup Pakistan.
National Orientation Plan - 2002 for All Supervisors & Team Leaders/ Members - Federal Communication Group - Islamabad, Ministry o f Health/UNICEF/WHO/Rotary International IFRC/JICA (Version-I - Spring Polio Compaign-2002 Round-11).
National Integrated communication Strategy - 2002, Routine Immunization, Polio Eradication & Vitamin-A Supplementation - Federal Communication Group - Islamabad-Pakistan Ministry o f Health/UNICEF/WHO/Rotary International IFRC/JICA.
Polio Eradication Initiative, Monitoring Guidelines, Polio Vaccination Campaigns Pakistan 2002, Revised February 15,2002 (In collaboration wi th Government o f Pakistan, W H O and UNICEF.
Progress Towards POLIO Eradication in Pakistan December 2002 - WHO/Islamabad.
Campaign Analysis for Provinces May-September 2002 (In collaboration wi th Government o f Pakistan, WHO, and UNICEF).
National Surveillance Bulletin-January 2003, National Surveillance Cell Federal EPI Pakistan (A monthly Bulletin o f the Pakistan Polio Eradication Initiative).
Executive Summary, Coverage Evaluation Survey, Expanded Program on Immunization Sindh, Balochistan, NWFP & FATA, Contech International Health Consultants, UNICEF.
C. Other
Agreement between Melinda and Bill Gates Foundation and the Wor ld Bank, June 6, 2002
Minutes o f HNP Sector Bord Meeting, December 5,2002.
Agreement for Procurement Services between The Government o f Nigeria by and through the Ministry o f Health and UNICEF, The United Nations Children's Fund for the Procurement o f Oral Polio Vaccine as part o f the Gpvemment's Campaign to eradicate Poliomyelities.
- 4 1 -
Agreement Letter to UNICEF from World Bank on the Purchase o f OPVs that UNICEF w i l l sign with buying countries, December 12, 2002.
Polio Eradication Program IDA Buy-down Mechanism, World Bank, Gates, Rotary/UNF Polio Collaboration, Technical Briefing to World Bank Board by Human Development Network and Resource Mobilization Department, December 17,2002.
Exchange o f letters between World Bank and WHO on WHO'S role in Project evaluation, dated March 2003. *Including electronic files
- 4 2 -

Annex 9: Statement of Loans and Credits PAKISTAN: Partnership for Polio Eradication
06-Feb-2003 Difference between expected
and actual disbursements” Original Amount in US$ Millions
Project ID FY Purpose IBRD IDA GEF Cancel. Undisb. Orig Frm Rev’d 2.95 0.00
PO71454 2003 AJK Community Infrastructure 8 Services 0.00 20.00 0.00 0.00 20.36 -0.17 0.00
P 0 7 4 7 9 7 2003 Banking Sector Technical Assistance 0.00 26.50 0.00 0.00 28.47
P 0 5 5 2 9 2
PO35823 PO56213
PO71092 PO49791
PO37834 PO10500
PO36015 PO10478
2002 BSRPP 0.00
2001 GEF-Protected Areas Management Project 0.00 2001 TRADE a TRANSPORT 0.00 2001 NWFP ON-FARM WATER MANAGEMENT PROJECT 0.00
1999 POVERTY ALLEVIATION FUND 0.00 1998 NORTHERN EDUCATION 0.00 1998 NATIONAL DRAINAGE PR 0.00
1997 IMPR FIN REP a AUDIT 0.00
1996 NWFP COMMUNITY INFRA 0.00
300.00
0.00 3.00
21.35
90.00 22.80
285.00
28.80 21.50
PO39281 1996 GHAZI BAROTHA HYDROP
PO34101 1996 PK-TELECOM REG a PRIVAT
350.00 0.00
35.00 0.00
0.00
10.08 0.00 0.00
0.00 0.00 0.00
0.00 0.00
0.00
0.00 0.00
0.00
0.00 0.09 0.24
0.00 0.00
111.22
10.63 1.49
21.83 40.74 12.17
106.99 18.36 5.18
-204.27 0.00 0.07 0.00 0.29 0.00
-0.79 0.00 -16.17 0.00
12.93 0.00
85.30 0.00 19.76 2.09 8.21 8.21
0.00 0.00 27.70 27.70 19.01 0.00 13.15 4.44 17.59 7.59
Total: 385.00 818.95 10.08 13.48 409.57 -46.59 36.90
- 43 -
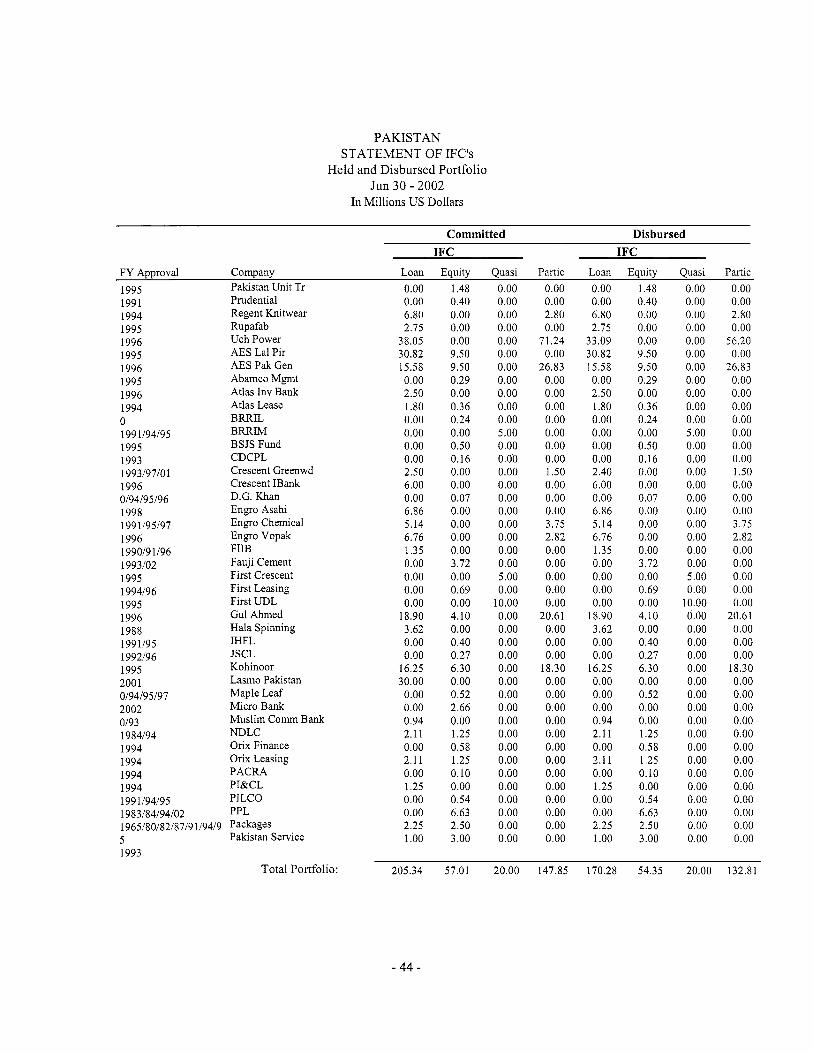
PAKISTAN STATEMENT OF IFC’s
Held and Disbursed Portfolio Jun 30 - 2002
In Millions U S Dollars
Committed Disbursed
1995 1991 1994 1995 1996 1995 1996 1995 1996 1994 0 1991194195 1995 1993 199319710 1 1996 0194195196 1998 199 1195197 1996 1990191196 1993102 1995 1994196 1995 1996 1988 1991195 1992196 1995 200 1 0194195197 2002 0193 1984194 1994 1994 1994 1994 199 1/94/95 1983184194102 1965180182l8719 119419 5 1993
IFC IFC F Y Approval Company Loan Equity Quasi Partic Loan Equity Quasi Partic
Pakistan Unit Tr Prudential Regent Knitwear Rupafab Uch Power AES La1 Pir A E S Pak Gen Abamco Mgmt Atlas Inv Bank Atlas Lease BRRIL BRRIM BSJS Fund CDCPL Crescent Greenwd Crescent IBank D.G. Khan Engro Asahi Engro Chemical Engro Vopak FIIB Fauji Cement First Crescent First Leasing First UDL Gul Ahmed Hala Spinning IHFL JSCL Kohinoor Lasmo Pakistan Maple Leaf Micro Bank Muslim Comm Bank N D L C Orix Finance Orix Leasing PACRA PI&CL PILCO PPL Packages Pakistan Service
Total Portfolio:
0.00 0.00 6.80 2.15
38.05 30.82 15.58 0.00 2.50 1.80 0.00 0.00 0.00 0.00 2.50 6.00 0.00 6.86 5.14 6.76 1.35 0.00 0.00 0.00 0.00
18.90 3.62 0.00 0.00
16.25 30.00 0.00 0.00 0.94 2.11 0.00 2.11 0.00 1.25 0.00 0.00 2.25 1 .oo
1.48 0.40 0.00 0.00 0.00 9.50 9.50 0.29 0.00 0.36 0.24 0.00 0.50 0.16 0.00 0.00 0.07 0.00 0.00 0.00 0.00 3.72 0.00 0.69 0.00 4.10 0.00 0.40 0.27 6.30 0.00 0.52 2.66 0.00 1.25 0.58 1.25 0.10 0.00 0.54 6.63 2.50 3.00
0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 5.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 5.00 0.00
10.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
0.00 0.00 2.80 0.00
7 1.24 0.00
26.83 0.00 0.00 0.00 0.00 0.00 0.00 0.00 1 S O 0.00 0.00 0.00 3.75 2.82 0.00 0.00 0.00 0.00 0.00
20.61 0.00 0.00 0.00
18.30 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
~
0.00 0.00 6.80 2.75
33.09 30.82 15.58 0.00 2.50 1.80 0.00 0.00 0.00 0.00 2.40 6.00 0.00 6.86 5.14 6.76 1.35 0.00 0.00 0.00 0.00
18.90 3.62 0.00 0.00
16.25 0.00 0.00 0.00 0.94 2.1 1 0.00 2.1 1 0.00 1.25 0.00 0.00 2.25 1 .oo
1.48 0.40 0.00 0.00 0.00 9.50 9.50 0.29 0.00 0.36 0.24 0.00 0.50 0.16 0.00 0.00 0.07 0.00 0.00 0.00 0.00 3.72 0.00 0.69 0.00 4.10 0.00 0.40 0.27 6.30 0.00 0.52 0.00 0.00 1.25 0.58 1.25 0.10 0.00 0.54 6.63 2.50 3.00
~
0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 5.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 5.00 0.00
10.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
0.00 0.00 2.80 0.00
56.20 0.00
26.83 0.00 0.00 0.00 0.00 0.00 0.00 0.00 1 S O 0.00 0.00 0.00 3.75 2.82 0.00 0.00 0.00 0.00 0.00
20.61 0.00 0.00 0.00
18.30 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
205.34 57.01 20.00 147.85 170.28 54.35 20.00 132.81
- 44 -

Approvals Pending Commitment
FY Approval Company Loan Equity Quasi Partic 2002 Network Leasing 2.00 0.00 0.00 0.00
Total Pending Commitment: 2.00 0.00 0.00 0.00
- 45 -
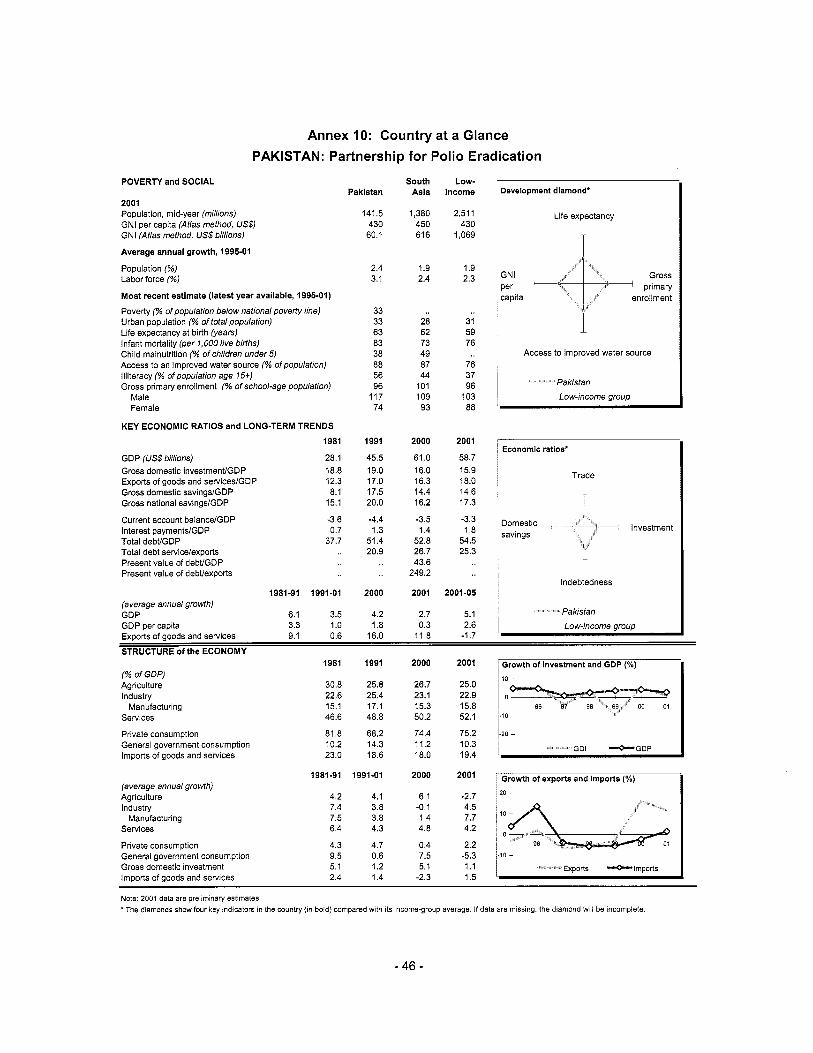
Annex 10: Country at a Glance' PAKISTAN: Partnership for Polio Eradication
POVERTY and SOCIAL Pakistan
2001 Population, mid-year (millions) GNI per capita (Atlas method, US$) GNI (Atlas method, US$ billions)
Average annual growth, 1995-01
Population (%) Labor force (%)
Most recent estimate (latest year available, 1995-01) Poverty (% of population below national poverty line) Urban population (% of total population) Life expectancy at birth (years) Infant mortality (per 1,000 live births) Child malnutrition (% of children under5) Access to an improved water source (% ofpopulationl Illiteracy (% of population age 75+1 Gross primary enrollment (% of school-age population)
Male Female
KEY ECONOMIC RATIOS and LONG-TERM TRENDS
1981
GDP (US$ billions) 28.1
Gross domestic savingslGDP 8.1
Gross domestic investmenffGDP 18.8 Exports of goods and serviceslGDP 12.3
Gross national savingslGDP 15.1
Current account balancelGDP -3.6 Interest paymentslGDP 0.7 Total debUGDP 37.7 Total debt servicelexports Present value of debt/GDP Present value of debtlexports
1981-91 1991-01 (average annual growth) GDP 6.1 3.5 GDP per capita 3.3 1 .o Exnnrts of anads and setvices 9.1 0.6
141.5 430 60.1
2.4 3.1
33 33 63 83 38 88 56 96
117 74
1991
45.5 19.0 17.0 17.5 20.0
-4.4 1.3
51.4 20.9
2000
4.2 1.8
16.0
South Asia
1,380 450 616
1.9 2.4
28 62 73 49 87 44
101 109 93
2000
61 .O 16.0 16.3 14.4 16.2
-3.5 1.4
52.8 26.7 43.6
249.2
2001
2.7 0.3
Low- income
2,511 430
1,069
1.9 2.3
31 59 76
76 37 96
103 88
2001
58.7 15.9 18.0 14.6 17.3
-3.3 1.8
54.5 25.3
2001-05
5.1 2.6
11.8 -1.7
1 Development diamond'
1 Life expectancy ~
, T Gross ' primary
GNi
capita enrollment per
I 1
Access to improved water source
I Pakistan Low-income group
' Economic ratios"
Trade
- I
, i Indebtedness
Pakistan
1 Low-income group Y- - - - - - - - r _ _ _
STRUCTURE of the ECONOMY
(% of GDPJ Agriculture Industry
Services
Private consumption General government consumption Imports of goods and services
Manufacturing
(average annual growth) Agriculture Industry
Services
Private consumption General government consumption Gross domestic investment ImDorts of aoods and services
Manufacturing
1981
30.8 22.6 15.1 46.6
81.8 10.2 23.0
1981-91
4.2 7.4 7.5 6.4
4.3 9.5 5.1 2.4
1991
25.8 25.4 17.1 48.8
68.2 14.3 18.6
I991 -01
4.1 3.8 3.8 4.3
4.7 0.6 1.2 1.4
2000
26.7 23.1 15.3 50.2
74.4 11.2 18.0
2000
6.1 -0.1 1.4 4.8
0.4 7.5 5.1
-2.3
2001
25.0 22.9 15.8 52.1
75.2 10.3 19.4
2001
-2.7 4.5 7.7 4.2
2.2 -5.3 1 .I 1.5
GDI *GDP
Growth of exports and imports ("A)
* O T
10 1
Exports *Imports
Note: 2001 data are preliminary estimates. *The diamonds show four key indicators in the country (in bold) compared with its income-group average. If data are missing, the diamond will be incomplete.
- 46 -
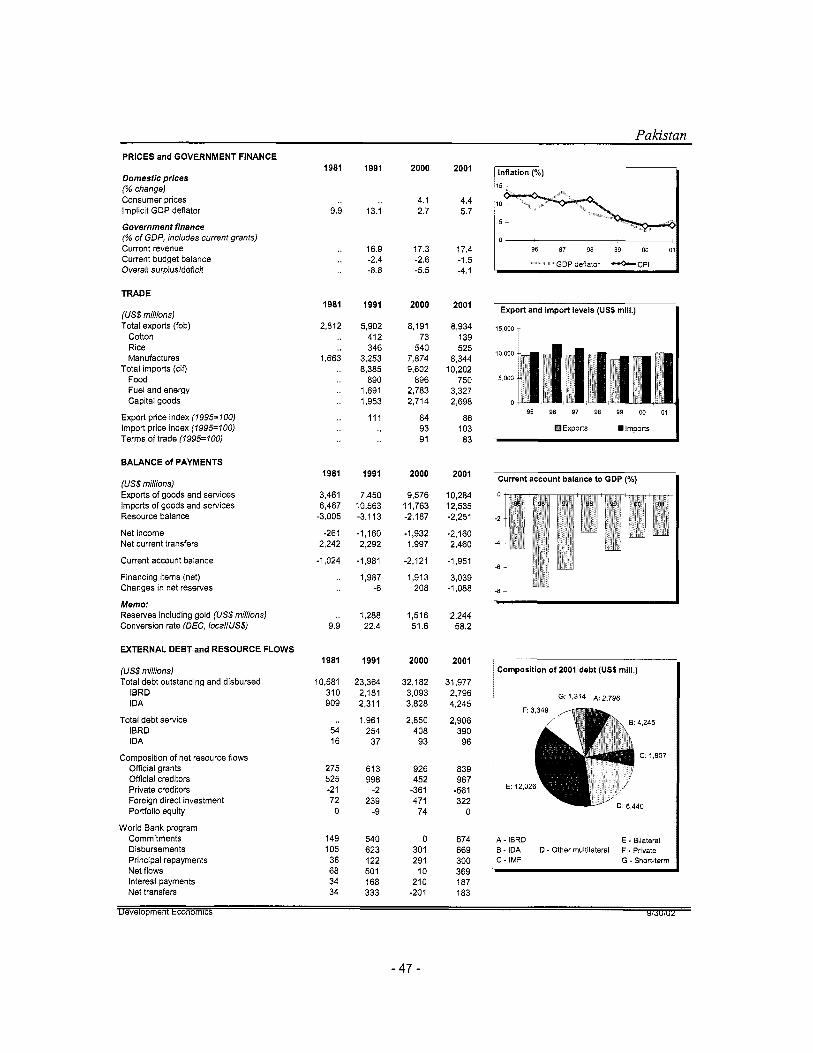
PRICES and GOVERNMENT FINANCE
Domestic prices (% change) Consumer prices Implicit GDP deflator
Government finance (% of GDP, includes current grants) Current revenue Current budget balance Overall surplus/deficit
TRADE
(US$ millions) Total exports (fob)
Cotton Rice Manufactures
Total imports (cif) Food Fuel and energy Capital goods
Export price index (1995=100) Import price index (7995=700) Terms of trade (1995=lOO)
BALANCE of PAYMENTS
(US$ millions) Exports of goods and services Imports of goods and services Resource balance
Net income Net current transfers
Current account balance
Financing items (net) Changes in net reserves
Memo: Reserves including gold (US$ millions) Conversion rate (DEC, /oca//US$)
EXTERNAL DEBT and RESOURCE FLOWS
(US$ millions) Total debt outstanding and disbursed
IBRD IDA
Total debt service IBRD IDA
Composition of net resource flows Official grants Official creditors Private creditors Foreign direct investment Portfolio equity
World Bank program Commitments Disbursements Principal repayments Net flows Interest payments Net transfers
I981
9.9
1981
2,812
1,663
1981
3,461 6,467
-3,005
-261 2,242
-1,024
9.9
1981
10,581 310 909
54 16
275 525 -2 1 72 0
149 105 36 68 34 34
1991
13.1
16.9 -2.4 -8.8
1991
5,902 412 346
3,253 8,385
890 1,691 1,953
111
1991
7,450 10,563 -3,113
-1,160 2,292
-1,981
1.987 -6
1,288 22.4
1991
23,364 2,181 2,311
1,961 254 37
613 998
-2 239
-9
540 623 122 50 1 168 333
2000
4.1 2.7
17.3 -2.6 -5.5
2000
8,191 73
540 7,874 9,602
896 2,783 2,714
84 93 91
2000
9,576 11,763 -2,187
-1,932 1,997
-2,121
1,913 208
1,516 51.6
2000
32,182 3,093 3,828
2,850 408
93
926 452
-361 471
74
0 301 291
10 210
-201
2001
4.4 5.7
17.4 -1.5 -4.1
2001
8,934 139 525
8,344 10,202
750 3,327 2,698
86 103 83
2001
10,284 12,535 -2,251
-2,160 2.460
-1,951
3,039 -1,088
2,244 58.2
2001
31,977 2,796 4,245
2,906 390 96
839 967
-561 322
0
674 669 300 369 187 183
98 97 98 99 on oll O
* GDP deflator *CPl
I Export and import levels (US$ mlll.)
15,000 - 10 000 1 5ooo
0
I I 95 BE 97 98 99 00 01
Exports Imports
Current account balance to GDP (%)
Composition of 2001 debt (US$ mill.)
G: 1,314 ~ : 2 , 7 g 6
4 - IBRD 3 . IDA D. Other multilateral F ~ Private 2 - IMF
E ~ Bilateral
G - Short-term
ul;veluplllal I1 CWIIU1lilC.D YIJUIUL
- 47 -
Additional Annex 11 : IDA Buy-Down Mechanism PAKISTAN: Partnership for Polio Eradication
Introduction
This annex describes the arrangements for the implementation o f the IDA buy-down mechanism for polio eradication projects, which aims to convert the terms o f a normal IDA development credit to grant terms through provision o f additional external donor resources under clearly defined performance criteria. In the context o f the Nigeria polio eradication project, the f i rs t operation utilizing this mechanism, resources for the buy-down will become available as a result o f an agreement between IDA and the Bill & Melinda Gates Foundation (the Gates Foundation)‘. Rotary International has indicated that it will finance the same mechanism for other polio eradication projects. The buy-down mechanism complies with IDA’S existing financial policies.
The Partnership
The World Bank’s Health, Nutrition & Population sector Anchor explored the possibility o f partnering wi th the Gates Foundation to assist polio eradication by providing countries with IDA financial resources but without IDA repayment obligations. The Gates Foundation agreed to provide funds to an IDA-administered trust fund (the Polio Eradication Trust Fund or PETF) that w i l l buy down the debt incurred by recipient countries for successful implementation o f polio eradication projects. In addition to making commitment and service charge payments to IDA on behalf o f the recipients during project implementation, the PETF will, upon successful project implementation, buy down the net present value o f the principal amount o f the development credit.
The Mechanism
IDA i s extending a development credit to Nigeria. The Development Credit Agreement w i l l include two special provisions:
1. The PETF wil l pay the applicable service charges and commitment charges, if any, and 2. The PETF w i l l buy down the principal amount o f the credit upon successful completion o f the
project (as determined by a World Health Organization (WHO) audit).
The buy-down will be funded by contributions to the PETF from the Gates Foundation. The buy-down mechanism operates in three stages-credit signing, project implementation, and project completion. These stages are described below.
At Credit Signing
IDA and PETF determine the discount rate (the prevailing SDR-basket Commercial Interest Reference Rates (CIRR) on the date o f credit signing) and the foreign exchange rate (SDRUSD) that will be used to calculate the estimated net present value at f inal buy-down. The PETF sets aside funds that are denominated in USD and invested pending disbursement. The set-aside amount equals IDA commitment and service charge payments over the projected implementation period and the estimated amount needed to buy down the principal o f the credit at the end o f the implementation period. IDA hedges the foreign exchange risk under i t s existing currency rebalancing mechanism.
- 48 -
During Project Implementation
Under the project, IDA, acting on a request from the recipient country, disburses funds to UNICEF, the agency responsible for procuring the polio vaccine. UNICEF in turn supplies the vaccines to the recipient government.
The PETF pays the commitment and service charges on the disbursed amounts during the implementation o f the project.
If the implementation period i s substantially longer than initially projected, funds required to pay service charges could exceed the funds set aside. However, the investment income on the set-aside buy-down amount would provide a cushion against this risk. If the implementation period exceeds five years, the responsibility for servicing the credit w i l l revert to the recipient country unless the Gates Foundation grants an extension.
At Project Completion
Upon completion o f the project, WHO conducts a performance audit to determine if the IDA funds achieved their intended results. The performance audit measures the results for two indicators:
1. Timely arrival o f oral polio vaccine (OPV) in the country at central level, and 2. Vaccination coverage for OPV during the vaccination campaigns.
If the W H O performance audit evaluates the project as satisfactory, the IDA buy-down will be triggered. The PETF w i l l then pay o f f the IDA credit at the net present value o f the credit based on the defined foreign exchange and discount rates to buy down the principal o f this credit (Repayment Amount). IDA will in turn cancel this credit and release the recipient from any future liability. If the credit i s not fully disbursed, the final Repayment Amount wi l l be calculated on a pro-rata basis. If the WHO performance audit evaluates the project as unsatisfactory, the recipient wi l l remain obligated to pay back IDA on the terms o f the credit.
- 4 9 -
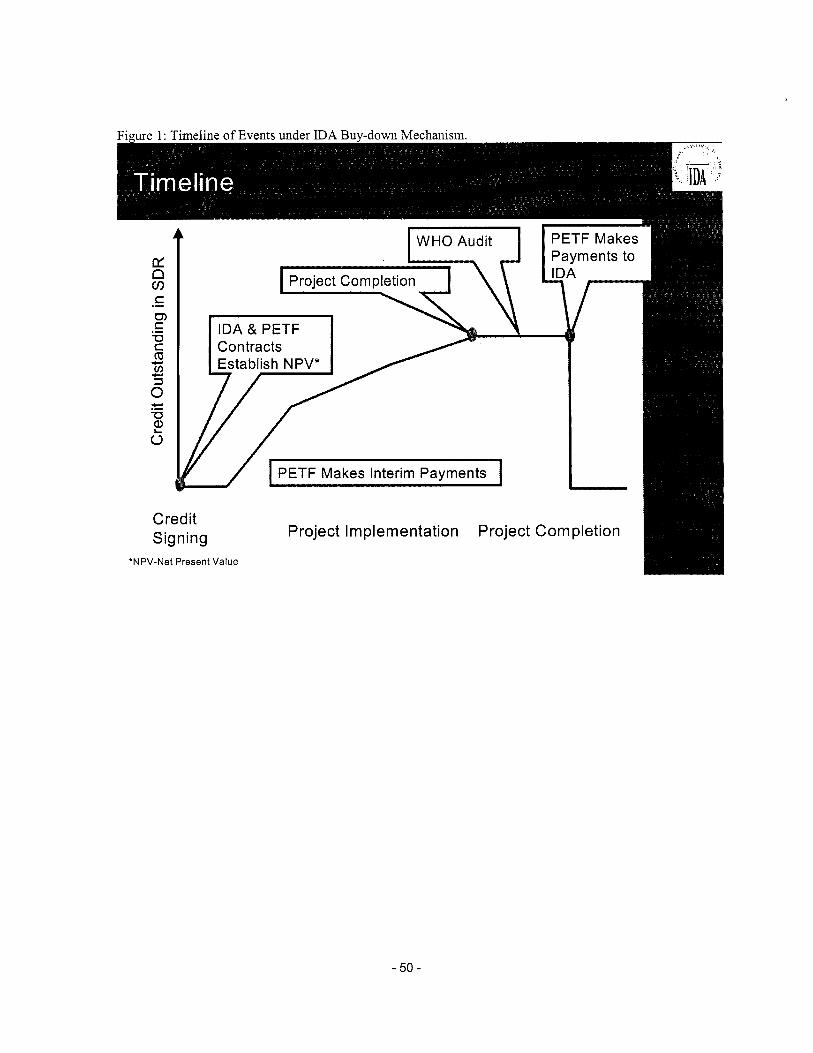
. -
I
Credit Signing
'NPV-Net Present Value
Project Implementation Project Completion
- 50 -
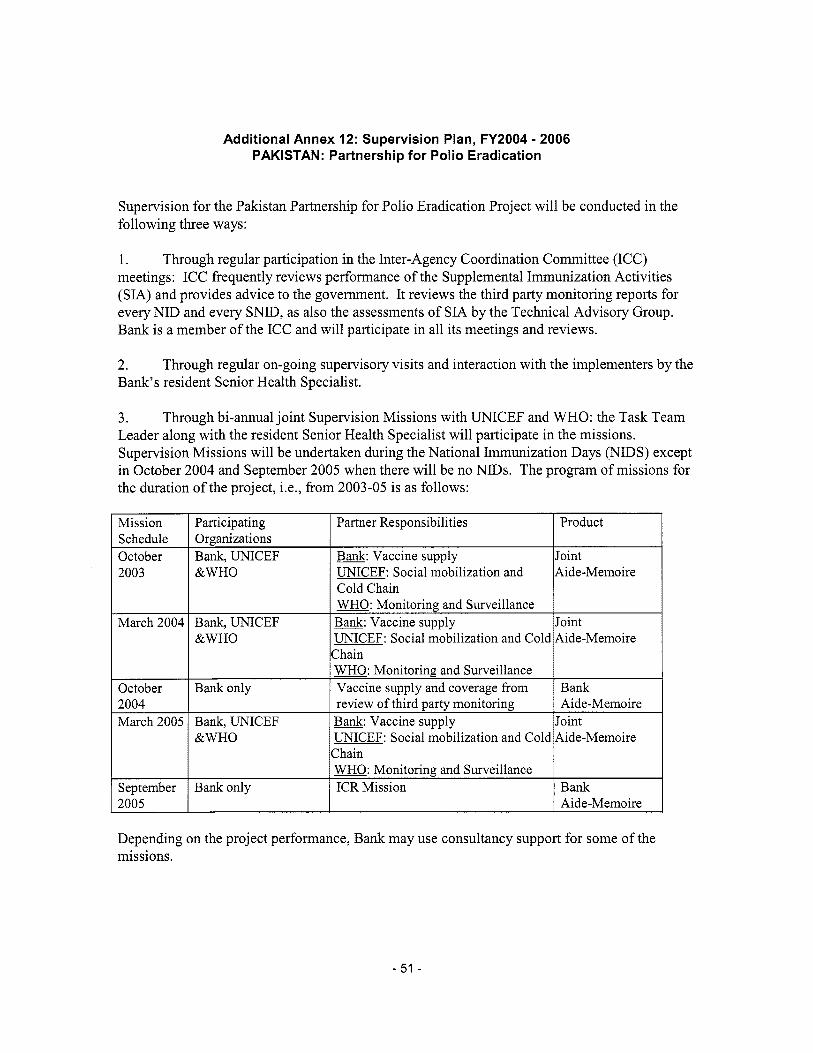
Additional Annex 12: Supervision Plan, FY2004 - 2006 PAKISTAN: Partnership for Polio Eradication
Mission Participating Schedule Organizations October Bank, UNICEF 2003 &WHO
March 2004 Bank, UNICEF &WHO
October Bank only
Supervision for the Pakistan Partnership for Polio Eradication Project will be conducted in the fol lowing three ways:
Partner Responsibilities Product
w: Vaccine supply Joint UNICEF: Social mobilization and Aide-Memoire Cold Chain WHO: Monitoring and Surveillance m: Vaccine supply Joint UNICEF: Social mobilization and Cold Aide-Memoire Chain WHO: Monitoring and Surveillance Vaccine supply and coverage from Bank
1. meetings: ICC frequently reviews performance o f the Supplemental Immunization Activities (SIA) and provides advice to the government. It reviews the third party monitoring reports for every NID and every SNID, as also the assessments o f S I A by the Technical Advisory Group. Bank i s a member o f the ICC and will participate in a l l i t s meetings and reviews.
Through regular participation in the Inter-Agency Coordination Committee (ICC)
2004 March 2005
2. Bank’s resident Senior Health Specialist.
Through regular on-going supervisory visits and interaction with the implementers by the
review o f third party monitoring Aide-Memoire Bank, UNICEF w: Vaccine supply Joint
3. Leader along with the resident Senior Health Specialist wil l participate in the missions. Supervision Missions will be undertaken during the National Immunization Days (NIDS) except in October 2004 and September 2005 when there will be no NIDs. The program o f missions for the duration o f the project, Le., fi-om 2003-05 i s as follows:
Through bi-annual jo in t Supervision Missions with UNICEF and WHO: the Task Team
September 2005
&WHO UNICEF: Social mobilization and Cold Aide-Memoire Chain WHO: Monitoring and Surveillance
Bank only ICR Mission Bank Aide-Memoire
Depending on the project performance, Bank may use consultancy support for some o f the missions.
- 51 -
































