Embed Size (px)
Citation preview

Prof Soumaya E Hadhoud
Dr M Kashif Ishaqi
Department of Pediatrics
TAIBAH UNIVERSITY
To demonstrate knowledge of the process and stages of Haematopoiesis
To demonstrate basic knowledge of the structure and function of Haematopoietic cells
To be able to interpret Normal blood counts
To demonstrate basic knowledge of pathophysiology clinical features and treatment outline of common diseases affecting blood cells
To be able to identify the Normal and abnormal blood cells
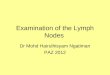
Plasma-liquid
55
Blood Cells-Formed elements
45
Three types
1-ErythrocytesRBCs
2-LeukocytesWBCsGranulocytes
Neutrophils
Eosinophils
Basophils
Agranulocytes
Lymphocytes
Monocytes
3-ThrombocytesPlatelets 3
What is Hematopoiesis
Hematopoiesis is a term describing the formation and development of blood cells
Cells of the blood are constantly being lost or destroyed Thus to maintain homeostasis the system must have the capacity for self renewal This system involves
Proliferation of progeny stem cells
Differentiation and maturation of the stem cells into the functional cellular elements
In the adult all blood cell formation (red blood cells white blood cells and platelets) occurs in the Red Bone Marrow or myeloid tissue
Hemocytoblasts (hematopoietic stem cells)
All blood cells arise from hematopoietic stemcell (HSC)
Hormones and growth factors push the cell toward a specific pathway of blood cell development
Hematopoiesis begins as early as the nineteenth day after fertilization in the yolk sac of the embryo
Only erythrocytes are made
The RBCs contain unique fetal hemoglobins
At about 6 weeks of gestation yolk sac production of erythrocytes decreases and production of RBCs in the human embryo itself begins
At two months the fetal liver becomes the chief site of blood cell production
Erythrocytes are produced
The beginnings of leukocyte and thrombocyte production occurs
The spleen kidney thymus and lymph nodes serve as minor sites of blood cell production
The lymph nodes will continue as an important site of lymphopoiesis (production of lymphocytes) throughout life but blood production in the other areas decreases and finally ceases as the bone marrow becomes the primary site of hematopoiesis at about 6 months of gestation and continues throughout life
When the bone marrow becomes the chief site of hematopoiesis leukocyte and thrombocyte production become more prominent
At birth liver and spleen stop hematopoietic activity
Bone marrow now becomes active site of hematopoiesis
Children up to teen years has hematopoiesis in all bones
Hematopoiesis gradually decreases in shafts of long bones
bull In adults red bone marrow is primarily found in bones of the
ndash Axial skeleton
ndash Pelvic and pectoral girdles
ndash Proximal epiphyses of the humerus and femur
Medullary
Hematopoiesis in the bone marrow is called medullary hematopoiesis
Extra medullary
Blood cell production in hematopoietic tissue other than bone marrow
Liver
Spleen
Compensatory mechanism to provide blood cells in times of need
This can lead to hepatomegaly andor splenomegaly (increase in size of the liver andor spleen because of increased functions in the organs)
bull Red blood cells ndashbull carry oxygen via hemoglobin
bull LeukocytesWhite Blood Cellsmake up the cells of the immune system
ndashbull These cells help clear parasites bacteria tumors debris-----
ThrombocytesPlateletsndashbullMust be present for clotting to occur
ndashbull Involved in hemostasis
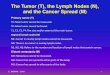
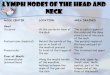
Red Blood Cell (RBC) synthesis is known as Erythropoiesis
bull In erythropoiesis the hemocytoblast goes through a series of morphological changes culminating in the formation of a cell full of hemoglobin
Sizehellip Same size as the nucleus of a small lymphocyte that is 72 um
Cell shape round
Cytoplasm Pink
Center pallor Hemoglobin is comparatively less in the center showing central pallor on dried film13 size of the cell
Normal RBC suspended in fluid is biconcave
Transport oxygen from lungs to tissues and carbon dioxide from tissues to lungs
72
mm
The appearance of normal circulating blood is relatively uniform with little variation in size and shape Red blood cells will have an area of paleness in the center which is approximately one-third the diameter of the cell
Composed of hemoglobin
Erythropoiesis= RBC production
Stimulated by hypoxia
Controlled by erythropoietin
Hormone synthesized in kidney
Hemolysis= destruction of RBCs
Releases bilirubin into blood stream
Normal lifespan of RBC = 120 days
O
2
O
2
O
2
O
2
oxyhaemoglobin
19-18
Protect body against microorganisms and remove dead cells and debris
MovementsAmeboid
Diapedesis
Chemotaxis
Passive Immunity
Active Immunity
Antigen ndash Antibody
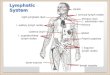
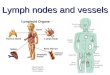
TypesNeutrophils Most common phagocytic cells destroy bacteria (60)
Eosinophils Detoxify chemicals reduce inflammation (4)
Basophils Allergic reactions Release histamine heparin increase inflam response (1)
Lymphocytes Immunity 2 types b amp t Cell types IgG-infection IgM-microbes IgA-Resp amp GI IgE- Allergy IgD-immune response
Monocytes Become macrophages
Basophil Eosinophil
Neutrophil
Lymphocyte
Monocyte
platelet
Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
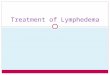
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

To demonstrate knowledge of the process and stages of Haematopoiesis
To demonstrate basic knowledge of the structure and function of Haematopoietic cells
To be able to interpret Normal blood counts
To demonstrate basic knowledge of pathophysiology clinical features and treatment outline of common diseases affecting blood cells
To be able to identify the Normal and abnormal blood cells
Plasma-liquid
55
Blood Cells-Formed elements
45
Three types
1-ErythrocytesRBCs
2-LeukocytesWBCsGranulocytes
Neutrophils
Eosinophils
Basophils
Agranulocytes
Lymphocytes
Monocytes
3-ThrombocytesPlatelets 3
What is Hematopoiesis
Hematopoiesis is a term describing the formation and development of blood cells
Cells of the blood are constantly being lost or destroyed Thus to maintain homeostasis the system must have the capacity for self renewal This system involves
Proliferation of progeny stem cells
Differentiation and maturation of the stem cells into the functional cellular elements
In the adult all blood cell formation (red blood cells white blood cells and platelets) occurs in the Red Bone Marrow or myeloid tissue
Hemocytoblasts (hematopoietic stem cells)
All blood cells arise from hematopoietic stemcell (HSC)
Hormones and growth factors push the cell toward a specific pathway of blood cell development
Hematopoiesis begins as early as the nineteenth day after fertilization in the yolk sac of the embryo
Only erythrocytes are made
The RBCs contain unique fetal hemoglobins
At about 6 weeks of gestation yolk sac production of erythrocytes decreases and production of RBCs in the human embryo itself begins
At two months the fetal liver becomes the chief site of blood cell production
Erythrocytes are produced
The beginnings of leukocyte and thrombocyte production occurs
The spleen kidney thymus and lymph nodes serve as minor sites of blood cell production
The lymph nodes will continue as an important site of lymphopoiesis (production of lymphocytes) throughout life but blood production in the other areas decreases and finally ceases as the bone marrow becomes the primary site of hematopoiesis at about 6 months of gestation and continues throughout life
When the bone marrow becomes the chief site of hematopoiesis leukocyte and thrombocyte production become more prominent
At birth liver and spleen stop hematopoietic activity
Bone marrow now becomes active site of hematopoiesis
Children up to teen years has hematopoiesis in all bones
Hematopoiesis gradually decreases in shafts of long bones
bull In adults red bone marrow is primarily found in bones of the
ndash Axial skeleton
ndash Pelvic and pectoral girdles
ndash Proximal epiphyses of the humerus and femur
Medullary
Hematopoiesis in the bone marrow is called medullary hematopoiesis
Extra medullary
Blood cell production in hematopoietic tissue other than bone marrow
Liver
Spleen
Compensatory mechanism to provide blood cells in times of need
This can lead to hepatomegaly andor splenomegaly (increase in size of the liver andor spleen because of increased functions in the organs)
bull Red blood cells ndashbull carry oxygen via hemoglobin
bull LeukocytesWhite Blood Cellsmake up the cells of the immune system
ndashbull These cells help clear parasites bacteria tumors debris-----
ThrombocytesPlateletsndashbullMust be present for clotting to occur
ndashbull Involved in hemostasis
Red Blood Cell (RBC) synthesis is known as Erythropoiesis
bull In erythropoiesis the hemocytoblast goes through a series of morphological changes culminating in the formation of a cell full of hemoglobin
Sizehellip Same size as the nucleus of a small lymphocyte that is 72 um
Cell shape round
Cytoplasm Pink
Center pallor Hemoglobin is comparatively less in the center showing central pallor on dried film13 size of the cell
Normal RBC suspended in fluid is biconcave
Transport oxygen from lungs to tissues and carbon dioxide from tissues to lungs
72
mm
The appearance of normal circulating blood is relatively uniform with little variation in size and shape Red blood cells will have an area of paleness in the center which is approximately one-third the diameter of the cell
Composed of hemoglobin
Erythropoiesis= RBC production
Stimulated by hypoxia
Controlled by erythropoietin
Hormone synthesized in kidney
Hemolysis= destruction of RBCs
Releases bilirubin into blood stream
Normal lifespan of RBC = 120 days
O
2
O
2
O
2
O
2
oxyhaemoglobin
19-18
Protect body against microorganisms and remove dead cells and debris
MovementsAmeboid
Diapedesis
Chemotaxis
Passive Immunity
Active Immunity
Antigen ndash Antibody
TypesNeutrophils Most common phagocytic cells destroy bacteria (60)
Eosinophils Detoxify chemicals reduce inflammation (4)
Basophils Allergic reactions Release histamine heparin increase inflam response (1)
Lymphocytes Immunity 2 types b amp t Cell types IgG-infection IgM-microbes IgA-Resp amp GI IgE- Allergy IgD-immune response
Monocytes Become macrophages
Basophil Eosinophil
Neutrophil
Lymphocyte
Monocyte
platelet
Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Plasma-liquid
55
Blood Cells-Formed elements
45
Three types
1-ErythrocytesRBCs
2-LeukocytesWBCsGranulocytes
Neutrophils
Eosinophils
Basophils
Agranulocytes
Lymphocytes
Monocytes
3-ThrombocytesPlatelets 3
What is Hematopoiesis
Hematopoiesis is a term describing the formation and development of blood cells
Cells of the blood are constantly being lost or destroyed Thus to maintain homeostasis the system must have the capacity for self renewal This system involves
Proliferation of progeny stem cells
Differentiation and maturation of the stem cells into the functional cellular elements
In the adult all blood cell formation (red blood cells white blood cells and platelets) occurs in the Red Bone Marrow or myeloid tissue
Hemocytoblasts (hematopoietic stem cells)
All blood cells arise from hematopoietic stemcell (HSC)
Hormones and growth factors push the cell toward a specific pathway of blood cell development
Hematopoiesis begins as early as the nineteenth day after fertilization in the yolk sac of the embryo
Only erythrocytes are made
The RBCs contain unique fetal hemoglobins
At about 6 weeks of gestation yolk sac production of erythrocytes decreases and production of RBCs in the human embryo itself begins
At two months the fetal liver becomes the chief site of blood cell production
Erythrocytes are produced
The beginnings of leukocyte and thrombocyte production occurs
The spleen kidney thymus and lymph nodes serve as minor sites of blood cell production
The lymph nodes will continue as an important site of lymphopoiesis (production of lymphocytes) throughout life but blood production in the other areas decreases and finally ceases as the bone marrow becomes the primary site of hematopoiesis at about 6 months of gestation and continues throughout life
When the bone marrow becomes the chief site of hematopoiesis leukocyte and thrombocyte production become more prominent
At birth liver and spleen stop hematopoietic activity
Bone marrow now becomes active site of hematopoiesis
Children up to teen years has hematopoiesis in all bones
Hematopoiesis gradually decreases in shafts of long bones
bull In adults red bone marrow is primarily found in bones of the
ndash Axial skeleton
ndash Pelvic and pectoral girdles
ndash Proximal epiphyses of the humerus and femur
Medullary
Hematopoiesis in the bone marrow is called medullary hematopoiesis
Extra medullary
Blood cell production in hematopoietic tissue other than bone marrow
Liver
Spleen
Compensatory mechanism to provide blood cells in times of need
This can lead to hepatomegaly andor splenomegaly (increase in size of the liver andor spleen because of increased functions in the organs)
bull Red blood cells ndashbull carry oxygen via hemoglobin
bull LeukocytesWhite Blood Cellsmake up the cells of the immune system
ndashbull These cells help clear parasites bacteria tumors debris-----
ThrombocytesPlateletsndashbullMust be present for clotting to occur
ndashbull Involved in hemostasis
Red Blood Cell (RBC) synthesis is known as Erythropoiesis
bull In erythropoiesis the hemocytoblast goes through a series of morphological changes culminating in the formation of a cell full of hemoglobin
Sizehellip Same size as the nucleus of a small lymphocyte that is 72 um
Cell shape round
Cytoplasm Pink
Center pallor Hemoglobin is comparatively less in the center showing central pallor on dried film13 size of the cell
Normal RBC suspended in fluid is biconcave
Transport oxygen from lungs to tissues and carbon dioxide from tissues to lungs
72
mm
The appearance of normal circulating blood is relatively uniform with little variation in size and shape Red blood cells will have an area of paleness in the center which is approximately one-third the diameter of the cell
Composed of hemoglobin
Erythropoiesis= RBC production
Stimulated by hypoxia
Controlled by erythropoietin
Hormone synthesized in kidney
Hemolysis= destruction of RBCs
Releases bilirubin into blood stream
Normal lifespan of RBC = 120 days
O
2
O
2
O
2
O
2
oxyhaemoglobin
19-18
Protect body against microorganisms and remove dead cells and debris
MovementsAmeboid
Diapedesis
Chemotaxis
Passive Immunity
Active Immunity
Antigen ndash Antibody
TypesNeutrophils Most common phagocytic cells destroy bacteria (60)
Eosinophils Detoxify chemicals reduce inflammation (4)
Basophils Allergic reactions Release histamine heparin increase inflam response (1)
Lymphocytes Immunity 2 types b amp t Cell types IgG-infection IgM-microbes IgA-Resp amp GI IgE- Allergy IgD-immune response
Monocytes Become macrophages
Basophil Eosinophil
Neutrophil
Lymphocyte
Monocyte
platelet
Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

What is Hematopoiesis
Hematopoiesis is a term describing the formation and development of blood cells
Cells of the blood are constantly being lost or destroyed Thus to maintain homeostasis the system must have the capacity for self renewal This system involves
Proliferation of progeny stem cells
Differentiation and maturation of the stem cells into the functional cellular elements
In the adult all blood cell formation (red blood cells white blood cells and platelets) occurs in the Red Bone Marrow or myeloid tissue
Hemocytoblasts (hematopoietic stem cells)
All blood cells arise from hematopoietic stemcell (HSC)
Hormones and growth factors push the cell toward a specific pathway of blood cell development
Hematopoiesis begins as early as the nineteenth day after fertilization in the yolk sac of the embryo
Only erythrocytes are made
The RBCs contain unique fetal hemoglobins
At about 6 weeks of gestation yolk sac production of erythrocytes decreases and production of RBCs in the human embryo itself begins
At two months the fetal liver becomes the chief site of blood cell production
Erythrocytes are produced
The beginnings of leukocyte and thrombocyte production occurs
The spleen kidney thymus and lymph nodes serve as minor sites of blood cell production
The lymph nodes will continue as an important site of lymphopoiesis (production of lymphocytes) throughout life but blood production in the other areas decreases and finally ceases as the bone marrow becomes the primary site of hematopoiesis at about 6 months of gestation and continues throughout life
When the bone marrow becomes the chief site of hematopoiesis leukocyte and thrombocyte production become more prominent
At birth liver and spleen stop hematopoietic activity
Bone marrow now becomes active site of hematopoiesis
Children up to teen years has hematopoiesis in all bones
Hematopoiesis gradually decreases in shafts of long bones
bull In adults red bone marrow is primarily found in bones of the
ndash Axial skeleton
ndash Pelvic and pectoral girdles
ndash Proximal epiphyses of the humerus and femur
Medullary
Hematopoiesis in the bone marrow is called medullary hematopoiesis
Extra medullary
Blood cell production in hematopoietic tissue other than bone marrow
Liver
Spleen
Compensatory mechanism to provide blood cells in times of need
This can lead to hepatomegaly andor splenomegaly (increase in size of the liver andor spleen because of increased functions in the organs)
bull Red blood cells ndashbull carry oxygen via hemoglobin
bull LeukocytesWhite Blood Cellsmake up the cells of the immune system
ndashbull These cells help clear parasites bacteria tumors debris-----
ThrombocytesPlateletsndashbullMust be present for clotting to occur
ndashbull Involved in hemostasis
Red Blood Cell (RBC) synthesis is known as Erythropoiesis
bull In erythropoiesis the hemocytoblast goes through a series of morphological changes culminating in the formation of a cell full of hemoglobin
Sizehellip Same size as the nucleus of a small lymphocyte that is 72 um
Cell shape round
Cytoplasm Pink
Center pallor Hemoglobin is comparatively less in the center showing central pallor on dried film13 size of the cell
Normal RBC suspended in fluid is biconcave
Transport oxygen from lungs to tissues and carbon dioxide from tissues to lungs
72
mm
The appearance of normal circulating blood is relatively uniform with little variation in size and shape Red blood cells will have an area of paleness in the center which is approximately one-third the diameter of the cell
Composed of hemoglobin
Erythropoiesis= RBC production
Stimulated by hypoxia
Controlled by erythropoietin
Hormone synthesized in kidney
Hemolysis= destruction of RBCs
Releases bilirubin into blood stream
Normal lifespan of RBC = 120 days
O
2
O
2
O
2
O
2
oxyhaemoglobin
19-18
Protect body against microorganisms and remove dead cells and debris
MovementsAmeboid
Diapedesis
Chemotaxis
Passive Immunity
Active Immunity
Antigen ndash Antibody
TypesNeutrophils Most common phagocytic cells destroy bacteria (60)
Eosinophils Detoxify chemicals reduce inflammation (4)
Basophils Allergic reactions Release histamine heparin increase inflam response (1)
Lymphocytes Immunity 2 types b amp t Cell types IgG-infection IgM-microbes IgA-Resp amp GI IgE- Allergy IgD-immune response
Monocytes Become macrophages
Basophil Eosinophil
Neutrophil
Lymphocyte
Monocyte
platelet
Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Hemocytoblasts (hematopoietic stem cells)
All blood cells arise from hematopoietic stemcell (HSC)
Hormones and growth factors push the cell toward a specific pathway of blood cell development
Hematopoiesis begins as early as the nineteenth day after fertilization in the yolk sac of the embryo
Only erythrocytes are made
The RBCs contain unique fetal hemoglobins
At about 6 weeks of gestation yolk sac production of erythrocytes decreases and production of RBCs in the human embryo itself begins
At two months the fetal liver becomes the chief site of blood cell production
Erythrocytes are produced
The beginnings of leukocyte and thrombocyte production occurs
The spleen kidney thymus and lymph nodes serve as minor sites of blood cell production
The lymph nodes will continue as an important site of lymphopoiesis (production of lymphocytes) throughout life but blood production in the other areas decreases and finally ceases as the bone marrow becomes the primary site of hematopoiesis at about 6 months of gestation and continues throughout life
When the bone marrow becomes the chief site of hematopoiesis leukocyte and thrombocyte production become more prominent
At birth liver and spleen stop hematopoietic activity
Bone marrow now becomes active site of hematopoiesis
Children up to teen years has hematopoiesis in all bones
Hematopoiesis gradually decreases in shafts of long bones
bull In adults red bone marrow is primarily found in bones of the
ndash Axial skeleton
ndash Pelvic and pectoral girdles
ndash Proximal epiphyses of the humerus and femur
Medullary
Hematopoiesis in the bone marrow is called medullary hematopoiesis
Extra medullary
Blood cell production in hematopoietic tissue other than bone marrow
Liver
Spleen
Compensatory mechanism to provide blood cells in times of need
This can lead to hepatomegaly andor splenomegaly (increase in size of the liver andor spleen because of increased functions in the organs)
bull Red blood cells ndashbull carry oxygen via hemoglobin
bull LeukocytesWhite Blood Cellsmake up the cells of the immune system
ndashbull These cells help clear parasites bacteria tumors debris-----
ThrombocytesPlateletsndashbullMust be present for clotting to occur
ndashbull Involved in hemostasis
Red Blood Cell (RBC) synthesis is known as Erythropoiesis
bull In erythropoiesis the hemocytoblast goes through a series of morphological changes culminating in the formation of a cell full of hemoglobin
Sizehellip Same size as the nucleus of a small lymphocyte that is 72 um
Cell shape round
Cytoplasm Pink
Center pallor Hemoglobin is comparatively less in the center showing central pallor on dried film13 size of the cell
Normal RBC suspended in fluid is biconcave
Transport oxygen from lungs to tissues and carbon dioxide from tissues to lungs
72
mm
The appearance of normal circulating blood is relatively uniform with little variation in size and shape Red blood cells will have an area of paleness in the center which is approximately one-third the diameter of the cell
Composed of hemoglobin
Erythropoiesis= RBC production
Stimulated by hypoxia
Controlled by erythropoietin
Hormone synthesized in kidney
Hemolysis= destruction of RBCs
Releases bilirubin into blood stream
Normal lifespan of RBC = 120 days
O
2
O
2
O
2
O
2
oxyhaemoglobin
19-18
Protect body against microorganisms and remove dead cells and debris
MovementsAmeboid
Diapedesis
Chemotaxis
Passive Immunity
Active Immunity
Antigen ndash Antibody
TypesNeutrophils Most common phagocytic cells destroy bacteria (60)
Eosinophils Detoxify chemicals reduce inflammation (4)
Basophils Allergic reactions Release histamine heparin increase inflam response (1)
Lymphocytes Immunity 2 types b amp t Cell types IgG-infection IgM-microbes IgA-Resp amp GI IgE- Allergy IgD-immune response
Monocytes Become macrophages
Basophil Eosinophil
Neutrophil
Lymphocyte
Monocyte
platelet
Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Hematopoiesis begins as early as the nineteenth day after fertilization in the yolk sac of the embryo
Only erythrocytes are made
The RBCs contain unique fetal hemoglobins
At about 6 weeks of gestation yolk sac production of erythrocytes decreases and production of RBCs in the human embryo itself begins
At two months the fetal liver becomes the chief site of blood cell production
Erythrocytes are produced
The beginnings of leukocyte and thrombocyte production occurs
The spleen kidney thymus and lymph nodes serve as minor sites of blood cell production
The lymph nodes will continue as an important site of lymphopoiesis (production of lymphocytes) throughout life but blood production in the other areas decreases and finally ceases as the bone marrow becomes the primary site of hematopoiesis at about 6 months of gestation and continues throughout life
When the bone marrow becomes the chief site of hematopoiesis leukocyte and thrombocyte production become more prominent
At birth liver and spleen stop hematopoietic activity
Bone marrow now becomes active site of hematopoiesis
Children up to teen years has hematopoiesis in all bones
Hematopoiesis gradually decreases in shafts of long bones
bull In adults red bone marrow is primarily found in bones of the
ndash Axial skeleton
ndash Pelvic and pectoral girdles
ndash Proximal epiphyses of the humerus and femur
Medullary
Hematopoiesis in the bone marrow is called medullary hematopoiesis
Extra medullary
Blood cell production in hematopoietic tissue other than bone marrow
Liver
Spleen
Compensatory mechanism to provide blood cells in times of need
This can lead to hepatomegaly andor splenomegaly (increase in size of the liver andor spleen because of increased functions in the organs)
bull Red blood cells ndashbull carry oxygen via hemoglobin
bull LeukocytesWhite Blood Cellsmake up the cells of the immune system
ndashbull These cells help clear parasites bacteria tumors debris-----
ThrombocytesPlateletsndashbullMust be present for clotting to occur
ndashbull Involved in hemostasis
Red Blood Cell (RBC) synthesis is known as Erythropoiesis
bull In erythropoiesis the hemocytoblast goes through a series of morphological changes culminating in the formation of a cell full of hemoglobin
Sizehellip Same size as the nucleus of a small lymphocyte that is 72 um
Cell shape round
Cytoplasm Pink
Center pallor Hemoglobin is comparatively less in the center showing central pallor on dried film13 size of the cell
Normal RBC suspended in fluid is biconcave
Transport oxygen from lungs to tissues and carbon dioxide from tissues to lungs
72
mm
The appearance of normal circulating blood is relatively uniform with little variation in size and shape Red blood cells will have an area of paleness in the center which is approximately one-third the diameter of the cell
Composed of hemoglobin
Erythropoiesis= RBC production
Stimulated by hypoxia
Controlled by erythropoietin
Hormone synthesized in kidney
Hemolysis= destruction of RBCs
Releases bilirubin into blood stream
Normal lifespan of RBC = 120 days
O
2
O
2
O
2
O
2
oxyhaemoglobin
19-18
Protect body against microorganisms and remove dead cells and debris
MovementsAmeboid
Diapedesis
Chemotaxis
Passive Immunity
Active Immunity
Antigen ndash Antibody
TypesNeutrophils Most common phagocytic cells destroy bacteria (60)
Eosinophils Detoxify chemicals reduce inflammation (4)
Basophils Allergic reactions Release histamine heparin increase inflam response (1)
Lymphocytes Immunity 2 types b amp t Cell types IgG-infection IgM-microbes IgA-Resp amp GI IgE- Allergy IgD-immune response
Monocytes Become macrophages
Basophil Eosinophil
Neutrophil
Lymphocyte
Monocyte
platelet
Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

At two months the fetal liver becomes the chief site of blood cell production
Erythrocytes are produced
The beginnings of leukocyte and thrombocyte production occurs
The spleen kidney thymus and lymph nodes serve as minor sites of blood cell production
The lymph nodes will continue as an important site of lymphopoiesis (production of lymphocytes) throughout life but blood production in the other areas decreases and finally ceases as the bone marrow becomes the primary site of hematopoiesis at about 6 months of gestation and continues throughout life
When the bone marrow becomes the chief site of hematopoiesis leukocyte and thrombocyte production become more prominent
At birth liver and spleen stop hematopoietic activity
Bone marrow now becomes active site of hematopoiesis
Children up to teen years has hematopoiesis in all bones
Hematopoiesis gradually decreases in shafts of long bones
bull In adults red bone marrow is primarily found in bones of the
ndash Axial skeleton
ndash Pelvic and pectoral girdles
ndash Proximal epiphyses of the humerus and femur
Medullary
Hematopoiesis in the bone marrow is called medullary hematopoiesis
Extra medullary
Blood cell production in hematopoietic tissue other than bone marrow
Liver
Spleen
Compensatory mechanism to provide blood cells in times of need
This can lead to hepatomegaly andor splenomegaly (increase in size of the liver andor spleen because of increased functions in the organs)
bull Red blood cells ndashbull carry oxygen via hemoglobin
bull LeukocytesWhite Blood Cellsmake up the cells of the immune system
ndashbull These cells help clear parasites bacteria tumors debris-----
ThrombocytesPlateletsndashbullMust be present for clotting to occur
ndashbull Involved in hemostasis
Red Blood Cell (RBC) synthesis is known as Erythropoiesis
bull In erythropoiesis the hemocytoblast goes through a series of morphological changes culminating in the formation of a cell full of hemoglobin
Sizehellip Same size as the nucleus of a small lymphocyte that is 72 um
Cell shape round
Cytoplasm Pink
Center pallor Hemoglobin is comparatively less in the center showing central pallor on dried film13 size of the cell
Normal RBC suspended in fluid is biconcave
Transport oxygen from lungs to tissues and carbon dioxide from tissues to lungs
72
mm
The appearance of normal circulating blood is relatively uniform with little variation in size and shape Red blood cells will have an area of paleness in the center which is approximately one-third the diameter of the cell
Composed of hemoglobin
Erythropoiesis= RBC production
Stimulated by hypoxia
Controlled by erythropoietin
Hormone synthesized in kidney
Hemolysis= destruction of RBCs
Releases bilirubin into blood stream
Normal lifespan of RBC = 120 days
O
2
O
2
O
2
O
2
oxyhaemoglobin
19-18
Protect body against microorganisms and remove dead cells and debris
MovementsAmeboid
Diapedesis
Chemotaxis
Passive Immunity
Active Immunity
Antigen ndash Antibody
TypesNeutrophils Most common phagocytic cells destroy bacteria (60)
Eosinophils Detoxify chemicals reduce inflammation (4)
Basophils Allergic reactions Release histamine heparin increase inflam response (1)
Lymphocytes Immunity 2 types b amp t Cell types IgG-infection IgM-microbes IgA-Resp amp GI IgE- Allergy IgD-immune response
Monocytes Become macrophages
Basophil Eosinophil
Neutrophil
Lymphocyte
Monocyte
platelet
Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

At birth liver and spleen stop hematopoietic activity
Bone marrow now becomes active site of hematopoiesis
Children up to teen years has hematopoiesis in all bones
Hematopoiesis gradually decreases in shafts of long bones
bull In adults red bone marrow is primarily found in bones of the
ndash Axial skeleton
ndash Pelvic and pectoral girdles
ndash Proximal epiphyses of the humerus and femur
Medullary
Hematopoiesis in the bone marrow is called medullary hematopoiesis
Extra medullary
Blood cell production in hematopoietic tissue other than bone marrow
Liver
Spleen
Compensatory mechanism to provide blood cells in times of need
This can lead to hepatomegaly andor splenomegaly (increase in size of the liver andor spleen because of increased functions in the organs)
bull Red blood cells ndashbull carry oxygen via hemoglobin
bull LeukocytesWhite Blood Cellsmake up the cells of the immune system
ndashbull These cells help clear parasites bacteria tumors debris-----
ThrombocytesPlateletsndashbullMust be present for clotting to occur
ndashbull Involved in hemostasis
Red Blood Cell (RBC) synthesis is known as Erythropoiesis
bull In erythropoiesis the hemocytoblast goes through a series of morphological changes culminating in the formation of a cell full of hemoglobin
Sizehellip Same size as the nucleus of a small lymphocyte that is 72 um
Cell shape round
Cytoplasm Pink
Center pallor Hemoglobin is comparatively less in the center showing central pallor on dried film13 size of the cell
Normal RBC suspended in fluid is biconcave
Transport oxygen from lungs to tissues and carbon dioxide from tissues to lungs
72
mm
The appearance of normal circulating blood is relatively uniform with little variation in size and shape Red blood cells will have an area of paleness in the center which is approximately one-third the diameter of the cell
Composed of hemoglobin
Erythropoiesis= RBC production
Stimulated by hypoxia
Controlled by erythropoietin
Hormone synthesized in kidney
Hemolysis= destruction of RBCs
Releases bilirubin into blood stream
Normal lifespan of RBC = 120 days
O
2
O
2
O
2
O
2
oxyhaemoglobin
19-18
Protect body against microorganisms and remove dead cells and debris
MovementsAmeboid
Diapedesis
Chemotaxis
Passive Immunity
Active Immunity
Antigen ndash Antibody
TypesNeutrophils Most common phagocytic cells destroy bacteria (60)
Eosinophils Detoxify chemicals reduce inflammation (4)
Basophils Allergic reactions Release histamine heparin increase inflam response (1)
Lymphocytes Immunity 2 types b amp t Cell types IgG-infection IgM-microbes IgA-Resp amp GI IgE- Allergy IgD-immune response
Monocytes Become macrophages
Basophil Eosinophil
Neutrophil
Lymphocyte
Monocyte
platelet
Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Medullary
Hematopoiesis in the bone marrow is called medullary hematopoiesis
Extra medullary
Blood cell production in hematopoietic tissue other than bone marrow
Liver
Spleen
Compensatory mechanism to provide blood cells in times of need
This can lead to hepatomegaly andor splenomegaly (increase in size of the liver andor spleen because of increased functions in the organs)
bull Red blood cells ndashbull carry oxygen via hemoglobin
bull LeukocytesWhite Blood Cellsmake up the cells of the immune system
ndashbull These cells help clear parasites bacteria tumors debris-----
ThrombocytesPlateletsndashbullMust be present for clotting to occur
ndashbull Involved in hemostasis
Red Blood Cell (RBC) synthesis is known as Erythropoiesis
bull In erythropoiesis the hemocytoblast goes through a series of morphological changes culminating in the formation of a cell full of hemoglobin
Sizehellip Same size as the nucleus of a small lymphocyte that is 72 um
Cell shape round
Cytoplasm Pink
Center pallor Hemoglobin is comparatively less in the center showing central pallor on dried film13 size of the cell
Normal RBC suspended in fluid is biconcave
Transport oxygen from lungs to tissues and carbon dioxide from tissues to lungs
72
mm
The appearance of normal circulating blood is relatively uniform with little variation in size and shape Red blood cells will have an area of paleness in the center which is approximately one-third the diameter of the cell
Composed of hemoglobin
Erythropoiesis= RBC production
Stimulated by hypoxia
Controlled by erythropoietin
Hormone synthesized in kidney
Hemolysis= destruction of RBCs
Releases bilirubin into blood stream
Normal lifespan of RBC = 120 days
O
2
O
2
O
2
O
2
oxyhaemoglobin
19-18
Protect body against microorganisms and remove dead cells and debris
MovementsAmeboid
Diapedesis
Chemotaxis
Passive Immunity
Active Immunity
Antigen ndash Antibody
TypesNeutrophils Most common phagocytic cells destroy bacteria (60)
Eosinophils Detoxify chemicals reduce inflammation (4)
Basophils Allergic reactions Release histamine heparin increase inflam response (1)
Lymphocytes Immunity 2 types b amp t Cell types IgG-infection IgM-microbes IgA-Resp amp GI IgE- Allergy IgD-immune response
Monocytes Become macrophages
Basophil Eosinophil
Neutrophil
Lymphocyte
Monocyte
platelet
Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

bull Red blood cells ndashbull carry oxygen via hemoglobin
bull LeukocytesWhite Blood Cellsmake up the cells of the immune system
ndashbull These cells help clear parasites bacteria tumors debris-----
ThrombocytesPlateletsndashbullMust be present for clotting to occur
ndashbull Involved in hemostasis
Red Blood Cell (RBC) synthesis is known as Erythropoiesis
bull In erythropoiesis the hemocytoblast goes through a series of morphological changes culminating in the formation of a cell full of hemoglobin
Sizehellip Same size as the nucleus of a small lymphocyte that is 72 um
Cell shape round
Cytoplasm Pink
Center pallor Hemoglobin is comparatively less in the center showing central pallor on dried film13 size of the cell
Normal RBC suspended in fluid is biconcave
Transport oxygen from lungs to tissues and carbon dioxide from tissues to lungs
72
mm
The appearance of normal circulating blood is relatively uniform with little variation in size and shape Red blood cells will have an area of paleness in the center which is approximately one-third the diameter of the cell
Composed of hemoglobin
Erythropoiesis= RBC production
Stimulated by hypoxia
Controlled by erythropoietin
Hormone synthesized in kidney
Hemolysis= destruction of RBCs
Releases bilirubin into blood stream
Normal lifespan of RBC = 120 days
O
2
O
2
O
2
O
2
oxyhaemoglobin
19-18
Protect body against microorganisms and remove dead cells and debris
MovementsAmeboid
Diapedesis
Chemotaxis
Passive Immunity
Active Immunity
Antigen ndash Antibody
TypesNeutrophils Most common phagocytic cells destroy bacteria (60)
Eosinophils Detoxify chemicals reduce inflammation (4)
Basophils Allergic reactions Release histamine heparin increase inflam response (1)
Lymphocytes Immunity 2 types b amp t Cell types IgG-infection IgM-microbes IgA-Resp amp GI IgE- Allergy IgD-immune response
Monocytes Become macrophages
Basophil Eosinophil
Neutrophil
Lymphocyte
Monocyte
platelet
Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Red Blood Cell (RBC) synthesis is known as Erythropoiesis
bull In erythropoiesis the hemocytoblast goes through a series of morphological changes culminating in the formation of a cell full of hemoglobin
Sizehellip Same size as the nucleus of a small lymphocyte that is 72 um
Cell shape round
Cytoplasm Pink
Center pallor Hemoglobin is comparatively less in the center showing central pallor on dried film13 size of the cell
Normal RBC suspended in fluid is biconcave
Transport oxygen from lungs to tissues and carbon dioxide from tissues to lungs
72
mm
The appearance of normal circulating blood is relatively uniform with little variation in size and shape Red blood cells will have an area of paleness in the center which is approximately one-third the diameter of the cell
Composed of hemoglobin
Erythropoiesis= RBC production
Stimulated by hypoxia
Controlled by erythropoietin
Hormone synthesized in kidney
Hemolysis= destruction of RBCs
Releases bilirubin into blood stream
Normal lifespan of RBC = 120 days
O
2
O
2
O
2
O
2
oxyhaemoglobin
19-18
Protect body against microorganisms and remove dead cells and debris
MovementsAmeboid
Diapedesis
Chemotaxis
Passive Immunity
Active Immunity
Antigen ndash Antibody
TypesNeutrophils Most common phagocytic cells destroy bacteria (60)
Eosinophils Detoxify chemicals reduce inflammation (4)
Basophils Allergic reactions Release histamine heparin increase inflam response (1)
Lymphocytes Immunity 2 types b amp t Cell types IgG-infection IgM-microbes IgA-Resp amp GI IgE- Allergy IgD-immune response
Monocytes Become macrophages
Basophil Eosinophil
Neutrophil
Lymphocyte
Monocyte
platelet
Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Sizehellip Same size as the nucleus of a small lymphocyte that is 72 um
Cell shape round
Cytoplasm Pink
Center pallor Hemoglobin is comparatively less in the center showing central pallor on dried film13 size of the cell
Normal RBC suspended in fluid is biconcave
Transport oxygen from lungs to tissues and carbon dioxide from tissues to lungs
72
mm
The appearance of normal circulating blood is relatively uniform with little variation in size and shape Red blood cells will have an area of paleness in the center which is approximately one-third the diameter of the cell
Composed of hemoglobin
Erythropoiesis= RBC production
Stimulated by hypoxia
Controlled by erythropoietin
Hormone synthesized in kidney
Hemolysis= destruction of RBCs
Releases bilirubin into blood stream
Normal lifespan of RBC = 120 days
O
2
O
2
O
2
O
2
oxyhaemoglobin
19-18
Protect body against microorganisms and remove dead cells and debris
MovementsAmeboid
Diapedesis
Chemotaxis
Passive Immunity
Active Immunity
Antigen ndash Antibody
TypesNeutrophils Most common phagocytic cells destroy bacteria (60)
Eosinophils Detoxify chemicals reduce inflammation (4)
Basophils Allergic reactions Release histamine heparin increase inflam response (1)
Lymphocytes Immunity 2 types b amp t Cell types IgG-infection IgM-microbes IgA-Resp amp GI IgE- Allergy IgD-immune response
Monocytes Become macrophages
Basophil Eosinophil
Neutrophil
Lymphocyte
Monocyte
platelet
Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

The appearance of normal circulating blood is relatively uniform with little variation in size and shape Red blood cells will have an area of paleness in the center which is approximately one-third the diameter of the cell
Composed of hemoglobin
Erythropoiesis= RBC production
Stimulated by hypoxia
Controlled by erythropoietin
Hormone synthesized in kidney
Hemolysis= destruction of RBCs
Releases bilirubin into blood stream
Normal lifespan of RBC = 120 days
O
2
O
2
O
2
O
2
oxyhaemoglobin
19-18
Protect body against microorganisms and remove dead cells and debris
MovementsAmeboid
Diapedesis
Chemotaxis
Passive Immunity
Active Immunity
Antigen ndash Antibody
TypesNeutrophils Most common phagocytic cells destroy bacteria (60)
Eosinophils Detoxify chemicals reduce inflammation (4)
Basophils Allergic reactions Release histamine heparin increase inflam response (1)
Lymphocytes Immunity 2 types b amp t Cell types IgG-infection IgM-microbes IgA-Resp amp GI IgE- Allergy IgD-immune response
Monocytes Become macrophages
Basophil Eosinophil
Neutrophil
Lymphocyte
Monocyte
platelet
Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Composed of hemoglobin
Erythropoiesis= RBC production
Stimulated by hypoxia
Controlled by erythropoietin
Hormone synthesized in kidney
Hemolysis= destruction of RBCs
Releases bilirubin into blood stream
Normal lifespan of RBC = 120 days
O
2
O
2
O
2
O
2
oxyhaemoglobin
19-18
Protect body against microorganisms and remove dead cells and debris
MovementsAmeboid
Diapedesis
Chemotaxis
Passive Immunity
Active Immunity
Antigen ndash Antibody
TypesNeutrophils Most common phagocytic cells destroy bacteria (60)
Eosinophils Detoxify chemicals reduce inflammation (4)
Basophils Allergic reactions Release histamine heparin increase inflam response (1)
Lymphocytes Immunity 2 types b amp t Cell types IgG-infection IgM-microbes IgA-Resp amp GI IgE- Allergy IgD-immune response
Monocytes Become macrophages
Basophil Eosinophil
Neutrophil
Lymphocyte
Monocyte
platelet
Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

19-18
Protect body against microorganisms and remove dead cells and debris
MovementsAmeboid
Diapedesis
Chemotaxis
Passive Immunity
Active Immunity
Antigen ndash Antibody
TypesNeutrophils Most common phagocytic cells destroy bacteria (60)
Eosinophils Detoxify chemicals reduce inflammation (4)
Basophils Allergic reactions Release histamine heparin increase inflam response (1)
Lymphocytes Immunity 2 types b amp t Cell types IgG-infection IgM-microbes IgA-Resp amp GI IgE- Allergy IgD-immune response
Monocytes Become macrophages
Basophil Eosinophil
Neutrophil
Lymphocyte
Monocyte
platelet
Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Basophil Eosinophil
Neutrophil
Lymphocyte
Monocyte
platelet
Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Cell fragments pinched off from megakaryocytes in red bone marrow
Important in preventing blood loss
Platelet plugs
Promoting formation and contraction of clots
Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Abnormalities of Haematopoiesis and resulting Blood disorders can affect any of the three main components of blood
Red blood cells which carry oxygen to the bodys tissues
White blood cells which fight infections
Platelets which help blood to clot
Blood disorders affect one or more parts of the blood and prevent your blood from doing its job They can be acute or chronic Many blood disorders are inherited Other causes include other diseases side effects of medicines and a lack of certain nutrients in your diet
Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Under normal conditions the production release and survival of blood cells is a highly regulated process Quantitative andor qualitative hematologic abnormalities may result when there is an imbalance between cell production release andor survival
Age sex and geographic location are involved in physiologic changes in normal values of the formed cellular elements
Normal values for a group are determined by calculating the mean for healthy individuals of the group and reporting the normal range as the mean +- 2 standard deviations
19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

19-24
The changes caused by disease may be detected by lab tests that measure deviations of the blood constituents from the normal values These lab test may include
Type and cross match
Complete blood count
Red blood count
Hemoglobin measurement
Hematocrit measurement(packed cell volume)
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin concentration (MCHC)
White blood count
Differential white blood count
Platelet count
Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Radiologic Studies
CTMRI of lymph tissues
Biopsies
Bone Marrow examination
Lymph node biopsies
Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Common Laboratory Tests for Hematologic and Lymphatic Disorders
19042011 28
19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

19042011 29
RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

RBC
Anemiasndashldquolacking bloodrdquo
Polycythemiandashldquomany blood cellsrdquo
WBC
Leukopeniandashlow white blood cell count
bull Leukemiandashhigh white blood cell count
ndash Acute quickly advancing blast--‐type cells
ndash Chronic slowly advancing more mature cells
Platelets
Thrombocytopenia
Thrombocytosis
ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

ErythrocytesRed Blood Cells
Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Definition of Anaemia
Reduction of haemoglobin concentration or red blood cell (RBC) volume below the range of normal values
Means and ranges of normal haemoglobinvaries with age and sex
Anaemia is not a diagnosis but sign of a disease which should be investigated
Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Normal Mean amp Lower Limits of Normal Hb HCT amp MCV
AGE (YR) HEMOGLOBIN(GDL)
Mean Lower Limit
HEMATOC RIT ()
Mean Lower Limit
MCV (Μm3)
MCV (fL) 70+ Age
(years)
Mean Lower Limit
Newborn 168 140 55 45 119 110
05-19 125 110 37 33 77 70
2-4 125 110 38 34 79 73
5-7 130 115 39 35 81 75
8-11 135 120 40 36 83 76
12-14 female 135 120 41 36 85 78
12-14 male 140 125 43 37 84 77
15-17 female 140 120 41 36 87 79
15-17 male 150 130 46 38 86 78Dr M KASHIF ISHAQI
What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

What happens in anaemia O2 carrying capacity of the blood
Increase cardiac output augmented oxygen extraction and shunting of blood flow towards vital organs and tissues
Increased concentration of 23-diphosphoglycerate within RBC with resultant right shift of the oxygen dissociation curve
Few physiological disturbances occur until Hb lt 80gL
Pallor only evident when Hb lt 80gL
Younger children less symptoms and signs
Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Symptoms amp signs of anaemiaSymptoms
Pallor
Lethargy amp irritability
Decreased exercise tolerance shortness of breath
Dizziness
Signs
Pale mucous membrane amp palmar creases
Tachycardia
Tachypnea
Flow murmur
Cardiac failure (severe anaemia)
Other signs related to underlying disease process
destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

destructionproduction
factory
Pathological classification
Substrate (Ineffective erythropoiesis)
Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Pathological classification
1 Inadequate production of RBC in the bone marrow
RBC precursors in the bone marrow (red cell aplasia)
eg Diamond Blackfan syndrome
Aplastic Anemia
Deficiency of specific factors
eg iron folate B12 deficiency
Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Pathological classification
2 Increased destruction of RBC
Intrinsic abnormalities of RBC
eg hereditary spherocytosis thalassaemia sickle cell anaemia
Immune mediated
eg autoimmune haemolytic anaemia Rhesus or ABO isoimmunization drugs
Dr M KASHIF ISHAQI
Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Dr M KASHIF ISHAQI
Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Anaemia
History
Physical examination
Laboratory Criteria
Age PrematuritySex x-linked eg G-6PD def Diet Iron early cow goat milk vegetarian motherJaundice pallor Dark colored urineGallstonesCholecystectomy TrasfusionSplenectomy chronic illness blood lossDrugs Pica Fava BeanFamily history
Pale Yellow sclera Visceromegaly LymphadenopathySigns of Nutritional deficiencyCongenital malformation
CBC HB WCC
MCV PLT Polys
Peripheral SmearRetics Count
BilirubinUnconjugated LDH Haptoglobin Urine DR
Dr M KASHIF ISHAQI
Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Low Hb=Anemia
MCV
Low
microcytic
Normal
normocytic
High
macrocytic
Measure Ferritin
Low Normalhigh
Iron def
Anemia
Anemia of
chronic disease
Congenital Hb dis
Reticulocyte count
high low Anemia of chronic disease
Renal failure
Marrow failure
Hemolytic anemia or
blood loss
Measure B12 + folate
Low
Megaloblastic
anemia
Normal
Dr M KASHIF ISHAQI
Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Sickle Cell
bull Red cells with pointed endsbull Crescent shapebull No central pallorbull Very dense hemoglobin
Key features
Associated disease
Hemoglobin SS
Hemoglobin SC
Hemoglobin SD
S- beta thalassaemia
Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Thalassaemia
1048697 Thalassemia spectrum of diseases characterized by
reduced or absent production of one or more globin chains
1048697 Disrupts the ratio of alphabeta production
- thalassaemia
Defect in globin chain synthesis
- thalassaemia trait - thalassaemia major
Low MCV
Trait Major
MCV
Hb N or sl
Hb elect HbA2 no A HbF
White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

White blood cellsWBC
Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

Most common malignant neoplasms in childhood (41 of all malignancies in children lt15 yrs of age)
Acute lymphoblastic leukemia (ALL) 77Acute myelogenous leukemia (AML) 11Chronic myelogenous leukemia (CML) 2ndash3Juvenile chronic myelogenous leukemia (JCML) 1ndash2 Chronic lymphoblastic leukemia (CLL) rare
Leukemias a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to an unregulated clonal proliferation of cells
These cells have a growth advantage over normal cellular elements because of
Proliferate uncontrolledFail to respond to normal growth inhibition mechanismsDo not undergo apoptotic changesInfiltrate normal organs
Leukemia
ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

ALL Clinical Presentations
General Malaise anorexia
Anemia
Neutropenia
Thrombocytopenia
Bone marrow infiltration
Pallor lethargy
Infection
Bruising petechiae nose bleeds
Bone pain
Reticulo-endothelial infiltration
Hepatosplenomegaly
Lymphadenopathy superior mediastinal obsruction
Other organInfitration
CNS
Testes
Headaches vomiting convulsions nerve palsies
Testicular enlargement
Rare at diagnosis more often at relapse
ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

ALL subtypes
Subtypes Descriptions
THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

THROMBOCYTESPLATELETS
THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus

THROMBOCYTOPENIA
DRUG INDUCED
BONE MARROW FAILURE
Viral Infections
Chemotherapy amp Radiation Therapy
Infiltration of Abnormal Cells
Aplastic Anemia
Leukemia
Metastatic Cancer
HYPERSPLENISM
OTHER CAUSESIdiopathic Thrombocytopenia Purpura (ITP)
HIV Virus