Embed Size (px)
Citation preview

The physical basis of medical imaging
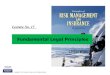
Technology is an essential element of our society.Medical imaging began on November 8, 1895, whenProfessor Wilhelm Conrad Roentgen of the Universityof Würzburg discovered X-rays. There have beennumerous refinements of X-ray techniques over thepast 100 years with development of invasive radiologyand computed tomography (CT). In addition, entirenew modalities have appeared including nuclearmedicine, ultrasonography, magnetic resonanceimaging [1]. The “4 sisters” of cardiac imaging havevery different biological and technological basis. It isimportant to operate a distinction, which is alsorelevant for the legal regulations of medical imagingbetween “ionising” and “non-ionising” techniques.Ionising techniques use high frequency electromagne-tic waves, such as X-rays (radiology) and gamma-rays(nuclear medicine). Ionising radiations are only onepart of the electromagnetic spectrum (Fig. 1).
There are numerous other radiations (e.g., visiblelight, infrared waves, radiofrequency electromagneticwaves) that do not posses the ability to ionise atoms ofthe absorbing matter. According to the general equationE = h·v radiation energy (E) is directly proportional tofrequency (v). Higher energies can be toxic to the cellthrough the production of free radicals. Obviously, theuse of high energies has also several advantages,including the possibility to go inside the body withoutobstacles represented by bone and air. However, what isimportant here is that these energies (employed innuclear medicine and radiology) have some environ-mental and biohazards impact: for sake of simplicity, wemight call them “red” imaging techniques. As always inmedicine, a responsible use of these technologies clearlyoutweighs the risk. Other technologies employed incardiac imaging pose no environmental burden orknown risk to the patient or to the operator [1]. Theyinclude magnetic resonance, which uses low frequencyelectromagnetic waves and ultrasound. Ultrasonography
Ann Ist Super Sanità 2003;39(2):205-212
Indirizzo per la corrispondenza (Address for correspondence): Eugenio Picano, Istituto di Fisiologia Clinica, Consiglio Nazionale delleRicerche, Via Moruzzi 1, 56124 Pisa. E-mail: [email protected].
Principle of responsibility in medical imaging
Anna SUHOVA (a), Vladislav CHUBUCHNY (b) and Eugenio PICANO (b)
(a) Scuola Superiore Sant’Anna, Università degli Studi, Pisa, Italy (b) Istituto di Fisiologia Clinica, Consiglio Nazionale delle Ricerche, Pisa, Italy
Summary. - Radiological and medico-nuclear procedures are an essential part of contemporary medicine.They employ ionising energy, differently from other imaging modalities such as echography or magneticresonance. The use of ionising testing is therefore associated to environmental impact and definite biorisks forthe patient and the operator. In many clinical conditions specialty guidelines accept the equivalence of medicalinformation provided by “red” (ionising) and “green” (noionising) techniques. Medical equivalence istranslated into physician freedom of choice. However, common sense, guidelines of Radiological MedicalSocieties and Euratom directive (incorporated in national laws, such as Italian law 187/26 of May 2000)suggest that a “red” technique should be used only when a “green” alternative is not competitive.
Key words: imaging, law, responsibility.
Riassunto (Il principio di reponsabilità nell’imaging medico). - Nell’imaging medico coesistonometodiche “verdi” (risonanza magnetica e ultrasuoni, innocue per il paziente e l’operatore, prive di impattoambientale) e “rosse” (radiologia e medicina nucleare, basate su radiazioni ionizzanti e quindi con debitoecologico e biorischi). In molte situazioni cliniche le linee guida delle società specialistiche equiparanometodiche rosse e verdi, lasciando libertà di scelta. Ma se non si percepisce la differenza d’innocuità traimmagine rossa e verde si delinea un bizzarro caso di daltonismo dell’immagine con conseguenze devastanti.L’immagine rossa dovrebbe essere usata solo quando quella verde non è competitiva. Lo suggeriscono le lineeguida delle grandi società mediche radiologiche e lo imporrebbero la legge europea (Direttiva Euratom 97/43)e quella italiana (187/26 maggio 2000).
Parole chiave: imaging, legge, responsabilità.

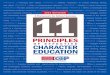
employs acoustic (mechanical) waves. Both these formsof physical energy are not capable to produce ionisingphenomena (Fig. 1). For sake of clarity, we might callthem “green” imaging techniques, with no environ-mental impact or associated biorisks.
Medical imaging, risk and environment
The increased complexity of technology and thepace of scientific progress might cause an increasednumber of risks. The use of radiological investigationsis an accepted part of medical practice, justified in termsof clear clinical benefits to the patient which should faroutweigh the small radiation risks. However, even smallradiation doses are not entirely without risk. A smallfraction of the genetic mutations and malignant diseasesoccurring in the population can be attributed to naturalbackground radiation. Diagnostic medical exposures,being the major source of man-made radiation exposureof the population, add about one sixth to the populationdose from background radiation [1-5].
The total effective dose (expressed in milliSievert[mSv]) received by an average person in the UnitedStates is 2.8 mSv per year: 2.4 mSv from natural sourcesand 0.4 mSv from man-made sources [2]. In 1987,the National Council of Radiation Protection andMeasurements estimated that nuclear medicine testsaccounted for 4% and X-ray testing of 11% of the totalradiation exposure of the average person in the UnitedStates [2]. Since 1987, the number of nuclear cardiologystudies has more than doubled in the country [6] and thenumber of radiological examinations also increasedsharply [7]. In the whole world, an estimated number of400 million of radiological procedures and 25 million ofnuclear medicine procedures were performed in 2002
[7]. Seven million nuclear cardiology studies withunsealed sources of radionuclides are performed eachyear in the United States, accounting for more than 50%of all nuclear imaging [6].
At the patient level, the effective dose of a singlenuclear cardiology stress procedure ranges from 23 mSvfrom a thallium scan to 10 mSv from a technetium 99mmethoxyisobutylisonitrile scan [3, 4] (Table 1, 2).
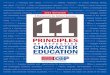
According to data provided by the InternationalCommission on Radiological Protection, this exposuredose corresponds to an additional risk of cancer that isbetween 1 in 1000 and 1 in 10 000 [8-11]. A singleexposure to 0.01 mSv (a chest radiograph, for instance)corresponds to an average loss of 2 minutes of lifeexpectancy, whereas a single exposure to 10 mSvcorresponds to 2 days of lost life expectancy [3, 10, 11](Table 3; Fig. 2).
The doses from positron emission tomography(PET), cardiac stress scintigraphy and CT examinationsare particularly high, show no sign of decreasing and theuse of these modalities is still rising [7]. PET and CTnow probably contribute almost half of the collectivedose from all X-ray examinations with ionisingradiations [1]. It is thus particularly important thatrequests for these methods are thoroughly justified [12].
Precautionary principle
Therefore, preventive action becomes veryimportant since in many cases scientific certainty aboutharmful effects of certain product or service only existsafter the damage has been suffered.
The precautionary principle is based on thisexistence of scientific uncertainty. A part of thisuncertainty is inherent to the reality and caused by the
Anna SUHOVA, Vladislav CHUBUCHNY and Eugenio PICANO206
Fig. 1. - Electromagnetic and acoustic spectrum. Only high energy electromagnetic waves (used in radiology andnuclear medicine) are ionising.
Electromagneticspectrum
Radio-waves
Acoustic waves
Magneticresonance
audible range
visiblerange
Radiology Nuclearmedicine
X-rays y-rays
Echography
1 MHz 5 MHz 10 MHz
106 109 1014 1014 10284.1 * 7.5 *
20 000
5 *
Frequency(hertz)

PRINCIPLE OF RESPONSIBILITY IN MEDICAL IMAGING
coincidences determining future. Another part is linkedto the scientific methods. Because it is not possible toexamine all possible hypotheses, certain degree ofuncertainty always exists about scientific results. Lawbased on the precautionary idea has to convert thisscientific uncertainty into social certainty [13].
The precautionary idea was originally accepted asa policy principle in environmental protection law. Theprecautionary principle became especially popular inthis field because of the many scientific uncertainties,such as the difficulties to determine a causal relationbetween pollution (ionising radiation) and harmfuleffects and the fact that long-term consequencescannot be subject to experimental research [14]. Theprecautionary idea means that protective action can benecessary despite scientific uncertainty about harmfuleffects of a certain application or product in case ofpotential risks.
In a communication, the European Commissionexplicitly considers precaution to be a policy principlefor the European institutions, not only in environ-
207
Table 1. - Typical effective doses from diagnostic medical exposures in the 1990s
Diagnostic procedure Typical effective dose Equivalent no. Approximate equivalent period (mSv) of chest X-rays of natural background radiation (*)
X-ray examinations:Limbs and joints (except hip) <0.01 <0.5 <1.5 daysChest (single PA film) 0.02 1 3 daysSkull 0.07 3.5 11 daysThoracic spine 0.7 35 4 monthsLumbar spine 1.3 65 7 monthsHip 0.3 15 7 weeksPelvis 0.7 35 4 monthsAbdomen 1.0 50 6 monthsIVU 2.5 125 14 monthsBarium swallow 1.5 75 8 monthsBarium meal 3 150 16 monthsBarium follow through 3 150 16 monthsBarium enema 7 350 3.2 yearsCT head 2.3 115 1 yearCT chest 8 400 3.6 yearsCT abdomen or pelvis 10 500 4.5 years
Radionuclide studies:Lung ventilation (Xe-133) 0.3 15 7 weeksLung perfusion (Tc-99m) 1 50 6 monthsKidney (Tc-99m) 1 50 6 monthsThyroid (Tc-99m) 1 50 6 monthsBone (Tc-99m) 4 200 1.8 yearsDynamic cardiac (Tc-99m) 6 300 2.7 yearsPET head (F-18 FDG) 5 250 2.3 yearsCardiac stress scintigraphy (Tc-99m) 10 500 4.5 yearsCardiac thallium scintigraphy 23 1150 10 years
(*) UK average background radiation = 2.2 mSv/year: regional averages range from 1.5 to 7.5 mSv/year. IVU: intravenousurography; CT: computed tomography. Adapted from [1].
Table 2. - Classification of the typical effective doses ofionising radiation from common imaging procedures [1]
Class Typical effective ExamplesDose (mSv)
0 0 US, MRI
I < 1 CXR, limb XR, pelvis XR
II (*) 1-5 IVU, lumbar spine XR, NM (e.g. skeletal scintigram), CT head & neck
III 5-10 CT chest and abdomen, NM (e.g. cardiac)
IV > 10 Some NM studies (e.g., cardiac thallium scintigraphy)
(*) The average annual background dose in most parts of Europefalls in Class II. US: ultrasound; MRI: magnetic resonanceimaging; CXR: chest X-ray; XR: X-ray; IVU: intravenousurography; NM: nuclear medicine; CT: computed tomography.

mental protection law but also for health and consumerprotection [15]. At the European level, the only explicitreference to the principle is made in the context ofenvironmental protection (art. 174 EU-Treaty). TheEU-Treaty provides that "a high level of human healthprotection shall be ensured in the definition andimplementation of all community policies andactivities" (art. 152 [1]). The Court of Justice and theCourt of First Instance of the European Union considerthese articles to be sufficient grounds for theapplication of the precautionary principle [16]. Thusvia the codification into law systems the precautionaryprinciple has developed from a policy guideline into alegal rule [17]. Precautionary principle can beinterpreted in different ways, more aggressive(“uncertainty requires shifting the burden and standardof proofs”), more conservative (“uncertainty does notjustify inaction”) or somewhat intermediate(“uncertainty justifies action”) [18]. However, there isno doubt that the precautionary principle regards
technologies of questionable (doubtful) environmentaland biohazard impact. In case of ionising testing, thisnegative impact is beyond doubt - although muchdebate exists on the amount of the harmful effect [5].A conservative and restrictive use of thesetechnologies is therefore highly desirable.
Responsibility in medical imaging diagnostics
In the European Community, a 97/43 EuratomDirective for nuclear medicine (97/43) establishes thatindication and execution of diagnostic proceduresshould follow three basic principles: the justificationprinciple (art. 3), the optimization principle (art. 4),and the responsibility principle (art. 5) [19]. Anyresponsible prescription of a nuclear test today shouldfollow these principles [12].
Art. 2 of the 97/43 Euratom Directive defines theclinical responsibility as “responsibility regardingindividual medical exposures attributed to apractitioner, notably: justification; optimization;clinical evaluation of the outcome; cooperation withother specialists and the staff, as appropriate, regardingpractical aspects; obtaining information, if appropriate,of previous examinations; providing existingradiological information and/or records to otherpractitioners and/or prescribers, as required; givinginformation on the risk of ionising radiation to patientsand other individuals involved, as appropriate” [19].
The patient, the cardiologist, and the referringphysician should be aware of the risks, costs, andenvironmental impact of this “subjective” choice, evenif quantification of these negative effects of low-levelradiation remains a challenge [20].
These considerations are also somewhat mirroredin the guidelines developed by the InternationalCommission on Radiological Protection, whoserecommendations form the basis of legislation in manycountries [11], and of the International Basic SafetyStandards issued by the International Atomic EnergyAgency [21]. In Italy, a 1995 law (art. 111, DL 230/95)
Anna SUHOVA, Vladislav CHUBUCHNY and Eugenio PICANO208
Table 3. - Radiation doses and estimated cancer risk from common radiological examinations and isotope scans [3,12]
Type of test Effective radiation dose Equivalent period Lifetime additional risk(mSv) of natural background of cancer per examination
Radiation
Chest radiograph 0.01 A few days Negligible riskSkull radiograph 0.1 A few weeks Minimal risk
(1 in 100000 to 1 in 1000000)Breast (mammography) 1 A few months to a year Very low riskCardiac gated study 10 A few years Low riskCardiac thallium scan (1 in 1000 to 1 in 10000)
mSv: milliSievert.
Fig. 2. -Typical effective doses from diagnostic medicalexposures. Adapted from [12].

PRINCIPLE OF RESPONSIBILITY IN MEDICAL IMAGING
states that a nuclear examination may be performedonly when it cannot be replaced by other techniquesthat do not employ ionising radiation [22].
The Council Directive 97/43 Euratom implies thatall new types of radiological practices (includingnuclear medicine) shall be justified. It clearly means thatif an exposure cannot be justified, it should beprohibited (art. 3). All well-established nuclear medicinepractices must be reviewed in the light of new dataabout their efficacy and consequences. Consequently,dosimetry should become a key element in thecompetition with other "radiologic" techniques. Thewinner will be the patient who will benefit from the bestindications of examinations with ionising radiations andwill escape from unnecessary exposures [23-26].
To the principle of justification it is necessary toadd the right of the patient to be informed aboutpotential risks of procedure, in particular, thatradionuclide isotopes increase the incidence of cancerin a different fashion and in relation of the isotopeused: for instance, for cardiac stress perfusionscintigraphy with a risk of fatal cancer ranging from1.2 out of 1000 to 2.5 out of 10 000 cases [2, 3].
By way of precaution in the Euratom Directives onradiological protection (97/43) has been adopted theALARA-principle. This principle describes that the doseof harmful exposure has to be kept as low as reasonablyachievable, economic and social factors being taken intoaccount. As a consequence, this principle was imple-mented in national legislations [13-15].
Because safety does not mean risk free, it wouldnot be reasonable to aim for a "zero-risk" situation.The optimization or ALARA-principle avoids takingprotective measures if the benefits are smaller than theeconomical or social burden. M.C. Boehler [16]mentioned that because of the precautionary principle,law in the field of radioprotection does no longer servescience but promotes ethical responsible conduct inour insecure world. The linear model is no translationof scientific knowledge but an intellectual constructionserving as a basis to take measures.
The ALARA-principle has to be applied byindividuals and companies on a case-by-case basis. Thepolicy options that, in accordance to the precautionaryprinciple, were taken by government have beentransferred by the ALARA-principle to companies andindividuals. All imaging departments should haveprotocols for each common clinical situation. Theprinciple does not impose specific and detailed obligationsbut can be considered a demand for self-regulation. Inreferral guidelines for imaging stated that all examinationsshould be optimised to obtain maximum information withthe minimum of radiation [1]. Standardization seemsnecessary to guarantee a correct application of theprecautionary principle. Since the recent Euratomdirectives have stimulated the promulgation of diagnosticreference levels in case of medical exposure and doseconstraints, this demand is explicitly put forward.
The Council Directive 97/43 Euratom (art. 5)implies that both the referring physician ordering thenuclear medicine test (the prescriber) and thephysician performing the test (the practitioner) areresponsible for the justification of the test exposing thepatient to ionising radiations [19].
The practical aspects for the procedure or part of itmay be delegated by the holder of the radiologicalinstallation or the practitioner, as appropriate, to one ormore individuals entitled to act in this respect in arecognized field of specialization.
Most equipment used in medical establishmentshas achieved a high degree of sophistication, and itsfaultless operation is decisive in making good medicaldiagnosis. In this respect, quality control or, in otherwords, regular “checks” are absolutely necessary andconstitute a major part of the physicist’s professionalresponsibility. All failures in providing uninterruptedcare may not only be a cause of concern for doctorsand patients, but may also involve problems of legalresponsibility. There is no excuse for any negligence orcarelessness, especially when radioisotope or radiationtherapy is employed [27].
Decision-making process
The European Commission is aware of thenecessity of a structured decision-making process. Inthe recent communication [15] stated that theEuropean Commission have to find the correct balancebetween the freedom and rights of individuals,industry and organizations on the one hand andenvironment, human, animal and plant health on theother hand. If this balance is found, proportionate, non-discriminatory, transparent and coherent actions can betaken. This communication is a first step to establishguidelines for applying the precautionary principle.
According to the European Commission, astructured decision-making process is provided by thethree elements of risk analysis: risk assessment, riskmanagement and risk communication.
Before adequate measures can be taken, a scientificevaluation has to be performed as good as possible.This risk assessment requires reliable scientific dataand logical reasoning, leading to a conclusion, whichexpresses the possibility of occurrence and the severityof a hazard's impact on environment or human, animaland plant health. It will cast light on the objectiveevidence, the gaps in knowledge and the scientificuncertainties.
The procedure to evaluate the policy options has tobe as transparent as possible. Dab stresses thatformalization of the decision-making process andpublic involvement become more important withincreasing uncertainty. The most unacceptable,
209

according to Dab, is not that the decision-maker ismistaken in this context of uncertainty, but that hisapproach is not transparent, coherent and explicit. Inthat case, he can lose faith if he is accused to havesacrificed health for economical reasons [28].
Prescribing physicians should be aware that theirchoices place economic and biohazard burdens on theplanet and the patient. Art. 3 of the 97/43 EuratomDirective stated that “medical exposure shall show asufficient net benefit, weighing the total potentialdiagnostic or therapeutic benefits it produces,including the direct health benefits to an individual andthe benefits to society, against the individual detrimentthat the exposure might cause, taking into account theefficacy, benefits and risks of available alternativetechniques having the same objective but involving noor less exposure to ionising radiation”.
Professional and legal responsibilities of medicalphysicists may be expected to grow in directproportion to the increased scope of physics andengineering methods and techniques to be applied inmedicine in future [27].
In every case of medical imaging diagnostics thechoice should be made in favour of the most harmlessand risk-free method. Accordingly among wide rangeof imaging modalities, ultrasound has been recom-mended as the appropriate investigation whereverpossible. Because ultrasound avoids ionising radiationand is relatively inexpensive, it is often recommendedwhere more expensive studies (e.g. CT) cannot bejustified or resources are limited [1]. The unexpensive,quick, reliable and non-invasive nature of ultrasoundmakes it an excellent initial investigation for a vastmajority of clinical referrals.
Although ultrasound technology is improvingsteadily, an alternative technique is needed for“acoustically hostile” patients. For these patients, fastmagnetic resonance imaging, which incorporates thebest aspects of nuclear and ultrasound scanning, canprovide an accurate second-line choice [12].
Because MRI does not use ionising radiation, MRIshould be preferred where both CT and MRI wouldprovide similar information and when both areavailable.
Why good medical practice by law?
In reality, at least 1 out of 4 ionising exams areinappropriate [29], and many more might be replacedby non-ionising procedures of comparable clinicalvalue [1]. This has created concerns for public healthbecause of radiation doses associated with unnecessaryexams [30-32]. There are at least three extra-scientificconditions, which may modulate prescription patterns:economic induction, medical lobbying, and inadequateperception of radiation risk by the prescriber.
Economic induction to prescription may modulatetesting. The imaging market consists of 600 millionprocedures every year. In 2001, over 100 million scanswere performed with a medical diagnostic productworldwide, generating UK £ 2.5 billion in revenue forthe manufacturers of contrast agents [7]. Economicinduction to prescription exists and usually it is morepervasive for more expensive diagnostic services [29].In addition, in many centres patients have access tosuch studies without physician referral [33].
Medical imaging superspecialists are expensively -and lifelong - trained to do one single thing. Forinstance, an imaging specialist has to undergo 6 yearsof medical school and 3 years of internship andadditional 4 to 5 years of imaging fellowship. Foracademic qualification, an additional 3 year PhDprogram is helpful. Basically, the uneventful training isstarted at the age of 19 and ends sometimes between 35and 40 years. At that time, the situation in the imagingmarket can be totally different from what it was at thebeginning, and emerging techniques may be at risk ofbecoming obsolete and non-competitive in somefields, due to the birth and growth of alternativemodalities [12]. Nevertheless, trained specialists existand must be kept alive. This makes a timelyreallocation of human and economic resources asensitive and not bloodless issue. According to aneminent cardio-pathologist, Giorgio Baroldi, “thespecialist falls in love with the only technique, better ifsophisticated, that he is able to master and must defendit if he wants to justify his survival, production,success and audience - and he becomes dangerous”[34]. Unfortunately we, the imaging experts, are allsuper- specialists. Last - and probably not least - manyclinicians and researchers working with patients withcardiovascular disease may not yet be familiar with theradiation doses that are received with the differentexaminations [33]. In addition, for the very sameexamination such as for instance computedtomography of the heart, radiation doses may differwidely [33]. To further complicate matters, radiationdose estimates can be expressed in various ways and itis not always clear in elite publications - not to speakof clinical practice - which parameters are used [33].Even more confusing, some guidelines - such as thosereleased by the UK Radiological Society and endorsedby European Union - clearly state that, generallyspeaking, a non-ionising exam should always bepreferred to a ionising exam - when information iscomparable [1]. Other guidelines issued by specialistsocieties, such as cardiological societies, overtly statethat the information provided by nuclear cardiologyand echocardiography (in evaluating cardiac function,myocardial viability, inducible ischemia andprognosis) is comparable and therefore … “the choiceof which test to perform depends on issues of localexpertise, available facilities and considerations of
Anna SUHOVA, Vladislav CHUBUCHNY and Eugenio PICANO210

PRINCIPLE OF RESPONSIBILITY IN MEDICAL IMAGING
cost-effectiveness” [35]. No mention is made ofenvironmental impact, biohazard and responsibility.Accuracy of “green” and “red” techniques is alsoconsidered largely comparable in other disease, suchas cancer detection. Yet, guidelines suggest that theycan be used without difference or preference: forinstance, American Cancer Society Guidelines forcancer detection recommend for colorectal cancerscreening flexible sigmoidoscopy or double-constrastbarium enema or colonscopy [36]. But colonscopy andsigmoidoscopy are “green”, and double-constrastbarium enema is “deep red”! The consequence is adaltonic Pontius Pilate - like hand washing withserious potential impact on public health.
To make things even more confusing, the “bestavailable evidence” of radiological risk estimation isprovided by the International Commission ofRadiological Protection [3, 4]. Such estimation isreferred to in the legislation of many countries,including Italy [22, 26] and European Union [19].Guidelines of the radiological society refer to thisestimation of risk [1]. And yet, such estimation isovertly challenged by other societies and distinguishedscientists working in the field [37]: “the internationalconsensus in that there are no major health risksassociated with diagnostic utilization of radio pharma-ceuticals. Moreover, the metrics that have been used toestimate the hypothetical risk have no relation tomodern medicine or accepted biological principles”.Maybe Michael Crichton - a writer and a Harvard-laureate physician - was right in stating that “medicalwriting is a highly skilled, calculated attempt toconfuse the reader” [38]. It is interesting to notice theInternational Agency for Research on Cancer found in2000 “sufficient evidence for carcinogenicity inhumans” of X-radiation and γ-radiation. The primaryexposure to these sources are “past use of atomicweapons and medical uses of radiations”. On the basisof this evidence, the National Institute ofEnvironmental Health Sciences nominated X-radiationand γ-radiation to the National Toxicology Programtogether with other 16 different substances. Thecommittee is scheduled to put the 17 substances into 1of 3 categories: known human carcinogen; reasonablyanticipated to be a carcinogen; insufficient evidence.The 11th Report on carcinogens is due for release inthe winter of 2004. The listing as a carcinogen “ ismeant to alert congress, regulating agencies and others,including the public, to see if current limits, labelling,etc. are sufficient to safeguard the public” [39].
Conclusions
Physicians and patients should always evaluate thecost-benefit and the risk-benefit ratios of their actions,not only the benefit. For instance, the radiation risk of
mammography is very low. In a population of 1million, one would expect 800 occult, naturallyoccurring cancers and only 1-3 cancers induced bymammography [40]. However, not always in clinicalpractice the benefit clearly outweighs risk. A usefulinvestigation is one in which the result - positive ornegative - will alter management or add confidence tothe clinician's diagnosis. A significant number ofradiological and mediconuclear investigations do notfulfil these aims and may add unnecessarily to patientirradiation due to repeating investigations which havealready been done, doing the wrong or inappropriateinvestigation.
The European law accepts high level of individualand environmental protection and adopts tight legalregulation criteria trying to restrict access to ionisingtesting to strictly needed indications. In everydaypractice, the application of the law is tempered bydiffuse ignorance of European legislation and thereforelack of its implementation into medical recommenda-tions and guidelines. Tighter interaction between legaland medical regulatory bodies is necessary to enhancethe level of social protection from “friendly fire” ofradiological and nuclear medical testing.
Received on 5 March 2003.Accepted on 12 May 2003.
REFERENCES
1. European Commission. Referral guidelines for imaging.Bruxelles: EC; 2001. (Radiation Protection, 118). 125 p.
2. National Council on Radiation Protection and Measurements.Ionising radiation exposure of the population of the UnitedStates. Bethesda, MD: National Council on Radiation Protectionand Measurements; 1987. (NCRP Report, 93).
3. International Commission on Radiological Protection (ICRP).Radiation and your patient: a guide for medical practitioners. Aweb module produced by Committee 3 of the ICRP. Oxford, UK:Pergamon Press; 2001.
4. International Commission on Radiological Protection (ICRP).Radiological protection in biomedical research. Oxford, UK:Pergamon Press; 1991. (Annals of the ICRP Issue, 52).
5. Eckermann KF, Leggett RW, Nelson CB et al. Health Risks fromlow-level environmental exposure to radionuclides:radionuclide-specific lifetime radiogenic cancer riskcoefficients for the US population, based on age-dependentintake, dosimetry and risk models. Washington, DC: UnitedStates Environmental Protection Agency Office to Radiationand Indoor Air; 1998. (Federal Guidance Report, 13).
6. Underwood R. Clinical nuclear cardiology. Introduction.European Heart House. June 28-30, 2001. Available from:http://www.escardio.org/education/nuclear2002/introduction.pdf.Last visited 26/2/2003.
7. Nycomed Amersham Visionaries. Imaging market (2002).Available from: http://www.amersham.co.uk/ar2000/Visionaries/07a.html. Last visited 26/2/2003.
211

8. Overbeek F, Pauwels EKJ, Broerse JJ. Carcinogenic risk indiagnostic nuclear medicine: biological and epidemiologicalconsiderations. Eur J Nucl Med 1994;21:997-1012.
9. Overbeek F, Pauwels EKJ, Bloem JL, et al. Somatic effects innuclear medicine and radiology. Appl Radiat Isot 1999;50:63-723.
10. Cohen BL. Catalog of risks extended and updated. Health Phys1991;61:317-35.
11. Cormack J, Towson JEC, Flower MA. Radiation protection anddosimetry in clinical practice. In: Murray IPC, Ell PJ (Ed.).Nuclear medicine. Vol. 2. London, UK: Churchill Livingstone;1998.
12. Picano E. Stress echocardiography: a historical perspective. Am JMed 2003;114:126-30.
13. Lierman S. The legal application of the precautionary and ALARAprinciples. Available from: http://ean.cepn.asso.fr/pdf/ program4/An-Lierman.pdf
14. Belveze H. Les réflexions sur l'utilisation du principe deprécaution au niveau de l'Union Européenne. 1999-09-27.
15. Commission of the European Communities. Communication fromthe commission on the precautionary principle, 2000/02/02.europa.eu.int/comm/dgs/health consumer/library/pub.
16. Boehler MC. Le principe de précaution et la radioprotection. In:Proceedings Nuclear Inter Jura. Helsinki: 1997. p. 149.
17. Bodansky D. The precautionary principle in US environmentallaw. In: Interpreting the precautionary principle. London:Earthscan Publications Ltd; p. 219.
18. Wiener JB, Rogers MD. Comparing precaution in the UnitedStates and Europe. Available from: http://www.env.duke.edu/solutions/publications.html.
19. Council Directive 97/43/Euratom of 30 June 1997 on healthprotection of individuals against the dangers of ionising radiationin relation to medical exposure, and repealing Directive84/466/Euratom. Official Journal of the European Communities L180, 09/07/1997 p. 0022-0027.
20. United Nations Scientific Committee on the Sources and Effectsof Ionising Radiation. Report on the effects of atomic radiationto the general Assembly, 2000. Available from:http://www.UNSCEAR.org. Last visited 26/2/2003.
21. International Atomic Energy Agency. International basic safetystandards for protection against ionising radiations and for thesafety of radioactive sources. Vienna: International Atomic EnergyAgency; 1996. (IAEA Safety Series, 115).
22. Italia. Decreto Legislativo 17 marzo 1995, n. 230. Attuazione delledirettive 89/618/Euratom, 90/641/Euratom, 92/3/Euratom e96/29/Euratom in materia di radiazioni ionizzanti. GazzettaUfficiale, 13 giugno 1995.
23. Bourguignon M.H. Implications of ICRP 60 and the patientdirective 97/43 Euratom for nuclear medicine. QJ Nucl Med2000;44:301-9.
24. Hall EJ. Lessons we have learned from our children: cancer risksfrom diagnostic radiology. Pediatr Radiol 2002;32:700-6.
25. Benner DJ, Sawant SG, Hande MP et al. Routine screeningmammography: how important is the radiation - risk side of thebenefit - risk equation? Int J Radiat Biol 2002;78:1065-7.
26. Decreto Legislativo 26 maggio 2000, n. 187. Attuazione delladirettiva 97/43/ EURATOM in materia di protezione sanitariadelle persone contro i pericoli delle radiazioni ionizzanti connessead esposizioni mediche. Gazzetta Ufficiale n. 157, 7 luglio 2000.
27. Chomicki O.A. Professional and legal responsibility of amedical physicist. Medical physics world 2001;17(2).
28. Dab W. Précaution et santé publique. Le cas des champsélectriques et magnétiques de basse fréquence. In: Le principede précaution dans la conduite des affaires humaines. Paris:Fondation Maison des Sciences de l'Homme, Institut Nationalde la Recherche Agronomique; 1997. p. 210
29. Ron E. Ionising radiation and cancer risk: evidence fromepidemiology. Pediatr Res 2002;32:232-7.
30. Stanley RJ. Inherent dangers in radiologic screening. Am JRoentgenol 2001;177:989-92.
31. United States Food and Drug Administration. Center forDevices and Radiological Health. Whole body scanning: usingcomputed tomography (CT). Available from: http://www.fda.gov/cdrh/ct. Last visited 26/2/2003.
32. Conference of Radiation Control Program Directors. Homepage. Available at: http://www.crcpd.org. Last visited 26/2/2003.
33. Morin RL, Gerber TC, McCollough CH. Radiation dose incomputed tomography of the heart. Circulation 2003;107:917-22.
34. Baroldi G. About inflammation and atherosclerosis. G It Cardiol1995;1:241-5.
35. Gibbons RJ, Chatterjee K, Daley J, Douglas JS, Fihn SD, GardinJM, Grunwald MA, Levy D, Lytle BW, O'Rourke RA, SchaferWP, Williams SV, Ritchie JL, Cheitlin MD, Eagle KA, GardnerTJ, Garson A Jr, Russell RO, Ryan TJ, Smith SC Jr.ACC/AHA/ACP-ASIM guidelines for the management ofpatients with chronic stable angina. A report of the AmericanCollege of Cardiology/American Heart Association Task Force onPractice Guidelines (Committee on Management of Patients WithChronic Stable Angina). J Am Coll Cardiol 1999;33:2092-197.
36. American Cancer Society. Guidelines for early detection of cancer.Available at: www.americancancersociety. ASCnewscenter. Lastvisited: 14/2/2001.
37. Abbott BG, Zaret BL. Contemporary cardiology and hystericnucleophobia. Am J Med 2003;114:131-4.
38. Crichton M. Letter. N Engl J Med 1976:564.
39. Radiological Society of North America. Government may labelradiation as a carcinogen. Newsletter. March 2003. Availablefrom: www.rsna.org/publications/rsnanews/mar03/carcinogens-1.html. Last visited: 26/2/2003.
40. Weissleder R. Primer of diagnostic imaging. 2nd ed. St Louis:Mosby Publ; 1997.
Anna SUHOVA, Vladislav CHUBUCHNY and Eugenio PICANO212